Preoperative Evaluation of Hand Nerve Injuries: A Comprehensive Clinical Guide
Key Takeaway
The preoperative evaluation of hand nerve injuries demands a meticulous, systematic approach. Accurate assessment is frequently confounded by polytrauma, patient intoxication, or pediatric noncompliance. A thorough clinical examination must evaluate the mechanism of injury, sensibility, motor function, and sudomotor activity. Utilizing the Seddon and Sunderland classifications alongside precise sensory mapping ensures accurate diagnosis, dictates surgical timing, and establishes reliable prognostic expectations for functional recovery.
PREOPERATIVE ASSESSMENT OF HAND NERVE INJURIES
The evaluation of peripheral nerve injuries in the hand represents a critical juncture in orthopedic and hand surgery. A missed nerve injury can lead to devastating long-term functional deficits, chronic neuropathic pain, and severe medicolegal repercussions. The preoperative assessment must be exhaustive, systematic, and meticulously documented. However, the acute trauma setting frequently presents significant barriers to a pristine clinical examination.
Confounding Factors in the Acute Evaluation
At times, it is exceedingly difficult to evaluate the true extent of nerve injury in the traumatized hand. The examining surgeon must navigate a myriad of confounding variables that can obscure neurologic deficits. Factors that frequently interfere with the examination of the nerves in the hand include:
- Life- or Limb-Threatening Injuries: In the polytraumatized patient, adherence to Advanced Trauma Life Support (ATLS) protocols takes precedence. Severe hemorrhage, vascular compromise, or compartment syndrome may overshadow isolated peripheral nerve deficits.
- Altered Mental Status: Patient intoxication (alcohol or illicit substances), traumatic brain injury, or systemic shock can render subjective sensory testing entirely unreliable.
- Psychological Distress: Extreme anxiety, pain, or lack of cooperation can lead to false-positive or false-negative sensory and motor findings.
- Pediatric Patients: Examining a frightened, injured child requires immense patience and reliance on objective, observational signs rather than subjective feedback.
- Extensive Soft Tissue Trauma: Massive crush injuries, degloving, or complex mangled extremities distort normal anatomy and limit the ability to perform isolated motor testing due to pain or mechanical disruption of the musculotendinous units.
These factors frequently cause isolated nerve injuries—particularly digital nerve lacerations—to be overlooked during the preliminary emergency department examination.
Surgical Warning: If the conditions are not satisfactory for a thorough and reliable examination during the initial evaluation, the hand must be reexamined within a reasonable period once the patient is stabilized, sober, and cooperative. Never definitively rule out a nerve injury based on an equivocal acute examination.
The "Index of Suspicion" Principle
A high index of suspicion is mandatory in the evaluation of all patients with hand injuries. The anatomical proximity of neurovascular bundles to the flexor tendon apparatus dictates that an injury to one structure highly correlates with an injury to the other.
Clinical Pearl: An injury to the digital nerves is the most frequently missed diagnosis in acute hand trauma. As a cardinal rule: If a flexor tendon function deficit (FDP or FDS) is present after a volar finger laceration, the surgeon must assume that at least one digital nerve has been transected until proven otherwise via direct surgical exploration.
To ensure no deficit is missed, the clinical evaluation must systematically address four critical pillars: (1) Type and Mechanism of Injury, (2) Sensibility Evaluation, (3) Motor Function, and (4) Sudomotor Function (Sweating).
PILLAR 1: TYPE AND MECHANISM OF INJURY
Understanding the mechanism of injury is paramount, as it directly informs the pathophysiology of the nerve damage, dictates the timing of surgical intervention, and establishes prognostic expectations. Nerve injuries seen in civilian and industrial practice are commonly caused by one of several distinct mechanisms:
- Direct Trauma: Includes blunt force blows to the limb, crush injuries, fractures (e.g., humeral shaft fractures affecting the radial nerve), and high- or low-velocity missile wounds.
- Lacerations: Sharp transections from knives, glass, or sheet metal. These are the most straightforward to diagnose but require meticulous microsurgical repair.
- Traction or Stretching: Avulsion injuries, often seen in high-energy trauma such as motorcycle accidents or industrial roller-crush injuries. These injuries often feature extensive zones of injury that complicate primary repair.
- Entrapment or Compression: Acute compartment syndrome, hematoma expansion, or prolonged positioning leading to acute compressive neuropathy.
Seddon and Sunderland Classifications
To determine the appropriate treatment algorithm and arrive at tentative prognostic projections, the surgeon must classify the nerve injury according to the frameworks established by Seddon (1943) and Sunderland (1951).
1. Neurapraxia (Seddon) / Type I (Sunderland)
* Pathophysiology: A local conduction block with focal demyelination. The axon, endoneurium, perineurium, and epineurium remain intact. There is no Wallerian degeneration.
* Clinical Example: Bumping the "funny bone" (ulnar nerve at the cubital tunnel) or "Saturday night palsy" (radial nerve compression).
* Prognosis: Excellent. Full recovery is expected within days to 12 weeks.
2. Axonotmesis (Seddon) / Type II (Sunderland)
* Pathophysiology: Disruption of the axon and myelin sheath, leading to Wallerian degeneration distal to the injury. The endoneurial tubes remain intact, providing a perfect conduit for regenerating axons.
* Prognosis: Good. Recovery occurs at a rate of approximately 1 mm/day (or 1 inch/month) as the axon regenerates down the intact endoneurial tube.
3. Type III (Sunderland)
* Pathophysiology: Disruption of the axon and the endoneurium. The perineurium and epineurium remain intact. Intrafascicular scarring may occur, leading to aberrant axonal routing.
* Prognosis: Variable. Recovery is incomplete, and surgical intervention (neurolysis or grafting) may occasionally be required if recovery plateaus.
4. Type IV (Sunderland)
* Pathophysiology: Disruption of the axon, endoneurium, and perineurium. Only the epineurium remains intact. The nerve is in continuity macroscopically, but functionally it is completely scarred (neuroma-in-continuity).
* Prognosis: Poor without surgery. Requires resection of the neuroma and nerve grafting or repair.
5. Neurotmesis (Seddon) / Type V (Sunderland)
* Pathophysiology: Complete transection of the nerve trunk, including the epineurium.
* Clinical Example: Sharp glass laceration to the volar wrist.
* Prognosis: No potential for spontaneous recovery. Mandates prompt microsurgical repair.
6. Type VI (Mackinnon Modification)
* Pathophysiology: A mixed injury combining various Sunderland grades across different fascicles within the same nerve trunk. Common in crush or traction injuries.
While sharp lacerations fall easily into the category of neurotmesis (Type V), closed injuries with partial nerve deficits are far more complex to classify acutely, and their prognosis requires serial examination and electrodiagnostic testing.
PILLAR 2: SENSIBILITY EVALUATION
When evaluating the injured hand for sensibility, the surgeon must possess an intimate knowledge of both the classic sensory distributions and the autonomous sensory zones of the median, radial, and ulnar nerves.
Autonomous Sensory Zones
Because of significant anatomical overlap and variations in sensory innervation (e.g., Martin-Gruber or Riche-Cannieu anastomoses), testing the classic broad distributions can yield false-negative results. The clinical examination must focus on the autonomous zones—areas innervated exclusively by a single nerve:
- Median Nerve: The volar pulp of the index finger.
- Ulnar Nerve: The volar pulp of the little finger.
- Radial Nerve: The dorsal aspect of the first web space (thumb-index web space).
Modalities of Sensory Testing
Sensory testing should be performed in a quiet environment, with the patient's eyes closed, comparing the injured digit to the contralateral uninjured digit.
- Light Touch and Threshold Testing: Evaluated using Semmes-Weinstein Monofilaments (SWMF). This is the most sensitive test for detecting early nerve compression or partial nerve injury. A normal threshold is typically the 2.83 monofilament.
- Innervation Density Testing: Evaluated using Static and Moving Two-Point Discrimination (2PD).
- Moving 2PD: Returns earlier than static 2PD. Normal is 2-3 mm.
- Static 2PD: Normal is < 6 mm. Values > 10 mm indicate severe impairment.
- Vibration Testing: Utilizing a 256 Hz tuning fork. Altered vibratory perception is often the earliest sign of nerve compression.
Pitfall: If the injury is a sharp laceration and the nerve has been completely transected, the sensory examination is usually definitive (absolute anesthesia in the autonomous zone). However, in closed crush injuries or partial lacerations, the depth of injury may not be fully known, and sensory findings may be patchy or delayed. Meticulous documentation of the exact sensory deficit prior to the administration of any local anesthetic is an absolute medicolegal requirement.
PILLAR 3: MOTOR FUNCTION EVALUATION
Motor evaluation requires isolating specific muscle functions to differentiate between tendon lacerations, pain-inhibited movement, and true denervation. The intrinsic muscles of the hand are the most critical indicators of distal median and ulnar nerve integrity.
Median Nerve Motor Evaluation
The median nerve innervates the LOAF muscles in the hand (Lumbricals 1 & 2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis - superficial head).
* Abductor Pollicis Brevis (APB) Test: The APB is the only muscle innervated exclusively by the median nerve in nearly all patients. Have the patient lay their hand flat on the table, palm up, and ask them to point their thumb toward the ceiling against resistance. Palpate the APB muscle belly for contraction.
* Anterior Interosseous Nerve (AIN) Test: Ask the patient to make an "OK" sign. AIN palsy results in an inability to flex the IP joint of the thumb (FPL) and the DIP joint of the index finger (FDP), resulting in a flat, "pincer" grasp rather than a round "O".
Ulnar Nerve Motor Evaluation
The ulnar nerve is the primary motor nerve of the hand, innervating the hypothenar muscles, all interossei, lumbricals 3 & 4, the adductor pollicis, and the deep head of the FPB.
* Intrinsic Muscle Testing: Ask the patient to abduct and adduct the extended fingers against resistance (testing dorsal and volar interossei).
* Froment’s Sign: Ask the patient to hold a piece of paper between the thumb and radial side of the index finger (key pinch) while the examiner pulls it away. If the ulnar nerve is injured (paralyzed adductor pollicis), the patient will compensate by hyperflexing the thumb IP joint using the median-innervated FPL.
* Wartenberg’s Sign: An abducted posture of the little finger due to unopposed action of the extensor digiti minimi (radial nerve) when the third palmar interosseous muscle (ulnar nerve) is paralyzed.
Radial Nerve Motor Evaluation
The radial nerve provides motor innervation to the extensor compartments of the forearm.
* Testing: Assess the patient's ability to extend the wrist (ECRL, ECRB, ECU), extend the fingers at the MCP joints (EDC, EIP, EDM), and extend/abduct the thumb (EPL, EPB, APL).
* Note: Finger extension at the PIP and DIP joints is controlled by the intrinsic muscles (median/ulnar nerves), not the radial nerve.
PILLAR 4: SUDOMOTOR FUNCTION (SWEATING)
Sudomotor function evaluation is an invaluable, objective tool, particularly when dealing with uncooperative patients, intoxicated individuals, or young children where subjective sensory testing is impossible.
Sympathetic postganglionic unmyelinated C-fibers travel alongside peripheral sensory nerves. When a peripheral nerve is completely transected, the sympathetic innervation to that specific dermatome is lost, resulting in localized anhidrosis (absence of sweating).
Objective Sudomotor Tests
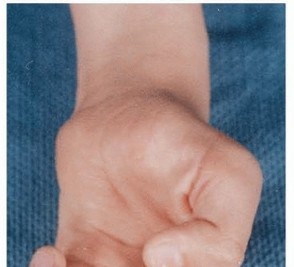
- The O'Rian Wrinkle Test: The patient's hand is immersed in warm water (approximately 40°C) for 20 to 30 minutes. Normal, innervated skin will exhibit characteristic wrinkling of the digital pulps. Denervated skin will remain entirely smooth and unwrinkled. This is a highly reliable, non-invasive test for pediatric digital nerve injuries.
- The Ninhydrin Test: The patient's fingertips are pressed onto high-quality paper. The paper is then sprayed with ninhydrin reagent and heated. Ninhydrin reacts with the amino acids present in sweat, turning purple. Areas of denervation will not produce sweat and will therefore leave no purple footprint on the paper.
- Tactile Adherence: A quick, bedside alternative. The examiner lightly drags a smooth object (like the plastic barrel of a pen) across the patient's digital pulp. Innervated, slightly moist skin will provide friction and resistance. Denervated, anhidrotic skin will feel completely smooth and slippery.
SURGICAL PLANNING AND EXPLORATION
Even if a wound is definitively scheduled to be explored in the operating room to determine the extent of the nerve injury, it is immensely helpful to document the exact preoperative neurologic status.
Intraoperative exploration remains the gold standard for diagnosing the extent of nerve injury in open wounds. Under tourniquet control and loupe or microscopic magnification, the surgeon must trace the nerve from the zone of uninjured tissue proximally into the zone of injury.
If a nerve is found to be contused but in continuity (Sunderland Type II-IV), the surgeon must rely on the preoperative clinical exam to determine if the deficit is complete or partial. If the preoperative exam demonstrated complete anesthesia and paralysis, and the nerve is macroscopically intact but severely bruised, the surgeon may opt for conservative management with serial examinations and delayed electrodiagnostic testing (EMG/NCS) at 3 to 4 weeks post-injury to assess for early signs of reinnervation.
Ultimately, the preoperative evaluation of hand nerve injuries is not merely a diagnostic formality; it is the foundational blueprint that guides surgical decision-making, dictates the necessity of microsurgical repair, and establishes the baseline against which all future postoperative recovery will be measured.
You Might Also Like