Introduction & Epidemiology
Hip posterior dislocation represents a high-energy traumatic injury requiring emergent recognition and reduction to mitigate severe long-term sequelae. It is the most common pattern of hip dislocation, accounting for approximately 80-90% of all traumatic hip dislocations. The typical mechanism involves an axial load applied to a flexed, adducted, and internally rotated hip, most frequently observed in motor vehicle collisions where the knee impacts the dashboard, driving the femoral head posteriorly out of the acetabulum. Other mechanisms include falls from height or direct impact to the posterior aspect of the hip.
The urgency of diagnosis and reduction cannot be overstated. Prolonged dislocation time directly correlates with increased rates of critical complications, particularly avascular necrosis (AVN) of the femoral head and sciatic nerve injury. While immediate closed reduction within 6 hours (and ideally within 1-2 hours) is the gold standard for simple dislocations, a thorough understanding of associated injuries, optimal reduction techniques, and indications for open reduction or surgical fixation is paramount for every orthopedic surgeon. This review aims to consolidate current best practices for the rapid diagnosis and emergency management of posterior hip dislocations.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the hip joint's anatomy and biomechanics is fundamental to both successful reduction and prevention of iatrogenic injury.
The hip joint is a ball-and-socket synovial joint characterized by its inherent stability, largely attributed to its deep bony articulation, robust capsuloligamentous structures, and surrounding powerful musculature.
Bony Anatomy
- Acetabulum: A hemispheric socket formed by the fusion of the ilium, ischium, and pubis. Its weight-bearing articular surface, the lunate surface, is horseshoe-shaped, open inferiorly at the acetabular notch. The depth and congruence of the acetabulum with the femoral head are crucial for stability.
- Femoral Head: Approximately two-thirds of a sphere, covered by articular cartilage except for the fovea capitis, which serves as the attachment site for the ligamentum teres.
Capsuloligamentous Structures
The joint capsule is exceptionally strong, attaching circumferentially to the acetabular rim and proximally to the intertrochanteric line anteriorly and the base of the femoral neck posteriorly. Three primary extracapsular ligaments reinforce the capsule and significantly contribute to hip stability:
*
Iliofemoral Ligament (Ligament of Bigelow/Y-ligament):
The strongest ligament, originating from the anterior inferior iliac spine (AIIS) and acetabular rim, fanning out to attach to the intertrochanteric line. It resists hyperextension, external rotation, and adduction.
*
Pubofemoral Ligament:
Originates from the superior pubic ramus and blends with the iliofemoral ligament anteriorly, attaching to the intertrochanteric line. It resists abduction and some external rotation.
*
Ischiofemoral Ligament:
Arises from the ischium posterior to the acetabulum and spirals superiorly and laterally to attach to the greater trochanter and joint capsule. It resists internal rotation, adduction, and extension.
The ligamentum teres , an intracapsular but extrasynovial structure, contains a branch of the obturator artery (foveal artery) which contributes to femoral head vascularity, especially in children, but plays a minimal role in mechanical stability in adults.
Musculature
A powerful array of muscles surrounds the hip, providing dynamic stability.
*
Anterior Compartment (Flexors):
Iliopsoas, rectus femoris, sartorius.
*
Medial Compartment (Adductors):
Adductor longus, brevis, magnus, gracilis, pectineus.
*
Lateral Compartment (Abductors):
Gluteus medius, gluteus minimus, tensor fascia lata.
*
Posterior Compartment (Extensors & External Rotators):
Gluteus maximus, and the
deep external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris)
. These short external rotators lie directly posterior to the hip capsule and are frequently injured or trapped in posterior dislocations, particularly the piriformis.
Neurovascular Structures
- Sciatic Nerve: The most commonly injured nerve in hip dislocations, running immediately posterior to the hip joint. It exits the pelvis through the greater sciatic notch, deep to the piriformis muscle, and descends between the greater trochanter and the ischial tuberosity. Its proximity makes it highly vulnerable to stretch, compression, or direct trauma during dislocation or reduction.
- Medial Circumflex Femoral Artery (MCFA): The primary blood supply to the femoral head in adults, ascending posteriorly and superiorly along the posterior aspect of the femoral neck, deep to the quadratus femoris and obturator externus. Damage to this artery, particularly its retinacular branches, is the main etiology of femoral head AVN following dislocation.
Biomechanics of Dislocation
Posterior dislocation typically occurs when the hip is flexed (often 60-90 degrees), adducted, and internally rotated. This position unwinds the iliofemoral ligament and places maximal stress on the posterior capsule and short external rotators, leading to their rupture. The femoral head is then levered out of the acetabulum posteriorly. The force involved is often sufficient to cause associated fractures, such as posterior acetabular wall fractures, femoral head fractures (Pipkin classification), or femoral neck fractures. The direction of displacement is almost always superiorly and posteriorly, with the femoral head resting on the posterior aspect of the ilium.
Indications & Contraindications
The management of hip posterior dislocation is dictated by the presence of associated injuries and the ability to achieve a stable, concentric reduction. The overarching principle is prompt reduction to minimize ischemia to the femoral head.
Indications for Emergency Closed Reduction
- All acute posterior hip dislocations without contraindications for closed reduction. This includes simple dislocations (no associated fractures or neurovascular compromise) and many complex dislocations where initial attempts at closed reduction are warranted if there are no absolute contraindications.
Indications for Operative Management (Open Reduction and/or Fixation)
Operative intervention is typically reserved for scenarios where closed reduction is unsuccessful, the hip remains unstable after closed reduction, or significant associated injuries necessitate surgical repair.
Table: Operative vs. Non-Operative Indications for Posterior Hip Dislocation
| Category | Non-Operative (Emergency Closed Reduction) | Operative (Open Reduction & Internal Fixation / Repair) |
|---|---|---|
| Dislocation Type | Simple posterior dislocation (no associated fracture or incarcerated fragment) | Irreducible closed dislocation (buttonholing of capsule/muscles, incarcerated fragments, femoral head osteochondral fragments, labral tears) |
| Associated Fractures | None | Acetabular fracture (posterior wall/column, transverse, T-type) requiring ORIF |
| Femoral head fracture (Pipkin classification, especially Type II, III, IV) requiring ORIF or excision of small fragments | ||
| Femoral neck fracture (requiring ORIF) | ||
| Greater trochanteric avulsion fracture (if displaced and requiring fixation) | ||
| Joint Stability | Stable after closed reduction | Unstable hip after successful closed reduction (re-dislocation with minimal provocative movement, gross instability on stress testing) |
| Neurovascular | Intact neurovascular status or minor/resolving neurological deficit | Irreparable/progressive neurovascular injury (e.g., sciatic nerve laceration) requiring exploration and repair |
| Timing | Acute presentation (< 6-12 hours post-injury) | Chronic dislocation (> 2-3 weeks post-injury, often requires advanced planning and potential osteotomy) |
| Imaging Findings | Clear joint space after reduction, no significant displaced fragments | Incarcerated osteochondral fragments on post-reduction X-rays/CT, widening of joint space, concentricity not achieved despite multiple reduction attempts |
| Other | Soft tissue interposition (e.g., piriformis, capsule, labrum) preventing concentric reduction |
Contraindications
Absolute contraindications to
attempting closed reduction
are rare but include:
*
Femoral neck fracture:
This is a crucial contraindication. Attempting closed reduction in the presence of an ipsilateral femoral neck fracture can convert a non-displaced fracture into a displaced one, or cause further displacement, increasing the risk of AVN or nonunion. This requires careful pre-reduction imaging.
*
Associated ipsilateral acetabular fracture
that would be significantly compromised by closed reduction maneuvers (e.g., a large, unstable posterior wall fragment). However, many simple posterior wall fractures can be reduced with the hip dislocation and addressed subsequently.
*
Hemodynamic instability
precluding safe anesthesia.
Relative contraindications include severe comorbidities that make general anesthesia risky, though the urgency of reduction often outweighs these concerns. For these patients, reduction under procedural sedation might be considered, if feasible and safe.
Pre-Operative Planning & Patient Positioning
Thorough and rapid pre-operative planning is essential for a successful outcome in hip posterior dislocations.
Initial Assessment & Resuscitation
- ATLS Protocol: As many hip dislocations result from high-energy trauma, primary and secondary surveys according to ATLS guidelines are paramount. Address immediate life threats (Airway, Breathing, Circulation, Disability, Exposure).
- Neurovascular Examination: Document precise neurological function (sciatic nerve: common peroneal and tibial divisions) and vascular status (distal pulses, capillary refill, ankle-brachial index if vascular injury suspected) prior to any reduction attempt. Compare to the contralateral limb. This is critical for post-reduction assessment and medico-legal documentation.
- Mechanism of Injury: Obtain as much information as possible regarding the injury mechanism, as this can suggest associated injuries (e.g., dashboard injury for knee and patellar trauma, direct lateral impact for acetabular fractures).
Imaging
- AP Pelvis X-ray: Confirms the diagnosis of hip dislocation. The femoral head will appear superior and lateral to the acetabulum, with internal rotation of the femur (lesser trochanter not visible). Evaluate for associated pelvic ring injuries or sacral fractures.
- Lateral Hip X-ray: Crucial for confirming the direction of dislocation (anterior vs. posterior) and identifying subtle femoral neck fractures or impaction injuries to the femoral head.
- Judet Views (Oblique X-rays): Iliac oblique and obturator oblique views are ideal for evaluating potential acetabular fractures, though these are often deferred until after initial reduction due to urgency.
-
CT Scan:
A CT scan of the pelvis and hip is generally recommended
after successful closed reduction
to:
- Confirm concentric reduction.
- Identify incarcerated osteochondral fragments or soft tissue within the joint.
- Precisely characterize associated acetabular or femoral head fractures (size, displacement, articular involvement).
- Assess for occult femoral neck or intertrochanteric fractures missed on plain radiographs.
-
Evaluate the extent of capsular or labral injury.
If closed reduction fails or is contraindicated due to suspected femoral neck fracture, a CT scan may be performed pre-reduction to guide operative planning.
Anesthesia & Analgesia
Adequate muscle relaxation and analgesia are crucial for safe and successful closed reduction.
*
Procedural Sedation:
Often sufficient for cooperative patients in the emergency department, administered by trained personnel.
*
General Anesthesia:
Provides optimal muscle relaxation and pain control, particularly for difficult reductions, uncooperative patients, or obese individuals. This is often the preferred method for optimal conditions.
*
Regional Anesthesia:
Spinal or epidural anesthesia can be considered, but may prolong time to reduction and may not be ideal in trauma patients.
Patient Positioning for Closed Reduction
The patient should be positioned on a firm surface, typically a stretcher or operating room table.
*
Supine Position:
This is the most common position for all standard closed reduction maneuvers. The patient lies supine with the pelvis stabilized.
*
Assistant:
A strong assistant is crucial to stabilize the pelvis, typically by applying counter-traction to the anterior superior iliac spines (ASISs) or by holding the iliac crests to prevent the patient from sliding during traction.
*
Operating Surgeon:
Stands over the patient, often at the side of the affected hip, or positioned to apply axial traction to the femur.
Detailed Surgical Approach / Technique
The primary goal is prompt, gentle, and successful reduction of the dislocated hip. This section details both closed reduction techniques and the indications and approach for open reduction.
Emergency Closed Reduction Techniques
Regardless of the specific maneuver, key principles apply:
1.
Adequate Muscle Relaxation:
Absolutely paramount. Without it, forceful reduction attempts can lead to iatrogenic fractures or cartilage damage.
2.
Axial Traction:
Apply steady, sustained axial traction in line with the femoral shaft, aiming to distract the femoral head from the acetabulum.
3.
Flexion:
The hip is typically flexed to relax the powerful hip flexors and iliofemoral ligament.
4.
Rotation:
Gentle internal and external rotation movements are used to disengage the femoral head from its posterior position and guide it back into the acetabulum.
5.
Adduction/Abduction:
Depending on the maneuver, controlled adduction or abduction may be used to clear the posterior rim.
6.
Pelvic Stabilization:
A strong assistant provides counter-traction to the pelvis.
1. Allis Maneuver (Most Commonly Used)
- Position: Patient supine. Surgeon stands over the patient, facing their feet.
- Hip Position: Flex the hip to 90 degrees and the knee to 90 degrees.
- Traction: Apply steady, upward axial traction along the line of the femur.
- Rotation: While maintaining traction, gently rotate the hip internally and externally.
- Leverage: As the femoral head approaches the acetabulum, gentle adduction may help guide it in. Some surgeons place a knee in the patient's groin for leverage (though this can be controversial due to potential injury).
- Reduction Sign: A palpable clunk or thud is typically felt and heard as the femoral head reduces.
2. Bigelow Maneuver (Less Common, but effective)
- Position: Patient supine. Surgeon stands at the side of the affected hip.
- Hip Position: Flex the hip to 90 degrees and the knee to 90 degrees.
- Traction: Apply axial traction.
- Rotation & Abduction: While maintaining traction and flexion, externally rotate the hip and abduct it. This unwinds the strong iliofemoral ligament, which can be taut and resistant in some dislocations.
- Reduction Sign: Palpable clunk.
3. Stimson Maneuver (Gravity-Assisted)
- Position: Patient prone, with the affected leg hanging off the edge of the bed.
- Hip Position: Hip and knee are flexed to 90 degrees.
- Traction: Apply downward axial traction to the lower leg or ankle.
- Weight: An assistant can apply downward pressure to the posterior aspect of the distal femur.
- Rotation: Gentle internal and external rotation of the leg can facilitate reduction.
- Reduction Sign: Palpable clunk. This maneuver requires the patient to be prone, which may not be feasible in all acute trauma situations.
Post-Reduction Assessment
- Palpation: Check for a reduced, stable hip.
- Range of Motion: Gently assess full, pain-free range of motion (flexion, extension, abduction, adduction, internal, external rotation). Pay close attention to any instability, particularly in adduction and internal rotation, which can suggest a posterior wall fracture.
- Neurovascular Re-assessment: Crucial to re-check sciatic nerve function and distal pulses. Document any changes immediately.
- Imaging: Obtain post-reduction AP pelvis and lateral hip X-rays to confirm concentric reduction and evaluate for newly apparent fractures (e.g., femoral head impaction, posterior wall). A CT scan is generally indicated post-reduction to definitively assess concentricity, identify incarcerated fragments, and evaluate for subtle associated fractures.
Indications for Open Reduction
Open reduction is necessary if:
*
Closed reduction fails:
After 2-3 gentle, well-muscles-relaxed attempts.
*
Non-concentric reduction:
Imaging reveals persistent subluxation or incarcerated fragments after closed attempts.
*
Associated fractures requiring fixation:
Large, displaced acetabular posterior wall fractures, displaced femoral head fractures (Pipkin types II-IV), or femoral neck fractures.
*
Neurological compromise:
If a patient with sciatic nerve deficit fails to improve after closed reduction, or if there is a suspicion of nerve entrapment, exploration may be warranted.
Open Reduction Technique (Posterior Approach: Kocher-Langenbeck)
This is the workhorse approach for posterior hip dislocations requiring open reduction, as it directly accesses the posterior capsule, short external rotators, and posterior acetabulum.
1. Patient Positioning
- Lateral Decubitus: Patient positioned in true lateral decubitus on a beanbag or bolsters, with the affected hip up. Ensure adequate padding of bony prominences. The knee should be slightly flexed.
- Prone (alternative): Can also be performed prone, though lateral is often preferred for access.
2. Incision
- Curvilinear Incision: Centered over the greater trochanter, extending proximally along the posterior iliac crest for 5-7 cm and distally along the femur for 8-10 cm. The incision follows the anterior border of the gluteus maximus, curving posteriorly superiorly.
3. Superficial Dissection
- Skin and Subcutaneous Tissue: Incise down to the deep fascia.
- Fascia Lata: Incise the fascia lata in line with the skin incision, distal to the gluteus maximus.
- Gluteus Maximus: Split the gluteus maximus muscle fibers bluntly in line with their fibers, or incise its tendinous insertion to the femur more proximally. Retract the muscle fibers superiorly and inferiorly.
- Greater Trochanter: Identify the greater trochanter.
4. Identification of Short External Rotators
- Deep to the gluteus maximus, the layer of short external rotators comes into view. From superior to inferior, these are typically: Piriformis, Superior Gemellus, Obturator Internus, Inferior Gemellus, and Quadratus Femoris.
- The sciatic nerve lies deep to the piriformis and superficial to the quadratus femoris. It is highly vulnerable. Careful identification and protection are paramount. Identify the nerve early and retract it gently, typically medially.
5. Capsulotomy and Joint Exposure
- Tenotomy of Rotators: The piriformis and obturator internus tendons are typically tenotomized close to their insertion on the greater trochanter. Some surgeons perform a more extensile tenotomy of all short external rotators to facilitate exposure. Tag these tendons with heavy sutures for later repair.
- Capsule Incision: The posterior capsule is now exposed. Make a T-shaped or H-shaped incision in the capsule to expose the femoral head and acetabulum. This allows for removal of incarcerated fragments and direct visualization of the joint.
- Fracture Assessment: If an acetabular posterior wall fracture is present, carefully assess its size, comminution, and displacement.
6. Reduction
- Direct Visualization: With the joint exposed, any interposed fragments (osteochondral, labral, capsular) are identified and removed.
- Reduction Maneuver: Using a bone hook or reduction clamps on the femoral neck, and gentle leverage, the femoral head is maneuvered back into the acetabulum under direct visualization. Ensure full engagement and concentric reduction.
- Stabilization: If a posterior wall fracture exists, temporary K-wire fixation may be used to hold fragments while assessing reduction and planning definitive fixation.
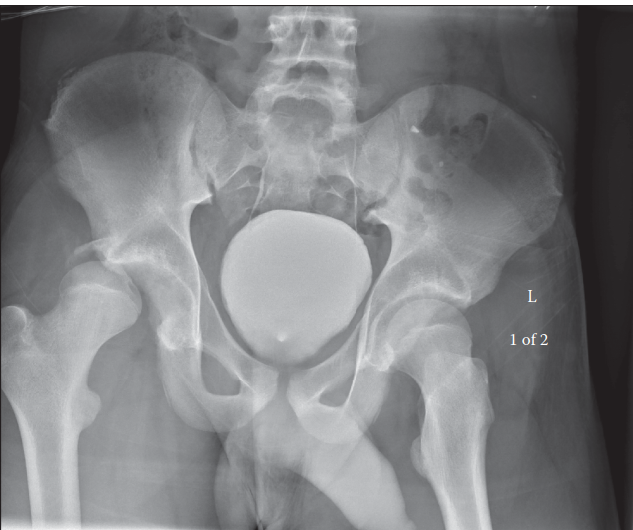
Illustration of a posterior hip dislocation, demonstrating the typical position of the femoral head posterior and superior to the acetabulum, highlighting the anatomical relationship with surrounding structures. This view would be consistent with what is encountered during open reduction via a posterior approach.
7. Fixation (if indicated)
- Acetabular Fracture Fixation: If a posterior wall or other acetabular fracture is present and requires fixation, plates and screws are applied according to standard principles of acetabular fracture management. Ensure stable reduction and restoration of articular congruity.
- Femoral Head Fracture Fixation: Pipkin Type I or II fractures often require headless compression screws placed from the non-articular portion of the femoral head into the fragment, ensuring stable fixation and avoiding articular penetration. Smaller fragments or Type IV fractures may require excision depending on size and location.
8. Closure
- Capsular Repair: Whenever possible, repair the posterior capsule to enhance stability.
- Rotator Repair: Reattach the tenotomized short external rotator tendons (e.g., piriformis, obturator internus) to their insertion site on the greater trochanter using transosseous sutures or suture anchors. This is crucial for restoring posterior stability and muscle function.
- Fascia Lata: Close the fascia lata.
- Skin: Close the subcutaneous tissues and skin.
Complications & Management
Hip posterior dislocation, especially when associated with fractures or delayed reduction, carries a significant risk of both immediate and long-term complications. Proactive management and early recognition are key to mitigating their impact.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Management / Salvage Strategies |
|---|---|---|
| Avascular Necrosis (AVN) | 5-40% (Time-dependent; <6h: 5-10%; >24h: 40%+) | Prevention: Urgent reduction (<6 hours). Early Stage: Core decompression, bone grafting (vascularized/non-vascularized). Late Stage: Total Hip Arthroplasty (THA), osteotomy (rare). Consider revascularization procedures in select cases. |
| Sciatic Nerve Injury | 10-20% (Peroneal division more common) | Immediate: Thorough pre/post-reduction neuro exam. Acute: Observation for neuropraxia (most resolve within 6-12 months). Persistent/Progressive: EMG/NCS at 3-6 weeks. Surgical exploration if suspected entrapment or laceration (rare). Foot drop brace for peroneal deficit. |
| Post-Traumatic Arthritis (PTA) | 10-50% (Higher with associated fractures, AVN, or non-concentric reduction) | Early: Physical therapy, activity modification, NSAIDs. Progressive: Intra-articular injections (corticosteroids, viscosupplementation). End-stage: Total Hip Arthroplasty (THA) – often complex due to previous trauma. |
| Recurrent Dislocation | 2-10% (Higher with inadequate initial reduction, associated fracture, soft tissue damage) | Acute Recurrence: Re-reduction. Recurrent Instability: Address underlying cause (e.g., acetabular deficiency, capsular laxity, retained fragments). Open reduction, capsular repair/plication, labral repair. Arthroplasty for chronic instability/damage. |
| Heterotopic Ossification (HO) | 10-60% (Higher with head injury, extensive soft tissue trauma, multiple procedures) | Prevention: NSAIDs (e.g., indomethacin) or low-dose radiation post-operatively for high-risk patients. Established HO: Excision only if symptomatic (pain, limited ROM) and mature (often >1 year post-injury). |
| Infection | <1-5% (Higher with open reduction, extensive soft tissue damage) | Prevention: Prophylactic antibiotics, meticulous surgical technique. Acute: Irrigation and debridement, appropriate intravenous antibiotics. Chronic: Multi-stage revision, suppressive antibiotics. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | 1-5% (DVT higher, PE less common) | Prevention: Pharmacologic (low molecular weight heparin, fondaparinux) and mechanical prophylaxis (compression devices). Early mobilization. Treatment: Anticoagulation. |
| Iatrogenic Fracture | <1% (Femoral neck, acetabulum) | Prevention: Adequate muscle relaxation, gentle reduction maneuvers. Management: Open reduction and internal fixation (ORIF) as indicated for specific fracture patterns. May complicate future AVN risk. |
| Chronic Dislocation | <1% (Delayed or missed diagnosis) | Extremely challenging. Often requires extensive soft tissue release, osteotomies (femoral or acetabular), or ultimately THA due to extensive arthritic changes and bone loss. Increased risk of AVN, nerve injury, and poor functional outcomes. |
Specific Considerations for Management:
- Avascular Necrosis (AVN): This remains the most devastating long-term complication. The incidence is directly proportional to the time to reduction and the energy of the injury. Monitoring for AVN involves clinical suspicion (groin pain, limited ROM) and imaging (MRI is most sensitive, plain radiographs show late changes). Early AVN can be managed with core decompression; advanced AVN typically necessitates total hip arthroplasty (THA).
- Sciatic Nerve Injury: The peroneal division is more commonly affected due to its relative fixation and more superficial course. Most sciatic nerve palsies following hip dislocation are neurapraxias and resolve spontaneously within 6-12 months. Serial neurological exams are vital. If the palsy worsens after reduction or is a complete deficit, consider nerve entrapment (e.g., by bone fragments or capsule) or laceration, warranting urgent nerve conduction studies/EMG and possible surgical exploration.
- Post-Traumatic Arthritis (PTA): Arises from articular cartilage damage during the initial dislocation, persistent incongruity, or subsequent AVN. It can manifest years after the initial injury. Non-operative management is initially pursued, but severe, symptomatic PTA often requires THA. Pre-existing trauma makes these THAs more challenging due to altered anatomy, hardware, and soft tissue scarring.
- Heterotopic Ossification (HO): The formation of mature bone in soft tissues where bone does not normally exist. Common around the hip after trauma, especially with associated head injury. Prophylaxis with NSAIDs (e.g., Indomethacin for 3-6 weeks) or single-dose radiation (700-800 cGy) post-operatively is effective for high-risk patients. Excision is reserved for symptomatic, mature HO that limits function.
Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol for posterior hip dislocation varies significantly depending on whether the injury was a simple dislocation, an irreducible dislocation requiring open reduction, or one associated with significant acetabular or femoral head fractures requiring fixation. The goals remain consistent: protect the reduction, restore range of motion, regain strength, and facilitate return to function while minimizing complications.
General Principles
- Protection of Reduction: Avoid positions of instability (flexion > 90°, adduction past midline, internal rotation) for 4-6 weeks, especially in cases with posterior wall fractures or capsular repair. Abduction pillows or braces are sometimes used, though their efficacy for simple dislocations is debatable.
- Early Mobilization: As soon as pain allows, within protective parameters, to prevent stiffness, DVT/PE, and promote healing.
- Gradual Progression: Rehabilitation is a phased approach, progressing from protected motion to strengthening and functional activities.
Phase 1: Acute Protection (Weeks 0-6)
-
Weight Bearing:
- Simple Dislocation (Closed Reduction): Touchdown weight-bearing (TDWB) or protected weight-bearing (PWB) with crutches/walker for 2-4 weeks. Progress to full weight-bearing (FWB) as tolerated.
- Open Reduction / Associated Fractures (e.g., posterior wall): Strict non-weight-bearing (NWB) for 6-12 weeks, depending on fracture stability, hardware, and surgeon preference. This protects the healing capsule, repaired soft tissues, and any internal fixation.
-
Range of Motion (ROM):
- Passive ROM: Gentle, pain-free ROM within protective limits. Avoid the "dislocating position" (flexion > 90°, adduction, internal rotation).
- Active-Assisted ROM: Progress as tolerated, focusing on controlled movements.
- Continuous Passive Motion (CPM): May be used by some surgeons for pain control and to prevent stiffness, but routine use is controversial.
-
Exercises:
- Isometric quadriceps and gluteal sets.
- Ankle pumps.
- Gentle hip abduction (isometric or limited range) to strengthen gluteus medius.
- Core stability exercises (gentle).
Phase 2: Intermediate Strength & Mobility (Weeks 6-12)
-
Weight Bearing:
- Gradual progression from PWB to FWB for simple dislocations.
- For fracture patients, initiation of PWB with gradual progression to FWB once radiographic evidence of fracture healing is present (typically 8-12 weeks).
- Range of Motion: Increase active and passive ROM. Work towards full flexion, extension, abduction, and rotation within pain tolerance.
-
Strengthening:
- Progressive resistive exercises for hip abductors, extensors, and flexors (e.g., resistance bands, light weights).
- Gluteal and core strengthening becomes more aggressive.
- Closed kinetic chain exercises (mini-squats, lunges within limits).
- Gait Training: Wean off assistive devices as strength and balance improve. Focus on normal gait mechanics.
Phase 3: Advanced Strengthening & Return to Activity (Weeks 12+)
- Weight Bearing: Full weight-bearing, unrestricted.
- Range of Motion: Should be near normal.
-
Strengthening:
- Continue progressive resistance exercises.
- Proprioceptive training (e.g., single-leg stance, balance boards).
- Functional exercises specific to patient's activities or sport.
- Sport-Specific Training: For athletes, gradual progression through sport-specific drills, agility training, and plyometrics.
- Return to Sport/Work: Typically cleared for unrestricted activity at 4-6 months, depending on the severity of injury, individual progress, and absence of complications (e.g., AVN symptoms, instability). High-impact sports may require longer.
Specific Considerations
- Sciatic Nerve Palsy: If present, a foot drop brace (AFO) may be necessary. Physical therapy focuses on gait training and strengthening of unaffected muscles. Electrical stimulation might be used.
- Heterotopic Ossification (HO): If prophylaxis was not used or failed, and HO is symptomatic, surgical excision is considered only after the HO has matured (typically 12-18 months post-injury).
- Monitoring for AVN: Patients should be regularly monitored for signs and symptoms of AVN. MRI is the most sensitive imaging modality.
- Patient Education: Emphasize adherence to precautions and exercises. Explain the potential for long-term complications like AVN and post-traumatic arthritis.
Summary of Key Literature / Guidelines
The management of hip posterior dislocation is guided by established principles derived from decades of clinical experience and research. Several key themes consistently emerge in orthopedic literature and form the basis of current guidelines.
-
Time is Muscle (and Bone): The single most critical factor influencing outcomes, particularly the risk of femoral head avascular necrosis (AVN), is the time to reduction . Numerous studies, from early reviews by Epstein and others to contemporary analyses, consistently demonstrate a direct inverse relationship between prompt reduction (ideally within 6 hours, optimally within 1-2 hours) and the incidence of AVN. Delays beyond 12-24 hours dramatically increase AVN rates to over 40-50%. This underscores the need for rapid diagnosis and immediate, concerted efforts at closed reduction in the emergency setting.
-
Role of Post-Reduction CT Scan: While plain radiographs confirm dislocation and initially assess reduction, a post-reduction CT scan has become the standard of care. This is advocated by major trauma societies and orthopedic textbooks. It is indispensable for:
- Confirming concentricity of reduction.
- Identifying intra-articular incarcerated fragments (osteochondral, labral, capsular) that preclude true concentric reduction or could lead to post-traumatic arthritis.
- Precisely characterizing associated fractures (e.g., posterior wall, femoral head, femoral neck) which often dictate the need for open reduction and internal fixation (ORIF). Missed fragments or subtle fractures are a common cause of poor long-term outcomes.
-
Management of Associated Fractures:
- Acetabular Fractures (Posterior Wall): Large, displaced, or unstable posterior wall fractures (typically >20-30% of the wall, or involving the weight-bearing dome) after reduction of the hip usually necessitate ORIF. The goal is to restore articular congruity and hip stability. Small, non-displaced fragments may be managed non-operatively, but careful follow-up is essential. The decision-making often involves assessing hip stability after reduction under fluoroscopy.
-
Femoral Head Fractures (Pipkin Classification):
These require meticulous management.
- Pipkin Type I (below fovea) and Type II (above fovea): Require anatomical reduction and stable internal fixation (typically headless compression screws). Excision of small, non-weight-bearing fragments may be considered.
- Pipkin Type III (Types I or II with associated femoral neck fracture): High risk of AVN. These are surgical emergencies and often require ORIF of both the femoral head and neck.
- Pipkin Type IV (Types I or II with associated acetabular fracture): Complex injuries requiring fixation of both the femoral head and acetabulum.
- Femoral Neck Fractures: The presence of an ipsilateral femoral neck fracture is a critical finding, as it is an absolute contraindication to closed reduction. Attempting closed reduction can displace an undisplaced fracture or worsen a displaced one, significantly increasing AVN risk. These require ORIF of the femoral neck, often followed by separate management of the hip dislocation (which may require open reduction).
-
Sciatic Nerve Injury: Incidence ranges from 10-20%. Most are neurapraxias and resolve spontaneously. However, consistent neurological documentation (pre- and post-reduction) is crucial. Persistent or progressive deficits, or suspicion of nerve entrapment on imaging, warrant urgent EMG/NCS and potential surgical exploration. The peroneal division is more commonly affected.
-
Avascular Necrosis Prophylaxis: While rapid reduction is the best prophylaxis, current literature does not support the routine use of anticoagulants or vasodilators for AVN prevention specifically in hip dislocations. These interventions lack robust evidence for efficacy in this context.
-
Heterotopic Ossification (HO) Prophylaxis: Patients undergoing open reduction, especially those with associated head injuries, are at higher risk for HO. Prophylaxis with non-steroidal anti-inflammatory drugs (NSAIDs) such as indomethacin (e.g., 25 mg TID for 3-6 weeks) or a single dose of post-operative radiation (700-800 cGy) has been shown to be effective in preventing symptomatic HO.
-
Surgical Approaches: The Kocher-Langenbeck (posterior) approach is the preferred method for open reduction of posterior hip dislocations and fixation of posterior acetabular and femoral head fractures. It provides excellent visualization of the posterior joint and relevant structures while minimizing disruption to the anterior stabilizing ligaments.
In conclusion, the successful management of posterior hip dislocation hinges on the principle of emergent, gentle reduction, thorough post-reduction assessment (including CT), and tailored treatment of any associated bony or soft tissue injuries. Adherence to these evidence-based guidelines is critical for optimizing patient outcomes and minimizing debilitating long-term complications.
