Comprehensive Introduction and Patho-Epidemiology
Posterior ankle impingement (PAI) syndrome represents a complex clinical entity characterized by acute or chronic debilitating pain at the posterior aspect of the ankle, which is predictably exacerbated by terminal forced plantar flexion. This condition is classically observed in high-demand athletes who subject their tibiotalar and subtalar joints to repetitive, extreme plantar flexion. Ballet dancers (particularly when assuming the en pointe or demi-pointe positions), elite soccer players striking the ball, fast bowlers in cricket, and gymnasts are disproportionately affected. The fundamental pathoanatomy involves a mechanical "nutcracker effect," wherein osseous or hypertrophic soft tissue structures become pathologically compressed between the posterior lip of the tibial plafond and the superior surface of the calcaneus during plantar flexion. Over time, this repetitive microtrauma initiates a cascade of localized inflammation, microhemorrhage, and subsequent fibrotic scarring, further exacerbating the impingement in a vicious cycle.
The anatomical culprits driving this mechanical conflict are broadly categorized into osseous and soft tissue etiologies. Osseous impingement is most frequently caused by an enlarged posterior process of the talus (specifically the lateral tubercle, known as a Stieda process), an unfused os trigonum, or a malunited fracture of the posterior talar process (Shepherd's fracture). Soft tissue impingement is typically secondary to hypertrophic changes within the posterior joint capsule, the posterior talofibular ligament (PTFL), the intermalleolar ligament, or the flexor hallucis longus (FHL) tenosynovium. In many chronic cases, a mixed picture of both osseous and soft tissue impingement is present, as the prominent bone irritates the surrounding synovial and capsular structures, leading to reactive hypertrophy and florid synovitis.
Historically, surgical management of PAI relied on open posteromedial or posterolateral approaches. While effective at removing the offending pathology, these open techniques were fraught with significant morbidity, including extensive soft tissue dissection, delayed wound healing, severe postoperative stiffness, and an unacceptably prolonged return to high-level athletic competition. The advent of posterior ankle arthroscopy, pioneered and popularized by van Dijk and colleagues in the late 1990s, revolutionized the management of this condition. By utilizing a two-portal endoscopic approach with the patient in the prone position, surgeons can now directly visualize and address the entire posterior ankle and subtalar compartments with minimal iatrogenic trauma.
Today, arthroscopic posterior débridement has definitively superseded open techniques as the gold standard of care. It offers equivalent, if not superior, clinical outcomes regarding pain relief and functional restoration, but with drastically reduced surgical morbidity. Patients experience diminished postoperative pain, a lower risk of wound complications, and an accelerated rehabilitation trajectory, allowing elite athletes to return to sport in a fraction of the time required by traditional open surgery. Mastery of this technique, however, demands a rigorous understanding of the dense posterior ankle anatomy and strict adherence to established surgical principles.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the posterior ankle anatomy is absolutely non-negotiable for safe and effective arthroscopic navigation. The posterior compartment is an anatomically unforgiving space, densely packed with critical neurovascular bundles and tendinous structures that leave zero margin for error. The posterior aspect of the talus features two distinct tubercles—medial and lateral—separated by a fibro-osseous sulcus that houses the flexor hallucis longus (FHL) tendon. The lateral tubercle is typically the larger of the two and serves as the attachment site for the posterior talofibular ligament (PTFL). When an accessory ossicle forms at this lateral tubercle and fails to fuse during skeletal maturation (typically between ages 8 and 13), it is termed an os trigonum, which is present in approximately 7% to 14% of the general population.
The Flexor Hallucis Longus (FHL) tendon is the most critical intraoperative landmark during posterior ankle arthroscopy. It serves as the anatomical "guardian" of the medial neurovascular bundle. The FHL muscle belly extends distally into the posterior compartment, transitioning into its tendon as it enters the fibro-osseous groove between the medial and lateral talar tubercles. During arthroscopy, all osseous and soft tissue resections must remain strictly lateral to the FHL tendon. The tendon itself is enveloped in a synovial sheath that frequently becomes inflamed in PAI syndrome, necessitating a careful tenosynovectomy. Recognizing the dynamic movement of the FHL by passively flexing and extending the hallux intraoperatively is a vital maneuver for maintaining spatial orientation.
Immediately medial to the FHL tendon lies the critical posterior neurovascular bundle, comprising the tibial nerve and the posterior tibial artery and vein. This bundle is situated behind the medial malleolus and is separated from the FHL by only a thin layer of fascia. The distance between the medial border of the FHL and the neurovascular bundle can be as little as 2 to 3 millimeters. Plunging motorized instruments, curettes, or scalpels medial to the FHL carries a catastrophic risk of transecting the tibial nerve or the posterior tibial artery, which can result in devastating, limb-threatening ischemic or neuropathic complications. Thus, the FHL constitutes the absolute medial limit of the safe working zone.
On the lateral aspect of the posterior compartment, the sural nerve and the small saphenous vein represent the primary structures at risk. The sural nerve courses distally along the posterolateral calf, crossing the lateral border of the Achilles tendon approximately 10 centimeters proximal to its insertion, and continues distally posterior to the lateral malleolus. The nerve is highly variable in its arborization and is particularly vulnerable during the establishment of the posterolateral portal. To mitigate this risk, the initial skin incision must be meticulously superficial, scoring only the dermis, followed by blunt dissection using a hemostat to sweep the subcutaneous tissues and the sural nerve safely out of the trajectory of the arthroscopic trocar.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic posterior débridement must be predicated on a rigorous clinical evaluation, precise advanced imaging, and the exhaustion of a structured conservative management protocol. Surgical intervention is rarely indicated as a first-line treatment, except in cases of acute, displaced fractures of the posterior talar process in high-demand athletes where immediate rigid fixation or excision is required to prevent nonunion and subsequent chronic impingement.
Conservative management should span a minimum of 3 to 6 months and must include absolute rest from the offending activity, aggressive use of nonsteroidal anti-inflammatory drugs (NSAIDs), and targeted physiotherapy focusing on intrinsic foot muscle strengthening, proprioception, and eccentric Achilles loading. Furthermore, an image-guided (ultrasound or fluoroscopy) diagnostic and therapeutic corticosteroid injection into the posterior impingement interval is highly recommended. A positive response to this injection not only provides temporary relief but also serves as a potent diagnostic tool, confirming that the posterior compartment is indeed the primary pain generator. When these modalities fail to provide durable relief, surgery is indicated.
Contraindications to posterior ankle arthroscopy are specific and must be respected to avoid severe complications. Active local or systemic infection is an absolute contraindication. Severe peripheral vascular disease that compromises the healing potential of the portal sites or increases the risk of ischemic complications with tourniquet use is also an absolute contraindication. Relative contraindications include profound anatomical distortion secondary to severe prior trauma, which obscures the normal landmarks (particularly the FHL), and extensive end-stage tibiotalar or subtalar osteoarthritis, where isolated débridement will fail to relieve the patient's generalized arthritic pain unless combined with an arthrodesis.
| Category | Specific Conditions | Clinical Rationale / Management Strategy |
|---|---|---|
| Absolute Indications | Failed conservative management (3-6 months) of symptomatic os trigonum or Stieda process. | Mechanical block requires surgical excision for symptom resolution. |
| Absolute Indications | Acute, displaced Shepherd’s fracture in an elite athlete. | High risk of nonunion and chronic PAI; requires early excision or fixation. |
| Absolute Indications | Symptomatic FHL tenosynovitis refractory to injections. | Requires arthroscopic release of the FHL retinaculum and tenosynovectomy. |
| Relative Indications | Concomitant posterior impingement with mild/moderate osteoarthritis. | Patient must be counseled that débridement may not resolve all arthritic pain. |
| Absolute Contraindications | Active localized soft tissue infection or osteomyelitis. | High risk of disseminating infection into the joint spaces. |
| Absolute Contraindications | Severe peripheral arterial disease (PAD). | Poor wound healing potential; tourniquet use is contraindicated. |
| Relative Contraindications | Severe anatomical distortion from prior trauma/surgery. | Loss of the FHL landmark increases the risk of tibial nerve injury. |
| Relative Contraindications | End-stage tibiotalar or subtalar osteoarthritis. | Isolated débridement will fail; requires conversion to arthroscopic arthrodesis. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the foundation of a successful posterior ankle arthroscopy. Standard weight-bearing radiographs, including anteroposterior, mortise, and lateral views, are mandatory. A lateral radiograph taken in maximal plantar flexion is particularly useful for demonstrating the mechanical abutment between the posterior talus and the calcaneus. However, advanced imaging is critical for surgical mapping. A non-contrast MRI is the modality of choice for evaluating the soft tissue envelope, identifying FHL tenosynovitis, bone marrow edema within an os trigonum or Stieda process, and assessing the integrity of the posterior capsuloligamentous complex. In cases of complex bony anatomy or suspected fractures, a fine-cut CT scan with 3D reconstructions provides invaluable spatial information regarding the size, shape, and exact location of the osseous impingement.
Optimal patient positioning is critical for adequate visualization, safe portal placement, and surgeon ergonomics. The procedure is typically performed under general anesthesia or a regional neuraxial block (spinal anesthesia), often supplemented with a popliteal sciatic nerve block for prolonged postoperative analgesia. The patient is carefully rolled into the prone position on a standard operating table. All bony prominences, particularly the patellae, anterior superior iliac spines, and the chest wall, must be meticulously padded to prevent pressure necrosis or neuropraxia.
A well-padded support, such as a dense foam block or a tightly rolled blanket, is placed under the distal tibia and lower leg. This elevation is crucial as it allows the foot to hang freely over the edge of the operating table, permitting unrestricted intraoperative manipulation of the ankle and subtalar joints. A well-padded pneumatic tourniquet is applied to the proximal thigh or proximal calf to ensure a completely bloodless surgical field, which is vital given the small working space and the need for pristine visualization of the neurovascular boundaries.

Maintaining the foot in a strictly neutral position (90 degrees to the tibia) with respect to dorsiflexion/plantar flexion and varus/valgus is one of the most critical safety maneuvers during portal placement. Keeping the foot in neutral tension is the safest posture to avoid iatrogenic neurovascular damage. If the foot is allowed to fall into plantar flexion, the posterior capsular structures relax, allowing the medial neurovascular bundle and the sural nerve to fall anteriorly, closer to the joint space and directly into the trajectory of the arthroscopic portals. Conversely, neutral positioning keeps these structures under appropriate tension, safely displacing them posteriorly and away from the working area.
Step-by-Step Surgical Approach and Fixation Technique
The posterior arthroscopic approach relies on a highly standardized two-portal technique: the posterolateral (viewing) portal and the posteromedial (working) portal. Precise establishment of these portals is the most critical and potentially dangerous step of the entire procedure.
Portal Placement and Trajectory
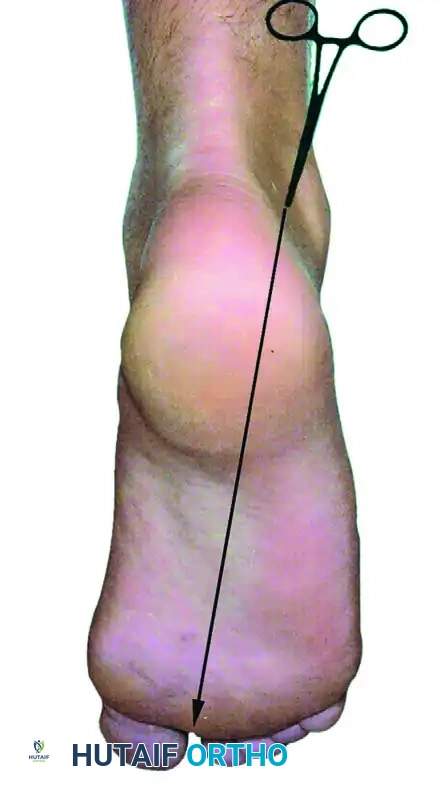
The posterolateral portal is established first. The surgeon palpates the tip of the lateral malleolus and the lateral border of the Achilles tendon. The portal is placed just superior to a line drawn horizontally from the tip of the lateral malleolus to the Achilles tendon, positioned immediately lateral to the tendon itself.

A superficial vertical skin incision is made using a #11 blade. It is imperative to incise only the dermis to avoid injuring the underlying sural nerve. A blunt hemostat is inserted through the skin incision and used to gently spread the subcutaneous tissues. A blunt arthroscopic trocar is then introduced. The trajectory is critical: the trocar must be aimed anteriorly, directed along an imaginary line pointing strictly toward the first web space of the forefoot. The trocar is advanced bluntly until it firmly bottoms out on the posterior bony aspect of the talus or the distal tibia.
The posteromedial portal is then established at the exact same horizontal level as the posterolateral portal, but positioned just medial to the medial border of the Achilles tendon. A similar superficial dermal incision is made. To ensure the safety of the medial neurovascular bundle, a "sliding technique" is utilized. A blunt hemostat or a blunt switching stick is inserted through the medial incision and directed laterally to contact the shaft of the arthroscope (which is already seated in the posterolateral portal) at a 90-degree angle.
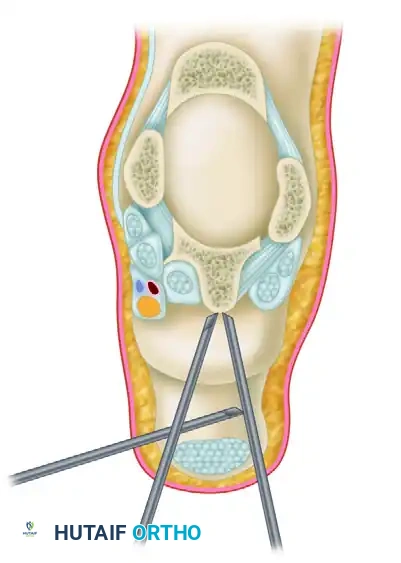
Once tactile metal-on-metal contact is achieved, the medial instrument is slid anteriorly down the shaft of the arthroscope until it hits the posterior bone and enters the arthroscopic field of view. This sliding maneuver guarantees that the instrument bypasses the posteromedial neurovascular bundle safely.
Compartment Preparation and FHL Identification
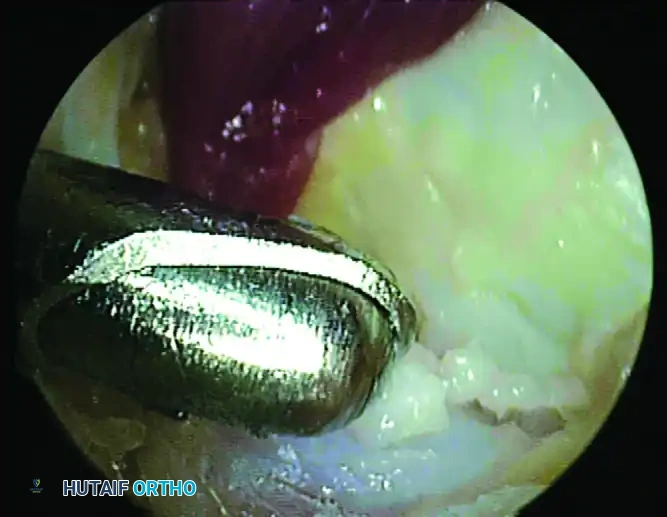
With both portals established, a 4.0-mm or 4.5-mm full-radius arthroscopic shaver is introduced via the posteromedial portal. The initial view is typically obscured by Rouviere's fat pad and the posterior joint capsule. The surgeon begins by systematically resecting this adipose tissue to clear the visual field, taking care to keep the shaver blades facing anteriorly (toward bone) at all times to avoid inadvertently catching posterior structures.
Before any osseous resection occurs, the flexor hallucis longus (FHL) tendon must be positively identified. This is the most critical intraoperative milestone. Using the shaver or a radiofrequency wand, the surgeon carefully clears the soft tissue overlying the FHL muscle belly and tendon. The FHL can be dynamically confirmed by having an assistant passively flex and extend the great toe; the tendon will be seen gliding robustly within its sheath.
Failure to identify the FHL early in the procedure leads to dangerous spatial disorientation. The FHL represents the absolute medial boundary; all pathology to be resected lies lateral to this structure.
Bony Resection and Os Trigonum Excision
Once the FHL is identified and protected, attention is directed to the bony impingement. To mobilize and extract an os trigonum or resect a Stieda process, the surgeon must systematically detach its soft tissue tethers. First, the posterior talofibular ligament (PTFL) is partially detached from the lateral aspect of the ossicle using a radiofrequency wand. Next, the posterior talocalcaneal ligament is released inferiorly. Finally, the proximal aspect of the flexor retinaculum is released to fully expose the bony fragment.
An arthroscopic grasper is used to assess the mobility of the fragment. If it is a fused Stieda process, a 4.0-mm arthroscopic burr is introduced to systematically resect the prominent bone until it is completely flush with the posterior talar body. If it is a separate os trigonum, a combination of a shaver, radiofrequency wand, and grasper is used to shell it out of its soft tissue envelope. The fragment is then extracted through the portal; if the ossicle is particularly large, the portal skin incision may need to be slightly enlarged to accommodate its removal without crushing the skin edges.
Following resection, a dynamic arthroscopic examination is mandatory. The surgeon visualizes the posterior compartment while an assistant passively dorsiflexes and forcefully plantarflexes the ankle. The surgeon must confirm that there is no residual impingement between the posterior lip of the tibia and the superior calcaneus, and that the FHL glides freely without tethering.
Adjunctive Arthroscopic Arthrodesis
In cases where posterior ankle impingement is accompanied by end-stage tibiotalar osteoarthritis, isolated débridement will not yield satisfactory results, and the procedure is converted to an arthroscopic ankle arthrodesis. If joint distraction is required, a transcalcaneal traction pin is placed and hooked to a traction device. Standard anterolateral and anteromedial portals can be added, or the fusion can be performed entirely through the posterior portals.
The articular cartilage is aggressively denuded from the tibial plafond and the talar dome using ring curettes and motorized shavers. An arthroscopic burr is then utilized to meticulously abrade the subchondral bone, removing the sclerotic layer to expose healthy, bleeding cancellous bone. This preparation must be exhaustive to optimize the fusion bed. Once prepared, percutaneous 6.5-mm or 7.0-mm cannulated compression screws are placed across the joint (typically two or three screws in a crossed or parallel configuration) under strict intraoperative fluoroscopic guidance to achieve rigid, compressive fixation.
Complications, Incidence Rates, and Salvage Management
Despite its high success rate and minimally invasive nature, posterior ankle arthroscopy is not without significant risks. The overall complication rate for isolated posterior débridement ranges from 4% to 20% in the literature, though the vast majority of these are minor and transient. The most feared complications are neurological injuries, specifically to the tibial nerve medially and the sural nerve laterally.
Neurological complications are most frequently transient neuropraxias secondary to aggressive portal placement, excessive traction on the soft tissues, or thermal injury from a radiofrequency wand. Sural nerve injury typically occurs during the creation of the posterolateral portal if the skin incision is too deep or if blunt dissection is not utilized. Tibial nerve injury is far more catastrophic and occurs if the surgeon loses spatial orientation and plunges instruments medial to the FHL tendon. Permanent axonotmesis of the tibial nerve requires complex microsurgical nerve grafting and often results in permanent intrinsic foot weakness and plantar numbness.
Infectious complications, including superficial portal site cellulitis or deep joint space septic arthritis, are rare (<1%) but require prompt recognition. Superficial infections are managed with oral antibiotics, while deep infections require emergent arthroscopic irrigation and débridement. Postoperative stiffness and complex regional pain syndrome (CRPS) can also occur, particularly if the patient is non-compliant with early range of motion protocols.
| Complication | Estimated Incidence | Mechanism / Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Transient Sural Neuropraxia | 3% - 8% | Portal placement trauma, retractor pressure. | Observation, gabapentinoids; typically resolves in 3-6 months. |
| Tibial Nerve Injury | < 1% | Plunging instruments medial to the FHL tendon. | Immediate microsurgical exploration and repair/grafting. |
| Superficial Portal Infection | 1% - 2% | Normal skin flora colonization of the incision. | Oral antibiotics (e.g., Cephalexin), local wound care. |
| Deep Septic Arthritis | < 0.5% | Intraoperative contamination or untreated superficial infection. | Emergent arthroscopic I&D, targeted IV antibiotics. |
| Achilles Tendon Injury | < 0.5% | Shaver/burr facing posteriorly during soft tissue clearance. | Open primary repair if >50% torn; conservative if minor. |
| CRPS / Severe Stiffness | 1% - 3% | Inadequate early ROM, exaggerated pain response. | Aggressive physiotherapy, sympathetic nerve blocks, pain management. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following an isolated arthroscopic posterior débridement is designed to be rapid and aggressive, aiming for immediate mobilization to prevent capsular scarring, FHL tethering, and joint stiffness. The protocol is broadly divided into three biological and functional phases.
Phase I: Immediate Postoperative Phase (Weeks 0-2)
Upon completion of the surgery, the portal sites are closed with simple interrupted non-absorbable sutures, and the patient is placed in a bulky compressive dressing or a removable controlled ankle motion (CAM) boot. Weight-bearing as tolerated (WBAT) with crutches is permitted immediately or within the first 48 hours, depending on patient comfort and the extent of the osseous resection. The primary goal in this phase is edema control and the prevention of adhesions. Early active range of motion (ROM) exercises, particularly isolated dorsiflexion and plantar flexion, as well as active great toe flexion/extension, are initiated immediately to ensure the FHL glides freely within its newly decompressed tunnel.
Phase II: Intermediate Rehabilitation Phase (Weeks 2-4)
Sutures are removed between 10 to 14 days postoperatively once the portal sites are completely sealed. The patient is typically weaned off the CAM boot and transitioned to a standard supportive athletic shoe. Physical therapy intensifies significantly during this phase. The focus shifts toward restoring full, symmetric ankle kinematics, enhancing proprioception (using wobble boards and unstable surfaces), and initiating strengthening protocols. Peroneal strengthening and eccentric Achilles stretching are heavily emphasized to restore dynamic stability to the hindfoot.
Phase III: Advanced Sport-Specific Phase (Weeks 4-6+)
By the fourth week, patients should have full, painless range of motion and normal gait mechanics. Rehabilitation transitions to sport-specific training. This includes plyometric exercises, cutting drills, and explosive jumping. Elite athletes are often cleared to return to full, unrestricted training between 4 to 6 weeks, provided they pass functional testing criteria (e.g., single-leg hop tests, pain-free maximal plantar flexion).
(Note: It is critical to recognize that if an adjunctive arthroscopic ankle arthrodesis was performed, this rapid rehabilitation protocol is entirely voided. Arthrodesis patients are placed in a strict non-weight-bearing short leg cast or rigid boot for a minimum of 6 to 8 weeks until definitive radiographic union is observed, followed by a graduated weight-bearing protocol.)
Summary of Landmark Literature and Clinical Guidelines
The clinical efficacy of arthroscopic posterior ankle débridement is supported by a robust body of orthopedic literature, demonstrating highly favorable outcomes and a dramatic shift in the standard of care over the past two decades. Good to excellent clinical outcomes, defined by complete or near-complete pain relief and restoration of pre-injury functional levels, have been consistently reported in 91% to 100% of patients undergoing this procedure for isolated PAI syndrome.
The pioneering work by van Dijk et al. in the late 1990s and early 2000s established the safety and anatomical basis of the prone two-portal technique. Their anatomical studies definitively proved that the FHL tendon could be reliably used as a medial safety boundary, drastically reducing the incidence of tibial nerve injuries that plagued early endoscopic attempts. Subsequent landmark cohort studies have focused heavily on the athletic population. A seminal study by Calder et al. evaluated a cohort of elite professional soccer players undergoing arthroscopic excision of the os trigonum. The study demonstrated that these high-demand athletes were able to return to full professional training at an astonishing average of just 5 weeks postoperatively, with no significant loss of kicking power or agility.
Current clinical guidelines strongly recommend arthroscopy over open surgery for PAI. While long-term comparative studies indicate that both open and arthroscopic techniques eventually yield statistically similar outcomes regarding pain relief at the 1-to-2-year mark, the short-term benefits of arthroscopy are undeniable. The minimally invasive approach offers a definitively earlier return to sports, lower narcotic consumption, and a significantly reduced rate of wound dehiscence and infection.
In the context of arthroscopic ankle arthrodesis for concomitant end-stage arthritis, the literature provides a Grade B recommendation (fair evidence) for its use in ankles with a coronal plane deformity of less than 15 degrees. Multiple prospective and retrospective series have reported that arthroscopic fusion rates are equivalent to open arthrodesis (ranging from 85% to 95%), but with the added benefits of shorter times to radiographic union, decreased blood loss, and profoundly less soft-tissue morbidity. While severe deformity remains a relative contraindication, highly experienced arthroscopists continue to push the boundaries, demonstrating successful arthroscopic fusions even in complex, multi-planar deformities.
In conclusion, arthroscopic posterior débridement remains a highly effective, reproducible, and safe surgical intervention for the management of posterior ankle impingement and os trigonum syndrome. Absolute mastery of the prone two-portal technique, rigorous respect for the anatomical boundaries—most notably the FHL tendon—and meticulous execution of soft tissue and bony resection are the fundamental cornerstones of surgical success. When executed correctly, this procedure reliably offers both elite athletes and the general patient population a rapid, durable return to their pre-injury level of function.
