Preserve Anatomy: Posterior Elbow Approach Without Olecranon Osteotomy
Introduction & Epidemiology
The posterior approach to the elbow joint provides extensive visualization of the distal humerus, olecranon, and coronoid fossa, facilitating complex intra-articular procedures. While various iterations exist, the approach without olecranon osteotomy offers the distinct advantage of preserving the integrity of the olecranon and the triceps insertion, thus mitigating potential complications associated with osteotomy fixation, nonunion, or hardware irritation. This technique maintains the functional continuity of the triceps mechanism, which is critical for elbow extension and stability, thereby potentially accelerating rehabilitation and improving long-term outcomes.
Elbow pathologies requiring a posterior approach are diverse, primarily including complex intra-articular fractures of the distal humerus, particularly AO/OTA Type C fractures, and certain types of olecranon fractures with distal extension. Other indications include total elbow arthroplasty, revision arthroplasty, excision of tumors originating from or abutting the posterior aspect of the distal humerus or proximal ulna, management of elbow stiffness via arthrolysis, and synovectomy. The prevalence of distal humerus fractures, for instance, exhibits a bimodal distribution, affecting younger, active individuals due to high-energy trauma and elderly populations, often with osteopenia, following low-energy falls. The increasing incidence of these injuries, coupled with the functional demands placed on the elbow, underscores the necessity for reproducible and effective surgical approaches that minimize iatrogenic morbidity.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy surrounding the elbow is paramount for safe and effective execution of the posterior approach.
Bony Anatomy
- Distal Humerus: Composed of the trochlea (medial), capitellum (lateral), medial and lateral epicondyles, and the olecranon and coronoid fossae. The supracondylar columns provide structural support.
- Proximal Ulna: Features the olecranon process (articulating with the olecranon fossa), the coronoid process (articulating with the coronoid fossa), and the trochlear notch.
- Proximal Radius: Consists of the radial head (articulating with the capitellum and radial notch of the ulna), radial neck, and radial tuberosity.
Ligamentous Structures
Elbow stability is conferred by both static and dynamic stabilizers. The primary static stabilizers include:
*
Medial Collateral Ligament (MCL) Complex:
Anterior bundle (primary valgus stabilizer), posterior bundle, and transverse ligament.
*
Lateral Collateral Ligament (LCL) Complex:
Radial collateral ligament, lateral ulnar collateral ligament (LUCL – critical for posterolateral rotatory stability), and annular ligament.
Preservation or meticulous repair of these structures is essential to prevent post-operative instability.
Musculotendinous Units
- Triceps Brachii: Comprises three heads (long, lateral, medial) converging into a broad aponeurosis that inserts predominantly onto the olecranon process. The triceps mechanism is the primary extensor of the elbow and contributes significantly to posterior stability.
- Anconeus: A small, triangular muscle originating from the posterior aspect of the lateral epicondyle and inserting onto the lateral side of the olecranon and proximal ulna. It assists in elbow extension and stabilization. Its blood supply is robust, making it a reliable pedicle for soft tissue flaps.
- Flexor Carpi Ulnaris (FCU): Originates from the medial epicondyle and olecranon. Its fascia forms part of the medial flap in some triceps-sparing approaches.
Neurovascular Structures
- Ulnar Nerve: Passes through the cubital tunnel posterior to the medial epicondyle, susceptible to injury during medial dissection or retraction. It supplies the FCU and medial half of the FDP, along with intrinsic hand muscles.
- Radial Nerve: Divides into superficial and deep branches anterior to the lateral epicondyle, supplying the anconeus, triceps, and supinator, and then innervating forearm extensors. It is generally protected laterally by the anconeus.
- Brachial Artery and its Collateral Branches: These provide blood supply to the joint and surrounding musculature. Anastomotic networks around the elbow are rich.
Biomechanics
The elbow is a trochleogingylomoid joint, allowing flexion and extension, with supination and pronation occurring at the proximal radioulnar joint. The olecranon-trochlear articulation provides significant bony stability, particularly in extension. The triceps' contribution to elbow extension is fundamental, and preserving its functional integrity is paramount for restoring normal kinematics. Any compromise to the triceps insertion or its muscle belly can lead to extensor lag and functional impairment. The lateral stability conferred by the LUCL is crucial to resist posterolateral rotatory instability.
Indications & Contraindications
The decision to utilize a posterior approach without olecranon osteotomy hinges on a comprehensive assessment of the patient's pathology, overall health, and the surgeon's experience.
Indications
-
Distal Humerus Fractures:
- Complex intra-articular fractures (e.g., AO/OTA Type C, comminuted supracondylar-intercondylar fractures) requiring extensive exposure for reduction and stable internal fixation.
- Certain capitellum or trochlear fractures that require direct posterior visualization.
- Fractures with significant posterior displacement or impaction.
-
Total Elbow Arthroplasty (TEA):
- Primary TEA for rheumatoid arthritis, osteoarthritis, or unreconstructable distal humerus fractures.
- Revision TEA.
-
Tumor Excision:
- Benign or malignant lesions of the distal humerus, olecranon, or surrounding soft tissues that are best accessed posteriorly.
-
Arthrolysis for Elbow Stiffness:
- Release of posterior capsular contractures, excision of heterotopic ossification (HO) in the olecranon fossa or posterior compartment.
-
Synovectomy:
- For inflammatory arthritides predominantly affecting the posterior elbow.
-
Removal of Loose Bodies:
- When intra-articular loose bodies are located posteriorly or require broad exposure for retrieval.
Contraindications
- Severe Soft Tissue Compromise: Extensive scarring, active infection, or poor vascularity in the posterior elbow region may preclude this approach.
- Inadequate Exposure: For specific fracture patterns (e.g., highly comminuted anterior coronoid fractures, certain types of radial head fractures) that may require an anteromedial or anterolateral approach for optimal reduction and fixation.
- Pre-existing Triceps Pathology: Significant triceps tendon rupture or avulsion may complicate mobilization of the triceps flap.
- Certain Revision Cases: Where previous posterior approaches have compromised the triceps mechanism beyond repair or sufficient tissue for a flap.
Operative vs. Non-Operative Indications
| Indication Category | Non-Operative Management | Operative Management (Posterior Approach) |
|---|---|---|
| Fractures |
- Stable, minimally displaced olecranon fractures (Type I & IIA)
- Stable, non-displaced distal humerus fractures (rare) - Stress fractures without displacement - Avulsion fractures of triceps with minimal displacement and preserved extension |
- Displaced intra-articular distal humerus fractures (Type C)
- Complex olecranon fractures (Type IIB, III) - Open fractures requiring debridement and stabilization - Capitellum/trochlear fractures requiring ORIF |
| Arthritis |
- Early osteoarthritis or inflammatory arthritis with mild symptoms
- Failed conservative management - Contraindications to surgery |
- End-stage arthritis (rheumatoid, osteoarthritis) causing severe pain and dysfunction
- Unreconstructable fractures in elderly patients (for TEA) - Post-traumatic arthritis with severe pain and limited ROM |
| Tumors |
- Benign lesions with minimal symptoms and no risk of malignant transformation
- Follow-up for incidentally found lesions |
- Symptomatic benign tumors
- Malignant tumors requiring wide excision or reconstruction - Tumors causing bone destruction or pathological fracture |
| Stiffness |
- Early stages of post-traumatic stiffness responding to aggressive physical therapy
- Contraindications to surgical release |
- Established elbow contractures (flexion/extension deficit >30°)
- Impingement due to heterotopic ossification - Failed non-operative treatment |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are crucial for successful surgical outcomes.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, including neurovascular status, range of motion, and assessment of soft tissue integrity.
-
Imaging Studies:
- Standard Radiographs: Anteroposterior (AP), lateral, and oblique views of the elbow.
- Computed Tomography (CT) Scans: Essential for complex intra-articular fractures, providing detailed information on fracture morphology, fragment displacement, articular involvement, and comminution. 3D reconstructions are invaluable for pre-operative templating of reduction strategies and implant placement.
- Magnetic Resonance Imaging (MRI): Useful for assessing soft tissue tumors, ligamentous injuries, or occult fractures not visible on plain radiographs or CT.
- Templating: For arthroplasty, templating on radiographs or CT is performed to determine implant size and position. For fracture fixation, planning the number, type, and trajectory of screws and plates is critical.
- Implant Selection: Selection of appropriate hardware (e.g., pre-contoured locking plates, low-profile implants) for specific fracture patterns or prosthetic components for arthroplasty.
- Tourniquet Considerations: Assessment of patient comorbidities influencing tourniquet time and pressure.
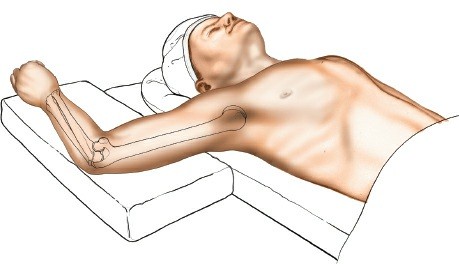
Patient Positioning
The patient is typically placed in a lateral decubitus position on the operating table, as indicated by the original content. This position allows for unrestricted elbow flexion and extension during the procedure, facilitating exposure and assessment of reduction and stability.

- Padded Table: Ensure adequate padding for the chest, pelvis, and particularly the contralateral arm and lower extremities to prevent pressure-related neuropathies or skin breakdown.
- Affected Limb: The arm is exsanguinated by elevation and a pneumatic tourniquet is applied as high as possible on the arm.
- Arm Support: The elbow is allowed to flex over the side of the table, with the forearm and hand lying freely. This can be facilitated by a sterile arm holder or by an assistant providing stable support.
-
Alternative Positions:
- Prone Position: The arm can be positioned on an arm board, allowing for similar range of motion. This is particularly useful for bilateral procedures or when specific imaging angles are required. However, it may limit access for an anesthesiologist.
- Supine Position with Arm Board: Less common for complex posterior approaches due to restricted elbow positioning, but can be utilized for more straightforward cases.

*
Sterilization:
The limb should be prepped and draped from the shoulder to the hand, allowing for full range of motion throughout the procedure.
Detailed Surgical Approach / Technique
The posterior approach without olecranon osteotomy aims to create a robust soft tissue flap that can be reflected to expose the elbow joint, while preserving the triceps insertion. The technique described here is commonly referred to as the anconeus-based triceps-sparing or triceps-reflecting approach .
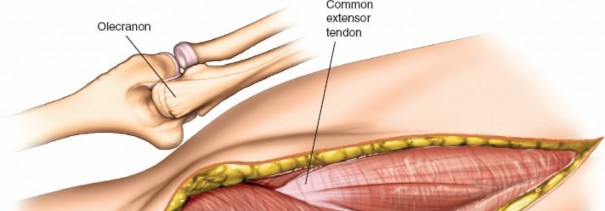
Landmarks and Incision

-
Palpate and Mark:
- Olecranon process: The prominent bony tip of the ulna.
- Medial epicondyle: Medial bony prominence of the distal humerus.
- Lateral epicondyle: Lateral bony prominence of the distal humerus.
- Ulnar nerve course: Palpate the ulnar nerve posterior to the medial epicondyle to anticipate its location.
-
Skin Incision: A straight posterior skin incision is preferred. It typically extends from approximately 5-7 cm proximal to the olecranon tip to about 3-4 cm distal to it. Some surgeons prefer a slightly curved or "S" shaped incision to allow for greater skin mobility. The incision should be centered over the olecranon.
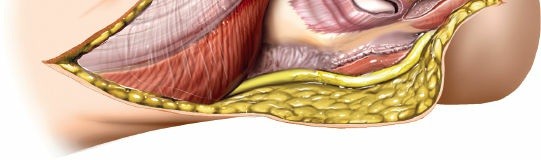
Subcutaneous Dissection & Ulnar Nerve Management
- Full-Thickness Flaps: Incise the skin and subcutaneous tissue. Raise full-thickness skin flaps medially and laterally to expose the deep fascia. This protects the cutaneous nerves and maintains vascularity to the skin.
-
Identify Ulnar Nerve:
The ulnar nerve is consistently identified and protected. It lies in the cubital tunnel posterior to the medial epicondyle. Carefully dissect it free from surrounding retinaculum and fascia. Its course proximally can be traced superior to the medial epicondyle, and distally beneath the fascia of the FCU.
- Ulnar Nerve Transposition (Optional but common): If significant distal humerus fracture comminution or hardware placement is anticipated to encroach upon the nerve, or if pre-existing ulnar nerve symptoms are present, anterior subcutaneous or submuscular transposition of the ulnar nerve is performed. This involves freeing the nerve proximally and distally, ensuring its release from all potential compression points, and relocating it anteriorly.

Triceps Mechanism Mobilization (Anconeus-Based Flap)
This specific technique, as outlined in the seed content, involves creating a triceps-fascia-FCU flap based laterally on the anconeus.
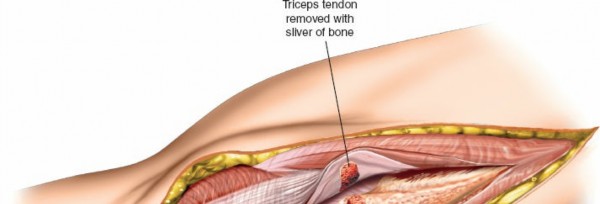
- Identify Triceps Aponeurosis: The triceps aponeurosis is visualized inserting onto the olecranon. Identify the fascia overlying the medial aspect of the triceps and the origin of the FCU.
- Incision of Triceps Fascia: Make a longitudinal incision through the triceps aponeurosis and fascia along the medial border of the triceps, extending from proximal to the olecranon to the musculotendinous junction. Continue this incision distally into the fascia overlying the flexor carpi ulnaris (FCU) muscle, several centimeters distal to the olecranon.
- Subperiosteal Dissection (Medial): Elevate the triceps-fascia-FCU flap subperiosteally from the medial aspect of the olecranon and the proximal ulna. This detachment allows for medial reflection of the entire triceps insertion.
-
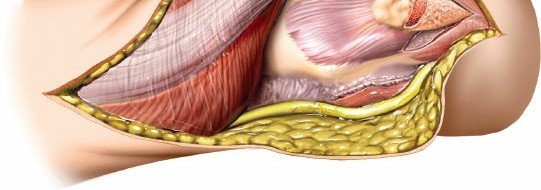
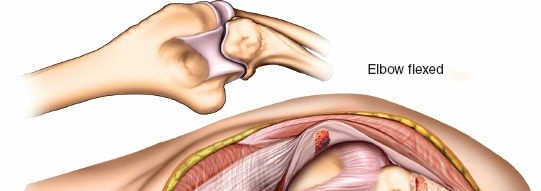
Reflection of Flap:
The entire triceps muscle, its insertion into the olecranon, and the fascia covering the flexor carpi ulnaris muscle are reflected medially as a single unit. The flap remains attached laterally to the anconeus muscle, which serves as its vascular pedicle and pivot point.
- Key Concept: The anconeus muscle's robust blood supply allows it to sustain the viability of the reflected triceps flap. The origin of the anconeus from the lateral epicondyle and its insertion onto the lateral aspect of the olecranon and ulna are kept intact.
- Dissection along lateral border of triceps: To achieve full reflection, the lateral border of the triceps may need to be carefully dissected from the posterolateral capsule, ensuring protection of the radial nerve branch to the anconeus.
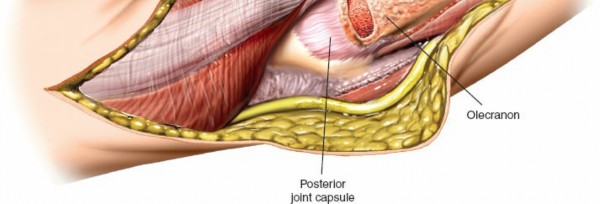
- Exposure of Posterior Capsule: Once the triceps-anconeus flap is fully mobilized and reflected, the posterior elbow capsule is exposed.
* This image likely depicts the triceps flap being reflected, exposing the underlying capsule or joint.
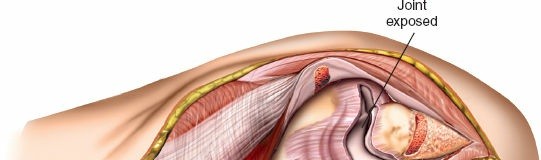
Capsulotomy and Joint Exposure
- "H" or Inverted "V" Capsulotomy: Incise the posterior capsule to gain access to the joint. A common technique is an "H" shaped capsulotomy, with a transverse incision across the olecranon fossa and two longitudinal limbs extending proximally and distally. An inverted "V" shaped capsulotomy with the apex pointing distally can also be performed.
- Joint Visualization: With the capsule opened, the olecranon fossa, distal humerus articular surface (trochlea and capitellum), and the coronoid process can be visualized. Dynamic elbow flexion and extension will aid in visualizing different aspects of the joint.

* This image shows the exposed olecranon fossa and posterior distal humerus, with the triceps mechanism retracted.
Reduction and Internal Fixation (for Fractures)
- Fragment Identification and Debridement: Identify all fracture fragments. Remove hematoma, loose bone fragments, and soft tissue interposition from the fracture site.
- Provisional Reduction: Use reduction clamps, Kirschner wires (K-wires), or temporary screws to achieve anatomical reduction of the articular surface. Begin with the most stable or largest fragments, typically focusing on the medial and lateral columns.
-
Definitive Fixation:
- Distal Humerus: Dual plating (medial and lateral column plating) is the gold standard for most complex distal humerus fractures. Plates are typically applied in a 90-90 configuration or parallel configuration. Screws are inserted to achieve interfragmentary compression where possible and provide stable fixation.
- Olecranon: For specific olecranon fractures, tension band wiring or plate fixation may be used.
- Articular Surface Assessment: Thoroughly assess the articular congruity under direct visualization and fluoroscopy throughout the reduction and fixation process.
- Stability Assessment: After fixation, gently move the elbow through a full range of motion to assess stability, implant prominence, and potential for impingement.
Total Elbow Arthroplasty (TEA)
- Component Preparation: After joint exposure, the distal humerus and proximal ulna are prepared using specific instrumentation to accommodate the prosthetic components. This involves sequential reaming and milling.
- Trial Reduction: Trial components are inserted to assess range of motion, stability, and alignment.
- Definitive Implantation: Cemented or uncemented components are implanted according to manufacturer guidelines.
Closure
- Capsule Repair: The posterior capsule is meticulously repaired using absorbable sutures. This helps restore joint integrity and provides an additional layer of soft tissue coverage.
- Triceps-Anconeus Flap Reattachment: The mobilized triceps-anconeus flap is securely reattached to its original insertion site on the medial aspect of the olecranon and proximal ulna using strong, non-absorbable sutures through drill holes or via transosseous sutures. Ensuring a robust repair is critical to prevent extensor lag.
- Fascial Closure: The deep fascia is closed, followed by subcutaneous tissue approximation.
- Skin Closure: The skin is closed with sutures or staples.
- Drainage: A suction drain may be placed if significant bleeding is anticipated, particularly in trauma cases.
Complications & Management
Despite meticulous surgical technique, complications can arise following a posterior elbow approach without olecranon osteotomy. Proactive recognition and appropriate management are crucial for optimal outcomes.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Etiology | Clinical Presentation | Management / Salvage Strategy |
|
Infection (SSI)
| ~1-5% | Surgical site contamination, post-op wound complications, patient factors. | Erythema, induration, warmth, pain, purulent discharge, fever, malaise. |
Superficial:
Oral antibiotics, local wound care.
Deep:
Surgical debridement, IV antibiotics (culture-guided), hardware removal if unstable or continued infection. For prosthetic joints, explantation and two-stage revision. |
|
Ulnar Neuropathy
| 5-20% (transient) | Direct trauma, traction, compression, pre-existing cubital tunnel syndrome, HO, unmanaged intra-op swelling/positioning. | Numbness/paresthesias in the ulnar nerve distribution (small finger, ulnar half of ring finger, ulnar forearm), intrinsic muscle weakness. |
Conservative:
Splinting, activity modification, NSAIDs.
Surgical:
Decompression and/or anterior transposition (subcutaneous or submuscular) if persistent or progressive deficits. Ensure complete release proximally and distally. |
|
Elbow Stiffness/Contracture
| 10-30% | Post-operative pain, inadequate rehabilitation, HO, arthrofibrosis, prolonged immobilization, swelling. | Restricted active and passive range of motion (flexion and/or extension deficit). |
Conservative:
Aggressive physical therapy, dynamic/static progressive splinting, manipulation under anesthesia (MUA) for appropriate cases.
Surgical:
Arthroscopic or open arthrolysis with capsular release and HO excision. |
|
Heterotopic Ossification (HO)
| 10-50% (radiographic), <5% (symptomatic) | Trauma severity, prolonged operative time, head injury, prior HO, genetic predisposition. | Pain, warmth, swelling, progressive loss of ROM beyond expected. |
Prophylaxis:
NSAIDs (Indomethacin) for 3-6 weeks, or single-dose radiation therapy (700-800 cGy within 72 hours pre/post-op), especially in high-risk patients.
Management:
Excision of mature HO after bone scan or plain radiograph maturation (typically 6-12 months post-op), combined with prophylaxis. |
|
Triceps Insufficiency/Avulsion
| <5% | Inadequate repair during closure, excessive tension, early aggressive rehabilitation, infection. | Extensor lag, inability to actively extend the elbow against gravity, pain with attempted extension. |
Conservative:
Prolonged immobilization in extension for partial tears.
Surgical:
Re-repair of the triceps mechanism (primary repair with transosseous sutures), augmentation with local tissue (e.g., fascial graft) or allograft for chronic or large defects. |
|
Wound Healing Complications
| 5-15% | Hematoma, seroma, skin edge necrosis, infection, excessive tension. | Erythema, drainage, skin dehiscence, local tenderness. |
Conservative:
Local wound care, dressing changes, debridement of necrotic tissue, antibiotics for infection.
Surgical:
Debridement, secondary closure, rotational or free flap coverage for large defects. |
|
Nonunion/Malunion (Fractures)
| 5-10% | Inadequate fixation, infection, poor bone quality, devitalized fragments, delayed union, early weight-bearing. | Persistent pain, instability, deformity, lack of radiographic healing, functional impairment. |
Surgical:
Revision ORIF with bone grafting (autograft or allograft), exchange nailing, or conversion to arthroplasty (for severe cases or elderly). For malunion, corrective osteotomy. |
|
Implant-Related Complications
| Variable | Screw prominence, plate irritation, breakage, loosening (arthroplasty). | Pain, tenderness over hardware, impingement, mechanical symptoms, radiographic signs of loosening. |
Surgical:
Hardware removal (if fracture healed), revision fixation, component revision (for arthroplasty). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is pivotal for restoring elbow function while protecting the surgical repair. Protocols are tailored to the specific pathology, surgical stability achieved, patient factors, and surgeon preference. The preserved triceps insertion in this approach generally allows for more aggressive, earlier mobilization compared to osteotomy-based approaches.
General Principles
- Pain Management: Adequate analgesia is critical to facilitate participation in therapy.
- Edema Control: Elevation, gentle compression, and cryotherapy help manage swelling.
- Protection of Surgical Site: Maintain wound integrity and prevent excessive stress on soft tissue repairs.
- Progressive Mobilization: Gradually restore range of motion (ROM) to prevent stiffness.
- Progressive Strengthening: Restore muscle strength and endurance.
- Patient Education: Instruct patients on precautions, exercises, and expected recovery trajectory.
Phases of Rehabilitation
Phase I: Immobilization and Early Protected Motion (Weeks 0-3)
- Goal: Protect soft tissue and bone repair, manage pain and swelling, initiate gentle ROM.
-
Immobilization:
- Fractures (ORIF): Typically splinted in 60-90 degrees of flexion for 1-2 weeks, then transitioned to a hinged elbow brace. The brace settings depend on the stability of fixation, often allowing 30-100 degrees of motion.
- Total Elbow Arthroplasty: Often immobilized in a posterior splint or hinged brace for 1-2 weeks, typically allowing 30-90 degrees of motion.
-
Range of Motion:
- Passive & Active-Assistive ROM (AAROM): Begin gentle, gravity-assisted flexion and passive extension exercises within the protected range. Focus on gentle wrist and hand ROM.
- Continuous Passive Motion (CPM) machine: May be used for 2-4 hours daily, particularly for arthrolysis or stiffness cases.
-
Precautions:
- No active resisted elbow extension against gravity due to triceps repair.
- Avoid lifting, pushing, or pulling.
- Monitor for signs of infection or nerve compromise.
Phase II: Moderate Protection and Progressive Motion (Weeks 3-8)
- Goal: Gradually increase ROM, initiate gentle strengthening, improve functional use.
-
Range of Motion:
- Advance passive and active ROM as tolerated, aiming for full flexion and gradual extension gains.
- Hinged brace settings are opened progressively (e.g., 0-130 degrees by week 6-8), as dictated by stability and patient tolerance.
-
Strengthening:
- Isometrics: Begin gentle isometric contractions for triceps, biceps, and forearm muscles within pain limits.
- Light Resistance: Progress to very light resistance exercises for wrist and hand.
- Elbow: Gentle active elbow flexion and active-assisted extension exercises. Avoid resisted elbow extension to protect triceps repair until radiographic union for fractures or robust soft tissue healing.
- Functional Activities: Begin light activities of daily living (ADLs) within pain limits, avoiding significant weight-bearing on the affected arm.
Phase III: Advanced Strengthening and Return to Activity (Weeks 8-16+)
- Goal: Achieve full, functional ROM, progressive strengthening, prepare for return to activity.
- Range of Motion: Continue working on any remaining ROM deficits.
-
Strengthening:
- Progress to moderate resistance exercises for all elbow and forearm musculature.
- Gradually introduce resisted elbow extension (e.g., light weights, elastic bands), building triceps strength.
- Incorporate eccentric exercises.
- Proprioception and Endurance: Begin exercises to improve proprioception and muscular endurance.
- Functional Activities: Gradually increase the complexity and intensity of ADLs.
-
Return to Activity:
- Low-impact sports/activities: Typically cleared around 3-4 months post-op, assuming good strength and ROM.
- High-impact/overhead sports or heavy labor: May require 6 months or longer, depending on the severity of the initial injury and surgical procedure, with full radiographic healing for fractures.
Specific Considerations
- Heterotopic Ossification Prophylaxis: Continue NSAIDs or radiation as prescribed if initiated.
- Ulnar Nerve Symptoms: Monitor for signs of ulnar neuropathy and adjust therapy accordingly.
- Fracture Healing: For ORIF, progression of weight-bearing and aggressive strengthening is often guided by radiographic evidence of bone healing.
- Patient Compliance: Emphasize the importance of adherence to protocols to prevent stiffness or re-injury.
Summary of Key Literature / Guidelines
The posterior elbow approach without olecranon osteotomy has evolved significantly, with various triceps-sparing and triceps-reflecting techniques gaining prominence for their potential to reduce osteotomy-related morbidity.
- Early Work: The pioneering work of Bryan and Morrey in the 1980s described a triceps-reflecting approach that involved detachment of the triceps tendon, often with a small wafer of olecranon, to optimize exposure for total elbow arthroplasty. While highly effective, the subsequent need for triceps reattachment carried inherent risks of detachment.
-
Triceps-Sparing Approaches:
Subsequent research and clinical experience led to the development of truly triceps-sparing approaches, such as the triceps-splitting (e.g., Campbell's approach, Mayo modified approach) and the anconeus-based triceps flap technique. These techniques prioritize preserving the triceps insertion to maintain its mechanical advantage and reduce complications.
- Anconeus-Based Flap: This approach, as detailed in this discussion, capitalizes on the robust vascularity of the anconeus muscle, allowing the entire triceps aponeurosis and a portion of the FCU fascia to be reflected medially, hinged on the anconeus laterally. Studies have demonstrated its efficacy in providing excellent exposure for distal humerus fractures and arthroplasty while maintaining triceps integrity.
- Outcomes & Complications: Comparative studies evaluating triceps-sparing versus olecranon osteotomy approaches for distal humerus fractures or TEA have shown varying results. Generally, triceps-sparing approaches are associated with lower rates of triceps insufficiency, nonunion, and hardware-related complications compared to osteotomy techniques. However, they can be technically more demanding, requiring careful soft tissue handling to avoid devascularization of the triceps flap. Stiffness and ulnar neuropathy remain common complications across all posterior approaches, irrespective of osteotomy use. Heterotopic ossification is also a recognized post-operative sequela, with varying incidence depending on the patient population and prophylactic measures.
- Current Consensus: For the majority of distal humerus fractures requiring ORIF and for total elbow arthroplasty, the preference is generally shifting towards techniques that avoid olecranon osteotomy where feasible. This is driven by the desire to minimize surgical morbidity, optimize rehabilitation, and potentially improve long-term functional outcomes. The anconeus-based triceps-reflecting approach offers a versatile and effective method to achieve this goal, providing ample exposure while preserving critical anatomical structures. The choice of specific triceps-sparing technique often depends on the exact pathology, surgeon comfort, and the extent of exposure required. For highly comminuted fractures or complex revision arthroplasty, some surgeons may still opt for an osteotomy to ensure maximal exposure and facilitate the most accurate reduction and fixation.
In conclusion, the posterior elbow approach without olecranon osteotomy, particularly the anconeus-based triceps-reflecting technique, represents a refined surgical method that offers extensive exposure of the elbow joint while preserving the vital triceps mechanism. Its continued application and refinement are central to achieving optimal functional recovery in patients undergoing complex elbow surgery.
Clinical & Radiographic Imaging