Introduction and Rationale
Radial longitudinal deficiency, commonly referred to as radial clubhand, presents a complex reconstructive challenge characterized by a spectrum of preaxial upper extremity anomalies. Among the most functionally debilitating aspects of this condition is the severe deficiency or complete congenital absence of the thumb. While children with radial dysplasia demonstrate remarkable neuroplasticity—often adapting to a thumbless hand by developing a compensatory ulnar-side-of-index to radial-side-of-long finger prehension, or a generalized finger-to-palm grasp—these adaptations are biomechanically inferior.
Despite this adaptability, overall hand function, fine motor dexterity, and long-term self-care capabilities remain significantly impaired. Successful pollicization of the index finger fundamentally alters the functional trajectory of the child's life, restoring the critical biomechanics of opposition, power pinch, and grasp.
Clinical Pearl: Normal and compensatory prehensile patterns are firmly established within the central nervous system during the first year of life. Therefore, to maximize cortical integration and functional outcomes, surgical reconstruction via pollicization should ideally be performed early, typically between 6 and 12 months of age.
Indications and Optimal Timing
Pollicization is universally recommended for both unilateral and bilateral cases of severe thumb hypoplasia (Modified Blauth Types IIIB, IV, and V) associated with radial clubhand.
In cases where a "floating thumb" (pouce flottant) deformity is present—characterized by a vestigial digit with inadequate musculotendinous connections and absent basal bony support—the remnant must be amputated prior to or concurrent with pollicization.
Surgical Warning: Surgeons must engage in thorough preoperative counseling with the parents. It must be unequivocally communicated that the floating thumb possesses no functional utility, cannot be reconstructed into a stable post, and will be discarded to allow for the creation of a biomechanically sound thumb utilizing the index finger.
While single-stage toe-to-hand transfers have been reported with success in certain congenital anomalies, the index finger remains the unequivocally preferred donor digit in radial dysplasia. The index finger provides superior anatomical proportions, highly acceptable aesthetic outcomes, and significantly less donor-site morbidity compared to microvascular toe transfers.
Delaying the procedure beyond the early developmental window can lead to persistent side-to-side grip patterns between the index and long fingers, particularly when handling smaller objects, as the child's motor cortex has already hardwired the compensatory thumbless grasp. Furthermore, it is well-documented that the functional outcome after pollicization in children with associated radial aplasia (and its inherent stiffness or soft tissue contractures) is generally less rewarding than in those with isolated thumb aplasia; thus, meticulous surgical execution is paramount.


Biomechanical Principles of the Buck-Gramcko Technique
The modern standard for index finger pollicization was popularized by Dieter Buck-Gramcko. His technique relies on profound anatomical reconfiguration rather than simple transposition. The core biomechanical tenets include:
- Skeletal Reassignment: The entire index metacarpal is resected except for the metacarpal head, which is preserved and rotated to act as the new trapezium. The index proximal phalanx becomes the new first metacarpal, the proximal interphalangeal (PIP) joint becomes the new metacarpophalangeal (MCP) joint, and the distal interphalangeal (DIP) joint becomes the new interphalangeal (IP) joint.
- Spatial Orientation: The index finger must be rotated exactly 160 degrees along its longitudinal axis to place the finger pulp into a true position of apposition facing the remaining digits. It is then secured in 40 degrees of palmar abduction.
- Prevention of Hyperextension Instability: A common pitfall is postoperative hyperextension at the new "CMC" joint. This is prevented by positioning the metacarpal head in 70 to 80 degrees of hyperextension relative to the proximal phalanx before rigid fixation.
- Dynamic Muscle Rebalancing: The intrinsic and extrinsic muscles of the index finger are detached and reassigned to replicate the absent thenar musculature, providing both functional control and aesthetic bulk.
Surgical Technique: The Buck-Gramcko Pollicization
Patient Positioning and Preparation
The patient is placed supine with the operative arm extended on a radiolucent hand table. General anesthesia is administered, and a well-padded pneumatic tourniquet is applied to the proximal arm. Loupe magnification (minimum 2.5x to 3.5x) is essential for the meticulous neurovascular dissection required in the pediatric hand.

Incision Design and Skin Flaps
The incision design is critical for creating a wide, supple first web space without tension.
- Palmar Incision: Make an S-shaped incision down the radial side of the hand, extending just onto the palmar surface. Begin this incision near the base of the index finger on the palmar aspect and terminate it proximally, just proximal to the wrist crease.
- Transverse Connecting Incision: Make a slightly curved transverse incision across the base of the index finger on the palmar surface. This should connect at right angles to the distal end of the first S-shaped incision.
- Dorsal Incision: Make a third incision on the dorsum of the proximal phalanx of the index finger, starting from the level of the PIP joint and extending proximally to meet the incision around the base of the index finger.
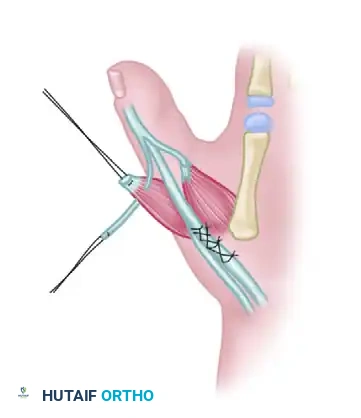
Neurovascular Dissection
Mobilization of the neurovascular pedicle is the most delicate phase of the operation. The index finger must survive on its native neurovascular bundles while being radically repositioned.
- Arterial Mobilization: Through the palmar incision, identify and free the common neurovascular bundle between the index and long fingers. To allow the index finger to be transposed radially and proximally without tethering, ligate and divide the proper digital artery supplying the radial side of the long finger.
- Neural Separation: Carefully separate the common digital nerve into its component proper digital nerves for the index and long fingers. This intraneural dissection must be carried proximally high into the palm to ensure absolutely no tension is present on the nerve after the index finger is rotated 160 degrees.
- Anomalous Structures: Occasionally, an anomalous neural ring is found encircling the digital artery. If encountered, this ring must be carefully split under magnification so that the artery does not kink or angulate after transposition.
- Note: In cases where the radial digital artery to the index finger is congenitally absent, pollicization can still be safely performed on a single vascular pedicle (the ulnar digital artery of the index finger), provided it is robust.
- Venous Preservation: On the dorsal aspect of the hand, meticulously preserve at least one, preferably two, of the large dorsal draining veins. Venous congestion is a primary cause of flap and digit failure in pollicization.
Musculotendinous Dissection
- Extrinsic Extensors: On the dorsum of the hand, identify the extensor digitorum communis (EDC) tendon to the index finger and sever it at the level of the metacarpophalangeal joint.
- Intrinsic Muscles: Identify the first dorsal interosseous (DI) and the first palmar interosseous (PI) muscles. Detach these interosseous muscles from their insertions on the proximal phalanx and the lateral bands of the dorsal aponeurosis.
- Muscle Stripping: Partially strip the origins of the interosseous muscles subperiosteally from the shaft of the second metacarpal. Exercise extreme caution during this step to preserve the neurovascular structures lying in close proximity to the muscle bellies.
Osteotomy and Skeletal Reconfiguration
The skeletal shortening and repositioning transform the long, triphalangeal index finger into a proportionally accurate thumb.


- Metacarpal Resection: Perform an osteotomy to resect the shaft of the second metacarpal.
- If the phalanges of the index finger are of normal length, resect the entire metacarpal shaft.
- The base of the metacarpal may be retained if necessary to achieve the proper length of the new thumb, though typically, the entire shaft is removed.
- Creating the New Trapezium: The retained metacarpal head will act as the new trapezium. Rotate the metacarpal head into flexion.
- Skeletal Fixation: Bring the proximal phalanx into complete hyperextension (70 to 80 degrees) in relation to the metacarpal head. This maximizes the stability of the new joint and prevents postoperative hyperextension deformity at the new "carpometacarpal" joint.
- Rotation and Abduction: Rotate the entire digit 160 degrees along its long axis to allow for true pulp-to-pulp apposition. Position the skeleton in approximately 40 degrees of palmar abduction.
- Pinning: Fix the metacarpal head to the carpus (or the retained metacarpal base) using one or two smooth Kirschner wires (K-wires). In very young children, the unossified carpal bones can often be pierced directly with a sharp needle or fine K-wire. Bony union at this junction is not strictly essential; robust fibrous fixation of the head is sufficient for excellent clinical function.

Tendon Transfers and Biomechanical Rebalancing
Reattaching the intrinsic and extrinsic muscles is vital for dynamic thumb control and for creating a cosmetically acceptable thenar eminence.
- New Abductor Pollicis Longus (APL): Suture the proximal end of the detached extensor digitorum communis (EDC) tendon to the base of the former proximal phalanx (which now acts as the first metacarpal). This provides basal abduction.
- New Extensor Pollicis Longus (EPL): Section the extensor indicis proprius (EIP) tendon, shorten it appropriately to account for the skeletal shortening, and repair it via end-to-end anastomosis.
- New Thenar Intrinsics (Milford's Technique): Milford stressed the critical importance of suturing the intrinsic tendons directly into the lateral bands to enhance extension of the new IP joints.
- Weave the lateral bands through the distal part of the interosseous muscles and turn them back distally to form a loop, suturing it to itself.
- First Palmar Interosseous (PI): Transferred to function as the new Adductor Pollicis (AP).
- First Dorsal Interosseous (DI): Transferred to function as the new Abductor Pollicis Brevis (APB).
- Flexor Pollicis Longus (FPL) Adjustment (Bartlett's Modification): Bartlett emphasized the importance of shortening the flexor pollicis longus (formerly the flexor digitorum profundus of the index) by an amount exactly equal to the length of the excised metacarpal. This restores the resting length-tension relationship and significantly enhances flexion power.
Skin Closure
Skin closure must be performed without any tension to prevent vascular compromise of the transposed digit.
- Fashion the dorsal skin flap to close the defect over the proximal phalanx.
- Rotate and advance the remaining palmar and lateral flaps to construct a wide, deep, and supple first web space.
- Use fine absorbable sutures (e.g., 5-0 or 6-0 chromic gut or fast-absorbing plain gut) to avoid the need for suture removal in a pediatric patient.




Postoperative Protocol and Rehabilitation
Immediate postoperative care is focused on protecting the vascularity of the transposed digit and allowing the tendon transfers and skeletal fixation to heal.
- Immobilization: The hand and forearm are immobilized in a well-padded, long-arm cast or rigid splint. The new thumb is positioned in palmar abduction and opposition, with the wrist in slight extension.
- Duration: Absolute immobilization is maintained for exactly 3 weeks.
- Pin Removal: At the 3-week mark, the cast is removed in the clinic. If K-wires were left protruding through the skin, they are extracted at this time. If buried, they may be left in place or removed later depending on surgeon preference and radiographic healing.
- Rehabilitation: Careful, active range-of-motion exercises are initiated immediately following cast removal. In pediatric patients, formal physical therapy is often substituted with "play therapy." Occupational therapists guide the parents in encouraging the child to grasp large objects (blocks, balls) initially, progressively moving to smaller objects (cereal pieces, beads) to stimulate the development of fine pinch mechanics.
- Night Splinting: A thermoplastic web-spacer splint is often fabricated for nighttime use over the next 3 to 6 months to prevent adductor contracture of the newly constructed first web space.
Complications and Pitfalls
While highly successful when executed correctly, pollicization carries specific risks:
* Vascular Compromise: The most devastating complication. Usually results from inadequate mobilization of the neurovascular bundle, failure to ligate the radial digital artery to the long finger, or tight skin closure.
* Hyperextension Deformity: Occurs if the metacarpal head is not adequately hyperextended (70-80 degrees) relative to the proximal phalanx during initial K-wire fixation.
* Web Space Contracture: Results from poorly designed skin flaps or failure to utilize postoperative night splinting.
* Weak Pinch: Often due to failure to appropriately shorten the extrinsic tendons (EIP and FDP) to match the new skeletal length, leading to a biomechanical lag.
