Introduction to Cavovarus Foot Reconstruction
The management of the rigid cavovarus foot presents one of the most formidable challenges in reconstructive foot and ankle surgery. Often presenting as a progressive deformity secondary to neuromuscular disorders—most notably Charcot-Marie-Tooth (CMT) disease—or following severe trauma, the cavovarus foot is characterized by a complex, multiplanar structural abnormality. The primary driver of this deformity is typically a rigid forefoot equinus, predominantly affecting the first ray, which forces the hindfoot into a compensatory varus alignment during the stance phase of gait.
When conservative measures such as custom orthoses and physical therapy fail to accommodate the deformity, surgical intervention becomes necessary to restore a stable, plantigrade, and braceable foot. The surgical algorithm dictates that soft tissue releases must be combined with precise bony realignments.
The Gould technique, which synergistically combines double plantar fasciotomies with dorsal closing wedge greenstick proximal metatarsal osteotomies, remains a cornerstone in the operative armamentarium for advanced, skeletally mature cavovarus deformities. This approach directly addresses the contracted plantar aponeurosis and the structural metatarsal equinus, effectively flattening the longitudinal arch and neutralizing the deforming forces.
Clinical Pearl: Always perform a Coleman block test during the preoperative clinical examination. If the hindfoot varus corrects when the first ray is allowed to drop off the block, the deformity is "forefoot-driven," and isolated forefoot correction (plantar fascia release and metatarsal osteotomies) may suffice. If the hindfoot remains in varus, concomitant calcaneal osteotomies or subtalar arthrodesis will be required.
Biomechanics and Pathoanatomy
In the classic neuromuscular cavovarus foot, a predictable pattern of muscle imbalance occurs. The peroneus longus (a strong plantarflexor of the first ray) overpowers the weakened tibialis anterior. Simultaneously, the strong posterior tibialis overpowers the weak peroneus brevis. This results in a plantarflexed first ray (metatarsus primus equinus) and forefoot adduction.
Over time, the plantar aponeurosis undergoes severe adaptive shortening, acting as a rigid bowstring that maintains the elevated medial longitudinal arch.
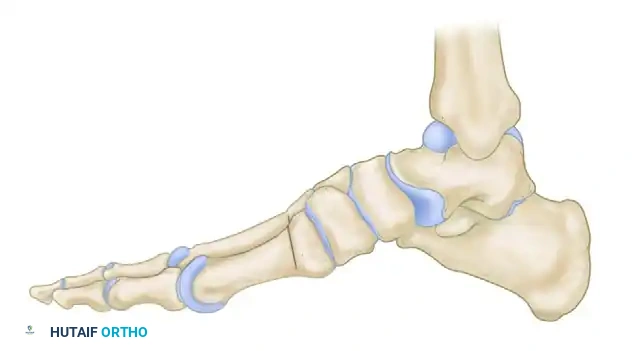
Preoperative lateral skeletal representation demonstrating severe forefoot equinus, elevated longitudinal arch, and cavus deformity typical of advanced Charcot-Marie-Tooth disease.
To correct this, the "bowstring" must be released via plantar fasciotomy, and the structural bony deformity must be corrected by elevating the metatarsal heads via dorsal closing wedge osteotomies.
Surgical Technique: Double Plantar Fasciotomies (Gould)
The plantar fascia is a dense, fibrous connective tissue structure that originates from the medial tuberosity of the calcaneus and fans out distally. In severe cavus deformities, a single medial release is often insufficient, necessitating Gould’s double fasciotomy approach to adequately release both the medial and lateral bands.
Medial Approach
- Positioning and Incision: The patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position. A tourniquet is applied to the proximal thigh. Make a 3 to 4 cm longitudinal incision along the medial border of the longitudinal arch, directly overlying the palpable band of the contracted plantar aponeurosis.
- Dissection: Deepen the incision through the subcutaneous fat. Carefully identify the medial plantar nerve and vessels, which lie in close proximity to the deep fascia of the abductor hallucis muscle.
- Nerve Protection: Gently mobilize and retract the medial plantar nerve superiorly (dorsally) using a blunt Ragnell or Senn retractor.
- Fascial Transection: Under direct visualization, isolate the medial and central bands of the plantar aponeurosis. Using heavy Mayo or curved dissecting scissors, transect the aponeurosis from medial to lateral.
Surgical Warning: The scissors should be opened only sufficiently to receive the fascial band. Wide, blind opening of the scissors in the deep plantar space risks catastrophic injury to the lateral plantar nerve and Baxter’s nerve (first branch of the lateral plantar nerve).
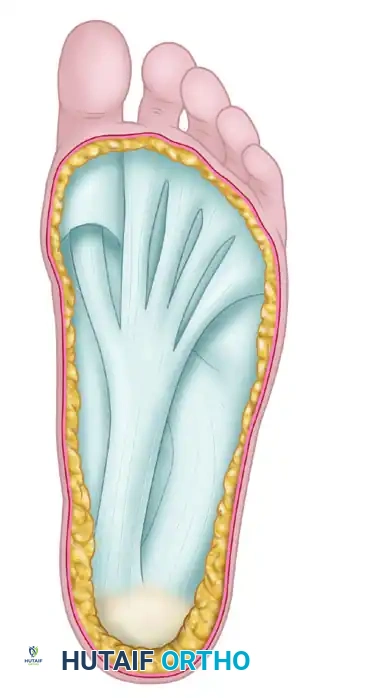
Anatomical representation of the plantar aponeurosis. The dense central and medial bands are the primary targets for release in the cavovarus foot.
Lateral Approach
- Incision: Through a separate lateral heel approach, make a 3 cm longitudinal incision in line with the lateral tubercle of the calcaneus.
- Identification: Dissect bluntly through the subcutaneous tissue to identify the lateral band of the plantar aponeurosis.
- Transection: With the points of curved scissors directed medially, carefully cut across the aponeurosis near its insertion on the calcaneal tuberosity. Staying proximal and lateral avoids damage to the main neurovascular bundle located more medially in the central compartment.
Surgical Technique: Closing Wedge Greenstick Dorsal Proximal Metatarsal Osteotomies
Following the soft tissue release, the structural bony equinus is addressed. The goal is to dorsiflex the metatarsals, thereby flattening the arch and restoring a plantigrade weight-bearing surface.
Incision and Exposure
Three distinct dorsal longitudinal incisions are utilized to access all five metatarsal bases while preserving adequate skin bridges to prevent necrosis:
* Incision 1: Centered over the dorsum of the first metatarsal base.
* Incision 2: Centered between the bases of the second and third metatarsals.
* Incision 3: Centered between the bases of the fourth and fifth metatarsals.
Carry the soft tissue dissection sharply down to the bone, extending approximately 1 cm distal to the tarsometatarsal (Lisfranc) joints.
Periosteal Elevation
Retract the extensor tendons medially or laterally as dictated by the exposure. Make a sharp, longitudinal incision into the periosteum of each metatarsal.
Carefully strip the periosteum medially and laterally using a Freer or Key elevator.
Critical Step: It is imperative to leave the periosteum attached at the plantar aspect of the metatarsals. This intact plantar periosteal hinge provides vital stability, acts as a tension band during closure, and significantly reduces the risk of nonunion or displacement.
Insert curved Hohmann retractors around the metatarsal shafts to protect the interosseous muscles and deep plantar arterial arch.
Executing the Osteotomies
The osteotomies are performed sequentially, typically starting from the lesser metatarsals and finishing with the first ray, which requires the most complex correction.
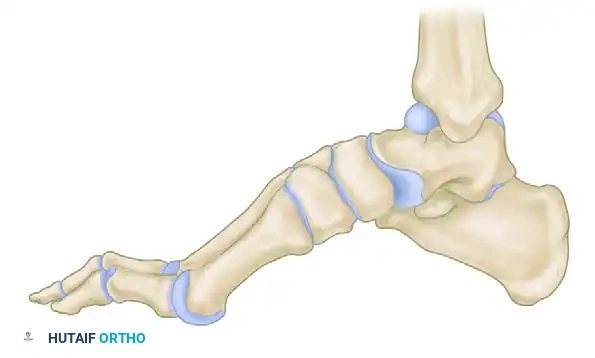
Lateral schematic demonstrating the planned dorsal closing wedge osteotomies at the proximal metaphysis of the metatarsals.
- The Proximal Cut: Using a thin-bladed oscillating power saw, make the proximal cut strictly vertical (perpendicular to the long axis of the foot). Penetrate only two-thirds to three-fourths of the way through the bone, deliberately stopping short of the plantar cortex.
- The Distal Cut: Make the distal cut approximately 4 mm distal to the first cut. Angle this cut proximally so that it converges with the apex of the first cut at the plantar cortex.
- Wedge Removal: Using a thin-bladed osteotome or a small rongeur, carefully extract the intervening dorsal wafer of bone.
Detail of the osteotomy execution. Note the preservation of the plantar cortex to create a greenstick hinge.
Specific Metatarsal Considerations
- The First Metatarsal (Biplane Correction): The first ray in a cavovarus foot is not only plantarflexed but often adducted (metatarsus primus varus). When making the distal cut on the first metatarsal, angle the saw blade obliquely (dorsal-lateral to plantar-medial) to create a biplane osteotomy. Closing this wedge will simultaneously dorsiflex and abduct the first ray, correcting both the equinus and the varus.
- The Fifth Metatarsal: The osteotomy of the fifth metatarsal must be made as proximal as possible, near the metaphyseal-diaphyseal junction. If made too distally, the angulation will create a prominent plantar bony ridge that can lead to intractable plantar keratosis and ulceration on the weight-bearing surface.
Osteotomy Closure
Once all wedges are removed, apply gentle, sustained upward pressure on the plantar aspect of the metatarsal heads. The intact plantar cortices will undergo a controlled "greenstick" fracture, allowing the dorsal gaps to close flush.

Closure of the dorsal gaps. The greenstick fracture of the plantar cortex allows for elevation of the metatarsal heads, flattening the longitudinal arch.
If the cuts were precise and the plantar hinge is intact, the osteotomies are often inherently stable and may not require internal fixation. However, if instability is noted, or if the plantar cortex completely fractures, stabilization with crossed Kirschner wires (K-wires) or low-profile dorsal plates is mandatory.
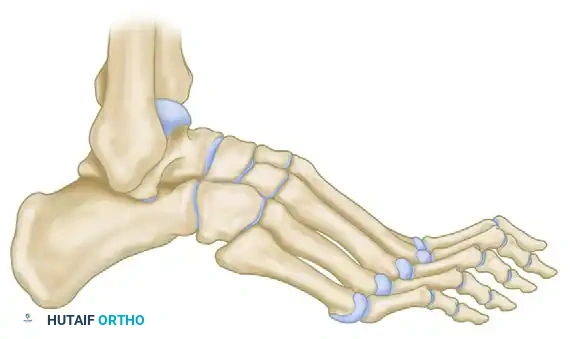
Postoperative lateral skeletal representation demonstrating a restored, plantigrade alignment following successful closing wedge osteotomies.
Adjunctive Soft Tissue Procedures
In the skeletally mature foot, bony correction alone is rarely sufficient if the underlying deforming muscle imbalances are not addressed. Failure to balance the foot will inevitably lead to recurrence of the cavovarus deformity.
The Jones Procedure
Gould routinely added the Jones procedure to increase and maintain the correction of the first ray. The extensor hallucis longus (EHL) is detached from the distal phalanx and transferred to the neck of the first metatarsal.
This transfer removes the deforming dorsiflexion force on the toe (which contributes to clawing) and converts the EHL into a dynamic dorsiflexor of the first metatarsal, counteracting the overpowering peroneus longus. The interphalangeal joint of the hallux is subsequently arthrodesed to prevent a drop-toe deformity.
The Hibbs Procedure
Equinus of the forefoot and severe clawing of the lesser toes often require the Hibbs procedure.
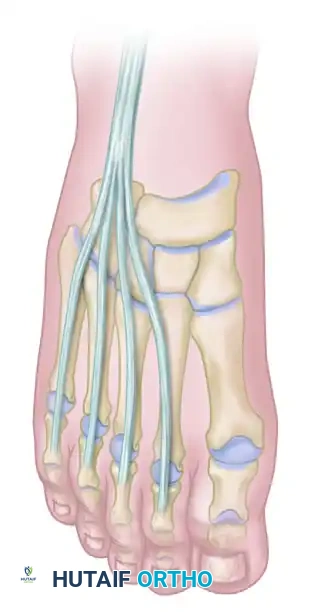
Anatomy of the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) tendons prior to transfer.
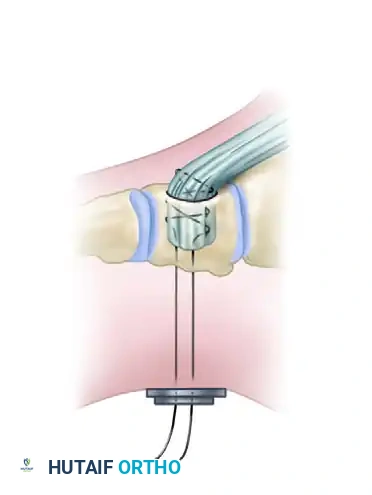
The Hibbs procedure involves the detachment of the extensor digitorum longus (EDL) tendons from the lesser toes. The proximal stumps of the EDL tendons are then tenodesed together and transferred into the middle cuneiform (or the base of the third metatarsal) via a bone tunnel or suture anchor.
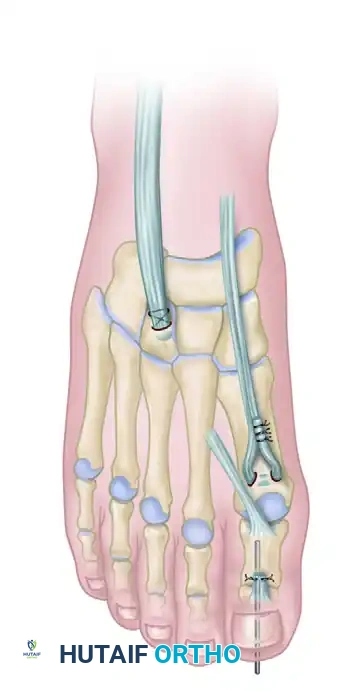
Completed Hibbs and Jones procedures. The EHL is transferred to the first metatarsal, and the EDL tendons are transferred to the middle cuneiform, providing dynamic dorsiflexion to the midfoot.
This transfer serves a dual purpose: it eliminates the hyperextension force at the metatarsophalangeal (MTP) joints (allowing the toes to drop into a corrected position) and recruits the EDL to assist in global ankle and midfoot dorsiflexion.
Postoperative Protocol and Rehabilitation
Meticulous postoperative care is essential to ensure bony union and soft tissue healing.
- Immediate Postoperative Phase (Weeks 0-2):
- The foot is placed in a well-padded, short-leg splint with the ankle in a strictly neutral (90-degree) position.
- The patient is strictly non-weight-bearing (NWB).
- Elevation is critical to manage edema, given the extensive dorsal incisions.
- Intermediate Phase (Weeks 2-6):
- Sutures are removed at 14 days.
- The patient is transitioned to a short-leg fiberglass cast.
- If the osteotomies were highly stable (intact greenstick hinges), touch-down weight-bearing may be permitted, but strict NWB is preferred if any fixation concerns exist.
- Late Phase (Weeks 6-12):
- Radiographs are obtained at 6 weeks to assess callus formation and bony union at the osteotomy sites.
- Once clinical and radiographic union is confirmed, the patient is transitioned to a controlled ankle motion (CAM) boot and begins progressive weight-bearing.
- Physical therapy is initiated, focusing on ankle range of motion, strengthening of the transferred tendons (biofeedback), and gait retraining.
- Long-Term:
- Patients are typically transitioned into supportive athletic wear with custom accommodative orthoses by 10 to 12 weeks.
- Due to the underlying neuromuscular etiology (e.g., CMT), lifelong monitoring is required to assess for deformity recurrence or contralateral progression.
Complications and Pitfalls
While highly effective, the Gould technique carries specific risks that the orthopedic surgeon must meticulously avoid:
- Nonunion/Delayed Union: Most commonly occurs if the plantar periosteal hinge is completely violated and the osteotomy is left unfixed. Meticulous saw technique is paramount.
- Transfer Metatarsalgia: Over-correction of the first ray (excessive dorsiflexion) can transfer weight-bearing forces to the lesser metatarsal heads, leading to painful plantar keratoses.
- Nerve Injury: The medial plantar nerve is at high risk during the medial fasciotomy, and the superficial peroneal nerve branches are at risk during the dorsal metatarsal exposures. Gentle, blunt retraction is required.
- Undercorrection: Failing to recognize a rigid hindfoot component (a negative Coleman block test) will result in residual varus. The Gould technique only addresses the forefoot; unrecognized hindfoot varus requires concurrent calcaneal osteotomy (e.g., Dwyer or lateralizing calcaneal osteotomy).
