Phalangeal & MTP Joint Dislocations: Surgical Management

Key Takeaway
Phalangeal and metatarsophalangeal (MTP) joint dislocations of the foot are complex injuries primarily driven by hyperextension mechanisms. While many interphalangeal dislocations are amenable to closed reduction, soft tissue interposition—particularly the plantar plate or sesamoids—frequently necessitates open surgical intervention. This guide details the biomechanics, classification, and step-by-step operative techniques required to achieve stable, congruent reductions and optimize functional outcomes in forefoot trauma.
INTRODUCTION TO FOREFOOT DISLOCATIONS
Phalangeal dislocations and metatarsophalangeal (MTP) joint dislocations represent a spectrum of forefoot trauma that, while relatively uncommon compared to fractures, demand precise anatomical understanding and prompt intervention. These injuries are predominantly driven by high-energy hyperextension vectors, leading to the disruption of the plantar plate, collateral ligaments, and joint capsule. Failure to recognize soft tissue incarceration—particularly involving the sesamoid complex or the plantar plate—can result in irreducible dislocations, chronic pain, and severe functional impairment.
This comprehensive guide delineates the pathoanatomy, radiographic evaluation, and step-by-step surgical management of interphalangeal and metatarsophalangeal dislocations, with a specific focus on the hallux and the complex first MTP joint.
INTERPHALANGEAL JOINT OF THE HALLUX
Pathoanatomy and Mechanism of Injury
Dislocation of the interphalangeal (IP) joint of the hallux is classically caused by a severe hyperextension force. This vector drives the distal phalanx into a position dorsal to the proximal phalanx. Because the plantar skin at the interphalangeal joint flexion crease is tightly tethered to the underlying fascia, tearing of this skin is a frequent complication, rendering the dislocation an open injury that requires urgent irrigation and debridement.
In the majority of cases, these dislocations can be reduced via closed methods. However, when a dislocation proves irreducible, the surgeon must suspect soft tissue interposition. The two primary obstacles to closed reduction are:
1. The Sesamoid Bone: An accessory interphalangeal sesamoid may become incarcerated within the joint space.
2. The Plantar Plate: The plantar plate may avulse from its proximal attachment and become interposed between the articular surfaces.
While the flexor hallucis longus (FHL) tendon can also be displaced into the joint, it is rarely the primary deterrent to reduction. Furthermore, these injuries are universally associated with the rupture of at least one collateral ligament, most commonly the tibial collateral ligament.
Classification of Hallux IP Dislocations
Miki, Yamamuro, and Kitai established a critical radiographic and clinical classification system identifying two distinct types of interphalangeal dislocations of the hallux based on the position of the plantar plate and the degree of deformity.
Type I: The "Deceiving" Dislocation
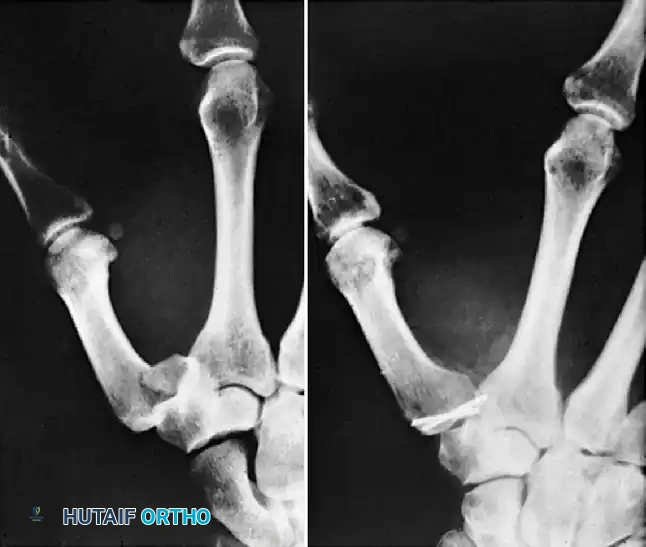
In a Type I injury, the plantar plate ruptures from one or both of its phalangeal attachments (typically the proximal attachment) and becomes trapped directly within the joint space. Clinically, the gross deformity is minimal, which can be highly deceiving to the evaluating physician. Radiographically, the interphalangeal joint space is markedly widened, but the distal phalanx is not locked in hyperextension.
Type II: The "Locked" Dislocation
The Type II dislocation is more common. The distal phalanx translates completely dorsal to the proximal phalanx, locking the joint in rigid hyperextension. The clinical deformity is obvious and striking. In these cases, the sesamoid bone, embedded within the plantar plate, acts as a mechanical block preventing closed reduction.

Closed Reduction Protocol
Initial management should always consist of an attempted closed reduction under a well-administered digital block.
Clinical Pearl: Do not attempt to simply "pull" the toe straight. Longitudinal traction must first be applied strictly in the axial plane of the deformity (hyperextension) to disengage the articular surfaces. Only when the base of the distal phalanx is level with the articular surface of the proximal phalanx should plantar flexion be applied.
If one or more collateral ligaments are torn and there is no interposition of the sesamoid or plantar plate, the joint will reduce easily with a palpable "clunk."
Post-Reduction Evaluation:
Post-reduction radiographs are mandatory. If the radiograph demonstrates residual widening of the joint space, the surgeon must assume the plantar plate remains incarcerated. This is an absolute indication for open reduction, even if the toe appears clinically straight.

Considerations for Lesser Toes
Historically, interphalangeal joint dislocations of the lesser toes have been highly amenable to closed reduction, followed by buddy taping to the adjacent toe for 3 weeks. However, literature by Brunet and Tubin highlights that a significant subset of these injuries may be more complex. In their series, nearly all dislocated lesser toe IP joints required open reduction due to plantar plate incarceration.
Furthermore, approximately 30% of dislocated lesser toe metatarsophalangeal joints required open reduction. While successfully reduced lesser toe IP joints were virtually asymptomatic at long-term follow-up, residual subluxations or dislocations at the MTP joints remained persistently painful.
For recurrent or highly unstable proximal interphalangeal (PIP) joint dislocations of the lesser toes, resection arthroplasty of the head and neck of the proximal phalanx may be required.

Surgical Technique: Open Reduction of Hallux IP Joint (Technique 86-17)
Open reduction is strictly indicated for irreducible dislocations or when post-reduction radiographs reveal joint space widening indicative of soft tissue interposition.
Step 1: Surgical Approach
* Perform the procedure under regional or general anesthesia with a forefoot tourniquet.
* Make a dorsal inverted L-shaped incision. The transverse limb should run parallel to the joint line, while the longitudinal limb extends dorsolaterally.
* Carefully dissect through the subcutaneous tissues, taking great care to preserve the extensor hallucis longus (EHL) insertion into the base of the distal phalanx. Iatrogenic injury to the EHL will result in a mallet toe deformity.
Step 2: Joint Exploration and Decompression
* Retract the EHL tendon to one side to expose the joint capsule.
* Identify the incarcerated plantar plate. Identification is often facilitated if the accessory sesamoid is embedded within it.
* Make a precise 3- to 4-mm longitudinal incision directly into the plantar plate to release the tension and allow it to be extracted from the joint space.
Step 3: Reduction
* Apply longitudinal traction to the great toe.
* If reduction is still impeded, utilize a blunt probe or a small Freer elevator to manually displace the sesamoid and plantar plate distally while maintaining traction. The joint should now reduce congruently.
Step 4: Stabilization
* Assess joint stability through a full range of motion. If the joint is stable, transarticular pinning is not strictly required.
* If the reduction is unstable (due to extensive collateral ligament disruption), hold the joint in a congruously reduced position.
* Drive one or two 0.062-inch Kirschner wires (K-wires) longitudinally from distal to proximal. The wires should cross the IP joint and rest securely in the subchondral bone at the base of the proximal phalanx.
* Cut the K-wires approximately 2 mm outside the skin and bend the ends to prevent migration.
Step 5: Closure and Immobilization
* Deflate the tourniquet and achieve meticulous hemostasis.
* Close the skin with nonabsorbable sutures.
* Apply a well-padded short leg cast that extends past the toes to protect the K-wires.
Postoperative Protocol for IP Dislocations
- Days 0-3: Strict rest and elevation of the extremity. Bathroom privileges only to minimize edema and prevent marginal wound necrosis.
- Weeks 1-3: Begin partial weight-bearing with crutches.
- Week 3: Remove the K-wires in the clinic. Transition the patient to weight-bearing as tolerated in a rigid, wooden-soled postoperative shoe. Initiate active and active-assisted range of motion (ROM) exercises for the IP joint.
- Week 6: Transition to a wide toe box shoe.
Surgical Warning: Marginal wound necrosis and prolonged digital swelling are common following this procedure. Reassure the patient that with strict elevation and time, these issues typically resolve. However, patients must be counseled preoperatively that some permanent limitation of interphalangeal joint motion is expected.
FIRST METATARSOPHALANGEAL (MTP) JOINT DISLOCATIONS
Pathoanatomy and Biomechanics
Dislocation of the first metatarsophalangeal joint is a rare but highly complex injury. The mechanism is extreme hyperextension of the great toe, which forces the proximal phalanx to displace onto the dorsum of the first metatarsal head and neck.
This displacement creates a formidable anatomical "noose" around the metatarsal head, making closed reduction exceptionally difficult. The metatarsal head becomes tightly trapped by the following structures:
* Medially: The medial head of the flexor hallucis brevis (FHB) and the abductor hallucis tendon.
* Laterally: The lateral head of the FHB and the adductor hallucis tendon.
* Dorsally: The displaced plantar plate and the deep transverse metatarsal ligament.
* Plantarward: The tight plantar aponeurosis prevents the metatarsal head from dropping back into position.
* Note: The flexor hallucis longus (FHL) tendon typically subluxates lateral to the metatarsal head.
The Jahss Classification
The integrity of the intersesamoid ligament dictates the reducibility of the first MTP joint. Jahss classified these dislocations based on this anatomical relationship:
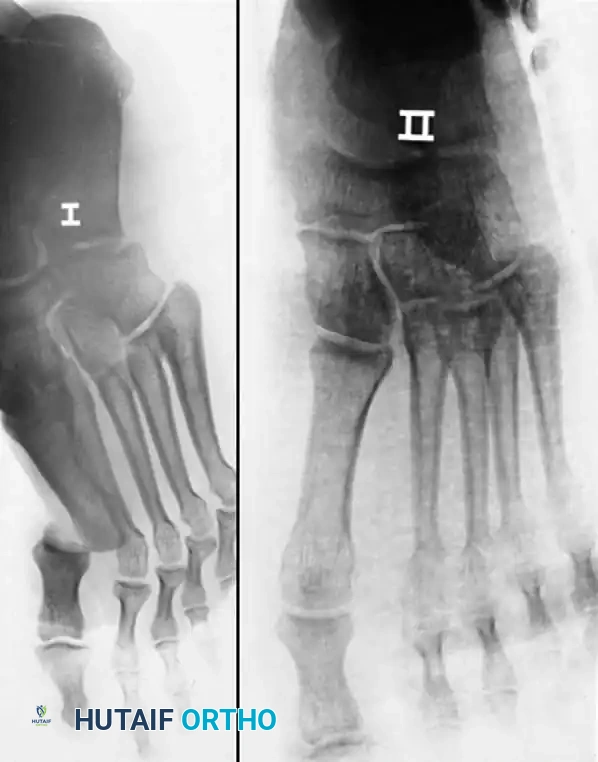
* Type I: The intersesamoid ligament is intact. The sesamoids are pulled dorsally over the metatarsal head. Closed reduction is usually impossible because the intact sesamoid complex acts as an unyielding block.
* Type IIA: The intersesamoid ligament is torn, resulting in wide separation of the tibial and fibular sesamoids. Closed reduction is frequently successful.
* Type IIB: The intersesamoid ligament is intact, but one of the sesamoids (usually the tibial) sustains a transverse fracture. The fracture allows the complex to widen, making closed reduction possible.
Surgical Approaches to the First MTP Joint
When closed reduction fails, open reduction is mandatory. The choice of surgical approach is critical to avoid iatrogenic complications:
1. Transverse Plantar Approach (Salamon, Gelberman, Huffer): Provides direct access to the plantar plate. However, it places the neurovascular bundles—specifically the medial plantar nerve to the great toe—at high risk. It also leaves a scar on the weight-bearing surface of the foot.
2. Midline Longitudinal Dorsal Approach (Yu and Garfin): Avoids plantar scarring and protects the plantar neurovascular bundles. It provides adequate exposure to lever the phalanx back into place.
3. Midline Medial Approach (Author's Preferred): Provides excellent visualization of the medial structures, allows for repair of the frequently torn tibial collateral ligament, and avoids both dorsal contractures and plantar weight-bearing scars.
Surgical Technique: Open Reduction via Midline Medial Approach (Technique 86-18)
Step 1: Incision and Exposure
* Make a 5-cm medial longitudinal incision centered directly over the first MTP joint.
* Utilize sharp dissection strictly through the skin to avoid injuring displaced or superficial cutaneous nerves.
* Elevate a full-thickness dorsal flap, utilizing the same tissue planes as one would during a standard hallux valgus (bunion) repair.
Step 2: Anatomical Assessment
* Systematically assess the magnitude of the injury. Inspect the medial collateral ligament (usually avulsed), the dorsal capsule, and the position of the plantar plate and enclosed sesamoids.
Step 3: Joint Reduction
* Insert a small Freer or periosteal elevator into the joint space.
* Simultaneously hyperextend the great toe and apply strong axial traction.
* Use the elevator as a skid to gently guide the base of the proximal phalanx over the dorsal lip of the metatarsal head and back into a congruous, reduced position.
Step 4: Capsuloligamentous Repair and Stabilization
* Once reduced, repair the torn collateral ligament (typically the tibial collateral) and the dorsal capsule using heavy absorbable sutures (e.g., 2-0 Vicryl).
* Assess the dynamic stability of the MTP joint. Perform gentle flexion and extension of the toe. Additionally, flex and extend the ankle to produce a tenodesis pull on the long flexor tendons to ensure the joint does not subluxate.
* If the reduction appears unstable, drill a smooth 0.062-inch K-wire across the MTP joint to maintain congruency.
Step 5: Closure
* Deflate the tourniquet and secure meticulous hemostasis to prevent postoperative hematoma.
* Close the skin with nonabsorbable, interrupted sutures.
Postoperative Protocol for First MTP Dislocations
- Immediate Post-op: Apply a bulky forefoot dressing designed to hold the toe congruously on the metatarsal head in approximately 10 to 15 degrees of extension. Over-wrap this with a short leg cast extending distal to the toes.
- Weeks 0-3: Allow partial weight-bearing with crutches.
- Week 3: Remove the cast and the transarticular K-wire (if utilized). Transition the patient to full weight-bearing in a stiff-soled, wide toe box shoe.
- Rehabilitation: Initiate active and active-assisted ROM exercises for the first MTP joint immediately upon pin removal. Utilize a silicone toe spacer in the first web space for an additional 3 weeks to maintain alignment and support the medial capsular repair.
Clinical Pearl: Patient expectation management is paramount. A permanent reduction in the terminal range of motion of the first MTP joint is virtually guaranteed following a complex dislocation. However, with aggressive rehabilitation, highly functional, pain-free motion is typically regained after several months. Return to high-impact activities (e.g., jogging) should be delayed until dynamic stability and strength are fully restored to prevent recurrent dislocation.
You Might Also Like