Periprosthetic Hip Fractures: Evaluate & Treat Complex Cases
Patient Presentation & History
A 78-year-old female presented to the emergency department following a low-energy fall at home. She reported twisting her body while standing, resulting in immediate, severe pain in her right hip and inability to bear weight. There was no direct impact to the hip.
Her relevant past medical history included:
* Bilateral total hip arthroplasty (THA) for severe osteoarthritis 12 years prior, right side cemented stem, left side uncemented.
* Osteoporosis, managed with oral alendronate for 8 years, discontinued 2 years ago due to gastrointestinal intolerance.
* Type 2 Diabetes Mellitus, well-controlled with oral hypoglycemics.
* Hypertension, managed with an ACE inhibitor.
* Coronary artery disease, status post PCI 5 years ago, currently on aspirin 81mg daily.
* Baseline mobility prior to injury was independent ambulation with a single point cane for longer distances.
Upon presentation, the patient was alert and oriented but in significant distress due to pain. She denied any head trauma, loss of consciousness, or other injuries. Review of systems was otherwise unremarkable except for localized pain.
Clinical Examination
General:
Patient was grimacing in pain, vital signs stable (BP 138/86, HR 88, RR 16, Temp 37.1°C, SpO2 98% on room air).
Inspection:
The right lower extremity appeared shortened and externally rotated compared to the left. A previously well-healed 15 cm lateral incision scar from the index THA was noted. No overt skin compromise, ecchymosis, or open wounds were observed.
Palpation:
Diffuse tenderness was elicited over the greater trochanter and the entire length of the right proximal and mid-femur. Crepitus was appreciated with gentle manipulation.
Range of Motion (ROM):
All active and passive ranges of motion of the right hip were severely limited and exquisitely painful. Any attempt at movement reproduced her pain.
Neurological Assessment:
*
Motor:
Intact strength (5/5) in ankle dorsiflexion, plantarflexion, toe extension, and hip flexion (distal to the suspected fracture site).
*
Sensory:
Intact sensation to light touch in the distribution of the sciatic, femoral, and obturator nerves. No paresthesias or numbness reported.
Vascular Assessment:
* Distal pulses (dorsalis pedis and posterior tibial) were palpable and symmetrical bilaterally. Capillary refill was brisk (<2 seconds) in the toes of the affected limb. No signs of compartment syndrome.
The clinical picture was highly suggestive of a displaced right periprosthetic femoral fracture.
Imaging & Diagnostics
Initial Radiographs:
Standard trauma series radiographs were obtained immediately. These included:
* Anteroposterior (AP) view of the pelvis.
* AP and lateral views of the entire right femur, extending from the hip joint to below the knee joint. This is critical to assess the full extent of the fracture and its relationship to the entire prosthetic stem.
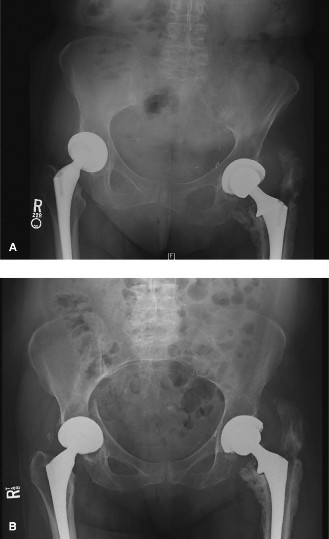
The radiographs revealed a comminuted, spiral fracture of the right femoral shaft involving the distal portion of the existing cemented femoral stem. There was significant displacement and shortening.
* The fracture extended from approximately 5 cm distal to the tip of the femoral stem, spiraling proximally to end at the level of the stem tip.
* The cement mantle around the distal stem appeared intact, and there was no evidence of gross lucency or subsidence suggestive of stem loosening on initial X-rays.
* There were cortical defects and comminution noted.
* No evidence of prior stress risers or cortical thickening was appreciated prior to the acute fracture.

Figure 1: Representative radiograph demonstrating a periprosthetic femoral fracture with significant comminution around a previously implanted femoral stem.
Computed Tomography (CT):
A CT scan of the right hip and femur was subsequently ordered to further delineate the fracture pattern, assess the extent of comminution, evaluate bone stock, and definitively determine the stability of the existing femoral stem. This was crucial for surgical planning given the complexity.
Key CT findings:
* Confirmed a highly comminuted spiral fracture of the femoral shaft, extending approximately 8 cm distal to the stem tip and spiraling up to the metaphyseal-diaphyseal junction adjacent to the stem tip.
* Evaluation of the stem-bone interface revealed no significant periprosthetic lucencies or cortical hypertrophy indicative of gross loosening. However, fine cuts through the cement mantle suggested a potential micro-motion or subtle debonding at the very tip of the stem, not definitively diagnostic of loosening but raising suspicion.
* Significant cortical bone loss and comminuted fragments were noted, particularly posterolaterally.
* The CT scan also assisted in assessing the rotational alignment and potential for achieving reduction.
Templating:
Pre-operative templating was meticulously performed using calibrated AP and lateral radiographs of the entire femur, as well as the CT scan.
* Using contralateral femur images for comparison (if available and not prosthetic), and standard templating guides for revision stems.
* Initial templating suggested that the existing stem, while potentially stable, was too short to bypass the comminuted fracture by at least two cortical diameters, making fixation around it challenging and prone to failure.
* Consideration was given to a long, extensively porous-coated, tapered fluted revision stem, aiming for distal fixation in healthy bone well past the fracture site. Various sizes and lengths were considered to provide adequate bypass and achieve stable diaphyseal fixation.
* Options for additional plate fixation and cerclage wires were also planned to augment stability and manage cortical defects.
Laboratory Diagnostics:
Pre-operative blood tests including complete blood count, basic metabolic panel, coagulation profile, and type and screen were performed. All were within normal limits, with no evidence of infection (ESR and CRP were not elevated). This helped rule out acute PJI as a primary cause or complicating factor.
Differential Diagnosis
When evaluating acute hip pain in a patient with a prior total hip arthroplasty, several critical diagnoses must be considered. A detailed comparison is essential for accurate diagnosis and appropriate treatment.
| Feature/Condition | Periprosthetic Hip Fracture (Our Case) | Atypical Femur Fracture (AFF) | Acute Periprosthetic Joint Infection (PJI) |
|---|---|---|---|
| Definition | Fracture of the femur occurring around a pre-existing hip arthroplasty. | Low-energy fracture of the subtrochanteric femur or femoral shaft, associated with long-term bisphosphonate use. | Infection involving the prosthesis and surrounding tissues, potentially acute or acute-on-chronic. |
| Patient History | Prior THA, often low-energy trauma, acute pain, inability to bear weight. May have contributing osteoporosis. | Elderly female, often long-term bisphosphonate use (>3-5 years). Prodromal dull thigh or groin pain (weeks/months) is common. Low-energy trauma or even spontaneous fracture. | Prior THA. Acute onset of pain, swelling, warmth, sometimes systemic symptoms (fever, chills). May have prior history of chronic low-grade pain, persistent drainage, or sinus tract. |
| Physical Exam | Deformity, shortening, external rotation (depending on fracture pattern), severe pain with attempted motion, localized tenderness. | Localized pain, limited weight-bearing, often less severe deformity than typical traumatic fracture. Tenderness at fracture site. | Joint effusion, warmth, redness, tenderness, restricted painful ROM. Sinus tract may be present. Systemic signs of sepsis (fever, tachycardia) if acute and severe. |
| Radiographic Findings | Fracture line clearly visible in relation to prosthesis. Vancouver classification for surgical planning (A, B1, B2, B3, C). Often comminution, varying fragment stability. | Unicortical lucency or "beaking" of the lateral cortex, followed by a transverse or short oblique fracture. Minimal or no comminution. Medial spike characteristic. Diffuse cortical thickening/hypertrophy distal to lesser trochanter. | No acute fracture line. Imaging may show implant loosening (progressive radiolucency at bone-cement or bone-implant interface, component subsidence), periosteal reaction, soft tissue swelling, or osteolysis. |
| Laboratory Findings | Usually normal, unless significant blood loss or pre-existing comorbidities (e.g., anemia). | Usually normal. Calcium, PTH, Vit D levels may be assessed in chronic bisphosphonate users. | Elevated ESR, CRP, leukocyte count. Gold standard: Positive joint aspirate for cell count (>3000-5000 WBCs/µL, >80% PMNs) and definitive microbial culture. |
| Treatment Implications | Operative: Fixation (plate/cables) for stable stem (B1, C), or revision arthroplasty (stem removal + new stem, +/- plate/graft) for loose stem or insufficient bypass (B2, B3). Non-operative rare. | Operative: Intramedullary nailing is the preferred treatment. Bisphosphonate cessation recommended. Surgical prophylactic nailing for contralateral stress reactions/symptoms. | Operative: Debridement and implant retention (DAIR) in acute cases, or one-stage/two-stage revision arthroplasty with prolonged antibiotic therapy. |
Surgical Decision Making & Classification
Given the patient's age, baseline functional status, and the significant displacement of the fracture, non-operative management was not a viable option. Non-operative treatment for periprosthetic fractures is typically reserved for very specific scenarios, such as non-ambulatory patients with stable Vancouver Type A fractures or those with prohibitive surgical risks, none of which applied here.
Classification:
The fracture was meticulously classified using the
Vancouver Classification System
:
*
Location:
The fracture involved the femoral shaft around the existing stem, placing it in
Type B
.
*
Stem Stability:
While initial X-rays suggested a stable stem, the CT raised subtle concerns, and importantly, the fracture pattern (comminuted, spiral, extending well distal to the stem tip) rendered the existing stem inadequate for providing stable bypass and fixation. Even if technically stable, the stem was functionally "loose" in the context of the fracture construct.
*
Bone Stock:
There was significant comminution and cortical defects, indicating compromised bone stock around the fracture site, though not global osteolysis.
Based on these findings, the fracture was classified as Vancouver B2 , primarily because the existing stem, even if "fixed," was functionally unable to provide stable fixation for the extensive fracture. The comminution also pushed it towards the B2/B3 border, but the primary driver was the need for stem revision due to insufficient bypass. The surgical plan would therefore involve stem revision, likely with a long diaphyseal engaging stem, combined with supplementary plate and cerclage wire fixation.
Decision for Operative Intervention:
1.
Displacement and Instability:
The fracture was significantly displaced and unstable, preventing any weight-bearing and causing severe pain.
2.
Functional Demands:
The patient was previously independently ambulatory and highly motivated to regain her mobility. Non-operative treatment would result in prolonged immobilization and likely malunion or nonunion, significantly compromising her functional recovery.
3.
Prosthesis Involvement:
The fracture involved the existing prosthesis, necessitating a strategy that addressed both the fracture and the implant-bone interface.
4.
Vancouver B2 Classification:
Mandates stem revision and fracture fixation due to functional stem instability relative to the fracture, or true stem loosening.
Pre-operative Planning Summary:
*
Type of surgery:
Revision THA (femoral side) with open reduction and internal fixation (ORIF) of the periprosthetic fracture.
*
Anticipated implant:
Long, extensively porous-coated, tapered fluted femoral revision stem (e.g., Corail, Wagner, ZMR). Plate fixation (e.g., LCP) and cerclage wires.
*
Approach:
Modified direct lateral (Hardinge) or posterior (Kocher-Langenbeck) depending on existing scar and anticipated exposure needs, potentially requiring an extended trochanteric osteotomy (ETO) for stem removal.
*
Blood management:
Type & cross-match, availability of blood products given potential for significant blood loss.
*
Team:
Senior orthopedic trauma surgeon, experienced assistant, intraoperative fluoroscopy.
Surgical Technique / Intervention
The surgical approach was chosen to provide maximal exposure for both stem removal and fracture fixation, while respecting previous surgical planes.
Patient Positioning:
The patient was placed in a lateral decubitus position on a fracture table. This allowed for unrestricted access to the entire length of the femur, facilitated traction and manipulation for reduction, and provided excellent intraoperative fluoroscopy access. Care was taken to pad all pressure points.
Surgical Approach:
The previous well-healed lateral approach scar was utilized. An extensile direct lateral approach (modified Hardinge) was performed. The fascia lata was incised, and the vastus lateralis was anteriorly reflected, exposing the lateral aspect of the greater trochanter and femoral shaft. Given the need for potential stem extraction and exposure of the extensive fracture, an
Extended Trochanteric Osteotomy (ETO)
was performed.
* The ETO involved making an osteotomy of the greater trochanter, including the attached abductor muscles, extending distally along the lateral femoral cortex for approximately 10-12 cm. This osteotomized fragment was then carefully reflected proximally, hinged on its posterior soft tissue attachments (vastus lateralis, remaining gluteus medius posterior fibers), exposing the proximal femur and the existing cemented stem. This provided an "open book" view of the proximal femur, significantly aiding stem removal and fracture reduction.
Stem Removal:
The existing cemented femoral stem was carefully extracted.
* Initially, the cement mantle was visualized. Osteotomes and a high-speed burr with a specialized long diamond tip were used to meticulously remove cement and break the bond between the cement and the bone, working circumferentially.
* Specialized trephines and ultrasonic cement removal devices can also be employed.
* Fenestrations (small cortical windows) were made distally to the cement mantle to allow for controlled cement removal and direct visualization of the distal stem tip.
* The stem was then carefully extracted using a dedicated stem extractor. Meticulous technique was paramount to preserve existing bone stock and avoid iatrogenic fracture extension.
* After stem removal, remaining cement fragments were thoroughly debrided from the femoral canal using curettes, burrs, and lavage.
Fracture Reduction:
With the ETO flap reflected and the canal clear, the comminuted periprosthetic fracture was visualized.
* Gentle traction and manipulation were applied to restore length, alignment, and rotation of the distal fracture fragment relative to the proximal femur.
* Provisional stability was achieved using large reduction clamps and multiple cerclage wires (e.g., stainless steel or polyethylene braided cable systems). These wires were carefully passed around the femur using specialized cable passers, taking care to protect soft tissues and ensure adequate tension for fragment reduction without devascularization. The ETO fragment was also provisionally reduced and secured with wires.
Femoral Revision Stem Insertion:
* The femoral canal was reamed sequentially to the appropriate size and prepared for the chosen revision stem. A long, extensively porous-coated, tapered fluted titanium revision stem (e.g., a Wagner Cone, ZMR) was selected based on pre-operative templating. These stems achieve diaphyseal fixation distally, bypassing the fracture by at least two cortical diameters, and resist subsidence and rotation.
* The chosen stem was inserted with appropriate press-fit and rotational stability, ensuring ideal anteversion and leg length. Intraoperative fluoroscopy confirmed satisfactory stem position and alignment.
Supplementary Fixation:
* Given the significant comminution and cortical defects, a long locking compression plate (LCP) was applied to the lateral aspect of the femur. The plate served as a neutralization plate, spanning the fracture zone and providing additional stability to the composite construct (stem + bone + plate).
* Screws were inserted proximally and distally into healthy bone, avoiding impingement with the revision stem. Bicortical fixation was achieved where possible.
* Additional cerclage wires were strategically placed along the fracture segments to compress comminuted fragments to the new stem and plate, enhancing circumferential stability and promoting healing. The ETO fragment was then definitively reattached to the proximal femur using bicortical screws through the plate and additional cerclage wires.
Irrigation and Closure:
The wound was thoroughly irrigated with copious amounts of saline. Hemostasis was achieved. A suction drain was placed deep to the vastus lateralis. The vastus lateralis was reattached, the fascia lata repaired, and the skin closed in layers.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-7):
*
Pain Management:
Multimodal analgesia including epidural or regional nerve blocks, oral opioids, NSAIDs (if not contraindicated), and acetaminophen.
*
DVT Prophylaxis:
Pharmacological (low molecular weight heparin or direct oral anticoagulants) initiated on post-operative day 1, combined with mechanical prophylaxis (intermittent pneumatic compression devices).
*
Antibiotics:
Prophylactic intravenous antibiotics continued for 24-48 hours.
*
Wound Care:
Daily dressing changes, drain removal typically on day 2-3 when output is minimal.
*
Weight-Bearing Status:
Strict
toe-touch weight-bearing (TTWB)
on the operated limb for the initial 6-8 weeks. This restriction is crucial due to the complexity of the fracture, the extent of stem revision, and the ETO. The goal is to protect the healing bone and allow for biological incorporation of the revision stem and union of the ETO.
*
Physical Therapy:
* Initiate early continuous passive motion (CPM) if tolerated (optional).
* Ankle pump exercises, quadriceps sets, gluteal sets.
* Gentle active-assisted range of motion (AAROM) of the hip and knee within pain limits, avoiding extremes of flexion, adduction, and internal rotation to prevent dislocation (if ETO was used and abductor mechanism disrupted temporarily).
* Transfers (bed to chair) with assistance, maintaining TTWB.
* Gait training with a wheeled walker, emphasizing TTWB.
Intermediate Phase (Weeks 6-12):
*
Radiographic Assessment:
Serial radiographs at 6 weeks and 12 weeks to assess fracture healing, ETO union, stem stability, and any signs of subsidence.
*
Weight-Bearing Progression:
If radiographic signs of early union are present and pain allows, progression from TTWB to
partial weight-bearing (PWB)
with 25-50% body weight, gradually increasing as tolerated. This is guided by radiographic evidence of healing and clinical stability.
*
Physical Therapy:
* Progressive strengthening exercises for hip abductors, extensors, and quadriceps.
* Balance and proprioception training.
* Gait training with walker, progressing to crutches, and eventually a single point cane as strength and confidence improve.
* Focus on functional activities of daily living (ADLs).
Late Phase (Months 3-6 and beyond):
*
Radiographic Assessment:
Further radiographs at 3 and 6 months post-operatively.
*
Weight-Bearing Progression:
If fracture union and stem stability are confirmed, progression to
full weight-bearing (FWB)
as tolerated.
*
Physical Therapy:
* Advanced strengthening, endurance, and balance training.
* Return to light recreational activities.
* Emphasis on restoring pre-injury functional level.
* Patient education regarding activity modification and fall prevention strategies.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
1.
Thorough Pre-operative Planning:
This is paramount. Obtain full-length AP and lateral radiographs of the entire femur, hip to knee, including the existing prosthesis. Crucially, a CT scan is often indispensable for complex fractures to delineate comminution, bone stock, and stem stability. Digital templating is a must to select the appropriate revision stem size, length, and predict screw placement.
2.
Vancouver Classification:
Master this system. It directly dictates the surgical strategy (fixation vs. revision) and choice of implant. Accurately differentiate B1 (stable stem, fixation only), B2 (loose stem/inadequate bypass, stem revision + fixation), and B3 (loose stem, poor bone stock, stem revision + bone graft/allograft).
3.
Stem Stability Assessment:
Do not solely rely on initial X-rays. Intraoperative assessment for rotational stability and piston-like motion, aided by fluoroscopy, is essential, especially for cemented stems where subtle lucencies might be obscured. If doubt exists for a B1, err on the side of stem revision (B2).
4.
Surgical Exposure:
Be prepared for extensile approaches (e.g., Extended Trochanteric Osteotomy - ETO) for difficult stem removal or complex fracture patterns. The ETO provides excellent visualization and protects the abductor mechanism.
5.
Stem Revision Principles:
If a revision stem is indicated, ensure it bypasses the most distal fracture line by at least two cortical diameters of intact bone. Extensively porous-coated or tapered fluted stems are preferred for diaphyseal engagement.
6.
Adjunctive Fixation:
Cerclage wires/cables are invaluable for reducing comminuted fragments, providing circumferential compression, and supporting the plate/stem construct. Locking plates provide stable bridging fixation and address cortical defects.
7.
Bone Grafting:
For Vancouver B3 fractures with significant bone loss or cortical defects, consider structural allografts or impaction grafting techniques to restore bone stock and promote healing.
8.
Post-operative Weight-Bearing:
This is perhaps the most critical post-operative instruction. Adhere strictly to a protected weight-bearing protocol (e.g., TTWB for 6-12 weeks) until radiographic evidence of early union and implant integration is evident. Patient compliance is key.
9.
Anatomical Reduction:
Restore length, alignment, and rotation to prevent mechanical failure and optimize functional outcomes.
Pitfalls:
1.
Inadequate Imaging:
Missing distal fracture extension on limited X-rays, leading to inadequate bypass length with the fixation construct and subsequent re-fracture.
2.
Underestimating Stem Loosening:
Treating a truly loose stem (B2) as stable (B1) with only ORIF will invariably lead to construct failure. A subtle stem lucency or piston effect intraoperatively necessitates stem revision.
3.
Insufficient Bypass:
Choosing a revision stem or plate that is too short, creating a stress riser at the distal end of the construct, predisposing to fracture distal to the implant.
4.
Aggressive Stem Removal:
Iatrogenic fracture propagation during cemented or ingrown uncemented stem extraction due to excessive force, inadequate cement removal, or uncontrolled osteotomy.
5.
Ignoring Cortical Defects:
Failure to address significant cortical defects with bone grafting or supplementary plating can compromise fixation strength and lead to non-union or re-fracture.
6.
Nerve Injury:
Sciatic nerve injury (posterior approach, excessive traction, large wires/screws) or femoral nerve injury (anterior approach, medial retraction) are significant risks in revision hip surgery.
7.
Vascular Injury:
Particularly during extensive dissection, cement removal, or revision for B3 fractures, leading to significant hemorrhage or limb-threatening ischemia.
8.
Infection:
Periprosthetic fractures have a higher risk of infection, especially in revision settings. Meticulous aseptic technique, thorough debridement, and appropriate antibiotic prophylaxis are crucial.
9.
Non-union/Malunion:
Can occur due to inadequate stability of the fixation construct, poor bone biology, or premature weight-bearing.
10.
Failure to Manage Comorbidities:
Poorly controlled diabetes, osteoporosis, or coagulopathy can significantly impact surgical outcomes and healing. Proactive perioperative management is essential.
Clinical & Radiographic Imaging