Perilunate Dislocation Trauma: Master Diagnosis & Management
Introduction & Epidemiology
Perilunate dislocations (PLDs) and perilunate fracture-dislocations (PLFDs) represent a spectrum of severe, high-energy wrist injuries characterized by disruption of the normal carpal alignment around the lunate, which maintains its articulation with the distal radius. These injuries are critical due to their potential for long-term morbidity, including chronic pain, instability, median nerve compression, and debilitating post-traumatic arthritis if not accurately diagnosed and appropriately managed.
The mechanism typically involves axial loading, hyperextension, and ulnar deviation of the wrist, often seen in falls from height, motor vehicle collisions, or sports injuries. Mayfield's classic four-stage theory describes the progressive sequential ligamentous failure that culminates in a perilunate or lunate dislocation. This progression usually begins with a scapholunate dissociation (Stage I), followed by dislocation of the capitate dorsally over the lunate (Stage II), then lunotriquetral dissociation (Stage III), and finally, complete lunate dislocation into the carpal tunnel (Stage IV). Associated carpal fractures, most commonly the scaphoid, triquetrum, or radial styloid, transform a pure dislocation into a fracture-dislocation.
Epidemiologically, PLDs are uncommon, accounting for approximately 10% of all carpal injuries, with an estimated incidence of 1.5 to 7.0 per 100,000 person-years. They predominantly affect young, active males, reflecting their association with high-energy trauma. Delayed diagnosis is a significant concern, with up to 25% of cases missed on initial presentation, often leading to chronic instability and poorer outcomes. Given the complex anatomy and devastating consequences of inadequate treatment, a systematic approach to diagnosis and immediate, definitive surgical management is paramount for optimizing functional recovery.
Surgical Anatomy & Biomechanics
A thorough understanding of wrist surgical anatomy and carpal biomechanics is fundamental to the successful diagnosis and management of perilunate injuries. The carpus is comprised of eight bones organized into proximal and distal rows, articulating with the distal radius and ulna proximally and the metacarpals distally. The lunate, often considered the "keystone" of the carpus, maintains a critical relationship with the radius proximally and the capitate distally, acting as a stable intercalated segment.
Key Carpal Bones and Articulations
- Proximal Row: Scaphoid, Lunate, Triquetrum, Pisiform (sesamoid).
- Distal Row: Trapezium, Trapezoid, Capitate, Hamate.
- Radiocarpal Joint: Articulation between the distal radius and the proximal carpal row (scaphoid, lunate, triquetrum).
- Midcarpal Joint: Articulation between the proximal and distal carpal rows.
Ligamentous Stabilizers
Wrist stability is primarily maintained by a complex array of intrinsic and extrinsic ligaments.
*
Intrinsic Ligaments:
These originate and insert within the carpus, providing primary stability between carpal bones.
*
Scapholunate Interosseous Ligament (SLIL):
The most critical intrinsic stabilizer of the proximal carpal row, preventing abnormal scaphoid flexion and lunate extension. Disruption leads to scapholunate dissociation. It has three distinct components: dorsal (strongest), palmar, and proximal membranous.
*
Lunotriquetral Interosseous Ligament (LTIL):
Stabilizes the lunate and triquetrum. Less commonly injured in isolation compared to SLIL, but often involved in the later stages of perilunate disruption.
*
Extrinsic Ligaments:
These connect the radius or ulna to the carpus.
*
Palmar Radiocarpal Ligaments:
Provide major volar stability.
*
Radioscaphocapitate (RSC):
Arises from the radial styloid, inserts into scaphoid waist and capitate neck. Critical in preventing scaphoid flexion and radial deviation.
*
Long Radioluante (LRL):
Arises from the radial metaphysis, inserts into the palmar aspect of the lunate.
*
Short Radiolunate (SRL):
Arises from the distal radius, inserts onto the volar lunate.
*
Dorsal Radiocarpal Ligament (DRC):
Arises from the distal radius, inserts into the triquetrum. Provides dorsal stability and is often the last ligament to fail in perilunate injury.
Carpal Kinematics and the Mayfield Classification
The carpal bones move in a coordinated manner, often described by the intercalated segment instability (ISI) model. The lunate, lacking direct muscular attachments, relies entirely on its surrounding ligamentous connections for stability. During a hyperextension injury, the force typically propagates from radial to ulnar, causing a sequential failure of ligaments around the lunate (Mayfield's great arc injury or Lesser arc injury pathway):
*
Stage I (Scapholunate Dissociation):
Rupture of the SLIL.
*
Stage II (Perilunate Dislocation):
Rupture of the dorsal radiocarpal ligaments and palmar radioscaphocapitate ligament, allowing the capitate to displace dorsally relative to the lunate. The lunate remains articulated with the radius. This is the classic perilunate dislocation.
*
Stage III (Perilunate Dislocation with Lunotriquetral Dissociation):
Rupture of the LTIL, leading to complete dissociation of the proximal carpal row.
*
Stage IV (Lunate Dislocation):
Complete disruption of all intrinsic and extrinsic ligaments, including the strong palmar radiolunate ligaments, allowing the lunate to dislocate volarly into the carpal tunnel, often rotating. The capitate then re-aligns with the radius.
Associated fractures (e.g., scaphoid waist, triquetrum, radial styloid, capitate head) are common and termed "great arc injuries," while pure ligamentous injuries are "lesser arc injuries." The integrity of these structures dictates treatment strategy and long-term prognosis.
Indications & Contraindications
The vast majority of acute perilunate dislocations and fracture-dislocations warrant operative intervention to achieve anatomical reduction, stabilize carpal relationships, and repair torn ligaments. Non-operative management is rarely indicated for these complex injuries due to the inherent instability and high risk of chronic dysfunction and arthritis.
Indications for Operative Management
- Acute Perilunate Dislocation (PLD) or Perilunate Fracture-Dislocation (PLFD): This is the primary indication. Timely surgical intervention (ideally within 1-2 weeks of injury) optimizes the chances of anatomical reduction and successful ligament repair.
- Irreducible Closed Dislocation: If closed reduction attempts are unsuccessful or unstable, open reduction is mandatory.
- Open Dislocation: Requires urgent surgical debridement, irrigation, reduction, and stabilization to prevent infection and facilitate healing.
- Associated Carpal Fractures: Fractures requiring fixation (e.g., scaphoid waist fracture, capitate fracture, triquetral avulsion) within the context of a PLD necessitate open management for stable osteosynthesis.
- Median Nerve Compression: While acute carpal tunnel syndrome due to median nerve compression can sometimes be relieved by closed reduction, persistent or severe symptoms warrant immediate surgical decompression and reduction.
- Persistent Instability after Closed Reduction: If, after a seemingly successful closed reduction, follow-up radiographs or clinical examination indicate persistent carpal instability, operative stabilization is required.
Contraindications for Operative Management
Absolute contraindications are exceedingly rare and typically relate to the patient's overall health status rather than the injury itself.
*
Severe Systemic Comorbidities:
Patients with life-threatening medical conditions that preclude safe anesthesia and surgery. In such cases, a focus on pain management and maintaining minimal function might be considered, though this decision carries significant long-term functional implications for the wrist.
*
Chronic/Untreated Dislocations (>6 weeks):
While not an absolute contraindication to
surgery
, the goals and techniques shift significantly. Acute ligament repair is typically not feasible, and salvage procedures (e.g., carpal fusions, proximal row carpectomy) are often the only viable options. Therefore, an "acute repair" may be contraindicated, but
some
form of surgery is almost always indicated for a chronic painful dislocation.
*
Patient Refusal:
If an adequately informed patient refuses surgical intervention, alternative non-operative strategies (splinting, pain management) would be pursued, though with a clear understanding of the anticipated poor functional outcome.
Operative vs. Non-Operative Indications Summary Table
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Injury Type | Acute Perilunate Dislocation or Fracture-Dislocation (PLD/PLFD), Open PLD/PLFD | Extremely rare for actual dislocations. May be considered for isolated, non-displaced carpal fractures without associated instability (e.g., some non-displaced triquetral avulsions) not part of a PLD. |
| Reducibility | Irreducible closed dislocation; unstable reduction post-closed manipulation | Only if completely stable and anatomically reduced (virtually never the case for PLD). |
| Associated Fractures | Scaphoid, capitate, triquetral, radial styloid fractures requiring fixation; displaced fragments obstructing reduction | None that significantly destabilize the carpus or require direct fixation. |
| Median Nerve | Acute carpal tunnel syndrome with neurological deficit requiring decompression | Mild, transient median nerve symptoms relieved completely by closed reduction and not recurring. |
| Timing | Acute injuries (<2 weeks post-injury) to facilitate ligament repair | N/A for true PLD. Chronic dislocations (>6 weeks) shift to salvage procedures rather than acute repair. |
| Patient Factors | Otherwise healthy, active patient with functional demands for the wrist | Severe systemic comorbidities precluding safe surgery; patient refusal after informed consent; very elderly, low-demand patient where a poor outcome is deemed acceptable over surgical risks. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for successful management of perilunate injuries, encompassing diagnostic imaging, surgical timing, patient counseling, and logistical preparation.
Diagnostic Imaging
-
Plain Radiographs:
Standard PA, lateral, and oblique views are the initial screening tools.
- PA View: Look for disruption of Gilula's lines (three smooth arcs connecting the proximal surfaces of the carpal bones), scapholunate dissociation (Terry-Thomas sign >3mm gap), loss of normal carpal alignment.
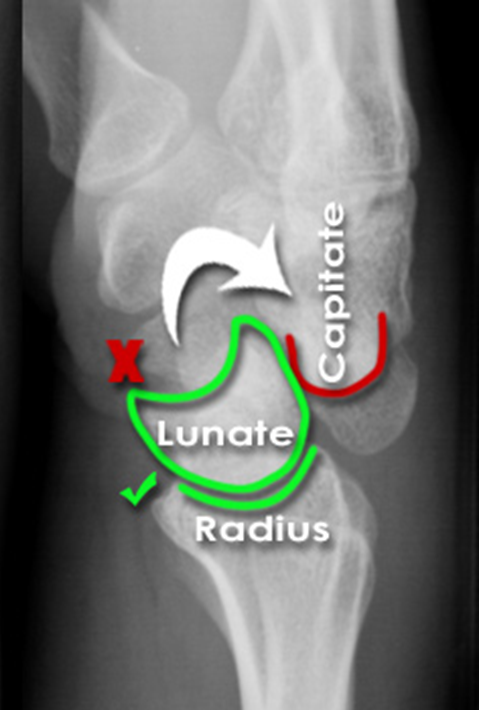
-
Lateral View:
The most critical view for diagnosing dislocations.
- Perilunate Dislocation: The lunate remains articulated with the radius, but the capitate is dislocated dorsally (or volarly) relative to the lunate. The "cup" of the lunate appears empty.
- Lunate Dislocation: The lunate itself dislocates volarly, often rotating into a spilled teacup appearance, while the capitate re-aligns with the radius.
- Oblique Views: Can aid in identifying subtle fractures.
-
Computed Tomography (CT) Scan:
Essential for comprehensive assessment.
- Provides detailed bony anatomy, identifies associated fractures (scaphoid, capitate, triquetrum, radial styloid) and their displacement, and confirms the precise nature of the dislocation.
- Crucial for pre-operative planning of fracture fixation.
- Can reveal chondral damage or loose bodies.
-
 CT scan demonstrating a dorsal perilunate dislocation with associated scaphoid fracture, illustrating the importance of detailed imaging for surgical planning.
CT scan demonstrating a dorsal perilunate dislocation with associated scaphoid fracture, illustrating the importance of detailed imaging for surgical planning.
- Magnetic Resonance Imaging (MRI): Less critical in the acute setting when plain films and CT confirm a dislocation, as surgical intervention is typically immediate. However, in cases of chronic instability or for clearer assessment of ligamentous integrity, MRI can be valuable.
Surgical Timing
Urgency is paramount. Acute perilunate injuries should be reduced and stabilized surgically as soon as the patient is medically optimized, ideally within hours to a few days. Delay beyond 2 weeks significantly complicates reduction, increases the difficulty of primary ligament repair, and is associated with poorer long-term outcomes due to edema, fibrosis, and ligamentous retraction.
Patient Counseling
Detailed discussion with the patient regarding the severity of the injury, the necessity of surgery, potential complications (e.g., stiffness, pain, arthritis, nonunion, median nerve issues), the intensive rehabilitation required, and the guarded long-term prognosis is essential to set realistic expectations.
Operating Room Setup & Patient Positioning
- Anesthesia: General anesthesia is standard. A regional block (e.g., axillary block) can be added for post-operative analgesia.
- Patient Positioning: Supine position on the operating table, with the affected arm abducted on a radiolucent hand table. A tourniquet is applied high on the arm for a bloodless field.
- Fluoroscopy: Essential for intra-operative assessment of reduction and K-wire placement. The C-arm should be draped and positioned to allow easy acquisition of PA and lateral views without contamination of the sterile field.
- Instrumentation: Small fragment set, mini-fragment set, various K-wires (0.035", 0.045", 0.062"), cannulated screws (e.g., Herbert screws for scaphoid), suture anchors, standard hand and wrist instruments. Arthroscopy equipment may be useful as an adjunct for diagnosis or debridement.
Detailed Surgical Approach / Technique
Surgical management of perilunate dislocations typically involves open reduction, internal fixation of any associated fractures, and primary repair or reconstruction of torn ligaments. A combined dorsal and palmar approach is often necessary for optimal visualization and management of all components of the injury.
Dual Approach: Dorsal and Palmar Incisions
A dual-incision approach is generally preferred to address the multi-planar displacement and extensive ligamentous disruption. The sequence typically involves initial assessment and reduction via the dorsal approach, followed by palmar access if required for lunate reduction, median nerve decompression, or palmar ligament repair.
1. Dorsal Approach
- Incision: A longitudinal incision centered over Lister's tubercle, extending proximally towards the mid-forearm and distally to the mid-carpus. This provides excellent exposure to the dorsal aspect of the radiocarpal and midcarpal joints.
-
Exposure:
- Identify and protect the superficial radial nerve and the dorsal cutaneous branch of the ulnar nerve.
- Incise the extensor retinaculum, typically between the third (extensor pollicis longus) and fourth (extensor digitorum communis, extensor indicis proprius) compartments, elevating it as a flap based radially or ulnarly. The third compartment is released and EPL reflected.
- Perform a "H" or "U" shaped dorsal capsulotomy, with the base of the flap left distally on the capitate. This maximizes exposure of the dorsal aspect of the scaphoid, lunate, triquetrum, and capitate.
-
Reduction:
- Initial reduction of the capitate onto the lunate is often performed first. This typically involves applying longitudinal traction to the wrist, with direct pressure on the dorsally displaced carpus (capitate) while counter-pressure is applied volarly to the lunate.
- Once the capitate is reduced onto the lunate, the lunate-radial articulation is addressed. The lunate may need to be "pushed" dorsally into its fossa if it's partially volarly subluxed.
- Fluoroscopic guidance is critical to confirm anatomical reduction in PA and lateral planes. The capitate should be centered over the lunate, and the lunate centered in the radial fossa.
-
Ligament Repair & K-wire Stabilization:
- SLIL Repair: The scapholunate interosseous ligament is almost invariably torn, usually off the lunate. Direct repair is attempted using absorbable sutures through bone tunnels or small suture anchors into the lunate, reattaching the ligament to its anatomical insertion. Augmentation with capsular repair is often performed.
- LTIL Repair: If the lunotriquetral interosseous ligament is found to be disrupted (less common in pure perilunate, more so in Stage III), it is repaired similarly.
-
K-wire Fixation:
- Once anatomical reduction of the scaphoid, lunate, and capitate is achieved, temporary K-wire fixation is applied to maintain the reduction.
-
Essential wires include:
- Scaphoid-Lunate (SL): One or two 0.045" K-wires across the scapholunate joint, perpendicular to the joint, from scaphoid to lunate, to stabilize the SLIL repair and prevent scaphoid flexion.
- Lunate-Capitate (LC): One or two 0.045" K-wires from the capitate into the lunate, traversing the midcarpal joint, to maintain the length and alignment of the midcarpal articulation.
- Scaphoid-Capitate (SC): An additional wire from scaphoid to capitate provides further rotational stability.
- Radiolunate (RL) or Radioscaphoid (RS): In highly unstable cases or for protection, a K-wire can be placed from the distal radius into the lunate or scaphoid to protect the radiocarpal joint. This is typically removed earlier.
- All K-wires are bent and cut beneath the skin to prevent migration and allow easy removal.
- Associated Fracture Fixation: Any associated fractures (e.g., scaphoid waist fracture, capitate neck fracture, triquetral body fracture) are internally fixed at this stage, often with headless compression screws (e.g., Herbert screw for scaphoid) or small fragment screws, under fluoroscopic guidance.
2. Palmar Approach (If indicated)
- Incision: A longitudinal incision is made along the thenar crease, extending proximally along the radial border of the flexor carpi ulnaris (FCU) or medially to the FCR tendon.
-
Exposure:
- Carefully protect the palmar cutaneous branch of the median nerve radially and the ulnar neurovascular bundle ulnarly.
- The transverse carpal ligament (TCL) is incised if median nerve compression is present or anticipated. This provides access to the floor of the carpal tunnel.
- The palmar radiocarpal ligaments (especially RSC, LRL, SRL) can be inspected and repaired if avulsed.
- Lunate Reduction (If Dislocated): If the lunate has dislocated volarly into the carpal tunnel (Stage IV), it is reduced back into the radial fossa by gentle manipulation, often by pushing it dorsally from within the carpal tunnel. Great care must be taken to avoid further median nerve injury.
- Ligament Repair: Palmar intrinsic and extrinsic ligaments (e.g., RSC) can be repaired if disrupted, often using suture anchors or direct repair techniques.
-
Median Nerve Decompression:
If the median nerve is compressed or visibly contused, a formal carpal tunnel release is performed.
-
 Intraoperative fluoroscopic image demonstrating multi-K-wire fixation following open reduction of a perilunate dislocation, ensuring stable carpal alignment.
Intraoperative fluoroscopic image demonstrating multi-K-wire fixation following open reduction of a perilunate dislocation, ensuring stable carpal alignment.
-
Arthroscopy (Adjunctive)
Wrist arthroscopy can be used in conjunction with open techniques for:
* Diagnostic assessment of ligamentous injuries and chondral surfaces.
* Assisted reduction of certain carpal components.
* Debridement of intra-articular debris.
* Confirmation of reduction and K-wire placement.
Closure
After ensuring stable reduction and fixation:
* Capsule repair (dorsal capsulotomy is closed securely to augment stability).
* Retinaculum is closed.
* Subcutaneous tissues and skin are closed in layers.
* A bulky compression dressing and a sugar-tong splint or long arm cast are applied with the wrist in slight extension and ulnar deviation.
Complications & Management
Despite optimal surgical treatment, perilunate dislocations are complex injuries with a significant risk of complications, both early and late. Understanding these complications and their management is crucial for long-term patient care.
Common Complications & Management Strategies
| Complication | Incidence (Approximate) | Management / Salvage Strategy |
|---|---|---|
| Median Nerve Neuropathy | 10-30% | Acute: Decompression (carpal tunnel release) often during primary surgery. Chronic: Surgical release if symptoms persist or re-emerge; nerve gliding exercises. |
| Post-Traumatic Arthritis (SNAC/SLAC Wrist) | High (50-100% long-term) | Early: Symptomatic management (NSAIDs, injections, activity modification). Late/Severe: Proximal Row Carpectomy (PRC), Four-Corner Fusion (4CF), Scaphotrapeziotrapezoid (STT) fusion, total wrist arthroplasty (less common), total wrist fusion. |
| Persistent Instability / Redislocation | 5-15% | Early: Revision open reduction and K-wire fixation, augmented ligament repair/reconstruction. Late: Ligament reconstruction (e.g., using tendon graft), dorsal capsulodesis, limited carpal fusion (e.g., STT, 4CF), salvage procedures (PRC, total wrist fusion). |
| Nonunion / Malunion of Fractures | 5-10% (esp. scaphoid) | Scaphoid: Revision open reduction and internal fixation (ORIF) with bone grafting (e.g., vascularized bone graft) and stable screw fixation. Other Carpal Fractures: Revision ORIF, nonunion excision, or carpal fusion if symptomatic. |
| Stiffness / Loss of ROM | Very Common (>50%) | Early and aggressive hand therapy is critical. Dynamic splinting, manipulation under anesthesia (MUA), tenolysis, capsulotomy, arthroscopic debridement if limited by osteophytes. |
| Infection | 1-5% | Surgical debridement, irrigation, intravenous antibiotics (culture-guided), K-wire removal (if applicable), wound care. |
| Complex Regional Pain Syndrome (CRPS) | 2-10% | Early diagnosis and multi-disciplinary management: Physical therapy, pain management (nerve blocks, medication), psychological support. |
| K-wire Complications | 5-10% | Wire migration (rare if bent/buried), skin irritation, superficial infection at pin sites. Managed by K-wire removal, local wound care, oral antibiotics. Fractures at wire sites are rare but can occur. |
| Avascular Necrosis (AVN) of Carpal Bones | Rare (esp. lunate) | Less common in acute PLD than isolated scaphoid fractures or chronic lunate dislocations. If present: observation, symptomatic management, or later salvage procedures (e.g., vascularized bone graft for scaphoid, PRC/fusion for lunate AVN). |
Discussion on Key Complications
- Post-Traumatic Arthritis: This is arguably the most common and devastating long-term complication. Even with successful anatomical reduction and fixation, the initial trauma to the articular cartilage and the disruption of normal carpal kinematics can lead to progressive degeneration. The development of Scapholunate Advanced Collapse (SNAC) or Scaphoid Nonunion Advanced Collapse (SLAC) wrist patterns is common, requiring challenging salvage procedures.
- Stiffness: The extensive ligamentous injury, prolonged immobilization, and post-operative fibrosis contribute significantly to wrist stiffness. Early and consistent hand therapy is crucial to mitigate this.
- Median Nerve Neuropathy: Direct compression by the volarly displaced lunate in lunate dislocations, or by edema and hematoma in perilunate dislocations, necessitates prompt decompression. Persistent symptoms require surgical release.
- Persistent Instability: Can arise from inadequate initial reduction, failed ligament repair, or progressive loosening of fixation. This often mandates revision surgery.
Close post-operative monitoring and a strong collaboration with experienced hand therapists are vital for early identification and management of these potential pitfalls.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is paramount for achieving optimal functional outcomes following surgical repair of perilunate dislocations. The protocol emphasizes protection in the early phase, followed by gradual restoration of motion, strength, and function, while protecting healing ligaments and bone.
Phase 1: Immobilization and Protection (Weeks 0-6/8)
- Goal: Protect surgical repair, minimize pain and swelling, promote initial soft tissue healing.
-
Immobilization:
- Immediately post-op: Bulky compressive dressing with a sugar-tong splint or a long arm cast, wrist positioned in slight extension (10-20 degrees) and ulnar deviation. This position reduces stress on the repaired SLIL.
- Duration: Typically 6 to 8 weeks, depending on the extent of injury, stability, and surgeon's preference. K-wires are maintained during this period.
-
Activities:
- Elevation of the hand above heart level to reduce swelling.
- Active range of motion (AROM) of fingers, thumb, elbow, and shoulder to prevent stiffness in uninvolved joints.
- Gentle forearm pronation/supination (if not restricted by cast/splint and K-wires do not cross the distal radioulnar joint).
- Patient education on avoiding weight-bearing, lifting, or forceful gripping with the affected hand.
- Pain & Edema Management: Analgesics, cryotherapy, light massage for unaffected areas.
Phase 2: Early Motion & K-wire Removal (Weeks 6/8 - 12)
- Goal: Safely initiate controlled wrist motion, restore basic strength, protect the maturing ligamentous repairs.
- K-wire Removal: Typically performed around 6-8 weeks post-operatively, after radiographic confirmation of stable carpal alignment and signs of early ligamentous healing. This can be done in the clinic setting under local anesthesia.
-
Initiating Motion (Post K-wire Removal):
- Hand therapy commences with gentle, active, pain-free range of motion exercises for the wrist (flexion, extension, radial and ulnar deviation, pronation, supination).
- Passive range of motion (PROM) is introduced cautiously by the therapist, respecting pain limits.
- Scar management begins (massage, silicone sheeting) to prevent adhesions.
-
Strengthening:
- Gentle isometric exercises for wrist flexors, extensors, and deviators.
- Light grip strengthening (e.g., soft putty, sponge squeeze).
- Proprioceptive exercises (e.g., gentle weight shifting on a stable surface).
- Activities: Continue to avoid heavy lifting, pushing, pulling, or sudden impacts.
Phase 3: Progressive Strengthening & Functional Return (Weeks 12+)
- Goal: Maximize wrist strength, endurance, and functional capabilities, prepare for return to work/sport.
-
Strengthening:
- Gradual progression to resistive exercises using TheraBands, light weights, and resistance equipment.
- Emphasis on wrist and forearm strengthening, including eccentric loading.
- Advanced grip and pinch strengthening.
- Proprioceptive training with unstable surfaces.
-
Endurance & Function:
- Sport-specific or work-specific task simulation.
- Gradual return to activities of daily living and work tasks.
- Return to sport typically not before 6 months, and often longer, depending on the sport and patient's recovery.
- Long-Term Monitoring: Patients should be counseled on the potential for long-term complications, particularly post-traumatic arthritis, and the need for ongoing surveillance. Periodic radiographic follow-up is advisable.
Key Considerations for Rehabilitation
- Individualized Approach: Protocols must be tailored to the specific injury (pure dislocation vs. fracture-dislocation), surgical findings, patient's age, comorbidities, and functional demands.
- Pain as a Guide: Activities should remain within pain tolerance. Pushing through pain can exacerbate inflammation and hinder healing.
- Hand Therapist Collaboration: Close communication and collaboration between the surgeon and an experienced certified hand therapist are crucial for guiding the patient through the complex rehabilitation process.
- Patient Compliance: Adherence to the protocol is vital for success. Patients need to understand the importance of diligent exercise and activity modification.
Summary of Key Literature / Guidelines
The understanding and management of perilunate dislocations have evolved significantly over decades, guided by anatomical studies, biomechanical research, and clinical outcomes data.
Landmark Contributions
- Mayfield's Classification (1980): A seminal work by Mayfield et al. described the sequential pattern of ligamentous disruption in experimentally induced perilunate dislocations, providing the foundation for understanding the pathomechanics and classification of these injuries. This remains the cornerstone for diagnosis and treatment planning.
- Taleisnik (1987): Further elaborated on carpal anatomy and instability patterns, emphasizing the role of the proximal carpal row as an intercalated segment and the importance of its intrinsic ligaments.
- Green's Operative Hand Surgery: A foundational text that consistently provides comprehensive, evidence-based guidance on the surgical management of carpal instabilities, including perilunate injuries.
Current Consensus & Guidelines
- Urgent Open Reduction and Internal Fixation (ORIF): The current standard of care dictates urgent open reduction, K-wire stabilization, and primary repair of disrupted ligaments (especially the SLIL) for acute perilunate dislocations and fracture-dislocations. Delays beyond 2 weeks are associated with significantly poorer outcomes.
- Role of CT Imaging: High-resolution CT scanning is universally recommended for pre-operative planning, providing precise details of carpal alignment and associated fractures, which are often missed or underestimated on plain radiographs.
- Combined Dorsal and Palmar Approaches: While a dorsal approach is often sufficient for reduction and ligament repair in pure perilunate dislocations, a combined dorsal and palmar approach is frequently necessary, particularly in cases of lunate dislocation, irreducible injuries, or if palmar ligament repair or median nerve decompression is required.
- Stable Fixation: Multi-K-wire fixation (scaphoid-lunate, lunate-capitate, scaphoid-capitate) is crucial to maintain carpal alignment and protect ligament repairs during the healing phase. Associated fractures require stable internal fixation (e.g., headless compression screws for scaphoid fractures).
- Aggressive Rehabilitation: A structured, progressive rehabilitation program, emphasizing early controlled motion post-immobilization, is essential to mitigate stiffness and restore function.
- Long-Term Outcomes & Arthritis: Numerous studies highlight a high incidence of post-traumatic arthritis (often SNAC or SLAC wrist) even after optimal acute management, with rates ranging from 50% to 100% in long-term follow-up. This underscores the severity of the initial injury and the importance of counseling patients on realistic expectations, including the potential for future salvage procedures (e.g., proximal row carpectomy, four-corner fusion).
- Salvage Procedures for Chronic Instability/Arthritis: For neglected chronic dislocations or failed primary repairs leading to symptomatic instability or advanced arthritis, options include ligament reconstruction, limited carpal fusions (e.g., four-corner fusion, scaphocapitate fusion), proximal row carpectomy, or total wrist fusion in severe, debilitating cases.
The literature consistently emphasizes that early, accurate diagnosis and meticulous surgical technique, followed by a dedicated rehabilitation program, are the cornerstones of successful management of perilunate dislocations, aiming to restore functional stability and minimize long-term morbidity. However, the high incidence of post-traumatic arthritis remains a significant challenge, highlighting the need for ongoing research into improved repair techniques and regenerative strategies.
