Patient Presentation & History
A 38-year-old male presented to the Level I Trauma Center following a high-energy motor vehicle versus pedestrian incident. He was struck directly from the side while crossing an intersection. Bystanders reported he was thrown approximately 15 meters. He arrived hemodynamically unstable, with a GCS of 10 (E2V3M5) due to presumed head injury and hypovolemic shock. Initial ATLS primary survey revealed a patent airway, labored breathing (respiratory rate 28/min), diminished breath sounds on the right with dullness to percussion suggestive of hemothorax, and bilateral open tibia/fibula fractures (Gustilo-Anderson IIIA left, IIIB right). Blood pressure was 70/40 mmHg, heart rate 130 bpm. Pelvic assessment on the primary survey demonstrated gross instability upon gentle palpation of the iliac crests, with significant external rotation of both lower extremities. Rectal examination revealed a normal sphincter tone but gross blood on the examining finger. No obvious perineal hematoma was noted initially, but significant crepitus was palpable over the symphysis pubis and right sacroiliac joint. Past medical history was significant for hypertension controlled with medication and a 15-pack-year smoking history.
Clinical Examination
Following initial resuscitation, intubation, and chest tube insertion for the hemothorax, a more detailed secondary survey was performed.
Inspection
- Pelvis: Gross asymmetry of the pelvis with apparent widening of the inter-iliac distance. Both lower extremities were externally rotated, with the right more pronounced than the left. No obvious open pelvic wounds, but extensive ecchymosis was developing over the perineum, scrotum, and right flank extending towards the iliac crest. A significant Morel-Lavallée lesion was suspected over the right greater trochanteric region due to a palpable fluctuant mass.
- Lower Extremities: Open Gustilo-Anderson IIIA fracture of the left distal tibia and fibula with significant soft tissue stripping. Open Gustilo-Anderson IIIB fracture of the right mid-shaft tibia and fibula with bone loss and extensive contamination. Obvious deformity of both lower limbs secondary to these injuries.
- Abdomen: Distended, diffusely tender but non-peritonitic. Palpable tenderness over the pubic symphysis.
Palpation
- Pelvic Stability: Gentle anterior-posterior compression and lateral compression maneuvers confirmed significant mechanical instability. Application of a pelvic binder temporarily improved gross stability. Tenderness was elicited over the pubic symphysis, bilateral iliac wings, and profoundly over the right sacroiliac joint and sacrum.
- Perineum/Rectum: Gross blood on rectal exam persisted. High-riding prostate was not definitively appreciated due to swelling, but urethral integrity was questioned. Vaginal examination was not performed given the patient's gender.
- Peripheral Pulses: Weak but palpable dorsalis pedis and posterior tibial pulses bilaterally. Capillary refill >3 seconds in both feet.
- Neurological: Despite intubation, gross motor function was assessed by noxious stimuli, revealing some withdrawal from painful stimuli in the left lower extremity but minimal response in the right. Formal sensory examination was limited. Anal sphincter tone was noted to be intact on repeat rectal exam after initial shock resolution.
Range of Motion
- Hip range of motion was severely limited by pain and mechanical instability. Efforts were not aggressive to avoid further displacement.
- Knee and ankle range of motion were assessed distal to the open tibial fractures, limited by the obvious fractures.
Neurological/Vascular Assessment
- Neurological: Due to the patient's altered mental status and intubation, a full neurological exam was deferred initially. However, sacral nerve root function was monitored via repeat rectal exams. Sciatic nerve function (peroneal and tibial divisions) was assessed by withdrawal to noxious stimuli. No obvious foot drop or significant motor deficits other than the general lack of cooperation.
- Vascular: A focused arterial doppler examination confirmed flow to both lower extremities. Given the severe pelvic trauma and open tibial fractures, a vascular surgery consultation was obtained, and serial vascular exams were planned. No significant limb length discrepancy was noted in the field, but this would be assessed once the pelvis was stabilized.
Imaging & Diagnostics
Initial Trauma Radiographs
- AP Pelvis: Demonstrated significant diastasis of the pubic symphysis (>2.5 cm), widening of the right sacroiliac joint, and a comminuted right sacral fracture extending into the neural foramen (Denis Zone II). There was also a subtle avulsion fracture of the right L5 transverse process. This confirmed an unstable pelvic ring injury consistent with a Young-Burgess Anterior-Posterior Compression Type III (APC III) or potentially a vertical shear component due to the sacral fracture pattern and L5 transverse process avulsion.
- Inlet View: Showed posterior displacement and internal rotation of the right hemipelvis, indicating significant posterior instability.
-
Outlet View:
Confirmed superior migration of the right hemipelvis, emphasizing the vertical shear component and the severity of the sacral disruption.
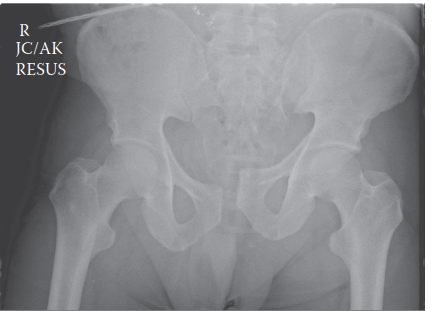
Figure 1: Representative AP pelvis radiograph demonstrating significant pubic symphysis diastasis, right SI joint widening, and comminution of the right sacral ala, indicative of an unstable pelvic ring injury.
CT Scan
- Pelvis CT with 3D Reconstructions: Performed once hemodynamically stabilized. This confirmed the APC III injury pattern with a >3 cm diastasis of the pubic symphysis, complete disruption of the anterior sacroiliac ligaments on the right, and partial disruption of the posterior sacroiliac ligaments. The right sacral fracture was definitively characterized as a Denis Zone II, comminuted, with significant displacement and involvement of the S1 and S2 neural foramina. Subtle avulsion of the right iliolumbar ligament attachment from L5 was also noted. 3D reconstructions were crucial for understanding the rotational and vertical displacement of the right hemipelvis.
- CT Angiogram (CTA): Performed due to persistent hypotension, gross pelvic instability, and suspected vascular injury. It revealed active extravasation from branches of the internal iliac artery on the right side, consistent with ongoing hemorrhage. No major named vessel injury was identified requiring immediate surgical repair, but smaller arterial branches were bleeding.
- CT Cystogram: Indicated due to gross hematuria and suspected urethral injury. It confirmed an extraperitoneal bladder rupture with extravasation of contrast into the retropubic space. No urethral injury was identified after a retrograde urethrogram (RUG) was performed prior to Foley catheter insertion, which confirmed an intact urethra.
Other Diagnostics
- FAST Exam: Positive in the perihepatic and perisplenic views, confirming free fluid in the abdomen.
- Laboratory Studies: Initial hemoglobin was 7.2 g/dL, requiring massive transfusion protocol activation. Coagulation profile was deranged (INR 1.8, PTT 45s), attributed to trauma-induced coagulopathy and initial resuscitation efforts.
Templating
Pre-operative templating based on CT 3D reconstructions was essential for planning surgical fixation. This involved:
*
Symphysis Pubis:
Determining plate length and screw trajectories for an open reduction internal fixation (ORIF) of the pubic symphysis, considering a 6- or 8-hole symphyseal plate.
*
Posterior Ring:
Planning percutaneous iliosacral screw trajectories (typically S1 and S2) to avoid neurovascular structures (sciatic nerve, internal iliac vessels) and confirm adequate bone stock. Alternative considerations included open posterior approach for sacroiliac plating or tension band wiring for the sacral fracture, depending on stability and comminution.
*
External Fixation:
Planning pin insertion sites for a supra-acetabular external fixator, if used as a temporary or definitive measure.
Differential Diagnosis
The patient's presentation with high-energy trauma and gross pelvic instability mandates a structured differential diagnosis approach, primarily focusing on the various types of pelvic ring injuries.
| Feature | Young-Burgess Anterior-Posterior Compression Type III (APC III) (Our Case) | Young-Burgess Lateral Compression Type III (LC III) | Vertical Shear (VS) |
|---|---|---|---|
| Mechanism | Direct anterior-posterior force (e.g., head-on collision, direct blow to symphysis). | Lateral force (e.g., T-bone collision, fall from height landing on side). | Vertical force (e.g., fall from height landing on feet/buttocks, pedestrian vs. vehicle). |
| Key Clinical Findings | - Marked pubic symphysis diastasis (>2.5 cm) | - Internal rotation of hemipelvis | - Significant vertical displacement of hemipelvis |
| - Scrotal/perineal bruising, bladder/urethral injury common | - Lower extremity internally rotated and shortened | - Lower extremity shortened | |
| - Open book deformity, palpable instability | - Tenderness over lateral compression sites (e.g., greater trochanter) | - Significant hemorrhage due to ligamentous disruption | |
| - Hemodynamic instability common | - Less common for immediate hemodynamic instability | - High incidence of neurovascular injury | |
| Key Imaging Findings | - Pubic symphysis diastasis | - Sacral impaction fracture (Denis Zone I/II) or fracture through iliac wing | - Complete disruption of anterior and posterior SI ligaments |
| - Sacroiliac joint widening (anterior), potential posterior ligament disruption | - Crescent fracture of ilium, possibly associated with APC-type injury on contralateral side (LC III) | - Sacral fracture (often oblique or transverse) with significant displacement | |
| - Disruption of sacrotuberous and sacrospinous ligaments | - Ligamentous disruption depends on severity (e.g., LC I-III) | - Lumbar transverse process fractures, L5-S1 facet disruption | |
| Initial Management Principles | - Immediate pelvic binder to reduce volume and tamponade hemorrhage | - Pelvic binder (may not be as effective for internal rotation) | - Immediate pelvic binder |
| - Aggressive resuscitation (fluids, blood products) | - Careful assessment for associated visceral injuries | - Aggressive resuscitation and hemorrhage control (angiography/embolization) | |
| - Angiography/embolization for ongoing hemorrhage | - Surgical fixation indicated for unstable variants (LC II/III) | - Urgent operative stabilization due to high instability | |
| - Urological consultation for suspected GU injury | - Usually less urgent for operative intervention if LC I, but requires close monitoring | - Neurological assessment paramount | |
| - Operative fixation (anterior and posterior ring) once stable | - Surgical fixation (anterior and posterior ring) |
Surgical Decision Making & Classification
The decision for operative versus non-operative management in pelvic ring injuries hinges on several critical factors, primarily hemodynamic stability, mechanical stability, and the presence of associated injuries.
In this case, the patient presented with:
1.
Hemodynamic Instability:
Persistent hypotension despite aggressive fluid resuscitation, requiring massive transfusion protocol and ultimately angiography for embolization. This mandates immediate hemorrhage control.
2.
Mechanical Instability:
Gross instability on clinical exam, pubic symphysis diastasis >2.5 cm, widened right SI joint, and a displaced sacral fracture confirmed by imaging (APC III/VS pattern). This is a completely unstable pelvic ring injury, rendering non-operative management futile for achieving an acceptable functional outcome.
3.
Associated Injuries:
Extraperitoneal bladder rupture, suspected urethral involvement (though later ruled out), and life-threatening open tibia/fibula fractures requiring immediate debridement and external fixation. These complex injuries often dictate a damage control orthopaedics (DCO) approach.
Classification:
The injury pattern aligns with:
*
Young-Burgess Classification:
Anteroposterior Compression Type III (APC III). This is characterized by complete disruption of the pubic symphysis, anterior and posterior sacroiliac ligaments, and often a sacral fracture. The external rotation of the hemipelvis is characteristic. The presence of a displaced sacral fracture and vertical displacement further adds elements of Vertical Shear (VS).
*
Tile Classification:
Type C. This classification denotes complete disruption of the posterior pelvic arch, rendering the pelvis unstable in all planes (rotational and vertical). This patient clearly fits a Type C injury due to the complete posterior ligamentous disruption and displaced sacral fracture.
Given the patient's polytrauma status and hemodynamic instability, a staged approach following damage control principles was adopted:
- Emergency Room/Resuscitation Bay: Pelvic binder application, massive transfusion protocol, ATLS algorithms.
- Angiography Suite: Embolization of actively bleeding internal iliac artery branches.
-
Operating Room - First Stage (Damage Control):
- Open reduction and external fixation of the bilateral open tibia/fibula fractures.
- Placement of an anterior pelvic external fixator (supra-acetabular) for initial pelvic stabilization, reduction, and tamponade of hemorrhage. This significantly decreased the pelvic volume and provided temporary stability.
- Cystorrhaphy for extraperitoneal bladder rupture by Urology.
- Operating Room - Second Stage (Definitive Fixation): Once hemodynamically stable and soft tissue conditions allowed (typically 5-10 days post-initial trauma), definitive internal fixation of the pelvic ring was planned. This was crucial for long-term stability and ambulation.
Surgical Technique / Intervention
Stage 1: Damage Control Orthopaedics (DCO)
- Patient Positioning: Supine on a radiolucent table.
-
Anterior Pelvic External Fixator:
- Pin Placement: Two Schanz pins (typically 5mm) were inserted into the supra-acetabular region, approximately 2 cm posterior and 2 cm superior to the anterior inferior iliac spine (AIIS). Entry point was approximately 2 cm superior to the iliac crest, aiming for the dense cortical bone of the posterior column. Fluoroscopic guidance (inlet/outlet/obturator oblique views) confirmed safe pin placement, avoiding the hip joint, sciatic nerve, and neurovascular bundle.
- Reduction & Frame Application: Gentle manual reduction of the symphysis diastasis and external rotation was performed. The external fixator frame was then constructed using carbon fiber rods connecting the Schanz pins. Compression across the symphysis was achieved by gradually tightening the clamps. This provides immediate stability and helps control ongoing pelvic hemorrhage by reducing pelvic volume.
Stage 2: Definitive Pelvic Internal Fixation (7 days post-injury)
- Patient Positioning: The patient was positioned supine on a radiolucent table with a bump under the ipsilateral hip for optimal fluoroscopic views. Preparations for intra-operative traction were made if needed.
-
Anterior Ring Fixation (Pubic Symphysis ORIF):
- Approach: Pfannenstiel incision was made (modified Stoppa approach for wider access to the retroperitoneal space was considered but deemed unnecessary given the bladder repair had been performed and anterior access was prioritized for plating). The rectus abdominis muscles were released from the pubic symphysis.
- Reduction: The symphysis diastasis was reduced using pointed reduction clamps or a pelvic clamp applied across the iliac crests. Intra-operative fluoroscopy (AP, inlet, outlet views) confirmed anatomical reduction of the symphysis and restoration of the anterior pelvic ring.
- Fixation: A 6-hole, 3.5mm reconstruction plate was contoured and applied to the superior aspect of the pubic symphysis, bridging the diastasis. Two cortices of fixation were achieved in each pubic ramus using bicortical screws. A second smaller plate (e.g., 4-hole reconstruction plate) was considered and applied inferiorly to enhance construct stability, creating a "double-plating" technique, which is particularly robust for APC III injuries.
-
Posterior Ring Fixation (Right Sacroiliac Joint & Sacral Fracture):
- Approach: Percutaneous iliosacral screw fixation was chosen due to less soft tissue disruption compared to an open approach, given the patient's existing soft tissue injuries and comorbidities.
- Reduction: Maintaining the reduction achieved by the anterior fixation, further reduction of the sacral fracture displacement was attempted using a joystick technique with a Schanz pin inserted into the posterior superior iliac spine (PSIS) or by adjusting the external fixator. Careful fluoroscopic monitoring was paramount.
-
Fixation:
- Iliosacral Screws: Under strict fluoroscopic guidance (inlet, outlet, and sacral alar views), two percutaneous cannulated iliosacral screws were placed from the right ilium into the S1 and S2 vertebral bodies. The S1 screw was directed into the S1 body, avoiding the S1 nerve root and anterior vascular structures. The S2 screw was directed into the S2 body, taking care to avoid the S2 nerve root and the sciatic notch. The "safe zones" for screw placement were meticulously identified. The goal was bicortical purchase into the sacral body where possible, especially for S1.
- Sacral Alar View: This oblique view (approximately 30-45 degrees from AP) was critical to visualize the sacral foramen and ensure the screw trajectory was safely within the sacral ala.
- Screw Length and Diameter: Typically 7.0mm or 8.0mm cannulated screws were used, with lengths determined by pre-operative templating and intra-operative measurements.
- Post-Fixation Assessment: Post-fixation fluoroscopy confirmed anatomical reduction and safe screw placement. Stability was re-checked gently.
Considerations for the Tibial Fractures
- The bilateral open tibia/fibula fractures were initially managed with thorough debridement, irrigation, and external fixation at the time of the first pelvic external fixator placement. Definitive management (e.g., intramedullary nailing, plate fixation) would be performed once soft tissue conditions improved, and the patient's overall stability allowed. This might involve staged procedures.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Days 0-7)
- Pain Management: Multimodal analgesia including epidural, regional blocks, and systemic medications to manage severe pain.
- Wound Care: Meticulous wound care for all surgical sites (pelvis, bilateral tibias). Close monitoring for signs of infection.
- DVT Prophylaxis: Pharmacological (low molecular weight heparin) and mechanical (intermittent pneumatic compression devices) prophylaxis initiated promptly.
- Mobilization: Bed rest initially with log rolling for position changes to maintain pelvic stability. Upper extremity exercises encouraged. Gradual progression to bedside chair sitting, depending on overall stability and pain.
- Weight Bearing: Non-weight bearing (NWB) on the affected right lower extremity and touch-down weight bearing (TDWB) on the left (due to the tibial fracture) for at least 8-12 weeks, until radiographic evidence of early union and clinical stability. The pubic symphysis plating provides rotational stability, but the posterior sacral fracture requires longer protection from axial loading.
- Bladder Management: Indwelling Foley catheter remained in place for at least 2-3 weeks post-cystorrhaphy, with a repeat cystogram to confirm bladder integrity prior to removal.
- Nutritional Support: Optimization of nutritional status to support healing, particularly for polytrauma patients.
Subacute Phase (Weeks 2-12)
- Physical Therapy: Progressive out-of-bed mobilization with assistive devices (walker/crutches), strictly adhering to weight-bearing restrictions. Focus on core strengthening, gluteal activation, and maintaining lower extremity range of motion (within pain limits). Non-weight bearing gait training initiated.
- Radiographic Follow-up: AP pelvis, inlet, and outlet views at 6 weeks and 12 weeks to assess for maintenance of reduction and early signs of union.
- Tibial Fractures: Continue management of the bilateral tibial fractures as per their respective protocols, likely involving staged definitive fixation.
Rehabilitation Phase (Months 3-6+)
- Gradual Weight Bearing: Progression from TDWB/NWB to partial weight bearing (PWB) and then full weight bearing (FWB) based on radiographic evidence of healing and clinical assessment of pelvic stability. This is a critical decision point for sacral fractures, often delayed for up to 3-4 months.
- Intensified PT: Emphasis on strength training, balance, proprioception, and functional mobility. Gait training without assistive devices.
- Return to Activity: Gradual return to activities of daily living. Return to sports or demanding physical labor can take 6-12 months, contingent on complete healing, pain resolution, and functional recovery.
- Complication Monitoring: Ongoing monitoring for chronic pain, nonunion/malunion, heterotopic ossification, neurological deficits (e.g., sacral nerve root irritation), and deep infection.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- ATLS Principles Paramount: The primary survey and aggressive resuscitation are critical. Pelvic trauma is a major source of hemorrhage.
- Gentle Pelvic Exam: Avoid repetitive, aggressive maneuvers to prevent dislodging clots and exacerbating hemorrhage. A single, gentle "springing" of the pelvis is sufficient to assess gross instability.
- Pelvic Binder: Apply promptly in any suspected unstable pelvic injury. Position it over the greater trochanters, not the iliac crests, for optimal compression.
- Hemorrhage Control: Angiography with embolization is the gold standard for arterial bleeding from pelvic fractures in hemodynamically unstable patients once mechanical stability is addressed. Venous bleeding is more common and controlled by volume reduction with external fixation.
- Urogenital Assessment: Always suspect bladder/urethral injury in pelvic trauma. Perform a retrograde urethrogram (RUG) before attempting Foley catheter insertion if urethral injury is suspected (e.g., blood at meatus, high-riding prostate, scrotal/perineal hematoma).
- Neurological Assessment: Thorough lower extremity neurological exam, especially sacral roots (DRE for tone), is crucial pre- and post-op to identify and monitor for nerve injury. Denis Zone II/III sacral fractures are at high risk.
- Damage Control Orthopaedics (DCO): For polytrauma patients, initial external fixation of the pelvis and long bone fractures can be life-saving. Definitive fixation is delayed until the patient is physiologically stable.
- Fluoroscopic Reliance: Intra-operative fluoroscopy with AP, inlet, outlet, and sacral alar views is indispensable for accurate reduction and safe iliosacral screw placement. Know your "safe zones" and critical trajectories.
- Reduction First, Then Fixation: Achieve and maintain anatomical reduction of the pelvic ring before applying definitive fixation. Poor reduction leads to poor outcomes (pain, malunion, functional deficit).
- Assess Posterior First: The posterior ring dictates pelvic stability. Address posterior instability (sacral fracture, SI joint disruption) first, then proceed to anterior fixation.
- Open Fractures: Open pelvic fractures (rare but devastating) require extensive debridement, antibiotics, and often colostomy/urinary diversion, in addition to fixation.
Pitfalls
- Missed Hemorrhage: Underestimating the volume of blood loss into the retroperitoneum.
- Aggressive Resuscitation Without Control: "Fill the tank" without "plugging the leak" leads to dilutional coagulopathy and worsening prognosis.
- Inadequate Pre-op Planning: Not utilizing CT 3D reconstructions for templating screw trajectories or plate contours.
- Neurovascular Injury During Fixation: Improper screw placement (iliosacral screws) can injure sacral nerve roots, sciatic nerve, internal iliac vessels, or superior gluteal artery. Meticulous fluoroscopy is paramount.
- Incomplete Posterior Fixation: Failing to recognize subtle posterior instability or under-fixing a significantly unstable posterior ring injury (e.g., using a single SI screw for a VS injury that requires two or more points of fixation, or open plating).
- Malreduction: Accepting a suboptimal reduction, leading to chronic pain, gait disturbance, and functional limitations.
- Early Weight Bearing: Premature weight bearing, especially with sacral fractures or ligamentous disruption, can lead to loss of reduction, implant failure, nonunion, or chronic pain.
- Missing Associated Injuries: Failure to diagnose bladder/urethral injuries, rectal lacerations, or vascular injuries.
- Soft Tissue Complications: Ignoring potential Morel-Lavallée lesions, leading to seroma, infection, or skin necrosis.
- Inadequate DVT Prophylaxis: High risk of DVT/PE in pelvic trauma, requiring aggressive prophylaxis.
