Pediatric Orthopedic MCQs (Set 4): Hip, Spine & Trauma | ABOS OITE 2004 Review

Key Takeaway
This high-yield Set 4 of pediatric orthopedic MCQs prepares candidates for ABOS & OITE exams. It focuses on critical topics like developmental dysplasia of the hip, management of pediatric scoliosis, and common physeal and diaphyseal fractures in children, emphasizing diagnosis and treatment principles.
Pediatric Orthopedic MCQs (Set 4): Hip, Spine & Trauma | ABOS OITE 2004 Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The mother of a 24-month-old girl reports that the child cannot rotate her right forearm. She also notes delayed development, with the child first walking at 18 months. The child has a five-word vocabulary and has not begun using simple phrases. Examination reveals that the right forearm is fixed in 80 degrees of pronation. The remainder of the examination of both upper extremities is otherwise normal. A radiograph is shown in Figure 41. Which of the following studies will best aid in diagnosis?
Explanation
Question 2
Figure 42 shows the radiograph of a patient with spinal muscular atrophy. Examination reveals good upper extremity function, and she can tie her shoes and propel a manual wheelchair. Posterior instrumentation and fusion may result in
Explanation
Question 3
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
Question 4
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
Question 5
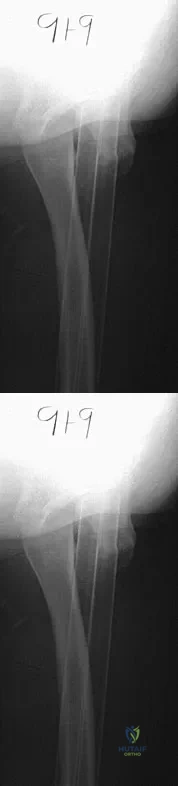
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
Question 6
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
Question 7
The patient shown in Figure 44 reports that her toes hurt when she walks. Management should consist of
Explanation
Question 8
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?
Explanation
Question 9
Examination of a 9-year-old boy reveals a right thoracic prominence on forward flexion. Neurologic examination is normal, and no other abnormalities are noted. AP radiographs reveal a 30-degree right thoracic curve. Initial management should consist of
Explanation
Question 10
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
Question 11
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
Question 12
A 14-year-old girl with a right thoracic curve from T4 through L2 measuring 78 degrees is scheduled to undergo posterior spinal fusion for scoliosis. The surgical plan is to fuse from T3 through L2, using pedicle screws at L2 and about the apex at T8. What neural monitoring modality is most likely to identify a reversible neurologic deficit during surgery?
Explanation
Question 13
Figure 46 shows the radiograph of an obese 12-year-old boy who has had left hip pain for the past 3 months. What is the best course of action?
Explanation
Question 14
A 7-year-old boy sustained a head contusion and small bowel injuries in a motor vehicle accident in which he was wearing a lap belt. He subsequently required a bowel resection. Six weeks after the accident, his parents note a painful mass in his lower back. His neurologic examination is normal. A radiograph and CT scans are shown in Figures 47a through 47c. Definitive management should now consist of
Explanation
Question 15
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
Question 16
A 10-year-old boy who has had progressive low back and right buttock pain for the past 3 days is now unable to bear weight on the right side secondary to pain. He has a temperature of 101.3 degrees F (38.5 degrees C). Examination reveals full hip range of motion; but he reports pain on the right side with external rotation. Pain is elicited with compression of the iliac wings and with direct palpation of the right sacroiliac (SI) joint. An MRI scan of the pelvis shows no abscess, but there is inflammation of the SI joint. Management should consist of
Explanation
Question 17
Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate
Explanation
Question 18
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
Question 19
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
Question 20
A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiographs show that the left distal femoral growth plate is now closed; however, the tibial growth plate is still open. Her bone age matches her chronologic age. Management should consist of
Explanation
Question 21
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
Question 22
A 12-year-old boy with hemophilia A and no known inhibitors sustains a tibia fracture and has pain with passive motion of the deep toe flexors. Appropriate management should consist of
Explanation
Question 23
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
Question 24
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
Question 25
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Question 26
A 13-year-old obese male presents with acute left hip pain and an inability to bear weight following a minor fall. He reports intermittent mild hip pain for 3 months prior. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following is the most significant risk factor for developing avascular necrosis (AVN) in this patient?
Explanation
Question 27
A 3-year-old girl is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Neurological examination is normal. As part of her initial workup, which of the following screening modalities is mandatory?
Explanation
Question 28
A 6-year-old boy falls from monkey bars and sustains a significantly displaced, extension-type supracondylar humerus fracture. On examination, he is unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely injured?
Explanation
Question 29
A 6-week-old female infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). At her 2-week follow-up, the parents report she has stopped actively kicking her left leg. Examination reveals decreased active knee extension on the left side. What is the most appropriate next step in management?
Explanation
Question 30
A 13-year-old girl twists her ankle while playing soccer. Radiographs reveal a fracture of the anterolateral aspect of the distal tibial epiphysis. What is the primary deforming force and mechanism responsible for this specific injury pattern?
Explanation
Question 31
A 4-year-old boy presents with a 2-day history of right hip pain and refusing to bear weight. His temperature is 38.8 Celsius (101.8 F). Laboratory studies show a WBC count of 13,000/mm3, ESR of 45 mm/hr, and CRP of 3.0 mg/dL. Radiographs of the hip are normal. Based on these findings, what is the most appropriate next step?
Explanation
Question 32
A 5-year-old boy sustains a closed, isolated midshaft femur fracture. He weighs 22 kg (48 lbs). According to the AAOS Clinical Practice Guidelines, which of the following is the most appropriate definitive treatment?
Explanation
Question 33
A 12-year-old boy presents with right hip pain and inability to bear weight for the past 24 hours. Radiographs confirm a slipped capital femoral epiphysis (SCFE).
According to the Loder classification, which of the following is the most likely major complication associated with his condition?

Explanation
Question 34
A 3-month-old girl with developmental dysplasia of the hip (DDH) is being treated with a Pavlik harness. During a follow-up visit, her parents report that she is no longer actively extending her knee on the treated side. Which of the following positioning errors is the most likely cause of this complication?
Explanation
Question 35
A 4-year-old boy is brought to the emergency department after a high-speed motor vehicle collision. Lateral cervical spine radiographs reveal a 3.5 mm anterior displacement of C2 on C3. Swischuk's line (posterior cervical line) passes 1 mm anterior to the anterior aspect of the posterior arch of C3. What is the most appropriate management?
Explanation
Question 36
A 14-year-old female presents with a progressive right thoracic scoliotic curve. Radiographs reveal an adolescent idiopathic scoliosis (AIS) curve measuring 55 degrees. Her Risser stage is 0. What is the primary indication for surgical intervention in this patient?
Explanation
Question 37
A 6-year-old boy presents with an established nonunion of a lateral humeral condyle fracture sustained 2 years ago.
He demonstrates a progressive cubitus valgus deformity. Which of the following neurologic complications is most strongly associated with this condition?

Explanation
Question 38
A 2-year-old boy is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Which of the following sets of screening studies is mandatory for this patient?
Explanation
Question 39
A 9-year-old boy is diagnosed with Legg-Calvé-Perthes disease.
Anteroposterior pelvis radiographs reveal that the lateral pillar of the femoral head has collapsed to less than 50% of its original height. According to the Herring Lateral Pillar Classification, into which group does he fall, and what is the general prognosis?
Explanation
Question 40
A 5-year-old girl sustains a Gartland type III supracondylar humerus fracture.
Upon evaluation in the emergency department, her hand is pink and warm, but the radial pulse is absent. What is the most appropriate next step in management?

Explanation
Question 41
A 3-year-old boy presents with a temperature of 38.8°C, an ESR of 45 mm/hr, a WBC count of 14,000/mm³, and refusal to bear weight on his left leg. According to the Kocher criteria, what is the approximate probability that this child has septic arthritis of the hip?
Explanation
Question 42
A 4-year-old boy sustains an isolated closed diaphyseal fracture of the right femur. He is treated with an early spica cast. What is the maximum acceptable amount of initial fracture shortening in this age group to account for expected overgrowth?
Explanation
Question 43
A 5-year-old girl presents with a painless waddling gait. Radiographs reveal developmental coxa vara. The Hilgenreiner Epiphyseal Angle (HEA) is measured at 65 degrees. What is the most appropriate management?
Explanation
Question 44
A 13-year-old girl sustains an inversion and external rotation injury to her ankle. Radiographs show a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. Avulsion of which ligament is responsible for this specific fracture pattern?
Explanation
Question 45
A 6-month-old infant is noted to have a left-sided thoracic scoliosis measuring 25 degrees. The Rib-Vertebral Angle Difference (RVAD) of Mehta is measured at 28 degrees. What does this finding indicate regarding the natural history of the curve?
Explanation
Question 46
A 14-year-old boy with Duchenne Muscular Dystrophy (DMD) has a progressive neuromuscular scoliosis of 40 degrees. His Forced Vital Capacity (FVC) is 45% of predicted. What is the recommended surgical strategy to optimize his quality of life and sitting balance?
Explanation
Question 47
A 4-month-old infant presents to the emergency department with a swollen left thigh. Radiographs reveal a metaphyseal "corner" fracture of the distal femur. Which of the following steps is the most critical next action?
Explanation
Question 48
A 9-year-old girl, whose weight is in the 40th percentile, presents with right groin pain and a limp. Radiographs confirm a slipped capital femoral epiphysis (SCFE).
Given her presentation, an endocrine workup is indicated. Which of the following is the most common underlying endocrine disorder associated with this condition?

Explanation
Question 49
A 5-year-old boy sustains a type III extension supracondylar humerus fracture. After closed reduction and percutaneous pinning, the hand is noted to be pink but lacks a palpable radial pulse. Doppler confirms a monophasic signal at the wrist. What is the most appropriate next step in management?
Explanation
Question 50
A 2-year-old boy is diagnosed with a congenital hemivertebra in the lower thoracic spine. Which of the following screening studies is most critically indicated in the initial workup?
Explanation
Question 51
A 3-month-old girl with developmental dysplasia of the hip (DDH) is being treated in a Pavlik harness. During a follow-up examination, the orthopedist notes decreased active extension of the left knee. What is the most likely cause of this finding?
Explanation
Question 52
A 14-year-old boy sustains a juvenile Tillaux fracture of the distal tibia while skateboarding.
This fracture pattern occurs due to the specific sequence of distal tibial physeal closure. What mechanism of injury is most classically responsible for this fracture?
Explanation
Question 53
A 6-year-old child falls from monkey bars and sustains a displaced extension-type supracondylar humerus fracture. Which of the following physical examination findings corresponds to the most common neurological injury associated with this specific fracture pattern?
Explanation
Question 54
Which of the following fixed spinopelvic radiographic parameters is most strongly associated with the severity and progression risk of an isthmic spondylolisthesis in a pediatric patient?
Explanation
Question 55
A 13-year-old boy underwent in situ pinning for a stable slipped capital femoral epiphysis (SCFE) 6 months ago. He now presents with a severely stiff, painful hip. Radiographs show a concentric, severe narrowing of the joint space. What is the most likely diagnosis?
Explanation
Question 56
A 6-year-old child sustains a displaced lateral condyle fracture of the humerus that is missed and not treated operatively. If this progresses to a nonunion, which of the following long-term complications is most likely to develop years later?
Explanation
Question 57
A 5-year-old boy presents with a limp, a temperature of 38.9°C (102°F), and an inability to bear weight on his right leg. Laboratory tests show an ESR of 55 mm/hr and a WBC count of 14,000/mm3. According to the modified Kocher criteria, what is the predictive probability that this child has septic arthritis of the hip?
Explanation
Question 58
An 8-month-old infant is evaluated for a left-sided thoracic spinal curve. Radiographs show an infantile idiopathic scoliosis with a Rib-Vertebra Angle Difference (RVAD) of 28 degrees. What is the most appropriate next step in management?
Explanation
Question 59
An 11-year-old boy weighing 65 kg (143 lbs) sustains a closed, length-stable midshaft femur fracture. If this fracture is treated with titanium elastic nails (TENs), the patient is at highest risk for which of the following complications compared to submuscular plating?
Explanation
Question 60
A 12-year-old premenarchal girl presents with adolescent idiopathic scoliosis. Radiographs demonstrate a right thoracic curve of 32 degrees. Her Risser stage is 0. What is the most appropriate management?
Explanation
Question 61
A 7-year-old boy with Down syndrome undergoes routine cervical spine screening radiographs. Flexion-extension views reveal an Atlanto-Dens Interval (ADI) of 9 mm. He is neurologically intact and asymptomatic. What is the recommended management?
Explanation
Question 62
A 13-year-old obese boy presents with 3 weeks of left knee pain and a limp. Examination reveals obligatory external rotation of the left hip when it is passively flexed. Radiographs confirm a mild slipped capital femoral epiphysis (SCFE). Which of the following is the most appropriate initial management?
Explanation
Question 63
A 6-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. On initial presentation, his hand is pink but the radial pulse is absent. Following closed reduction and percutaneous pinning, the hand remains pink and well-perfused, but the radial pulse is still non-palpable. What is the most appropriate next step in management?
Explanation
Question 64
A 14-year-old female gymnast presents with persistent low back pain that radiates to her posterior thighs. Nonoperative management has failed after 6 months. Radiographs demonstrate a Grade III isthmic spondylolisthesis at L5-S1 with a slip angle of 45 degrees. Which of the following surgical treatments is most appropriate?
Explanation
Question 65
A 7-year-old boy presents with a painless limp of 2 months duration. Radiographs reveal fragmentation and increased density of the right capital femoral epiphysis consistent with Legg-Calve-Perthes disease. Which of the following is the most significant prognostic factor for the final outcome of his hip?
Explanation
Question 66
A 2-month-old girl is being treated with a Pavlik harness for developmental dysplasia of the hip. At her 2-week follow-up, the mother reports that the infant has stopped kicking her left leg. On examination, the left knee does not actively extend, but passive range of motion is normal. Which of the following is the most appropriate management?
Explanation
Question 67
A 6-month-old infant is referred for a left thoracic curve measuring 25 degrees. The rib-vertebra angle difference (RVAD) of Mehta at the apical vertebra is 25 degrees. There are no other abnormalities. What is the most likely natural history of this curve?
Explanation
Question 68
A 6-year-old boy weighing 22 kg (48 lbs) sustains a closed, isolated midshaft femur fracture after falling from a tree. What is the most appropriate treatment?
Explanation
Question 69
A 13-year-old boy sustains an ankle injury. Radiographs and CT scan demonstrate a fracture of the distal tibia with a sagittal fracture through the epiphysis, an axial fracture through the physis, and a coronal fracture through the posterior metaphysis. This injury is best classified as an equivalent to which Salter-Harris pattern?
Explanation
Question 70
A 14-year-old girl sustains a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. What is the primary mechanism of injury for this specific fracture pattern?
Explanation
Question 71
A 14-year-old girl underwent uncomplicated in situ pinning for a stable SCFE 6 months ago. She now presents with a worsening limp and a stiff hip. Examination reveals a painful, global restriction of hip motion. Radiographs show concentric narrowing of the hip joint space. What is the most likely diagnosis?
Explanation
Question 72
A newborn male is noted to have congenital scoliosis due to a fully segmented hemivertebra at T8.
Which of the following screening evaluations is mandatory to detect associated, occult abnormalities?
Explanation
Question 73
A 4-week-old infant is referred for congenital muscular torticollis. The head is tilted to the right and rotated to the left. A firm mass is palpable in the right sternocleidomastoid muscle. In addition to physical therapy for the neck, what additional screening is most strongly indicated?
Explanation
Question 74
A 5-year-old boy sustains a fall and presents with elbow pain. Radiographs reveal a displaced (>2 mm) lateral condyle fracture of the humerus. If left untreated, what is the most likely long-term complication of this injury?
Explanation
Question 75
A 10-year-old boy is evaluated for a leg length discrepancy 2 years after sustaining a distal femoral physeal fracture. Radiographs show a central 30% bony bar across the distal femoral physis with 2 years of growth remaining. What is the most appropriate management?
Explanation
Question 76
A 7-year-old girl with spastic quadriplegic cerebral palsy presents for routine evaluation. Pelvic radiographs demonstrate a Reimers migration percentage of 55% in the right hip. There is no evidence of joint space narrowing or femoral head deformity. What is the most appropriate surgical management?
Explanation
Question 77
A 12-year-old obese boy presents with acute-on-chronic left hip pain and inability to bear weight. Radiographs confirm an unstable slipped capital femoral epiphysis (SCFE). Which of the following is the most appropriate initial management to minimize the risk of avascular necrosis?
Explanation
Question 78
A 3-month-old girl is being treated for developmental dysplasia of the hip with a Pavlik harness. During a follow-up visit, the mother notes that the child is no longer kicking her left leg. Examination reveals absent active knee extension on the left. The most appropriate next step is to:
Explanation
Question 79
A 6-year-old boy presents with a limp and hip pain. Radiographs demonstrate Legg-Calve-Perthes disease with >50% lateral pillar collapse (Herring Group C). According to the literature, which of the following best describes the expected outcome?
Explanation
Question 80
A 5-year-old boy sustains a completely displaced extension-type supracondylar fracture of the humerus. On examination, the hand is pink and warm, but the radial pulse is absent. After urgent closed reduction and percutaneous pinning, the hand remains pink and warm, but the radial pulse remains non-palpable. What is the most appropriate next step?
Explanation
Question 81
A 14-year-old boy sustains a Salter-Harris III fracture of the anterolateral distal tibial epiphysis (Tillaux fracture). This fracture pattern is directly caused by avulsion from which of the following structures?
Explanation
Question 82
A newborn is diagnosed with a congenital hemivertebra in the thoracic spine. Which of the following is the most appropriate initial screening protocol for associated anomalies?
Explanation
Question 83
A 13-year-old premenarchal girl presents with adolescent idiopathic scoliosis. Radiographs demonstrate a right thoracic curve of 55 degrees and a Risser stage of 0. Which of the following is the most appropriate treatment?
Explanation
Question 84
A 6-year-old boy falls onto his outstretched arm and sustains a lateral condyle fracture of the humerus. Radiographs show a displacement of 4 mm. Which of the following is the most appropriate management?
Explanation
Question 85
A 14-year-old male gymnast presents with chronic low back pain and a waddling gait. Radiographs reveal a Grade III isthmic spondylolisthesis at L5-S1 with a slip angle of 55 degrees. Nonoperative management has failed. What is the most appropriate surgical intervention?
Explanation
Question 86
A 7-month-old infant is brought to the emergency department with a swollen right thigh. Radiographs reveal a spiral fracture of the femoral shaft. The parents state the child caught his leg in the crib rails. What is the most critical next step in management?
Explanation
Question 87
A 4-year-old boy presents with a 2-day history of right hip pain, a temperature of 38.8°C, and refusal to bear weight. Laboratory tests show an ESR of 50 mm/hr and a WBC of 14,000/mm³. Radiographs are unremarkable. What is the most appropriate next step?
Explanation
Question 88
A 6-year-old boy sustains a Bado Type I Monteggia fracture-dislocation. If a neurologic deficit is present upon initial examination, which of the following nerve branches is most likely affected?
Explanation
Question 89
A 10-month-old infant presents with a left-sided thoracic curve measuring 30 degrees. The diagnosis of infantile idiopathic scoliosis is suspected. Which of the following radiographic parameters is most predictive of whether this curve will progress or spontaneously resolve?
Explanation
Question 90
A 6-week-old infant is being treated with a Pavlik harness for developmental dysplasia of the left hip. The parents report that the child has stopped kicking the left leg. On examination, the left knee remains actively flexed, but the infant does not actively extend it. Patellar reflex is absent on the left. What is the most appropriate next step in management?
Explanation
Question 91
A 6-year-old boy falls from the monkey bars and sustains a significantly displaced extension-type supracondylar humerus fracture. Prior to reduction, the examiner notes that the child cannot flex the interphalangeal joint of the thumb or the distal interphalangeal joint of the index finger. Which of the following nerves is most likely injured?
Explanation
Question 92
A 13-year-old obese boy presents to the emergency department with sudden, severe left hip pain after tripping on a step. He is entirely unable to bear weight on the left leg, even with the use of crutches. Radiographs demonstrate a displaced slipped capital femoral epiphysis (SCFE). Which of the following represents the most significant complication risk specific to this presentation compared to a patient who can bear weight?
Explanation
None
