Introduction & Epidemiology
Pediatric buckle fractures, also known as torus fractures, represent a common injury in the skeletally immature population. These stable, incomplete fractures typically occur in the metaphyseal region of long bones, most frequently the distal radius, following an axial load or impaction injury. The term "buckle" refers to the compression of the cortex, leading to a localized bulge or wrinkle rather than a complete break through both cortices. These fractures account for a significant proportion of pediatric upper extremity trauma, often exceeding 50% of all distal forearm fractures in children, particularly those between 6 and 10 years of age.
The distal radius is highly susceptible due to its cancellous bone structure at the metaphysis, which is less rigid than cortical bone and thus prone to compression under axial force, such as a fall onto an outstretched hand (FOOSH). The mechanism involves an axial compressive force that exceeds the elastic limit of the bone but is insufficient to cause a complete cortical breach.
Clinically, buckle fractures present with localized pain, swelling, and tenderness, but typically without overt deformity or neurovascular compromise. Radiographically, they are characterized by a subtle cortical bulge or angulation, most commonly visible on lateral views of the distal radius. Due to their inherent stability and minimal displacement, buckle fractures have historically been managed with rigid immobilization, such as short arm casts. However, a growing body of evidence, driven by principles of judicious resource utilization and patient comfort, supports equally efficacious outcomes with less restrictive modalities, particularly the Velcro wrist brace. This review aims to consolidate current understanding and practical guidance on the optimal management of pediatric buckle fractures, emphasizing the role of the Velcro wrist brace.
Surgical Anatomy & Biomechanics
Understanding the unique characteristics of pediatric bone is paramount when discussing buckle fractures. The bone in children differs significantly from that of adults in several key aspects:
- Physis (Growth Plate): Present in skeletally immature bone, the physis is typically weaker than surrounding ligaments and bone, making it a common site for physeal injuries (Salter-Harris fractures). Buckle fractures, however, typically occur in the metaphysis, sparing the physis, though adjacent injuries are possible.
- Thicker, Stronger Periosteum: The pediatric periosteum is thicker and more osteogenic, contributing to fracture stability and robust healing. This robust periosteal sleeve often remains intact even in more complex pediatric fractures, providing inherent stability and facilitating rapid callus formation. In buckle fractures, the periosteum usually remains completely intact, acting as a natural splint.
- Increased Porosity and Elasticity: Pediatric bone has a higher remodeling capacity, increased porosity, and greater elasticity compared to adult bone. This increased elasticity allows for greater deformation before complete fracture, contributing to the occurrence of incomplete fracture patterns like greenstick and buckle fractures.
-
Metaphyseal-Diaphyseal Junction:
The distal radial metaphysis, where buckle fractures most commonly occur, is composed predominantly of cancellous bone. This region acts as a "crumple zone" under axial load. When a compressive force is applied along the longitudinal axis of the bone, the cancellous bone compacts, causing the outer cortex to buckle or wrinkle, often on the side opposite the impact point due to eccentric loading.

The biomechanics of a buckle fracture involve axial compression exceeding the bone's elastic limit. Instead of a sharp break, the bone deforms plastically, leading to a localized buckling or invagination of the cortex. This mechanism ensures inherent stability as the opposing cortex remains intact, and any angular deformation is minimal and stable. The intact periosteum further contributes to this stability, preventing significant displacement or instability. The absence of a complete cortical breach and the stable nature of the deformity are fundamental to understanding the appropriate non-operative management approach.
Indications & Contraindications
The management of pediatric distal radius fractures hinges on accurate diagnosis and a thorough understanding of fracture stability and growth plate involvement. For pediatric buckle fractures, non-operative management is universally indicated. The decision to use a Velcro wrist brace versus a more rigid cast is primarily driven by fracture stability, patient comfort, and established evidence.
Indications for Velcro Wrist Brace in Buckle Fractures
A Velcro wrist brace is indicated for nearly all unequivocally diagnosed distal radius buckle fractures due to their inherent stability. Specific criteria include:
- Radiographic confirmation of a buckle fracture: Presence of a cortical bulge or wrinkle without a complete cortical breach on at least one view (often best seen on the lateral).
- Clinical stability: Absence of gross deformity, significant angulation, or rotational displacement.
- No neurovascular compromise: Intact sensation, motor function, and perfusion to the hand and fingers.
- Patient and parental compliance: Ability to adhere to brace-wearing instructions and recognize potential issues.
- Absence of concomitant injuries: No other fractures, dislocations, or significant soft tissue injuries requiring different management.
Contraindications for Velcro Wrist Brace
While buckle fractures are typically stable, certain findings necessitate a more rigid form of immobilization (e.g., short arm cast) or even operative intervention for other types of pediatric distal radius fractures:
- Complete Fracture: Any complete cortical breach, even with minimal displacement (e.g., greenstick fractures with significant angulation or potential for displacement).
- Significant Displacement or Angulation: Displaced metaphyseal fractures (>15-20 degrees angulation) or those with translational shift that may require reduction.
- Rotational Deformity: Though rare in buckle fractures, any rotational malalignment.
- Irreducible Fracture: For fractures that do not reduce adequately with closed manipulation.
-
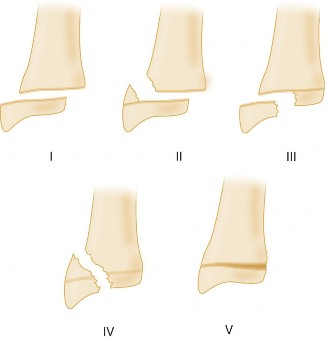
Physeal Involvement (Salter-Harris types):
- Salter-Harris I: Often stable, but may require cast immobilization depending on clinical suspicion and mechanism.
- Salter-Harris II: Stable types can be managed with closed reduction and casting. Unstable or significantly displaced types may require pinning.
- Salter-Harris III, IV, V: These are intra-articular or complex physeal fractures requiring anatomical reduction, often surgically, to prevent growth disturbance or articular incongruity.
- Open Fractures: Require immediate surgical debridement and often fixation.
- Neurovascular Compromise: Urgent reduction and stabilization are required, potentially operative.
- Compartment Syndrome: Signs or symptoms necessitate immediate fasciotomy.
- Polytrauma or Multiple Injuries: The need for comprehensive management may influence immobilization choice.
- Patient Non-Compliance: If there are concerns regarding a patient's or caregiver's ability to maintain the brace, a cast may be a safer alternative.
The following table summarizes the indications for non-operative (Velcro brace vs. Cast) versus operative management for pediatric distal radius injuries, placing buckle fractures clearly within the non-operative, minimally restrictive category.
| Category | Indication for Velcro Brace (Buckle Fracture) | Indication for Short Arm Cast (Non-Buckle) | Indication for Operative Management |
|---|---|---|---|
| Fracture Type | Distal radius buckle (torus) fracture | Stable greenstick fractures with minimal angulation | Significantly displaced metaphyseal fractures (>15-20° angulation post-reduction) |
| Minimally displaced Salter-Harris I & II fractures | Irreducible fractures | ||
| Unstable Salter-Harris II fractures (e.g., apex volar/dorsal angulation) | |||
| Salter-Harris III, IV, V fractures (often intra-articular, unstable physeal) | |||
| Open fractures | |||
| Associated neurovascular injury requiring exploration or stable fixation | |||
| Displacement/Stability | No displacement, inherently stable | <15-20° angulation, stable after closed reduction (if needed) | Gross displacement, instability post-reduction, rotational deformity |
| Impending or established compartment syndrome | |||
| Associated Injuries | None | None | Polytrauma with need for definitive fixation, associated severe soft tissue injury |
| Neurovascular Status | Intact | Intact | Compromised (requires urgent intervention) |
| Patient Factors | Compliant patient/family | Compliant patient/family, preference for cast (e.g., for sports during recovery) | Non-compliance where stable fixation is paramount |
| Mechanism | Low-energy axial compression | Low to moderate energy trauma | High-energy trauma, significant forces |
|
Pre-Operative Planning & Patient Positioning
For the management of a pediatric buckle fracture, traditional "pre-operative planning" and "patient positioning" in the surgical sense are not applicable , as these injuries are managed non-operatively. However, the principles of meticulous assessment and preparation for non-operative care are critically important.
Assessment and Diagnostic Work-up
- Clinical History: Obtain a detailed history of the injury mechanism, time of injury, initial symptoms, and any previous wrist injuries. Ascertain handedness, activity level, and baseline function.
-
Physical Examination:
- Inspection: Observe for swelling, ecchymosis, and subtle deformities. Gross deformity is generally absent in buckle fractures.
- Palpation: Localize tenderness, typically over the dorsal or volar aspect of the distal radial metaphysis. Assess for crepitus, which is usually absent.
- Neurovascular Assessment: Meticulously assess capillary refill, radial and ulnar pulses, and sensation to all digits (median, ulnar, radial nerve distributions) and motor function. This is crucial to rule out concomitant nerve injury or vascular compromise, though rare with buckle fractures.
- Range of Motion: Pain limits wrist and finger range of motion, but gross restriction should be differentiated from pain-induced guarding. Assess elbow and shoulder to rule out proximal injuries.
-
Radiographic Evaluation:
- Standard Views: Obtain true anteroposterior (AP) and lateral radiographs of the wrist, ensuring inclusion of the entire distal radius and ulna. The fracture is often subtle, appearing as a slight bulge, often on the dorsal cortex on a lateral view. Oblique views may be helpful in ambiguous cases.
- Growth Plate Assessment: Careful scrutiny for physeal involvement, especially in younger children where radiolucent physeal lines can obscure subtle Salter-Harris I injuries.
-
Contralateral Views:
Rarely indicated for buckle fractures, but can be considered in very young children or complex cases to compare physes.

Preparation for Non-Operative Management (Velcro Wrist Brace Application)
Once a buckle fracture is confirmed and the decision for Velcro brace management is made, the "preparation" involves:
-
Patient and Parental Education:
- Explain the nature of the buckle fracture: stable, incomplete, excellent prognosis.
- Rationale for the Velcro brace: provides adequate support and protection, reduces pain, allows for easier hygiene and skin checks, comparable outcomes to casting, and improves patient comfort and acceptance.
- Instructions on brace wearing: wear at all times, including during sleep (except for hygiene), duration (typically 3-4 weeks).
- Activity restrictions: avoidance of contact sports, climbing, or activities that could reinjure the wrist. Encourage light activities that do not put direct stress on the wrist.
- Expected recovery: emphasize rapid pain relief and early return to activity.
- Signs of concern: worsening pain, swelling, numbness, tingling, skin irritation, inability to move fingers.
-
Brace Selection:
- Choose an appropriately sized, prefabricated pediatric wrist brace. It should extend from the mid-forearm to just proximal to the metacarpophalangeal (MCP) joints, allowing full finger and thumb mobility.
- Ensure proper fit: snug but not overly tight, allowing for full circulation. Velcro straps should be easily adjustable.
-
Pain Management:
- Recommend over-the-counter analgesics (acetaminophen, ibuprofen) as needed. Narcotics are almost never required for buckle fractures.
-
Follow-up Planning:
- A follow-up appointment is typically scheduled in 3-4 weeks for clinical reassessment and brace discontinuation. Routine follow-up radiographs are often not necessary for uncomplicated buckle fractures given their stability and excellent healing prognosis, though some centers still opt for a single follow-up film. Evidence suggests clinical assessment alone is sufficient for stable buckle fractures.
Detailed Surgical Approach / Technique
It is imperative to state unequivocally that pediatric buckle fractures of the distal radius do not require surgical intervention, nor do they necessitate formal closed reduction maneuvers typically employed for displaced fractures. The inherent stability and minimal displacement characteristic of a buckle fracture mean that the "technique" involved is entirely non-operative and centers on appropriate immobilization and symptom management.
Therefore, this section will focus on the non-operative management technique for buckle fractures, specifically detailing the application and rationale for a Velcro wrist brace, contrasting it with principles for other, more unstable pediatric distal radius fractures where reduction or more rigid immobilization would be considered.
Management Technique: Application of the Velcro Wrist Brace
The goal of immobilization for a buckle fracture is primarily pain control and protection during the initial healing phase, which is rapid.
-
Patient Comfort and Positioning:
- The patient should be seated comfortably with the affected arm supported on a table or in the parent's lap.
- The wrist should be placed in a neutral to slight extension position (approximately 10-20 degrees of extension), which is generally the position of comfort and optimal functional alignment. No specific "reduction" maneuver is required or performed.
-
Brace Selection and Sizing:
- Select a prefabricated pediatric wrist brace that provides adequate support without restricting finger or thumb movement. The brace should span approximately two-thirds of the forearm length and allow full MCP and interphalangeal joint range of motion.
-
Many commercial braces are available in pediatric sizes, offering semi-rigid support with metal or plastic stays (dorsal and/or volar) and multiple adjustable Velcro straps.

-
Brace Application:
- Open all Velcro straps and position the hand and forearm into the brace. Ensure the thumb is positioned correctly if the brace has a thumb spica component (some pediatric braces do not, allowing full thumb mobility).
- Begin fastening the straps, starting from the most distal one (around the wrist/hand) and working proximally.
- Tighten each strap snugly but not restrictively, ensuring there is no excessive pressure or blanching of the skin. Check that two fingers can comfortably slide under the straps.
- Verify that the brace does not impinge on the elbow or significantly restrict forearm rotation.
- Confirm full, pain-free range of motion of the fingers and thumb.
- Educate the patient and parent on how to remove, reapply, and adjust the brace.
-
Post-Application Check:
- Recheck neurovascular status distal to the brace.
- Ask the child to move their fingers and thumb to ensure no restriction or discomfort.
-
Confirm the brace is comfortable and provides adequate support.

Why a Velcro Wrist Brace is Sufficient (and often superior to casting)
- Inherent Stability: Buckle fractures are inherently stable. The intact cortex and periosteum prevent displacement. Therefore, rigid immobilization (e.g., plaster or fiberglass cast) is biomechanically unnecessary.
- Pain Control: The primary role of immobilization in buckle fractures is pain relief. A well-fitting brace provides sufficient support to reduce micro-motion at the fracture site, thereby alleviating pain effectively.
-
Reduced Complications:
Compared to casting, a brace offers several advantages:
- Fewer skin issues: Easier to maintain hygiene, reduced risk of cast-related skin irritation, pressure sores, or infection.
- Less risk of cast complications: No issues with cast too tight, pressure points, or compartment syndrome due to cast application.
- Improved hygiene: Allows for washing the hand and forearm.
- Improved Patient Acceptance and Comfort: Children generally prefer braces due to their lighter weight, removability for short periods (e.g., bathing), and less restrictive nature. This can improve compliance.
- Cost-Effectiveness: Prefabricated braces can be more cost-effective than cast application and removal services.
-
Equivalent Outcomes:
Numerous studies have demonstrated equivalent functional outcomes, healing times, and complication rates for buckle fractures managed with a Velcro brace compared to rigid casting.

Contrast with Management Principles for Other Pediatric Distal Radius Fractures
For other, more unstable pediatric distal radius fractures (e.g., significantly angulated greenstick fractures, displaced Salter-Harris II), the approach would involve:
- Closed Reduction: Often performed under conscious sedation or regional anesthesia. Techniques involve traction, manipulation (e.g., three-point molding), and often exaggerated supination or pronation depending on the deformity. The goal is anatomical or near-anatomical reduction.
- Immobilization after Reduction: Following successful closed reduction, a rigid short arm or long arm cast (depending on fracture stability and location) is applied to maintain the reduction. Radiographs are essential post-reduction and post-casting to confirm maintenance of alignment.
-
Open Reduction and Internal Fixation (ORIF):
This is reserved for:
- Irreducible fractures.
- Significantly displaced or unstable physeal fractures (e.g., Salter-Harris III, IV, or some unstable IIs) where anatomical reduction is critical for growth plate function and articular congruity.
- Open fractures.
- Neurovascular compromise requiring direct visualization or stabilization.
- Common fixation methods include K-wires (percutaneous or open), bioabsorbable pins, or rarely, plates and screws (in older adolescents with larger bone size).
-
Internervous Planes / Dissection:
For operative approaches (not for buckle fractures), specific internervous planes would be utilized to access the distal radius, such as the interval between the brachioradialis and the radial artery/flexor carpi radialis for a volar approach, or between the extensor carpi ulnaris and extensor digiti minimi for a dorsal approach. This type of dissection is entirely irrelevant for a buckle fracture.

In summary, the "technique" for buckle fractures is elegantly simple: accurate diagnosis, robust patient/parent education, and appropriate application of a comfortable, protective Velcro wrist brace. Any discussion of surgical approaches, dissection, or fixation for these injuries is a fundamental misunderstanding of their pathology and optimal management.
Complications & Management
Pediatric buckle fractures are associated with an exceptionally low rate of complications, largely owing to their inherent stability and the rapid healing capacity of pediatric bone. Most complications are minor and resolve without long-term sequelae. The vast majority of management errors relate to over-immobilization rather than under-treatment.
Common Complications and Their Management
| Complication | Incidence | Description | Salvage/Management Strategy |
| Immediate/Acute Complications | ~1-5% | Pain/Swelling/Bruising: Due to vascular trauma. | Management: Rest, analgesia, RICE (Rest, Ice, Compression, Elevation). Reassurance. Ensure no progression to compartment syndrome. |
| Immediate/Acute Complications | Infrequent (~<1%) | Neurovascular Compromise: Swelling can rarely lead to nerve neuropraxia (e.g., AIN syndrome from distal radius fracture) or vascular compromise (very rare for buckle). Compartment Syndrome (extremely rare for buckle, but theoretical). | Management: Urgent removal of any restrictive dressing/brace. Close observation. If persistent deficit, emergent evaluation for possible intrinsic compartment syndrome or nerve decompression. Requires clear differentiation from initial presentation of neurovascular injury. |
Table: Common Complications and Management in Pediatric Forearm Fractures (including considerations for buckle fractures)
| Complication | Incidence (approx.) | Description & Relevance to Buckle Fractures | Salvage/Management Strategy |
|
Delayed Complications
|
~1-5%
|
Malunion/Deformity:
Due to instability (rare for buckle), inadequate immobilization, or underlying growth plate disturbance (rare). |
Management:
Non-symptomatic mild deformity often requires no specific intervention. Significant symptomatic malunion or progression of deformity requires corrective osteotomy. Typically not an issue with buckle fractures due to inherent stability. |
| |
~1-2%
|
Refracture:
Rare, usually due to premature return to high-impact activities or repeat trauma. |
Management:
Treat as a new fracture, usually with standard cast immobilization. |
|
Neurological Deficits:
Often transient following closed injury. Usually, specific nerve involvement rarely seen with buckle fracture directly. |
Rare
|
Post-traumatic stiffness:
While less likely with brace vs cast, stiffness can occur with extended immobilization. |
Management:
Early mobilization (once comfortable), physiotherapy/OT referral if persistent. Patient education on gentle, active ROM exercises. |
|
Minor Wound/Site Irritation:
|
~1-2%
| Skin irritation, blistering, pressure points from the brace or adhesive. |
Management:
Adjust brace fit, padding, skin care (e.g., emollients, gentle cleansing). If severe, temporary alternative immobilization (soft splint) might be considered. |
Non-specific Pain/Discomfort:
Most common "complication," especially in the initial days. |
Up to 10-15%
| Minor pain, soreness, tenderness not suggestive of serious pathology. Often exacerbated by movement or accidental bumps. |
Management:
Reassurance, simple analgesics (acetaminophen, ibuprofen), confirmation of proper brace fit, limited activity/protection. Pain typically subsides quickly within a week. |
Potential Challenges
- Undiagnosed Complete Fracture: While uncommon, if misdiagnosed as a buckle fracture, a truly unstable fracture can displace further. Careful radiographic review is critical.
- Velcro Brace Non-Compliance: Lack of proper instruction or poor compliance can lead to issues, but typically not severe complications for this inherently stable fracture.
- Unnecessary Restriction: The risk of over-treatment with casting is unnecessary economic burden, temporary impairment of daily activities, and potential psychological impact on the child.
- Patient/Parent Expectation: Some parents may perceive a brace as inadequate due to a lack of understanding of buckle fracture stability. Education is key.
Overall, buckle fractures are one of the most benign pediatric injuries, and serious complications are exceedingly rare with appropriate non-operative management. Emphasis should be on correct diagnosis, effective pain control, and avoiding unnecessary over-treatment.
Post-Operative Rehabilitation Protocols
As previously established, the management of a pediatric buckle fracture does not involve operative intervention. Consequently, there is no "post-operative" rehabilitation protocol in the traditional sense. Instead, the focus is on a structured "post-immobilization" or "recovery" protocol aimed at restoring full function rapidly, ensuring pain resolution, and preventing deconditioning or unnecessary apprehension. The inherent stability and rapid healing of buckle fractures mean that aggressive physical therapy is rarely, if ever, required.
Phases of Recovery and Functional Restoration
Phase 1: During Immobilization (First 3-4 Weeks with Velcro Wrist Brace)
-
Goals:
- Protect the healing fracture site.
- Control pain and swelling.
- Maintain range of motion in unaffected joints.
- Educate patient and parents on brace care and activity precautions.
-
Activities:
- Brace Wear: The Velcro wrist brace is worn continuously, day and night, for the prescribed duration (typically 3-4 weeks). It may be removed briefly for hygiene (e.g., showering/bathing), during which time the child should avoid stressing the wrist.
- Finger and Thumb Mobility: Encourage full, active, pain-free range of motion of the fingers and thumb frequently throughout the day. This prevents stiffness in unaffected joints and maintains distal circulation.
- Elbow and Shoulder Mobility: Encourage full, active range of motion of the elbow and shoulder to prevent stiffness and deconditioning of the entire upper extremity.
- Pain Management: As-needed over-the-counter analgesics (e.g., ibuprofen, acetaminophen).
- Activity Restrictions: Avoid contact sports, climbing, lifting heavy objects, or any activities that could put direct stress on the injured wrist. Light activities, such as writing or computer use, are generally permissible if pain-free.
- Warning Signs: Instruct parents to monitor for increased pain, swelling, numbness, tingling, or skin irritation and to contact the clinician if any of these occur.
Phase 2: After Brace Discontinuation (Typically Week 3-4 Onwards)
-
Goals:
- Achieve full, pain-free wrist range of motion.
- Restore normal grip strength and upper extremity function.
- Gradually return to pre-injury activities, including sports.
-
Activities:
- Brace Removal: At the designated follow-up (typically 3-4 weeks), the brace is discontinued. Clinical assessment is paramount; radiographs are generally not indicated at this stage for buckle fractures.
-
Active Range of Motion:
Immediately encourage active, pain-free wrist range of motion exercises. This includes:
- Wrist flexion and extension ("up and down")
- Radial and ulnar deviation ("side to side")
- Forearm pronation and supination ("turning palm up and down")
- Gentle circling motions
-
Strengthening (as tolerated):
- Squeezing a soft ball or putty for grip strength.
- Light weight-bearing activities as pain allows (e.g., pushing off a table).
- Functional activities: carrying light objects, dressing, personal care.
- Proprioception and Coordination: Engaging in activities that require fine motor control and coordination (e.g., drawing, building blocks for younger children, sports-specific drills for older children).
-
Return to Activity:
- Non-contact Sports/Light Play: Generally permissible once pain-free wrist motion and strength are nearly normal, typically within 1-2 weeks post-brace removal.
- Contact Sports/High-Impact Activities: A gradual return is recommended. Typically, 4-6 weeks from the time of injury (i.e., 1-3 weeks post-brace removal) is sufficient, provided there is full pain-free range of motion, normal strength, and no tenderness. A protective brace or wrap might be considered initially for sports, but is often not strictly necessary.
- Formal Physical Therapy: Referral to a physical or occupational therapist is rarely indicated for uncomplicated buckle fractures. The vast majority of children will regain full function with parent-supervised home exercises and gradual return to play. Persistent pain, stiffness, or parental apprehension are the primary indications for formal therapy.
Key Principles
- Early Motion: Encourage early, active, pain-free motion once the brace is removed. This capitalizes on the rapid healing of pediatric bone and minimizes stiffness.
- Listen to Pain: Pain should be the primary guide. Activities that cause sharp, significant pain should be avoided. Mild discomfort during range of motion is acceptable.
- Gradual Progression: Avoid sudden, high-impact activities. Progress gradually through weight-bearing and sport-specific movements.
- Reassurance: Reassure both the child and parents that buckle fractures heal quickly and completely, and long-term issues are highly improbable. This helps to overcome apprehension.
By following these simple, non-intensive recovery guidelines, children with buckle fractures typically achieve full, unrestricted function within 4-6 weeks of injury.
Summary of Key Literature / Guidelines
The optimal management of pediatric buckle fractures has evolved significantly over the past two decades, moving from rigid casting to more flexible immobilization strategies. This shift is strongly supported by a growing body of evidence emphasizing equivalent outcomes with reduced burden.
Key Findings and Recommendations from Literature:
-
Velcro Brace vs. Rigid Cast: Equivalent Outcomes:
- Multiple randomized controlled trials (RCTs) and systematic reviews have robustly demonstrated that management with a simple removable wrist brace or soft bandage yields outcomes equivalent to rigid plaster or fiberglass casts for distal radius buckle fractures.
- Meta-analyses (e.g., areas of research by Flynn et al., Boutis et al., and the BUCKLED Trial): These studies consistently report no significant differences in pain scores, functional outcomes (e.g., PRWE-P, PROMIS scores), complication rates (including refracture), or need for further intervention between brace and cast groups. Healing times are identical.
- Patient Preference: Studies often indicate a strong preference for braces by both children and parents due to improved comfort, ability to maintain hygiene, and ease of removal for brief periods.
- Cost-Effectiveness: Brace management can be more cost-effective due to reduced healthcare visits (no cast removal appointment), less material cost, and fewer cast-related complications.
-
Duration of Immobilization:
- The consensus in the literature supports a short duration of immobilization, typically 3-4 weeks . Given the rapid healing potential of pediatric bone, particularly for stable metaphyseal injuries, longer immobilization periods offer no additional benefit and may contribute to stiffness or deconditioning.
- Some studies have even explored shorter durations (e.g., 2 weeks) with good results, though 3-4 weeks remains the most common recommendation.
-
Role of Follow-up Radiographs:
- For unequivocally diagnosed, stable distal radius buckle fractures, routine follow-up radiographs at the time of immobilization removal are generally not indicated .
- Evidence suggests that clinical assessment alone is sufficient to confirm healing and allow for brace discontinuation. The inherent stability of these fractures means displacement after initial diagnosis is extremely rare. This reduces radiation exposure and healthcare costs.
-
Early Return to Activity:
- Given the excellent prognosis, a gradual return to activity, including sports, is encouraged once pain-free wrist motion and strength are restored, typically within 1-3 weeks after brace removal. Formal physical therapy is rarely necessary.
Relevant Guidelines and Consensus Statements:
- American Academy of Orthopaedic Surgeons (AAOS): While specific clinical practice guidelines (CPGs) for buckle fractures are limited, general principles for pediatric forearm fractures emphasize non-operative management for stable injuries and the importance of appropriate immobilization based on fracture stability.
- Pediatric Orthopaedic Society of North America (POSNA): Similar to AAOS, POSNA's general recommendations for distal radius fractures in children align with conservative management for stable, minimally displaced fractures, implicitly supporting less rigid immobilization for buckle fractures.
- Emergency Medicine and Pediatric Emergency Medicine Societies: Many emergency department protocols and guidelines now endorse removable brace management for buckle fractures, recognizing their benign nature and the efficiency benefits.
Summary:
The current academic consensus strongly supports the use of a Velcro wrist brace for 3-4 weeks for the vast majority of pediatric distal radius buckle fractures. This approach provides effective pain control and protection, is preferred by patients and parents, is cost-effective, and yields functional outcomes equivalent to more rigid casting, all while minimizing unnecessary radiation exposure and healthcare utilization. True operative intervention for buckle fractures is contraindicated. The "Velcro wrist brace is best" for pediatric buckle fractures is not just a preference, but an evidence-based standard of care.
Clinical & Radiographic Imaging

