Comprehensive Introduction and Patho-Epidemiology
Onychocryptosis, universally recognized in clinical parlance as an ingrown toenail, represents a pervasive, recurrent, and often debilitating condition encountered with high frequency across orthopedic, podiatric, and general surgical practices. The fundamental pathophysiology is characterized by the mechanical penetration of the lateral or medial edge of the rigid nail plate into the adjacent, highly innervated soft tissue of the lateral nail fold. This mechanical breach of the epidermal barrier incites a robust, cascading foreign-body inflammatory response. As the nail plate acts as a persistent irritant, the localized tissue undergoes profound edematous changes, secondary bacterial colonization (predominantly by Staphylococcus aureus and mixed skin flora), and the eventual formation of highly vascularized, hypertrophic granulation tissue that further engulfs the offending nail margin.
The epidemiological profile of onychocryptosis demonstrates a distinct bimodal distribution, though it overwhelmingly afflicts adolescents and young adults in their second and third decades of life. There is a documented male predominance, likely attributable to higher rates of hyperhidrosis, greater participation in high-impact athletic activities, and historically poorer adherence to proper nail hygiene. Extrinsic etiological factors include the utilization of restrictive, narrow-toe-box footwear, and improper nail trimming biomechanics—specifically, the aggressive excision of the lateral nail corners, which leaves a residual spicule that inevitably pierces the advancing paronychial tissue as the nail plate grows distally. Intrinsic factors such as a naturally incurvated nail plate (pincer nail deformity), disproportionately wide nail plates relative to the nail bed, and underlying biomechanical foot abnormalities (e.g., hallux valgus, overpronation) also significantly predispose patients to this condition.
While early-stage disease—manifesting primarily as localized erythema and mild hyperalgesia—may be successfully managed via conservative modalities such as warm water soaks, cotton wicking, and gutter splinting, refractory cases and advanced clinical presentations definitively necessitate surgical intervention. Historically, the evolution of surgical management for onychocryptosis has been fraught with high recurrence rates and unacceptable cosmetic morbidities resulting from complete nail avulsions without matrix extirpation. The paradigm shifted dramatically with the introduction of the partial nail plate and matrix removal technique, originally described by A.M. Winograd in 1929. Although Winograd’s seminal manuscript detailed a modest cohort of merely five patients, the fundamental anatomical logic of his procedure—sharp excision of the offending nail margin coupled with complete, targeted ablation of the underlying germinal matrix—established a new gold standard in operative care.
Clinically, the severity of onychocryptosis is most frequently stratified utilizing the Heifetz or Mozena classification systems. Stage I disease is characterized by localized inflammation, edema, and pain with applied pressure, devoid of frank purulence. Stage II introduces active infection, marked by seropurulent drainage and escalating erythema. Stage III is the most advanced, defined by chronic, indurated hypertrophy of the lateral nail fold, extensive exuberant granulation tissue, and profound functional impairment. The Winograd technique is particularly indicated and highly efficacious in late Stage II and Stage III disorders. Furthermore, it remains the definitive salvage procedure of choice following previous, unsuccessful partial or complete nail avulsions where recurrent, deeply embedded keratinous spicules have formed, rendering conservative or chemical ablation techniques inadequate.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the perionychial anatomy is an absolute prerequisite for the successful execution of any matrix ablation procedure. The nail unit is a complex, highly specialized appendage comprising the nail plate, the nail bed (which is subdivided into the sterile and germinal matrices), the eponychium (proximal nail fold), the paronychium (lateral nail folds), and the hyponychium (distal nail bed). The nail plate itself is a dense, keratinized structure that provides rigid dorsal protection to the distal phalanx and acts as a crucial counter-force mechanism during the biomechanical phases of toe-off in the normal gait cycle.
The germinal matrix represents the biological engine of nail plate production and is the primary anatomical target in the Winograd procedure. Histologically, it consists of rapidly dividing basal cells that undergo keratinization to form the substance of the nail plate. Anatomically, the germinal matrix extends proximally 5 to 8 mm beneath the eponychium, terminating distally at the lunula—the visible, crescent-shaped, opaque whitish area at the base of the nail plate. The most critical, and often most treacherous, anatomical features for the operating surgeon are the lateral horns of the germinal matrix. These horns curve deeply and proximally into the lateral cul-de-sacs of the proximal nail fold, extending significantly further laterally and proximally than the visible margins of the nail plate would suggest.
The vascular supply to the hallux nail unit is robust, derived from the proper plantar digital arteries, which course distally along the plantar-lateral and plantar-medial aspects of the digit. These vessels send perforating branches dorsally to form a rich, complex superficial arcade that supplies the matrix, nail bed, and surrounding folds. This intricate vascular network explains the profound bleeding encountered during sharp dissection of the matrix and underscores the absolute necessity of an effective digital tourniquet to achieve the bloodless field required for precise anatomical identification. Innervation is provided primarily by the proper plantar digital nerves, with supplementary contribution from the dorsal digital nerves. A comprehensive digital block must therefore achieve circumferential anesthesia to ensure complete patient comfort during the deep dissection required for matrix extirpation.
Biomechanically, the nail plate and its stabilizing soft tissue envelopes function synergistically. The nail plate firmly adheres to the underlying sterile matrix via longitudinal epidermal ridges, which prevent lateral subluxation of the plate during ambulation. When a partial matrixectomy is performed, the transverse width of the nail plate is permanently reduced. If the adjacent hypertrophic paronychial tissue is not adequately addressed or if the lateral nail fold is not properly reconstructed, the lack of lateral counter-pressure from the now-narrowed nail plate can lead to medial migration of the soft tissue, potentially predisposing the patient to future impingement, even in the absence of a recurrent nail spicule. Therefore, the surgical approach must respect not only the eradication of the matrix but also the postoperative biomechanical equilibrium of the toe.
Exhaustive Indications and Contraindications
The decision to proceed with a partial nail plate and matrix removal via the Winograd technique must be predicated on a rigorous evaluation of the patient's clinical presentation, vascular status, and history of prior interventions. The procedure is not a first-line treatment for mild, early-stage disease, but rather a definitive surgical solution for advanced, refractory, or recurrent pathology. Proper patient selection is paramount to avoiding catastrophic complications such as ischemic necrosis or chronic osteomyelitis, particularly in patients with compromised peripheral perfusion.
Absolute indications for the Winograd procedure include Stage II and Stage III onychocryptosis that has failed a dedicated trial of conservative management. It is the procedure of choice for patients presenting with chronic, recurrent ingrown toenails who have previously undergone simple nail avulsion without matrixectomy, a practice that historically yields recurrence rates approaching 70-80%. Furthermore, the presence of massive, fibrotic granulation tissue that physically obstructs the nail gutter and prevents the egress of purulent exudate necessitates the sharp excision and debridement inherent to the Winograd approach. In cases of severe pincer nail deformity where the lateral margins of the nail plate curl inward to pinch the underlying sterile matrix, bilateral partial matrixectomies may be indicated to permanently narrow the nail plate and relieve the mechanical impingement.
Contraindications must be meticulously respected. Absolute contraindications revolve primarily around vascular insufficiency. Patients with severe peripheral arterial disease (PAD), an Ankle-Brachial Index (ABI) of less than 0.5, or absent palpable pedal pulses accompanied by atrophic skin changes should not undergo elective matrix ablation, as the induced surgical trauma and the use of a digital tourniquet may precipitate digital gangrene. Similarly, patients with uncontrolled diabetes mellitus exhibiting profound microvascular disease and dense peripheral neuropathy are at extreme risk for non-healing surgical wounds and secondary deep-space infections. In such compromised hosts, conservative management or, if absolutely necessary, simple avulsion without tourniquet application or matrix destruction is the safer, albeit temporary, alternative.
Relative contraindications include active, fulminant cellulitis extending proximally beyond the metatarsophalangeal joint. While localized paronychia and purulence at the nail fold are expected and effectively treated by the removal of the offending nail spicule, profound ascending infection should ideally be cooled down with a short course of systemic antibiotics and elevation prior to elective matrixectomy. Additionally, patients with known bleeding diatheses or those on aggressive, unyielding anticoagulant therapy require careful perioperative optimization to prevent catastrophic postoperative hematoma formation within the tightly confined space of the nail fold.
| Clinical Parameter | Absolute Indications | Relative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Disease Stage | Stage III (Hypertrophic granulation) | Stage I with severe occupational impact | Ischemic digits (Severe PAD) | Active ascending cellulitis |
| Prior Treatment | Failed conservative management | Prophylactic for pincer nails | Uncontrolled Diabetes with poor microvasculature | Bleeding diatheses |
| Recurrence | Recurrent spicule post-avulsion | - | Raynaud's phenomenon (severe) | Immunocompromised state |
| Anatomical | Chronic fibrotic paronychia | - | Active osteomyelitis of distal phalanx | Non-compliant patient |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for a Winograd procedure begins with a comprehensive clinical evaluation of the affected extremity. The surgeon must meticulously assess the vascular status of the foot, documenting the presence and quality of the dorsalis pedis and posterior tibial pulses, as well as capillary refill time at the distal tuft of the hallux. Neurological assessment, utilizing a 10-gram Semmes-Weinstein monofilament, is critical to rule out underlying peripheral neuropathy, which could mask postoperative ischemic or infectious complications. Radiographic evaluation (AP, lateral, and oblique views of the hallux) is generally reserved for cases of chronic, long-standing infection to rule out underlying osteomyelitis of the distal phalanx, or to identify subungual exostoses that may be mimicking or exacerbating the clinical presentation.
Achieving profound anesthesia is the cornerstone of a successful and humane procedure. A traditional digital block is performed targeting the four digital nerves at the base of the proximal phalanx. The preferred anesthetic agent is a 50/50 mixture of 1% Lidocaine (for rapid onset) and 0.5% Bupivacaine (for prolonged postoperative analgesia). Traditionally, the use of epinephrine in digital blocks was strictly proscribed due to theoretical risks of irreversible vasospasm and digital ischemia. However, extensive modern literature and large-scale meta-analyses have unequivocally demonstrated the safety of epinephrine-containing local anesthetics in healthy patients without peripheral vascular disease. Nevertheless, in the context of a Winograd procedure where a mechanical tourniquet is utilized, plain local anesthetic remains the standard of care to avoid compounding ischemic insults.
A completely bloodless surgical field is an absolute, non-negotiable requirement for the sharp matrixectomy phase of the procedure. The germinal matrix presents as a pearly white, glistening tissue that is visually indistinguishable from adjacent subcutaneous fat, fibrous connective tissue, and periosteum in the presence of active bleeding. Exsanguination of the digit is achieved by elevating the toe and applying a sterile Penrose drain or a commercial digital ring tourniquet (e.g., T-Ring) tightly around the base of the proximal phalanx. The tourniquet must be secured with a hemostat to prevent slippage during the procedure. The surgeon must note the exact time of tourniquet inflation; while digital tourniquets are generally safe for up to 45-60 minutes, the procedure typically requires less than 20 minutes of ischemia time.
Patient positioning is straightforward but critical for surgical ergonomics. The patient is placed in the supine position on the operating table. The affected foot is positioned extending slightly beyond the distal edge of the table. This positioning allows the surgeon, who is typically seated at the foot of the table, unobstructed, 360-degree access to the digit. The surgical site is meticulously prepped with a broad-spectrum antiseptic solution (Chlorhexidine gluconate or Povidone-iodine), ensuring the solution penetrates the nail folds and the hyponychium. The foot is then draped in a standard sterile fashion, isolating the hallux while maintaining visualization of the distal foot to monitor overall perfusion status upon tourniquet release.
Step-by-Step Surgical Approach and Fixation Technique
Although "fixation" in orthopedic surgery typically implies the use of hardware for osteosynthesis, in the context of nail surgery, it refers to the definitive surgical extirpation of the offending tissue and the stabilization of the remaining nail fold to ensure optimal healing and biomechanical function. The surgical approach can be broadly divided into chemical ablation (phenol matrixectomy) and sharp excision (the classic Winograd procedure). Both techniques demand meticulous attention to anatomical detail.
Chemical Ablation (Phenol Matrixectomy)
While the classic Winograd procedure utilizes sharp dissection, chemical ablation using phenol is a highly effective, less invasive alternative for partial matrix removal, particularly in patients without massive hypertrophic granulation tissue. Phenol acts as a potent caustic agent that induces coagulative necrosis, denaturing cellular proteins and effectively destroying the germinal matrix cells.
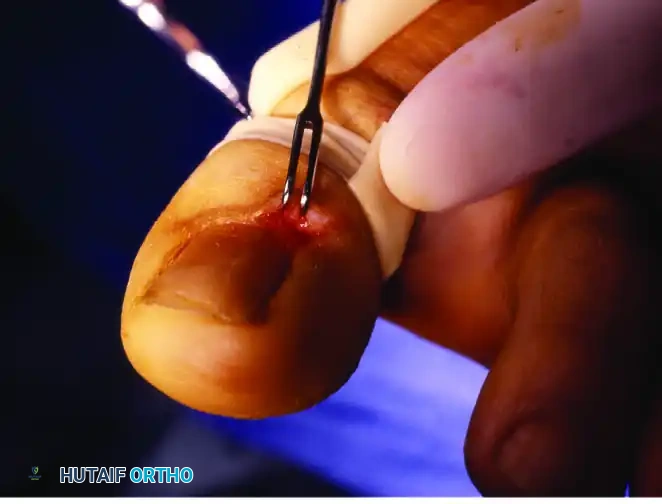
Step 1: Nail Elevation
The procedure commences with the blunt elevation of the offending lateral or medial nail edge. Using a small periosteal elevator, a Freer elevator, or a straight hemostat, the nail plate is gently separated from the underlying highly vascular sterile matrix. This longitudinal elevation must extend proximally under the eponychium to fully free the nail root.

Step 2: Tissue Protection
Phenol is a non-selective caustic agent; it will destroy any tissue it contacts. Therefore, protecting the surrounding healthy skin is paramount to prevent iatrogenic chemical burns. A protective barrier of antibiotic ointment or sterile petroleum jelly is meticulously applied around the eponychial and paronychial nail folds, isolating the surgical gutter.

Step 3: Phenol Application
An 88% phenol solution is the standard concentration utilized. A small, tightly wound cotton pledget or a specialized miniature applicator is dipped into the phenol solution. It is critical to express excess phenol to prevent spillage. The applicator is introduced deeply into the newly created nail groove, ensuring it reaches the absolute proximal and lateral extents of the germinal matrix beneath the eponychium.

The phenol is typically applied for three consecutive cycles, each lasting 30 to 60 seconds, with fresh phenol applied each time. Following the final application, the area must be thoroughly and vigorously lavaged with 70% isopropyl alcohol or sterile normal saline. This step is critical to neutralize the phenol, dilute its concentration, and wash away any residual caustic agent from the surgical site.

Step 4: Dressing Application
The ablated nail groove is packed with a nonadherent gauze (e.g., Adaptic or Xeroform) to prevent premature closure of the wound edges and allow for continued drainage of the expected serous exudate. A bulky, nonconstricting toe dressing is then applied to provide mechanical protection.

The final clinical appearance of the nail immediately following successful phenol ablation demonstrates a clear, widened lateral gutter completely devoid of the offending nail plate, with the surrounding soft tissue architecture preserved and protected from chemical injury.

The Winograd Procedure (Sharp Matrixectomy)
For severe, recurrent, or highly hypertrophic cases (Stage III), the sharp excision technique described by Winograd provides definitive, mechanical eradication of the matrix and allows for concurrent debridement of fibrotic tissue.
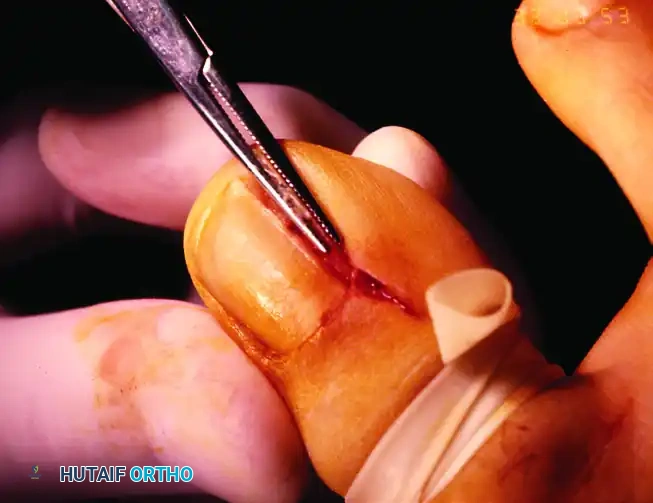
Phase 1: Incision and Exposure
The procedure begins with a precise longitudinal incision designed to expose the hidden proximal nail root and the underlying germinal matrix. Beginning approximately 5 to 8 mm proximal to the visible lunula, a full-thickness longitudinal incision is made through the eponychium, extending distally to the distal edge of the nail plate.

Using sharp dissection with a #15 blade or fine tenotomy scissors, the eponychial flap is carefully elevated and reflected laterally. This maneuver reveals the proximal nail root overlying the lateral margin of the germinal matrix. It is crucial that the remainder of the eponychium is left completely undisturbed to prevent unnecessary, permanent cosmetic deformity of the cuticle.
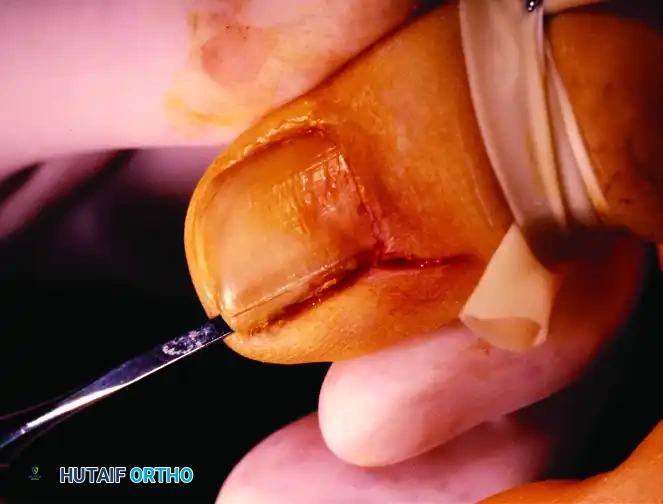
Phase 2: Nail Plate Mobilization and Splitting
Once the proximal root is fully exposed, the offending segment of the nail plate must be isolated. Using a small nasal elevator or a straight hemostat, the lateral border of the nail is lifted out of the paronychial fold. The instrument is passed proximally and distally beneath the lateral fourth of the exposed nail, completely separating it from the underlying sterile matrix.

To ensure a perfectly straight and controlled resection, the nail plate is scored longitudinally using a scalpel or the edge of the elevator to create a precise track for the splitter.
The nail margin is then incised along the scored mark utilizing a heavy-duty, double-action nail splitter or an English anvil. It is absolutely imperative that the lower jaw of the splitter is advanced fully to reach the most proximal edge of the nail plate beneath the reflected eponychial flap.
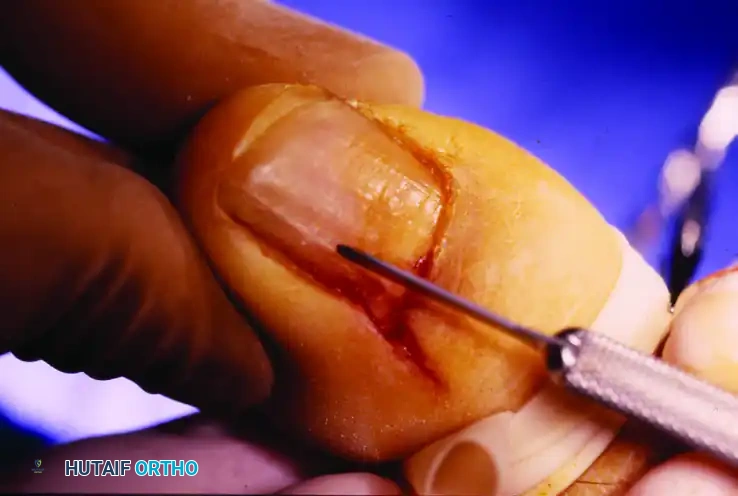
Phase 3: Extraction of the Nail Segment
With the eponychial cover reflected and the undersurface of the nail plate thoroughly separated from its bed, the isolated longitudinal segment is ready for complete extraction.

The isolated lateral segment of the nail is grasped firmly with a straight hemostat. The surgeon must gently remove this entire portion of the plate by applying a controlled, rolling motion toward the midline of the toe. Pulling straight distally or laterally risks tearing the proximal root, leaving a keratinous remnant deep within the fold.
Removal of the nail plate completely exposes the underlying matrix. The pearly, glistening colored germinal matrix will now be clearly visible in the bloodless field. The surgeon must carefully note how the matrix curves deeply onto the undersurfaces of the paronychium and eponychium.
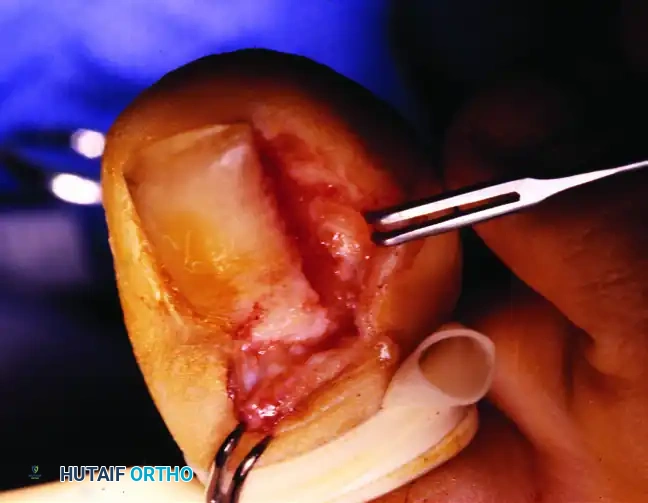
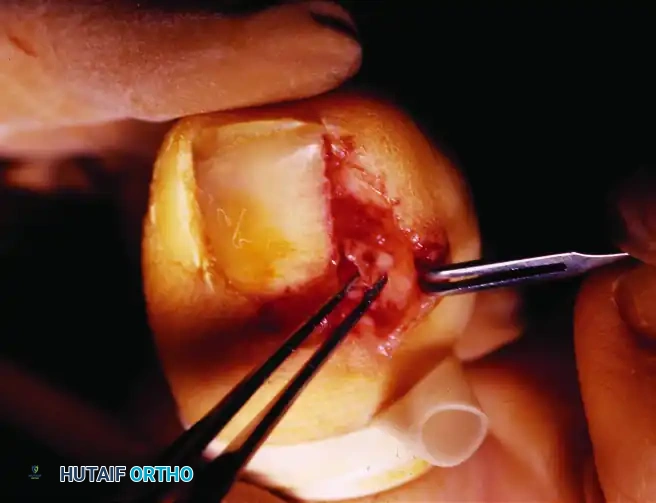
Phase 4: Matrix Ablation (The Critical Step)
The ultimate success of the Winograd procedure, and the prevention of recurrence, hinges entirely on the complete, aggressive eradication of the matrix in the affected gutter.

The exposed matrix is removed by meticulous sharp dissection using a #15 or a specialized #64 Beaver scalpel blade. The lateral nail fold must be forcefully retracted to fully expose the lateral margin of the matrix. The entire matrix—both the sterile portion in the distal bed and the germinal portion proximally—must be excised. Special, uncompromising care is taken to remove the proximal lateral horn of the germinal matrix. Because this tissue is intimately adherent to the underlying bone, complete ablation frequently requires the deliberate excision of the dorsal periosteum of the distal phalanx.
Phase 5: Closure and Dressing
Once the nail plate and matrix have been completely eradicated, and any hypertrophic granulation tissue excised, the surgical site is prepared for closure. The tourniquet is released, and meticulous hemostasis is achieved using direct pressure; electrocautery is generally avoided to prevent thermal necrosis of adjacent healthy matrix.
The proximal eponychial flap is returned to its original anatomical location. While suturing is technically optional and secondary intention healing is acceptable, closing the wound with 1 or 2 simple interrupted sutures (using 4-0 or 5-0 Nylon) generally shortens convalescence, improves immediate postoperative hemostasis, and yields a superior cosmetic result.


