INTRODUCTION TO FEMORAL NECK FRACTURE OUTCOMES
Femoral neck fractures remain one of the most challenging injuries in orthopedic traumatology, historically dubbed the "unsolved fracture." Despite advancements in implant design, intraoperative imaging, and biological understanding, internal fixation of the femoral neck is associated with a uniquely high complication profile. The precarious retrograde blood supply to the femoral head, combined with the immense shear forces acting across the fracture site, creates a biomechanically and biologically hostile environment for bone healing.
As a consultant orthopedic surgeon, anticipating, recognizing, and managing these complications is paramount. The primary adverse outcomes following internal fixation include failure of fixation, clinically significant femoral neck shortening, nonunion, osteonecrosis (avascular necrosis), and deep postoperative infection. Determining the exact etiology of a complication is the critical first step in formulating a successful revision strategy.
FAILURE OF INTERNAL FIXATION
Internal fixation may fail due to a confluence of mechanical and biological factors. The most common culprits include inadequate anatomical reduction, poor implant selection, suboptimal implant positioning, unrecognized nonunion, osteonecrosis, and occult infection.
Biomechanics of Fixation Failure
Failure typically manifests as varus collapse, retroversion of the femoral head, or hardware cutout. The femoral neck is subjected to massive compressive and shear forces during physiological loading. If a fracture is left in varus or retroversion during the index procedure, the resultant joint reaction forces will drive the hardware through the cancellous bone of the femoral head, leading to catastrophic cutout.
Surgical Warning: A non-anatomical reduction, particularly one leaving the fracture in varus or retroversion, is the single greatest predictor of early fixation failure. Accept nothing less than an anatomical or slightly valgus reduction.
Management Strategies Based on Patient Demographics
Determining the root cause of fixation failure dictates the salvage pathway:
- Young, Physiologically Active Patients: Early recognition of inadequate reduction or poor implant positioning demands immediate revision open reduction and internal fixation (ORIF). If the failure is recognized late and has progressed to a nonunion or malunion, a valgus-producing intertrochanteric osteotomy is the gold standard to redirect shear forces into compressive forces.
- Elderly or Low-Demand Patients: Revision internal fixation in the geriatric population carries an unacceptably high failure rate due to osteopenia and compromised healing potential. Femoral neck nonunion, malunion, hardware cutout, and osteonecrosis in this demographic are definitively treated with conversion to a Total Hip Arthroplasty (THA) or, in highly selected frail patients, a bipolar hemiarthroplasty.
FEMORAL NECK SHORTENING AND IMPLANT SELECTION
Historically, the paradigm for treating femoral neck fractures involved using partially threaded cannulated screws to allow for dynamic compression across the fracture site. While compression promotes primary bone healing, excessive sliding leads to significant femoral neck shortening.
The Pathophysiology of Shortening
Significant shortening alters the biomechanics of the hip joint by decreasing femoral offset. This reduces the lever arm of the hip abductors (gluteus medius and minimus), resulting in abductor weakness, a persistent Trendelenburg gait, increased energy expenditure, and diminished patient-reported outcome measures (PROMs).
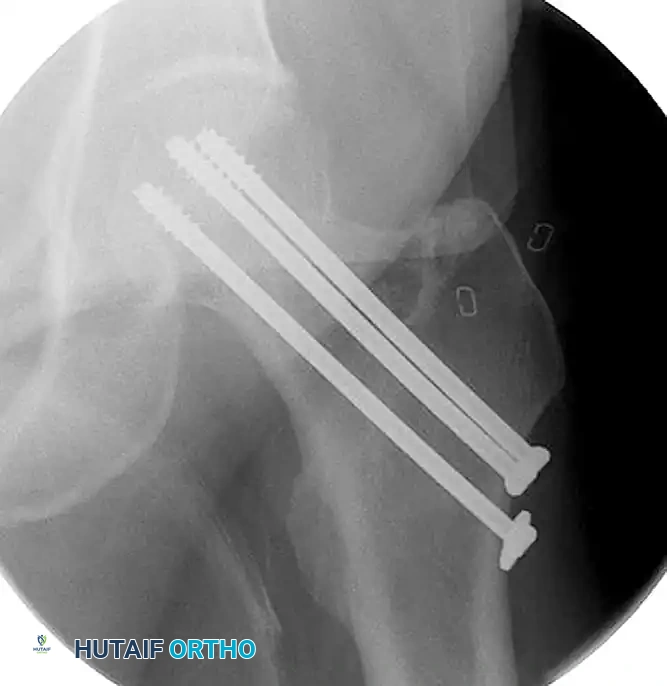
Figure 55-15A: Intraoperative fluoroscopic anteroposterior view demonstrating the initial fixation of a minimally displaced femoral neck fracture utilizing three partially threaded cannulated screws.
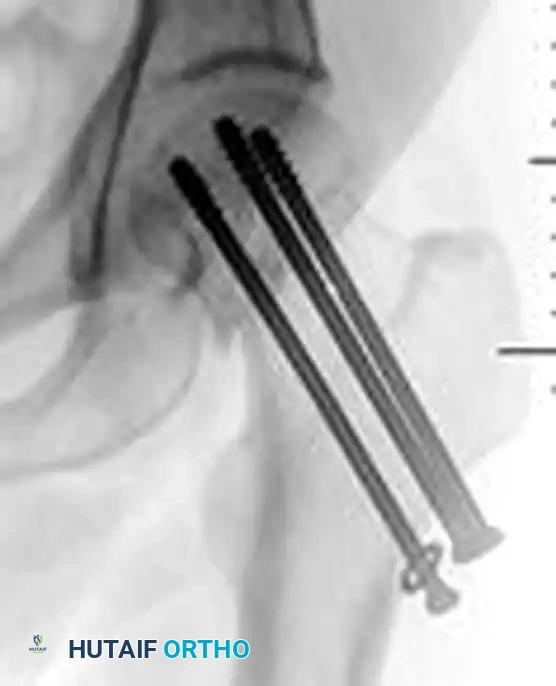
Figure 55-15B: Postoperative anteroposterior radiograph revealing significant femoral neck shortening. The dynamic compression allowed by the partially threaded screws has resulted in a loss of femoral offset and abductor lever arm.
Strategies to Minimize Shortening
To mitigate the risk of excessive shortening, modern osteosynthesis principles emphasize length-stable constructs, particularly in young patients where functional outcomes are paramount.
- Fully Threaded Screws: In an attempt to minimize femoral neck shortening, a partially threaded screw used for compression can be exchanged for, or augmented with, a fully threaded screw. Fully threaded screws act as position screws, maintaining length and preventing further collapse once initial compression is achieved.
- Fixed-Angle Devices: For vertically oriented fracture patterns (Pauwels Type III) or basicervical variants, a Sliding Hip Screw (SHS) or Dynamic Hip Screw (DHS) with a derotation screw provides superior biomechanical stability against shear forces compared to multiple cancellous screws.

Figure 55-16A: Preoperative radiograph at the time of injury demonstrating a displaced femoral neck fracture with significant biomechanical instability.

Figure 55-16B: Postoperative anteroposterior radiograph after operative reduction and fixation utilizing a fixed-angle sliding hip screw construct to provide controlled collapse while resisting excessive varus deformity.

Figure 55-16C: Postoperative lateral radiograph confirming central placement of the lag screw within the femoral head, optimizing the tip-apex distance (TAD).
NONUNION AND MALUNION
Nonunion of the femoral neck occurs in up to 15-30% of displaced fractures treated with internal fixation. It is defined as a lack of radiographic progression of healing at 6 months post-injury, accompanied by persistent groin or thigh pain.
Valgus Intertrochanteric Osteotomy
In young, active patients with a viable femoral head, a valgus intertrochanteric osteotomy is the procedure of choice for nonunion.
- Biomechanical Rationale: The osteotomy alters the mechanical axis of the proximal femur. By resecting a laterally based wedge of bone from the intertrochanteric region, the femoral neck is placed into valgus. This converts the deleterious shear forces (Pauwels III) at the nonunion site into favorable compressive forces (Pauwels I), stimulating osteogenesis.
- Surgical Technique: The procedure is performed via a lateral approach. Preoperative templating is critical to determine the exact angle of the wedge to be resected. Fixation is typically achieved using a fixed-angle blade plate or a proximal femoral locking plate.
Clinical Pearl: When performing a valgus osteotomy, ensure that the resultant mechanical axis does not create excessive valgus at the knee. Concomitant advancement of the greater trochanter may be necessary to restore abductor tension if significant shortening has occurred.
OSTEONECROSIS (AVASCULAR NECROSIS)
Osteonecrosis (AVN) is a devastating complication resulting from the disruption of the delicate blood supply to the femoral head, primarily the lateral epiphyseal branches of the medial circumflex femoral artery (MCFA). AVN can occur in up to 30% of displaced fractures and 10% of nondisplaced fractures.
The Role of Intracapsular Tamponade
While the initial trauma undoubtedly tears retinacular vessels, secondary ischemia can occur due to an intracapsular hematoma. The hip capsule is a robust, unyielding structure. Bleeding from the fracture site accumulates within the joint, exponentially raising intracapsular pressure. If this pressure exceeds the capillary perfusion pressure of the remaining intact vessels, a tamponade effect occurs, leading to irreversible ischemia of the femoral head.
Capsulotomy: Indications and Technique
To mitigate the risk of tamponade-induced osteonecrosis, decompression of the hip joint via capsulotomy is a critical consideration.
- Young Patients: We routinely perform open or percutaneous capsulotomies in young patients with both displaced and nondisplaced femoral neck fractures. The preservation of the native femoral head is of utmost importance in this demographic.
- Geriatric Population: Capsulotomy is only occasionally performed in the elderly. The biological healing potential is lower, and the threshold for converting to an arthroplasty is much lower if AVN develops.
- Evidence Base: Although there is no universally conclusive, large-scale randomized controlled trial proving that capsulotomy definitively decreases the frequency of osteonecrosis, the biomechanical rationale is sound. It can be performed quickly and safely, and the potential benefit of reducing AVN risk far outweighs the minimal surgical morbidity.
Surgical Technique for Capsulotomy: A percutaneous capsulotomy can be performed using a long Kelly clamp or a Cobb elevator passed anterior to the femoral neck under fluoroscopic guidance. Alternatively, an open anterior approach (Smith-Petersen) allows for direct visualization, hematoma evacuation, and precise anatomical reduction of the fracture.
POST-TRAUMATIC INFECTION
Deep infection following the internal fixation of femoral neck fractures is a catastrophic complication that can be quite problematic to eradicate. The presence of avascular bone (the femoral head) and metallic implants creates an ideal environment for bacterial biofilm formation.
Treatment Algorithm for Infection
The management of postoperative infection depends on the chronicity of the infection, the stability of the fixation, and the status of fracture healing.
- Acute Infection with Stable Hardware: If the infection is recognized early (within 3-4 weeks of the index surgery) and the hardware remains rigidly fixed, the goal is to suppress the infection. This requires aggressive surgical débridement, copious irrigation, and the administration of culture-specific intravenous antibiotics. The hardware is maintained to allow for fracture union. Once clinical and radiographic union is achieved, the hardware is electively removed to eradicate any residual biofilm.
- Chronic Infection or Hardware Failure: Hardware failure in the presence of deep infection is an absolute indication for immediate hardware removal. The necrotic bone must be radically excised.
- Salvage Procedures: In cases of infected nonunion with hardware failure, a resection arthroplasty (Girdlestone procedure) may be required to clear the infection. Once inflammatory markers (ESR, CRP) have normalized and joint aspirates are sterile, a staged conversion to a Total Hip Arthroplasty can be considered, often utilizing antibiotic-loaded cement spacers in the interim.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of femoral neck fracture fixation relies heavily on strict adherence to postoperative rehabilitation protocols.
- Weight-Bearing Status: For young patients treated with multiple cannulated screws or an SHS, weight-bearing is typically restricted to toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB) for 6 to 8 weeks to prevent early varus collapse. In elderly patients, immediate weight-bearing as tolerated (WBAT) is often permitted to prevent the complications of prolonged recumbency (atelectasis, deep vein thrombosis, decubitus ulcers), accepting a higher risk of mechanical failure.
- Thromboembolic Prophylaxis: Chemical prophylaxis (e.g., Low Molecular Weight Heparin or Direct Oral Anticoagulants) combined with mechanical prophylaxis is mandatory for a minimum of 28 to 35 days postoperatively, as pelvic and hip trauma carries a profound risk for deep vein thrombosis (DVT) and pulmonary embolism (PE).
- Radiographic Surveillance: Serial radiographs (AP and cross-table lateral) should be obtained at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year. The surgeon must meticulously evaluate for signs of varus subsidence, screw back-out, loss of joint space, or subchondral sclerosis indicative of impending osteonecrosis. Early detection of these radiographic signs allows for timely intervention before catastrophic clinical failure occurs.
