-
- Exogenous: most common osteomyelitis in adults
- Acute osteomyelitis from open fracture or bone exposed at surgery
- Chronic osteomyelitis from neglected wounds: diabetic feet, decubitus ulcers
- Hematogenous: most common osteomyelitis in children
- Pediatric patients
- Immature immune system
- Metaphysis or epiphysis of long bones
- Lower extremity more often than upper
- Adult patients
- Immunocompromised (elderly, undergoing chemotherapy transplant recipient)
- Vertebrae most common adult hematogenous site
- Patient undergoing dialysis—rib and spine osteomyelitis
- IV drug abuser—medial or lateral clavicle osteomyelitis
- Acute osteomyelitis
- Short duration, usually less than 2 weeks
- Symptoms include tenderness, limb, refusal to use limb
- Fever and systemic symptoms variable
- Laboratory findings:
- CRP—most sensitive test (increased in ≈97%)
-
Most rapid rise and fall
—good measure of treatment success - ESR—increased in approximately 90%
- CBC—WBCs increased in only a third
-
Aspiration and biopsy cultures—
most specific test - Histopathology: bony spicules with live osteocytes surrounded by inflammatory cells
- Treatment
-
6 weeks of antibiotics directed at specific organisms identified by culture
Source of Bite | Organism | Primary Antimicrobi Regimen | ---|---|---| Human | Streptococcus viridans(100%)
Bacteroides spp. (82%)
Staphylococcus
epidermidis
(53%)
Corynebacterium
spp. (41%)
Staphylococcus aureus(29%)
Peptostreptococcus
spp.
Eikenella spp.
| Early treatment (no amoxicillin/clav (Augmentin)
With signs of infect ampicillin/sulba cefoxitin, ticarc (Timentin), or p tazobactam
Patients with penic clindamycin pl ciprofloxacin or trimethoprim/s Eikenella organism clindamycin, na
metronidazole, first-generation and erythromy to fluoroquinol trimethoprim/s treated with cef ampicillin Dog | Pasteurella canis
S. aureus Bacteroides spp.
Fusobacterium
spp.
Capnocytophaga
spp.
| Amoxicillin/clavula (Augmentin) or (adults); clinda trimethoprim/s (children)
P. canis is resistant t cephalexin, clin erythromycin
Antirabies treatme considered
Only 5% of dog bit become infecte Cat | Pasteurella
multocida
| Amoxicillin/clavula cefuroxime axe Table 1.33 Bite Injuries | S. aureus
Possibly
tularemia
| doxycycline Cephalexin should
P. multocida is resis doxycycline, ce clindamycin; m resistant to eryt
Of cat bite wounds infected; cultur
| ---|---|---| Rat | Streptobacillus moniliformis
Spirillum minus
| Amoxicillin/clavula doxycycline Antirabies treatme
indicated Pig | Polymicrobial (aerobes and anaerobes)
| Amoxicillin/clavulanat generation cephalo ticarcillin/clavulana ampicillin/sulbacta cilastatin Skunk, raccoon, bat | Varies
| Amoxicillin/clavula doxycycline Antirabies treatme Pit viper (snake) | Pseudomonas spp.
Enterobacteriaceae
S. epidermidis Clostridium spp.
| Antivenin therapy Ceftriaxone Tetanus prophylaxi Brown recluse spider | Toxin
| Dapsone Catfish sting | Toxins (may become secondarily infected)
| Amoxicillin/clavulanat
Adapted from Gilbert DN et al: The Sanford guide to
antimicrobial therapy, Hyde Park, VT, 2010, Antimicrobial Therapy, p 48. - Surgery is reserved for draining abscesses or failure to improve on antibiotics.
- Subacute osteomyelitis : Brodie abscess 1. Residual of acute osteomyelitis versus hematogenous seeding of growth plate trauma
- Painful limp with no systemic signs
- Adolescent to early adult (<25 years)—stronger immune system
-
Localized radiolucency with sclerotic rim at
metaphysis of long bones - Almost exclusively S. aureus (may be lower virulence)
- Treatment: surgical débridement and 6 weeks of IV antibiotics
- Rule out tumors (chondroblastoma): “ Biopsy all infections, culture all tumors.”
- Chronic osteomyelitis
- History
- Prior trauma/surgery or soft tissue wound
- Previous acute osteomyelitis or septic arthritis
- Should be considered in all nonunions
- Often chronic wound or draining sinus
- Laboratory findings
- Less helpful, can be normal
- Open bone biopsy/culture best test (sinus tract cultures not helpful)
- Histopathology
- Dead bone (avascular) (osteocytes have no nuclei)
- Fibrosis of marrow space
- Chronic inflammatory cells
- Treatment
- Surgery required for chronic osteomyelitis
- Basic principles
- Multiple procedures frequently required
- Removal of infected hardware
- Removal of dead bone, which serves as a “foreign object”
- Débridement of bone until punctate bleeding is restored (“paprika sign”)
-
Débridement of compromised or
necrotic soft tissue - Consideration of preoperative sinus tract injection with methylene blue
- Consideration of antibiotic spacers: PMMA cement versus biologics
- Restoration of vascularity or soft tissue muscle coverage
- Six weeks of antibiotics directed at specific cultures
- Adequate minimal inhibitory concentration (MIC) of antibiotics at site of infection
- Host classification (Cierny-Mader; Table 1.34)
- A: healthy
- B: wound healing comorbidities
- BL (local): compromised vascularity
Table 1.34 Chronic Osteomyelitis: Infected Host Types Type Description Risk --- A | Normal immune response; nonsmoker
| Minimal B | Local or mild systemic deficiency; smoker
| Moderate C | Major nutritional or systemic disorder
| High
1. Arterial disease, venous stasis, irradiation, scarring,
smoking
4. BS (systemic): compromised immune system
1. Diabetes mellitus, malnutrition, end-stage renal disease, malignancy, alcoholism, rheumatologic diseases, immunocompromised status
1. HIV,
immunosuppressive therapy, DMARDs
5. BL/S (combined local and systemic)
6. C: compromised patient (palliative care or amputation)
1. No quality-of-life improvement if cured
2. Morbidity of procedure exceeds that of the disease.
3. Poor prognosis, poor cooperation with care
7.
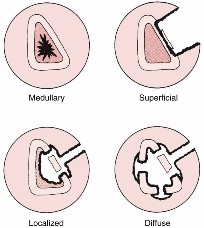
Anatomic lesion classification (
Fig. 1.50)
1. #### I: medullary—nidus endosteal
1. Residual hematogenous or intramuscular infected nonunion
2. Treatment: unroofing
2. #### II: superficial—infection on surface defect of coverage
1. Full-thickness soft tissue wounds: venous stasis/pressure ulcer
2. Treatment: decortication and soft tissue coverage
3. #### III: localized—cortical infection without loss of stability
1. Infected fracture union with butterfly fragment or prior plate
2. Treatment: sequestrectomy, soft tissue coverage, with or without bone graft
4. #### IV: diffuse—permeative throughout bone, unstable before or after débridement
1. Periprosthetic infection, septic arthritis or infected nonunions
2. Treatment: stabilization, soft tissue coverage, and bone graft
8. Imaging of osteomyelitis
1. Radiographs
1. Acute osteomyelitis
1. Soft tissue swelling (early)

---
FIG. 1.50 Cierny’s anatomic classification of adult chronic osteomyelitis.
2. Bone demineralization or regional osteopenia (≈2 weeks after infection)
2. Chronic osteomyelitis
1. Periosteal reaction, cortical erosions, bony lucency, and sclerotic changes
2. Bony lysis around hardware and prosthetic joints
3. #### Sequestra—dead bone nidus with surrounding granulation tissue
4. #### Involucrum—periosteal new bone forming later
2. #### MRI best method to show early osteomyelitis and anatomic location
1. Penumbra sign
1. Bright signal in surrounding bone
2. Darker abscess and sclerotic bone
2. Negative finding rules out osteomyelitis
3. Positive finding may overestimate extent of disease
3. Fluorodeoxyglucose positron emission
tomography (FDG-PET)
1. Shows malignancies and infections: increased glycolysis
2. Most sensitive test for chronic osteomyelitis
3. More specific than MRI or bone scan
9. Empiric treatment for osteomyelitis prior to definitive culture findings
1. Newborn (up to 4 months of age)
1.
S. aureus, gram-negative bacilli, and group B streptococci
1. Nafcillin or oxacillin plus a third-generation cephalosporin
2. If MRSA: vancomycin plus a third-generation cephalosporin
2. Children 4 months of age or older
1.
S. aureus and group A streptococci
1. Nafcillin or oxacillin versus vancomycin (MRSA)
2. Immunization has almost eliminated
Haemophilus influenzae
bone infections.
3. Adults (21 years of age or older)
1.
S. aureus
10. Antibiotic spacers/beads
1. Nafcillin or oxacillin versus vancomycin (MRSA)
1. Provide very high antibiotic levels at local area
2. 2–4 g per bag (40 g) of cement (>2 g reduces compressive strength)
3. Pouch can be formed and covered with adherent film.
4. Antibiotics must be heat stable.
1. Cephalosporins, aminoglycosides, vancomycin, clindamycin
2. Antibiotics inactivated by heat must be avoided
1. Tetracycline, fluoroquinolones, polymyxin B,
chloramphenicol
5. Antibiotics elute out over 2–6 weeks.
1. Elution increased with
1. Surface area— beads
2. Higher porosity
—vacuum mixing should not be used.
3. Larger antibiotic crystals— cement should be mixed until doughy, then antibiotics added.
4. Atypical or unusual organisms
1. ####
Salmonella
osteomyelitis—sickle cell
1. Microinfarcts of bone and bowel
2. Spleen dysfunction
3. Bone crisis versus diaphyseal osteomyelitis
2.
Pseudomonas osteomyelitis
1. IV drug abuse and osteomyelitis of medial/lateral clavicle
2. Puncture wounds through rubber/synthetic shoes
3. TB osteomyelitis
1. One-third of the world is infected with TB.
2. One-third of TB in pediatric and HIV-positive patients is extrapulmonary.
3. Spine most common: Pott disease (spinal gibbus)
4. One-fourth of extrapulmonary TB is in hips and knees.
5. Often involves bones on both side of joint
4. Fungal osteomyelitis
1. Long-term IV medications or parental nutrition
5. Treatment
1. Immunosuppression by disease or drugs (RA, transplantation)
2.
Candida —most common; is part of normal flora
3.
Aspergillus —rare in bone
4. Regional varieties—via inhalation or direct inoculation
5.
Coccidioides —southwest United States to South America
6.
Histoplasma —soil and bird/bat guano, Ohio and Mississippi river valleys
7.
Blastomyces —rotting wood, central southeastern United States
8.
Cryptococcus —pigeon droppings, northwest United States/Canada
9. Débridement of osteonecrosis, resection of sinuses and/or synovitis
10. Antifungals: amphotericin
1. Chronic regional multifocal osteomyelitis (CRMO) (also chronic nonbacterial osteomyelitis [CNO])
1. Children/adolescents with multifocal bone pain but no systemic symptoms
2. Exacerbations and remissions, more than 6 months of pain
3. Autoinflammatory disease; a diagnosis of exclusion
4. No abscess, fistula, or sequestrum
5. Laboratory findings: WBC count normal; ESR, CRP may be elevated
6. X-rays demonstrate multiple metaphyseal lytic or sclerotic lesions.
7. Whole-body spin tau inversion recovery (STIR) MRI more sensitive
8. Culture results negative—antibiotics do not help
9. Histologic findings
1. Early: PMNs and osteoclasts
2. Later: lymphocytes, fibrosis, and reactive bone
1. Especially in the
