Comprehensive Introduction and Patho-Epidemiology
The nomenclature surrounding osteochondral lesions of the talus (OLT) has historically been fraught with ambiguity, reflecting an evolving understanding of their etiology and natural history. Terms such as osteochondritis dissecans, osteochondral fracture, transchondral fracture, and talar dome fracture have been used interchangeably in the literature. However, the modern orthopedic consensus recognizes that these lesions represent a continuum of osteochondral injury, predominantly driven by acute trauma or chronic microtrauma, rather than a primary inflammatory or spontaneous necrotic process. The historical timeline of OLT recognition provides critical context for modern management. In 1888, König coined the term osteochondritis dissecans to describe loose bodies in the knee, theorizing spontaneous bone necrosis as the primary driver. By 1922, Kappis recognized the morphological similarities between knee lesions and those in the ankle joint. It was not until 1959 that Berndt and Harty conducted their exhaustive review and cadaveric study, definitively concluding that "osteochondritis dissecans" of the talus is, in reality, a trauma-induced transchondral fracture. They established the foundational four-stage classification system that remains a cornerstone of orthopedic education today.

Osteochondral lesions of the talus account for approximately 4% of all osteochondral lesions in the human body; however, this figure likely underestimates the true incidence significantly. Advanced imaging studies and arthroscopic evaluations suggest that OLTs may occur in up to 50% of acute ankle sprains and fractures, particularly within athletic and high-demand military populations. A significant clinical challenge is the initial misdiagnosis and subsequent delay in appropriate management. Nearly 50% of OLTs are missed on initial emergency department radiographs, frequently dismissed as simple, uncomplicated "ankle sprains." This delay can lead to progressive subchondral cystic changes, fragment detachment, and accelerated early-onset osteoarthritis.

While a definitive history of trauma is documented in over 85% of patients, Flick and Gould demonstrated a distinct anatomical variance in traumatic etiology that dictates the morphological pattern of the lesion. They found that 98% of lateral lesions were associated with a definitive history of trauma, whereas only 70% of medial lesions had a clear traumatic antecedent. This discrepancy suggests that while lateral lesions are almost exclusively acute shear fractures, medial lesions may develop from a combination of acute trauma, chronic repetitive microtrauma, and localized vascular insufficiency. Other proposed, though statistically less common, etiologies include localized osteonecrosis, systemic vasculopathies, endocrine or metabolic factors, underlying joint malalignment (such as varus hindfoot alignment increasing medial compartment contact pressures), and genetic predispositions affecting cartilage matrix integrity.

Detailed Surgical Anatomy and Biomechanics
A profound understanding of talar dome anatomy and ankle joint biomechanics is an absolute prerequisite for the surgical management of OLTs. The talus is a unique osseous structure; roughly 60% to 70% of its surface is covered by articular cartilage, and it serves as the critical intercalary segment transmitting the entire weight of the body from the tibial plafond to the foot. The talar dome is trapezoidal, being wider anteriorly than posteriorly. This anatomical configuration dictates that the talus is highly constrained within the ankle mortise during dorsiflexion, providing maximal bony stability, but is relatively unconstrained during plantarflexion, relying heavily on the lateral ligamentous complex (anterior talofibular and calcaneofibular ligaments) for stability.
The articular cartilage of the talar dome is distinct from that of the knee. It is significantly thinner (averaging 1.0 to 1.5 mm compared to the knee's 2.0 to 3.0 mm) but possesses a higher compressive stiffness and a different proteoglycan composition. This unique extracellular matrix makes the talar cartilage more resilient to the immense compressive forces of weight-bearing but potentially less capable of intrinsic repair following shear injury. The blood supply to the talus is notoriously tenuous, lacking direct muscular or tendinous attachments. It relies entirely on an extraosseous arterial ring formed by the anterior tibial, posterior tibial, and peroneal arteries, which give rise to the artery of the tarsal canal, the deltoid branches, and the artery of the sinus tarsi. The subchondral bone of the talar dome is supplied by terminal end-arteries, rendering it highly susceptible to localized avascular necrosis following microvascular disruption from shear trauma.

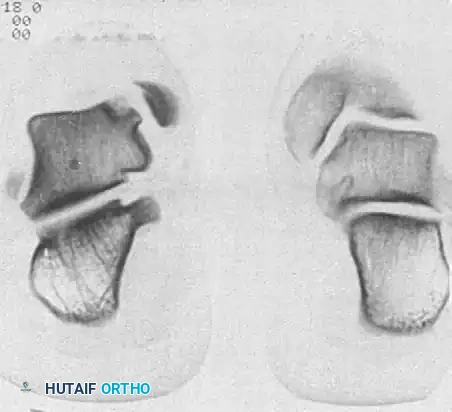
The anatomical location of the lesion dictates its morphological characteristics and the underlying mechanism of injury, famously summarized by the mnemonic DIAL and PIMP (though variations exist). Medial talar dome lesions are statistically more common. The mechanism of injury typically involves plantar flexion, inversion, and lateral rotation of the tibia on the talus. These lesions are typically located on the posterior-medial aspect of the dome. Morphologically, they are deep, cup-shaped, and usually non-displaced, remaining stable within their subchondral crater. Conversely, lateral talar dome lesions result from inversion combined with strong dorsiflexion. They are typically located on the anterior-lateral aspect of the dome. Morphologically, they are shallow, wafer-shaped, and highly prone to displacement, frequently generating mechanical symptoms such as catching and locking within the joint.
Exhaustive Indications and Contraindications
Treatment algorithms for osteochondral lesions of the talus are highly nuanced and must be individualized. The decision-making process is dictated by patient age, skeletal maturity, activity level, lesion size, anatomical location, morphological stability, and the presence of subchondral cystic changes. Accurate staging using both CT and MRI is paramount for guiding these treatment algorithms.
Conservative Management
Non-operative treatment is generally indicated for incomplete medial and lateral lesions (Stage II), completely detached but undisplaced medial lesions (Stage III), and almost all lesions occurring in skeletally immature patients with open physes. The standard protocol involves immobilization in a short-leg cast or a strict non-weight-bearing controlled ankle motion (CAM) boot for 4 to 6 weeks, followed by progressive weight-bearing and physical therapy focusing on peroneal strengthening and proprioceptive recovery. However, the orthopedic surgeon must be acutely aware of the surgical warning: literature indicates that non-operative management of chronic, cystic talar lesions yields successful outcomes in only 45% to 54% of cases. Prolonged conservative treatment in displaced or highly symptomatic lesions is contraindicated as it may lead to progressive, irreversible degenerative joint disease.
Operative Management
Surgical intervention is strictly indicated for all displaced lesions (Stage IV), completely detached lateral lesions (Stage III) due to their high non-union rate and propensity for displacement, and any lesion failing 4 to 6 months of rigorous conservative therapy. The choice of surgical procedure is heavily dependent on the cross-sectional area of the lesion, typically using a cutoff of 1.5 cm² or 15 mm in diameter, as well as the depth of subchondral bone involvement.
| Surgical Procedure | Primary Indications | Absolute/Relative Contraindications |
|---|---|---|
| Arthroscopic Debridement & Microfracture | Primary lesions < 1.5 cm²; Intact subchondral plate; Failed conservative care. | Lesions > 1.5 cm²; Massive subchondral cysts; Diffuse osteoarthritis; Uncorrected instability. |
| Retrograde Drilling & Bone Grafting | Intact articular cartilage with underlying subchondral cyst; Skeletally immature patients. | Breached/unstable articular cartilage; Lesions requiring structural support. |
| Osteochondral Autograft Transfer (OATS) | Lesions > 1.5 cm²; Failed prior microfracture; Deep cystic lesions requiring structural bone graft. | Diffuse kissing lesions; Advanced age (>50 years is relative); Knee pathology (if harvesting from knee). |
| Autologous Chondrocyte Implantation (ACI) | Large, uncontained lesions > 2.0 cm²; Failed primary marrow stimulation techniques. | Uncorrected malalignment; Severe joint space narrowing; Inability to comply with strict rehab. |
| Internal Fixation of Fragment | Acute, large (>1.5 cm²), structurally intact osteochondral fragments (typically lateral). | Chronic, fragmented, or avascular loose bodies; Small wafer fragments unable to hold fixation. |
Pre-Operative Planning, Templating, and Patient Positioning
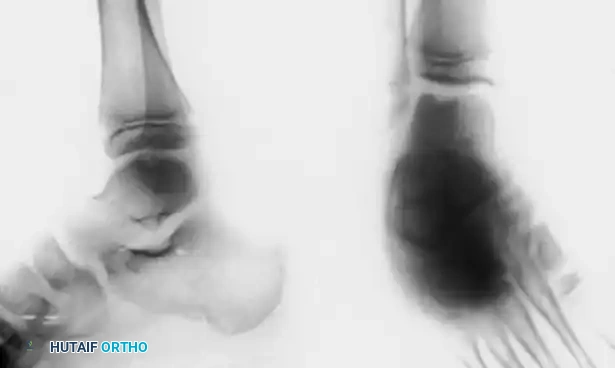
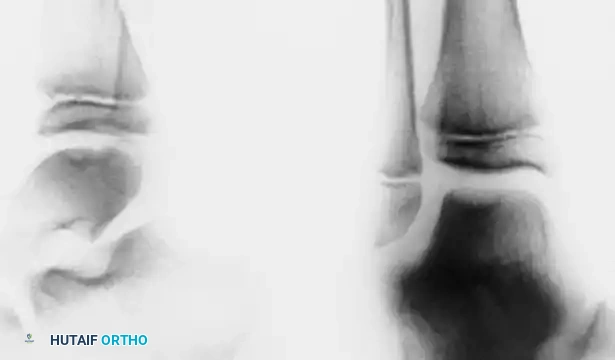
Pre-operative planning is the most critical phase in the surgical management of OLTs. The surgeon must synthesize clinical examination findings with advanced imaging to precisely map the lesion's topography. Standard anteroposterior (AP), lateral, and mortise radiographs often fail to isolate the lesion due to tibial overlap. Oblique and plantar flexion views are mandatory to profile the talar dome.

Advanced Imaging Protocols
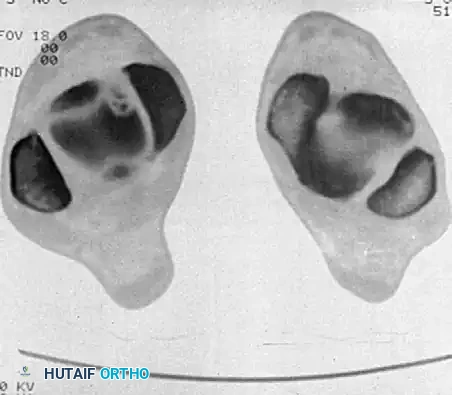
If radiographs are negative but clinical suspicion remains high, advanced imaging is required. Computed Tomography (CT) utilizing 2-mm cuts in both axial and coronal planes is the gold standard for defining the osseous architecture, exact size, location, and the presence of subchondral cysts. CT is indispensable for preoperative templating, specifically to determine if a medial malleolar osteotomy is required for access to a posterior-medial lesion. Magnetic Resonance Imaging (MRI) is the modality of choice for evaluating the integrity of the articular cartilage and identifying early (Stage I) lesions characterized solely by bone marrow edema. MRI is highly sensitive for detecting synovial fluid interposition between the fragment and the talar bed, which is a definitive indicator of mechanical instability.
Patient Positioning and Setup
For arthroscopic procedures, the patient is typically positioned supine on the operating table with a thigh tourniquet applied. The operative leg is placed in a dedicated leg holder or allowed to hang freely over the edge of the bed if a lateral decubitus position is preferred by the surgeon. A non-invasive ankle distractor utilizing a sterile strap around the hindfoot and midfoot is highly recommended to open the anterior joint space, as the tight congruency of the ankle mortise makes visualization challenging. Invasive skeletal distraction via a calcaneal pin is rarely necessary today due to advancements in small-joint arthroscopy instruments. The surgeon must mark the superficial peroneal nerve branches, the dorsalis pedis artery, and the saphenous vein prior to insufflation to avoid iatrogenic injury during portal placement.


Step-by-Step Surgical Approach and Fixation Technique
Surgical strategies fall into three broad categories: Debridement and Marrow Stimulation, Direct Repair (Fixation), and Cartilage Restoration. The approach is dictated by the precise mapping obtained during preoperative CT imaging.
Arthroscopic Debridement and Microfracture
For lesions smaller than 1.5 cm², arthroscopic excision of the fragment, curettage of the necrotic base, and marrow stimulation (microfracture) remains the gold standard primary intervention.
1. Portal Placement: Standard anteromedial (medial to the tibialis anterior tendon) and anterolateral (lateral to the peroneus tertius) portals are established. A 2.7-mm or 4.0-mm 30-degree arthroscope is utilized.
2. Diagnostic Sweep: A thorough diagnostic arthroscopy is performed. The lesion is identified and probed. The Cheng et al. arthroscopic classification is utilized to grade the cartilage integrity.
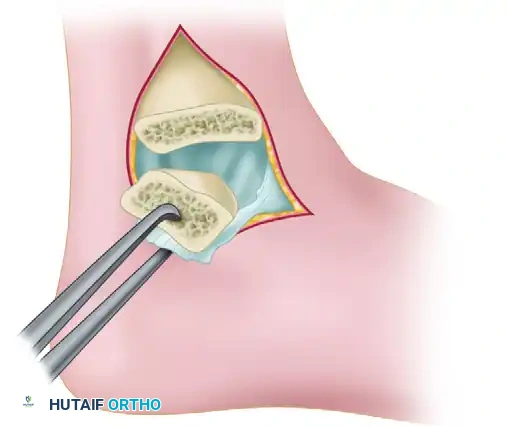
3. Debridement: Unstable cartilage flaps and the loose osteochondral fragment are excised using arthroscopic biters and shavers.
4. Curettage: The sclerotic base of the crater is aggressively curetted using ring curettes until healthy, bleeding punctate subchondral bone is encountered. It is imperative to maintain vertical walls (the "containment rim") around the defect to hold the subsequent super-clot.
5. Microfracture: An arthroscopic awl (typically 45-degree or 60-degree) is used to create holes 3 to 4 mm apart and 4 to 5 mm deep into the subchondral plate. The goal is to penetrate the subchondral bone to release marrow elements, including mesenchymal stem cells, which will form a fibrocartilage repair tissue (Type I and Type III collagen mix). The tourniquet is deflated to confirm marrow egress (fat droplets and blood) from the microfracture holes.

Retrograde Percutaneous Drilling and Bone Grafting
For early lesions with intact overlying cartilage but significant subchondral cystic changes, retrograde drilling preserves the articular surface while stimulating healing.
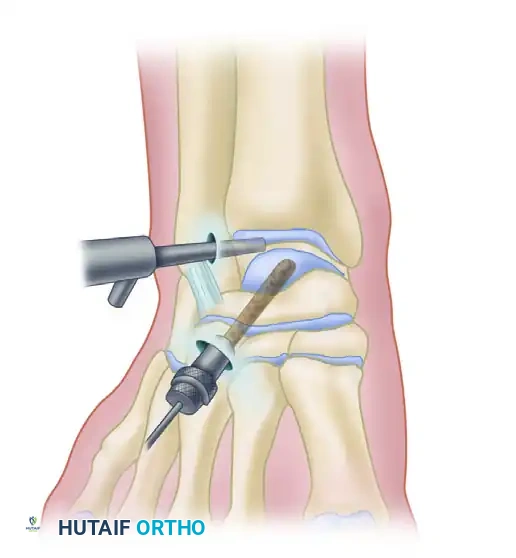
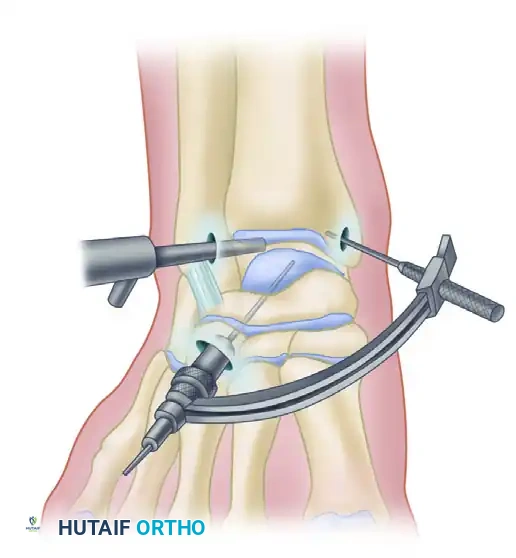
1. Targeting: Under arthroscopic visualization, the intact articular cartilage is confirmed. A modified anterior cruciate ligament (ACL) drill guide is placed through the anterolateral portal, targeting the exact center of the lesion.
2. Drilling: A guide pin is advanced percutaneously from the sinus tarsi (for medial lesions) or the medial talar neck (for lateral lesions) into the subchondral cyst, stopping 1 to 2 mm short of the articular cartilage.
3. Fluoroscopic Confirmation: Intraoperative C-arm fluoroscopy confirms the trajectory and depth in multiple planes.
4. Decompression and Grafting: The tract is over-drilled using a cannulated drill bit. The cystic contents are curetted. To prevent articular collapse, the void is backfilled. Options include cancellous autograft from the distal tibia, surgical-grade calcium sulfate, or bone marrow aspirate concentrate (BMAC) harvested from the iliac crest.
Open Medial Malleolar Osteotomy and Cartilage Restoration (OATS)
When large (>1.5 cm²), posterior-medial lesions require structural grafting (Osteochondral Autograft Transfer System) or direct fixation, an open approach via medial malleolar osteotomy is strictly required for perpendicular access.
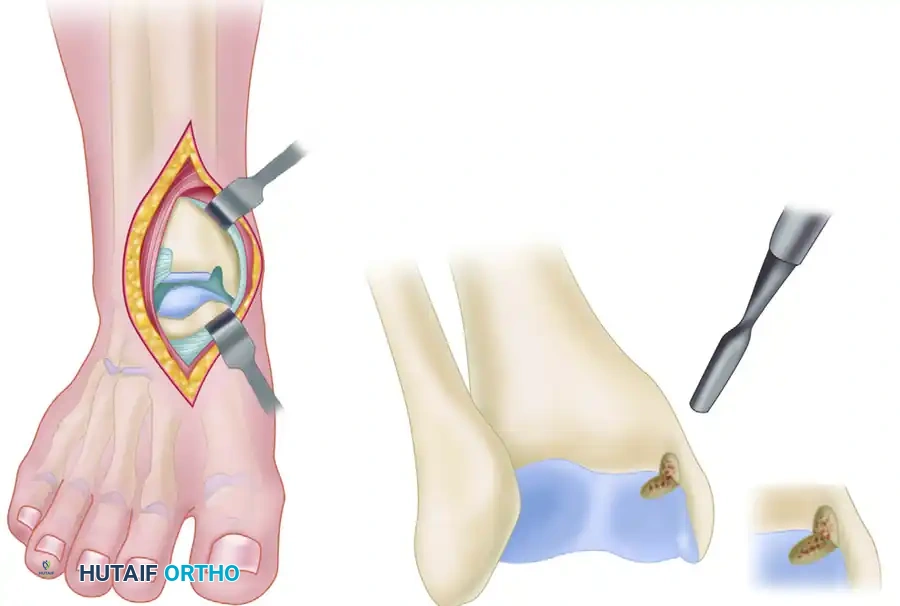
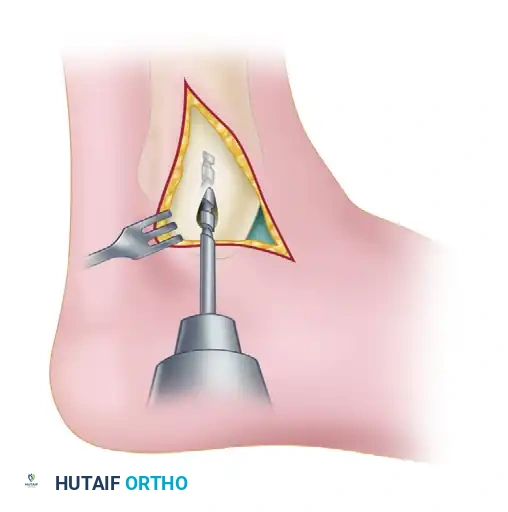
1. Incision and Exposure: A longitudinal incision is made over the medial malleolus, protecting the saphenous vein and nerve. The periosteum is incised, and the anterior and posterior borders of the malleolus are defined.
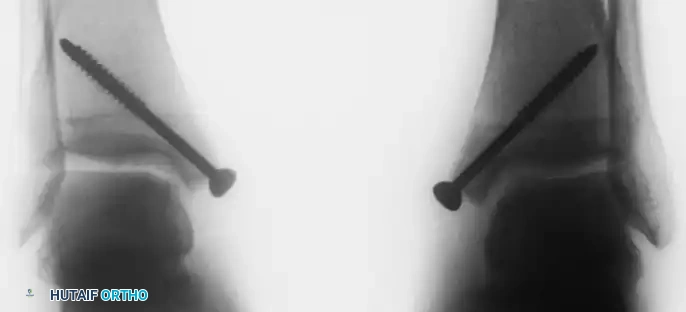
2. Pre-drilling: This is a crucial step. Before the osteotomy is made, two parallel holes are drilled from the tip of the medial malleolus proximally into the tibial metaphysis. These are tapped and measured for 4.0-mm partially threaded cancellous screws. This ensures perfect, anatomical reduction during closure.
3. Osteotomy: A chevron-type (V-shaped) osteotomy is performed using a fine-toothed oscillating saw, directed toward the axilla of the medial clear space. The osteotomy is completed with a thin osteotome to preserve bone dust and create a rough, interdigitating surface for optimal healing.
4. Exposure: The medial malleolus is reflected inferiorly on its intact deltoid ligament hinge, exposing the posterior-medial talar dome.
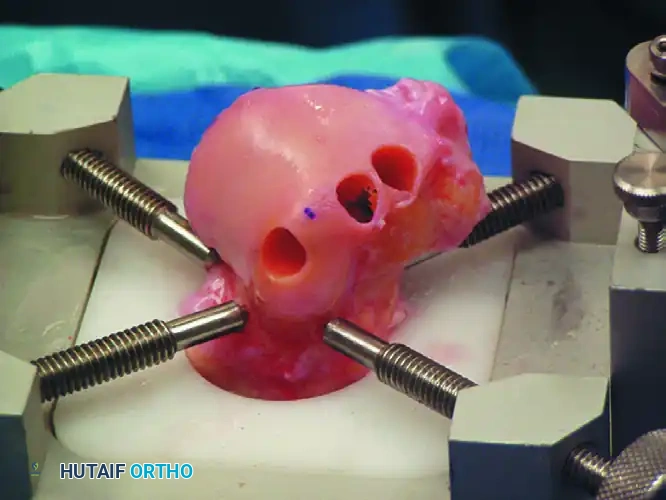
5. Lesion Management (OATS): The lesion is sized. A recipient socket is cored out of the talus to a specific depth (typically 12-15 mm). A matching osteochondral plug is harvested from a non-weight-bearing portion of the ipsilateral knee (e.g., the lateral periphery of the lateral femoral condyle) and press-fit into the talar defect, ensuring the cartilage cap is perfectly flush with the surrounding native talar cartilage.
6. Closure: The malleolus is reduced, the pre-drilled holes are aligned, and the two 4.0-mm cancellous screws are inserted, achieving rigid interfragmentary compression.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of OLTs carries inherent risks. The avascular nature of the talar dome, combined with the high mechanical demands of the ankle joint, predisposes patients to several specific complications. The surgeon must be prepared to manage these effectively.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Medial Malleolar Non-union | 1% - 3% | Thermal necrosis from saw; Inadequate fixation; Smoking. | Revision open reduction internal fixation (ORIF) with autologous bone grafting. |
| Symptomatic Hardware | 10% - 15% | Prominent screw heads at the medial malleolus. | Hardware removal after radiographic confirmation of osteotomy union (typically >6 months). |
| Subchondral Cyst Recurrence | 15% - 20% | Failure of microfracture fibrocartilage; Fluid tracking into subchondral plate. | Revision surgery with structural grafting (OATS or bulk allograft) to restore subchondral support. |
| Progressive Osteoarthritis | 20% - 30% (Long-term) | Large initial lesion size; Uncorrected hindfoot malalignment; Chronic instability. | Joint-preserving osteotomies (supramalleolar); Ankle arthrodesis; Total Ankle Arthroplasty (TAA) in older patients. |
| Iatrogenic Nerve Injury | 2% - 5% | Superficial peroneal nerve injury during anterolateral portal placement. | Prevention via careful portal mapping; Neuroma excision if conservative management fails. |
Salvage management for massive, uncontained lesions or failed primary cartilage restoration procedures is highly complex. In cases where the subchondral bone loss is extensive, fresh bipolar osteochondral allografts may be utilized to reconstruct the entire talar shoulder. However, in cases of diffuse degenerative joint disease secondary to a failed OLT, the surgeon must pivot from joint preservation to joint sacrifice. Ankle arthrodesis remains the gold standard for pain relief in young, high-demand laborers, while Total Ankle Arthroplasty is increasingly indicated for older, lower-demand patients seeking to maintain sagittal plane motion.
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol must be strictly tailored to the specific surgical intervention performed. The biological requirements for fibrocartilage maturation (post-microfracture) differ vastly from the requirements for osseous integration of a structural graft (post-OATS or medial malleolar osteotomy).
Phase I: Maximum Protection and Biological Healing (Weeks 0-6)
For microfracture procedures, the primary goal is to protect the delicate mesenchymal super-clot while stimulating chondrocyte differentiation through motion. Patients are placed in a posterior splint for 3 to 5 days to allow portals to heal, followed by transition to a CAM boot. They are strictly non-weight-bearing (NWB) for 4 to 6 weeks. However, early, aggressive active and passive range of motion (ROM) exercises are initiated out of the boot multiple times daily. The mechanical shear of joint motion is essential for organizing the fibrocartilage matrix.
For OATS procedures or cases involving a medial malleolar osteotomy, the ankle is immobilized in a short-leg cast or locked CAM boot. Weight-bearing is strictly prohibited to prevent graft subsidence or osteotomy displacement. ROM exercises are delayed until radiographic evidence of early osteotomy consolidation is observed, typically around 4 weeks.
Phase II: Progressive Loading and Strengthening (Weeks 6-12)
Once the initial biological healing phase is complete, patients begin a progressive weight-bearing protocol. This typically starts with 25% body weight using crutches, advancing by 25% every 4 to 7 days until full weight-bearing is achieved. Physical therapy intensifies, focusing on closed-kinetic-chain exercises. Isotonic and isokinetic strengthening of the peroneal, tibialis posterior, and gastrocnemius-soleus complexes is paramount to restore dynamic ankle stability. Proprioceptive training using wobble boards and BAPS (Biomechanical Ankle Platform System) boards is initiated to retrain mechanoreceptors disrupted during the initial injury and subsequent surgery.
Phase III: Return to Sport and High-Demand Activity (Months 3-6+)
Return to high-impact activities, running, and cutting sports is generally not permitted until 4 to 6 months post-operatively. Criteria for return to sport include full, painless range of motion, resolution of all joint effusions, and isokinetic strength testing demonstrating at least 90% strength compared to the contralateral, uninjured limb. Patients must be counseled that maximal medical improvement, particularly regarding deep aching after strenuous activity, may take up to 12 to 18 months as the subchondral bone continues to remodel.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of osteochondral lesions of the talus is heavily guided by landmark literature that has shaped modern clinical algorithms. The foundational work by Berndt and Harty (1959) remains the bedrock of OLT understanding, definitively linking the pathology to trauma and establishing the radiographic staging system.
In the modern era, the work by Chuckpaiwong et al. (2008) is arguably the most clinically significant regarding surgical indications. Their retrospective review of 105 patients undergoing microfracture demonstrated a distinct precipice in clinical outcomes based on lesion size. They found that microfracture yielded excellent results in lesions smaller than 1.5 cm², but the failure rate approached 97% for lesions larger than 1.5 cm². This study effectively established the 1.5 cm² threshold that currently dictates the transition from marrow stimulation to structural cartilage restoration techniques like OATS or ACI.
Furthermore, systematic reviews by Zengerink et al. (2010) evaluated the success rates of various treatment modalities. They concluded that bone marrow stimulation (microfracture) provides successful clinical outcomes in 85% of primary, appropriately sized lesions, solidifying its place as the primary workhorse procedure. However, for lesions failing primary microfracture, structural grafting (OATS) demonstrated superior outcomes compared to repeat microfracture.
Current clinical guidelines from the American Orthopaedic Foot & Ankle Society (AOFAS) emphasize a stepwise approach: exhaustive non-operative management for stable lesions, arthroscopic marrow stimulation for primary lesions under 1.5 cm², and structural autograft/allograft reconstruction for massive, cystic, or revision scenarios. The integration of advanced orthobiologics, such as Bone Marrow Aspirate Concentrate (BMAC) and Platelet-Rich Plasma (PRP) as adjuncts to microfracture, represents the current frontier of research, aiming to improve the histological quality of the repair tissue from Type I fibrocartilage to more durable Type II hyaline-like cartilage. Future textbook iterations will undoubtedly focus on these biological augmentations as long-term outcome data matures.
