Orthopedics Hand Review | Dr Hutaif Hand & Wrist Review -...
Updated: Feb 2026
50 Views
Key Medical Takeaway
Looking for accurate information on Orthopedics Mcqs Hand0019? Based on the question of figures, a 43-year-old bricklayer’s left hand weakness, atrophy, positive Froment sign, and ulnar nerve motor denervation distal to the wrist, without sensory loss, points to ulnar nerve motor branch compression. MRI reveals a ganglion cyst near the hook of the hamate compressing this branch. The best next step is excision of the ganglion cyst.
Table of Contents
Score: 0%
Orthopedics Mcqs Hand0019
QUESTION 1
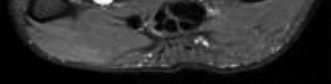
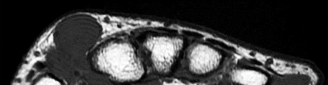
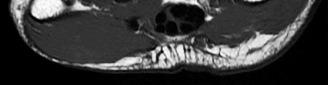
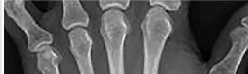
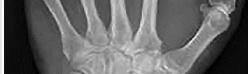
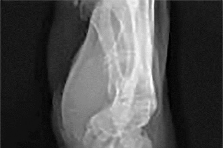
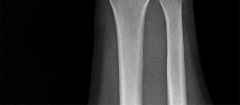
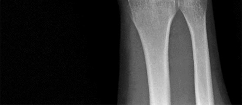
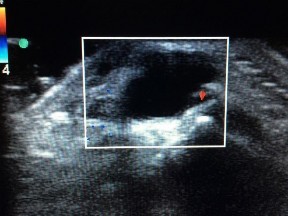
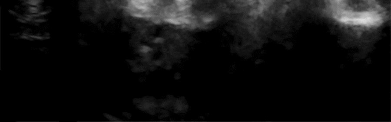
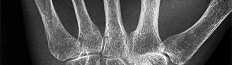
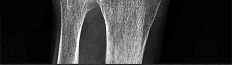
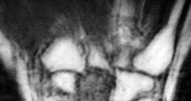
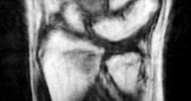
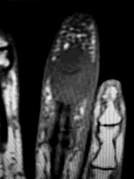
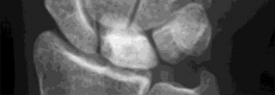
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step? --- ---
1
Cubital tunnel release
2
Guyon's canal release
3
Hook-of-hamate excision
4
Excision of the ganglion cyst
The MR images show a lesion consistent with a ganglion cyst located near the hook of the hamate. The ulnar nerve divides into motor and sensory branches just proximal to this lesion. In this case, the ganglion cyst compresses the ulnar nerve motor branch but not the sensory branch, resulting in motor dysfunction but no sensory disturbance. Excision of the ganglion cyst should alleviate his symptoms. Compression of the ulnar nerve proximal to the motor branch take-off (in either the cubital tunnel or proximal Guyon’s canal) would cause both sensory and motor dysfunction. Although chronic nonunion of the hook of the hamate can cause ulnar nerve symptoms, the hook of the hamate appears intact on the MR image. The MR image shows a lesion that is well circumscribed with high intensity on T1 and T2 images, consistent with a benign ganglion cyst, and ganglion cysts are relatively common lesions in this area.
QUESTION 2
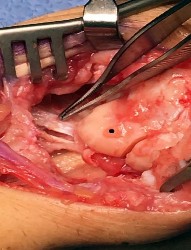
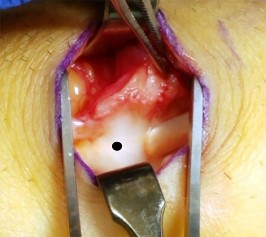
Figure 1 depicts an intraoperative photograph obtained following proximal row carpectomy. The black dot denotes the capitate. The top of the figure is radial and the bottom of the figure is ulnar. Surgical disruption of the structure identified by the forceps would result in ---
1
loss of active thumb interphalangeal (IP) flexion.
2
distal radioulnar joint instability.
3
avascular necrosis of the capitate.
4
ulnar carpal translocation.
The structure identified by the forceps is the radioscaphocapitate ligament. During a proximal row carpectomy, it is very important to identify and protect this ligament. Compromise of the ligament would result in ulnar translocation of the carpus and early failure of the proximal row carpectomy procedure. If the ligament is injured during surgery, immediate repair should be performed. Green and associates discuss the importance of the radioscaphocapitate ligament in stabilizing the carpus after this procedure is performed. Nakamura and associates compared 3-mm, 6-mm, and 10-mm radial styloidectomies, and only the 3-mm styloidectomy subsequently preserved carpal stability. Compromise of the radioscaphocapitate ligament occurred when larger portions of the radial styloid were excised. Distal radioulnar joint instability would result only from the disruption of the distal radioulnar joint stabilizers. Avascular necrosis would not occur, because the capitate receives its blood supply mainly from the palmar vessels. Finally, loss of active thumb IP flexion would not occur, because the flexor pollicis longus tendon would remain intact even if ligament compromise were to occur.
QUESTION 3
A 51-year-old male 2-pack per day smoker presents with a hyperkeratotic light brown plaque on the dorsum of his left ring finger that has been present for 7 years. It measures 14 mm by 13 mm. Initially, it responded to topical wart treatments, but has failed to do so recently so he sought evaluation by a dermatologist who biopsied the lesion. The results revealed squamous cell carcinoma (SCC) in situ, and he was referred for further surgical management. He has no other skin lesions, no history of SCC and no axillary lymphadenopathy. What is the next step in management?
1
Continued observation and re-evaluation in 6 months
2
Sentinel lymph node biopsy
3
Wide excision
4
Primary ray resection
SCC in situ is a low-grade malignancy that typically presents as painless lesions on areas of high sun exposure such as the dorsum of the hand and fingers. The recommended treatment for lesions smaller than 100 mm is wide excision with 4 mm margins to a depth 1 layer below the tumor, along with any adjacent area of induration. Sentinel lymph node biopsy is typically not indicated in the setting of a low-grade tumor such as this one and in the absence of axillary lymphadenopathy.
QUESTION 4
Figures 1 and 2 are the radiographs of a 36-year-old right-hand-dominant man who has had persistent wrist pain for 6 months after a motor vehicle collision. The initial treatment was splint immobilization. What is the best next step? ---
1
Therapy/rehabilitation
2
Open reduction and internal fixation (ORIF)
3
Proximal row carpectomy
4
Wrist arthrodesis
This patient has a chronic untreated volar lunate dislocation. Lunate dislocations are usually the result of a high-energy injury. Recommended treatment for an acute lunate dislocation is ORIF with repair of injured structures (ligament and bone). If the patient has paresthesias in a median nerve distribution, carpal tunnel release is recommended in the same setting as ORIF. Six months after injury, the prognosis for successful ORIF is poor and proximal row carpectomy is recommended. Among perilunate/lunate dislocations, 25% are initially missed. If a patient arrives for treatment and there is evidence of radiocarpal _and midcarpal arthrosis, wrist arthrodesis is recommended._
QUESTION 5
A 54-year-old laborer has a 6-month history of lateral elbow pain. An elbow examination reveals full range of motion, tenderness over the lateral epicondyle, and pain with resisted wrist extension with the elbow in extension. Elbow radiograph findings are normal. You perform a steroid injection and the patient's symptoms are decreased 6 weeks later. One year after receiving the injection, this patient—when compared to a patient who did not have a steroid injection—is likely to
1
have no difference in elbow pain.
2
no longer have elbow pain.
3
need surgery.
4
experience tendon rupture.
This patient has signs and symptoms of lateral epicondylitis. Treatments include various forms of physical therapy, iontophoresis, corticosteroid injection, nitroglycerin patch treatment, blood injections, prolotherapy, and surgical intervention. No single treatment is superior to other treatments for this common problem. Several studies have demonstrated a short-term decrease in symptoms following steroid injection (6 weeks) but an increased likelihood of persistent symptoms 1 year after treatment. Steroid injection at this site has not been associated with increased risk for tendon rupture or need for _surgical intervention._
QUESTION 6
A 50-year-old patient underwent multiple débridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
1
free vascularized fibula.
2
calcium sulfate pellets.
3
corticocancellous autograft.
4
demineralized bone matrix.
The patient developed a large bone defect after undergoing multiple débridements for an open fracture. The most appropriate graft in this setting is a vascularized bone graft. Considering the length of the defect, a free vascularized fibular graft would be a suitable graft. The indications for a vascularized bone graft include infection, inadequate vascularity of the surrounding tissues, bone defects larger than 6 centimeters, and previous failed bone grafts. The osteocytes survive in the vascularized graft, allowing primary bone healing and thereby limiting a loss of graft strength. In contrast, nonvascularized bone graft heals by creeping substitution with a loss of its initial strength. Calcium sulfate pellets and calcium phosphate cement are synthetic bone substitutes with osteoconductive properties. Their role in fracture healing is limited. Demineralized bone matrix is the matrix remaining after allograft undergoes decalcification processing. These products alone would not be optimal in the treatment of such a large bone defect.
QUESTION 7
Figures 1 through 3 demonstrate the radiographs obtained from a 45-year-old construction worker who
has wrist pain, loss of motion, and loss of strength. Nonsurgical measures have failed, and the patient requests surgery. What is the best surgical option for this patient? --- --- ---
1
Proximal row carpectomy
2
Excision of the proximal pole of the scaphoid
3
Bone grafting with fixation of the scaphoid
4
Scaphoid excision with four-corner fusion
This patient has a physically demanding occupation. His radiographs show a long-standing nonunion with avascular necrosis and collapse of the proximal pole. This condition is referred to as a scaphoid nonunion advanced collapse wrist (SNAC). He has advanced arthritis of the capitolunate joint, but the radiolunate joint is preserved. The best option for him would be scaphoid excision with four-corner fusion. Proximal row carpectomy, would be incorrect because of the advanced arthritis of the capitolunate joint. This procedure relies on normal cartilage/joint articulation of the capitate as well as of the lunate fossa of the distal radius. Proximal pole scaphoid excision alone would not address the advanced arthritis of the capitolunate joint. Scaphoid fixation with bone grafting would not address the midcarpal arthritis and advanced proximal pole collapse.
QUESTION 8
The radiographs shown in Figures 1 and 2 reveal squamous cell carcinoma of the thumb involving the
distal phalanx. Following biopsy confirmation, what would be the most appropriate course of management? ---
1
Curettage and bone grafting
2
External beam radiation
3
Ray amputation of the thumb
4
Interphalangeal (IP) joint disarticulation
Squamous cell carcinoma of the fingertip/nail region is uncommon but remains the most common malignancy in the hand. A high degree of suspicion is needed to diagnose this condition. Biopsy and radiographs are necessary initially. The subsequent treatment depends on the extent of the lesion at the time of presentation. Treatment can vary from Mohs micrographic surgery (MMS) to digital amputation. Amputation is recommended when bone involvement is present. In this patient, because the distal phalanx tip is involved and no further bone involvement proximally was observed, an amputation at the IP joint level is recommended. More proximal involvement would require a more proximal amputation level. Curettage and bone graft is not appropriate for this malignant lesion. External beam radiation therapy is not a first-line treatment option for this condition. Metastatic spread is uncommon. MMS is inappropriate when bone invasion has occurred.
QUESTION 9
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence? ---
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
---
QUESTION 10
What cardiac condition causes most upper extremity emboli?
1
Atrial fibrillation
2
Viral cardiomyopathy
3
Valvular disease
4
Atrial septal defect
Atrial fibrillation is responsible for approximately 80% of all upper extremity emboli. All other cardiac conditions listed can cause upper extremity emboli; however, atrial fibrillation is the most common cause. Patients with an upper extremity embolic event should undergo prompt evaluation, with a careful history and physical examination as well as focused laboratory tests for hypercoagulability. Arterial Doppler studies or angiography is/are warranted. Electrocardiogram and echocardiogram are also used to evaluate for potential cardiac abnormalities. Consultation with vascular, radiology, and cardiology personnel is often necessary when patients present with upper extremity emboli. Treatment usually involves anticoagulation, embolectomy if necessary, and treatment for any recognized cardiac _abnormality._
QUESTION 11
Which characteristic of complex regional pain syndrome (CRPS) type 2 differentiates it from CRPS 1?
1
Positive bone scan result
2
Identified nerve injury
3
Pseudomotor changes
4
No identified nerve injury
CRPS 2 develops after nerve injury, whereas CRPS 1 occurs without nerve injury. The diagnostic criteria are otherwise the same for the 2 conditions. A 3-phase bone scan can be helpful; a pattern of increased uptake in all 3 phases, and particularly diffuse periarticular uptake in and around the joints of the affected extremity during the delayed phase, is considered typical of CRPS, especially during the first 6 months; however, it is not specific enough to be used as a diagnostic criteria. Unfortunately, the pathophysiological mechanisms underlying CRPS remain unclear, and, as such, no standard diagnostic test for CRPS exists. There are 3 major sets of diagnostic criteria for CRPS: the International Association for the Study of Pain (IASP) criteria, the Budapest Research Criteria, and the Veldman criteria. According to IASP, CRPS type
1 involves an initiating noxious event or a cause of immobilization; continuing pain/allodynia/hyperalgesia for which the pain is disproportionate to any known inciting event; evidence of edema, changes in skin blood flow, or abnormal pseudomotor activity in the region of pain; and exclusion of the diagnosis by the existence of other conditions that would otherwise account for the degree of pain and dysfunction. CRPS type 2 is a syndrome that develops after nerve injury, contends IASP. Spontaneous pain or allodynia/hyperalgesia occurs and is not necessarily limited to the territory of the injured nerve; there is or has been evidence of edema, a skin blood flow abnormality, or abnormal sudomotor activity in the region of pain since the inciting event; and the diagnosis is excluded by the existence of conditions that would otherwise account for the degree of pain and dysfunction.
QUESTION 12
A 72-year-old woman with diabetes mellitus has right hand numbness. Provocative test findings are consistent with carpal tunnel syndrome, and electrodiagnostic study (EDS) findings show prolonged median motor and sensory distal latencies with low-amplitude thenar compound muscle action potential. Poor prognosis is most associated with which factor?
1
Diabetes
2
Older age
3
Female gender
4
Severity of EDS findings
Although carpal tunnel syndrome remains a clinical diagnosis, EDS findings have become important tools. Moderate disease is defined as abnormal median sensory distal latency and prolonged median motor distal latency. Severe disease is defined as prolonged median motor and sensory distal latencies witheither absent sensory nerve action potential or mixed nerve action potential or low-amplitude or absent thenar compound muscle action potential. Although female gender and diabetes are considered risk factors, there is little association with postsurgical outcome. Severe disease as confirmed by EDS is the factor most _strongly associated with poor recovery after surgery._
QUESTION 13
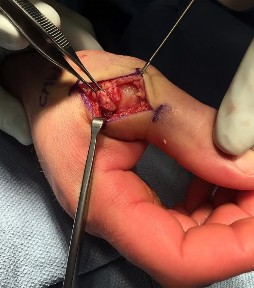
Figures 1 and 2 show the intraoperative photographs obtained from a man who is undergoing open reduction and internal fixation of a fifth carpometacarpal joint fracture dislocation. If the structure marked with an arrow in Figure 2 is cut, the patient can expect to experience ---
1
the inability to extend the small finger.
2
weakness of small finger abduction.
3
sensory loss of the dorsal ulnar hand.
4
clawing of the small and ring fingers.
The arrow in Figure 2 marks the dorsal sensory branch of the ulnar nerve. Injury to this nerve results in sensory loss of the dorsal ulnar palm and the dorsal small and ring finger digits. The dorsal sensory branch of the ulnar nerve exits the main ulnar nerve at an average distance of 8.3 cm from the proximal border of the pisiform. It becomes subcutaneous on the ulnar aspect of the forearm at an average distance of 5
cm from the proximal edge of the pisiform. It then travels dorsal to the extensor carpi ulnaris tendon to innervate the dorsal ulnar hand and the dorsal ring and small digits. Injuries to this nerve can occur from open and arthroscopic procedures (such as triangular fibrocartilage complex repair) as well as from procedures requiring percutaneous pinning. Care must be taken to identify and protect this nerve to avoid the complications of numbness and possible neuroma formation. The inability to extend the small finger would be caused by an injury to the extensor tendon(s) in this area, and the inability to abduct the small finger would require an injury to the abductor digiti minimi muscle/tendon unit or the ulnar nerve motor branch, which is located on the volar aspect of the proximal palm. Clawing of the small and ring fingers would be caused by absent intrinsic function due to an injury to the ulnar motor nerve branch located on _the volar proximal palm._
QUESTION 14
After performing an uneventful partial palmar fasciectomy for Dupuytren contracture of the palm and ring finger, a general postsurgical pain medication prescription should include how many narcotic pills?
1
0
2
10
3
20
4
30
After the designation of pain as the fifth vital sign, opioid analgesic use has steadily increased. Many surgeons routinely prescribe 30 or more pills after elective hand surgery. However, studies show that patients generally use fewer than 30 pills. Patients who underwent bone procedures used 14 pills, and those undergoing soft-tissue procedures used 9 pills. Education and decision aids may help physicians size prescriptions appropriately to avoid overmedication. Patients undergoing small soft-tissue surgeries such as trigger releases should not need narcotics. Those undergoing small-joint surgeries, carpal tunnel releases, and Dupuytren fasciectomy may benefit from a prescription of 10 pills. More extensive surgery, such as open fracture treatment, may justify more pills, but prescriptions should not exceed 40 tablets _under typical circumstances._
QUESTION 15
Figure 1 points to the "tear drop" of the wrist. This radiographic landmark represents which anatomic portion of the wrist? ---
1
Ulnar head
2
Volar ulnar corner
3
Radial styloid
4
Lister tubercle
Medoff described the radiographic teardrop of the distal radius. This radiographic landmark matches the critical volar ulnar corner of the distal radius. A malreduction of the volar ulnar corner of the distal radius in an intra-articular distal radius fracture leads to volar subluxation of the lunate and the rapid development of posttraumatic arthritis at the distal radioulnar and radiolunate joints. Knowledge of the specific shape and appearance of this radiographic landmark helps the surgeon when he or she is critically analyzing postreduction imaging. The volar portion of the ulnar head may be mistaken for this teardrop sign and should be separately identified as distinct from the distal radius. The radial styloid and Lister tubercle are not part of the volar aspect of the lunate facet.
QUESTION 16
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament? ---
1
Extensor pollicis longus (EPL) tendon
2
Adductor aponeurosis
3
EPB and dorsal capsule
4
Ulnar sesamoid bone and volar plate
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block _the UCL with this type of injury._
QUESTION 17
Figure 1 is the clinical photograph of a 65-year-old right-hand dominant man who has finger contracture and stiffness. He experiences minimal pain but has severe functional limitations and elects for treatment with injectable collagenase _Clostridium histolyticum_. What types of collagen will be affected by this injection? ---
1
Types I and II
2
Types II and III
3
Types I and III
4
Types III and IV
Type II collagen is the predominant type found in articular cartilage. Type IV collagen is the predominant type found in the basement membranes of neurovascular structures. Collagenase _Clostridium_ __histolyticum__ _injection targets type I and type III collagen._
QUESTION 18
Nerve conduction velocity is slowed by
1
increased skin temperature.
2
increased perineural blood flow.
3
external compression.
4
hand dominance.
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no _association between hand dominance and nerve conduction velocity._
QUESTION 19
When performing a Green transfer for cerebral palsy—flexor carpi ulnaris (FCU) to extensor carpi radialis brevis (ECRB)—in addition to improving wrist extension, what other motion may be improved if the FCU is routed around the ulna instead of through the interosseous membrane?
1
Thumb extension
2
Forearm supination
3
Finger extension
4
Forearm pronation
The typical upper extremity deformity in spastic hemiplegic cerebral palsy consists of shoulder internal rotation, elbow flexion, forearm pronation and wrist flexion, and ulnar deviation. The pronation position of the forearm can make bimanual activities more challenging for the child. The wrist flexion and ulnar deviation deformity interferes with finger function and therefore with grasp and release patterns. By transferring the FCU tendon to the ECRB, the deforming force is released, and central wrist extension is augmented. This transfer can lead to a supination moment when it is routed around the ulna to the ECRB insertion on the dorsum of the wrist. Thumb and finger extension are not affected by an FCU-to-ECRB _tendon transfer. Forearm supination, not pronation, is potentially improved with this tendon transfer._
QUESTION 20
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup? --- ---
1
MR imaging with contrast
2
MR imaging without contrast
3
CT scan along the scaphoid axis
4
Axial-cut CT scans with reformats
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding _scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis._
QUESTION 21
While attempting to recreate the inclination of the distal radius during volar fixation of an intra-articular sagittal split fracture, use of intraoperative fluoroscopic imaging in the position shown in Figure 1 would be helpful in showing
1
intra-articular screw penetration.
2
alignment of the joint surface.
3
alignment of the sigmoid notch.
4
dorsal screw penetration.
The image demonstrates a rotational fluoroscopic view of the lateral distal radius while attempting to recreate the inclination of the distal radius. This view is most useful to ensure against intra-articular screw penetration. The overall alignment of the joint surface is best viewed with a posteroanterior tilt of 11 degrees. The alignment of the sigmoid notch is not seen well on lateral images. Carpal alignment is seen
well on lateral images. Dorsal screw penetration is best viewed dynamically with a flexed wrist tangential _view._
QUESTION 22
Figures 1 through 4 are the radiographs, sagittal-cut CT scan, and coronal T1 MR image of a 16-year-old boy who has wrist stiffness and pain after sustaining an injury 2 years ago. There is no bleeding from the proximal pole during surgery. Which procedure will most likely result in restoration of alignment and healing? --- --- --- ---
4+5 extensor compartmental artery (ECA) vascularized bone graft
The imaging studies show an established scaphoid waist nonunion with a humpback deformity (significant flexion through the nonunion site) and carpal collapse. In addition, the proximal pole appears sclerotic on the plain radiographs and appears poorly perfused on the MR image. Correction of alignment of this scaphoid nonunion would require a volar approach with a structural bone graft. Additionally, the graft would need to provide a vascular supply to the bone. Both the 1,2 ICSRA (the Zaidenberg graft) and the 4+5 ECA grafts are vascularized grafts from the dorsal distal radius. Neither of these grafts would correct the humpback deformity, and the 4+5 ECA graft pedicle is not long enough to reach the scaphoid. An iliac crest bone graft could be used to correct the deformity, but would not provide an adequate blood supply. A free-vascularized medial femoral condyle graft provides both adequate bone graft to correct the _deformity and revascularization of the scaphoid._
QUESTION 23
Figure 1 is the radiograph of an 18-year-old, right hand-dominant man who has right side thumb pain after a tackle during a rugby game. Examination shows ecchymosis and swelling of the right thumb along with tenderness to palpation about the thumb CMC joint and metacarpal base. What ligament is holding the small fracture fragment in anatomical location to the trapezium? ---
1
Posterior oblique
2
Dorsal radial
3
Anterior oblique
4
Dorsal trapeziometacarpal
Bennett fractures are defined as intra-articular thumb metacarpal base fractures. The fracture is often caused by axial loading, and concomitant injuries to the thumb MCP joint and trapezium are common. The palmar ulnar aspect of the base of the metacarpal stays in place through its attachment to the trapezium by way of the anterior oblique ligament. The metacarpal shaft is displaced dorsally, proximally, and radially by the pull of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and adductor pollicis brevis. These fractures are often considered unstable and are treated surgically.
QUESTION 24
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option? --- ---
1
Long-arm thumb spica casting
2
Bracing and bone stimulation
3
Scaphoid excision with intercarpal fusion
4
Bone grafting with screw placement
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
QUESTION 25
Figures 1 through 3 are the radiographs of a 55-year-old woman who underwent a volar plating of an extra-articular distal radius fracture 2 weeks ago. She is experiencing weakness with flexion of the interphalangeal (IP) thumb joint. IP joint flexion was normal before surgery. What is the best next step? --- --- ---
1
Observation
2
Electromyogram/nerve conduction study (EMG/NCS)
3
CT scan
4
Immediate exploration
Prevalence of flexor tendon rupture after distal radius fracture is between 2% and 12%. The FPL tendon is the most common flexor tendon rupture associated with volar plating. It is usually seen with plates that are distal to the watershed line (W) and with plates extending volar to the critical line (C) (Figure below). The watershed line (W) is the location of the origin of the volar carpal ligaments and the bone prominence
---
at which flexor tendons are most closely opposed to the distal radius (Figure 4). In this scenario, the lateral radiograph shows that the plate is not distal to the watershed line (W) and is between the critical line (C) and the line parallel to the volar cortex of the radius (R). This is the optimal position for the plate. Placement of a volar locking plate distal to the watershed line of the distal radius and excessive plate prominence has been associated with FPL tendon rupture. This patient is only 2 weeks past surgery and there is some FPL function. FPL weakness after volar distal radius plating is common and has been seen in as many as 50% of patients. This usually recovers spontaneously by 2 months, and no treatment is needed. A nerve conduction study would be indicated if an anterior interosseous nerve compression were considered, but it is too early for this test. A CT scan could be obtained to judge the alignment of the fracture fragment and position of the screws, but it is not indicated in this case. Exploration could be performed if an FPL rupture were considered, but, because it is only 2 weeks after surgery, there is some FPL function, the plate is proximal to the watershed line, and immediate exploration is not indicated. If this does not improve after 2 to 3 months, further investigation with ultrasound or MRI would be indicated.
QUESTION 26
Figures 1 through 3 show the radiographs obtained from a 40-year-old woman who injured her right index finger in a bicycle collision. Failure to restore sagittal plane alignment would likely result in --- --- ---
1
overlapping of the digits.
2
index finger proximal interphalangeal (PIP) joint arthritis.
3
extensor lag at the PIP joint.
4
hyperextension at the PIP joint.
The radiographs reveal an extra-articular proximal phalanx fracture of the index finger. The fracture is comminuted with dorsal angulation of the distal fragment. The question specifically asks about the restoration of sagittal alignment. The fracture is comminuted with dorsal angulation of the distal fragment. The other options are incorrect, because overlapping of the digits occurs with rotational malalignment, the development of arthritis may occur with intra-articular fractures, and hyperextension would not occur _with this type of deformity._
QUESTION 27
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
1
retrograde to protect the dorsal blood supply to the scaphoid.
2
retrograde eccentrically in the dorsal scaphoid to avoidtrapezium impingement.
3
deep and centrally placed, respecting the articular surface.
4
anterograde to protect the volar blood supply to the scaphoid
QUESTION 28
Figures 1 through 3 are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step? --- --- ---
1
Early range of motion (ROM) program with a removable short-arm splint
2
Long-arm casting in pronation for 4 weeks
3
Pin fixation of the DRUJ
4
Fixation of the ulnar styloid fracture
styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure below). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar
with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
---
QUESTION 29
Figures 1 through 3 are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis? --- --- ---
1
Long-arm cast
2
Percutaneous screw fixation
3
Open reduction and internal fixation (ORIF) with bone graft
4
Proximal row carpectomy
---|--- EXPLANATION:
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal
row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
QUESTION 30
Figures 1 and 2 depict the postoperative radiographs obtained from a 22-year-old man who was involved in a motor vehicle accident. The most likely limitation in motion arising from this treatment is --- ---
1
loss of wrist flexion.
2
loss of wrist extension.
3
loss of elbow extension.
4
loss of pronation.
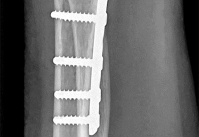
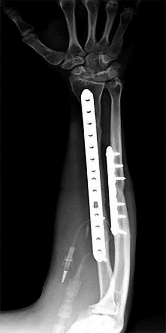
This patient sustained fractures of his radius and ulna; both were treated with plate and screw fixation. The plate used on the radius was straight, resulting in loss of the radial bow, which is critical for enabling the radius to curve around the ulna during pronation. This patient is unable to pronate beyond 20°. Schemitsch and Richards correlated a good functional outcome, defined as more than 80% of normal rotation of the forearm, with restoration of the normal amount and location of the radial bow. Additionally, they related the restoration of grip strength with appropriate restoration of the radial bow. Matthews and associates reported little significant loss of rotation with 10° of angulation; however, 20° of angulation _resulted in a statistically and clinically significant loss of forearm rotation._
QUESTION 31
A unilateral "piano key" sign, indicates
1
distal radioulnar joint (DRUJ) instability.
2
interosseous membrane disruption.
3
midcarpal instability.
4
physiologic motion of hypermobility syndrome.
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
QUESTION 32
Assuming that the fracture shown in this radiograph (Figure
1
is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active


2
metacarpophalangeal (MP) joint extension.
3
proximal interphalangeal (PIP) joint extension.
4
MP flexion.
5
PIP joint flexion.
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous _pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints._
QUESTION 33
Figure 1 shows a radiograph obtained from an active 30-year-old man who sustained an injury to his ring finger 1 week earlier. The most appropriate treatment is ---
1
open reduction and internal fixation (ORIF).
2
a mallet splint.
3
repair of the terminal tendon.
4
arthrodesis.
---
Figure 1 reveals evidence of an intra-articular distal phalanx fracture with a distal interphalangeal (DIP) joint dorsal subluxation. This injury is unstable and requires surgical management for an active individual. Volar distal phalanx fractures are often associated with flexor digitorum profundus avulsion injuries, which are addressed concomitantly. This injury was treated with ORIF of the intra-articular fracture, pinning of the DIP joint, and repair of an avulsed flexor digitorum profundus tendon with a button on the dorsal nail plate, as shown in Figure 2. Splint immobilization would not maintain a reduction of this unstable injury. The terminal tendon is not injured in this patient but is often injured in a dorsal distal phalanx fracture with a volar dislocation. Arthrodesis of the DIP is a salvage procedure and would not be considered acutely.
QUESTION 34
Figures 1 and 2 show the intraoperative photographs obtained during surgical treatment for de Quervain tendonitis. For orientation purposes, dorsal is at the top. Figure 1 is obtained just after the initial first extensor compartment release, and Figure 2 shows the floor of the first extensor compartment. If the structure marked by the black dot is not addressed, the most common postoperative problem would be --- ---
1
persistent pain.
2
tendon subluxation.
3
altered sensation.
4
tendon rupture.
The black dot identifies an accessory compartment of the extensor pollicis brevis (EPB) tendon. The incidence of accessory EPB compartment in patients undergoing surgical treatment for de Quervain syndrome ranges from 46% to 60%. Failure to release this compartment at the time of initial surgery can cause persistent postoperative pain. The patient would not experience altered sensation if this compartment were not released. Altered sensation would most commonly occur following injury to the dorsal radial sensory nerve branch during surgery. EPB tendon subluxation also would not occur should the accessory compartment not be released. For EPB tendon subluxation to occur, its own compartment would need to be released first. Finally, EPB tendon rupture would be an extremely uncommon complication of failure to release the accessory compartment.
QUESTION 35
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure? ---
1
Suprascapular
2
Radial
3
Anterior branch of axillary
4
Spinal accessory (cranial nerve XI)
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette _of the shoulder and is a stabilizer of the humeral head._
QUESTION 36
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
1
retrograde to protect the dorsal blood supply to the scaphoid.
2
retrograde eccentrically in the dorsal scaphoid to avoidtrapezium impingement.
3
deep and centrally placed, respecting the articular surface.
4
anterograde to protect the volar blood supply to the scaphoid.
The position of a scaphoid screw for scaphoid fracture repair (Figure 1) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an eccentrically placed screw. Dodds and associates
---
demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
QUESTION 37
Figures 1 through 3 are the clinical photograph and radiographs of a 25-year-old, left-hand-dominant man who injured his left index finger. Which treatment option will most effectively allow satisfactory fracture alignment and maximize motion? --- --- ---
1
Buddy-taping to the long finger with an early range of motion (ROM) program
2
Closed reduction and static external fixation in extension
3
Open reduction and internal fixation (ORIF) with an early ROM program
4
Digital splinting for 4 weeks followed by a ROM program
This patient has an oblique index proximal phalanx fracture with malrotation. Buddy-taping and digital splinting would not predictably maintain fracture reduction and would result in a malunion with rotational deformity and possible shortening. Closed reduction and spanning external fixation in extension would result in significant digital stiffness. ORIF (Figures 4 and 5) followed by an early ROM program would allow anatomic fracture alignment and give this patient the best chance to regain the majority of motion in the shortest amount of time.
---
---
QUESTION 38
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
1
increased rates of soft-tissue infection.
2
greater initial construct stiffness and peak load until failure.
3
a slower return of digital range of motion.
4
an earlier time to bony union.
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased _rates of infection. Neither fixation method would increase the time to healing._
QUESTION 39
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
1
Quadrigia
2
Intrinsic tightness
3
Lumbrical plus deformity
4
Disruption of the tendon repair
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit. Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon
repair causes limited flexion of the injured finger.
QUESTION 40
What is the most common complication after distal biceps tendon repair at the elbow?
1
Lateral antebrachial cutaneous neuritis
2
Radial sensory neuritis
3
Symptomatic heterotopic ossification
4
Rupture of the repair
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
QUESTION 41
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
1
Positive froment sign with the ulnar palm flat on a table
2
Weak thumb abduction with the dorsal palm flat on a table
3
Inability to flex the thumb with the palm flat on a table
4
Inability to extend the thumb with the palm flat on a table
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
**Question 42of 100** Figure 1 shows an injury sustained by a 60-year-old man 4 weeks ago. Since that time he has had substantial pain and catching of his finger during attempts at range of motion. What is the most appropriate treatment at this point?
---
1. Tendon debridement
2. Release of the A2 pulley
3. Tendon repair with core sutures
4. Tendon repair with epitendinous sutures
PREFERRED RESPONSE: D
EXPLANATION:
Approximately 70% laceration of the flexor digitorum profundus tendon with active locking is best treated with epitendinous sutures. Performing this procedure under local anesthetic allows for better assessment
of whether the triggering has been resolved. Cyclic loading has been shown to increase with high-grade partial lacerations. Use of core sutures adds little strength to a partial laceration. Debridement alone is reserved for injuries involving less than 60% of the tendon diameter. Release of the A2 wouldcompromise _pulley function._
QUESTION 42
Video 1 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted.
What is the most appropriate course of treatment?
Upon examination, this patient is exhibiting dislocation of the ECU tendon because of a disrupted sheath. He has failed nonsurgical measures, so surgery that would involve either direct repair or reconstruction of the tendon sheath is indicated. An option for reconstruction is to use a portion of the extensor retinaculum as a sheath substitute. Deepening of the ECU tendon groove at the distal ulna with direct repair of the sheath is another option, although a 2016 paper by Ghatan and associates did not find depth of the groove as a risk factor for subluxation. TFCC repair, lunotriquetral fusion, and DRUJ tenodesis are not appropriate because the examination clearly shows ECU tendon dislocation. TFCC and lunotriquetral ligament tears can occur along with ECU tendon dislocation, but no other examination findings suggest these conditions for this patient.
QUESTION 43
Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?
1
4-strand repair with 6-0 epitendinous suture with Bier block anesthesia
2
4-strand repair with 6-0 epitendinous suture under local anesthesia only
3
6-strand repair with regional anesthesia
4
Repair of the flexor tendon with incision of the remaining A2 pulley
Wide-awake repair under only local anesthesia, regardless of the technique, allows direct inspection of the tendon repair and active excursion. Regional anesthesia and Bier block anesthesia do not allow active motion (Bier block necessitates continued use of a tourniquet, which limits muscle function). The A2
pulley should be preserved, especially the distal 50%, to maintain tendon function. All of the listed techniques for suture repair are acceptable options.
QUESTION 44
Figures 1 through 3 demonstrate the MRIs obtained from a 36-year-old man with an injury to the elbow. The expected result of nonsurgical treatment would be weakness of ---
1
finger flexion.
2
elbow extension.
3
finger extension.
4
forearm supination.
The axial T2-weighted MRIs demonstrate a distal biceps rupture. The increased signal is noted superficial to the brachialis muscle and adjacent to the biceps tuberosity. The distal biceps tendon is not seen in the distal cuts and has retracted proximally. The physical examination of patients with these injuries show abnormal contour of the arm and tenderness in the antecubital fossa. The hook test is a provocative maneuver that documents biceps integrity. When performing the maneuver, the examiner attempts to hook a finger around the distal biceps tendon while the patient actively supinates with the elbow held in flexion. Nonsurgical treatment has been documented to result in an average loss of 40% of supination strength and 30% of elbow flexion strength. Repair is optimal within several weeks of injury. The alternative options would not occur with a distal biceps rupture.
QUESTION 45
The examination finding shown in Video 1 is consistent with which defect?
1
Trigger finger
2
Flexor digitorum profundus (FDP) incompetence
3
Flexor digitorum sublimis (FDS) incompetence
4
Extensor digitorum communis (EDC) incompetence
The video shows the lack of tenodesis caused by the incompetence of the FDP tendon to the ring finger, which can be attributable to a laceration, tendon rupture, or avulsion. Note how the ring finger stays extended (compared to the other digits) when the extensor tendons are tightened during wrist extension. The other fingers are pulled into flexion by the FDP tendons when the extensor tendons are relaxed during wrist extension. With the wrist flexed, the extensor mechanism to all fingers appears to be functioning normally. Findings indicating a trigger finger would be locking in flexion of the proximal interphalangeal joint. FDS incompetence can only be detected by blocking FDP function of the other fingers and actively flexing the examined finger.
QUESTION 46
A 23-year-old man cut the dorsal and ulnar aspects of his long finger on a table saw. The dorsal and ulnar skin over the middle phalanx is missing, with a 2-cm x 2-cm area of loss. There is a 50% loss of the extensor tendon (ulnar), and the remaining tendon has no tenosynovium. The physician should recommend irrigation and debridement and
1
tendon repair, and thenar flap coverage.
2
full-thickness skin graft.
3
reversed cross-finger flap from the ring finger.
4
cross-finger flap coverage from the ring finger.
The patient has exposed bone and tendon and a partial tendon injury. The remaining radial tendon is satisfactory and no tendon repair is required. The exposed bone and tendon necessitate vascularized tissue coverage. A reversed cross-finger flap from the ring finger is suitable for coverage of the dorsal surface of an adjacent digit.
QUESTION 47
A 45-year-old man feels a pop in the anterior aspect of his elbow while lifting furniture. He denies any antecedent pain or injury. Which examination method is best for diagnosing a distal biceps rupture?
1
The examiner brings a finger from medial to lateral across the antecubital fossa, feeling for a cord-like structure.
2
The examiner brings a finger from lateral to medial across the antecubital fossa, feeling for a cord-like structure.
3
With the elbow flexed to 90°and the forearm pronated, the examiner resists patient supination, evaluating for pain at the bicipital groove.
4
With the patient’s arm elevated to 90° of forward flexion, the elbow extended, and the forearm supinated, the examiner resists elevation distal to the elbow, evaluating for pain at the bicipital groove.
QUESTION 48
Rupture of the distal biceps tendon is predictably identified by the hook test, which is performed by bringing a finger from lateral to medial across the antecubital fossa of a flexed elbow, feeling for a cord-like structure on which the examiner can "hook" a finger. Bringing the finger from medial to lateral can cause a false-negative result, hooking the lacertus fibrosus, which can remain intact even with a ruptured distal biceps tendon. The Yergason test (option
1
and the Speed test (option
2
are used to assist in diagnosing proximal, not distal, biceps and labral pathology. Even if the distal biceps tendon is ruptured, the supinator remains intact. Although supination weakness may be present, an inability to supinate should not be observed.
When treating a closed long finger central slip tendon rupture conservatively, what is the most appropriate plan of care?
3
Splint the proximal interphalangeal (PIP) joint in flexion with early motion of the distal interphalangeal (DIP) joint
4
Allow early motion of the PIP joint with DIP extension joint splinting
5
Splint both the PIP and DIP joints in full extension
Closed central slip injuries treated nonsurgically require extension splinting of the PIP joint. DIP joint active range of motion is allowed during this time period. This allows the connections between the lateral bands and the central slip to pull the central slip distally with DIP joint active motion, minimizing the gap
across the central tendon injury and keeping the DIP joint from getting stiff as well.
QUESTION 49
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension? --- ---
1
Removal of hardware with tendon transfer
2
Repair of the extensor pollicis longus (EPL) tendon primarily
3
Thumb interphalangeal (IP) arthrodesis
4
Nonsurgical treatment with cast placement keeping the thumb in a fully extended position for 4 weeks
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through _view, are useful for avoiding this complication._
QUESTION 50
A 35-year-old man sustained a traumatic low ulnar nerve palsy 18 months ago. The extent of the clawing and intrinsic atrophy as well as the active radial deviation are seen in Figures 1 through
1
No hyperextensibility of any of the proximal interphalangeal (PIP) joints is observed. Preoperatively, the patient is not able to fully extend the PIP joints with the wrist in neutral position and the examiner holding the metacarpophalangeal (MCP) joints flexed. Figure 4 shows the intraoperative photograph obtained during the intrinsic reconstruction procedure that is performed. The tendon grafts were inserted distally into the


















2
proximal phalanx.
3
radial lateral bands.
4
first annular pulley.
5
second annular pulley.
Originally, Burkhalter and Strait recommended bony insertion into the proximal phalanx through a drill hole. This procedure does require more surgical dissection and flexes only the MCP joints; thus it cannot extend the PIP joints directly. It does improve clawing in the fingers if the PIPs can extend with preoperative MCP flexion. The ability to extend the PIP joints is evaluated preoperatively using the Bouvier test. With the wrist in neutral position, the examiner holds the MCPs flexed and looks for the ability in that position to actively extend the PIPs. If the patient is able to do so, then the test is considered positive, and this describes "simple" clawing. In such cases, procedures that flex only the MCPs are appropriate. The insertion sites for these procedures include the proximal phalanx, the first annular pulley, and the second annular pulley. If the Bouvier test is negative, then it is best to insert the tendon grafts distally into the lateral bands. This technique has a low chance of leading to hyperextension of the PIP joints, particularly when performed with a wrist extensor motor (which leaves the flexor digitorum superficialis undisturbed) and with no preoperative hyperextensibility of the PIPs.
QUESTION 51
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
1
Substance P
2
Glutamate
3
Rho kinase
4
Nitric oxide
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin _promotes nitric oxide activity to increase vasodilation._
QUESTION 52
The pathology of the lesion shown in Figures 1 and 2 reveal what cellular pattern? --- ---
1
Uniform distribution of stromal cells and giant cells
2
Mixture of mature fat cells and spindle cells
3
Mucin-filled space with occasional spindled fibroblasts
4
Lobular pattern of vascular proliferation with inflammation
QUESTION 53
Figures 1 through 5 show the radiographs obtained from a 37-year-old man who has a 10-year history of right, ulnar-sided wrist pain and a volar ulnar prominence with wrist supination. Approximately 20 years ago, he had a forearm injury that was definitively treated in a long arm cast. What surgical treatment option is most likely to improve his symptoms and maintain pronosupination? --- ---
The patient sustained a radial shaft fracture with subsequent apex volar malunion. As a result, his distal ulna subluxates volarly with wrist supination. Radiographs of the wrist reveal minimal arthritic changes. The most appropriate treatment option is to surgically correct his radial shaft malunion, which would indirectly address his DRUJ instability. A DRUJ ligament reconstruction or triangular fibrocartilage complex repair could be used to augment DRUJ stability; however, they might be unnecessary after correction of the radial shaft malunion. A DRUJ ligament reconstruction alone would not achieve stability of the DRUJ joint and maintain full wrist pronosupination. An ulnar head implant arthroplasty would not be reliable in eliminating the instability or the pain. Similarly, a one-bone forearm procedure might
improve the patient's pain and instability but at the cost of abnormal wrist and forearm mechanics and _kinematics._
QUESTION 54
What sign or symptom may occur with cubital tunnel syndrome that does not occur with Guyon neuropathy?
1
Abnormal sensation of the dorsal ulnar hand
2
A positive Froment sign
3
Abnormal sensation in the volar ring and small fingers
4
Weakness of the interosseous muscles
Ulnar neuropathy at the elbow is termed cubital tunnel syndrome, whereas ulnar nerve compression at the wrist is considered Guyon neuropathy. Patients with cubital tunnel syndrome have numbness on the dorsal ulnar aspect of the hand due to involvement of the dorsal ulnar sensory nerve branch (DUSN). Ulnar neuropathy at both the elbow and the wrist may manifest with abnormal sensation about the volar ring and small fingers and with weakness of the interosseous muscles, which can lead to a positive Froment sign. The Froment sign is considered positive when flexion of the thumb interphalangeal joint occurs to compensate for a lack of adductor function. Patients with a Guyon neuropathy do not have symptoms of numbness in the dorsal ulnar distribution, because the DUSN branch arises more proximally in the _forearm and is not compressed in the ulnar tunnel at the wrist._
QUESTION 55
You are counseling a 55-year-old woman for a right carpal tunnel release. What can you tell her about the treatment benefit (grip strength and paresthesia relief) 1 year after surgery compared with continued splinting, NSAID use, physical therapy, and a single steroid injection?
1
No change in paresthesias and grip strength
2
Increase in grip strength and decrease in paresthesias
3
Decrease in grip strength and increase in paresthesias
4
Increase in grip strength and paresthesias
Gerritsen and associates, Hui and associates, and Jarvik and associates compared the effectiveness of surgical versus nonsurgical treatment for the relief of carpal tunnel symptoms. All three studies showed that surgery was superior for the relief of paresthesias and the improvement of grip strength. According to the American Academy of Orthopaedic Surgeons Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome, strong evidence supports the assertion that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months than splinting, NSAIDs, physical therapy, and a single steroid injection. The other choices, including no change in grip strength and
paresthesias, decrease in grip strength and increase in paresthesias, and increase in grip strength and _paresthesias, are not supported by the evidence._
QUESTION 56
Figure 1 is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step? ---
1
Supervised hand therapy
2
Hemi-hamate autograft
3
Dynamic external fixation
4
Open reduction and internal fixation (ORIF)
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A "V sign" (Figure 2) is evident, indicating dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress. Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 3 through 5.
---
---
---
---
QUESTION 57
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
1
Lumbrical plus deformity
2
Intrinsic tightness
3
Quadrigia effect
4
Proximal interphalangeal joint contracture
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
QUESTION 58
A 45-year-old woman has a distal radius fracture, which is treated with open reduction and internal fixation. The surgery was uncomplicated, and the patient is discharged to home. At the first follow-up appointment, the patient demonstrates signs that are concerning for complex regional pain syndrome (CRPS). What factor is included in the International Association for the Study of Pain (IASP) criteria (Budapest criteria) for the diagnosis of CRPS?
1
Hypoesthesia
2
Elevated white blood cell count
3
Elevated C-reactive protein level
4
Pain disproportionate to the inciting event
The diagnosis of CRPS is complex. The IASP has approved diagnostic criteria to standardize both the diagnosis and the study of CRPS. The criteria are:
1. Continuing pain disproportionate to any inciting event
2. At least one symptom in three of the following four categories
1. Sensory: reports of hyperesthesia and/or allodynia
2. Vasomotor: reports of temperature asymmetry and/or skin color changes and/or skin color asymmetry
3. Sudomotor/edema: reports of edema and/or sweating changes and/or sweating asymmetry
4. Motor/trophic: reports of decreased range of motion (ROM) and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, skin, nails)
3. At least one sign at the time of evaluation in two (for clinical diagnosis) or three (for inclusion in scientific studies) of the following categories
1. Sensory: evidence of hyperesthesia (to pinprick) and/or allodynia (to light touch and/or deep somatic pressure and/or joint movement)
2. Vasomotor: evidence of temperature asymmetry and/or skin color changes and/or skin color asymmetry
3. Sudomotor/edema: evidence of edema and/or sweating changes and/or sweating asymmetry
4. Motor/trophic: evidence of decreased ROM and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, skin, nails)
4. No other diagnosis better explains the signs and symptoms.
Decreased sensation and focal numbness are not consistent with CRPS. Laboratory and imaging studies can be helpful in evaluating for the exclusion of differential diagnoses for CRPS, including infection, rheumatic disease, fracture, nonunion, tenosynovitis, or osteomyelitis.
QUESTION 59
A 64-year-old woman with rheumatoid arthritis cannot fully extend her fingers actively at the metacarpophalangeal (MCP) level. Full passive extension is possible, but she cannot actively maintain that extension when her fingers are released. The MCP joints do extend when her wrist is passively flexed. What is the most likely cause of this problem?
1
Extensor tendon ruptures at the wrist
2
Subluxation of the extensor mechanisms at the MCP joint
3
Caput ulnae syndrome
4
Posterior interosseous nerve palsy
Loss of MCP extension is common in the setting of rheumatoid arthritis, but potential causes are varied. An understanding of various etiologies is needed to address the multiple facets of inflammatory arthropathy, for which causes include extensor tendon rupture, MCP joint flexion contracture/dislocation, subluxation of the extensor tendons at the MCP joint (sagittal band rupture), and posterior interosseous nerve (PIN) palsy. These causes are differentiated during an examination. Extensor tendon ruptures, as seen with caput ulnae syndrome (Vaughan-Jackson syndrome) allow for passive MCP extension, not active extension or the ability to maintain extension actively, and would not involve finger extension with passive flexion tenodesis of the wrist. Flexion contractures of the MCP joints, as may be seen in dislocations, would not allow active or passive motion. Subluxation of the extensor tendons at the MCP joints, as seen in attenuation of the sagittal bands, will usually preclude the initiation of active extension, but patients will be able to maintain extension of the MCP joints once they are placed in extension by the examiner. With a PIN palsy, no active extension or active hold is possible, but passive extension and tenodesis with wrist flexion are maintained. Synovitis of the elbow is the most likely cause of the PIN palsy. An extensor tenosynovitis or caput ulnae syndrome would not prohibit MCP extension unless the condition progressed to the point of causing other pathology.
QUESTION 60
Figures 1 and 2 show the radiographs obtained from a 56-year-old man who has been experiencing progressive wrist pain since he felt a pop while throwing a 25-pound bag over his shoulder 6 months ago. Failure to address the injury surgically might lead to progressive arthritic changes in what order? --- ---
This patient demonstrates scapholunate dissociation with an associated dorsal intercalated segment instability deformity. Chronic scapholunate ligament tears lead to scapholunate advanced collapse (SLAC) wrist. Watson and Ballet describe SLAC wrist as having a predictable progression of arthritic changes, starting at the radial styloid, progressing to the radioscaphoid joint, and advancing to the lunocapitate joint. Some authors have described the radiolunate joint as being affected in very late-stage _SLAC wrist._
QUESTION 61
A 44-year-old man sustains the injury shown in Figures 1 through
1
What is the most appropriate treatment?












Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.
---
---
---
QUESTION 62
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of ---
1
serum and urine protein electrophoresis.
2
a chest CT scan.
3
MRI with intravenous contrast.
4
age-appropriate presurgical laboratory studies.
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
QUESTION 63
A 65-year-old right–hand-dominant woman has been experiencing thenar and wrist pain for 18 months. She has no history of trauma. The pain worsens during the opening of jars, grasping, writing, and repetitive thumb use. Examination reveals tenderness to palpation over the volar thenar eminence, just distal to the scaphoid tubercle, and along the flexor carpi radialis sheath. A Watson scaphoid shift test produces pain but no instability or clunk. Radiographs reveal isolated scaphotrapeziotrapezoidal (STT) arthritis with mild dorsal intercalated segment instability (DISI) deformity. She has worn a splint on and off for the past year, has had multiple cortisone injections, and has modified her activity, all of which helped initially. She wants to move forward with surgical intervention. STT arthrodesis is chosen over distal pole scaphoid excision. What factor in her evaluation indicates that arthrodesis would be preferred over distal pole excision?
1
Failure of pain relief from steroid injection and NSAID use
2
Tenderness that is distal to the scaphoid tubercle
3
Isolated STT arthritis on radiograph
4
Mild DISI deformity on radiograph
Isolated STT arthritis is common and can cause substantial patient disability and pain. After nonsurgical treatment has failed, surgical intervention is warranted. Surgical options include distal pole scaphoid excision, STT arthrodesis, or carpometacarpal (CMC) arthroplasty, if concomitant thumb CMC degenerative changes are present. Distal pole scaphoid excision is less commonly employed for the treatment of STT arthritis, because of the potential development of intercalated segmental instability. However, distal pole scaphoid excision is less technically demanding, engenders fewer surgical complications, and promotes a faster return to previous activity levels. In any patient with preoperative carpal malalignment, removing the distal pole of the scaphoid would exacerbate that deformity and could lead to symptoms from the DISI deformity. Thus, in this patient with mild DISI deformity seen on _preoperative radiographs, STT arthrodesis is the most appropriate treatment option._
QUESTION 64
What vitamin supplement has been shown in some studies to reduce the risk of complex regional pain syndrome following a distal radius fracture?
1
A
2
B
3
C
4
D
Two studies have shown that supplemental vitamin C reduces the risk of developing complex regional pain syndrome following a distal radius fracture. The recommended dose is 500 mg daily for 50 days. Supplemental vitamin C is a recommendation of the AAOS evidence-based Clinical Practice Guidelines
and has moderate evidence. The vitamin supplements listed as alternative options have not been shown to prevent disproportionate pain following a distal radius fracture.
QUESTION 65
Figures 1 through 3 demonstrate the radiographs obtained from a 25-year-old man who injured his right,
by punching a wall 3 weeks earlier. He notes pain and deformity about the ulnar aspect of his hand. The best treatment option is --- --- ---
1
closed reduction and cast immobilization.
2
open reduction and internal fixation (ORIF).
3
arthrodesis.
4
resection arthroplasty.
The initial radiographs reveal a fourth and fifth carpometacarpal (CMC) joint fracture dislocation. The injury is associated with a shear fracture of the dorsal rim of the hamate. Further assessment with CT might be helpful in fully evaluating the extent of injury. Extensor carpi ulnaris is a deforming force at the base of the fifth metacarpal. This unstable fracture dislocation could be treated with closed reduction and pinning if the patient presented within a few days of injury. However, because he presented in a delayed fashion (3 weeks after injury), open reduction with internal fixation was required (Figures 4 and 5). In the series by Zhang and associates, patients with fourth and fifth CMC fracture dislocations presenting in a delayed fashion and treated nonsurgically had suboptimal results. Therefore, closed reduction and casting are not appropriate. An arthrodesis and resection arthroplasty are salvage procedures considered for a painful arthritic joint and would less likely should not be considered for this acute injury.
---
---
QUESTION 66
Figures 1 and 2 are the radiographs of a 36-year-old man who has had left wrist pain for the past 6 months following a fall onto his outstretched arm. Examination reveals a positive ballottement test, dorsal and ulnar carpal tenderness, and a painful snap with ulnar deviation, pronation, and axial compression. Injury to what ligament is the cause of this patient's pain?
1
Short radiolunate
2
Dorsal scapholunate interosseous
3
Volar lunotriquetral interosseous
4
Radioscaphocapitate
---
---
EXPLANATION:
The radiographs reveal a volarly tilted lunate on the lateral view (Figure 1) and an incongruous lunotriquetral articulation on the AP gripped view (Figure 2). The patient has what appears to be radiographic findings of volar intercalated segmental instability (VISI), a type of carpal instability, dissociative. An injury to the volar lunotriquetral ligament is the most important contributor to this type of instability. An injury to the dorsal scapholunate ligament typically leads to a dorsal intercalated segmental instability. Isolated injuries to the dorsal radiocarpal ligament and the radioscaphocapitate
ligament do not lead to VISI, although combined injuries may lead to instability between the radius and _the proximal row._
QUESTION 67
A 17-year-old boy with left spastic hemiplegia secondary to cerebral palsy is being evaluated for persistent swan neck deformities of the affected hand. Splinting has been tried with some improvement, but the patient does not want to wear the splints any more. On physical examination, he demonstrates full extension of the metacarpophalangeal (MCP) joints, 30° of hyperextension of the proximal interphalangeal (PIP) joints, and flexion of the distal interphalangeal (DIP) joints when he attempts to actively extend his digits. He is able to initiate flexion at the PIP joints with his MCP joints held in neutral extension. He has equal PIP flexion when the MCP joints are extended and flexed. What is the most appropriate surgical treatment to address his swan neck deformity?
1
Central slip tenotomy
2
Terminal tendon release
3
Dorsal rerouting of the lateral bands
4
Intrinsic lengthening
This patient demonstrates full extension of the MCP joints when he actively extends his fingers, indicative of overpull of the extrinsic finger extensors. This clinical scenario can be corrected by a central slip tenotomy. A terminal tendon release is used to address a Boutonnière deformity. The patient does not demonstrate intrinsic tightness (equal PIP flexion while the MCP flexed and extended), therefore his swan neck would be unlikely to respond to intrinsic lengthening. Dorsal rerouting of the lateral bands is performed for a Boutonnière deformity. A central slip tenotomy would balance the extension forces between the PIP and DIP joints.
QUESTION 68
When performing a radioscapholunate (RSL) fusion for posttraumatic radiocarpal arthritis, excision of the distal pole of the scaphoid will cause a decrease in
1
the nonunion rate.
2
wrist extension.
3
carpal height.
4
avascular necrosis.
RSL arthrodesis is a motion-sparing option for posttraumatic radioscaphoid or radiolunate arthritis when the midcarpal joint is preserved. Preserving the midcarpal joint allows the dart-thrower motion to remain. Mühldorfer-Fodor and associates reported that the rates of nonunion for RSL fusion were reduced by excision of the distal pole of the scaphoid. Multiple studies have shown increased radial and ulnar deviation with excision of the distal pole of the scaphoid; excision of the triquetrum further increases the radial-ulnar arc of motion. Bain and associates and Pervaiz and associates reported increased wrist
flexion-extension arcs with distal scaphoid and triquetrum excisions in cadaveric models; other authors _have reported no difference._
QUESTION 69
Figure 1 shows the radiograph obtained from a 67-year-old woman who has progressive wrist pain. She undergoes a salvage motion-sparing surgery that relies on the intact cartilage of the capitate head. It is necessary to preserve what structure during this procedure?
1
Long radiolunate ligament
2
Radioscaphocapitate ligament
3
Dorsal radiocarpal ligament
4
Dorsal intercarpal ligament
---
EXPLANATION:
The radioscaphocapitate ligament must be preserved in cases of proximal row carpectomy or scaphoidectomy with four-corner fusion. Failure to do so can result in ulnar translocation of the carpus. The attachment of the long radiolunate ligament to the lunate is compromised in proximal row carpectomy, although it is left intact in scaphoidectomy with four-corner fusion. Preservation of the dorsal radiocarpal ligament through a limited arthrotomy is advocated by Ozyurekoglu and Turker as a method of preserving the blood and nerve supply of the carpus, but this technique has not been proven to be _required. The authors did cut through the dorsal intercarpal ligament in their exposure._
**Question 71of 100** At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
A. Radioscaphoid
1. Radiolunate
2. Scapholunate
3. Capitolunate
PREFERRED RESPONSE: A
EXPLANATION:
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal _involvement). The radiolunate joint is often spared._
QUESTION 70
Figures 1 through 3 show the clinical photographs obtained from a 45-year-old woman who is right-hand dominant. She has pain in the left ring proximal interphalangeal (PIP) joint that gets worse during lifting or gripping activities. On examination, she has PIP range of motion of 15° to 50° with laxity of the radial collateral ligament and tenderness around the joint. The flexor and extensor tendons are intact. She has rotational malalignment when making a composite fist. Radiographs reveal end-stage arthritis at the PIP joint. She elects to move forward with surgery and undergoes arthroplasty. What component of the examination is essential to determine which implant arthroplasty—silicone or surface replacement—is best?
1
Preoperative range of motion
2
Flexor tendon integrity
3
Rotational malalignment
4
Collateral ligament stability
---
---
--- EXPLANATION:
This patient has end-stage arthritis in conjunction with ligament insufficiency. The treatment for arthritis is arthroplasty or fusion. Given that her ring finger is affected, arthroplasty is recommended to preserve motion and grip. Two types of arthroplasties are available: silicone and surface replacement. The prerequisites are the same for both and include good bone stock, good sensibility of the joint, adequate soft-tissue coverage, and normally functioning tendons. Adequate collateral ligaments are required for surface replacement arthroplasty. This patient has a deficiency of the radial collateral ligament, evidenced by her clinical examination. Thus, silicone arthroplasty is the recommended option for joint replacement in this patient.
QUESTION 71
Figures 1 and 2 show the clinical photograph and ultrasonography image obtained from an 8-month-old boy who has a 2-month history of a well-circumscribed mass in the palm, just proximal to the palmar digital crease of the index finger. The mass has not changed in size and does not seem to cause pain. What is the best next step in treatment? --- ---
1
rasonography-guided aspiration
2
Excisional biopsy
3
Observation
4
MRI of the hand for further characterization of the mass
The history, clinical photograph, and ultrasonography evaluation point to a diagnosis of ganglion cyst. The likelihood of resolution of ganglion cysts without intervention in pediatric patients ranges from 66-79%. Therefore the most appropriate treatment at this time is observation. Because the diagnosis is confirmed with the information provided, excisional biopsy and further imaging are not necessary.
QUESTION 72
Figures 1 and 2 are the radiographs of a 55-year-old woman homemaker with a 1-year history of insidious onset left wrist pain. She has failed conservative treatment and desires surgery. Her medical history is complicated by a smoking history of 1.5 packs of cigarettes per day. At the time of surgery her capitate articular surface is normal in appearance. The best procedure for her would be --- ---
1
radial shortening osteotomy.
2
capitate shortening osteotomy.
3
scaphoid excision and four-corner fusion.
4
proximal row carpectomy.
This patient has Lichtman stage 3B Kienbock disease. She is 55 years old and is a "low-demand" patient; however, she is a heavy smoker. Based on her condition and her current smoking status, salvage treatment that does not require bone healing such as a proximal row carpectomy is likely the best treatment option. A radial shortening osteotomy and a capitate shortening osteotomy may be helpful in offloading the lunate, but both procedures require bone healing and are better options in earlier stages of Kienbock disease. A scaphoid excision and four-corner fusion is typically performed for scapholunate advanced collapse or scaphoid nonunion advanced collapse wrist arthritis and would not be recommended in this _scenario, as the lunate is avascular._
QUESTION 73
Figures 1 through 3 show the MRI images and a radiograph obtained from a 31-year-old woman who has a 1-year history of diffuse right wrist pain that is gradually worsening. She denies fever or chills and also denies a history of injury. Her examination reveals no swelling, no erythema, an 80 degree arc of active wrist flexion and extension, and dorsal wrist tenderness. The most likely diagnosis is --- --- ---
1
scapholunate advanced collapse (SLAC) wrist with cystic capitate changes.
2
idiopathic avascular necrosis (AVN) of the capitate.
3
capitate osteomyelitis.
4
aneurysmal bone cyst in the capitate.
QUESTION 74
At a minimum 2-year follow-up and compared with the metacarpophalangeal (MCP) joint, pyrolytic carbon resurfacing arthroplasties of the proximal interphalangeal (PIP) joint
1
produce less squeaking or clicking.
2
result in more dislocations.
3
provide superior pain relief.
4
result in better motion compared with the preoperative status.
Wall and Stern published a report on MCP joint pyrolytic carbon arthroplasty for osteoarthritis and another on PIP joint pyrolytic carbon resurfacing arthroplasty for osteoarthritis. They found different outcomes, and MCP joint implants outperformed PIP joint implants. Of eleven MCP joint arthroplasties, two produced asymptomatic squeaking and clicking, whereas eleven of 31 PIP joint implants produced this problem. No dislocations were reported among the MCP joint implants, but five PIP joint dislocations were observed. Outcomes were measured by the Michigan Hand Outcomes Questionnaire in both studies and were satisfactory for the MCP joint implants, with an average score of 80. The PIP implants did not fare as well, showing a higher degree of pain along with an average score of 53. The authors noted that, in the 15 patients in the PIP study who had unilateral surgery, the uninvolved, nonsurgical hand motion was actually statistically significantly (_P_ <0.01) better than the surgical hand. MCP joint motion increased from 62º before surgery to 76º after surgery, whereas PIP joint motion got worse after surgery, with the average motion decreasing from 57º to 31º.
QUESTION 75
A 25-year-old man sustains a left brachial plexus injury from a fall while rock climbing. Examination reveals poor intrinsic function of the hand, ptosis, and miosis. He is able to abduct and forward flex his shoulder with full strength. This combination of physical findings is most suggestive of what pattern of nerve injury?
1
C5-C6 postganglionic injury
2
C8-T1 preganglionic injury
3
C5 through C7 preganglionic injury
4
C8-T1 postganglionic injury
A preganglionic lesion occurs proximal to the spinal foramen, whereas a postganglionic lesion occurs distal to the spinal foramen in the root, trunk, division, cord, or branches of the brachial plexus. The Horner sign, which is characterized by miosis, ptosis, anhydrosis, and enophthalmos, results from an injury to the sympathetic ganglion, which lies in close proximity to the T1 root level. The presence of a Horner sign is highly suggestive of a T1 preganglionic injury. Other physical examination indicators of a preganglionic injury include atrophy of the parascapular muscles (injury to the dorsal rami of the cervical spinal nerve roots), winged scapula (injury to the long thoracic nerve) and hemidiaphragmatic paralysis (phrenic nerve injury). The lack of intrinsic hand function in this patient is also suggestive of an injury at the level of C8-T1. Preservation of shoulder abduction and forward flexion would not typically be seen with an injury to the C5-C6 roots or the upper trunk.
QUESTION 76
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention? ---
1
Thumb carpometacarpal (CMC) arthroplasty with ligament suspensionplasty
2
Thumb CMC and thumb metacarpophalangeal (MCP) joint fusion
3
Thumb CMC arthroplasty with ligament suspensionplasty and thumb MCP joint stabilization
4
Trapezial resection and distraction arthroplasty
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
QUESTION 77
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
1
unrecognized injury to the recurrent motor branch.
2
neuropraxia of the proper palmar digital nerve.
3
new-onset stenosing flexor tenosynovitis.
4
injury to the flexor digitorum profundus to the index finger.
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If _it were injured, the result would not be weakness of interphalangeal joint extension._
QUESTION 78
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is --- --- --- ---
1
capitate excision with interposition arthroplasty.
2
capitate proximal pole excision and drilling.
3
proximal row carpectomy (PRC).
4
vascularized bone graft.
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. _PRC would leave the capitate articulating with the radius and is not indicated._
QUESTION 79
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
1
Avascular necrosis of the proximal pole of the scaphoid
2
Dorsal intercalated segment instability (DISI)
3
Volar intercalated segment instability
4
Thumb metacarpophalangeal joint hyperextension
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended _by some authors to prevent this complication._
QUESTION 80
A 65-year-old woman has severe pain and numbness in her hand. She notes frequent awakenings at nighttime and difficulty with fine tasks. She also has a history of cervical radiculopathy and notes intermittent pain in her upper arm and periscapular region. An examination reveals a positive Tinel sign over the midforearm and carpal tunnel. Electrodiagnostic testing shows a median nerve sensory distal latency of 3.8 ms (normal latency is 3.5 ms). Which intervention or test would best predict if carpal tunnel release would be successful in relieving this patient's symptoms?
1
Trigger point injections with lidocaine
2
Carpal tunnel corticosteroid injection
3
Ultrasound of the wrist
4
Carpal tunnel view radiograph
This patient demonstrates several upper extremity issues including possible carpal tunnel syndrome, cervical radiculopathy, and pronator syndrome. The electrodiagnostic testing is equivocal, and a corticosteroid carpal tunnel injection should be performed prior to surgical intervention to assess its effectiveness in eliminating the patient's symptoms. Positive response (meaning improvement in symptoms), after corticosteroid injection at the carpal tunnel correlates well with symptom relief following surgery. Trigger-point injections are not indicated for carpal tunnel syndrome. Ultrasound and carpal tunnel view radiograph can provide diagnostic information but would not be helpful in determining _treatment in this specific case._
QUESTION 81
A 35-year-old man has a brachial plexus injury affecting the lateral cord. He partially improves with observation and now has complete return of median nerve function and pectoral muscle function. What nerve transfer is most likely to restore the motor function he is lacking?
1
Median and ulnar fascicles to musculocutaneous nerve transfer
2
Medial triceps branch to axillary nerve transfer
3
ntercostal nerve to triceps branch of radial nerve transfer
4
Anterior interosseous nerve (AIN) to ulnar motor transfer
The lateral cord of the brachial plexus gives off the lateral pectoral nerve, the musculocutaneous nerve, and then contributes to the median nerve. The patient has had recovery of function of these components except for the musculocutaneous nerve. The musculocutaneous nerve innervates the biceps and the brachialis, which provide elbow flexion. To restore motor function, a nerve transfer would have to provide _reinnervation of the biceps and brachialis._
QUESTION 82
Figure 1 shows the clinical photograph obtained from a child with a congenital difference of the hand. What clinical feature(s) is/are characteristic of this condition? ---
1
Cardiac anomalies
2
Radial deviation of the thumb
3
Acrosyndactyly with proximal sinus tracts
4
Absence of the ulna
The clinical photograph reveals a child with amniotic band syndrome or constriction band syndrome. If a band causes an autofusion of the digits without amputation, acrosyndactyly can occur, as demonstrated in the clinical photograph. Typically, a proximal sinus tract with a distal syndactyly is present. Radial deviation of the thumb can be seen most frequently in Apert syndrome. Cardiac anomalies are associated with many congenital upper extremity differences but are not characteristic of amniotic band syndrome. _Ulnar longitudinal deficiency is characterized by hypoplasia or complete absence of the ulna._
QUESTION 83
A 55-year-old man was injured when a large piece of sheet metal lacerated his medial elbow while working at a factory. He underwent primary repair of the lacerated structures shown in Figures 1 and 2 on the day of injury. In addition to this surgical treatment, what nerve transfer procedure should be considered during this primary operative intervention to improve his functional recovery? --- ---
1
Flexor digitorum superficialis (FDS) branch transfer to the extensor carpi radialis brevis (ECRB) branch
2
Third web space median fascicle transfer to the ulnar sensory fascicle
3
Flexor carpi ulnaris fascicle (FCU) transfer to the biceps branch
4
Terminal anterior interosseous nerve (AIN) transfer to the deep ulnar motor fascicle
In adults, the repair of high ulnar nerve injuries typically yields incomplete motor recovery and disappointing functional results despite early surgical intervention and careful surgical technique. Early transfer of the terminal branch of the AIN to the deep ulnar motor fascicle can rapidly reinnervate distal targets and potentially preserve motor end plate function in the intrinsic musculature of the hand because of the proximity of the nerve transfer to the target muscle. Sensory deficits due to an ulnar nerve injury
can be restored through a transfer of median sensory fascicles to the distal ulna sensory fascicles. This procedure typically would not be considered at the time of the original surgery, because sensory recovery is more likely than motor recovery in the setting of a high ulnar nerve injury. For radial nerve injuries, wrist extension can be restored through an FDS branch of the median nerve transfer to the ECRB branch of the radial nerve. The FCU fascicle of the ulnar nerve can be transferred to the biceps branch of the _musculocutaneous nerve to restore elbow flexion and supination._
QUESTION 84
Based on the best available evidence, what is the maximum number of days at which a successful manipulation can be performed following collagenase injection?
1
7
2
5
3
3
4
1
In the original clinical trial, the authors performed manipulation at 24 to 72 hours following the collagenase injection for Dupuytren disease. Evidence now suggests that up to 7 days is a safe and well-_tolerated interval for manipulation following collagenase injection._
QUESTION 85
A 20-year-old woman with spastic hemiplegia is evaluated for function and hygiene issues with her right wrist. Her wrist has a resting posture of 90° of flexion and can be passively extended to 65° of flexion. Her fingers are flexed into her palm but can be passively extended with the wrist at 95°. What treatment is likely to provide the most durable result for improved hygiene, function, and cosmesis?
1
Flexor carpi ulnaris to extensor carpi radialis brevis transfer
2
Fractional lengthening of the wrist and finger flexor tendons
3
Wrist arthrodesis with proximal row carpectomy
4
Botulinum toxin injection
The patient has a static deformity of the wrist with a fixed flexion deformity of more than 45°. Soft-tissue procedures such as those referenced in options A and B would not be sufficient to address the degree of contracture. Additionally, Botulinum toxin injections would not provide relief for capsular contractures. Wrist arthrodesis combined with a proximal row carpectomy has been shown to provide a functional and _cosmetic alternative for patients with severe wrist flexion contractures._
QUESTION 86
The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using
1
clinical examination.
2
invasive pressure measurement.
3
arterial Doppler study.
4
MRI.
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow, and an abnormality would be a late finding. MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the _history and physical examination._
QUESTION 87
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure
1
Which interposed structure is preventing reduction?



2
Flexor tendons
3
Lateral band
4
Lumbrical
5
Volar plate
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
QUESTION 88
Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate treatment option? --- ---
1
Emergent surgery, including open carpal tunnel release, open reduction of the perilunate dislocation, repair of the scapholunate ligament, and intercarpal pinning
2
Emergent surgery, including open carpal tunnel release, closed reduction of the perilunate dislocation, and casting
3
Elective outpatient surgery, including open carpal tunnel release, open reduction of the perilunate dislocation, repair of the scapholunate ligament, and intercarpal pinning
4
Emergent surgery, including open reduction of the perilunate dislocation, repair of the scapholunate ligament, and intercarpal pinning
This patient sustained a lesser-arc perilunate dislocation. As a result of the injury, he also developed acute carpal tunnel syndrome. The closed reduction attempt was unsuccessful; therefore, this injury is best managed with emergent surgery, an open carpal tunnel release, an open reduction of the perilunate dislocation, scapholunate ligament repair, and intercarpal pinning. Outpatient surgery in a delayed fashion is not advised because of the acuity and severity of the carpal tunnel syndrome. Closed reduction and casting is not advised, because it commonly leads to continued carpal instability with subsequent dorsal
intercalated segment instability deformity and scaphoid lunate advanced collapse wrist arthritis.
QUESTION 89
In the injury shown in Figures 1 and 2, what ligament remains intact? --- ---
1
Short radiolunate
2
Scapholunate
3
Radioscaphocapitate
4
Dorsal radiocarpal
Perilunate dislocations result from high-energy injuries to the extended wrist. The injury shown is a lunate dislocation. Two classification systems have been described, the Mayfield system and the Herzberg system. Mayfield described the four stages of progressive ligamentous instability following injury. In stage I, the radioscaphocapitate and scapholunate ligaments fail. Stage II involves dislocation of the lunocapitate joint, usually a dorsal dislocation of the capitate. In stage III, the lunotriquetral ligament fails. In stage IV, the dorsal radiocarpal ligament is torn, and the lunate dislocates volarly. The short radiolunate ligament is the only ligament that remains intact, resulting in rotation of the lunate volarly. Herzberg and associates further classified perilunate dislocations as stage I injuries and lunate dislocations as stage II injuries. Lunate dislocations were further classified into stage IIA, in which the lunate exhibits rotation less than 90°, and stage IIB, in which the lunate exhibits rotation greater than 90°. The radiographs _represent a Mayfield stage IV, Herzberg stage IIA injury._
QUESTION 90
Figures 1 and 2 are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 9 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem? ---
1
Laceration of a branch of the posterior interosseous nerve (PIN)
2
Postsurgical tendon adhesion
3
Laceration of the (EDC) tendons to long and ring fingers
4
Neuropraxia of the PIN
Plating of the proximal radius from a dorsal or Thompson approach (between the extensor carpi radialis brevis and extensor digitorum communis) allows complete visualization of the PIN through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 1 and 2.Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the _extensor indicis proprius_ and the EDC of the ring finger to the _extensor digiti quinti_ proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the _mobile wad and the digital extensors will be more easily found._
QUESTION 91
Which examination finding points toward a brachial plexus injury rather than root avulsion?
1
Winging of the scapula
2
Intact rhomboid function
3
A biceps with 0/5 strength
4
An ipsilateral clavicle fracture
A brachial plexus injury distal to the root level should leave the rhomboid muscle with intact function. Root avulsions of C5-6 will cause weakness of the rhomboids. The branching of the dorsal scapular nerve is proximal and often spared with upper brachial plexus injuries. Winging and biceps weakness may occur
with either injury, and an ipsilateral fracture does not differentiate an avulsion from a brachial plexus _injury._
QUESTION 92
The development of complex regional pain syndrome (CRPS) following distal radius fracture is associated with what factor?
1
Diabetes
2
Fibromyalgia
3
Nonsurgical fracture management
4
Male gender
CRPS is an uncommon complication following distal radius fractures; its incidence is reported to range between 1% and 37%. Two recent studies have evaluated for risk factors in the development of CRPS following distal radius fractures. Female gender, concomitant fracture of the distal ulna, and surgical treatment were all associated with an increased likelihood of CRPS, as was fibromyalgia. Older age was _identified as conferring both an increased and a decreased risk for CRPS in the two studies._
QUESTION 93
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of ---
1
intravenous (IV) antibiotics and admission to a medical intensive care unit.
2
emergent radical debridement including thumb amputation.
3
emergent revascularization of the thumb with a vein graft.
4
urgent irrigation of the thumb flexor tendon sheath.
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an _infection, and revascularization is not indicated._
QUESTION 94
A 35-year-old man who is left-hand dominant has pain and swelling around his left index metacarpal phalangeal (MCP) joint following a motor vehicle accident 2 months ago. Radiographs reveal no fractures. He has point tenderness over the radial side of the MCP joint and increased laxity with ulnarly applied stress. He has failed conservative treatment including 5 weeks of immobilization. If the patient elects to live with this condition and not have surgery, what would be the most common outcome?
1
Development of a trigger finger
2
Presence of intrinsic tightness
3
Weakness of pinch strength
4
Subluxation of the extensor tendon with MCP joint motion
The thumb MCP ulnar collateral ligament (UCL) and index MCP radial collateral ligament (RCL) are the primary stabilizers to pinch. Secondary stabilizers include the volar plate, dorsal capsule, and accessory collateral ligaments. With insufficiency of either the thumb MCP UCL or the index MCP RCL, pinch strength will be severely weakened. The other options listed are unlikely to occur with this _particular injury._
QUESTION 95
Figures 1 and 2 are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, decrease wrist range of motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment? --- ---
1
Proximal row carpectomy
2
Radial shortening osteotomy and vascularized bone grafting
3
Scaphoid excision and midcarpal arthrodesis
4
Capitate hamate fusion
This patient has late-stage Kienböck disease. According to the Lichtman classification for Kienböck disease, this would represent stage IIIB, with lunate collapse/fragmentation, loss of carpal height secondary to proximal capitate migration, and a flexed scaphoid. The lateral radiograph reveals a radioscaphoid angle exceeding 60 degrees, so disease stage is IIIB. According to Condit and associates, when the presurgical radioscaphoid angle exceeds 60 degrees, results are poor when an attempt to maintain the lunate is made. As a result, the procedure with the most predictable outcome is a proximal row carpectomy. A radial-shortening osteotomy could be performed because the ulnar variance is negative. Considering the marked lunate fragmentation and collapse, a vascularized bone graft likely is contraindicated and associated with less predictable results than a proximal row carpectomy. There is no role for supervised hand therapy and splinting in the setting of advanced Kienböck disease. Similarly, _there is no role for maintenance of the lunate in the setting of advanced collapse and fragmentation._
QUESTION 96
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
1
Silicone replacement arthroplasty through a volar approach
2
Surface replacement arthroplasty through a volar approach
3
Silicone replacement arthroplasty through a dorsal approach
4
Surface replacement arthroplasty through a dorsal approach
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
QUESTION 97
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew _Eikenella corrodens_. The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment? ---
---
---
---
1
Continued IV antibiotics for 4 weeks
2
Continued oral antibiotics for 6 weeks
3
Bone scan, biopsy, and metastatic work-up
4
Surgical débridement along with antibiotics
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection _and not a tumor, and MRI already has provided enough diagnostic information._
QUESTION 98
Figure 1 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step? ---
1
Observation
2
Vascularized bone grafting to the lunate
3
Core decompression of the radius and ulna
4
Immobilization
Lunate or perilunate dislocations are usually treated with open reduction and internal fixation through a dorsal or combined dorsal and volar approach. A high index of suspicion is necessary when treating patients who sustain multiple trauma because as many as 25% of lunate or perilunate dislocations are missed initially. The radio dense appearance of the lunate seen in Figure 1 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease. Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect longterm outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect _hand function._