
Question 76
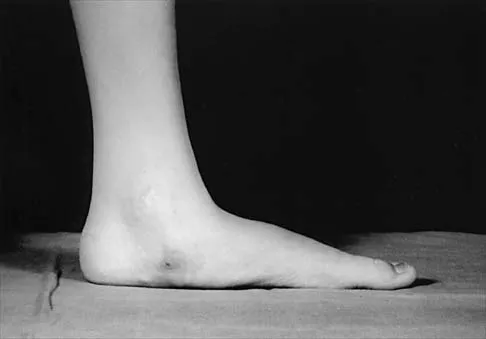
Figure 33 shows the oblique radiograph of an 11-year-old boy who has a mild left flatfoot deformity. Examination reveals that subtalar motion is limited and painful. Despite casting for 6 weeks, the patient reports foot pain that limits participation in sport activities. A CT scan shows no subtalar joint abnormalities. Management should now include

Explanation
The radiograph shows an incompletely ossified calcaneonavicular coalition. When symptomatic, a trial of cast immobilization is reasonable. If this fails to provide relief, the preferred treatment is resection of the coalition. Before attempting surgery, a CT scan should be obtained to rule out ipsilateral subtalar coalition. Recurrence of the coalition is usually prevented with interposition of autogenous fat graft or with local interposition of the extensor digitorum brevis muscle. Approximately 80% of patients treated in this manner have decreased pain and improved subtalar motion. When the flatfoot deformity is mild, calcaneal lengthening or medial translation osteotomy is unnecessary. Primary triple arthrodesis may be indicated if degenerative changes are present in the subtalar or midfoot joints. Peroneal lengthening has been described for treatment of the peroneal spastic flatfoot without demonstrable tarsal coalition. Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
References:
- Luhmann SJ, Rich MM, Schoenecker PL: Painful idiopathic rigid flatfoot in children and adolescents. Foot Ankle Int 2000;21:59-66.
Question 77
A nonambulatory verbal 6-year-old child with spastic quadriplegic cerebral palsy has progressive bilateral hip subluxation of more than 50%. There is no pain with range of motion, but abduction is limited to 20 degrees maximum. An AP radiograph is seen in Figure 34. Management should consist of

Explanation
The natural history of the patient's hips, if left untreated, is gradual progression to dislocation. To prevent future pain, prevention of dislocation is often helpful. The patient is too old for soft-tissue releases alone. Therefore, the treatment of choice is medial release of both hips to obtain 45 degrees or better of hip abduction in conjunction with psoas tenotomy and bilateral femoral varus osteotomies. Presedo A, Oh CW, Dabney KY, et al: Soft-tissue releases to treat spastic hip subluxation in children with cerebral palsy. J Bone Joint Surg Am 2005;87:832-841.
References:
- Miller F, Bagg MR: Age and migration percentage as risk factors for progression in spastic hip disease. Dev Med Child Neurol 1995;37:449-455.
Question 78
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of



Explanation
35b 35c The patient has an open fracture of the physis of the distal phalanx with a portion of the nail bed interposed in the physis. Seymour initially described this injury in the distal phalanges of fingers. Optimal treatment consists of removing the interposed tissue, irrigating the fracture, and a short course of antibiotics. The nail should be preserved to provide stability. Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34. Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
References:
- Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 79
Figure 36 shows the radiograph of a 14-year-old boy who has been treated in the past for Perthes' disease with an abduction brace. He now has hip pain that limits his activity, and nonsteroidal anti-inflammatory drugs have failed to provide relief. What is the most appropriate treatment?

Explanation
Several authors have reported good success in relieving pain with shelf acetabuloplasty. This patient's Perthes' disease is in the healed phase; therefore, proximal femoral varus and Salter innominate osteotomies aimed at improving containment are not indicated. The medial one half of the patient's femoral head is markedly deformed, and rotating it into a weight-bearing position with proximal femoral valgus osteotomy is unlikely to relieve pain. Hip arthrodesis can always be performed as a salvage procedure if the shelf acetabuloplasty fails. Daly K, Bruce C, Catterall A: Lateral shelf acetabuloplasty in Perthes' disease: A review of the end of growth. J Bone Joint Surg Br 1999;81:380-384.
References:
- Yoo WJ, Choi IH, Chung CY, et al: Valgus femoral osteotomy for hinge abduction in Perthes disease: Decision-making and outcomes. J Bone Joint Surg Br 2004;86:726-730.
Question 80
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
Breech positioning has been noted as the risk factor that most increases the relative risk of developmental dysplasia of the hip in multiple series and meta-analysis. All the other factors also increase the risk but to a lesser magnitude. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
References:
- Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 81
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?

Explanation
37b Premature consolidation is a complication that is unique to gradual bone lengthening after corticotomy. Causes include excessive latency period, inadequate distraction rate, exuberant bone formation, patient compliance problems, and mechanical failure of the distraction apparatus. The femur and fibula are most commonly involved. This patient did not have an incomplete corticotomy, as initial distraction occurred before the distraction device was noted to seize up. The radiographs show bowing of the Ilizarov wires and mature regenerate bone, both suggestive of premature consolidation. No wire breakage or joint subluxation is seen on the radiographs. Treatment for premature consolidation includes continuing distraction until the consolidation bridge ruptures, or additional surgery may include closed rotational osteoclasis or repeat corticotomy. Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
References:
- Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 82
A 4-year-old child was born with bilateral congenital radial clubhands. Which of the following associated conditions is a contraindication to centralization of the hands on the ulna?
Explanation
Patients born with bilateral radial clubhands may have difficulty getting their hands to their mouth. The centralization procedure would take away that ability if there is a lack of elbow flexion. Green DP, Hotchkiss RN, Pederson WC: Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 344-349.
References:
- Herring JA: Tachjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 382, 511.
Question 83
A 6-year-old Little League pitcher has had pain in the right elbow for the past 2 weeks. Examination reveals mild lateral elbow joint tenderness with full range of motion and no effusion or collateral laxity. A radiograph is shown in Figure 38. Initial management should consist of

Explanation
The radiograph shows osteochondritis dissecans (OCD) of the capitellum, one manifestation of "pitcher's elbow." The lesion is nondisplaced, and healing is possible if the inciting throwing activities are curtailed. Long arm cast treatment may be reasonable for the noncompliant patient but should not exceed 6 weeks duration. Surgical treatment is indicated for loose bodies or cartilage flaps. Elbow OCD lesions are now being seen in younger children as more participate in organized sports, especially baseball and gymnastics. Bauer M, Jonsson K, Josefsson PO, et al: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160. Takahara M, Ogino T, Sasaki I, et al: Long term outcome of osteochondritis dissecans of the humeral capitellum. Clin Orthop 1999;363:108-115.
References:
- Byrd JW, Jones KS: Arthroscopic surgery for isolated capitellar osteochondritis dissecans in adolescent baseball players: Minimum three-year follow-up. Am J Sports Med 2002;30:474-478.
Question 84
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
In approximately 15% of children with Down syndrome, atlantoaxial instability develops because of ligament laxity, making them susceptible to spinal cord injury with relatively minor trauma. The American Academy of Pediatrics recommends lateral flexion-extension views of the cervical spine in any patient with Down syndrome who wishes to participate in sports. A normal ADI is up to 4 mm. Patients with Down syndrome with an ADI of more than 5 mm should not participate in contact sports or sports with a high risk for neck injury, such as diving, gymnastics, high jump, or butterfly stroke. Cervical fusion has a very high rate of complications in patients with Down syndrome and is recommended only for patients who have myelopathic signs or symptoms. Atlantoaxial instability in Down syndrome: Subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-154. Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
References:
- Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547-1554.
Question 85
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
This child has the potential to walk and therefore should have all the contracted structures in the feet released as necessary to place the feet in a plantigrade position for fitting of ankle-foot orthoses. Physical therapy, manipulation, and casting may provide some benefit in a newborn with flexible feet but are not effective in an older infant with rigid clubfeet. Botulinum injections and tendon transfers are of no use because there are no muscles functioning below the knee. Tendon releases are more effective than tendon transfers in children with myelomeningocele. Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
References:
- Dias LS: Surgical management of acquired foot and ankle deformities, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 161-170.
Question 86
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of


Explanation
39b The radiographs confirm a slipped capital femoral epiphysis of the left hip, as well as a widened growth plate on the contralateral hip. This is considered a stable slip because the patient is able to walk. Treatment options for stable slips include in situ pinning, bone graft epiphysiodesis, and in some centers severe slips are treated with primary osteotomy and epiphyseal fixation. Percutaneous in situ fixation is the most popular and widely used method of treatment. This juvenile patient has an endocrine condition and a widened growth plate on the right side; therefore, strong consideration should be given to pinning the contralateral hip "pre-slip." Muscle strengthening, hip spica casting, and closed reduction have no place in the primary treatment of a stable slipped capital femoral epiphysis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140. Loder R, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
References:
- Aronson DD, Carlson WE: Slipped capital femoral epiphysis: A prospective study of fixation with a single screw. J Bone Joint Surg Am 1992;74:810-819.
Question 87
A 7-year-old boy with spastic diplegia is a limited community ambulator. He has a moderately severe crouched gait. The parents request a treatment that will result in a permanent decrease in lower extremity muscle tone. This is best accomplished with
Explanation
Posterior rhizotomy provides a permanent reduction in tone of spastic muscles. Potential drawbacks of the procedure include excessive muscle weakness, hip dislocation, and spinal deformity. Intramuscular botulinum-A toxin results in permanent blockade of presynaptic release of acetylcholine across the neuromuscular junction. The clinical effect usually resolves after 3 to 6 months due to neural regeneration. Tone-reduction AFOs have not been shown to reduce tone. A baclofen pump could offer prolonged reduction in tone, but not a single intrathecal injection. Arens LJ, Peacock WJ, Peter J: Selective posterior rhizotomy: A long-term follow-up study. Childs Nerv Syst 1989;5:148-152. Koman LA, Paterson Smith B, Balkrishnan R: Spasticity associated with cerebral palsy in children: Guidelines for the use of botulinum-A toxin. Paediatr Drugs 2003;5:11-23.
References:
- Johnson MB, Goldstein L, Thomas SS, et al: Spinal deformity after selective dorsal rhizotomy in ambulator patients with cerebral palsy. J Pediatr Orthop 2004;24:529-536.
Question 88
Figure 40 shows the radiographs of a 2-year-old boy who has a deformed leg. The patient is ambulatory and has no pain. What is the most appropriate management?

Explanation
The patient has a prefractured stage of congenital pseudarthrosis of the tibia and is at risk for fracture. The PTB orthosis may prevent or delay the fracture. Osteotomy is frequently complicated by nonunion. When established nonunion does not respond to intramedullary nailing and bone grafting, vascularized grafting may succeed. Amputation is a salvage procedure. Murray HH, Lovell WW: Congenital pseudarthrosis of the tibia: A long-term follow-up study. Clin Orthop 1982;166:14-20.
References:
- Crossett LS, Beaty JH, Betz RR, et al: Congenital pseudarthrosis of the tibia: Long-term follow-up study. Clin Orthop 1989;245:16-18.
Question 89
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
In children, the main route of infection in skeletal TB is through hematogenous spread from a primary source. The mycobacterium is deposited in the end arterials in the vertebral body adjacent to the anterior aspect of the vertebral end plate. Thus, the anterior portion of the vertebral body is most commonly involved. The lower thoracic region is the most common segment; next in decreasing order of frequency are the lumbar, upper thoracic, cervical, and sacral regions. Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
References:
- Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 1831-1835.
Question 90
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of

Explanation
The radiograph shows excessive thoracic kyphosis (normal 20 degrees to 50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann's kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann's kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees. Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248. Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
References:
- Tribus CB: Scheuermann's kyphosis in adolescents and adults: Diagnosis and management. J Am Acad Orthop Surg 1998;6:36-43.
Question 91
What is the most important sign of impending modulation with rapid progression of a spinal deformity in neurofibromatosis?
Explanation
Rib penciling is the only singular factor; 87% of the curves progressed significantly in patients with three or more penciled ribs. Modulation in neurofibromatosis scoliosis implies the change from an idiopathic type to a dysplastic type of curve with rapid progression and the need for aggressive stabilization by fusion. Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
References:
- Durrani AA, Crawford AH, Chouhdry SN, et al: Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69-75.
Question 92
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Explanation
42b The child has a trigger thumb deformity. A trigger thumb is a developmental mechanical problem rather than a congenital deformity. The anomaly generally is not noted at birth. A fixed flexion deformity of the IP joint of the thumb most commonly occurs in children in the first 2 years of life. A stretching and splinting program may correct the deformity in the first year of life, but nonsurgical management after age 3 years results in a success rate of only 50%. Release of the proximal annular pulley of the flexor sheath is recommended at this age. Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259. Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
References:
- Herring JA: Disorders of the upper extremity: Thumb dysplasia, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 445.
Question 93
A 3-year-old boy had been treated with serial casting for a right congenital idiopathic clubfoot deformity. The parents are concerned because the child now walks on the lateral border of the right foot. Examination shows that the foot passively achieves a plantigrade position with neutral heel valgus and ankle dorsiflexion to 15 degrees. The forefoot inverts during active ankle dorsiflexion. Mild residual metatarsus adductus is present. Management should now consist of
Explanation
Dynamic midfoot supination that is the result of peroneal weakness is a common residual problem after cast correction or surgical reconstruction of a congenital idiopathic clubfoot. Dynamic supination is unlikely to resolve spontaneously. Most parents do not want to use brace support forever. Transfer of the posterior tibialis to the dorsum of the foot has shown poor results in clubfeet. Preferred treatments include: 1) transfer of the entire anterior tibialis tendon to the lateral cuneiform, or 2) split transfer of the anterior tibialis tendon to the cuboid or to the peroneus brevis tendon. Kuo KN, Hennigan SP, Hastings ME: Anterior tibial tendon transfer in residual dynamic clubfoot deformity. J Pediatr Orthop 2001;21:35-41. Garceau GJ: Anterior tibial tendon transfer for recurrent clubfoot. Clin Orthop 1972;84:61-65.
References:
- Miller GM, Hsu JD, Hoffer MM, et al: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 94
Figures 43a and 43b show the clinical photographs of a 4-month-old child with bilateral popliteal pterygium. The fixed knee contractures measure 100 degrees bilaterally. What future treatment is most likely to successfully correct this deformity?


Explanation
43b Congenital popliteal webbing with contractures of 60 degrees is a difficult deformity to correct. The anatomy of the web is of considerable importance. MRI can delineate the extent of the posterior fibrous band that often stretches from the ischium to the calcaneus. The sciatic nerve, usually shortened, most often runs just anterior to this fibrous band. For mild contractures of less than 20 degrees, nonsurgical management is usually adequate. Hamstring lengthening and postoperative splinting are usually sufficient for contractures of 20 degrees to 40 degrees. Moderate contractures of up to 60 degrees usually require Z-plasties in the popliteal fossa and postoperative serial casting to avoid undue tension on neurovascular structures. Contractures of more than 60 degrees require a femoral shortening osteotomy or gradual correction with an external fixator. However, rapid recurrence following fixator removal is common if formal soft-tissue procedures and postoperative splinting are not performed. Parikh SN, Crawford AH, Do TT, et al: Popliteal pterygium syndrome: Implications for orthopaedic management. J Pediatr Orthop B 2004;13:197-201.
References:
- Brunner R, Hefti F, Tgetgel JD: Arthrogrypotic joint contracture at the knee and foot: Correction with a circular frame. J Pediatr Orthop B 1997;6:192-197.
Question 95
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm3 (normal to 10,500/mm3) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of

Explanation
The symptoms, physical findings, and laboratory studies are most consistent with a diagnosis of infectious sacroiliitis, usually caused by Staphylococcus aureus. Initial radiographs will be normal, and the diagnosis of sacroiliitis is often delayed. A technetium Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip. Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop 1993;287:98-106.
References:
- Osman AA, Govender S: Septic sacroiliitis. Clin Orthop 1995;313:214-219.
Question 96
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
Many congenital limb deficiencies and bowing deformities result in growth retardation. If unilateral, a gradually progressive limb-length discrepancy will result; however, the proportional lengths of the lower extremities will remain at a relatively constant ratio. For example, if the right foot is at the level of the left knee at birth, this will still be true at maturity. This concept can be useful for early prediction of limb-length discrepancy by using a "multiplier method," as described by Paley and associates. This method can facilitate early treatment decisions, such as the need for amputation, without having to wait for serial scanography measurements. Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
References:
- Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 97
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
While some curly toe deformities spontaneously improve in younger children, the deformity is likely to persist in a 6-year-old child. Taping techniques result in no change or only a temporary decrease in deformity. Studies have shown that simple flexor tenotomy is as effective as flexor tendon transfer. Arthrodesis is rarely indicated. Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
References:
- Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood. J Bone Joint Surg Br 1984;66:770-771.
Question 98
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Explanation
Mild scoliosis is not a painful condition, but it usually presents during adolescence. Intermittent back pain is reported by 25% to 30% of adolescents whether or not scoliosis is present. Such pain is often attributed to muscle strain from tight muscles, poor posture, or heavy school backpacks. The clinician must distinguish typical pain (mild, intermittent, nonlimiting) from atypical pain. The latter requires more careful examination and imaging studies (bone scan or MRI) to determine the source of pain. The patient's age and right thoracic curve pattern are typical for idiopathic scoliosis; therefore, imaging of the neuroaxis is not necessary to look for cord syrinx, tethering, or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368. Hollingworth P: Back pain in children. Br J Rheum 1996;35:1022-1028.
References:
- Siambanes D, Martinez JW, Butler EW, et al: Influence of school backpacks on adolescent back pain. J Pediatr Orthop 2004;24:211-217.
Question 99
What zone of the physis is widened in rickets?
Explanation
Rickets causes widening of the hypertrophic layer of the physis because of the failure of mineralization and vascular invasion. The other zones of the physis may be altered in other disease conditions but remain relatively unchanged in rickets. Hunziker EB, Schenk RK, Cruz-Orive LM: Quantitation of chondrocyte performance in growth-plate cartilage during longitudinal bone growth. J Bone Joint Surg Am 1987;69:162-173.
References:
- Iannotti JP: Growth plate physiology and pathology. Orthop Clin North Am 1990;21:1-17.
Question 100
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm3 and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
The patient has diskitis. Administration of IV antibiotics speeds resolution and minimizes recurrence. Bed rest and cast immobilization have been successfully used to treat this disorder but can be associated with prolonged recovery and frequent recurrence, even when oral antibiotics are administered. A perivertebral abscess seen in association with this condition usually resolves without surgery. Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop 1995;15:652-660.
References:
- Crawford AH, Kucharzyk DW, Ruda R, et al: Diskitis in children. Clin Orthop 1991;266:70-79.
Finish Exam?
You cannot change answers after submitting.
