Score: 0%
ORTHOPEDIC MCQS ONLINE HAND 017
QUESTION 1
of 100
Figures 1a through 1c are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury, she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?



Figures 1a through 1c are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury, she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?
1
Observation only
2
Fluoroscopic-guided intralesional steroid injection followed by serial radiographs.
3
Immediate curettage without bone grafting
4
Splint immobilization with curettage and possible grafting after the fracture has healed
_
This patient has a fracture of the middle phalanx attributable to the presence of an enchondroma. Enchondromas are the most common benign bone tumor affecting the hand. This particular enchondroma has thinned the cortices extensively so that even minor trauma can cause a pathologic fracture. Observation is not the best treatment because a fracture is present, and, at a minimum, the digit should be immobilized. Intralesional steroid injections have a role in the treatment of simple bone cysts; however, this treatment is not recommended for enchondromas. Immediate curettage alone is not the best treatment because it does not include bone graft (either autograft or allograft) or bone graft substitute. Also, it would be best to allow the fracture to heal prior to curettage to prevent fracture displacement. An enchondroma this size necessitates a graft because of high risk for refracture if curettage alone is performed. Many surgeons believe it is best if a fracture heals prior to curettage and grafting because this allows better graft containment and eliminates concern about fracture displacement. Recent data suggest early surgery using injectable calcium sulfate cement in the fracture setting can achieve satisfactory results. Splint
immobilization would allow fracture healing, and then curettage with bone graft can be performed after healing occurs.
RECOMMENDED READINGS
1. Jacobson ME, Ruff ME. Solitary enchondroma of the phalanx. J Hand Surg Am. 2011 Nov;36(11):1845-7. doi: 10.1016/j.jhsa.2011.05.002. Epub 2011 Jun 11. Review. PubMed PMID: 21658859.
2. Sassoon AA, Fitz-Gibbon PD, Harmsen WS, Moran SL. Enchondromas of the hand: factors affecting recurrence, healing, motion, and malignant transformation. J Hand Surg Am. 2012 Jun;37(6):1229-34. doi: 10.1016/j.jhsa.2012.03.019. Epub 2012 Apr 27. PubMed PMID: 22542061.
CLINICAL SITUATION FOR QUESTIONS 2 THROUGH 5
A 45-year-old man injured his arm when it was forcibly extended while he was flexing his elbow. He notes swelling in the antecubital fossa and arm weakness. The physician suspects a distal biceps rupture.
immobilization would allow fracture healing, and then curettage with bone graft can be performed after healing occurs.
RECOMMENDED READINGS
1. Jacobson ME, Ruff ME. Solitary enchondroma of the phalanx. J Hand Surg Am. 2011 Nov;36(11):1845-7. doi: 10.1016/j.jhsa.2011.05.002. Epub 2011 Jun 11. Review. PubMed PMID: 21658859.
2. Sassoon AA, Fitz-Gibbon PD, Harmsen WS, Moran SL. Enchondromas of the hand: factors affecting recurrence, healing, motion, and malignant transformation. J Hand Surg Am. 2012 Jun;37(6):1229-34. doi: 10.1016/j.jhsa.2012.03.019. Epub 2012 Apr 27. PubMed PMID: 22542061.
CLINICAL SITUATION FOR QUESTIONS 2 THROUGH 5
A 45-year-old man injured his arm when it was forcibly extended while he was flexing his elbow. He notes swelling in the antecubital fossa and arm weakness. The physician suspects a distal biceps rupture.
QUESTION 2
of 100
Video 2 shows the squeeze test for a biceps tendon rupture. This test

Video 2 shows the squeeze test for a biceps tendon rupture. This test
1
is performed with the elbow in flexion to minimize the function of the brachialis.
2
can help surgeons evaluate the biceps tendon by lengthening the musculotendinous unit.
3
can help surgeons diagnose a partial biceps tear.
4
likely can generate a false-positive result when the lacertus fibrosus is torn.
- is performed with the elbow in flexion to minimize the function of the brachialis._
QUESTION 3
of 10
A distal biceps repair may be performed through a 1- or 2-incision technique. When comparing the 2 methods, the literature indicates that the 2-incision technique provides
A distal biceps repair may be performed through a 1- or 2-incision technique. When comparing the 2 methods, the literature indicates that the 2-incision technique provides
1
a larger arc of forearm rotation.
2
a more satisfactory clinical result.
3
more anatomic placement of the repair.
4
higher risk for lateral antebrachial cutaneous neuropraxia.
- more anatomic placement of the repair._
QUESTION 4
of 100
Which distal biceps repair technique has the highest load to failure in vitro?
Which distal biceps repair technique has the highest load to failure in vitro?
1
Suspensory cortical button (Endobutton)
2
Suture anchor
3
Transosseous suture
4
Interference screw
- Suspensory cortical button (Endobutton)_
QUESTION 5
of 100
What is the most common complication following distal biceps tendon repair?
What is the most common complication following distal biceps tendon repair?
1
Posterior interosseous nerve palsy
2
Rerupture of the repair
3
Lateral antebrachial cutaneous neuropraxia
4
Superficial radial sensory neuropathy
The distal biceps tendon is commonly torn with an eccentric contraction of the biceps when the elbow is taken into extension. Patients treated nonsurgically will note loss of at least 50% supination strength and may develop discomfort with resistive activities. The video shows the squeeze test to evaluate the integrity of the biceps tendon. The test is similar to the Thompson test in the evaluation of an Achilles tendon rupture. The distal arm is squeezed with the elbow flexed 60 to 80 degrees and the forearm pronated. By shortening the musculotendinous unit, the intact biceps tendon will lead to forearm supination. If the biceps is torn, the forearm will not supinate as shown in the video. The maneuver is performed with the elbow in flexion to minimize tension on the brachialis muscle and isolate the biceps. Ruland and associates evaluated 25 patients with suspected distal biceps ruptures and correctly diagnosed all but 1 false-positive result that involved a partial tear. The lacertus fibrosus is not evaluated with this maneuver.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
QUESTION 6
of 100
Figures 6a and 6b are the radiographs of an injury for which a closed reduction procedure was unsuccessful. A dorsal approach to the metacarpophalangeal (MP) joint is chosen for open reduction. What is the most likely structure to impede the reduction?


Figures 6a and 6b are the radiographs of an injury for which a closed reduction procedure was unsuccessful. A dorsal approach to the metacarpophalangeal (MP) joint is chosen for open reduction. What is the most likely structure to impede the reduction?
1
Flexor tendon
2
Adductor aponeurosis
3
Dorsal capsule
4
Palmar plate
The radiograph shows the proximal phalanx nearly parallel with the metacarpal, where the simple dorsal dislocation of the phalanx is nearly perpendicular to the joint. A simple dislocation can be converted into a complex dislocation with attempts at closed reduction. The palmar plate, which is entrapped within the MP joint, should be incised longitudinally through its midline, allowing the metacarpal head to be reduced. For reduction of a simple dislocation, the wrist should be flexed to allow relaxation of the flexor tendons, and distal traction as well as volar-directed pressure to the base of the proximal phalanx can be successful in reducing a simple dislocation. Surgical reduction can be approached either dorsally or volarly. The volar approach jeopardizes the digital nerve. With a dorsal approach, the extensor hood and dorsal capsule should be incised longitudinally.
RECOMMENDED READINGS
1. Becton JL, Christian JD Jr, Goodwin HN, Jackson JG 3rd. A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am. 1975 Jul;57(5):698-700.
2. Green DP, Terry GC. Complex dislocation of the metacarpophalangeal joint. Correlative pathological anatomy. J Bone Joint Surg Am. 1973 Oct;55(7):1480-6.
RECOMMENDED READINGS
1. Becton JL, Christian JD Jr, Goodwin HN, Jackson JG 3rd. A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am. 1975 Jul;57(5):698-700.
2. Green DP, Terry GC. Complex dislocation of the metacarpophalangeal joint. Correlative pathological anatomy. J Bone Joint Surg Am. 1973 Oct;55(7):1480-6.
QUESTION 7
of 100
The arrow in Figure 7 points to the “teardrop” of the wrist. This radiographic landmark represents which anatomic portion of the wrist?

The arrow in Figure 7 points to the “teardrop” of the wrist. This radiographic landmark represents which anatomic portion of the wrist?
1
Ulnar head
2
Volar ulnar corner
3
Radial styloid
4
Lister tubercle
Medoff described the radiographic teardrop of the distal radius. This radiographic landmark matches the critical volar ulnar corner of the distal radius. A malreduction of the volar ulnar corner of the distal radius in an intra-articular distal radius fracture leads to volar subluxation of the lunate and the rapid development of posttraumatic arthritis at the distal radioulnar and radiolunate joints. Knowledge of the specific shape and appearance of this radiographic landmark helps the surgeon when he or she is critically analyzing postreduction imaging.
The volar portion of the ulnar head may be mistaken for this teardrop sign and should be separately identified as distinct from the distal radius. The radial styloid and Lister tubercle are not part of the volar aspect of the lunate facet.
RECOMMENDED READINGS
1. Medoff RJ. Essential radiographic evaluation for distal radius fractures. Hand Clin. 2005 Aug;21(3):279-88. Review. PubMed PMID: 16039439.
2. Harness NG, Jupiter JB, Orbay JL, Raskin KB, Fernandez DL. Loss of fixation of the volar lunate facet fragment in fractures of the distal part of the radius. J Bone Joint Surg Am. 2004 Sep;86-A(9):1900-8.
The volar portion of the ulnar head may be mistaken for this teardrop sign and should be separately identified as distinct from the distal radius. The radial styloid and Lister tubercle are not part of the volar aspect of the lunate facet.
RECOMMENDED READINGS
1. Medoff RJ. Essential radiographic evaluation for distal radius fractures. Hand Clin. 2005 Aug;21(3):279-88. Review. PubMed PMID: 16039439.
2. Harness NG, Jupiter JB, Orbay JL, Raskin KB, Fernandez DL. Loss of fixation of the volar lunate facet fragment in fractures of the distal part of the radius. J Bone Joint Surg Am. 2004 Sep;86-A(9):1900-8.
QUESTION 8
of 100
Which ligament is most important in maintaining stability of the scapholunate joint?

Which ligament is most important in maintaining stability of the scapholunate joint?
1
Dorsal scapholunate interosseous
2
Dorsal radiocarpal
3
Proximal (membranous) scapholunate interosseous
4
Volar scapholunate interosseous
Scapholunate instability frequently develops as a consequence of blunt trauma to the wrist and is associated with significant clinical morbidity. The ligamentous anatomy and kinematics of the
carpus are complex and have been the focus of much clinical and biomechanical research. Multiple ligamentous structures contribute to the structure and function of the scapholunate articulation.
The wrist can be viewed as a 3-tiered structure with the forearm bones and carpometacarpal segments separated by the intercalated proximal row. The link between the distal and proximal carpal rows depends in large part on the scapholunate articulation. Instability of this articulation leads to altered kinematics and clinical symptomatology.
Multiple ligaments contribute to scapholunate joint integrity. They can be divided into intrinsic and extrinsic groups. The scapholunate interosseous ligament (SLIL) is described as intrinsic and is a C-shaped ligamentous structure that can be divided into 3 parts for descriptive purposes. The dorsal component is the thickest, with an average thickness of 3 mm and is approximately 5 mm in proximal-distal dimension. It attaches the proximal pole of the scaphoid to the dorsal aspect of the lunate. The proximal component has variable thickness and is composed largely of fibrocartilage. The volar component averages only 1 mm in thickness and 5 mm in proximal-distal dimension. It merges with the radioscapholunate ligament proximally and with the radioscaphocapitate (RSC) ligament distally. The other stabilizers are referred to as extrinsic because they connect the scaphoid and lunate to the radius and other carpal bones. Several ligaments at the palmar aspect of the carpus contribute to scapholunate stability. The RSC ligament runs from the radial styloid to the scaphoid fossa. The long radiolunate ligament (LRL) extends from the volar radius to the volar lunate. The radioscapholunate ligament (RSL) attaches the volar distal radius to the volar aspect of the SLIL. The scaphotrapezial ligament (ST) attaches the distal pole of the scaphoid to the trapezium.
Other extrinsic ligaments contributing to scapholunate stability are found at the dorsal aspect of the carpus. The dorsal radiocarpal ligament (DRC) originates from the dorsal distal radius and inserts onto the dorsum of the lunate, triquetrum, and lunotriquetral interosseous ligament. The dorsal intercarpal ligament (DIC) attaches to the dorsum of the triquetrum and extends radially, past the lunate, to insert on the dorsal distal pole of the scaphoid.
Although the exact contribution of each ligament to scapholunate stability is not fully understood, some interesting observations have been made. The SLIL appears to be the primary stabilizing structure. Sectioning the SLIL alone, without disturbing the extrinsic stabilizers, leads to substantial widening of the scapholunate interval and altered motion patterns of both the scaphoid and lunate. Sectioning the RSC and ST ligaments with an intact SLIL does not significantly alter scaphoid or lunate kinematics with respect to motion in the flexion-extension and radial-ulnar planes. Similarly, sectioning of the ST and DIC ligaments by another study group demonstrated no alterations in scapholunate motion, whereas DRC sectioning led to only modest ulnar deviation of the lunate. Although many ligaments contribute to the stability of the scapholunate joint, the SLIL appears to be the primary stabilizer. The most robust and functionally important part of the SLIL appears to be the dorsal component. The role of the secondary stabilizers is significant, and more work is necessary to fully understand their contributions.
RECOMMENDED READINGS
1. [Rajan PV, Day CS. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. Review. PubMed PMID: 26143029.](http://www.ncbi.nlm.nih.gov/pubmed/26143029)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26143029)
2. Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg Am. 1985 Jul;10(4):492-8. PubMed PMID: 4020059.
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005 Jan;30(1):24-34. PubMed PMID: 15680552.
4. Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part III. J Hand Surg Am. 2007 Mar;32(3):297-309.
**Question 9 of 100**
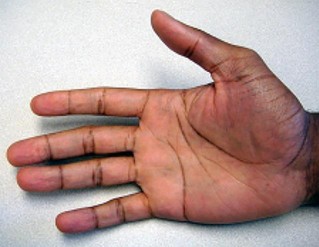
Figures 9a and 9b are the clinical photographs of a 22-year-old man who was injured 1 year ago when he grasped an opponent during a football game. He experienced immediate pain and has been unable to close his ring finger into a fist since then. He also has noticed swelling and a painful lump in his palm with attempted forceful gripping. What is the most likely diagnosis
1. Lumbrical plus finger
2. Distal rupture of the profundus tendon with entrapment at the superficialis chiasm
3. Distal rupture of the profundus tendon with the proximal tendon stump in the palm
4. Quadrigia
_PREFERRED RESPONSE: 3- Distal rupture of the profundus tendon with the proximal tendon stump in the palm_
**DISCUSSION**
The most common location (ring) and mechanism at which the flexor digitorum profundus (FDP) tendon ruptures resulting in a jersey finger (rupture of the FDP with attempted active flexion while the finger is being forcibly extended) is at its distal insertion at the base of the distal phalanx (as in the description of a player attempting to escape another player’s grasp). The proximal tendon stump often retracts into the palm where it forms a tender lump. This patient can passively flex but has no ability to actively flex the distal interphalangeal joint. Although this is a classic description, this injury also can occur during an altercation or when attempting to separate fighting dogs by the collar, for example.
A lumbrical plus deformity may result from this injury, but that is not demonstrated in these clinical photographs. Lumbrical plus would demonstrate paradoxical extension of the proximal interphalangeal (PIP) joint with attempted active flexion, secondary to a proximally retracted FDP that is applying progressive tension to its lumbrical. This PIP extension worsens with attempted active flexion because there is increasingly more tension applied to the lumbrical.
carpus are complex and have been the focus of much clinical and biomechanical research. Multiple ligamentous structures contribute to the structure and function of the scapholunate articulation.
The wrist can be viewed as a 3-tiered structure with the forearm bones and carpometacarpal segments separated by the intercalated proximal row. The link between the distal and proximal carpal rows depends in large part on the scapholunate articulation. Instability of this articulation leads to altered kinematics and clinical symptomatology.
Multiple ligaments contribute to scapholunate joint integrity. They can be divided into intrinsic and extrinsic groups. The scapholunate interosseous ligament (SLIL) is described as intrinsic and is a C-shaped ligamentous structure that can be divided into 3 parts for descriptive purposes. The dorsal component is the thickest, with an average thickness of 3 mm and is approximately 5 mm in proximal-distal dimension. It attaches the proximal pole of the scaphoid to the dorsal aspect of the lunate. The proximal component has variable thickness and is composed largely of fibrocartilage. The volar component averages only 1 mm in thickness and 5 mm in proximal-distal dimension. It merges with the radioscapholunate ligament proximally and with the radioscaphocapitate (RSC) ligament distally. The other stabilizers are referred to as extrinsic because they connect the scaphoid and lunate to the radius and other carpal bones. Several ligaments at the palmar aspect of the carpus contribute to scapholunate stability. The RSC ligament runs from the radial styloid to the scaphoid fossa. The long radiolunate ligament (LRL) extends from the volar radius to the volar lunate. The radioscapholunate ligament (RSL) attaches the volar distal radius to the volar aspect of the SLIL. The scaphotrapezial ligament (ST) attaches the distal pole of the scaphoid to the trapezium.
Other extrinsic ligaments contributing to scapholunate stability are found at the dorsal aspect of the carpus. The dorsal radiocarpal ligament (DRC) originates from the dorsal distal radius and inserts onto the dorsum of the lunate, triquetrum, and lunotriquetral interosseous ligament. The dorsal intercarpal ligament (DIC) attaches to the dorsum of the triquetrum and extends radially, past the lunate, to insert on the dorsal distal pole of the scaphoid.
Although the exact contribution of each ligament to scapholunate stability is not fully understood, some interesting observations have been made. The SLIL appears to be the primary stabilizing structure. Sectioning the SLIL alone, without disturbing the extrinsic stabilizers, leads to substantial widening of the scapholunate interval and altered motion patterns of both the scaphoid and lunate. Sectioning the RSC and ST ligaments with an intact SLIL does not significantly alter scaphoid or lunate kinematics with respect to motion in the flexion-extension and radial-ulnar planes. Similarly, sectioning of the ST and DIC ligaments by another study group demonstrated no alterations in scapholunate motion, whereas DRC sectioning led to only modest ulnar deviation of the lunate. Although many ligaments contribute to the stability of the scapholunate joint, the SLIL appears to be the primary stabilizer. The most robust and functionally important part of the SLIL appears to be the dorsal component. The role of the secondary stabilizers is significant, and more work is necessary to fully understand their contributions.
RECOMMENDED READINGS
1. [Rajan PV, Day CS. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. Review. PubMed PMID: 26143029.](http://www.ncbi.nlm.nih.gov/pubmed/26143029)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26143029)
2. Drewniany JJ, Palmer AK, Flatt AE. The scaphotrapezial ligament complex: an anatomic and biomechanical study. J Hand Surg Am. 1985 Jul;10(4):492-8. PubMed PMID: 4020059.
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005 Jan;30(1):24-34. PubMed PMID: 15680552.
4. Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part III. J Hand Surg Am. 2007 Mar;32(3):297-309.
**Question 9 of 100**
Figures 9a and 9b are the clinical photographs of a 22-year-old man who was injured 1 year ago when he grasped an opponent during a football game. He experienced immediate pain and has been unable to close his ring finger into a fist since then. He also has noticed swelling and a painful lump in his palm with attempted forceful gripping. What is the most likely diagnosis
1. Lumbrical plus finger
2. Distal rupture of the profundus tendon with entrapment at the superficialis chiasm
3. Distal rupture of the profundus tendon with the proximal tendon stump in the palm
4. Quadrigia
_PREFERRED RESPONSE: 3- Distal rupture of the profundus tendon with the proximal tendon stump in the palm_
**DISCUSSION**
The most common location (ring) and mechanism at which the flexor digitorum profundus (FDP) tendon ruptures resulting in a jersey finger (rupture of the FDP with attempted active flexion while the finger is being forcibly extended) is at its distal insertion at the base of the distal phalanx (as in the description of a player attempting to escape another player’s grasp). The proximal tendon stump often retracts into the palm where it forms a tender lump. This patient can passively flex but has no ability to actively flex the distal interphalangeal joint. Although this is a classic description, this injury also can occur during an altercation or when attempting to separate fighting dogs by the collar, for example.
A lumbrical plus deformity may result from this injury, but that is not demonstrated in these clinical photographs. Lumbrical plus would demonstrate paradoxical extension of the proximal interphalangeal (PIP) joint with attempted active flexion, secondary to a proximally retracted FDP that is applying progressive tension to its lumbrical. This PIP extension worsens with attempted active flexion because there is increasingly more tension applied to the lumbrical.
QUESTION 9
is iatrogenic secondary to a distal advancement of the FDP or a repair in the setting of tendon substance loss. Either of these pulls the FDP too far distally. Because the long ring and small finger FDP tendons are interconnected through a common muscle belly, pulling 1 tendon distally effectively pulls the others distally. Then, with attempted active flexion, there is not enough excursion of the profundi to fully flex the fingers, and a flexor lag is seen in the ulnar 3 digits. The index can be spared because its FDP is often functionally separate from the others. An entrapment of the FDP at the superficialis chiasm may produce a triggering or a mass overlying Camper chiasm at the level of the proximal phalanx and not the palm. With the exception of the small finger, rupture of the FDP in the palm is rare.
RECOMMENDED READINGS




RECOMMENDED READINGS
1
[Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg Am. 1977 Jan; 2(1):66-9. PubMed PMID: 839056.](http://www.ncbi.nlm.nih.gov/pubmed/839056)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/839056)
2
Imbriglia JE, Goldstein SA. Intratendinous ruptures of the flexor digitorum profundus tendon of the small finger. J Hand Surg Am. 1987 Nov; 12(6):985-91. PubMed PMID: 3693855
**Question 10 of 100**
When treating the injury shown in Figure 10, what is the most important indication for surgery?

3
Clinical appearance
4
Joint subluxation
5
Patient age
The injury depicted in Figure 10 is a Bennett fracture/subluxation/dislocation. It is an intra-articular fracture separating the volar ulnar aspect of the metacarpal base from the remaining thumb metacarpal. The volar-ulnar fragment (single, variable size) is held in place by its ligamentous attachment to the trapezium, known as the anterior oblique ligament. The metacarpal shaft is displaced in a dorsal and radial direction because of the force of the abductor pollicis longus and adductor pollicis. The main indication for surgery is displacement of this intra-articular injury. Displacement exceeding 2 to 3 mm of the metacarpal shaft or the articular surface is the main indication for surgery. The appearance of the hand is important, but is not an indication for surgery in this scenario. Patients of any age and occupation may be candidates for surgery. A contraindication to surgery could be preexisting substantial osteoarthrosis. For a reducible Bennett fracture/dislocation, a closed reduction and percutaneous fixation with Kirschner wires usually is the recommended treatment. Reduction without fixation does not maintain the reduction. Even if the fracture is nondisplaced or displaced less than 2 to 3 mm, it must be watched carefully. Percutaneous fixation must be considered because of the likelihood for displacement. Reduction is accomplished with longitudinal traction, downward pressure on the base of the thumb
metacarpal with abduction, and extension and pronation of thumb metacarpal. If the fracture is displaced and irreducible, open reduction and internal fixation through a Wagner (volar) incision is recommended. If the fracture/subluxation is reduced and maintained, there is no significant difference in the outcome between closed reduction and pinning and open reduction.
RECOMMENDED READINGS
3. Rivlin M, Fei W, Mudgal CS. Bennett Fracture. J Hand Surg Am. 2015 Aug;40(8):1667-8. doi: 10.1016/j.jhsa.2015.05.017. Epub 2015 Jul 3. Review. PubMed PMID: 26143965.
4. Carlsen BT, Moran SL. Thumb trauma: Bennett fractures, Rolando fractures, and ulnar collateral ligament injuries. J Hand Surg Am. 2009 May-Jun;34(5):945-52. doi: 10.1016/j.jhsa.2009.03.017. Review.
5. Soyer AD. Fractures of the base of the first metacarpal: current treatment options. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):403-12. Review. PubMed PMID: 11505928
**Question 11 of 100**
After biopsy confirmation, the most appropriate treatment for the squamous cell carcinoma of the thumb involving the distal phalanx shown in Figures 11a and 11b is
1. ray amputation.
2. curettage and bone grafting.
3. radiation therapy.
4. amputation at the interphalangeal joint level.
_PREFERRED RESPONSE: 4- amputation at the interphalangeal joint level._
**DISCUSSION**
Squamous cell carcinoma of the fingertip/nail region is uncommon. A high degree of suspicion is needed to diagnose this condition. Radiographs and biopsy are necessary to make the diagnosis. The treatment choice is dependent upon the extent of the lesion at the time of presentation. It can vary from Mohs microsurgery to digital amputation. Amputation is recommended when there is bone involvement. Because the distal phalanx tip is involved and no further bone is involved proximally, an amputation at the interphalangeal joint level is recommended. More proximal involvement would require a more proximal amputation level. Only the distal phalanx is involved. Curettage and bone graft is not appropriate for this malignant lesion. Radiation alone is not an appropriate treatment option for this condition. Metastatic spread is uncommon.
RECOMMENDED READINGS
6. Plate AM, Steiner G, Posner MA. Malignant tumors of the hand and wrist. J Am Acad Orthop Surg. 2006 Nov;14(12):680-92. PubMed PMID: 17077340.
7. Askari M, Kakar S, Moran SL. Squamous cell carcinoma of the hand: a 20-year review. J Hand Surg Am. 2013 Nov;38(11):2124-33. doi: 10.1016/j.jhsa.2013.08.090. Epub 2013 Sep 17.
**Question 12 of 100**
Figure 12 is a radiograph of a 60-year-old woman with symptomatic thumb basal joint arthritis. Which procedure should be performed in addition to a trapeziectomy to improve her prognosis for long-term pain relief?
1. Ligament reconstruction and tendon interposition
2. Excision of the proximal third of the trapezoid
3. Thumb metacarpophalangeal (MP) fusion
4. Prosthetic trapeziometacarpal arthroplasty
_PREFERRED RESPONSE: 2- Excision of the proximal third of the trapezoid_
**DISCUSSION**
Multiple factors can lead to incomplete pain relief following trapeziectomy. The prevalence of concomitant scaphotrapezoid arthritis at the time of trapeziectomy has been reported by Tomaino and associates to be as high as 62%. This patient’s radiographs demonstrate scaphotrapezoid arthritis in addition to Eaton stage IV pantrapezial arthritis. Resection of the proximal third of the trapezoid should be considered at the time of surgery. There are no significant arthritic changes at the MP joint, precluding the need for MP arthrodesis. Hematoma arthroplasty involves resection of the trapezium and pinning the thumb metacarpal without ligament reconstruction. The results of hematoma arthroplasty are comparable to trapezium resection with ligament reconstruction. Prosthetic implant arthroplasty will address the trapeziometacarpal arthritis. The implants have demonstrated acceptable short-term results but are associated with a high complication rate, and revision often is necessary.
RECOMMENDED READINGS
8. [Tomaino MM, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am. 1999 Nov;24(6):1220-4. PubMed PMID: 10584944.](http://www.ncbi.nlm.nih.gov/pubmed/10584944)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10584944)
9. [Berger AJ, Meals RA. Management of osteoarthrosis of the thumb joints. J Hand Surg Am. 2015 Apr;40(4):843-50. doi: 10.1016/j.jhsa.2014.11.026. Epub 2015 Mar 6. Review. PubMed PMID: 25754790.](http://www.ncbi.nlm.nih.gov/pubmed/25754790)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25754790)
metacarpal with abduction, and extension and pronation of thumb metacarpal. If the fracture is displaced and irreducible, open reduction and internal fixation through a Wagner (volar) incision is recommended. If the fracture/subluxation is reduced and maintained, there is no significant difference in the outcome between closed reduction and pinning and open reduction.
RECOMMENDED READINGS
3. Rivlin M, Fei W, Mudgal CS. Bennett Fracture. J Hand Surg Am. 2015 Aug;40(8):1667-8. doi: 10.1016/j.jhsa.2015.05.017. Epub 2015 Jul 3. Review. PubMed PMID: 26143965.
4. Carlsen BT, Moran SL. Thumb trauma: Bennett fractures, Rolando fractures, and ulnar collateral ligament injuries. J Hand Surg Am. 2009 May-Jun;34(5):945-52. doi: 10.1016/j.jhsa.2009.03.017. Review.
5. Soyer AD. Fractures of the base of the first metacarpal: current treatment options. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):403-12. Review. PubMed PMID: 11505928
**Question 11 of 100**
After biopsy confirmation, the most appropriate treatment for the squamous cell carcinoma of the thumb involving the distal phalanx shown in Figures 11a and 11b is
1. ray amputation.
2. curettage and bone grafting.
3. radiation therapy.
4. amputation at the interphalangeal joint level.
_PREFERRED RESPONSE: 4- amputation at the interphalangeal joint level._
**DISCUSSION**
Squamous cell carcinoma of the fingertip/nail region is uncommon. A high degree of suspicion is needed to diagnose this condition. Radiographs and biopsy are necessary to make the diagnosis. The treatment choice is dependent upon the extent of the lesion at the time of presentation. It can vary from Mohs microsurgery to digital amputation. Amputation is recommended when there is bone involvement. Because the distal phalanx tip is involved and no further bone is involved proximally, an amputation at the interphalangeal joint level is recommended. More proximal involvement would require a more proximal amputation level. Only the distal phalanx is involved. Curettage and bone graft is not appropriate for this malignant lesion. Radiation alone is not an appropriate treatment option for this condition. Metastatic spread is uncommon.
RECOMMENDED READINGS
6. Plate AM, Steiner G, Posner MA. Malignant tumors of the hand and wrist. J Am Acad Orthop Surg. 2006 Nov;14(12):680-92. PubMed PMID: 17077340.
7. Askari M, Kakar S, Moran SL. Squamous cell carcinoma of the hand: a 20-year review. J Hand Surg Am. 2013 Nov;38(11):2124-33. doi: 10.1016/j.jhsa.2013.08.090. Epub 2013 Sep 17.
**Question 12 of 100**
Figure 12 is a radiograph of a 60-year-old woman with symptomatic thumb basal joint arthritis. Which procedure should be performed in addition to a trapeziectomy to improve her prognosis for long-term pain relief?
1. Ligament reconstruction and tendon interposition
2. Excision of the proximal third of the trapezoid
3. Thumb metacarpophalangeal (MP) fusion
4. Prosthetic trapeziometacarpal arthroplasty
_PREFERRED RESPONSE: 2- Excision of the proximal third of the trapezoid_
**DISCUSSION**
Multiple factors can lead to incomplete pain relief following trapeziectomy. The prevalence of concomitant scaphotrapezoid arthritis at the time of trapeziectomy has been reported by Tomaino and associates to be as high as 62%. This patient’s radiographs demonstrate scaphotrapezoid arthritis in addition to Eaton stage IV pantrapezial arthritis. Resection of the proximal third of the trapezoid should be considered at the time of surgery. There are no significant arthritic changes at the MP joint, precluding the need for MP arthrodesis. Hematoma arthroplasty involves resection of the trapezium and pinning the thumb metacarpal without ligament reconstruction. The results of hematoma arthroplasty are comparable to trapezium resection with ligament reconstruction. Prosthetic implant arthroplasty will address the trapeziometacarpal arthritis. The implants have demonstrated acceptable short-term results but are associated with a high complication rate, and revision often is necessary.
RECOMMENDED READINGS
8. [Tomaino MM, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am. 1999 Nov;24(6):1220-4. PubMed PMID: 10584944.](http://www.ncbi.nlm.nih.gov/pubmed/10584944)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10584944)
9. [Berger AJ, Meals RA. Management of osteoarthrosis of the thumb joints. J Hand Surg Am. 2015 Apr;40(4):843-50. doi: 10.1016/j.jhsa.2014.11.026. Epub 2015 Mar 6. Review. PubMed PMID: 25754790.](http://www.ncbi.nlm.nih.gov/pubmed/25754790)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25754790)
QUESTION 10
of 100
A functional nerve transfer involves
A functional nerve transfer involves
1
transection of a nonfunctioning nerve fascicle(s) with transfer to a nonfunctioning nerve.
2
transection of a functioning nerve fascicle(s) with transfer to a nonfunctioning nerve.
3
growing nerve fibers across a gap using a nerve growth factor scaffold.
4
implanting a neuromatous nerve end into neighboring muscle.
Nerve transfer can provide some function to a functionless nerve. Typically, nerve transfer includes intrafascicular dissection; cutting of a functioning nerve fascicle; and suturing the
released, functioning nerve fascicle to a nonfunctioning nerve branch. A common application of nerve transfer in the upper extremity involves attachment of a functioning motor fascicle of the ulnar nerve to the nonfunctioning musculocutaneous branch to the biceps muscle to restore active elbow flexion in patients with nerve root avulsion brachial plexus injuries. Motor nerves can be transferred to other motor nerves, and sensory nerves can be transferred to other sensory nerves. Treatment of acute nerve gaps with nerve grafting, conduits, or nerve growth factors does not describe nerve transfer. Although implanting neuromas into neighboring muscle tissue can decrease symptoms related to the neuroma, this does not describe a nerve transfer, and a neuroma cannot reinnervate a muscle.
RECOMMENDED READINGS
10. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. doi: 10.1016/j.jhsa.2009.12.002. Review. PubMed PMID: 20141906.
11. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
released, functioning nerve fascicle to a nonfunctioning nerve branch. A common application of nerve transfer in the upper extremity involves attachment of a functioning motor fascicle of the ulnar nerve to the nonfunctioning musculocutaneous branch to the biceps muscle to restore active elbow flexion in patients with nerve root avulsion brachial plexus injuries. Motor nerves can be transferred to other motor nerves, and sensory nerves can be transferred to other sensory nerves. Treatment of acute nerve gaps with nerve grafting, conduits, or nerve growth factors does not describe nerve transfer. Although implanting neuromas into neighboring muscle tissue can decrease symptoms related to the neuroma, this does not describe a nerve transfer, and a neuroma cannot reinnervate a muscle.
RECOMMENDED READINGS
10. Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. doi: 10.1016/j.jhsa.2009.12.002. Review. PubMed PMID: 20141906.
11. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
QUESTION 11
of 100
Four months after sustaining a severe crush injury to his dominant right hand, a 28-year-old man continues to report painless hand stiffness with limited grip strength. Initial and subsequent radiographs demonstrate no fracture. He has been treated with 12 weeks of supervised hand therapy without experiencing substantial improvement and has not received surgical treatment. An examination reveals no substantial hand swelling. There is a noteworthy limitation of proximal interphalangeal (PIP) flexion with the metacarpophalangeal (MP) joints in extension, with near-full PIP motion with the MP joints flexed. The most appropriate course of treatment is
Four months after sustaining a severe crush injury to his dominant right hand, a 28-year-old man continues to report painless hand stiffness with limited grip strength. Initial and subsequent radiographs demonstrate no fracture. He has been treated with 12 weeks of supervised hand therapy without experiencing substantial improvement and has not received surgical treatment. An examination reveals no substantial hand swelling. There is a noteworthy limitation of proximal interphalangeal (PIP) flexion with the metacarpophalangeal (MP) joints in extension, with near-full PIP motion with the MP joints flexed. The most appropriate course of treatment is
1
continued therapy with dynamic splinting.
2
extensor tenolysis.
3
stellate ganglion blocks.
4
distal intrinsic releases.
This patient has classic intrinsic tightness following a severe crush injury to the hand. It is possible that there has been an unrecognized compartment syndrome of the hand as a result of the trauma. An examination reveals findings consistent with intrinsic tightness with limited PIP flexion while the MP joints are fully extended, with greater PIP flexion with the MP joints flexed. Considering
that this patient’s condition has not improved with 12 weeks of supervised therapy, it is unlikely that further therapy will be of benefit. Because his stiffness is not associated with pain, complex regional pain syndrome is not a consideration. Extensor tenolysis is not an appropriate treatment option because the examination is not consistent with extensor tendon tightness. The most appropriate treatment consists of distal intrinsic releases followed by supervised hand therapy. Subtle degrees of intrinsic tightness are often missed, and a high index of suspicion must be maintained when patients describe weakness and stiffness following hand trauma.
RECOMMENDED READINGS
12. BUNNELL S. Ischaemic contracture, local, in the hand. J Bone Joint Surg Am. 1953 Jan;35-A(1):88-
101/. PubMed PMID: 13022710. View Abstract at PubMed
13. HARRIS C Jr, RIORDAN DC. Intrinsic contracture in the hand and its surgical treatment. J Bone Joint Surg Am. 1954 Jan;36-A(1):10-20. PubMed PMID: 13130583.Abstract at PubMed
14. Smith RJ. Balance and kinetics of the fingers under normal and pathological conditions. Clin Orthop Relat Res. 1974 Oct;(104):92-111. PubMed PMID: 4412165.Abstract at PubMed
that this patient’s condition has not improved with 12 weeks of supervised therapy, it is unlikely that further therapy will be of benefit. Because his stiffness is not associated with pain, complex regional pain syndrome is not a consideration. Extensor tenolysis is not an appropriate treatment option because the examination is not consistent with extensor tendon tightness. The most appropriate treatment consists of distal intrinsic releases followed by supervised hand therapy. Subtle degrees of intrinsic tightness are often missed, and a high index of suspicion must be maintained when patients describe weakness and stiffness following hand trauma.
RECOMMENDED READINGS
12. BUNNELL S. Ischaemic contracture, local, in the hand. J Bone Joint Surg Am. 1953 Jan;35-A(1):88-
101/. PubMed PMID: 13022710. View Abstract at PubMed
13. HARRIS C Jr, RIORDAN DC. Intrinsic contracture in the hand and its surgical treatment. J Bone Joint Surg Am. 1954 Jan;36-A(1):10-20. PubMed PMID: 13130583.Abstract at PubMed
14. Smith RJ. Balance and kinetics of the fingers under normal and pathological conditions. Clin Orthop Relat Res. 1974 Oct;(104):92-111. PubMed PMID: 4412165.Abstract at PubMed
QUESTION 12
of 100
Figures 15a and 15b are the radiographs of a 36-year-old right-hand-dominant man who has had persistent wrist pain for 6 months after a motor vehicle collision. The initial treatment was splint immobilization. What is the best next step?


Figures 15a and 15b are the radiographs of a 36-year-old right-hand-dominant man who has had persistent wrist pain for 6 months after a motor vehicle collision. The initial treatment was splint immobilization. What is the best next step?
1
Therapy/rehabilitation
2
Open reduction and internal fixation (ORIF)
3
Proximal row carpectomy
4
Wrist arthrodesis
This patient has a chronic untreated volar lunate dislocation. Lunate dislocations are usually the result of a high-energy injury. Recommended treatment for an acute lunate dislocation is ORIF with repair of injured structures (ligament and bone). If the patient has paresthesias in a median nerve distribution, carpal tunnel release is recommended in the same setting as ORIF. Six months after injury, the prognosis for successful ORIF is poor and proximal row carpectomy is recommended. Among perilunate/lunate dislocations, 25% are initially missed. If a patient arrives for treatment and there is evidence of radiocarpal and midcarpal arthrosis, wrist arthrodesis is recommended.
RECOMMENDED READINGS
15. Stanbury SJ, Elfar JC. Perilunate dislocation and perilunate fracture-dislocation. J Am Acad Orthop Surg. 2011 Sep;19(9):554-62. Review. PubMed PMID: 21885701.View Abstract at PubMed
16. Budoff JE. Treatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008 Oct;33(8):1424-32. doi: 10.1016/j.jhsa.2008.07.016. Review. PubMed PMID: 18929215.
RECOMMENDED READINGS
15. Stanbury SJ, Elfar JC. Perilunate dislocation and perilunate fracture-dislocation. J Am Acad Orthop Surg. 2011 Sep;19(9):554-62. Review. PubMed PMID: 21885701.View Abstract at PubMed
16. Budoff JE. Treatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008 Oct;33(8):1424-32. doi: 10.1016/j.jhsa.2008.07.016. Review. PubMed PMID: 18929215.
QUESTION 13
of 100
Distal pole scaphoid excision is contraindicated for patients with
Distal pole scaphoid excision is contraindicated for patients with
1
carpal instability.
2
scaphotrapezotrapezoidal (STT) arthritis.
3
failed STT arthrodesis.
4
distal scaphoid nonunion.
Distal pole scaphoid excision is a surgical option for STT arthritis, a failed STT arthrodesis, and distal pole scaphoid nonunion involving the distal 25% of the scaphoid. Distal pole scaphoid excision may lead to a nondissociative intercalated segment instability pattern, so carpal instability is a contraindication. Presurgical assessment for a dorsally unstable midcarpal joint should be performed. This procedure involves excision of the distal quarter of the scaphoid with postsurgical immobilization for 4 to 6 weeks. STT arthrodesis is a technically demanding procedure with reported complication rates as high as 78%. Postsurgical immobilization is continued for 6 to 8 weeks until evidence of STT fusion healing is seen.
RECOMMENDED READINGS
17. Garcia-Elias M. Excisional arthroplasty for scaphotrapeziotrapezoidal osteoarthritis. J Hand Surg Am. 2011 Mar;36(3):516-20. doi: 10.1016/j.jhsa.2010.12.016. Review. PubMed PMID: 21371628.
18. Zimmermann MS, Weiss AP. Scaphotrapezium-trapezoid arthrosis. J Hand Surg Am. 2012 Oct;37(10):2139-41; quiz 2141. doi: 10.1016/j.jhsa.2012.05.007. Epub 2012 Jul 3. Review.
RECOMMENDED READINGS
17. Garcia-Elias M. Excisional arthroplasty for scaphotrapeziotrapezoidal osteoarthritis. J Hand Surg Am. 2011 Mar;36(3):516-20. doi: 10.1016/j.jhsa.2010.12.016. Review. PubMed PMID: 21371628.
18. Zimmermann MS, Weiss AP. Scaphotrapezium-trapezoid arthrosis. J Hand Surg Am. 2012 Oct;37(10):2139-41; quiz 2141. doi: 10.1016/j.jhsa.2012.05.007. Epub 2012 Jul 3. Review.
QUESTION 14
of 100
What is the most common site of nerve compression in radial tunnel syndrome?

What is the most common site of nerve compression in radial tunnel syndrome?
1
Fibrous bands anterior to the radiocapitellar joint
2
Recurrent radial vessels
3
Medial edge of the extensor carpi radialis brevis (ECRB)
4
Proximal aponeurotic edge of the supinator (arcade of Frohse)
Radial tunnel syndrome occurs as the result of radial nerve compression at 5 potential sites. These are the fibrous bands anterior to the radiocapitellar joint, the radial recurrent vessels (known as the leash of Henry), the medial edge of the ECRB, the proximal aponeurotic edge of the supinator (arcade of Frohse), and the distal edge of the supinator. The arcade of Frohse is the most common site of compression. The chief discomfort is deep, aching pain in the dorsoradial proximal forearm. Motor and sensory symptoms usually are absent. This condition often is seen when pain persists after surgery for lateral epicondylitis. Lateral epicondylitis and radial tunnel syndrome coexist 5% of the time.
Examination findings are tenderness 4 cm distal to the lateral epicondyle, pain with resisted supination, and pain with resisted long finger extension. Electromyogram/nerve conduction study and MRI results usually are normal. A steroid injection can be diagnostic and also may provide temporary relief of symptoms. Surgery involves decompression of all potential areas of compression and allows good to excellent results in only 50% to 90% of cases. Symptoms may take 9 to 18 months to resolve after surgery.
RECOMMENDED READINGS
19. Lawrence T, Mobbs P, Fortems Y, Stanley JK. Radial tunnel syndrome. A retrospective review of 30 decompressions of the radial nerve. J Hand Surg Br. 1995 Aug;20(4):454-9. PubMed PMID: 7594982.View Abstract at PubMed
20. Lubahn JD, Cermak MB. Uncommon nerve compression syndromes of the upper extremity. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):378-86. Review. PubMed PMID: 9826421.
**CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 21**
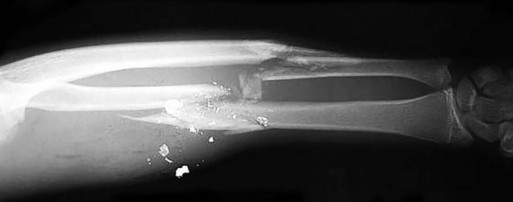
Figures 18a and 18b are the radiographs of a 31-year-old man with an isolated 9-mm gunshot injury to his right forearm. The entry and exit holes are smaller than 1 cm. Motor and sensory function in his right wrist and hand are intact. In the emergency department, the wounds are irrigated and dressed, a long-arm splint is applied, intravenous cefazolin is administered, and a tetanus vaccination is provided. Over the ensuing 2 hours, he experiences increasing pain in his right forearm and new numbness in his right hand. His radial and ulnar arteries remain palpable at the wrist level, and capillary refill is less than 1 second over the digital pulps.
Examination findings are tenderness 4 cm distal to the lateral epicondyle, pain with resisted supination, and pain with resisted long finger extension. Electromyogram/nerve conduction study and MRI results usually are normal. A steroid injection can be diagnostic and also may provide temporary relief of symptoms. Surgery involves decompression of all potential areas of compression and allows good to excellent results in only 50% to 90% of cases. Symptoms may take 9 to 18 months to resolve after surgery.
RECOMMENDED READINGS
19. Lawrence T, Mobbs P, Fortems Y, Stanley JK. Radial tunnel syndrome. A retrospective review of 30 decompressions of the radial nerve. J Hand Surg Br. 1995 Aug;20(4):454-9. PubMed PMID: 7594982.View Abstract at PubMed
20. Lubahn JD, Cermak MB. Uncommon nerve compression syndromes of the upper extremity. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):378-86. Review. PubMed PMID: 9826421.
**CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 21**
Figures 18a and 18b are the radiographs of a 31-year-old man with an isolated 9-mm gunshot injury to his right forearm. The entry and exit holes are smaller than 1 cm. Motor and sensory function in his right wrist and hand are intact. In the emergency department, the wounds are irrigated and dressed, a long-arm splint is applied, intravenous cefazolin is administered, and a tetanus vaccination is provided. Over the ensuing 2 hours, he experiences increasing pain in his right forearm and new numbness in his right hand. His radial and ulnar arteries remain palpable at the wrist level, and capillary refill is less than 1 second over the digital pulps.
QUESTION 15
of 100
What is the most appropriate next step in the treatment of increasing forearm pain and new numbness?
What is the most appropriate next step in the treatment of increasing forearm pain and new numbness?
1
Perform angiography
2
Perform emergent forearm fasciotomies
3
Administer narcotics
4
Obtain forearm compartment pressure measurements
- Obtain forearm compartment pressure measurements_
QUESTION 16
of 100
Which compartment pressure measurement combinations are concerning for compartment syndrome?
Which compartment pressure measurement combinations are concerning for compartment syndrome?
1
15 mm Hg absolute, 40 mm Hg lower than diastolic blood pressure
2
20 mm Hg absolute, 10 mm Hg lower than diastolic blood pressure
3
25 mm Hg absolute, 35 mm Hg lower than diastolic pressure
4
25 mm Hg absolute, 40 mm Hg lower than diastolic pressure
- 20 mm Hg absolute, 10 mm Hg lower than diastolic blood pressure_
QUESTION 17
of 100
Which muscles are in the superficial volar compartment of the forearm?
Which muscles are in the superficial volar compartment of the forearm?
1
Supinator, flexor digitorum profundus, flexor pollicis longus, pronator quadratus
2
Pronator teres, flexor carpi radialis longus, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris
3
Brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis
4
Extensor digitorum communis, extensor carpi ulnaris, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, extensor indicis proprius, extensor digiti minimi
- Pronator teres, flexor carpi radialis longus, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris_
QUESTION 18
of 100
Which principle of fracture fixation should be considered when performing plate fixation of both shaft fractures for this patient?
Which principle of fracture fixation should be considered when performing plate fixation of both shaft fractures for this patient?
1
Compression plating on the compression side of the bone
2
Compression plating on the tension side of the bone
3
Bridge plating
4
Insertion of 4.5-mm rather than 3.5-mm screws
This patient sustained comminuted fractures of the radius and ulna. The radial and ulnar artery pulses are palpable at the wrist, and perfusion to the hand is adequate. Consequently, angiography may not provide useful information. The most appropriate next step is to measure forearm compartment pressures.
A forearm compartment pressure measurement higher than 30 mm Hg, or within 20 mm Hg of the diastolic blood pressure, is concerning for compartment syndrome. There are 4 muscle compartments in the forearm: deep volar, superficial volar, mobile wad, and dorsal. Release of the volar compartments should include the carpal tunnel and may effectively decrease pressures in the dorsal and mobile wad compartments.
Compression plating of diaphyseal radius and ulna fractures is appropriate for management of simple fracture patterns. Compression permits the creation of a near-zero strain environment conducive to primary bone healing. Compression plates are conceptually most effective when placed on the tension side of bone. To minimize strain, there should be at least 6 cortices of screw purchase proximal and distal to the fracture. In most cases, 3.5-mm plate and screws are preferred. Larger, 4.5-mm implants may be more likely to propagate fracture lines in the event of device removal.
Severely comminuted shaft fractures are currently treated with the intention to optimize rather than minimize strain by use of a load-sharing implant. A 2% to 10% strain environment is conducive to callus formation and can be created with bridge plating; insertion of fewer screws that are more widely spaced, and use of either a flexible implant material (eg, titanium) or locked plate. A locked intramedullary nail device can also be used to create a controlled-strain environment; however, angulation and rotation of the fracture can be more difficult to control. Temporary external fixation is considered in the event of severe soft-tissue loss and/or fracture contamination.
RECOMMENDED READINGS
21. Schulte LM, Meals CG, Neviaser RJ. Management of adult diaphyseal both-bone forearm fractures. J Am Acad Orthop Surg. 2014 Jul;22(7):437-46. doi: 10.5435/JAAOS-22-07-437. Review. PubMed PMID: 24966250.
22. Prasarn ML, Ouellette EA. Acute compartment syndrome of the upper extremity. J Am Acad Orthop Surg. 2011 Jan;19(1):49-58. Erratum in: J Am Acad Orthop Surg. 2011 May;19(5):50A. PubMed PMID: 21205767.
23. Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652.
A forearm compartment pressure measurement higher than 30 mm Hg, or within 20 mm Hg of the diastolic blood pressure, is concerning for compartment syndrome. There are 4 muscle compartments in the forearm: deep volar, superficial volar, mobile wad, and dorsal. Release of the volar compartments should include the carpal tunnel and may effectively decrease pressures in the dorsal and mobile wad compartments.
Compression plating of diaphyseal radius and ulna fractures is appropriate for management of simple fracture patterns. Compression permits the creation of a near-zero strain environment conducive to primary bone healing. Compression plates are conceptually most effective when placed on the tension side of bone. To minimize strain, there should be at least 6 cortices of screw purchase proximal and distal to the fracture. In most cases, 3.5-mm plate and screws are preferred. Larger, 4.5-mm implants may be more likely to propagate fracture lines in the event of device removal.
Severely comminuted shaft fractures are currently treated with the intention to optimize rather than minimize strain by use of a load-sharing implant. A 2% to 10% strain environment is conducive to callus formation and can be created with bridge plating; insertion of fewer screws that are more widely spaced, and use of either a flexible implant material (eg, titanium) or locked plate. A locked intramedullary nail device can also be used to create a controlled-strain environment; however, angulation and rotation of the fracture can be more difficult to control. Temporary external fixation is considered in the event of severe soft-tissue loss and/or fracture contamination.
RECOMMENDED READINGS
21. Schulte LM, Meals CG, Neviaser RJ. Management of adult diaphyseal both-bone forearm fractures. J Am Acad Orthop Surg. 2014 Jul;22(7):437-46. doi: 10.5435/JAAOS-22-07-437. Review. PubMed PMID: 24966250.
22. Prasarn ML, Ouellette EA. Acute compartment syndrome of the upper extremity. J Am Acad Orthop Surg. 2011 Jan;19(1):49-58. Erratum in: J Am Acad Orthop Surg. 2011 May;19(5):50A. PubMed PMID: 21205767.
23. Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652.
QUESTION 19
of 100
A 17-year-old boy has the injury shown in Figure 22. After closed reduction, the joint is stable throughout range of motion. In the absence of appropriate postreduction treatment, what is the most likely outcome?

A 17-year-old boy has the injury shown in Figure 22. After closed reduction, the joint is stable throughout range of motion. In the absence of appropriate postreduction treatment, what is the most likely outcome?
1
Swan-neck deformity
2
Mallet deformity
3
Inability to extend the proximal and distal interphalangeal (DIP) joints
4
Boutonniere deformity
The injury depicted is a volar dislocation of the proximal interphalangeal (PIP) joint. Both dorsal and volar PIP dislocations are associated with injury to the collateral ligaments. However, in a dorsal dislocation, the volar plate is injured; in a volar dislocation, the central slip is either ruptured or detached from its insertion on the base of the middle phalanx. Although closed reduction is appropriate, following reduction, the central slip detachment must be appropriately addressed, either with immobilization of the PIP in extension or with surgical repair. In the absence of surgery, the central slip insufficiency will lead to formation of a boutonniere deformity. A swan-neck deformity will develop with a volar plate injury, causing PIP hyperextension and secondary DIP flexion. Mallet deformity is a flexion deformity of the DIP joint secondary to terminal extensor avulsion from the distal phalanx. A central slip avulsion from the PIP joint will result in a PIP flexion deformity. The triangular ligament ruptures, allowing migration of the lateral bands in a
volar direction, producing a hyperextension posture of the DIP joint with minimal active DIP flexion.
RECOMMENDED READINGS
24. Schernberg F, Elzein F, Gillier P, Gerard Y. Dislocations of the proximal interphalangeal joints of the long fingers. Anatomo-clinical study and therapeutic results. Ann Chir Main. 1982;1(1):18-28. English, French. PubMed PMID: 9303039.View Abstract at PubMed
25. Spinner M, Choi BY. Anterior dislocation of the proximal interphalangeal joint. A cause of rupture of the central slip of the extensor mechanism. J Bone Joint Surg Am. 1970 Oct;52(7):1329-36. PubMed PMID: 5469189.
volar direction, producing a hyperextension posture of the DIP joint with minimal active DIP flexion.
RECOMMENDED READINGS
24. Schernberg F, Elzein F, Gillier P, Gerard Y. Dislocations of the proximal interphalangeal joints of the long fingers. Anatomo-clinical study and therapeutic results. Ann Chir Main. 1982;1(1):18-28. English, French. PubMed PMID: 9303039.View Abstract at PubMed
25. Spinner M, Choi BY. Anterior dislocation of the proximal interphalangeal joint. A cause of rupture of the central slip of the extensor mechanism. J Bone Joint Surg Am. 1970 Oct;52(7):1329-36. PubMed PMID: 5469189.
QUESTION 20
of 100
An 18-year-old man has a closed ring-finger metacarpal shaft fracture. Which finding is an indication that surgery is necessary?

An 18-year-old man has a closed ring-finger metacarpal shaft fracture. Which finding is an indication that surgery is necessary?
1
Transverse fracture
2
Rotation of the fractured finger
3
Spiral fracture
4
Shortening of the fractured finger
Figure 23
Most metacarpal fractures can be treated without surgery. The absolute indications for surgery are open fractures and fractures with rotation that interferes with function (Figure 23). Relative indications include multiple metacarpal fractures and unacceptable angulation (which is somewhat subjective). Transverse fractures and spiral fractures in nonborder digits often are stable. If they
do not have rotation, they can often be treated without surgery. Shortening of the fracture by itself is not an indication for surgery. The capacity of the metaphalangeal joint for active hyperextension often compensates for the extensor lag produced by metacarpal shortening in the clinical setting. A cadaver study revealed that every 2 mm of metacarpal shortening resulted in approximately 7 degrees of extensor lag.
RECOMMENDED READINGS
26. Kozin SH, Thoder JJ, Lieberman G. Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg. 2000 Mar-Apr;8(2):111-21. Review. PubMed PMID: 10799096. View Abstract at PubMed
27. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008 Oct;16(10):586-95. Review. PubMed PMID: 18832602. View Abstract at PubMed
28. Strauch RJ, Rosenwasser MP, Lunt JG. Metacarpal shaft fractures: the effect of shortening on the extensor tendon mechanism. J Hand Surg Am. 1998 May;23(3):519-23. PubMed PMID: 9620194. View Abstract at PubMed
Most metacarpal fractures can be treated without surgery. The absolute indications for surgery are open fractures and fractures with rotation that interferes with function (Figure 23). Relative indications include multiple metacarpal fractures and unacceptable angulation (which is somewhat subjective). Transverse fractures and spiral fractures in nonborder digits often are stable. If they
do not have rotation, they can often be treated without surgery. Shortening of the fracture by itself is not an indication for surgery. The capacity of the metaphalangeal joint for active hyperextension often compensates for the extensor lag produced by metacarpal shortening in the clinical setting. A cadaver study revealed that every 2 mm of metacarpal shortening resulted in approximately 7 degrees of extensor lag.
RECOMMENDED READINGS
26. Kozin SH, Thoder JJ, Lieberman G. Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg. 2000 Mar-Apr;8(2):111-21. Review. PubMed PMID: 10799096. View Abstract at PubMed
27. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008 Oct;16(10):586-95. Review. PubMed PMID: 18832602. View Abstract at PubMed
28. Strauch RJ, Rosenwasser MP, Lunt JG. Metacarpal shaft fractures: the effect of shortening on the extensor tendon mechanism. J Hand Surg Am. 1998 May;23(3):519-23. PubMed PMID: 9620194. View Abstract at PubMed
QUESTION 21
of 100
Surgeons can improve the biomechanical stability of a zone II flexor tendon suture repair by
Surgeons can improve the biomechanical stability of a zone II flexor tendon suture repair by
1
avoiding the use of an epitendinous suture.
2
locking the tendon with the core suture.
3
using a fine-caliber suture.
4
maintaining the flexor tendon pulleys.
Biomechanical stability of zone II flexor tendon repairs can be improved by increasing the suture spread distance at the repair site (near-far), increasing the number of strands at the repair site, increasing the caliber of the suture, using sutures that lock the tendon, and adding an epitendinous repair circumferentially around the tendon. Although maintaining the flexor tendon pulleys and initiating early active motion benefits the functional outcome, these steps do not impact the biomechanical stability of the flexor tendon repair. However, they add more biomechanical stress on the repair site.
RECOMMENDED READINGS
29. [Barrie KA, Wolfe SW, Shean C, Shenbagamurthi D, Slade JF 3rd, Panjabi MM. A biomechanical comparison of multistrand flexor tendon repairs using an in situ testing model. J Hand Surg Am. 2000 May;25(3):499-506. PubMed PMID: 10811755. ](http://www.ncbi.nlm.nih.gov/pubmed/10811755)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10811755)
30. [Lee SK, Goldstein RY, Zingman A, Terranova C, Nasser P, Hausman MR. The effects of core suture purchase on the biomechanical characteristics of a multistrand locking flexor tendon repair: a cadaveric study. J Hand Surg Am. 2010 Jul;35(7):1165-71. doi: 10.1016/j.jhsa.2010.04.003. Epub 2010 Jun 11. PubMed PMID: 20541326. ](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)
31. Miller B, Dodds SD, deMars A, Zagoreas N, Waitayawinyu T, Trumble TE. Flexor tendon repairs: the impact of fiberwire on grasping and locking core sutures. J Hand Surg Am. 2007 May-Jun;32(5):591-
[6/. PubMed PMID: 17481994. ](http://www.ncbi.nlm.nih.gov/pubmed/17481994)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17481994)
32. [Boyer MI, Strickland JW, Engles D, Sachar K, Leversedge FJ. Flexor tendon repair and rehabilitation: state of the art in 2002. Instr Course Lect. 2003;52:137-61. Review. PubMed PMID: 12690845. ](http://www.ncbi.nlm.nih.gov/pubmed/12690845)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690845)
RECOMMENDED READINGS
29. [Barrie KA, Wolfe SW, Shean C, Shenbagamurthi D, Slade JF 3rd, Panjabi MM. A biomechanical comparison of multistrand flexor tendon repairs using an in situ testing model. J Hand Surg Am. 2000 May;25(3):499-506. PubMed PMID: 10811755. ](http://www.ncbi.nlm.nih.gov/pubmed/10811755)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10811755)
30. [Lee SK, Goldstein RY, Zingman A, Terranova C, Nasser P, Hausman MR. The effects of core suture purchase on the biomechanical characteristics of a multistrand locking flexor tendon repair: a cadaveric study. J Hand Surg Am. 2010 Jul;35(7):1165-71. doi: 10.1016/j.jhsa.2010.04.003. Epub 2010 Jun 11. PubMed PMID: 20541326. ](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020541326)
31. Miller B, Dodds SD, deMars A, Zagoreas N, Waitayawinyu T, Trumble TE. Flexor tendon repairs: the impact of fiberwire on grasping and locking core sutures. J Hand Surg Am. 2007 May-Jun;32(5):591-
[6/. PubMed PMID: 17481994. ](http://www.ncbi.nlm.nih.gov/pubmed/17481994)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17481994)
32. [Boyer MI, Strickland JW, Engles D, Sachar K, Leversedge FJ. Flexor tendon repair and rehabilitation: state of the art in 2002. Instr Course Lect. 2003;52:137-61. Review. PubMed PMID: 12690845. ](http://www.ncbi.nlm.nih.gov/pubmed/12690845)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690845)
QUESTION 22
of 100
Figures 25a through 25c are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?




Figures 25a through 25c are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?
1
Early range of motion (ROM) program with a removable short-arm splint
2
Long-arm casting in pronation for 4 weeks
3
Fixation of the ulnar styloid fracture
4
Pin fixation of the DRUJ
Figure 25
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure 25d). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
RECOMMENDED READINGS
33. May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002 Nov;27(6):965-
[71/. PubMed PMID: 12457345.](http://www.ncbi.nlm.nih.gov/pubmed/12457345)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12457345)
34. [Sammer DM, Shah HM, Shauver MJ, Chung KC. The effect of ulnar styloid fractures on patient-rated outcomes after volar locking plating of distal radius fractures. J Hand Surg Am. 2009 Nov;34(9):1595-602. doi: 10.1016/j.jhsa.2009.05.017. PubMed PMID: 19896004. ](http://www.ncbi.nlm.nih.gov/pubmed/19896004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19896004)
35. [Wysocki RW, Ruch DS. Ulnar styloid fracture with distal radius fracture. J Hand Surg Am. 2012 Mar;37(3):568-9. doi: 10.1016/j.jhsa.2011.08.035. Epub 2011 Oct 22. Review. PubMed PMID: 22018474. ](http://www.ncbi.nlm.nih.gov/pubmed/22018474)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22018474)
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure 25d). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
RECOMMENDED READINGS
33. May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002 Nov;27(6):965-
[71/. PubMed PMID: 12457345.](http://www.ncbi.nlm.nih.gov/pubmed/12457345)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12457345)
34. [Sammer DM, Shah HM, Shauver MJ, Chung KC. The effect of ulnar styloid fractures on patient-rated outcomes after volar locking plating of distal radius fractures. J Hand Surg Am. 2009 Nov;34(9):1595-602. doi: 10.1016/j.jhsa.2009.05.017. PubMed PMID: 19896004. ](http://www.ncbi.nlm.nih.gov/pubmed/19896004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19896004)
35. [Wysocki RW, Ruch DS. Ulnar styloid fracture with distal radius fracture. J Hand Surg Am. 2012 Mar;37(3):568-9. doi: 10.1016/j.jhsa.2011.08.035. Epub 2011 Oct 22. Review. PubMed PMID: 22018474. ](http://www.ncbi.nlm.nih.gov/pubmed/22018474)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22018474)
QUESTION 23
of 100
Figures 26a through 26c are the radiographs of a 34-year-old laborer who injured his wrist in high school and has experienced progressive wrist pain despite use of a splint and medications. Which procedure offers the best long-term prognosis for pain relief and improved function for this patient?



Figures 26a through 26c are the radiographs of a 34-year-old laborer who injured his wrist in high school and has experienced progressive wrist pain despite use of a splint and medications. Which procedure offers the best long-term prognosis for pain relief and improved function for this patient?
1
Scapholunate ligament reconstruction
2
Scaphoid excision and 4-corner fusion
3
Scaphoid-trapezium-trapezoid (STT) arthrodesis
4
Proximal row carpectomy (PRC)
This patient likely sustained a scapholunate ligament injury years prior that has led to arthritic changes. The radiographs demonstrate a stage IV scaphoid lunate advanced collapse (SLAC) wrist. Treatment options for a stage IV SLAC wrist include scaphoid excision with 4-corner fusion, full-wrist fusion, or total wrist arthroplasty. Considering the patient’s age and the arthritic changes about the proximal pole of the capitate, scaphoid excision and intercarpal fusion is the most appropriate procedure. Proximal row carpectomy is not indicated because of this patient’s age and arthritic changes about the proximal pole of the capitate. Wall and associates reported a higher probability of failure with PRC among patients younger than age 40. STT arthrodesis is not indicated because this would lead to increased load through the arthritic radio-scaphoid articulation. Scapholunate ligament reconstruction is not appropriate for this patient because of the wrist arthritic changes, which necessitate a salvage procedure.
RECOMMENDED READINGS
36. [Wall LB, Didonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: minimum 20-year followup. J Hand Surg Am. 2013 Aug;38(8):1498-504. doi: 10.1016/j.jhsa.2013.04.028. Epub 2013 Jun 25. PubMed PMID: 23809467. ](http://www.ncbi.nlm.nih.gov/pubmed/23809467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23809467)
37. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013. ](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
CLINICAL SITUATION FOR QUESTIONS 27 THROUGH 30
A 25-year-old teacher has a traumatic fracture-dislocation of the ring finger proximal interphalangeal (PIP) joint. During surgical exploration, comminution of the palmar 60% of the middle phalanx is present, and the dorsal base of the middle phalanx is intact with healthy articular cartilage.
RECOMMENDED READINGS
36. [Wall LB, Didonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: minimum 20-year followup. J Hand Surg Am. 2013 Aug;38(8):1498-504. doi: 10.1016/j.jhsa.2013.04.028. Epub 2013 Jun 25. PubMed PMID: 23809467. ](http://www.ncbi.nlm.nih.gov/pubmed/23809467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23809467)
37. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013. ](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
CLINICAL SITUATION FOR QUESTIONS 27 THROUGH 30
A 25-year-old teacher has a traumatic fracture-dislocation of the ring finger proximal interphalangeal (PIP) joint. During surgical exploration, comminution of the palmar 60% of the middle phalanx is present, and the dorsal base of the middle phalanx is intact with healthy articular cartilage.
QUESTION 24
of 100
PIP stability is dependent upon which percentage of intact middle phalanx articular surface?
PIP stability is dependent upon which percentage of intact middle phalanx articular surface?
1
20%
2
40%
3
60%
4
80%
- 60%_
QUESTION 25
of 100
The most appropriate course of treatment is
The most appropriate course of treatment is
1
extension block splinting.
2
hemi-hamate arthroplasty.
3
implant arthroplasty.
4
volar plate arthroplasty.
- hemi-hamate arthroplasty._
QUESTION 26
of 100
The primary goal of treatment for PIP joint injuries using a hemi-hamate articular graft is to restore
The primary goal of treatment for PIP joint injuries using a hemi-hamate articular graft is to restore
1
concavity of the middle phalangeal base.
2
convexity of the proximal phalangeal condyles.
3
collateral ligament integrity.
4
volar plate integrity.
- concavity of the middle phalangeal base._
QUESTION 27
of 100
The patient develops painful posttraumatic arthritis and marked restriction of motion. Arthrodesis is selected as the next step in treatment. Which degree of flexion is recommended?
The patient develops painful posttraumatic arthritis and marked restriction of motion. Arthrodesis is selected as the next step in treatment. Which degree of flexion is recommended?
1
0
2
20
3
40
4
60
Fractures of the volar base of the middle phalanx are very common injuries. After a congruent reduction, stability of the PIP joint is the most important treatment consideration. If the joint is stable, simple immobilization for comfort followed by early protected motion is adequate treatment. Clinical and cadaveric studies have demonstrated that injuries involving 20% of the volar articular surface of the middle phalanx are uniformly stable, whereas compromise of 60% of the articular surface leads to uniform instability. The threshold at which dorsal subluxation becomes problematic appears to be fractures involving 40% or more of the articular surface. Injuries of this pattern need to be examined carefully for evidence of instability and treated accordingly.
Regarding acute treatment options, extension block splinting is not recommended because of the inherent instability associated with this injury. The case in question involves a young patient; therefore, the use of primary implant arthroplasty is not the treatment of choice. In the ring finger, motion is important for power grip, so arthrodesis should be avoided if a reasonable alternative exists. Volar plate arthroplasty, although an option, has generated disappointing results for longterm joint motion and stability. Hemi-hamate arthroplasty has been described as a useful and predictable method with which to reconstruct the volar base of the middle phalanx in cases in which comminution prevents direct internal fixation. When performing hemi-hamate arthroplasty, a free osteocartilaginous graft is harvested from the dorsal and distal surface of the hamate. Using the portion of the hamate that articulates with the concave contour of the fourth to fifth
carpometacarpal joints provides a midline ridge that approximates that of the native middle phalangeal base.
Reconstruction with hemi-hamate autograft can restore the concavity of the middle phalangeal base in the anteroposterior direction. This concavity provides a volar buttress-to-dorsal subluxation of the middle phalanx. Hemi-hamate grafting is performed to the middle phalanx, not the proximal phalanx. Collateral ligament integrity is generally sacrificed to achieve adequate exposure to perform this procedure. It is not generally necessary to perform formal collateral ligament repair or reconstruction once adequate bony reconstruction is achieved. Volar plate integrity is not the primary aim of hemi-hamate arthroplasty; however, the volar plate is repaired to the middle phalangeal insertion of the collateral ligaments at the conclusion of the procedure.
Arthrodesis of the small joints of the hand is a predictable and effective method with which to control pain and instability when preservation of functional motion is not possible. This procedure offers a lower complication rate than prosthetic arthroplasty and yields satisfactory functional results. The trend is to favor arthrodesis for the radial digits and arthroplasty for the ulnar digits because of the importance of PIP flexion in the ulnar digits for power grip. Another consideration is age; younger, more active patients are more prone to eventual prosthetic failure and recurrence of digital deformity. A variety of recommendations have been made by various authors regarding the optimal position for PIP arthrodesis. The consensus is that approximately 40 degrees of flexion is optimal for the ring finger PIP joint.
RECOMMENDED READINGS
1. [Tyser AR, Tsai MA, Parks BG, Means KR Jr. Stability of acute dorsal fracture dislocations of the proximal interphalangeal joint: a biomechanical study. J Hand Surg Am. 2014 Jan;39(1):13-8. doi: 10.1016/j.jhsa.2013.09.025. Epub 2013 Nov 6. PubMed PMID: 24211175.](http://www.ncbi.nlm.nih.gov/pubmed/24211175)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24211175)
2. [Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519. ](http://www.ncbi.nlm.nih.gov/pubmed/14507519)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14507519)
3. [Capo JT, Hastings H 2nd, Choung E, Kinchelow T, Rossy W, Steinberg B. Hemicondylar hamate replacement arthroplasty for proximal interphalangeal joint fracture dislocations: an assessment of graft suitability. J Hand Surg Am. 2008 May-Jun;33(5):733-9. doi: 10.1016/j.jhsa.2008.01.012. PubMed PMID: 18590857. ](http://www.ncbi.nlm.nih.gov/pubmed/18590857)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18590857)
4. Woodworth JA, McCullough MB, Grosland NM, Adams BD. Impact of simulated proximal interphalangeal arthrodeses of all fingers on hand function. J Hand Surg Am. 2006 Jul-Aug;31(6):940-
[6/. PubMed PMID: 16843153. ](http://www.ncbi.nlm.nih.gov/pubmed/16843153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16843153)
Regarding acute treatment options, extension block splinting is not recommended because of the inherent instability associated with this injury. The case in question involves a young patient; therefore, the use of primary implant arthroplasty is not the treatment of choice. In the ring finger, motion is important for power grip, so arthrodesis should be avoided if a reasonable alternative exists. Volar plate arthroplasty, although an option, has generated disappointing results for longterm joint motion and stability. Hemi-hamate arthroplasty has been described as a useful and predictable method with which to reconstruct the volar base of the middle phalanx in cases in which comminution prevents direct internal fixation. When performing hemi-hamate arthroplasty, a free osteocartilaginous graft is harvested from the dorsal and distal surface of the hamate. Using the portion of the hamate that articulates with the concave contour of the fourth to fifth
carpometacarpal joints provides a midline ridge that approximates that of the native middle phalangeal base.
Reconstruction with hemi-hamate autograft can restore the concavity of the middle phalangeal base in the anteroposterior direction. This concavity provides a volar buttress-to-dorsal subluxation of the middle phalanx. Hemi-hamate grafting is performed to the middle phalanx, not the proximal phalanx. Collateral ligament integrity is generally sacrificed to achieve adequate exposure to perform this procedure. It is not generally necessary to perform formal collateral ligament repair or reconstruction once adequate bony reconstruction is achieved. Volar plate integrity is not the primary aim of hemi-hamate arthroplasty; however, the volar plate is repaired to the middle phalangeal insertion of the collateral ligaments at the conclusion of the procedure.
Arthrodesis of the small joints of the hand is a predictable and effective method with which to control pain and instability when preservation of functional motion is not possible. This procedure offers a lower complication rate than prosthetic arthroplasty and yields satisfactory functional results. The trend is to favor arthrodesis for the radial digits and arthroplasty for the ulnar digits because of the importance of PIP flexion in the ulnar digits for power grip. Another consideration is age; younger, more active patients are more prone to eventual prosthetic failure and recurrence of digital deformity. A variety of recommendations have been made by various authors regarding the optimal position for PIP arthrodesis. The consensus is that approximately 40 degrees of flexion is optimal for the ring finger PIP joint.
RECOMMENDED READINGS
1. [Tyser AR, Tsai MA, Parks BG, Means KR Jr. Stability of acute dorsal fracture dislocations of the proximal interphalangeal joint: a biomechanical study. J Hand Surg Am. 2014 Jan;39(1):13-8. doi: 10.1016/j.jhsa.2013.09.025. Epub 2013 Nov 6. PubMed PMID: 24211175.](http://www.ncbi.nlm.nih.gov/pubmed/24211175)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24211175)
2. [Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519. ](http://www.ncbi.nlm.nih.gov/pubmed/14507519)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14507519)
3. [Capo JT, Hastings H 2nd, Choung E, Kinchelow T, Rossy W, Steinberg B. Hemicondylar hamate replacement arthroplasty for proximal interphalangeal joint fracture dislocations: an assessment of graft suitability. J Hand Surg Am. 2008 May-Jun;33(5):733-9. doi: 10.1016/j.jhsa.2008.01.012. PubMed PMID: 18590857. ](http://www.ncbi.nlm.nih.gov/pubmed/18590857)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18590857)
4. Woodworth JA, McCullough MB, Grosland NM, Adams BD. Impact of simulated proximal interphalangeal arthrodeses of all fingers on hand function. J Hand Surg Am. 2006 Jul-Aug;31(6):940-
[6/. PubMed PMID: 16843153. ](http://www.ncbi.nlm.nih.gov/pubmed/16843153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16843153)
QUESTION 28
of 100
Figures 31a through 31d are the radiographs and MR images of a 52-year-old man who has a 7-week history of right ring finger pain, redness, and swelling. He accidentally stuck his finger with a toothpick 1 week before developing symptoms. There is purulent drainage from the puncture wound site. He was treated with oral antibiotics for 10 days and intravenous (IV) antibiotics for 3 weeks before being seen. Initial cultures grew _Eikenella corrodens_. What is/are the best next step(s)?


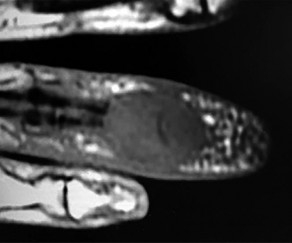

Figures 31a through 31d are the radiographs and MR images of a 52-year-old man who has a 7-week history of right ring finger pain, redness, and swelling. He accidentally stuck his finger with a toothpick 1 week before developing symptoms. There is purulent drainage from the puncture wound site. He was treated with oral antibiotics for 10 days and intravenous (IV) antibiotics for 3 weeks before being seen. Initial cultures grew _Eikenella corrodens_. What is/are the best next step(s)?
1
Continued IV antibiotics for 4 weeks
2
Bone scan followed by biopsy of the region
3
Drainage of the abscess with debridement of bone and soft tissue
4
Amputation through the distal interphalangeal (DIP) joint
This patient had a septic DIP joint that was treated with antibiotics alone. As a result, he developed osteomyelitis with bone destruction and an abscess. The correct answer is debridement of both bone and soft tissue with abscess drainage. Antibiotic treatment without surgery would not successfully eliminate this infection. A bone scan and biopsy are not appropriate because this problem is an infection and not a tumor, and the MR imaging provided enough diagnostic information. Amputation is not indicated prior to an attempt to salvage the digit. Amputation through the DIP joint would not remove the infected bone in the middle phalanx and would provide an inadequate level of resection.
RECOMMENDED READINGS
5. [Robinson LG, Kourtis AP. Tale of a toothpick: Eikenella corrodens osteomyelitis. Infection. 2000 Sep;28(5):332-3. PubMed PMID: 11073145. ](http://www.ncbi.nlm.nih.gov/pubmed/11073145)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11073145)
6. [Cuenca-Estrella M, Ramos JM, Esteban J, Soriano F, Vallejo JV. Eikenella corrodens thumb osteomyelitis. Postgrad Med J. 1996 Mar;72(845):188.](http://www.ncbi.nlm.nih.gov/pubmed/8731720)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8731720)
7. [Schmidt DR, Heckman JD. Eikenella corrodens in human bite infections of the hand. J Trauma. 1983 Jun;23(6):478-82. PubMed PMID: 6345799. ](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)
8. [Rayan GM, Putnam JL, Cahill SL, Flournoy DJ. Eikenella corrodens in human mouth flora. J Hand Surg Am. 1988 Nov;13(6):953-6. PubMed PMID: 3066818. ](http://www.ncbi.nlm.nih.gov/pubmed/3066818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3066818)
RECOMMENDED READINGS
5. [Robinson LG, Kourtis AP. Tale of a toothpick: Eikenella corrodens osteomyelitis. Infection. 2000 Sep;28(5):332-3. PubMed PMID: 11073145. ](http://www.ncbi.nlm.nih.gov/pubmed/11073145)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11073145)
6. [Cuenca-Estrella M, Ramos JM, Esteban J, Soriano F, Vallejo JV. Eikenella corrodens thumb osteomyelitis. Postgrad Med J. 1996 Mar;72(845):188.](http://www.ncbi.nlm.nih.gov/pubmed/8731720)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8731720)
7. [Schmidt DR, Heckman JD. Eikenella corrodens in human bite infections of the hand. J Trauma. 1983 Jun;23(6):478-82. PubMed PMID: 6345799. ](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%206345799)
8. [Rayan GM, Putnam JL, Cahill SL, Flournoy DJ. Eikenella corrodens in human mouth flora. J Hand Surg Am. 1988 Nov;13(6):953-6. PubMed PMID: 3066818. ](http://www.ncbi.nlm.nih.gov/pubmed/3066818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3066818)
QUESTION 29
of 100
Which treatment for an acute median nerve injury with a 3-cm gap between the nerve ends produces the best functional result?
Which treatment for an acute median nerve injury with a 3-cm gap between the nerve ends produces the best functional result?
1
Primary nerve repair under tension
2
Nerve graft autograft
3
Nerve graft allograft
4
Nerve conduit
The gold standard for the treatment of gaps in major peripheral nerves is cabled autografting. Allografts and conduits are beneficial and have their own indications; however, studies have not demonstrated equivalent outcomes compared to those achieved with autografts. Although joints may be positioned to bring disrupted nerve ends together so that the repair is not under tension,
the excessive degrees of wrist flexion needed to achieve a primary repair may lead to a problematic and dysfunctional flexion contracture.
There is recent attention and scientific interest in human allograft for nerve grafting. RANGER Registry database publications have demonstrated equivalence to autograft. More long-term studies will help to determine which injuries are most appropriate for allograft reconstruction.
RECOMMENDED READINGS
9. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. _AAOS Comprehensive Orthopaedic Review_. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
10. [Whitlock EL, Tuffaha SH, Luciano JP, Yan Y, Hunter DA, Magill CK, Moore AM, Tong AY, Mackinnon SE, Borschel GH. Processed allografts and type I collagen conduits for repair of peripheral nerve gaps. Muscle Nerve. 2009 Jun;39(6):787-99. doi: 10.1002/mus.21220. PubMed PMID: 19291791. ](http://www.ncbi.nlm.nih.gov/pubmed/19291791)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19291791)
the excessive degrees of wrist flexion needed to achieve a primary repair may lead to a problematic and dysfunctional flexion contracture.
There is recent attention and scientific interest in human allograft for nerve grafting. RANGER Registry database publications have demonstrated equivalence to autograft. More long-term studies will help to determine which injuries are most appropriate for allograft reconstruction.
RECOMMENDED READINGS
9. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. _AAOS Comprehensive Orthopaedic Review_. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
10. [Whitlock EL, Tuffaha SH, Luciano JP, Yan Y, Hunter DA, Magill CK, Moore AM, Tong AY, Mackinnon SE, Borschel GH. Processed allografts and type I collagen conduits for repair of peripheral nerve gaps. Muscle Nerve. 2009 Jun;39(6):787-99. doi: 10.1002/mus.21220. PubMed PMID: 19291791. ](http://www.ncbi.nlm.nih.gov/pubmed/19291791)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19291791)
QUESTION 30
of 100
Figure 33 is the radiograph of a 62-year-old right-hand-dominant man who has wrist pain. When discussing surgical options with the patient, which radiographic finding, if present, would prevent scaphoid excision and 4-corner fusion from being the best course of treatment?

Figure 33 is the radiograph of a 62-year-old right-hand-dominant man who has wrist pain. When discussing surgical options with the patient, which radiographic finding, if present, would prevent scaphoid excision and 4-corner fusion from being the best course of treatment?
1
Avascular necrosis of the scaphoid
2
Degenerative changes at the midcarpal joint
3
Degenerative changes at the lunate fossa
4
Ulna styloid fracture
Scaphoid nonunion advanced collapse is a common pattern of posttraumatic wrist arthritis. Treatment options include denervation, radial styloidectomy, excision of the distal nonunited scaphoid fragment, proximal row carpectomy (PRC), capitolunate arthrodesis, 4-corner arthrodesis, and complete wrist arthrodesis. Radial styloidectomy is not effective if there is degenerative change at the midcarpal joint. PRC is not an effective option when there is degenerative change at the proximal capitate. Four-corner arthrodesis is not an effective option if there is degenerative arthritic change at the lunate fossa; if this level of change is present, complete wrist arthrodesis is recommended.
RECOMMENDED READINGS
11. [Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis--update on evaluation and treatment. J Hand Surg Am. 2011 Apr;36(4):729-35. doi: 10.1016/j.jhsa.2011.01.018. Review. PubMed PMID: 21463735. ](http://www.ncbi.nlm.nih.gov/pubmed/21463735)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21463735)
12. [Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008 Oct;61(10):1210-8. Epub 2007 Oct 22. PubMed PMID: 17951122. ](http://www.ncbi.nlm.nih.gov/pubmed/17951122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17951122)
13. [Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg Am. 1994 Sep;19(5):751-9. PubMed PMID: 7806795. ](http://www.ncbi.nlm.nih.gov/pubmed/7806795)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7806795)
RECOMMENDED READINGS
11. [Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis--update on evaluation and treatment. J Hand Surg Am. 2011 Apr;36(4):729-35. doi: 10.1016/j.jhsa.2011.01.018. Review. PubMed PMID: 21463735. ](http://www.ncbi.nlm.nih.gov/pubmed/21463735)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21463735)
12. [Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008 Oct;61(10):1210-8. Epub 2007 Oct 22. PubMed PMID: 17951122. ](http://www.ncbi.nlm.nih.gov/pubmed/17951122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17951122)
13. [Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg Am. 1994 Sep;19(5):751-9. PubMed PMID: 7806795. ](http://www.ncbi.nlm.nih.gov/pubmed/7806795)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7806795)
QUESTION 31
of 100
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
1
Quadrigia
2
Intrinsic tightness
3
Lumbrical plus deformity
4
Disruption of the tendon repair
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit.
Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon repair causes limited flexion of the injured finger.
RECOMMENDED READINGS
14. Malerich MM, Baird RA, McMaster W, Erickson JM. Permissible limits of flexor digitorum profundus tendon advancement--an anatomic study. J Hand Surg Am. 1987 Jan; 12(1):30-3. PubMed PMID: 3805640. View Abstract at PubMed
15. Schreuders TA. The quadriga phenomenon: a review and clinical relevance. J Hand Surg Eur Vol. 2012 Jul;37(6):513-22. doi: 10.1177/1753193411430810. Epub 2011 Dec 14. Review.
PubMed PMID: 22170246. View Abstract at PubMed
Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon repair causes limited flexion of the injured finger.
RECOMMENDED READINGS
14. Malerich MM, Baird RA, McMaster W, Erickson JM. Permissible limits of flexor digitorum profundus tendon advancement--an anatomic study. J Hand Surg Am. 1987 Jan; 12(1):30-3. PubMed PMID: 3805640. View Abstract at PubMed
15. Schreuders TA. The quadriga phenomenon: a review and clinical relevance. J Hand Surg Eur Vol. 2012 Jul;37(6):513-22. doi: 10.1177/1753193411430810. Epub 2011 Dec 14. Review.
PubMed PMID: 22170246. View Abstract at PubMed
QUESTION 32
of 100
A 20-year-old man has middle finger metacarpophalangeal (MP) joint pain with difficulty extending his MP joint. The skin is not injured, yet the digit seems to be slightly ulnar deviated. He can maintain extension but has difficulty extending his MP joint from full MP joint flexion. If surgery is recommended, which structure most likely needs to be repaired to restore active motion?
A 20-year-old man has middle finger metacarpophalangeal (MP) joint pain with difficulty extending his MP joint. The skin is not injured, yet the digit seems to be slightly ulnar deviated. He can maintain extension but has difficulty extending his MP joint from full MP joint flexion. If surgery is recommended, which structure most likely needs to be repaired to restore active motion?
1
Extensor digitorum communis
2
Sagittal band
3
Joint capsule
4
Radial collateral ligament
This is an example of a closed sagittal band MP joint injury. The radial sagittal band ruptures , and the extensor tendon subluxes ulnarly . When the MP joint is flexed, it is difficult to fully extend it, but when the MP joint is held in full extension, active extension can maintain the position. In the setting of an extensor digitorum injury, extension cannot be maintained even if the MP joint is positioned in extension. The joint capsule is often injured when the sagittal band is injured, but repairing it will not restore extension. The radial collateral ligament of the MP joint is rarely injured with a sagittal band injury, and repairing it would not restore MP joint extension. When the MP joint is fully extended if the extensor tendon centralizes and full MP joint extension can be maintained, this injury usually is treated with a splint [yoke splint]) for 6 to 8 weeks. Surgery is recommended if the extensor tendon does not centralize with passive extension or if an injury is chronic. Surgery often is recommended for high-level athletes.
RECOMMENDED READINGS
16. Kleinhenz BP, Adams BD. Closed Sagittal Band Injury of the Metacarpophalangeal Joint. J Am Acad Orthop Surg. 2015 Jul;23(7):415-23. doi: 10.5435/JAAOS-D-13-00203. Review. PubMed PMID:
[26111875/. ](http://www.ncbi.nlm.nih.gov/pubmed/26111875)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26111875)
17. [Catalano LW 3rd, Gupta S, Ragland R 3rd, Glickel SZ, Johnson C, Barron OA. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. J Hand Surg Am. 2006 Feb;31(2):242-5. PubMed PMID: 16473685. ](http://www.ncbi.nlm.nih.gov/pubmed/16473685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16473685)
18. [Lin JD, Strauch RJ. Closed soft tissue extensor mechanism injuries (mallet, boutonniere, and sagittal band). J Hand Surg Am. 2014 May;39(5):1005-11. doi: 10.1016/j.jhsa.2013.11.018. Review. PubMed PMID: 24766832. ](http://www.ncbi.nlm.nih.gov/pubmed/24766832)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766832)
RECOMMENDED READINGS
16. Kleinhenz BP, Adams BD. Closed Sagittal Band Injury of the Metacarpophalangeal Joint. J Am Acad Orthop Surg. 2015 Jul;23(7):415-23. doi: 10.5435/JAAOS-D-13-00203. Review. PubMed PMID:
[26111875/. ](http://www.ncbi.nlm.nih.gov/pubmed/26111875)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26111875)
17. [Catalano LW 3rd, Gupta S, Ragland R 3rd, Glickel SZ, Johnson C, Barron OA. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. J Hand Surg Am. 2006 Feb;31(2):242-5. PubMed PMID: 16473685. ](http://www.ncbi.nlm.nih.gov/pubmed/16473685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16473685)
18. [Lin JD, Strauch RJ. Closed soft tissue extensor mechanism injuries (mallet, boutonniere, and sagittal band). J Hand Surg Am. 2014 May;39(5):1005-11. doi: 10.1016/j.jhsa.2013.11.018. Review. PubMed PMID: 24766832. ](http://www.ncbi.nlm.nih.gov/pubmed/24766832)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766832)
QUESTION 33
of 100
What is the most appropriate indication for use of a skin graft in Dupuytren disease?
What is the most appropriate indication for use of a skin graft in Dupuytren disease?
1
70 degrees primary proximal interphalangeal (PIP) joint contracture
2
50 degrees recurrent metacarpophalangeal (MP) joint contracture with an isolated cord
3
50 degrees recurrent PIP contracture with an isolated cord
4
50 degrees recurrent PIP contracture with diffuse skin involvement
Skin grafts are especially useful for patients with Dupuytren disease who have severe, diffuse disease and recurrences, particularly with multiple joint involvement. Although rarely required for primary cases, if disease is infiltrative and diffuse, skin grafts can be useful. Full-thickness skin grafts are preferred, providing more aesthetic and durable skin coverage while exhibiting less tendency to retract than partial-thickness grafts. Most authors have observed that recurrence is uncommon beneath a graft, although a recent article by Roush and Stern did not find that full-thickness skin grafting prevented recurrences. Grafts rarely do not “take” even though they often are placed directly over neurovascular bundles and the flexor sheath.
RECOMMENDED READINGS
19. [Hall PN, Fitzgerald A, Sterne GD, Logan AM. Skin replacement in Dupuytren's disease. J Hand Surg Br. 1997 Apr;22(2):193-7. PubMed PMID: 9149986. ](http://www.ncbi.nlm.nih.gov/pubmed/%209149986)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%209149986)
20. [Heuston JT. The control of recurrent Dupuytren's contracture by skin replacement. Br J Plast Surg. 1969 Apr;22(2):152-6. PubMed PMID: 4891593. ](http://www.ncbi.nlm.nih.gov/pubmed/4891593)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4891593)
21. MCCASH CR. THE OPEN PALM TECHNIQUE IN DUPUYTREN'S CONTRACTURE. Br J Plast
[Surg. 1964 Jul;17:271-80. PubMed PMID: 14191131. ](http://www.ncbi.nlm.nih.gov/pubmed/14191131)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14191131)
22. [Roush TF, Stern PJ. Results following surgery for recurrent Dupuytren's disease. J Hand Surg Am. 2000 Mar;25(2):291-6. PubMed PMID: 10722821. ](http://www.ncbi.nlm.nih.gov/pubmed/10722821)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10722821)
RECOMMENDED READINGS
19. [Hall PN, Fitzgerald A, Sterne GD, Logan AM. Skin replacement in Dupuytren's disease. J Hand Surg Br. 1997 Apr;22(2):193-7. PubMed PMID: 9149986. ](http://www.ncbi.nlm.nih.gov/pubmed/%209149986)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%209149986)
20. [Heuston JT. The control of recurrent Dupuytren's contracture by skin replacement. Br J Plast Surg. 1969 Apr;22(2):152-6. PubMed PMID: 4891593. ](http://www.ncbi.nlm.nih.gov/pubmed/4891593)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4891593)
21. MCCASH CR. THE OPEN PALM TECHNIQUE IN DUPUYTREN'S CONTRACTURE. Br J Plast
[Surg. 1964 Jul;17:271-80. PubMed PMID: 14191131. ](http://www.ncbi.nlm.nih.gov/pubmed/14191131)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14191131)
22. [Roush TF, Stern PJ. Results following surgery for recurrent Dupuytren's disease. J Hand Surg Am. 2000 Mar;25(2):291-6. PubMed PMID: 10722821. ](http://www.ncbi.nlm.nih.gov/pubmed/10722821)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10722821)
QUESTION 34
of 100
Figures 37a through 37c are the radiographs of a 45-year-old construction worker who has severe wrist pain. He has failed nonsurgical measures and requests surgery. The most appropriate surgical option is



Figures 37a through 37c are the radiographs of a 45-year-old construction worker who has severe wrist pain. He has failed nonsurgical measures and requests surgery. The most appropriate surgical option is
1
bone graft with fixation of the scaphoid.
2
proximal row carpectomy.
3
scaphoid excision with 4-corner fusion.
4
total wrist joint replacement.
The radiographs show a long-standing scaphoid nonunion with avascular necrosis and collapse of the proximal pole. This is referred to as a scaphoid nonunion advanced collapse wrist. He also has advanced arthritis of the capitolunate joint. This patient has a physically demanding occupation, so the best option for him is scaphoid excision with 4-corner fusion. Proximal row carpectomy would be inappropriate because of the advanced arthritis of the capitolunate joint. This procedure’s success is reliant upon normal cartilage/joint articulation of the capitate and lunate fossa of the distal radius. A total wrist replacement is not appropriate for a man with a physically demanding job. Finally, the patient has a long-standing scaphoid nonunion with advanced proximal pole collapse. Therefore, bone grafting with fixation is not an option at this point.
RECOMMENDED READINGS
23. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013.](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
24. [Shah CM, Stern PJ. Scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist arthritis. Curr Rev Musculoskelet Med. 2013 Mar;6(1):9-17. doi: 10.1007/s12178-012-9149-4. PubMed PMID: 23325545. ](http://www.ncbi.nlm.nih.gov/pubmed/23325545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23325545)
RECOMMENDED READINGS
23. [Weiss KE, Rodner CM. Osteoarthritis of the wrist. J Hand Surg Am. 2007 May-Jun;32(5):725-46. Review. PubMed PMID: 17482013.](http://www.ncbi.nlm.nih.gov/pubmed/17482013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17482013)
24. [Shah CM, Stern PJ. Scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist arthritis. Curr Rev Musculoskelet Med. 2013 Mar;6(1):9-17. doi: 10.1007/s12178-012-9149-4. PubMed PMID: 23325545. ](http://www.ncbi.nlm.nih.gov/pubmed/23325545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23325545)
QUESTION 35
of 100
A 35-year-old man has substantial pain at the base of his dominant right thumb. Orthosis use, anti-inflammatory medication, and corticosteroid injections have failed to improve his symptoms. Which condition is a contraindication to the surgery shown in the radiograph (Figure 38)?

A 35-year-old man has substantial pain at the base of his dominant right thumb. Orthosis use, anti-inflammatory medication, and corticosteroid injections have failed to improve his symptoms. Which condition is a contraindication to the surgery shown in the radiograph (Figure 38)?
1
Lack of hyperextension of the thumb metacarpophalangeal (MCP) joint
2
Scapholunate advance collapse
3
Arthritis of the scaphotrapezial-trapezoid (STT) joint
4
Bilateral disease
There are multiple surgical options for treatment of symptomatic thumb carpometacarpal (CMC) joint arthritis, including trapeziectomy with or without suspensionplasty and with or without tendon interposition, prosthetic replacement, or arthrodesis. However, for a young manual laborer, a more robust solution is required so he can withstand the rigors of occupational activities. Arthrodesis of the CMC joint provides good pain relief but a relatively high nonunion rate (8%-21%). Presence of STT arthritis is a contraindication to CMC fusion because the STT joint will undergo increased stresses following CMC fusion, which will cause early failure of the surgical intervention. Bilateral thumb CMC fusions can be performed, and bilateral disease is not a contraindication to this procedure. Concomitant wrist arthritis does not preclude CMC fusion because this can be addressed with scaphoid excision and partial wrist fusion, which is not compromised by CMC fusion. Lack of MCP joint hyperextension does not preclude CMC fusion; substantial MCP hyperextension should be addressed at the time of arthroplasty for CMC arthritis with MCP fusion or volar capsulodesis.
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
RECOMMENDED READINGS
25. [Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg Am. 2009 Jan; 34(1):20-6. doi: 10.1016/j.jhsa.2008.09.022. PubMed PMID: 19121726.](http://www.ncbi.nlm.nih.gov/pubmed/19121726)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19121726)
26. [Goldfarb CA, Stern PJ. Indications and techniques for thumb carpometacarpal arthrodesis. Tech Hand Up Extrem Surg. 2002 Dec;6(4):178-84. PubMed PMID: 16520598. ](http://www.ncbi.nlm.nih.gov/pubmed/16520598)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16520598)
QUESTION 36
of 100
Figures 39a and 39b are the clinical photographs of an 18-month-old child who had a fingertip amputation 4 days ago. The mother had used a tight dressing to keep the child from removing it. The hand is tense and swollen. The child is irritable, in pain, afebrile, and not moving the hand. What is the most appropriate treatment?




Figures 39a and 39b are the clinical photographs of an 18-month-old child who had a fingertip amputation 4 days ago. The mother had used a tight dressing to keep the child from removing it. The hand is tense and swollen. The child is irritable, in pain, afebrile, and not moving the hand. What is the most appropriate treatment?
1
Bulky dressing, splint, and elevation
2
Elevation and oral (PO) steroids
3
Compartment measurements
4
Carpal tunnel and compartment release
Figure 39c
Figure 39d
This irritable patient refuses to move his hand during a difficult examination. The hand is in an
intrinsic minus position with the extension of the metacarpophalangeal joints and flexion of the proximal interphalangeal joints. Patients who are difficult to examine may require compartment pressure measurements. Observation with elevation and possible PO steroids to decrease swelling are not indicated. This scenario has been ongoing for 4 days, and a carpal tunnel release with a release of the interosseous, thenar, hypothenar, and adductor compartments (Figures 39c and 39d) is now necessary. Finger fasciotomies are probably not needed.
If this scenario involved the forearm and a prolonged ischemic process, it may not have been prudent to perform a fasciotomy; with dead muscle, risk for infection is high. In small pediatric hands with compartment syndrome, it is often easier to find the median nerve in the forearm rather than the hand because significant edema in the hand distorts the anatomy.
RECOMMENDED READINGS
27. [Ouellette EA, Kelly R. Compartment syndromes of the hand. J Bone Joint Surg Am. 1996 Oct;78(10):1515-22. PubMed PMID: 8876579. ](http://www.ncbi.nlm.nih.gov/pubmed/%208876579)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%208876579)
28. [DiFelice A Jr, Seiler JG 3rd, Whitesides TE Jr. The compartments of the hand: an anatomic study. J Hand Surg Am. 1998 Jul;23(4):682-6. PubMed PMID: 9708383. ](http://www.ncbi.nlm.nih.gov/pubmed/9708383)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9708383)
**Question 40 of 100**
A 48-year-old right-hand-dominant man has had progressive unilateral right hand weakness and numbness involving his ring and small fingers for 6 months. There is no history of trauma, and the patient reports no pain. An examination reveals intrinsic weakness and atrophy, with normal strength of the flexor digitorum profundus and small flexor carpi ulnaris and abductor pollicis brevis muscles. A sensory examination reveals more than 12 mm of 2-point discrimination to the small finger and ulnar ring finger. Dorsal ulnar hand sensation and the remainder of the examination findings are normal. What is the most likely diagnosis?
1. Ulnar neuropathy at the level of Guyon’s canal
2. Ulnar neuropathy at the level of the cubital tunnel
3. Amyotrophic lateral sclerosis (ALS)
4. Pancoast tumor
_PREFERRED RESPONSE: 1- Ulnar neuropathy at the level of Guyon’s canal_
**DISCUSSION**
This patient has advanced ulnar neuropathy with significant motor weakness and atrophy, along with late sensory findings. ALS would result in symmetrical findings, and this patient’s findings are unilateral. Although a Pancoast tumor may cause ulnar nerve findings, there is typically associated pain and other physical findings. The findings for this patient are more typical for ulnar neuropathy. Although compression at the level of the cubital tunnel would be more common, this patient has profound weakness of the intrinsics with no involvement of the more proximal groups. In addition, his sensory findings are advanced, but there is no involvement of the dorsal ulnar hand, indicating a more distal site of compression. There is an electrical confirmed normal conduction of the ulnar nerve across the elbow with denervation of the intrinsics. MR imaging revealed a large ganglion within Guyon’s canal that was compressing the ulnar nerve, and these findings were confirmed at surgery.
RECOMMENDED READINGS
29. [Chen SH, Tsai TM. Ulnar tunnel syndrome. J Hand Surg Am. 2014 Mar;39(3):571-9. doi: 10.1016/j.jhsa.2013.08.102. Review. PubMed PMID: 24559635. ](http://www.ncbi.nlm.nih.gov/pubmed/24559635)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24559635)
30. [Kuschner SH, Gelberman RH, Jennings C. Ulnar nerve compression at the wrist. J Hand Surg Am. 1988 Jul;13(4):577-80. PubMed PMID: 3418064. ](http://www.ncbi.nlm.nih.gov/pubmed/3418064)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3418064)
Figure 39d
This irritable patient refuses to move his hand during a difficult examination. The hand is in an
intrinsic minus position with the extension of the metacarpophalangeal joints and flexion of the proximal interphalangeal joints. Patients who are difficult to examine may require compartment pressure measurements. Observation with elevation and possible PO steroids to decrease swelling are not indicated. This scenario has been ongoing for 4 days, and a carpal tunnel release with a release of the interosseous, thenar, hypothenar, and adductor compartments (Figures 39c and 39d) is now necessary. Finger fasciotomies are probably not needed.
If this scenario involved the forearm and a prolonged ischemic process, it may not have been prudent to perform a fasciotomy; with dead muscle, risk for infection is high. In small pediatric hands with compartment syndrome, it is often easier to find the median nerve in the forearm rather than the hand because significant edema in the hand distorts the anatomy.
RECOMMENDED READINGS
27. [Ouellette EA, Kelly R. Compartment syndromes of the hand. J Bone Joint Surg Am. 1996 Oct;78(10):1515-22. PubMed PMID: 8876579. ](http://www.ncbi.nlm.nih.gov/pubmed/%208876579)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%208876579)
28. [DiFelice A Jr, Seiler JG 3rd, Whitesides TE Jr. The compartments of the hand: an anatomic study. J Hand Surg Am. 1998 Jul;23(4):682-6. PubMed PMID: 9708383. ](http://www.ncbi.nlm.nih.gov/pubmed/9708383)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9708383)
**Question 40 of 100**
A 48-year-old right-hand-dominant man has had progressive unilateral right hand weakness and numbness involving his ring and small fingers for 6 months. There is no history of trauma, and the patient reports no pain. An examination reveals intrinsic weakness and atrophy, with normal strength of the flexor digitorum profundus and small flexor carpi ulnaris and abductor pollicis brevis muscles. A sensory examination reveals more than 12 mm of 2-point discrimination to the small finger and ulnar ring finger. Dorsal ulnar hand sensation and the remainder of the examination findings are normal. What is the most likely diagnosis?
1. Ulnar neuropathy at the level of Guyon’s canal
2. Ulnar neuropathy at the level of the cubital tunnel
3. Amyotrophic lateral sclerosis (ALS)
4. Pancoast tumor
_PREFERRED RESPONSE: 1- Ulnar neuropathy at the level of Guyon’s canal_
**DISCUSSION**
This patient has advanced ulnar neuropathy with significant motor weakness and atrophy, along with late sensory findings. ALS would result in symmetrical findings, and this patient’s findings are unilateral. Although a Pancoast tumor may cause ulnar nerve findings, there is typically associated pain and other physical findings. The findings for this patient are more typical for ulnar neuropathy. Although compression at the level of the cubital tunnel would be more common, this patient has profound weakness of the intrinsics with no involvement of the more proximal groups. In addition, his sensory findings are advanced, but there is no involvement of the dorsal ulnar hand, indicating a more distal site of compression. There is an electrical confirmed normal conduction of the ulnar nerve across the elbow with denervation of the intrinsics. MR imaging revealed a large ganglion within Guyon’s canal that was compressing the ulnar nerve, and these findings were confirmed at surgery.
RECOMMENDED READINGS
29. [Chen SH, Tsai TM. Ulnar tunnel syndrome. J Hand Surg Am. 2014 Mar;39(3):571-9. doi: 10.1016/j.jhsa.2013.08.102. Review. PubMed PMID: 24559635. ](http://www.ncbi.nlm.nih.gov/pubmed/24559635)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24559635)
30. [Kuschner SH, Gelberman RH, Jennings C. Ulnar nerve compression at the wrist. J Hand Surg Am. 1988 Jul;13(4):577-80. PubMed PMID: 3418064. ](http://www.ncbi.nlm.nih.gov/pubmed/3418064)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3418064)
QUESTION 37
of 100
Figure 41 is the radiograph of a 13-year-old gymnast who has a 6-month history of wrist pain. She has a 20% loss of motion, and she especially experiences pain with forced dorsiflexion. The most likely cause of her pain is

Figure 41 is the radiograph of a 13-year-old gymnast who has a 6-month history of wrist pain. She has a 20% loss of motion, and she especially experiences pain with forced dorsiflexion. The most likely cause of her pain is
1
a stress reaction of the distal radial physis.
2
avascular necrosis of the lunate.
3
enthesopathy of the flexor carpi radialis.
4
an occult dorsal carpal ganglion.
As young gymnasts become more competitive during their early teens, repeated impacts such as floor work and other compressive stresses associated with axial loading and forced dorsiflexion can cause injury to the distal radial/ulnar 0 at the junction of the zones of hypertrophy and provisional calcification. This condition is strongly influenced by both the intensity and the duration of training. Signs and symptoms to be elicited include local tenderness, stiffness, and pain with forced dorsiflexion. Radiographs demonstrate physeal widening, haziness, cystic changes, and metaphyseal beaking. Repeated episodes may be apparent as parallel lines of injury are demonstrated. Symptoms predictably respond to cessation of offending activities and casting. However, in more severe cases, it may take up to 6 months for symptoms to subside. It may be difficult to get parents and coaches on board with such a plan of care, however. Enthesopathies are more commonly seen in older (collegiate) gymnasts. Occult dorsal carpal ganglia may produce
dorsal wrist pain but rarely causes stiffness. Osteonecrosis of the capitate and lunate has been reported in gymnasts, but this condition is rare.
RECOMMENDED READINGS
31. [Dobyns JH, Gabel GT. Gymnast's wrist. Hand Clin. 1990 Aug;6(3):493-505. Review. PubMed PMID: 2211859. ](http://www.ncbi.nlm.nih.gov/pubmed/%202211859)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%202211859)
32. [Roy S, Caine D, Singer KM. Stress changes of the distal radial epiphysis in young gymnasts. A report of twenty-one cases and a review of the literature. Am J Sports Med. 1985 Sep-Oct;13(5):301-8. PubMed PMID: 4051086. ](http://www.ncbi.nlm.nih.gov/pubmed/4051086)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4051086)
dorsal wrist pain but rarely causes stiffness. Osteonecrosis of the capitate and lunate has been reported in gymnasts, but this condition is rare.
RECOMMENDED READINGS
31. [Dobyns JH, Gabel GT. Gymnast's wrist. Hand Clin. 1990 Aug;6(3):493-505. Review. PubMed PMID: 2211859. ](http://www.ncbi.nlm.nih.gov/pubmed/%202211859)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%202211859)
32. [Roy S, Caine D, Singer KM. Stress changes of the distal radial epiphysis in young gymnasts. A report of twenty-one cases and a review of the literature. Am J Sports Med. 1985 Sep-Oct;13(5):301-8. PubMed PMID: 4051086. ](http://www.ncbi.nlm.nih.gov/pubmed/4051086)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4051086)
QUESTION 38
of 100
Figures 42a through 42c are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?



Figures 42a through 42c are the radiographs of a 27-year-old man who has had wrist pain since falling 1 day ago. Which treatment offers the best prognosis for prevention of carpal collapse and progressive arthritis?
1
Long-arm cast
2
Percutaneous screw fixation
3
Open reduction and internal fixation (ORIF) with bone graft
4
Proximal row carpectomy
Although this patient’s history includes a recent fall, the radiographs show evidence of a scaphoid nonunion with carpal collapse but no arthritis. Obtaining union of the scaphoid is important to prevent progressive carpal collapse and arthritic changes. ORIF with bone graft is most appropriate to obtain union and correct the collapse deformity. Screw fixation with volar wedge graft often is
performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
RECOMMENDED READINGS
33. Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: current concepts. J Am Acad Orthop Surg. 2013 Sep;21(9):548-57. doi: 10.5435/JAAOS-21-09-548. Review. PubMed PMID: 23996986. View Abstract at PubMed
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
performed to realign a scaphoid humpback deformity, although cancellous bone graft also is a reasonable option. Vascularized bone graft is considered for a nonunion of long duration, avascular necrosis of the proximal pole, and failed prior surgery. Cast immobilization will not lead to union of the scaphoid. Percutaneous screw fixation is not indicated for the treatment of a displaced nonunion. A proximal row carpectomy is a salvage procedure and is not indicated for this patient because there are no arthritic changes.
RECOMMENDED READINGS
33. Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: current concepts. J Am Acad Orthop Surg. 2013 Sep;21(9):548-57. doi: 10.5435/JAAOS-21-09-548. Review. PubMed PMID: 23996986. View Abstract at PubMed
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
QUESTION 39
of 100
The radiograph in Figure 43 shows a fracture in a 40-year-old man who has failed nonsurgical measures and is requesting surgery. Bone grafting with internal fixation is recommended. The patient has smoked 1 pack of cigarettes daily for 20 years. What is the success rate for surgical union in this scenario?

The radiograph in Figure 43 shows a fracture in a 40-year-old man who has failed nonsurgical measures and is requesting surgery. Bone grafting with internal fixation is recommended. The patient has smoked 1 pack of cigarettes daily for 20 years. What is the success rate for surgical union in this scenario?
1
0% to 20%
2
21% to 40%
3
60% to 80%
4
81% to 100%
It is well known that tobacco use has a negative effect on fracture healing. Little and associates’ study showed that union was achieved in 47 of 64 cases with nonvascularized scaphoid bone grafting with internal fixation. However, 13 of the 17 patients with a nonunion were smokers, revealing only a 24% success rate. A Mayo Clinic study assessing the success of vascularized bone graft on scaphoid nonunion in smokers showed success rate of only 46%. An additional study revealed a success rate of only 40% among smokers. A study by Nåsell and associates showed that the effect of smoking cessation intervention on all patients undergoing surgery for acute fractures of both upper and lower extremities during the first 6 weeks after surgery was beneficial. The overall complication rate in this study was lowered by 18%. A smoking cessation intervention during the perioperative period for surgery for scaphoid nonunion may provide some fracture-healing benefits.
RECOMMENDED READINGS
35. Little CP, Burston BJ, Hopkinson-Woolley J, Burge P. Failure of surgery for scaphoid non-union is associated with smoking. J Hand Surg Br. 2006 Jun;31(3):252-5. Epub 2006 Feb 20. PubMed PMID: 16488521.View Abstract at PubMed
36. Steinmann SP, Adams JE. Scaphoid fractures and nonunions: diagnosis and treatment. J Orthop Sci. 2006 Jul;11(4):424-31. Review. PubMed PMID: 16897211. View Abstract at PubMed
37. Dinah AF, Vickers RH. Smoking increases failure rate of operation for established non-union of the scaphoid bone. Int Orthop. 2007 Aug;31(4):503-5. Epub 2006 Sep 1. PubMed PMID: 16947049.
38. Nåsell H, Adami J, Samnegård E, Tønnesen H, Ponzer S. Effect of smoking cessation intervention on results of acute fracture surgery: a randomized controlled trial. J Bone Joint Surg Am. 2010 Jun;92(6):1335-42. doi: 10.2106/JBJS.I.00627. PubMed PMID: 20516308. View Abstract at PubMed
RECOMMENDED READINGS
35. Little CP, Burston BJ, Hopkinson-Woolley J, Burge P. Failure of surgery for scaphoid non-union is associated with smoking. J Hand Surg Br. 2006 Jun;31(3):252-5. Epub 2006 Feb 20. PubMed PMID: 16488521.View Abstract at PubMed
36. Steinmann SP, Adams JE. Scaphoid fractures and nonunions: diagnosis and treatment. J Orthop Sci. 2006 Jul;11(4):424-31. Review. PubMed PMID: 16897211. View Abstract at PubMed
37. Dinah AF, Vickers RH. Smoking increases failure rate of operation for established non-union of the scaphoid bone. Int Orthop. 2007 Aug;31(4):503-5. Epub 2006 Sep 1. PubMed PMID: 16947049.
38. Nåsell H, Adami J, Samnegård E, Tønnesen H, Ponzer S. Effect of smoking cessation intervention on results of acute fracture surgery: a randomized controlled trial. J Bone Joint Surg Am. 2010 Jun;92(6):1335-42. doi: 10.2106/JBJS.I.00627. PubMed PMID: 20516308. View Abstract at PubMed
QUESTION 40
of 100
The video in Figure 44 demonstrates a unilateral “piano key” sign, which indicates

The video in Figure 44 demonstrates a unilateral “piano key” sign, which indicates
1
distal radioulnar joint (DRUJ) instability.
2
interosseous membrane disruption.
3
midcarpal instability.
4
physiologic motion of hypermobility syndrome.
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments.
This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ.
Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
RECOMMENDED READINGS
39. [Mulford JS, Axelrod TS. Traumatic injuries of the distal radioulnar joint. Orthop Clin North Am. 2007 Apr;38(2):289-97, vii. Review. PubMed PMID: 17560410.](http://www.ncbi.nlm.nih.gov/pubmed/17560410)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17560410)
40. [Moritomo H. The distal interosseous membrane: current concepts in wrist anatomy and biomechanics. J Hand Surg Am. 2012 Jul;37(7):1501-7. doi: 10.1016/j.jhsa.2012.04.037. Review. PubMed PMID: 22721462. ](http://www.ncbi.nlm.nih.gov/pubmed/22721462)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22721462)
This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ.
Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
RECOMMENDED READINGS
39. [Mulford JS, Axelrod TS. Traumatic injuries of the distal radioulnar joint. Orthop Clin North Am. 2007 Apr;38(2):289-97, vii. Review. PubMed PMID: 17560410.](http://www.ncbi.nlm.nih.gov/pubmed/17560410)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17560410)
40. [Moritomo H. The distal interosseous membrane: current concepts in wrist anatomy and biomechanics. J Hand Surg Am. 2012 Jul;37(7):1501-7. doi: 10.1016/j.jhsa.2012.04.037. Review. PubMed PMID: 22721462. ](http://www.ncbi.nlm.nih.gov/pubmed/22721462)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22721462)
QUESTION 41
of 100
In addition to the anterior oblique ligament, which other structure is an important stabilizer of the thumb carpometacarpal (CMC) joint when the thumb is in a position of opposition?
In addition to the anterior oblique ligament, which other structure is an important stabilizer of the thumb carpometacarpal (CMC) joint when the thumb is in a position of opposition?
1
Osseous architecture
2
Abductor pollicis brevis
3
Radiovolar joint capsule
4
Dorsoradial ligament
The anterior oblique (volar) ligament was considered the primary stabilizing structure of the thumb CMC joint until alternative theories were offered in the mid 1970s. Multiple clinical and anatomic studies since that time have supported the theory that the primary stabilizing structure is the dorsoradial ligament.
Shah and Patel reported on 4 cases of thumb CMC dislocation in 1983 and demonstrated that in each case, the dorsal ligaments were ruptured while the anterior oblique ligament remained intact. Strauch and associates sectioned the supporting structures of 38 cadaveric specimens. Isolated sectioning of the dorsoradial ligament complex led to the maximum degree of subluxation. Preserving the dorsoradial complex alone maintained the highest degree of stability.
The radiovolar and dorsal capsular ligaments are thin and insert farther from the articular surface, allowing for increased mobility. The ulnovolar capsule and anterior oblique (volar) ligament attach close to the articular surface and are short and robust. Further stability comes from the infratendinous layer of the abductor pollicis longus tendon. The abductor pollicis brevis does not substantially contribute to stability of the CMC joint.
RECOMMENDED READINGS
41. [Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am. 1973 Dec;55(8):1655-66. PubMed PMID: 4804988. ](http://www.ncbi.nlm.nih.gov/pubmed/%204804988)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%204804988)
42. [Shah J, Patel M. Dislocation of the carpometacarpal joint of the thumb. A report of four cases. Clin Orthop Relat Res. 1983 May;(175):166-9. PubMed PMID: 6839582. ](http://www.ncbi.nlm.nih.gov/pubmed/6839582)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6839582)
43. Strauch RJ, Behrman MJ, Rosenwasser MP. Acute dislocation of the carpometacarpal joint of the thumb: an anatomic and cadaver study. J Hand Surg Am. 1994 Jan;19(1):93-8.
44. [Bosmans B, Verhofstad MH, Gosens T. Traumatic thumb carpometacarpal joint dislocations. J Hand Surg Am. 2008 Mar;33(3):438-41. doi: 10.1016/j.jhsa.2007.11.022. Review. PubMed PMID: 18343304. ](http://www.ncbi.nlm.nih.gov/pubmed/18343304)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18343304)
Shah and Patel reported on 4 cases of thumb CMC dislocation in 1983 and demonstrated that in each case, the dorsal ligaments were ruptured while the anterior oblique ligament remained intact. Strauch and associates sectioned the supporting structures of 38 cadaveric specimens. Isolated sectioning of the dorsoradial ligament complex led to the maximum degree of subluxation. Preserving the dorsoradial complex alone maintained the highest degree of stability.
The radiovolar and dorsal capsular ligaments are thin and insert farther from the articular surface, allowing for increased mobility. The ulnovolar capsule and anterior oblique (volar) ligament attach close to the articular surface and are short and robust. Further stability comes from the infratendinous layer of the abductor pollicis longus tendon. The abductor pollicis brevis does not substantially contribute to stability of the CMC joint.
RECOMMENDED READINGS
41. [Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am. 1973 Dec;55(8):1655-66. PubMed PMID: 4804988. ](http://www.ncbi.nlm.nih.gov/pubmed/%204804988)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%204804988)
42. [Shah J, Patel M. Dislocation of the carpometacarpal joint of the thumb. A report of four cases. Clin Orthop Relat Res. 1983 May;(175):166-9. PubMed PMID: 6839582. ](http://www.ncbi.nlm.nih.gov/pubmed/6839582)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6839582)
43. Strauch RJ, Behrman MJ, Rosenwasser MP. Acute dislocation of the carpometacarpal joint of the thumb: an anatomic and cadaver study. J Hand Surg Am. 1994 Jan;19(1):93-8.
44. [Bosmans B, Verhofstad MH, Gosens T. Traumatic thumb carpometacarpal joint dislocations. J Hand Surg Am. 2008 Mar;33(3):438-41. doi: 10.1016/j.jhsa.2007.11.022. Review. PubMed PMID: 18343304. ](http://www.ncbi.nlm.nih.gov/pubmed/18343304)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18343304)
QUESTION 42
of 100
Figures 46a through 46e are the radiographs and CT scans of a 21-year-old right-hand-dominant man who injured his right hand in a martial arts competition 3 weeks before seeking treatment. An
examination reveals substantial ulnar-sided hand swelling and tenderness at the base of the fifth metacarpal. Digital flexion is nearly full with no malrotation. The most appropriate treatment is


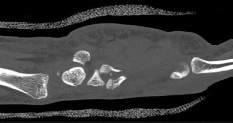
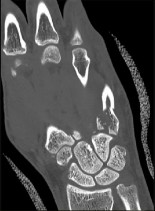

Figures 46a through 46e are the radiographs and CT scans of a 21-year-old right-hand-dominant man who injured his right hand in a martial arts competition 3 weeks before seeking treatment. An
examination reveals substantial ulnar-sided hand swelling and tenderness at the base of the fifth metacarpal. Digital flexion is nearly full with no malrotation. The most appropriate treatment is
1
cast immobilization.
2
closed reduction percutaneous pin fixation.
3
open reduction and internal fixation.
4
fifth carpometacarpal (CMC) arthrodesis.
This fifth metacarpal base fracture is displaced, comminuted, and impacted. It is also associated with dorsal subluxation of the metacarpal on the hamate. The CT scan confirms the impaction of a sizable portion of the articular surface of the metacarpal base. In addition, the injury is 3 weeks old and is not likely to reduce by closed means. Open reduction, which would enable more accurate restoration of the articular surface, is necessary. If the patient had arrived for treatment earlier, a closed reduction percutaneous pinning may have been successful but may not have reduced the impacted articular segment. This injury usually results from a longitudinally directed force along the axis of the fifth metacarpal. Although a fifth CMC arthrodesis is an option, it likely is not appropriate as an initial treatment option and should be reserved for patients with painful posttraumatic arthritis.
RECOMMENDED READINGS
45. [Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am. 1974 Oct;56(7):1459-63. PubMed PMID: 4433366. ](http://www.ncbi.nlm.nih.gov/pubmed/4433366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4433366)
46. [Kjaer-Petersen K, Jurik AG, Petersen LK. Intra-articular fractures at the base of the fifth metacarpal. A clinical and radiographical study of 64 cases. J Hand Surg Br. 1992 Apr;17(2):144-7. PubMed PMID: 1588193. ](http://www.ncbi.nlm.nih.gov/pubmed/1588193)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1588193)
RECOMMENDED READINGS
45. [Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am. 1974 Oct;56(7):1459-63. PubMed PMID: 4433366. ](http://www.ncbi.nlm.nih.gov/pubmed/4433366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4433366)
46. [Kjaer-Petersen K, Jurik AG, Petersen LK. Intra-articular fractures at the base of the fifth metacarpal. A clinical and radiographical study of 64 cases. J Hand Surg Br. 1992 Apr;17(2):144-7. PubMed PMID: 1588193. ](http://www.ncbi.nlm.nih.gov/pubmed/1588193)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1588193)
QUESTION 43
of 100
Which characteristic of complex regional pain syndrome (CRPS) type 2 differentiates it from CRPS 1?
Which characteristic of complex regional pain syndrome (CRPS) type 2 differentiates it from CRPS 1?
1
Positive bone scan result
2
Identified nerve injury
3
Pseudomotor changes
4
No identified nerve injury
CRPS 2 develops after nerve injury, whereas CRPS 1 occurs without nerve injury. The diagnostic criteria are otherwise the same for the 2 conditions. A 3-phase bone scan can be helpful; a pattern of increased uptake in all 3 phases, and particularly diffuse periarticular uptake in and around the joints of the affected extremity during the delayed phase, is considered typical of CRPS, especially during the first 6 months; however, it is not specific enough to be used as a diagnostic criteria.
Unfortunately, the pathophysiological mechanisms underlying CRPS remain unclear, and, as such, no standard diagnostic test for CRPS exists. There are 3 major sets of diagnostic criteria for CRPS: the International Association for the Study of Pain (IASP) criteria, the Budapest Research Criteria, and the Veldman criteria. According to IASP, CRPS type 1 involves an initiating noxious event or a cause of immobilization; continuing pain/allodynia/hyperalgesia for which the pain is disproportionate to any known inciting event; evidence of edema, changes in skin blood flow, or abnormal pseudomotor activity in the region of pain; and exclusion of the diagnosis by the existence of other conditions that would otherwise account for the degree of pain and dysfunction. CRPS type 2 is a syndrome that develops after nerve injury, contends IASP. Spontaneous pain or allodynia/hyperalgesia occurs and is not necessarily limited to the territory of the injured nerve; there is or has been evidence of edema, a skin blood flow abnormality, or abnormal sudomotor activity in the region of pain since the inciting event; and the diagnosis is excluded by the existence of conditions that would otherwise account for the degree of pain and dysfunction.
RECOMMENDED READINGS
47. [Borchers AT, Gershwin ME. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014 Mar;13(3):242-65. doi: 10.1016/j.autrev.2013.10.006. Epub 2013 Oct 23. Review. PubMed PMID: 24161450. ](http://www.ncbi.nlm.nih.gov/pubmed/24161450)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24161450)
48. [Patterson RW, Li Z, Smith BP, Smith TL, Koman LA. Complex regional pain syndrome of the upper extremity. J Hand Surg Am. 2011 Sep;36(9):1553-62. doi: 10.1016/j.jhsa.2011.06.027. Review. PubMed PMID: 21872098.](http://www.ncbi.nlm.nih.gov/pubmed/21872098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872098)
49. [Cappello ZJ, Kasdan ML, Louis DS. Meta-analysis of imaging techniques for the diagnosis of complex regional pain syndrome type I. J Hand Surg Am. 2012 Feb;37(2):288-96. doi: 10.1016/j.jhsa.2011.10.035. Epub 2011 Dec 15. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/22177715)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22177715)
50. [Patterson RW, Li Z, Smith BP, Smith TL, Koman LA. Complex regional pain syndrome of the upper extremity. J Hand Surg Am. 2011 Sep;36(9):1553-62. doi: 10.1016/j.jhsa.2011.06.027. Review. PubMed PMID: 21872098. ](http://www.ncbi.nlm.nih.gov/pubmed/21872098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872098)
Unfortunately, the pathophysiological mechanisms underlying CRPS remain unclear, and, as such, no standard diagnostic test for CRPS exists. There are 3 major sets of diagnostic criteria for CRPS: the International Association for the Study of Pain (IASP) criteria, the Budapest Research Criteria, and the Veldman criteria. According to IASP, CRPS type 1 involves an initiating noxious event or a cause of immobilization; continuing pain/allodynia/hyperalgesia for which the pain is disproportionate to any known inciting event; evidence of edema, changes in skin blood flow, or abnormal pseudomotor activity in the region of pain; and exclusion of the diagnosis by the existence of other conditions that would otherwise account for the degree of pain and dysfunction. CRPS type 2 is a syndrome that develops after nerve injury, contends IASP. Spontaneous pain or allodynia/hyperalgesia occurs and is not necessarily limited to the territory of the injured nerve; there is or has been evidence of edema, a skin blood flow abnormality, or abnormal sudomotor activity in the region of pain since the inciting event; and the diagnosis is excluded by the existence of conditions that would otherwise account for the degree of pain and dysfunction.
RECOMMENDED READINGS
47. [Borchers AT, Gershwin ME. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014 Mar;13(3):242-65. doi: 10.1016/j.autrev.2013.10.006. Epub 2013 Oct 23. Review. PubMed PMID: 24161450. ](http://www.ncbi.nlm.nih.gov/pubmed/24161450)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24161450)
48. [Patterson RW, Li Z, Smith BP, Smith TL, Koman LA. Complex regional pain syndrome of the upper extremity. J Hand Surg Am. 2011 Sep;36(9):1553-62. doi: 10.1016/j.jhsa.2011.06.027. Review. PubMed PMID: 21872098.](http://www.ncbi.nlm.nih.gov/pubmed/21872098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872098)
49. [Cappello ZJ, Kasdan ML, Louis DS. Meta-analysis of imaging techniques for the diagnosis of complex regional pain syndrome type I. J Hand Surg Am. 2012 Feb;37(2):288-96. doi: 10.1016/j.jhsa.2011.10.035. Epub 2011 Dec 15. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/22177715)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22177715)
50. [Patterson RW, Li Z, Smith BP, Smith TL, Koman LA. Complex regional pain syndrome of the upper extremity. J Hand Surg Am. 2011 Sep;36(9):1553-62. doi: 10.1016/j.jhsa.2011.06.027. Review. PubMed PMID: 21872098. ](http://www.ncbi.nlm.nih.gov/pubmed/21872098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872098)
QUESTION 44
of 100
Figure 48a is a radiograph of a 55-year-old man who had a thumb carpometacarpal (CMC) resection arthroplasty with a total trapezium resection and ligament reconstruction using one-half of the flexor carpi radialis. He has persistent pain around his thumb base. What is the best course of treatment?

Figure 48a is a radiograph of a 55-year-old man who had a thumb carpometacarpal (CMC) resection arthroplasty with a total trapezium resection and ligament reconstruction using one-half of the flexor carpi radialis. He has persistent pain around his thumb base. What is the best course of treatment?
1
Thumb metacarpal-to-index metacarpal fusion
2
Resection of the proximal trapezoid
3
Revision of the thumb CMC arthroplasty with an implant arthroplasty
4
Revision of the CMC arthroplasty with a suture suspension arthroplasty
The radiograph reveals an excellent postsurgical metacarpal scaphoid joint space, so revision of the CMC joint or fusion is not appropriate. The scaphoid trapezoid joint is irregular (Figure 48b) and is a common cause of the described symptoms. The sensitivity of the radiographic diagnosis of scaphoid trapezium trapezoid arthritis is 44%, and the specificity is 86%. The true prevalence of scaphotrapezoid arthritis is approximately 62%. Resection of the proximal trapezoid is not associated with morbidity. Routine intraoperative assessment of the scaphoid trapezoid joint is recommended so that proximal trapezoid excision (Figures 48c and 48d) can be performed if degenerative change (Figure 48b) is present.
RECOMMENDED READINGS
51. [Tomaino MM, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am. 1999 Nov;24(6):1220-4. PubMed PMID: 10584944. ](http://www.ncbi.nlm.nih.gov/pubmed/10584944)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10584944)
52. [Eaton RG, Glickel SZ, Littler JW. Tendon interposition arthroplasty for degenerative arthritis of the trapeziometacarpal joint of the thumb. J Hand Surg Am. 1985 Sep;10(5):645-54. PubMed PMID: 4045141. ](http://www.ncbi.nlm.nih.gov/pubmed/4045141)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4045141)
RECOMMENDED READINGS
51. [Tomaino MM, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am. 1999 Nov;24(6):1220-4. PubMed PMID: 10584944. ](http://www.ncbi.nlm.nih.gov/pubmed/10584944)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10584944)
52. [Eaton RG, Glickel SZ, Littler JW. Tendon interposition arthroplasty for degenerative arthritis of the trapeziometacarpal joint of the thumb. J Hand Surg Am. 1985 Sep;10(5):645-54. PubMed PMID: 4045141. ](http://www.ncbi.nlm.nih.gov/pubmed/4045141)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4045141)
QUESTION 45
of 100
Which treatment option helps prevent complex regional pain syndrome (CRPS)?
Which treatment option helps prevent complex regional pain syndrome (CRPS)?
1
Vitamin C
2
Therapy to desensitize and exercise the affected limb
3
Surgical release of affected nerves
4
Opioid pain medication
_
Vitamin C can play a part in preventing CRPS, but it has not been shown to have an effect on the treatment of CRPS. Occupational and physical therapies are ideal for the treatment of newly diagnosed CRPS. Although peripheral nerve release may help in cases of CRPS, surgery can lead to a rebound effect with worsening of pain symptoms. Opioids are not more effective than therapy for CRPS.
RECOMMENDED READINGS
53. [Zimmerman RM, Astifidis RP, Katz RD. Modalities for Complex Regional Pain Syndrome. J Hand Surg Am. 2015 Jul;40(7):1469-72. doi: 10.1016/j.jhsa.2015.03.010. Epub 2015 Apr 21. Review. PubMed PMID: 25910590. ](http://www.ncbi.nlm.nih.gov/pubmed/25910590)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25910590)
54. [Malay S, Chung KC. Testing the validity of preventing chronic regional pain syndrome with vitamin C after distal radius fracture. [Corrected]. J Hand Surg Am. 2014 Nov;39(11):2251-7. doi: 10.1016/j.jhsa.2014.08.009. Epub 2014 Sep 16. Review. Erratum in: J Hand Surg Am. 2014 Dec;39(12):2551. PubMed PMID: 25239047. ](http://www.ncbi.nlm.nih.gov/pubmed/25239047)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25239047)
RECOMMENDED READINGS
53. [Zimmerman RM, Astifidis RP, Katz RD. Modalities for Complex Regional Pain Syndrome. J Hand Surg Am. 2015 Jul;40(7):1469-72. doi: 10.1016/j.jhsa.2015.03.010. Epub 2015 Apr 21. Review. PubMed PMID: 25910590. ](http://www.ncbi.nlm.nih.gov/pubmed/25910590)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25910590)
54. [Malay S, Chung KC. Testing the validity of preventing chronic regional pain syndrome with vitamin C after distal radius fracture. [Corrected]. J Hand Surg Am. 2014 Nov;39(11):2251-7. doi: 10.1016/j.jhsa.2014.08.009. Epub 2014 Sep 16. Review. Erratum in: J Hand Surg Am. 2014 Dec;39(12):2551. PubMed PMID: 25239047. ](http://www.ncbi.nlm.nih.gov/pubmed/25239047)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25239047)
QUESTION 46
of 100
Figure 50a is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?

Figure 50a is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
RECOMMENDED READINGS
55. [Quitkin HM, Rosenwasser MP, Strauch RJ. The efficacy of silver nitrate cauterization for pyogenic granuloma of the hand. J Hand Surg Am. 2003 May;28(3):435-8. PubMed PMID: 12772100. ](http://www.ncbi.nlm.nih.gov/pubmed/12772100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12772100)
56. [Giblin AV, Clover AJ, Athanassopoulos A, Budny PG. Pyogenic granuloma – the quest for optimum treatment: audit of treatment of 408 cases. J Plast Reconstr Aesthet Surg. 2007;60(9):1030-5. Epub 2007 May 2. PubMed PMID: 17478135.](http://www.ncbi.nlm.nih.gov/pubmed/17478135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17478135)
RECOMMENDED READINGS
55. [Quitkin HM, Rosenwasser MP, Strauch RJ. The efficacy of silver nitrate cauterization for pyogenic granuloma of the hand. J Hand Surg Am. 2003 May;28(3):435-8. PubMed PMID: 12772100. ](http://www.ncbi.nlm.nih.gov/pubmed/12772100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12772100)
56. [Giblin AV, Clover AJ, Athanassopoulos A, Budny PG. Pyogenic granuloma – the quest for optimum treatment: audit of treatment of 408 cases. J Plast Reconstr Aesthet Surg. 2007;60(9):1030-5. Epub 2007 May 2. PubMed PMID: 17478135.](http://www.ncbi.nlm.nih.gov/pubmed/17478135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17478135)
QUESTION 47
of 100
When performing an index finger ray amputation, the orthopaedic surgeon should move the
When performing an index finger ray amputation, the orthopaedic surgeon should move the
1
first dorsal interosseous muscle to the long-finger extensor hood.
2
extensor indicis proprius (EIP) to the extensor digitorum communis of the long finger.
3
radial digital nerve index finger to the interosseous muscle.
4
flexor digitorum superficialis (FDS) index to the long-finger proximal phalanx.
Ray amputation often is performed to improve function and decrease pain by removing the digit through the metacarpal. Hyperesthesia and painful light touch are the most disabling complications. The digital nerves should be placed proximal to the wound to prevent a symptomatic neuroma. The radial and ulnar digital nerves can be sutured together, transposed to the interosseous muscle, or resected proximally, although no technique is superior. Excessive mobilization is discouraged, and care is taken to protect the radial digital nerve to the long finger at the time of index ray amputation. Transfer of the first dorsal interosseous, EIP and FDS to the long finger are procedures that have fallen out of favor because of lack of benefit and resulting stiffness.
RECOMMENDED READINGS
57. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
58. Murray JF, Carman W, MacKenzie JK. Transmetacarpal amputation of the index finger: a clinical assessment of hand strength and complications. J Hand Surg Am. 1977 Nov;2(6):471-
81/. PubMed PMID: 925334.
CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
A 60-year-old man has a symptomatic contracture of his dominant-hand ring finger. Treatment options are discussed, and he elects to proceed with palmar fasciectomy.
RECOMMENDED READINGS
57. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
58. Murray JF, Carman W, MacKenzie JK. Transmetacarpal amputation of the index finger: a clinical assessment of hand strength and complications. J Hand Surg Am. 1977 Nov;2(6):471-
81/. PubMed PMID: 925334.
CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
A 60-year-old man has a symptomatic contracture of his dominant-hand ring finger. Treatment options are discussed, and he elects to proceed with palmar fasciectomy.
QUESTION 48
of 100
What is the effect of a spiral cord in Dupuytren contracture on the digital neurovascular bundle?
What is the effect of a spiral cord in Dupuytren contracture on the digital neurovascular bundle?
1
Circumferential constriction
2
Palmar and midline displacement
3
Dorsal and lateral displacement
4
No effect
- Palmar and midline displacement_
QUESTION 49
of 100
Which finding is associated with the highest positive predictive value for the presence of a spiral cord?
Which finding is associated with the highest positive predictive value for the presence of a spiral cord?
1
Dupuytren diathesis
2
Metacarpophalangeal (MCP) joint flexion contracture
3
Proximal interphalangeal (PIP) joint flexion contracture
4
Knuckle pads
- Proximal interphalangeal (PIP) joint flexion contracture_
QUESTION 50
of 100
Following palmar fasciectomy for Dupuytren contracture performed under general anesthesia, the tourniquet is released and the surgical finger remains pale and cool to touch. The next appropriate steps are to flex the digit, warm the digit, and
Following palmar fasciectomy for Dupuytren contracture performed under general anesthesia, the tourniquet is released and the surgical finger remains pale and cool to touch. The next appropriate steps are to flex the digit, warm the digit, and
1
apply topical phentolamine.
2
apply topical lidocaine.
3
administer intravenous heparin.
4
administer intravenous streptokinase.
- apply topical lidocaine._
QUESTION 51
of 100
Following application of topical lidocaine, copious arterial bleeding is noted from the region of 1 neurovascular bundle, and the digit remains cool and pale. What is the best next step?
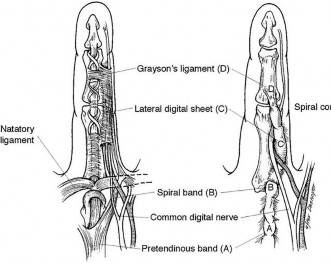
Following application of topical lidocaine, copious arterial bleeding is noted from the region of 1 neurovascular bundle, and the digit remains cool and pale. What is the best next step?
1
Intraoperative arteriogram
2
Wound closure and observation
3
Ligation of the digital artery
4
Primary repair of the digital artery
Figure 52
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
1. [Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226. ](http://www.ncbi.nlm.nih.gov/pubmed/17256226)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17256226)
2. [Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988. ](http://www.ncbi.nlm.nih.gov/pubmed/1769988)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1769988)
3. [Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263. ](http://www.ncbi.nlm.nih.gov/pubmed/11721263)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11721263)
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
1. [Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226. ](http://www.ncbi.nlm.nih.gov/pubmed/17256226)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17256226)
2. [Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988. ](http://www.ncbi.nlm.nih.gov/pubmed/1769988)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1769988)
3. [Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263. ](http://www.ncbi.nlm.nih.gov/pubmed/11721263)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11721263)
QUESTION 52
of 100
The video in Figure 56 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?

The video in Figure 56 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?
1
Triangular fibrocartilage complex (TFCC) repair
2
Lunotriquetral fusion
3
Distal radioulnar joint (DRUJ) tenodesis
4
Extensor carpi ulnaris (ECU) tendon sheath reconstruction
Upon examination, this patient is exhibiting dislocation of the ECU tendon because of a disrupted sheath. He has failed nonsurgical measures, so surgery that would involve either direct repair or reconstruction of the tendon sheath is indicated. An option for reconstruction is to use a portion of the extensor retinaculum as a sheath substitute. Deepening of the ECU tendon groove at the distal ulna with direct repair of the sheath is another option, although a 2016 paper by Ghatan and associates did not find depth of the groove as a risk factor for subluxation. TFCC repair, lunotriquetral fusion, and DRUJ tenodesis are not appropriate because the examination clearly shows ECU tendon dislocation. TFCC and lunotriquetral ligament tears can occur along with ECU tendon dislocation, but no other examination findings suggest these conditions for this patient.
RECOMMENDED READINGS
4. [MacLennan AJ, Nemechek NM, Waitayawinyu T, Trumble TE. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J Hand Surg Am. 2008 Jan;33(1):59-64. doi: 10.1016/j.jhsa.2007.10.002. PubMed PMID: 18261666. ](http://www.ncbi.nlm.nih.gov/pubmed/18261666)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18261666)
5. [Allende C, Le Viet D. Extensor carpi ulnaris problems at the wrist--classification, surgical treatment and results. J Hand Surg Br. 2005 Jun;30(3):265-72. Epub 2005 Apr 7.](http://www.ncbi.nlm.nih.gov/pubmed/15862366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15862366)
6. [Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br. 2001 Dec;26(6):556-9. PubMed PMID: 11884112. ](http://www.ncbi.nlm.nih.gov/pubmed/11884112)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884112)
7. [Ghatan AC, Puri SG, Morse KW, Hearns KA, von Althann C, Carlson MG. Relative Contribution of the Subsheath to Extensor Carpi Ulnaris Tendon Stability: Implications for Surgical Reconstruction and Rehabilitation. J Hand Surg Am. 2016 Feb;41(2):225-32. doi: 10.1016/j.jhsa.2015.10.024. Epub 2015 Dec 12. PubMed PMID: 26691954. ](http://www.ncbi.nlm.nih.gov/pubmed/26691954)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26691954)
RECOMMENDED READINGS
4. [MacLennan AJ, Nemechek NM, Waitayawinyu T, Trumble TE. Diagnosis and anatomic reconstruction of extensor carpi ulnaris subluxation. J Hand Surg Am. 2008 Jan;33(1):59-64. doi: 10.1016/j.jhsa.2007.10.002. PubMed PMID: 18261666. ](http://www.ncbi.nlm.nih.gov/pubmed/18261666)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18261666)
5. [Allende C, Le Viet D. Extensor carpi ulnaris problems at the wrist--classification, surgical treatment and results. J Hand Surg Br. 2005 Jun;30(3):265-72. Epub 2005 Apr 7.](http://www.ncbi.nlm.nih.gov/pubmed/15862366)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15862366)
6. [Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br. 2001 Dec;26(6):556-9. PubMed PMID: 11884112. ](http://www.ncbi.nlm.nih.gov/pubmed/11884112)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884112)
7. [Ghatan AC, Puri SG, Morse KW, Hearns KA, von Althann C, Carlson MG. Relative Contribution of the Subsheath to Extensor Carpi Ulnaris Tendon Stability: Implications for Surgical Reconstruction and Rehabilitation. J Hand Surg Am. 2016 Feb;41(2):225-32. doi: 10.1016/j.jhsa.2015.10.024. Epub 2015 Dec 12. PubMed PMID: 26691954. ](http://www.ncbi.nlm.nih.gov/pubmed/26691954)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26691954)
QUESTION 53
of 100
Four days after undergoing a coronary bypass graft, a 65-year-old man has tingling in his right-dominant little and ring fingers and weakness in his right hand. An examination reveals sensory loss in his right hand ring and small fingers and weakness in the flexor digitorum profundus of his small finger. What is the best next step?
Four days after undergoing a coronary bypass graft, a 65-year-old man has tingling in his right-dominant little and ring fingers and weakness in his right hand. An examination reveals sensory loss in his right hand ring and small fingers and weakness in the flexor digitorum profundus of his small finger. What is the best next step?
1
Assure the patient that his symptoms will subside in due time
2
Order MR imaging of the cervical spine
3
Order electromyography (EMG) and nerve conduction velocity studies
4
Pad the elbow medially and avoid attitudes of full elbow flexion
Perioperative neuropathies are multifocal in origin and not only related to positioning or pressure over the ulnar nerve. The most common major causes of neuropathy and ulnar neuropathies are stretch, compression, and ischemia, particularly associated with cardiac surgery. There can also be mechanical derangement of the nerve itself. Nerves that are asymptomatic but dysfunctional presurgically are susceptible to this injury during the surgical procedure. Symptoms are often bilateral.
Pure sensory lesions are frequently transient. Unlike motor lesions, most pure sensory lesions will improve within 3 to 5 days after diagnosis. Ulnar neuropathy is often bilateral, particularly for males, and can be detected by contralateral EMG studies. A nonsymptomatic limb often produces abnormal EMG study findings. Other factors that can be associated with ulnar neuropathy are body mass index of 35 or higher, prolonged bed rest, and history of substantial recent weight loss. With motor findings, these symptoms will probably be prolonged. EMG and nerve conduction studies are not indicated at this time, nor are radiographic cervical spine studies. The best thing to do initially is to protect the elbow and avoid the attitude of flexion.
RECOMMENDED READINGS
8. Alvine FG, Schurrer ME. Postoperative ulnar-nerve palsy. Are there predisposing factors? J Bone Joint Surg Am. 1987 Feb;69(2):255-9. PubMed PMID: 3805087.
9. Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994 Sep;19(5):817-20. PubMed PMID: 7806810.
Pure sensory lesions are frequently transient. Unlike motor lesions, most pure sensory lesions will improve within 3 to 5 days after diagnosis. Ulnar neuropathy is often bilateral, particularly for males, and can be detected by contralateral EMG studies. A nonsymptomatic limb often produces abnormal EMG study findings. Other factors that can be associated with ulnar neuropathy are body mass index of 35 or higher, prolonged bed rest, and history of substantial recent weight loss. With motor findings, these symptoms will probably be prolonged. EMG and nerve conduction studies are not indicated at this time, nor are radiographic cervical spine studies. The best thing to do initially is to protect the elbow and avoid the attitude of flexion.
RECOMMENDED READINGS
8. Alvine FG, Schurrer ME. Postoperative ulnar-nerve palsy. Are there predisposing factors? J Bone Joint Surg Am. 1987 Feb;69(2):255-9. PubMed PMID: 3805087.
9. Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994 Sep;19(5):817-20. PubMed PMID: 7806810.
QUESTION 54
of 100
Which treatment factor associated with the acute injury shown in the clinical photographs and radiograph (Figures 58a through 58c) is most important?



Which treatment factor associated with the acute injury shown in the clinical photographs and radiograph (Figures 58a through 58c) is most important?
1
Anatomic alignment of the fracture fragments
2
Splinting of the distal interphalangeal (DIP) joint in extension
3
Early motion of the PIP joint
4
Nail bed repair
This is an example of a closed-mallet deformity with disruption of the extensor tendon with a fracture. There is full passive correction of the deformity (Figure 58b). The radiograph does not show subluxation of the distal phalanx on the middle phalanx (Figure 58c), so the most important part of this treatment is to maintain the DIP joint in full extension for 6 to 8 weeks. This can be done with a dorsal or volar DIP joint splint with the proximal interphalangeal (PIP) joint free. PIP motion should be encouraged but is not the hallmark of treatment. The DIP joint should not be allowed to flex for the period of immobilization. Attention should be paid to the health of the dorsal skin. A transarticular Kirschner wire can be used to maintain extension for a patient who would have difficulty performing his or her occupation, such as a surgeon or dentist. Night splinting may be continued for another month. The fracture fragments do not need to be
anatomically aligned. This injury is not associated with a nail bed injury, so nail bed repair is not needed.
Mallet deformities result from extensor tendon disruption at the DIP joint through either tendon or bone. A functional range of motion with a minimal extensor lag will be obtained. Patients should be informed about the potential for a residual DIP extensor lag and swan-neck finger deformity with all methods of treatment.
RECOMMENDED READINGS
10. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005 Sep;13(5):336-
44/. Review. PubMed PMID: 16148359.
11. Leinberry C. Mallet finger injuries. J Hand Surg Am. 2009 Nov;34(9):1715-7. doi: 10.1016/j.jhsa.2009.06.018. Epub 2009 Sep 20. PubMed PMID: 19773131.
12. Renfree KJ. Acute, closed tendinous mallet injuries. J Hand Surg Am. 2014 Dec;39(12):2502-5; quiz 2505. doi: 10.1016/j.jhsa.2014.08.045. Epub 2014 Oct 22. PubMed PMID: 25443171.
13. Moradi A, Kachooei AR, Mudgal CS. Mallet fracture. J Hand Surg Am. 2014 Oct;39(10):2067-9. doi: 10.1016/j.jhsa.2014.06.022. Epub 2014 Aug 16. Review. PubMed PMID: 25135247.
anatomically aligned. This injury is not associated with a nail bed injury, so nail bed repair is not needed.
Mallet deformities result from extensor tendon disruption at the DIP joint through either tendon or bone. A functional range of motion with a minimal extensor lag will be obtained. Patients should be informed about the potential for a residual DIP extensor lag and swan-neck finger deformity with all methods of treatment.
RECOMMENDED READINGS
10. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005 Sep;13(5):336-
44/. Review. PubMed PMID: 16148359.
11. Leinberry C. Mallet finger injuries. J Hand Surg Am. 2009 Nov;34(9):1715-7. doi: 10.1016/j.jhsa.2009.06.018. Epub 2009 Sep 20. PubMed PMID: 19773131.
12. Renfree KJ. Acute, closed tendinous mallet injuries. J Hand Surg Am. 2014 Dec;39(12):2502-5; quiz 2505. doi: 10.1016/j.jhsa.2014.08.045. Epub 2014 Oct 22. PubMed PMID: 25443171.
13. Moradi A, Kachooei AR, Mudgal CS. Mallet fracture. J Hand Surg Am. 2014 Oct;39(10):2067-9. doi: 10.1016/j.jhsa.2014.06.022. Epub 2014 Aug 16. Review. PubMed PMID: 25135247.
QUESTION 55
of 100
A 53-year-old woman is experiencing thumb weakness. She has a remote history of a wrist fracture treated with a cast. She cannot lift her thumb off of a table when her hand is lying flat, palm-down. What is the most appropriate course of treatment?
A 53-year-old woman is experiencing thumb weakness. She has a remote history of a wrist fracture treated with a cast. She cannot lift her thumb off of a table when her hand is lying flat, palm-down. What is the most appropriate course of treatment?
1
Abductor pollicis longus reconstruction with palmaris autograft
2
Extensor pollicis brevis repair
3
Extensor pollicis longus (EPL) repair
4
Extensor indicis proprius (EIP) to extensor pollicis longus tendon transfer
The EPL is the only tendon that will lift a thumb off of a table as described. It is the most frequently ruptured tendon associated with distal radius fractures. Rupture is more common with nondisplaced fractures. Rupture after a nondisplaced or minimally displaced fracture suggests an ischemic etiology. The patient will not be able to lift her thumb off of a table with her hand lying flat, palm-down. Direct repair is often difficult because of retraction of tendon ends, atrophy, and
fraying. The EIP has a similar amplitude and direction of pull. Prerequisites for the use of the EIP to EPL tendon transfer include independent extension of the index finger.
RECOMMENDED READINGS
14. Shah MA, Buford WL, Viegas SF. Effects of extensor pollicis longus transposition and extensor indicis proprius transfer to extensor pollicis longus on thumb mechanics. J Hand Surg Am. 2003 Jul;28(4):661-
8/. PubMed PMID: 12877857.
15. Gelb RI. Tendon transfer for rupture of the extensor pollicis longus. Hand Clin. 1995 Aug;11(3):411-
22/. Review. PubMed PMID: 7559819.
fraying. The EIP has a similar amplitude and direction of pull. Prerequisites for the use of the EIP to EPL tendon transfer include independent extension of the index finger.
RECOMMENDED READINGS
14. Shah MA, Buford WL, Viegas SF. Effects of extensor pollicis longus transposition and extensor indicis proprius transfer to extensor pollicis longus on thumb mechanics. J Hand Surg Am. 2003 Jul;28(4):661-
8/. PubMed PMID: 12877857.
15. Gelb RI. Tendon transfer for rupture of the extensor pollicis longus. Hand Clin. 1995 Aug;11(3):411-
22/. Review. PubMed PMID: 7559819.
QUESTION 56
of 100
Figure 60a is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?


Figure 60a is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?
1
Supervised hand therapy
2
Hemi-hamate autograft
3
Dynamic external fixation
4
Open reduction and internal fixation (ORIF)
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A “V sign” (Figure 60b) is evident, indicating
dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress.
Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 60c through 60e.
RECOMMENDED READINGS
16. Calfee RP, Kiefhaber TR, Sommerkamp TG, Stern PJ. Hemi-hamate arthroplasty provides functional reconstruction of acute and chronic proximal interphalangeal fracture-dislocations. J Hand Surg Am. 2009 Sep;34(7):1232-41. doi: 10.1016/j.jhsa.2009.04.027. PubMed PMID: 19700071.
17. Frueh FS, Calcagni M, Lindenblatt N. The hemi-hamate autograft arthroplasty in proximal interphalangeal joint reconstruction: a systematic review. J Hand Surg Eur Vol. 2015 Jan;40(1):24-32. doi: 10.1177/1753193414554356. Epub 2014 Oct 22. Review. PubMed PMID: 25342651.
18. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP Fracture/Dislocation Treatment Technique: Use of a Hemi-Hamate Resurfacing Arthroplasty. Tech Hand Up Extrem Surg. 2002 Dec;6(4):185-92. PubMed PMID: 16520599.
19. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519.
dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress.
Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 60c through 60e.
RECOMMENDED READINGS
16. Calfee RP, Kiefhaber TR, Sommerkamp TG, Stern PJ. Hemi-hamate arthroplasty provides functional reconstruction of acute and chronic proximal interphalangeal fracture-dislocations. J Hand Surg Am. 2009 Sep;34(7):1232-41. doi: 10.1016/j.jhsa.2009.04.027. PubMed PMID: 19700071.
17. Frueh FS, Calcagni M, Lindenblatt N. The hemi-hamate autograft arthroplasty in proximal interphalangeal joint reconstruction: a systematic review. J Hand Surg Eur Vol. 2015 Jan;40(1):24-32. doi: 10.1177/1753193414554356. Epub 2014 Oct 22. Review. PubMed PMID: 25342651.
18. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP Fracture/Dislocation Treatment Technique: Use of a Hemi-Hamate Resurfacing Arthroplasty. Tech Hand Up Extrem Surg. 2002 Dec;6(4):185-92. PubMed PMID: 16520599.
19. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519.
QUESTION 57
of 100
A 35-year-old man has a markedly displaced distal radius fracture. An initial sensory examination is intact. He undergoes closed reduction of the fracture with acceptable restoration of alignment and is immobilized in a sugar-tong splint with the wrist in 5 degrees of flexion. Eighteen hours later, he returns to the emergency department with worsening pain and progressive numbness in his thumb and index and long fingers. He now cannot feel pin-prick in that distribution. His forearm is soft, minimally swollen, and nontender. What is the best next step?
A 35-year-old man has a markedly displaced distal radius fracture. An initial sensory examination is intact. He undergoes closed reduction of the fracture with acceptable restoration of alignment and is immobilized in a sugar-tong splint with the wrist in 5 degrees of flexion. Eighteen hours later, he returns to the emergency department with worsening pain and progressive numbness in his thumb and index and long fingers. He now cannot feel pin-prick in that distribution. His forearm is soft, minimally swollen, and nontender. What is the best next step?
1
Admission and observation
2
Fracture repair and carpal tunnel release
3
Fracture repair and fasciotomy
4
Change the sugar tong, placing the wrist in 15-degree extension
Acute carpal tunnel syndrome (CTS) can occur following wrist fracture, dislocation, or with any etiology that causes swelling hemorrhage into the carpal tunnel. It is important to differentiate from the more common chronic CTS; acute CTS is analogous to a compartment syndrome and warrants prompt release to optimize the outcome. Acute CTS can be clinically distinguished based upon the temporal history by progressively worsening pain and numbness, whereas a median nerve contusion causes immediate sensory loss posttrauma without the progression seen in acute CTS. Sometimes pressure measurements can help differentiate between contusions and acute CTS. An injection would be insufficient, and observation would result in a needless delay, increasing the chance for a poorer result. Forearm fasciotomy would not have a role here because the clinical findings indicate acute CTS and not a compartment syndrome of the forearm. The initial position of 5 degrees of flexion is not an extreme position for the nerve, and changing to 15 degrees of extension would not substantially relieve pressure within the carpal tunnel.
RECOMMENDED READINGS
20. Ford DJ, Ali MS. Acute carpal tunnel syndrome. Complications of delayed decompression. J Bone Joint Surg Br. 1986 Nov;68(5):758-9. PubMed PMID: 3782239.
21. Michelsen H, Posner MA. Medical history of carpal tunnel syndrome. Hand Clin. 2002 May;18(2):257-
68/. Review. PubMed PMID: 12371028.
RECOMMENDED READINGS
20. Ford DJ, Ali MS. Acute carpal tunnel syndrome. Complications of delayed decompression. J Bone Joint Surg Br. 1986 Nov;68(5):758-9. PubMed PMID: 3782239.
21. Michelsen H, Posner MA. Medical history of carpal tunnel syndrome. Hand Clin. 2002 May;18(2):257-
68/. Review. PubMed PMID: 12371028.
QUESTION 58
of 100
Figure 62 is the clinical photograph of a very functional 17-year-old boy with cerebral palsy and quadriplegia. He has no active supination but has full passive supination. His ability to determine position and sensibility without visual input are good. Radiographs show no osseous malalignment. Which treatment can best improve this patient’s function?

Figure 62 is the clinical photograph of a very functional 17-year-old boy with cerebral palsy and quadriplegia. He has no active supination but has full passive supination. His ability to determine position and sensibility without visual input are good. Radiographs show no osseous malalignment. Which treatment can best improve this patient’s function?
1
Physical therapy for supination strengthening
2
Humeral derotation osteotomy
3
Pronator quadratus muscle release
4
Pronator teres muscle transfer

The inability to actively supinate affects many functions; this patient has a pronation deformity of the forearm that affects function. Transfer of the pronator teres by rerouting the insertion point allows this muscle to act primarily as a supinator of the forearm rather than as a pronator. This can markedly improve his ability to accomplish activities of daily living. Release of the pronator quadratus is not necessary because there is full passive supination and no presurgical contracture. A physical therapy program would not be helpful in this situation because of the total absence, rather than weakness, of active supination. A humeral derotational osteotomy is not necessary because this patient has normal radiograph findings and bony alignment.
RECOMMENDED READINGS
22. Cobeljic G, Rajkovic S, Bajin Z, Lešic A, Bumbaširevic M, Aleksic M, Atkinson HD. The results of surgical treatment for pronation deformities of the forearm in cerebral palsy after a mean follow-up of
17.5 years. J Orthop Surg Res. 2015 Jul 8;10:106. doi: 10.1186/s13018-015-0251-3. PubMed PMID: 26152666.
23. Van Heest AE, House JH, Cariello C. Upper extremity surgical treatment of cerebral palsy. J Hand Surg Am. 1999 Mar;24(2):323-30. PubMed PMID: 10194018.
RECOMMENDED READINGS
22. Cobeljic G, Rajkovic S, Bajin Z, Lešic A, Bumbaširevic M, Aleksic M, Atkinson HD. The results of surgical treatment for pronation deformities of the forearm in cerebral palsy after a mean follow-up of
17.5 years. J Orthop Surg Res. 2015 Jul 8;10:106. doi: 10.1186/s13018-015-0251-3. PubMed PMID: 26152666.
23. Van Heest AE, House JH, Cariello C. Upper extremity surgical treatment of cerebral palsy. J Hand Surg Am. 1999 Mar;24(2):323-30. PubMed PMID: 10194018.
QUESTION 59
of 100
A closed reduction of a volar thumb metacarpophalangeal (MP) joint dislocation is less likely to be successful with
A closed reduction of a volar thumb metacarpophalangeal (MP) joint dislocation is less likely to be successful with
1
interposed sesamoids seen on radiograph.
2
a palpable extensor pollicis longus (EPL) tendon.
3
a nonpalpable abductor pollicis longus (APL) tendon.
4
a torn MP ulnar collateral ligament.
A volar thumb MP joint dislocation is an uncommon injury, occurring much less often than dorsal dislocation. Thumb volar MP dislocations often necessitate an open reduction because of interposed tissue including the EPL, extensor pollicis brevis (EPB), dorsal capsule, or volar plate. Several presurgical factors are associated with failure of a closed reduction. A closed reduction is less likely to be successful with no palpable EPL, displacement of the EPL or EPB, interposed sesamoids on radiographs, and paradoxical MP joint flexion and interphalangeal joint extension on attempting MP extension. The dorsal capsule is often noted to be disrupted following the injury, but this does not necessarily lead to an irreducible joint. The APL tendon inserts on the base of the thumb metacarpal and is not involved in the pathoanatomy of an irreducible MP dislocation. A collateral ligament injury is often associated with a volar thumb MP dislocation regardless of the ability to perform a closed reduction.
RECOMMENDED READINGS
24. Beck JD, Klena JC. Closed reduction and treatment of 2 volar thumb metacarpophalangeal dislocations: report of 2 cases. J Hand Surg Am. 2011 Apr;36(4):665-9. doi: 10.1016/j.jhsa.2010.12.006. Epub 2011 Feb 25. PubMed PMID: 21353397.
25. Hirata H, Takegami K, Nagakura T, Tsujii M, Uchida A. Irreducible volar subluxation of the metacarpophalangeal joint of the thumb. J Hand Surg Am. 2004 Sep;29(5):921-4. PubMed PMID: 15465245.
RECOMMENDED READINGS
24. Beck JD, Klena JC. Closed reduction and treatment of 2 volar thumb metacarpophalangeal dislocations: report of 2 cases. J Hand Surg Am. 2011 Apr;36(4):665-9. doi: 10.1016/j.jhsa.2010.12.006. Epub 2011 Feb 25. PubMed PMID: 21353397.
25. Hirata H, Takegami K, Nagakura T, Tsujii M, Uchida A. Irreducible volar subluxation of the metacarpophalangeal joint of the thumb. J Hand Surg Am. 2004 Sep;29(5):921-4. PubMed PMID: 15465245.
QUESTION 60
of 100
Figures 64a and 64b are the clinical photographs of a 46-year-old man with diabetes who has wound drainage and worsening hand pain. Which treatment is most appropriate?


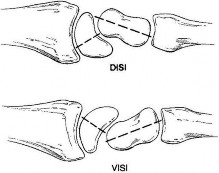
Figures 64a and 64b are the clinical photographs of a 46-year-old man with diabetes who has wound drainage and worsening hand pain. Which treatment is most appropriate?
1
Soaks and intravenous antibiotics
2
Soaks and oral antibiotics
3
Emergent surgical debridement
4
Immediate ray resection


This patient has the classic appearance of a collar button hand abscess. Although antibiotics, soaks, and elevation are important interventions, surgery is required. This infection rarely evolves into a flexor tenosynovitis, so decompression of the flexor tendon sheath is not indicated. Both volar and dorsal incisions often are required to effectively drain the abscess. Amputation is not appropriate as first-line treatment.
RECOMMENDED READINGS
26. McDonald LS, Bavaro MF, Hofmeister EP, Kroonen LT. Hand infections. J Hand Surg Am. 2011 Aug;36(8):1403-12. doi: 10.1016/j.jhsa.2011.05.035. Review. PubMed PMID: 21816297.
27. Osterman M, Draeger R, Stern P. Acute hand infections. J Hand Surg Am. 2014 Aug;39(8):1628-35; quiz 1635. doi: 10.1016/j.jhsa.2014.03.031. Review. PubMed PMID: 25070032.
**Question 65 of 100**
Dorsal intercalated segment instability (DISI) describes which carpal deformity?
1. Scaphoid extension
2. Lunate extension
3. Lunate flexion
4. Triquetral flexion
_PREFERRED RESPONSE: 2- Lunate extension_
**DISCUSSION**
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998 Jan-Feb;6(1):24-35. Review
Figure 65
The DISI deformity (Figure 65) simply describes dorsal lunate tilt or lunate extension on a lateral radiograph. DISI deformity usually occurs after dissociation between the lunate and the scaphoid (as in a scapholunate ligament tear). The scaphoid has a tendency to flex, and, when the scapholunate ligament is torn, the lunate loses its attachment to the scaphoid and shifts into an extended position.
The scaphoid does not extend when the scapholunate ligament is torn. The triquetral bone extends with the lunate, assuming there is an intact lunotriquetral ligament. The midcarpal joint and capitate extend when the lunate flexes. Conversely, when the lunate extends into a DISI deformity, the midcarpal joint tends to compensate with flexion at the capitolunate joint.
RECOMMENDED READINGS
28. Bednar JM, Osterman AL. Carpal Instability: Evaluation and Treatment. J Am Acad Orthop Surg. 1993 Oct;1(1):10-17. PubMed PMID: 10675851.
29. Walsh JJ, Berger RA, Cooney WP. Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg. 2002 Jan-Feb;10(1):32-42. Review. PubMed PMID: 11809049.
RECOMMENDED READINGS
26. McDonald LS, Bavaro MF, Hofmeister EP, Kroonen LT. Hand infections. J Hand Surg Am. 2011 Aug;36(8):1403-12. doi: 10.1016/j.jhsa.2011.05.035. Review. PubMed PMID: 21816297.
27. Osterman M, Draeger R, Stern P. Acute hand infections. J Hand Surg Am. 2014 Aug;39(8):1628-35; quiz 1635. doi: 10.1016/j.jhsa.2014.03.031. Review. PubMed PMID: 25070032.
**Question 65 of 100**
Dorsal intercalated segment instability (DISI) describes which carpal deformity?
1. Scaphoid extension
2. Lunate extension
3. Lunate flexion
4. Triquetral flexion
_PREFERRED RESPONSE: 2- Lunate extension_
**DISCUSSION**
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998 Jan-Feb;6(1):24-35. Review
Figure 65
The DISI deformity (Figure 65) simply describes dorsal lunate tilt or lunate extension on a lateral radiograph. DISI deformity usually occurs after dissociation between the lunate and the scaphoid (as in a scapholunate ligament tear). The scaphoid has a tendency to flex, and, when the scapholunate ligament is torn, the lunate loses its attachment to the scaphoid and shifts into an extended position.
The scaphoid does not extend when the scapholunate ligament is torn. The triquetral bone extends with the lunate, assuming there is an intact lunotriquetral ligament. The midcarpal joint and capitate extend when the lunate flexes. Conversely, when the lunate extends into a DISI deformity, the midcarpal joint tends to compensate with flexion at the capitolunate joint.
RECOMMENDED READINGS
28. Bednar JM, Osterman AL. Carpal Instability: Evaluation and Treatment. J Am Acad Orthop Surg. 1993 Oct;1(1):10-17. PubMed PMID: 10675851.
29. Walsh JJ, Berger RA, Cooney WP. Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg. 2002 Jan-Feb;10(1):32-42. Review. PubMed PMID: 11809049.
QUESTION 61
of 100
Figures 66a and 66b are the radiographs of a healthy 54-year-old right-hand-dominant man 3 months after he fell onto his outstretched left hand. He was initially treated with 8 weeks of closed reduction and casting. He reports ongoing ulnar-sided wrist pain, stiffness, and diminished function. An examination reveals a clinical sag deformity with a loss of radial length but no substantial swelling. The distal radius is nontender, and rotation is nearly full. Wrist motion is limited, with 55 degrees of flexion, 25 degrees of extension, and full digital motion. The most appropriate treatment is


Figures 66a and 66b are the radiographs of a healthy 54-year-old right-hand-dominant man 3 months after he fell onto his outstretched left hand. He was initially treated with 8 weeks of closed reduction and casting. He reports ongoing ulnar-sided wrist pain, stiffness, and diminished function. An examination reveals a clinical sag deformity with a loss of radial length but no substantial swelling. The distal radius is nontender, and rotation is nearly full. Wrist motion is limited, with 55 degrees of flexion, 25 degrees of extension, and full digital motion. The most appropriate treatment is
1
distal ulna excision (Darrach procedure).
2
wrist arthrodesis and distal ulna excision.
3
immediate distal radius corrective osteotomy.
4
delayed distal radius corrective osteotomy.


This patient has a substantial nascent malunion of his distal radius. Although a distal ulna excision would likely improve his ulnar-sided wrist pain, the Darrach procedure is more appropriate for older, somewhat less active individuals. In addition, the distal radius malunion is substantial, and it would be preferable to address the malunion given the major loss of radial length, inclination, and increased palmar tilt. The joint surface of the distal radius is uninvolved, and there is no evidence of arthrosis. It is preferable to osteotomize the distal radius sooner rather than later. Delayed osteotomy is often more difficult with more severe soft-tissue contractures, and improved results have been demonstrated following surgical treatment of nascent rather than mature distal radius malunions. Advantages include easier correction, no need for structural bone grafts, less overall total disability, and earlier return to work.
RECOMMENDED READINGS
30. Bilgin SS, Armangil M. Correction of nascent malunion of distal radius fractures. Acta Orthop Traumatol Turc. 2012;46(1):30-4. PubMed PMID: 22441449.
31. Jupiter JB, Ring D. A comparison of early and late reconstruction of malunited fractures of the distal end of the radius. J Bone Joint Surg Am. 1996 May;78(5):739-48. PubMed PMID: 8642031.
RECOMMENDED READINGS
30. Bilgin SS, Armangil M. Correction of nascent malunion of distal radius fractures. Acta Orthop Traumatol Turc. 2012;46(1):30-4. PubMed PMID: 22441449.
31. Jupiter JB, Ring D. A comparison of early and late reconstruction of malunited fractures of the distal end of the radius. J Bone Joint Surg Am. 1996 May;78(5):739-48. PubMed PMID: 8642031.
QUESTION 62
of 100
By which mechanism can a true aneurysm of the ulnar artery result?
By which mechanism can a true aneurysm of the ulnar artery result?
1
Stab wound
2
Arterial catheterization
3
Blunt trauma
4
Gunshot wound
True aneurysms contain all arterial layers. As such, they occur following an arterial injury that allows the vessel to gradually dilate. A true aneurysm is more uniform in shape and is characterized by having an endothelial lining. True aneurysms result from repeated blunt trauma or vessel diseases that weaken the wall. A pseudoaneurysm, or false aneurysm, results from an arterial wall penetration. The extravasated hematoma subsequently organizes and then recanalizes. The lumen of this false aneurysm has no endothelial lining. Pseudoaneurysms result from penetrating injuries from external sources or from fractures.
RECOMMENDED READINGS
32. Koman LA, Ruch DS, Smith BP, Smith TL. Vascular disorders. In: Green DP, Hotchkiss RN, Pederson WC, eds. Green’s Operative Hand Surgery. 4th ed. Philadelphia, PA: Churchill Livingstone; 1999:2286-2287
33. Ho PK, Weiland AJ, McClinton MA, Wilgis EF. Aneurysms of the upper extremity. J Hand Surg Am. 1987 Jan; 12(1):39-46. PubMed PMID: 3805642.
RECOMMENDED READINGS
32. Koman LA, Ruch DS, Smith BP, Smith TL. Vascular disorders. In: Green DP, Hotchkiss RN, Pederson WC, eds. Green’s Operative Hand Surgery. 4th ed. Philadelphia, PA: Churchill Livingstone; 1999:2286-2287
33. Ho PK, Weiland AJ, McClinton MA, Wilgis EF. Aneurysms of the upper extremity. J Hand Surg Am. 1987 Jan; 12(1):39-46. PubMed PMID: 3805642.
QUESTION 63
of 100
Figures 68a and 68b are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?


Figures 68a and 68b are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?
1
Long-arm thumb spica casting
2
Bracing and bone stimulation
3
Scaphoid excision with intercarpal fusion
4
Bone grafting with screw placement


Figures 68a and 68b show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present.
Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
RECOMMENDED READINGS
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
35. Buijze GA, Ochtman L, Ring D. Management of scaphoid nonunion. J Hand Surg Am. 2012 May;37(5):1095-100; quiz 1101. doi: 10.1016/j.jhsa.2012.03.002. Review. PubMed PMID: 22541157.
Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
RECOMMENDED READINGS
34. Kawamura K, Chung KC. Treatment of scaphoid fractures and nonunions. J Hand Surg Am. 2008 Jul-Aug;33(6):988-97. doi: 10.1016/j.jhsa.2008.04.026. Review. PubMed PMID: 18656779.
35. Buijze GA, Ochtman L, Ring D. Management of scaphoid nonunion. J Hand Surg Am. 2012 May;37(5):1095-100; quiz 1101. doi: 10.1016/j.jhsa.2012.03.002. Review. PubMed PMID: 22541157.
QUESTION 64
of 100
Figures 69a and 69b are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is
currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, midrange wrist motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment?


Figures 69a and 69b are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is
currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, midrange wrist motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment?
1
Proximal row carpectomy
2
Radial shortening osteotomy and vascularized bone grafting
3
Scaphoid excision and midcarpal arthrodesis
4
Capitate hamate fusion
This patient has late-stage Kienböck disease. According to the Lichtman classification for Kienböck disease, this would represent stage IIIB, with lunate collapse/fragmentation, loss of carpal height secondary to proximal capitate migration, and a flexed scaphoid. The lateral radiograph reveals a radioscaphoid angle exceeding 60 degrees, so disease stage is IIIB. According to Condit and associates, when the presurgical radioscaphoid angle exceeds 60 degrees, results are poor when an attempt to maintain the lunate is made. As a result, the procedure with the most predictable outcome is a proximal row carpectomy. A radial-shortening osteotomy could be performed because the ulnar variance is negative. Considering the marked lunate fragmentation and collapse, a vascularized bone graft likely is contraindicated and associated with less predictable results than a proximal row carpectomy. There is no role for supervised hand therapy and splinting in the setting of advanced Kienböck disease. Similarly, there is no role for maintenance of the lunate in the setting of advanced collapse and fragmentation.
RECOMMENDED READINGS
36. Condit DP, Idler RS, Fischer TJ, Hastings H 2nd. Preoperative factors and outcome after lunate decompression for Kienböck's disease. J Hand Surg Am. 1993 Jul;18(4):691-6. PubMed PMID: 8349983.
37. Goldfarb CA, Hsu J, Gelberman RH, Boyer MI. The Lichtman classification for Kienböck's disease: an assessment of reliability. J Hand Surg Am. 2003 Jan;28(1):74-80. PubMed PMID: 12563641.
38. Lichtman DM, Mack GR, MacDonald RI, Gunther SF, Wilson JN. Kienböck's disease: the role of silicone replacement arthroplasty. J Bone Joint Surg Am. 1977 Oct;59(7):899-908. PubMed PMID: 908720.
39. Nakamura R, Horii E, Watanabe K, Nakao E, Kato H, Tsunoda K. Proximal row carpectomy versus limited wrist arthrodesis for advanced Kienböck's disease. J Hand Surg Br. 1998 Dec;23(6):741-5. PubMed PMID: 9888672.
RECOMMENDED READINGS
36. Condit DP, Idler RS, Fischer TJ, Hastings H 2nd. Preoperative factors and outcome after lunate decompression for Kienböck's disease. J Hand Surg Am. 1993 Jul;18(4):691-6. PubMed PMID: 8349983.
37. Goldfarb CA, Hsu J, Gelberman RH, Boyer MI. The Lichtman classification for Kienböck's disease: an assessment of reliability. J Hand Surg Am. 2003 Jan;28(1):74-80. PubMed PMID: 12563641.
38. Lichtman DM, Mack GR, MacDonald RI, Gunther SF, Wilson JN. Kienböck's disease: the role of silicone replacement arthroplasty. J Bone Joint Surg Am. 1977 Oct;59(7):899-908. PubMed PMID: 908720.
39. Nakamura R, Horii E, Watanabe K, Nakao E, Kato H, Tsunoda K. Proximal row carpectomy versus limited wrist arthrodesis for advanced Kienböck's disease. J Hand Surg Br. 1998 Dec;23(6):741-5. PubMed PMID: 9888672.
QUESTION 65
of 100
Figures 70a through 70c are the radiographs of a 55-year-old woman who underwent a volar plating of an extra-articular distal radius fracture 2 weeks ago. She is experiencing weakness with flexion of the interphalangeal (IP) thumb joint. IP joint flexion was normal before surgery. What is the best next step?


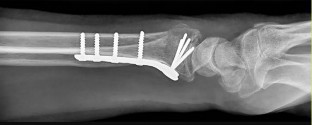
Figures 70a through 70c are the radiographs of a 55-year-old woman who underwent a volar plating of an extra-articular distal radius fracture 2 weeks ago. She is experiencing weakness with flexion of the interphalangeal (IP) thumb joint. IP joint flexion was normal before surgery. What is the best next step?
1
Observation
2
Electromyogram/nerve conduction study (EMG/NCS)
3
CT scan
4
Immediate exploration
Treatment of a displaced or unstable distal radius fracture with a volar plate is common. The differential diagnosis of flexor pollicis longus (FPL) dysfunction after volar plating of a distal radius fracture includes scar entrapment of the FPL tendon, hardware irritation, FPL impingement or rupture, and injury to the anterior interosseous nerve.
Prevalence of flexor tendon rupture after distal radius fracture is between 2% and 12%. The FPL tendon is the most common flexor tendon rupture associated with volar plating. It is usually seen with plates that are distal to the watershed line (W) and with plates extending volar to the critical line (C) (Figure 70d). The watershed line (W) is the location of the origin of the volar carpal ligaments and the bone prominence at which flexor tendons are most closely opposed to the distal radius (Figure 70d). In this scenario, the lateral radiograph shows that the plate is not distal to the watershed line (W) and is between the critical line (C) and the line parallel to the volar cortex of the radius (R). This is the optimal position for the plate. Placement of a volar locking plate distal to the watershed line of the distal radius and excessive plate prominence has been associated with FPL tendon rupture.
This patient is only 2 weeks past surgery and there is some FPL function. FPL weakness after volar distal radius plating is common and has been seen in as many as 50% of patients. This usually recovers spontaneously by 2 months, and no treatment is needed. A nerve conduction study would be indicated if an anterior interosseous nerve compression were considered, but it is too early for this test. A CT scan could be obtained to judge the alignment of the fracture fragment and position of the screws, but it is not indicated in this case. Exploration could be performed if an FPL rupture were considered, but, because it is only 2 weeks after surgery, there is some FPL function, the plate is proximal to the watershed line, and immediate exploration is not indicated. If this does not improve after 2 to 3 months, further investigation with ultrasound or MRI would be indicated.
RECOMMENDED READINGS
40. Chilelli BJ, Patel RM, Kalainov DM, Peng J, Zhang LQ. Flexor pollicis longus dysfunction after volar plate fixation of distal radius fractures. J Hand Surg Am. 2013 Sep;38(9):1691-7. doi: 10.1016/j.jhsa.2013.06.005. Epub 2013 Jul 30. PubMed PMID: 23910382.
41. Soong M, Earp BE, Bishop G, Leung A, Blazar P. Volar locking plate implant prominence and flexor tendon rupture. J Bone Joint Surg Am. 2011 Feb 16;93(4):328-35. doi: 10.2106/JBJS.J.00193. Epub 2011 Jan 14. PubMed PMID: 21239658.
42. Agnew SP, Ljungquist KL, Huang JI. Danger zones for flexor tendons in volar plating of distal radius fractures. J Hand Surg Am. 2015 Jun;40(6):1102-5. doi: 10.1016/j.jhsa.2015.02.026. Epub 2015 Apr
2/. PubMed PMID: 25843531.
43. Griffin JW, Chhabra AB. Complications after volar plating of distal radius fractures. J Hand Surg Am. 2014 Jun;39(6):1183-5; quiz 1186. doi: 10.1016/j.jhsa.2014.03.038. Epub 2014 May 5. Review.
PubMed PMID: 24810935.
Prevalence of flexor tendon rupture after distal radius fracture is between 2% and 12%. The FPL tendon is the most common flexor tendon rupture associated with volar plating. It is usually seen with plates that are distal to the watershed line (W) and with plates extending volar to the critical line (C) (Figure 70d). The watershed line (W) is the location of the origin of the volar carpal ligaments and the bone prominence at which flexor tendons are most closely opposed to the distal radius (Figure 70d). In this scenario, the lateral radiograph shows that the plate is not distal to the watershed line (W) and is between the critical line (C) and the line parallel to the volar cortex of the radius (R). This is the optimal position for the plate. Placement of a volar locking plate distal to the watershed line of the distal radius and excessive plate prominence has been associated with FPL tendon rupture.
This patient is only 2 weeks past surgery and there is some FPL function. FPL weakness after volar distal radius plating is common and has been seen in as many as 50% of patients. This usually recovers spontaneously by 2 months, and no treatment is needed. A nerve conduction study would be indicated if an anterior interosseous nerve compression were considered, but it is too early for this test. A CT scan could be obtained to judge the alignment of the fracture fragment and position of the screws, but it is not indicated in this case. Exploration could be performed if an FPL rupture were considered, but, because it is only 2 weeks after surgery, there is some FPL function, the plate is proximal to the watershed line, and immediate exploration is not indicated. If this does not improve after 2 to 3 months, further investigation with ultrasound or MRI would be indicated.
RECOMMENDED READINGS
40. Chilelli BJ, Patel RM, Kalainov DM, Peng J, Zhang LQ. Flexor pollicis longus dysfunction after volar plate fixation of distal radius fractures. J Hand Surg Am. 2013 Sep;38(9):1691-7. doi: 10.1016/j.jhsa.2013.06.005. Epub 2013 Jul 30. PubMed PMID: 23910382.
41. Soong M, Earp BE, Bishop G, Leung A, Blazar P. Volar locking plate implant prominence and flexor tendon rupture. J Bone Joint Surg Am. 2011 Feb 16;93(4):328-35. doi: 10.2106/JBJS.J.00193. Epub 2011 Jan 14. PubMed PMID: 21239658.
42. Agnew SP, Ljungquist KL, Huang JI. Danger zones for flexor tendons in volar plating of distal radius fractures. J Hand Surg Am. 2015 Jun;40(6):1102-5. doi: 10.1016/j.jhsa.2015.02.026. Epub 2015 Apr
2/. PubMed PMID: 25843531.
43. Griffin JW, Chhabra AB. Complications after volar plating of distal radius fractures. J Hand Surg Am. 2014 Jun;39(6):1183-5; quiz 1186. doi: 10.1016/j.jhsa.2014.03.038. Epub 2014 May 5. Review.
PubMed PMID: 24810935.
QUESTION 66
of 100
The success of proximal interphalangeal (PIP) joint arthroplasty for arthritis at the index finger PIP joint is dependent upon


The success of proximal interphalangeal (PIP) joint arthroplasty for arthritis at the index finger PIP joint is dependent upon
1
ulnar collateral ligament stability.
2
radial collateral ligament stability.
3
use of a nonconstrained prosthesis.
4
use of a dorsal surgical approach.
PIP joint arthroplasty is a surgical treatment option for patients with PIP joint arthritis. However, this procedure is dependent upon radial collateral ligament stability, even when a 1-piece silicone implant is used. A key pinch or pinching the thumb tip to the radial aspect of the index finger middle phalanx places tremendous load on the radial collateral ligament of the index PIP joint. Presurgical instability, surgical technique, and surgical dissection are important variables; arthroplasty may threaten the integrity of the ligament. As a result, most surgeons will recommend PIP joint fusion for the index finger, which plays a role in key pinch, and will offer PIP joint arthroplasty for the long and ring fingers, for which there is less thumb-to-side pinching and motion is a priority.
Arthrodesis limits motion but is associated with better reliability over the long term compared to arthroplasty for the PIP joint of the index finger. Infection is no more likely at the index PIP joint than at any other joint. Although a silicone (1-piece) arthroplasty may help in cases of collateral ligament instability, it is not required if the radial collateral ligament can be preserved or satisfactorily reconstructed. Both volar and dorsal approaches for PIP arthroplasty have been described without producing conclusive evidence demonstrating superiority of 1 approach over the other.
RECOMMENDED READINGS
44. Pellegrini VD Jr, Burton RI. Osteoarthritis of the proximal interphalangeal joint of the hand: arthroplasty or fusion? J Hand Surg Am. 1990 Mar;15(2):194-209. PubMed PMID: 2133611.
45. Branam BR, Tuttle HG, Stern PJ, Levin L. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007 Jul-Aug;32(6):775-88. PubMed PMID: 17606054.
CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 77
Figures 72a through 72b are the radiographs of a 45-year-old man who has severe right wrist pain and paresthesias in the median nerve distribution following a fall from a ladder.
Arthrodesis limits motion but is associated with better reliability over the long term compared to arthroplasty for the PIP joint of the index finger. Infection is no more likely at the index PIP joint than at any other joint. Although a silicone (1-piece) arthroplasty may help in cases of collateral ligament instability, it is not required if the radial collateral ligament can be preserved or satisfactorily reconstructed. Both volar and dorsal approaches for PIP arthroplasty have been described without producing conclusive evidence demonstrating superiority of 1 approach over the other.
RECOMMENDED READINGS
44. Pellegrini VD Jr, Burton RI. Osteoarthritis of the proximal interphalangeal joint of the hand: arthroplasty or fusion? J Hand Surg Am. 1990 Mar;15(2):194-209. PubMed PMID: 2133611.
45. Branam BR, Tuttle HG, Stern PJ, Levin L. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007 Jul-Aug;32(6):775-88. PubMed PMID: 17606054.
CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 77
Figures 72a through 72b are the radiographs of a 45-year-old man who has severe right wrist pain and paresthesias in the median nerve distribution following a fall from a ladder.
QUESTION 67
of 100
What is the most appropriate initial treatment?
What is the most appropriate initial treatment?
1
Cast immobilization
2
Closed reduction
3
Admission, observation, and elevation
4
Carpal tunnel injection
- Closed reduction_
QUESTION 68
of 100
Which ligament remains intact in this injury?
Which ligament remains intact in this injury?
1
Short radiolunate
2
Long radiolunate
3
Radioscaphocapitate
4
Scapholunate
Perilunate dislocations (Figure 72c) are relatively rare but make up an important spectrum of carpal pathology. These injuries are typically associated with high-energy trauma such as a motor vehicle collision or a fall from height. Mayfield and associates described a series of injuries using 4 stages with predictable disruption to the scapholunate articulation (stage 1), lunocapitate articulation (stage 2), and lunotriquetral articulation (stage 3) prior to allowing for a lunate dislocation into the carpal tunnel (stage 4) through the space of Poirier. These authors distinguished these purely ligamentous “lesser arc injuries” from “greater arc injuries” in which the energy absorbed by the wrist leads to fractures of the radius, capitate, triquetrum, and ulnar styloid.
On radiographic assessment, the posterior-anterior view typically shows disruption of “Gilula’s arcs,” which are formed by the proximal and distal articular surfaces of the proximal row and the proximal cortical margins of the distal row. On the lateral view, a perilunate dislocation will show a lunate that is in its normal position on the radius within the lunate fossa. The carpus will typically be displaced dorsally. A lunate dislocation (stage 4 injury) such as seen in this scenario will reveal the lunate displaced volarly into the carpal tunnel. The short radiolunate ligament remains intact in a lunate dislocation, which allows for the lunate to remain attached to the radius. The lunate typically causes direct compression of the median nerve in the carpal tunnel and is 1 reason why patients often have acute carpal tunnel syndrome. Although the bony and ligamentous injuries can be addressed electively within a few days of injury, acute carpal tunnel is a surgical emergency and should be addressed within the first few hours after diagnosis. An emergency department reduction of a lunate dislocation can be attempted and, if successful, may decrease carpal tunnel symptoms and obviate the need for emergent surgery. In cases in which the lunate is in the carpal tunnel, a combined dorsal and volar approach should be used. The volar approach allows for carpal tunnel release and direct reduction of the lunate. The dorsal approach allows for better visualization of the carpus and fixation of associated bony fractures and ligament injuries. Closed reduction and pinning can lead to worse outcomes following treatment.
RECOMMENDED READINGS
46. Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am. 1980 May;5(3):226-41. PubMed PMID: 7400560.
47. Gilula LA. Carpal injuries: analytic approach and case exercises. AJR Am J Roentgenol. 1979 Sep;133(3):503-17. Review. PubMed PMID: 111512.
48. Sotereanos DG, Mitsionis GJ, Giannakopoulos PN, Tomaino MM, Herndon JH. Perilunate dislocation and fracture dislocation: a critical analysis of the volar-dorsal approach. J Hand Surg Am. 1997 Jan;22(1):49-56. PubMed PMID: 9018612.
On radiographic assessment, the posterior-anterior view typically shows disruption of “Gilula’s arcs,” which are formed by the proximal and distal articular surfaces of the proximal row and the proximal cortical margins of the distal row. On the lateral view, a perilunate dislocation will show a lunate that is in its normal position on the radius within the lunate fossa. The carpus will typically be displaced dorsally. A lunate dislocation (stage 4 injury) such as seen in this scenario will reveal the lunate displaced volarly into the carpal tunnel. The short radiolunate ligament remains intact in a lunate dislocation, which allows for the lunate to remain attached to the radius. The lunate typically causes direct compression of the median nerve in the carpal tunnel and is 1 reason why patients often have acute carpal tunnel syndrome. Although the bony and ligamentous injuries can be addressed electively within a few days of injury, acute carpal tunnel is a surgical emergency and should be addressed within the first few hours after diagnosis. An emergency department reduction of a lunate dislocation can be attempted and, if successful, may decrease carpal tunnel symptoms and obviate the need for emergent surgery. In cases in which the lunate is in the carpal tunnel, a combined dorsal and volar approach should be used. The volar approach allows for carpal tunnel release and direct reduction of the lunate. The dorsal approach allows for better visualization of the carpus and fixation of associated bony fractures and ligament injuries. Closed reduction and pinning can lead to worse outcomes following treatment.
RECOMMENDED READINGS
46. Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am. 1980 May;5(3):226-41. PubMed PMID: 7400560.
47. Gilula LA. Carpal injuries: analytic approach and case exercises. AJR Am J Roentgenol. 1979 Sep;133(3):503-17. Review. PubMed PMID: 111512.
48. Sotereanos DG, Mitsionis GJ, Giannakopoulos PN, Tomaino MM, Herndon JH. Perilunate dislocation and fracture dislocation: a critical analysis of the volar-dorsal approach. J Hand Surg Am. 1997 Jan;22(1):49-56. PubMed PMID: 9018612.
QUESTION 69
of 100
Figures 75a and 75b are the initial radiographs from a volar plating of the distal radius performed 8 months previously. This patient has not been able to actively extend her thumb for 2 days. What is the most appropriate course of treatment?


Figures 75a and 75b are the initial radiographs from a volar plating of the distal radius performed 8 months previously. This patient has not been able to actively extend her thumb for 2 days. What is the most appropriate course of treatment?
1
Cast placement, keeping the thumb in a fully extended position for 4 weeks
2
Repair of the extensor pollicis longus (EPL) tendon and hardware removal
3
Removal of hardware with tendon transfer of the extensor indicis proprius (EIP) to the EPL
4
Tendon transfer of the EIP to the EPL
Although the fracture is aligned in an anatomic position, there is prominence of at least 1 of the distal screws noted on the lateral radiograph view. Most likely, the prominent screw(s) is the cause of EPL tendon rupture. The best solution is removal of offending hardware combined with EIP to
EPL tendon transfer. If the tendon transfer is performed without hardware removal, the prominent screw(s) may rupture the adjacent extensor tendons. Also, it is rarely possible to repair the EPL tendon primarily because of damage to the tendon over a long segment. Casting would not provide any benefit in this situation. This problem can be avoided by using screws that do not violate the dorsal cortex.
RECOMMENDED READINGS
49. Berglund LM, Messer TM. Complications of volar plate fixation for managing distal radius fractures. J Am Acad Orthop Surg. 2009 Jun;17(6):369-77. Review. PubMed PMID: 19474446.
50. Benson EC, DeCarvalho A, Mikola EA, Veitch JM, Moneim MS. Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res. 2006 Oct;451:218-22. PubMed PMID: 16770281.
EPL tendon transfer. If the tendon transfer is performed without hardware removal, the prominent screw(s) may rupture the adjacent extensor tendons. Also, it is rarely possible to repair the EPL tendon primarily because of damage to the tendon over a long segment. Casting would not provide any benefit in this situation. This problem can be avoided by using screws that do not violate the dorsal cortex.
RECOMMENDED READINGS
49. Berglund LM, Messer TM. Complications of volar plate fixation for managing distal radius fractures. J Am Acad Orthop Surg. 2009 Jun;17(6):369-77. Review. PubMed PMID: 19474446.
50. Benson EC, DeCarvalho A, Mikola EA, Veitch JM, Moneim MS. Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res. 2006 Oct;451:218-22. PubMed PMID: 16770281.
QUESTION 70
of 100
A 50-year-old man has had persistent pain in his index finger proximal interphalangeal (PIP) joint because of degenerative joint disease despite undergoing nonsurgical treatment. His PIP range of motion is between 20 and 40 degrees. Which surgical procedure will be associated with the lowest risk for long-term complications for this patient?
A 50-year-old man has had persistent pain in his index finger proximal interphalangeal (PIP) joint because of degenerative joint disease despite undergoing nonsurgical treatment. His PIP range of motion is between 20 and 40 degrees. Which surgical procedure will be associated with the lowest risk for long-term complications for this patient?
1
Arthrodesis
2
Pyrocarbon arthroplasty
3
Silicone arthroplasty
4
Distraction arthroplasty
The surgical options for PIP arthritis include arthrodesis and arthroplasty. PIP arthrodesis is considered for patients with high-demand jobs, joint instability, loss of bone stock, presurgical range of motion of less than 30 degrees, and involvement of the index finger. Following PIP arthroplasty, pain relief and 40 to 60 degrees of motion can be expected. Silicone implants are not considered for PIP arthroplasty of the index and long fingers for active patients because of risk for implant failure likely related to high stress. Vitale and associates compared 65 patients with an index finger PIP arthroplasty to 14 patients with an index finger PIP arthrodesis. At median followup of 67 months, they reported a 4.3 times increased risk for complications among patients undergoing arthroplasty. In light of these findings, the authors of the study changed their practice
to arthrodesis rather than arthroplasty for the symptomatic index finger PIP joint. Distraction arthroplasty is not performed for the PIP joint.
RECOMMENDED READINGS
51. Keller TC, Seamon JB, Dacus AR. Treatment of osteoarthritic conditions of the hand. In: Chung KC, Murray PM. eds. Hand Surgery Update V. Rosemont, IL: American Society for Surgery of the Hand; 2012: 505-519.
52. Vitale MA, Fruth KM, Rizzo M, Moran SL, Kakar S. Prosthetic Arthroplasty Versus Arthrodesis for Osteoarthritis and Posttraumatic Arthritis of the Index Finger Proximal Interphalangeal Joint. J Hand Surg Am. 2015 Oct;40(10):1937-48. doi: 10.1016/j.jhsa.2015.05.021. Epub 2015 Jul 15. PubMed PMID: 26188383.
53. Stern PJ, Ho S. Osteoarthritis of the proximal interphalangeal joint. Hand Clin. 1987 Aug;3(3):405-13. PubMed PMID: 3654772.
to arthrodesis rather than arthroplasty for the symptomatic index finger PIP joint. Distraction arthroplasty is not performed for the PIP joint.
RECOMMENDED READINGS
51. Keller TC, Seamon JB, Dacus AR. Treatment of osteoarthritic conditions of the hand. In: Chung KC, Murray PM. eds. Hand Surgery Update V. Rosemont, IL: American Society for Surgery of the Hand; 2012: 505-519.
52. Vitale MA, Fruth KM, Rizzo M, Moran SL, Kakar S. Prosthetic Arthroplasty Versus Arthrodesis for Osteoarthritis and Posttraumatic Arthritis of the Index Finger Proximal Interphalangeal Joint. J Hand Surg Am. 2015 Oct;40(10):1937-48. doi: 10.1016/j.jhsa.2015.05.021. Epub 2015 Jul 15. PubMed PMID: 26188383.
53. Stern PJ, Ho S. Osteoarthritis of the proximal interphalangeal joint. Hand Clin. 1987 Aug;3(3):405-13. PubMed PMID: 3654772.
QUESTION 71
of 100
Figures 77a and 77b are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 6 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem?


Figures 77a and 77b are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 6 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem?
1
Postsurgical tendon adhesion
2
Laceration of the extensor digitorum communis (EDC) tendons to long and ring fingers
3
Laceration of a branch of the posterior interosseous nerve (PIN)
4
Neuropraxia of the PIN
Plating of the proximal radius from a dorsal or Thompson approach (between the extensor carpi radialis brevis and extensor digitorum communis) allows complete visualization of the PIN
through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 77a and 77b.
Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the extensor indicis proprius and the EDC of the ring finger to the extensor digiti quinti proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the mobile wad and the digital extensors will be more easily found.
RECOMMENDED READINGS
54. Lister GD, Belsole RB, Kleinert HE. The radial tunnel syndrome. J Hand Surg Am. 1979 Jan;4(1):52-
9/. PubMed PMID: 759504.
55. Konjengbam M, Elangbam J. Radial nerve in the radial tunnel: anatomic sites of entrapment neuropathy. Clin Anat. 2004 Jan;17(1):21-5. PubMed PMID: 14695583.
56. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part I: radial nerve. J Hand Surg Am. 2009 Dec;34(10):1906-14. doi: 10.1016/j.jhsa.2009.10.016. PubMed PMID: 19969199.
through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 77a and 77b.
Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the extensor indicis proprius and the EDC of the ring finger to the extensor digiti quinti proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the mobile wad and the digital extensors will be more easily found.
RECOMMENDED READINGS
54. Lister GD, Belsole RB, Kleinert HE. The radial tunnel syndrome. J Hand Surg Am. 1979 Jan;4(1):52-
9/. PubMed PMID: 759504.
55. Konjengbam M, Elangbam J. Radial nerve in the radial tunnel: anatomic sites of entrapment neuropathy. Clin Anat. 2004 Jan;17(1):21-5. PubMed PMID: 14695583.
56. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part I: radial nerve. J Hand Surg Am. 2009 Dec;34(10):1906-14. doi: 10.1016/j.jhsa.2009.10.016. PubMed PMID: 19969199.
QUESTION 72
of 100
Nerve conduction velocity is slowed by
Nerve conduction velocity is slowed by
1
increased skin temperature.
2
increased perineural blood flow.
3
external compression.
4
hand dominance.
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no association between hand dominance and nerve conduction velocity.
RECOMMENDED READINGS
57. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
58. Freedman M, Helber G, Pothast J, Shahwan TG, Simon J, Sher L. Electrodiagnostic evaluation of compressive nerve injuries of the upper extremities. Orthop Clin North Am. 2012 Oct;43(4):409-16. doi:10.1016/j.ocl.2012.07.010. Epub 2012 Sep 10. Review. PubMed PMID: 23026456.
59. Lundborg G. A 25-year perspective of peripheral nerve surgery: evolving neuroscientific concepts and clinical significance. J Hand Surg Am. 2000 May;25(3):391-414. Review. PubMed PMID: 10811744.
RECOMMENDED READINGS
57. Dodds SD. Peripheral Nervous System. In Boyer MI, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:113-126.
58. Freedman M, Helber G, Pothast J, Shahwan TG, Simon J, Sher L. Electrodiagnostic evaluation of compressive nerve injuries of the upper extremities. Orthop Clin North Am. 2012 Oct;43(4):409-16. doi:10.1016/j.ocl.2012.07.010. Epub 2012 Sep 10. Review. PubMed PMID: 23026456.
59. Lundborg G. A 25-year perspective of peripheral nerve surgery: evolving neuroscientific concepts and clinical significance. J Hand Surg Am. 2000 May;25(3):391-414. Review. PubMed PMID: 10811744.
QUESTION 73
of 100
Assuming that the fracture shown in this radiograph (Figure 79) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active
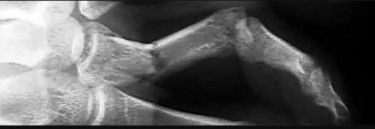
Assuming that the fracture shown in this radiograph (Figure 79) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active
1
metacarpophalangeal (MP) joint extension.
2
proximal interphalangeal (PIP) joint extension.
3
MP flexion.
4
PIP joint flexion.
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints.
RECOMMENDED READINGS
60. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008 Oct;16(10):586-95. Review. PubMed PMID: 18832602.
61. Faruqui S, Stern PJ, Kiefhaber TR. Percutaneous pinning of fractures in the proximal third of the proximal phalanx: complications and outcomes. J Hand Surg Am. 2012 Jul;37(7):1342-8. doi: 10.1016/j.jhsa.2012.04.019. PubMed PMID: 22721457.
RECOMMENDED READINGS
60. Henry MH. Fractures of the proximal phalanx and metacarpals in the hand: preferred methods of stabilization. J Am Acad Orthop Surg. 2008 Oct;16(10):586-95. Review. PubMed PMID: 18832602.
61. Faruqui S, Stern PJ, Kiefhaber TR. Percutaneous pinning of fractures in the proximal third of the proximal phalanx: complications and outcomes. J Hand Surg Am. 2012 Jul;37(7):1342-8. doi: 10.1016/j.jhsa.2012.04.019. PubMed PMID: 22721457.
QUESTION 74
of 100
A 45-year-old right-hand-dominant man has stiffness of his right ring finger 6 months after an 8-foot fall from a ladder. The patient recalls immediate pain and a “tearing” sensation in his finger right after sustaining the injury and reports a progressive loss of digital extension despite undergoing 5 months of supervised hand therapy. An examination demonstrates active and passive proximal interphalangeal (PIP) joint motion of 60 degrees/100 degrees with active distal interphalangeal (DIP) joint motion of 0/45 degrees. Radiograph findings are normal. What is the most appropriate course of treatment?
A 45-year-old right-hand-dominant man has stiffness of his right ring finger 6 months after an 8-foot fall from a ladder. The patient recalls immediate pain and a “tearing” sensation in his finger right after sustaining the injury and reports a progressive loss of digital extension despite undergoing 5 months of supervised hand therapy. An examination demonstrates active and passive proximal interphalangeal (PIP) joint motion of 60 degrees/100 degrees with active distal interphalangeal (DIP) joint motion of 0/45 degrees. Radiograph findings are normal. What is the most appropriate course of treatment?
1
Continued supervised therapy with the addition of dynamic splinting
2
PIP joint volar release and flexor tendon reconstruction followed by immediate supervised therapy
3
PIP joint volar release and flexor tenolysis followed by immediate supervised therapy
4
PIP joint volar release, pulley reconstruction, and temporary PIP joint pinning followed by immediate supervised therapy
This is a classic example of a flexor tendon sheath rupture with gradual loss of active and passive extension and an unremarkable radiograph. Originally described by Bollen in 67 British rock climbers, closed ruptures of the digital flexor pulley system often appear in a delayed fashion with PIP joint flexion contractures. The mechanism of injury is a rapidly applied extension force in the acutely flexed digit, resulting in a closed rupture of the retinacular sheath, rather than a flexor profundus avulsion. In the setting of a significant PIP flexion contracture, a rupture of multiple pulleys including A2, A3, and A4 most commonly is found. In such a scenario, significant flexor tendon bowstringing results, precluding successful nonsurgical management. The proper treatment includes release of the sheath scar and pulley reconstruction. Temporary PIP joint pinning also may be required.
This patient already has participated in a prolonged course of hand therapy with worsening and a fixed PIP contracture, so continued therapy is not recommended. Response 2 is incorrect because the flexor tendons are functioning well with reasonable active DIP motion. Similarly, Response 3 is incorrect because there are no findings consistent with flexor tendon adhesions.
RECOMMENDED READINGS
62. Bollen SR. Soft tissue injury in extreme rock climbers. Br J Sports Med. 1988 Dec;22(4):145-7. PubMed PMID: 3228682.
63. Bowers WH, Kuzma GR, Bynum DK. Closed traumatic rupture of finger flexor pulleys. J Hand Surg Am. 1994 Sep;19(5):782-7. PubMed PMID: 7806800.
This patient already has participated in a prolonged course of hand therapy with worsening and a fixed PIP contracture, so continued therapy is not recommended. Response 2 is incorrect because the flexor tendons are functioning well with reasonable active DIP motion. Similarly, Response 3 is incorrect because there are no findings consistent with flexor tendon adhesions.
RECOMMENDED READINGS
62. Bollen SR. Soft tissue injury in extreme rock climbers. Br J Sports Med. 1988 Dec;22(4):145-7. PubMed PMID: 3228682.
63. Bowers WH, Kuzma GR, Bynum DK. Closed traumatic rupture of finger flexor pulleys. J Hand Surg Am. 1994 Sep;19(5):782-7. PubMed PMID: 7806800.
QUESTION 75
of 100
A 20-year-old right-hand-dominant man has experienced left palm pain for several weeks. He says the pain began after swinging his bat during a game. He can no longer swing his bat without experiencing pain that is located about the proximal volar ulnar palm. Standard hand and wrist radiograph findings are negative. Which study is most appropriate to diagnose this patient’s condition?
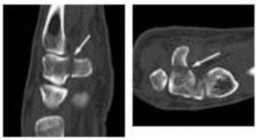
A 20-year-old right-hand-dominant man has experienced left palm pain for several weeks. He says the pain began after swinging his bat during a game. He can no longer swing his bat without experiencing pain that is located about the proximal volar ulnar palm. Standard hand and wrist radiograph findings are negative. Which study is most appropriate to diagnose this patient’s condition?
1
Bone scan
2
Ultrasound
3
CT scan
4
Carpal tunnel radiograph view
This patient has a hamate hook fracture as shown in Figures 81a and 81b. Physicians should have a high index of suspicion when evaluating this patient’s history and examination findings. This fracture is commonly seen in people who participate in racquet sports, baseball, and golf. It may develop following repetitive swinging or occur as the result of an acute swinging injury. Patients
will describe pain while swinging or an inability to swing. An examination shows specific tenderness at the volar ulnar palm directly over the hamate hook. Standard radiograph findings often are negative, even with special views such as the carpal tunnel view. Because of the complex local anatomy and superposition of other carpal bones and local pain, these fractures often are missed on standard radiographs. MR imaging shows local bone edema and is excellent for diagnosis of this particular fracture but is somewhat limited in detection of cortical interruption. Bone scans show a focal hot spot but are nonspecific for definition of this particular fracture. Although ultrasound can detect radiographically occult hamate hook fractures, Celi and associates recommend CT scan to confirm the diagnosis. CT scan has a specificity of 98% and a sensitivity of 100%. The majority of surgeons recommend hamate hook excision in this situation, although some authors recommend open reduction and internal fixation.
RECOMMENDED READINGS
64. Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008 Jan;190(1):10-6. PubMed PMID: 18094287.
65. Celi J, de Gautard G, Della Santa JD, Bianchi S. Sonographic diagnosis of a radiographically undiagnosed hook of the hamate fracture. J Ultrasound Med. 2008 Aug;27(8):1235-9. PubMed PMID: 18645083.
66. Bachoura A, Wroblewski A, Jacoby SM, Osterman AL, Culp RW. Hook of hamate fractures in competitive baseball players. Hand (N Y). 2013 Sep;8(3):302-7. doi: 10.1007/s11552-013-9527-4. PubMed PMID: 24426938.
67. Bishop AT, Beckenbaugh RD. Fracture of the hamate hook. J Hand Surg Am. 1988 Jan;13(1):135-9. PubMed PMID: 3351218.
will describe pain while swinging or an inability to swing. An examination shows specific tenderness at the volar ulnar palm directly over the hamate hook. Standard radiograph findings often are negative, even with special views such as the carpal tunnel view. Because of the complex local anatomy and superposition of other carpal bones and local pain, these fractures often are missed on standard radiographs. MR imaging shows local bone edema and is excellent for diagnosis of this particular fracture but is somewhat limited in detection of cortical interruption. Bone scans show a focal hot spot but are nonspecific for definition of this particular fracture. Although ultrasound can detect radiographically occult hamate hook fractures, Celi and associates recommend CT scan to confirm the diagnosis. CT scan has a specificity of 98% and a sensitivity of 100%. The majority of surgeons recommend hamate hook excision in this situation, although some authors recommend open reduction and internal fixation.
RECOMMENDED READINGS
64. Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008 Jan;190(1):10-6. PubMed PMID: 18094287.
65. Celi J, de Gautard G, Della Santa JD, Bianchi S. Sonographic diagnosis of a radiographically undiagnosed hook of the hamate fracture. J Ultrasound Med. 2008 Aug;27(8):1235-9. PubMed PMID: 18645083.
66. Bachoura A, Wroblewski A, Jacoby SM, Osterman AL, Culp RW. Hook of hamate fractures in competitive baseball players. Hand (N Y). 2013 Sep;8(3):302-7. doi: 10.1007/s11552-013-9527-4. PubMed PMID: 24426938.
67. Bishop AT, Beckenbaugh RD. Fracture of the hamate hook. J Hand Surg Am. 1988 Jan;13(1):135-9. PubMed PMID: 3351218.
QUESTION 76
of 100
Figures 82a and 82b are the clinical photographs of a 16-year-old boy who has a 2-day history of pain, swelling, nausea, and erythema in his entire left upper extremity. His temperature is 38.8°C and his white blood cell count is 25,000/µL (reference range, 4,500-11,000µl). What is the most appropriate course of treatment?
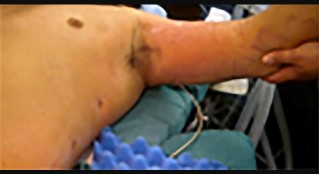

Figures 82a and 82b are the clinical photographs of a 16-year-old boy who has a 2-day history of pain, swelling, nausea, and erythema in his entire left upper extremity. His temperature is 38.8°C and his white blood cell count is 25,000/µL (reference range, 4,500-11,000µl). What is the most appropriate course of treatment?
1
Oral antibiotics
2
Intravenous (IV) antibiotics
3
MR imaging
4
Immediate surgery


This patient has all the signs of necrotizing fasciitis. Advancing erythema, fever, pain, and elevated white blood cell counts are all indications of a serious soft-tissue infection that necessitates immediate surgical debridement. IV antibiotics alone will not resolve this infection.
Although necrotizing soft-tissue infections are uncommon and often are seen in patients who are immunocompromised, they also can occur in healthy individuals and may be associated with only minor trauma. Swelling, erythema, pain, fever, and blistering are classic symptoms. Laboratory and radiograph studies including MR imaging should help confirm the diagnosis but should not delay surgery.
Wide surgical excision of the fascia subcutaneous tissue and skin, if needed, should be performed (Figures 82c and 82d). Debridement should extend to normal tissue. Wound debridement and inspection should be done on a daily basis. Associated mortality is high and survival is dependent upon early diagnosis and surgical debridement.
RECOMMENDED READINGS
68. Stevens DL. The flesh-eating bacterium: what's next? J Infect Dis. 1999 Mar;179 Suppl 2:S366-74. Review. PubMed PMID: 10081509.
69. Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987 Nov;206(5):661-5. PubMed PMID: 3314752.
70. Ogilvie CM, Miclau T. Necrotizing soft tissue infections of the extremities and back. Clin Orthop Relat Res. 2006 Jun;447:179-86. PubMed PMID: 16672902.
71. Chauhan A, Wigton MD, Palmer BA. Necrotizing fasciitis. J Hand Surg Am. 2014 Aug;39(8):1598-601; quiz 1602. doi: 10.1016/j.jhsa.2014.04.010. Epub 2014 May 23. Review. PubMed PMID:
Although necrotizing soft-tissue infections are uncommon and often are seen in patients who are immunocompromised, they also can occur in healthy individuals and may be associated with only minor trauma. Swelling, erythema, pain, fever, and blistering are classic symptoms. Laboratory and radiograph studies including MR imaging should help confirm the diagnosis but should not delay surgery.
Wide surgical excision of the fascia subcutaneous tissue and skin, if needed, should be performed (Figures 82c and 82d). Debridement should extend to normal tissue. Wound debridement and inspection should be done on a daily basis. Associated mortality is high and survival is dependent upon early diagnosis and surgical debridement.
RECOMMENDED READINGS
68. Stevens DL. The flesh-eating bacterium: what's next? J Infect Dis. 1999 Mar;179 Suppl 2:S366-74. Review. PubMed PMID: 10081509.
69. Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987 Nov;206(5):661-5. PubMed PMID: 3314752.
70. Ogilvie CM, Miclau T. Necrotizing soft tissue infections of the extremities and back. Clin Orthop Relat Res. 2006 Jun;447:179-86. PubMed PMID: 16672902.
71. Chauhan A, Wigton MD, Palmer BA. Necrotizing fasciitis. J Hand Surg Am. 2014 Aug;39(8):1598-601; quiz 1602. doi: 10.1016/j.jhsa.2014.04.010. Epub 2014 May 23. Review. PubMed PMID:
QUESTION 77
Question 83 of 100
A close-range gunshot injury necessitates partial amputation of a patient’s right index finger at the metacarpophalangeal (MCP) joint. Intraoperative exploration reveals an intact ulnar digital artery and ulnar skin bridge. What is the most appropriate treatment?
A close-range gunshot injury necessitates partial amputation of a patient’s right index finger at the metacarpophalangeal (MCP) joint. Intraoperative exploration reveals an intact ulnar digital artery and ulnar skin bridge. What is the most appropriate treatment?
1
Replantation of the index finger
2
Ray resection
3
MCP joint fusion
4
Middle finger transposition to the index metacarpal
Replantation following a blast injury is problematic. Stiffness after replantation is common and impedes hand function. Ray resection leads to the loss of the index finger but will allow the earliest unrestricted use of the hand. MCP joint fusion would necessitate either shortening or bone grafting, internal fixation, and soft-tissue reconstruction, resulting in a stiff insensate index finger. Although middle finger transposition to the index metacarpal is possible, the gap left behind between the new index and the ring finger is unsightly and functionally problematic because patients can drop or lose small objects through the gap. Typically, the index ray is transferred to the middle finger position for reconstruction of the middle finger.
RECOMMENDED READINGS
72. Gupta A, Wolff TW. Management of the Mangled Hand and Forearm. J Am Acad Orthop Surg. 1995 Jul;3(4):226-236. PubMed PMID: 10795029.
73. Hanel DP, Lederman ES. Index transposition after resection of the long finger ray. J Hand Surg Am. 1993 Mar;18(2):271-7. PubMed PMID: 8463593.
74. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
RECOMMENDED READINGS
72. Gupta A, Wolff TW. Management of the Mangled Hand and Forearm. J Am Acad Orthop Surg. 1995 Jul;3(4):226-236. PubMed PMID: 10795029.
73. Hanel DP, Lederman ES. Index transposition after resection of the long finger ray. J Hand Surg Am. 1993 Mar;18(2):271-7. PubMed PMID: 8463593.
74. Blazar PE, Garon MT. Ray Resections of the Fingers: Indications, Techniques, and Outcomes. J Am Acad Orthop Surg. 2015 Aug;23(8):476-84. doi: 10.5435/JAAOS-D-14-00056. Review. PubMed PMID: 26209144.
QUESTION 78
of 100
A 75-year-old woman has persistent pain at the metacarpophalangeal (MCP) joint of her right thumb attributable to degenerative arthritis. Bracing and corticosteroid injections have provided only temporary relief. What is the best surgical option?
A 75-year-old woman has persistent pain at the metacarpophalangeal (MCP) joint of her right thumb attributable to degenerative arthritis. Bracing and corticosteroid injections have provided only temporary relief. What is the best surgical option?
1
Silicone arthroplasty
2
Surface replacement arthroplasty
3
Arthrodesis in 15 to 20 degrees of flexion and slight pronation
4
Arthrodesis in 45 to 50 degrees of flexion and slight supination
Symptomatic thumb MCP arthritis is best managed with arthrodesis. The majority of thumb motion occurs at the carpometacarpal and interphalangeal joints, and, as such, arthrodesis of the thumb MCP is well tolerated. The ideal position for arthrodesis of the MCP joint is in slight flexion and pronation, which optimizes key pinch. A study by Saldana and associates recommended 20 degrees of flexion for women and 25 degrees for men. Arthroplasty for thumb MCP problems does not offer enough stability against pinch forces and is not performed.
RECOMMENDED READINGS
75. Rizzo M. Metacarpophalangeal joint arthritis. J Hand Surg Am. 2011 Feb;36(2):345-53. doi: 10.1016/j.jhsa.2010.11.035. Review. PubMed PMID: 21276901.
76. Saldana MJ, Clark EN, Aulicino PL. The optimal position for arthrodesis of the metacarpophalangeal joint of the thumb: a clinical study. J Hand Surg Br. 1987 Jun;12(2):256-9. PubMed PMID: 3624991.
RECOMMENDED READINGS
75. Rizzo M. Metacarpophalangeal joint arthritis. J Hand Surg Am. 2011 Feb;36(2):345-53. doi: 10.1016/j.jhsa.2010.11.035. Review. PubMed PMID: 21276901.
76. Saldana MJ, Clark EN, Aulicino PL. The optimal position for arthrodesis of the metacarpophalangeal joint of the thumb: a clinical study. J Hand Surg Br. 1987 Jun;12(2):256-9. PubMed PMID: 3624991.
QUESTION 79
of 100
Figure 85 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step?
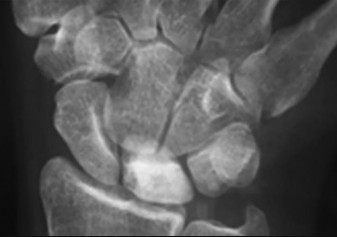
Figure 85 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step?
1
Observation
2
Vascularized bone grafting to the lunate
3
Core decompression of the radius and ulna
4
Immobilization
Lunate or perilunate dislocations are usually treated with open reduction and internal fixation through a dorsal or combined dorsal and volar approach. A high index of suspicion is necessary when treating patients who sustain multiple trauma because as many as 25% of lunate or perilunate dislocations are missed initially.
The radio dense appearance of the lunate seen in Figure 85 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease.
Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect long-term outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect hand function.
RECOMMENDED READINGS
77. Stanbury SJ, Elfar JC. Perilunate dislocation and perilunate fracture-dislocation. J Am Acad Orthop Surg. 2011 Sep;19(9):554-62. Review. PubMed PMID: 21885701.
78. White RE Jr, Omer GE Jr. Transient vascular compromise of the lunate after fracture-dislocation or dislocation of the carpus. J Hand Surg Am. 1984 Mar;9(2):181-4. PubMed PMID: 6715820.
79. Vitale MA, Seetharaman M, Ruchelsman DE. Perilunate dislocations. J Hand Surg Am. 2015 Feb;40(2):358-62; quiz 362. doi: 10.1016/j.jhsa.2014.10.006. Epub 2014 Nov 15. PubMed PMID: 25459380.
80. Forli A, Courvoisier A, Wimsey S, Corcella D, Moutet F. Perilunate dislocations and transscaphoid perilunate fracture-dislocations: a retrospective study with minimum ten-year follow-up. J Hand Surg Am. 2010 Jan;35(1):62-8. doi: 10.1016/j.jhsa.2009.09.003. Epub 2009 Nov 22.
The radio dense appearance of the lunate seen in Figure 85 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease.
Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect long-term outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect hand function.
RECOMMENDED READINGS
77. Stanbury SJ, Elfar JC. Perilunate dislocation and perilunate fracture-dislocation. J Am Acad Orthop Surg. 2011 Sep;19(9):554-62. Review. PubMed PMID: 21885701.
78. White RE Jr, Omer GE Jr. Transient vascular compromise of the lunate after fracture-dislocation or dislocation of the carpus. J Hand Surg Am. 1984 Mar;9(2):181-4. PubMed PMID: 6715820.
79. Vitale MA, Seetharaman M, Ruchelsman DE. Perilunate dislocations. J Hand Surg Am. 2015 Feb;40(2):358-62; quiz 362. doi: 10.1016/j.jhsa.2014.10.006. Epub 2014 Nov 15. PubMed PMID: 25459380.
80. Forli A, Courvoisier A, Wimsey S, Corcella D, Moutet F. Perilunate dislocations and transscaphoid perilunate fracture-dislocations: a retrospective study with minimum ten-year follow-up. J Hand Surg Am. 2010 Jan;35(1):62-8. doi: 10.1016/j.jhsa.2009.09.003. Epub 2009 Nov 22.
QUESTION 80
of 100
A patient with a displaced and comminuted fracture of the radial head and neck also has pain and swelling about the ipsilateral distal radioulnar joint. Which treatment option may exacerbate the wrist disorder?
A patient with a displaced and comminuted fracture of the radial head and neck also has pain and swelling about the ipsilateral distal radioulnar joint. Which treatment option may exacerbate the wrist disorder?
1
Cross-pinning of the radius and ulna
2
Open reduction and internal fixation (ORIF) of the radial head and neck fracture
3
Metallic radial head implant arthroplasty
4
Radial head excision
This scenario describes a forearm-axial instability pattern, which must be recognized before pursuing treatment. Fracture or dislocation of the lateral elbow compartment (radial head/capitellum) associated with ipsilateral distal radioulnar joint derangement is a form of radioulnar dissociation commonly known as Essex-Lopresti fracture dislocation. Radial head excision sets off a chain of events, and delayed diagnosis can result in considerable morbidity following these injuries. Excision of the radial head allows proximal migration of the radius, causing potential problems at both the elbow and wrist. After such proximal migration has occurred, there is no reliable method of forearm reconstruction.
There are a number of treatments for this condition. Salvage of the radial head by open reduction and internal fixation is preferable if possible. However, in cases of marked comminution, radial metallic head implant arthroplasty is an acceptable substitute. The need for soft-tissue repair or pin stabilization of the distal radioulnar joint has not been defined, although some form of forearm immobilization is necessary to allow healing of the injured interosseous membrane.
RECOMMENDED READINGS
81. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-ulnar dissociation. A review of twenty cases. J Bone Joint Surg Am. 1992 Dec;74(10):1486-97. PubMed PMID: 1469008.
82. Edwards GS Jr, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res. 1988 Sep;(234):61-9. PubMed PMID: 3409602.
There are a number of treatments for this condition. Salvage of the radial head by open reduction and internal fixation is preferable if possible. However, in cases of marked comminution, radial metallic head implant arthroplasty is an acceptable substitute. The need for soft-tissue repair or pin stabilization of the distal radioulnar joint has not been defined, although some form of forearm immobilization is necessary to allow healing of the injured interosseous membrane.
RECOMMENDED READINGS
81. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-ulnar dissociation. A review of twenty cases. J Bone Joint Surg Am. 1992 Dec;74(10):1486-97. PubMed PMID: 1469008.
82. Edwards GS Jr, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res. 1988 Sep;(234):61-9. PubMed PMID: 3409602.
QUESTION 81
of 100
Figure 87 is the clinical photograph of a woman who plans to have carpal tunnel release surgery on her right upper extremity. The literature indicates that elevated risk for late-onset lymphedema after elective hand surgery is associated with

Figure 87 is the clinical photograph of a woman who plans to have carpal tunnel release surgery on her right upper extremity. The literature indicates that elevated risk for late-onset lymphedema after elective hand surgery is associated with
1
prior radiation therapy and axillary node dissection.
2
a long interval between breast cancer treatment and hand surgery.
3
a forearm tourniquet.
4
an upper arm tourniquet.
A 2015 study by Baltzer and associates assessed risk for developing late-onset upper extremity lymphedema after elective hand surgery among women previously treated for same-sided breast cancer who did not have presurgical lymphedema. The study concluded that lymphedema is uncommon and self-limited following elective hand surgery among breast cancer survivors. This study also showed that use of a tourniquet appears to be safe for elective hand surgery for this population. Also, a combination of radiation therapy and axillary node surgery and a shorter
interval between hand surgery and breast cancer treatment appears to put these women at higher risk for late-onset lymphedema after elective hand surgery.
RECOMMENDED READINGS
83. [Baltzer,HL, et al. Late Onset Upper Extremity Lymphedema Following Elective Hand Surgery in Breast Cancer Survivors. J Hand Surg Am. 2015 Sep: (40):9.Supplement,pg e4. DOI: ](http://dx.doi.org/10.1016/j.jhsa.2015.06.014)http://dx.doi.org/10.1016/j.jhsa.2015.06.014 (accessed on 06/06/2016).
84. Habbu R, Adams JE. Role of elective hand surgery and tourniquet use in patients with prior breast cancer treatment. J Hand Surg Am. 2011 Sep;36(9):1537-9; quiz 1540. doi: 10.1016/j.jhsa.2011.06.020. Epub 2011 Aug 6. Review. PubMed PMID: 21820817.
interval between hand surgery and breast cancer treatment appears to put these women at higher risk for late-onset lymphedema after elective hand surgery.
RECOMMENDED READINGS
83. [Baltzer,HL, et al. Late Onset Upper Extremity Lymphedema Following Elective Hand Surgery in Breast Cancer Survivors. J Hand Surg Am. 2015 Sep: (40):9.Supplement,pg e4. DOI: ](http://dx.doi.org/10.1016/j.jhsa.2015.06.014)http://dx.doi.org/10.1016/j.jhsa.2015.06.014 (accessed on 06/06/2016).
84. Habbu R, Adams JE. Role of elective hand surgery and tourniquet use in patients with prior breast cancer treatment. J Hand Surg Am. 2011 Sep;36(9):1537-9; quiz 1540. doi: 10.1016/j.jhsa.2011.06.020. Epub 2011 Aug 6. Review. PubMed PMID: 21820817.
QUESTION 82
of 100
Figures 88a through 88d are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is




Figures 88a through 88d are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
1
capitate excision with interposition arthroplasty.
2
capitate proximal pole excision and drilling.
3
proximal row carpectomy (PRC).
4
vascularized bone graft.
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of
osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
RECOMMENDED READINGS
85. Hattori Y, Doi K, Sakamoto S, Yukata K, Shafi M, Akhundov K. Vascularized pedicled bone graft for avascular necrosis of the capitate: case report. J Hand Surg Am. 2009 Sep;34(7):1303-7. doi: 10.1016/j.jhsa.2009.04.012. Epub 2009 Jun 4. PubMed PMID: 19497683.
86. Lapinsky AS, Mack GR. Avascular necrosis of the capitate: a case report. J Hand Surg Am. 1992 Nov;17(6):1090-2. Review. PubMed PMID: 1430946.
87. Peters SJ, Degreef I, De Smet L. Avascular necrosis of the capitate: report of six cases and review of the literature. J Hand Surg Eur Vol. 2015 Jun;40(5):520-5. doi: 10.1177/1753193414524876. Epub 2014 Feb 25. Review. PubMed PMID: 24570346.
RESPONSES FOR QUESTIONS 89 THROUGH 94
1. Low median nerve palsy
2. Posterior interosseous nerve (PIN) palsy
3. Anterior interosseous nerve (AIN) palsy
4. Radial tunnel syndrome
5. Cubital tunnel syndrome
6. Carpal tunnel syndrome
7. Ulnar tunnel syndrome
8. Wartenberg syndrome
9. Thoracic outlet syndrome
osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
RECOMMENDED READINGS
85. Hattori Y, Doi K, Sakamoto S, Yukata K, Shafi M, Akhundov K. Vascularized pedicled bone graft for avascular necrosis of the capitate: case report. J Hand Surg Am. 2009 Sep;34(7):1303-7. doi: 10.1016/j.jhsa.2009.04.012. Epub 2009 Jun 4. PubMed PMID: 19497683.
86. Lapinsky AS, Mack GR. Avascular necrosis of the capitate: a case report. J Hand Surg Am. 1992 Nov;17(6):1090-2. Review. PubMed PMID: 1430946.
87. Peters SJ, Degreef I, De Smet L. Avascular necrosis of the capitate: report of six cases and review of the literature. J Hand Surg Eur Vol. 2015 Jun;40(5):520-5. doi: 10.1177/1753193414524876. Epub 2014 Feb 25. Review. PubMed PMID: 24570346.
RESPONSES FOR QUESTIONS 89 THROUGH 94
1. Low median nerve palsy
2. Posterior interosseous nerve (PIN) palsy
3. Anterior interosseous nerve (AIN) palsy
4. Radial tunnel syndrome
5. Cubital tunnel syndrome
6. Carpal tunnel syndrome
7. Ulnar tunnel syndrome
8. Wartenberg syndrome
9. Thoracic outlet syndrome
QUESTION 83
of 100
Figure 89



Figure 89
1
Low median nerve palsy
2
Posterior interosseous nerve (PIN) palsy
3
Anterior interosseous nerve (AIN) palsy
4
Radial tunnel syndrome
5
Cubital tunnel syndrome
- Cubital tunnel syndrome_
QUESTION 84
of 100
Figure 90
Figure 90
1
Low median nerve palsy
2
Posterior interosseous nerve (PIN) palsy
3
Anterior interosseous nerve (AIN) palsy
4
Radial tunnel syndrome
5
Cubital tunnel syndrome
- Anterior interosseous nerve (AIN) palsy**
QUESTION 85
of 100
Which condition results in weak wrist extension in radial deviation?
Which condition results in weak wrist extension in radial deviation?
1
Low median nerve palsy
2
Posterior interosseous nerve (PIN) palsy
3
Anterior interosseous nerve (AIN) palsy
4
Radial tunnel syndrome
5
Cubital tunnel syndrome
- Posterior interosseous nerve (PIN) palsy**
QUESTION 86
of 100
Figure 92
Figure 92
1
Low median nerve palsy
2
Posterior interosseous nerve (PIN) palsy
3
Anterior interosseous nerve (AIN) palsy
4
Radial tunnel syndrome
5
Cubital tunnel syndrome
- Ulnar tunnel syndrome**
QUESTION 87
of 100
In which condition is the primary finding weakness in opposition (abductor pollicis brevis)?
In which condition is the primary finding weakness in opposition (abductor pollicis brevis)?
1
Low median nerve palsy
2
Posterior interosseous nerve (PIN) palsy
3
Anterior interosseous nerve (AIN) palsy
4
Radial tunnel syndrome
5
Cubital tunnel syndrome
- Low median nerve palsy_
QUESTION 88
of 100
A ganglion cyst is the most common etiology in which condition?
A ganglion cyst is the most common etiology in which condition?
1
Low median nerve palsy
2
Posterior interosseous nerve (PIN) palsy
3
Anterior interosseous nerve (AIN) palsy
4
Radial tunnel syndrome
5
Cubital tunnel syndrome
Cubital tunnel syndrome is the second-most-common compression neuropathy (after carpal tunnel syndrome). Advanced ulnar neuropathy is characterized by numerous eponymous signs and by motor atrophy (eg, fist dorsal interosseous, adductor pollicis). The first sign to appear is the Wartenberg sign (Figure 89), which involves the small finger resting in an abducted position because of unopposed pull of the extensor digiti minimi (because interossei are weak from ulnar neuropathy). Froment’s sign (Figure 92) is also seen in advanced ulnar neuropathy secondary to weakness of the adductor pollicis and first dorsal interosseous and compensation by the flexor pollicis longus (FPL) (median innervated) and extensor pollicis longus (radial innervated).
The AIN provides motor to the FPL, flexor digitorum profundus (FDP) to the index and middle fingers, and to the pronator quadratus. AIN palsy is a motor deficit that can affect all or part of those muscles. Figure 90 shows a “flattened” OK sign that is seen in AIN palsy attributable to weakness of the FPL and FDP to the index finger.
PIN palsy is also a pure motor syndrome. It affects the finger and thumb extensors and the extensor carpi ulnaris (ECU) and extensor carpi radialis brevis (ECRB). The extensor carpi radialis longus (ECRL) is innervated by the radial nerve, so, in PIN palsy, the patient will have a weak wrist extension (because there is no ECU and ECRB involvement) in slight radial deviation (because only the ECRL is firing).
Low median nerve palsy is a deficit of the median nerve at the wrist/carpal tunnel. As such, the primary motor deficit is of the thenar muscles and, clinically, this results in weakness in opposition attributable to abductor pollicis brevis weakness. This is often treated with an opposition transfer (tendon transfer).
Ulnar tunnel syndrome is compression of the ulnar nerve at the wrist. It is less common than cubital tunnel syndrome. The most common etiology is a ganglion cyst, and MRI is helpful when assessing for this condition. Other etiologies include hypothenar hammer syndrome, hook-of-the-hamate fractures, and anomalous muscles.
RECOMMENDED READINGS
1. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part II: median nerve. J Hand Surg Am. 2009 Dec;34(10):1915-20. doi: 10.1016/j.jhsa.2009.10.017. PubMed PMID: 19969200.
2. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part I: radial nerve. J Hand Surg Am. 2009 Dec;34(10):1906-14. doi: 10.1016/j.jhsa.2009.10.016. PubMed PMID: 19969199.
3. Chen SH, Tsai TM. Ulnar tunnel syndrome. J Hand Surg Am. 2014 Mar;39(3):571-9. doi: 10.1016/j.jhsa.2013.08.102. Review. PubMed PMID: 24559635.
4. Draeger RW, Stern PJ. The inverted pyramid sign and other eponymous signs of ulnar nerve palsy. J Hand Surg Am. 2014 Dec;39(12):2517-20; quiz 2521. doi: 10.1016/j.jhsa.2014.07.048. Epub 2014 Sep
16/. PubMed PMID: 25239048.
The AIN provides motor to the FPL, flexor digitorum profundus (FDP) to the index and middle fingers, and to the pronator quadratus. AIN palsy is a motor deficit that can affect all or part of those muscles. Figure 90 shows a “flattened” OK sign that is seen in AIN palsy attributable to weakness of the FPL and FDP to the index finger.
PIN palsy is also a pure motor syndrome. It affects the finger and thumb extensors and the extensor carpi ulnaris (ECU) and extensor carpi radialis brevis (ECRB). The extensor carpi radialis longus (ECRL) is innervated by the radial nerve, so, in PIN palsy, the patient will have a weak wrist extension (because there is no ECU and ECRB involvement) in slight radial deviation (because only the ECRL is firing).
Low median nerve palsy is a deficit of the median nerve at the wrist/carpal tunnel. As such, the primary motor deficit is of the thenar muscles and, clinically, this results in weakness in opposition attributable to abductor pollicis brevis weakness. This is often treated with an opposition transfer (tendon transfer).
Ulnar tunnel syndrome is compression of the ulnar nerve at the wrist. It is less common than cubital tunnel syndrome. The most common etiology is a ganglion cyst, and MRI is helpful when assessing for this condition. Other etiologies include hypothenar hammer syndrome, hook-of-the-hamate fractures, and anomalous muscles.
RECOMMENDED READINGS
1. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part II: median nerve. J Hand Surg Am. 2009 Dec;34(10):1915-20. doi: 10.1016/j.jhsa.2009.10.017. PubMed PMID: 19969200.
2. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part I: radial nerve. J Hand Surg Am. 2009 Dec;34(10):1906-14. doi: 10.1016/j.jhsa.2009.10.016. PubMed PMID: 19969199.
3. Chen SH, Tsai TM. Ulnar tunnel syndrome. J Hand Surg Am. 2014 Mar;39(3):571-9. doi: 10.1016/j.jhsa.2013.08.102. Review. PubMed PMID: 24559635.
4. Draeger RW, Stern PJ. The inverted pyramid sign and other eponymous signs of ulnar nerve palsy. J Hand Surg Am. 2014 Dec;39(12):2517-20; quiz 2521. doi: 10.1016/j.jhsa.2014.07.048. Epub 2014 Sep
16/. PubMed PMID: 25239048.
QUESTION 89
of 100
A 55-year-old patient has ongoing right-hand pain despite having 4 months of treatment that included splinting, activity modification, and nonsteroidal anti-inflammatory drugs. She reports loss of dexterity and worsening hand writing during the last year. She has cramping of her affected hand, particularly in the first web space. Her symptoms are often worse at night. She has difficulty adducting her small finger and notes decreased sensation on the dorsum of her hand, particularly ulnarly. Division of which anatomical structure can most likely alleviate her symptoms?
A 55-year-old patient has ongoing right-hand pain despite having 4 months of treatment that included splinting, activity modification, and nonsteroidal anti-inflammatory drugs. She reports loss of dexterity and worsening hand writing during the last year. She has cramping of her affected hand, particularly in the first web space. Her symptoms are often worse at night. She has difficulty adducting her small finger and notes decreased sensation on the dorsum of her hand, particularly ulnarly. Division of which anatomical structure can most likely alleviate her symptoms?
1
Transverse carpal ligament
2
Lacertus fibrosus
3
Osborne ligament
4
Volar carpal ligament at Guyon’s canal
Cubital tunnel syndrome is the second-most-common compressive peripheral neuropathy after carpal tunnel syndrome. The diagnosis is typically established through a combination of a supportive history, positive clinical signs, and electrodiagnostic studies. Patients often experience hand paresthesias and/or numbness and hand pain (and less commonly medial elbow pain). Numbness usually affects the small finger, the ulnar aspect of the ring finger, and the dorsum of the hand (via the dorsal cutaneous branch of the ulnar nerve). When symptoms affect motor function, patients will have weakness of the hand intrinsics muscles and may exhibit atrophy. The Wartenberg sign is the observation of an abducted posture of the small finger in an affected hand attributable to an imbalance caused by an intact extensor digiti minimi and functional impairment of the affected third volar interosseous muscle attributable to atrophy and weakness. There are many surgical options for cubital tunnel syndrome, but all share division of the Osborne ligament because the nerve passes anterior to the olecranon and posterior to the medial epicondyle at the elbow.
Division of the transverse carpal ligament will decompress the median nerve and alleviate symptoms involving the thumb, index, and long fingers. Release of the lacertus fibrosus will not affect symptoms secondary to ulnar nerve compression. Ulnar nerve compression at Guyon’s canal will cause numbness to the small finger and intrinsic muscle weakness but not numbness to the
dorsum of the hand because the dorsal ulnar sensory nerve branches from the ulnar nerve prior to Guyon’s canal.
RECOMMENDED READINGS
5. Palmer BA, Hughes TB. Cubital tunnel syndrome. J Hand Surg Am. 2010 Jan;35(1):153-63. doi: 10.1016/j.jhsa.2009.11.004. Review. PubMed PMID: 20117320.
6. Soltani AM, Best MJ, Francis CS, Allan BJ, Panthaki ZJ. Trends in the surgical treatment of cubital tunnel syndrome: an analysis of the national survey of ambulatory surgery database. J Hand Surg Am. 2013 Aug;38(8):1551-6. doi: 10.1016/j.jhsa.2013.04.044. Epub 2013 Jul 3. PubMed PMID: 23830676.
Division of the transverse carpal ligament will decompress the median nerve and alleviate symptoms involving the thumb, index, and long fingers. Release of the lacertus fibrosus will not affect symptoms secondary to ulnar nerve compression. Ulnar nerve compression at Guyon’s canal will cause numbness to the small finger and intrinsic muscle weakness but not numbness to the
dorsum of the hand because the dorsal ulnar sensory nerve branches from the ulnar nerve prior to Guyon’s canal.
RECOMMENDED READINGS
5. Palmer BA, Hughes TB. Cubital tunnel syndrome. J Hand Surg Am. 2010 Jan;35(1):153-63. doi: 10.1016/j.jhsa.2009.11.004. Review. PubMed PMID: 20117320.
6. Soltani AM, Best MJ, Francis CS, Allan BJ, Panthaki ZJ. Trends in the surgical treatment of cubital tunnel syndrome: an analysis of the national survey of ambulatory surgery database. J Hand Surg Am. 2013 Aug;38(8):1551-6. doi: 10.1016/j.jhsa.2013.04.044. Epub 2013 Jul 3. PubMed PMID: 23830676.
QUESTION 90
of 100
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is

According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
1
retrograde to protect the dorsal blood supply to the scaphoid.
2
retrograde eccentrically in the dorsal scaphoid to avoid trapezium impingement.
3
deep and centrally placed, respecting the articular surface.
4
anterograde to protect the volar blood supply to the scaphoid.
Figure 96
The position of a scaphoid screw for scaphoid fracture repair (Figure 96) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.
Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an
eccentrically placed screw. Dodds and associates demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws.
The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
RECOMMENDED READINGS
7. Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid. Treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am. 1996 Dec;78(12):1829-37. PubMed PMID: 8986659.
8. McCallister WV, Knight J, Kaliappan R, Trumble TE. Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Joint Surg Am. 2003 Jan;85-A(1):72-7. PubMed PMID: 12533575.
9. Dodds SD, Panjabi MM, Slade JF 3rd. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am. 2006 Mar;31(3):405-13. PubMed PMID: 16516734.
The position of a scaphoid screw for scaphoid fracture repair (Figure 96) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.
Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an
eccentrically placed screw. Dodds and associates demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws.
The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
RECOMMENDED READINGS
7. Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid. Treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am. 1996 Dec;78(12):1829-37. PubMed PMID: 8986659.
8. McCallister WV, Knight J, Kaliappan R, Trumble TE. Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Joint Surg Am. 2003 Jan;85-A(1):72-7. PubMed PMID: 12533575.
9. Dodds SD, Panjabi MM, Slade JF 3rd. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am. 2006 Mar;31(3):405-13. PubMed PMID: 16516734.
QUESTION 91
of 100
A 64-year-old woman with rheumatoid arthritis cannot fully extend her fingers actively at the metacarpophalangeal (MCP) level. Full passive extension is possible, but she cannot actively maintain that extension when her fingers are released. The MCP joints do extend when her wrist is passively flexed. What is the most likely cause of this problem?
A 64-year-old woman with rheumatoid arthritis cannot fully extend her fingers actively at the metacarpophalangeal (MCP) level. Full passive extension is possible, but she cannot actively maintain that extension when her fingers are released. The MCP joints do extend when her wrist is passively flexed. What is the most likely cause of this problem?
1
Extensor tendon ruptures at the wrist
2
Subluxation of the extensor mechanisms at the MCP joint
3
Caput ulnae syndrome
4
Posterior interosseous nerve palsy
Loss of MCP extension is common in the setting of rheumatoid arthritis, but potential causes are varied. An understanding of various etiologies is needed to address the multiple facets of inflammatory arthropathy, for which causes include extensor tendon rupture, MCP joint flexion
contracture/dislocation, subluxation of the extensor tendons at the MCP joint (sagittal band rupture), and posterior interosseous nerve (PIN) palsy. These causes are differentiated during an examination.
Extensor tendon ruptures, as seen with caput ulnae syndrome (Vaughan-Jackson syndrome) allow for passive MCP extension, not active extension or the ability to maintain extension actively, and would not involve finger extension with passive flexion tenodesis of the wrist. Flexion contractures of the MCP joints, as may be seen in dislocations, would not allow active or passive motion.
Subluxation of the extensor tendons at the MCP joints, as seen in attenuation of the sagittal bands, will usually preclude the initiation of active extension, but patients will be able to maintain extension of the MCP joints once they are placed in extension by the examiner. With a PIN palsy, no active extension or active hold is possible, but passive extension and tenodesis with wrist flexion are maintained. Synovitis of the elbow is the most likely cause of the PIN palsy. An extensor tenosynovitis or caput ulnae syndrome would not prohibit MCP extension unless the condition progressed to the point of causing other pathology.
RECOMMENDED READINGS
10. Millender LH, Nalbuff EA, Holdsworth DE. Posterior interosseous nerve syndrome secondary to rheumatoid synovitis. J Bone Joint Surg Am. 1973 Mar; 55(2):375-7. PubMed PMID: 4696167.
11. Steichen JB, Christensen AW. Posterior interosseous nerve compression syndrome. In: Gelberman RH ed. Operative Nerve Repair and Reconstruction. Philadelphia, PA: JB Lippincott; 1991:1151-1157.
contracture/dislocation, subluxation of the extensor tendons at the MCP joint (sagittal band rupture), and posterior interosseous nerve (PIN) palsy. These causes are differentiated during an examination.
Extensor tendon ruptures, as seen with caput ulnae syndrome (Vaughan-Jackson syndrome) allow for passive MCP extension, not active extension or the ability to maintain extension actively, and would not involve finger extension with passive flexion tenodesis of the wrist. Flexion contractures of the MCP joints, as may be seen in dislocations, would not allow active or passive motion.
Subluxation of the extensor tendons at the MCP joints, as seen in attenuation of the sagittal bands, will usually preclude the initiation of active extension, but patients will be able to maintain extension of the MCP joints once they are placed in extension by the examiner. With a PIN palsy, no active extension or active hold is possible, but passive extension and tenodesis with wrist flexion are maintained. Synovitis of the elbow is the most likely cause of the PIN palsy. An extensor tenosynovitis or caput ulnae syndrome would not prohibit MCP extension unless the condition progressed to the point of causing other pathology.
RECOMMENDED READINGS
10. Millender LH, Nalbuff EA, Holdsworth DE. Posterior interosseous nerve syndrome secondary to rheumatoid synovitis. J Bone Joint Surg Am. 1973 Mar; 55(2):375-7. PubMed PMID: 4696167.
11. Steichen JB, Christensen AW. Posterior interosseous nerve compression syndrome. In: Gelberman RH ed. Operative Nerve Repair and Reconstruction. Philadelphia, PA: JB Lippincott; 1991:1151-1157.
QUESTION 92
of 100
A 50-year-old woman has had acute weakness in her dominant hand for 6 weeks. Before noticing the onset of weakness, she experienced several weeks of vague discomfort in her shoulder and forearm, generalized fatigue, and a low-grade fever. There is no history of trauma. An examination reveals weakness of thumb and index finger distal interphalangeal (DIP) joint flexion. Electrodiagnostic testing shows fibrillations and positive sharp waves in the flexor pollicis longus and index flexor digitorum profundus muscles. The next appropriate step is
A 50-year-old woman has had acute weakness in her dominant hand for 6 weeks. Before noticing the onset of weakness, she experienced several weeks of vague discomfort in her shoulder and forearm, generalized fatigue, and a low-grade fever. There is no history of trauma. An examination reveals weakness of thumb and index finger distal interphalangeal (DIP) joint flexion. Electrodiagnostic testing shows fibrillations and positive sharp waves in the flexor pollicis longus and index flexor digitorum profundus muscles. The next appropriate step is
1
observation.
2
corticosteroid injection.
3
immediate surgical decompression.
4
tendon transfers.
This clinical scenario describes anterior interosseous nerve (AIN) syndrome. Identifying factors include weakness of the muscles innervated by the AIN, which include the flexor pollicis longus, index flexor digitorum profundus, and pronator quadratus. The same findings are present when fascicles contributing to the AIN are affected more proximally in the median nerve or brachial plexus, at which the findings are referred to as pseudo-anterior interosseous syndrome.
AIN syndrome can be present following blunt or penetrating trauma. It can also be seen in the absence of trauma, in which case there may be a prodrome of upper extremity discomfort, generalized fatigue, and/or fever. Clinical findings include weakness of the thumb interphalangeal (IP) joint and index DIP joint flexion, sometimes referred to as the “Playboy bunny sign.” Pronator quadratus weakness is also present; however, there is uncertainty as to the validity of manual muscle testing in determining pronator quadratus weakness. Electrodiagnostic studies demonstrate evidence of denervation of the muscles supplied by the AIN.
In the setting of acute trauma exploration, decompression and repair of the AIN is indicated early. In the case of a spontaneous and sudden onset of symptoms, especially when associated with other indications of an inflammatory process, a viral or inflammatory neuritis is much more likely. In these cases, multiple studies demonstrate a high incidence of spontaneous resolution over 6 to 12 months. Although systemic corticosteroids may be of benefit in the case of inflammatory neuritis, there are no data to support their use and no data to support the use of AIN corticosteroid injection. Although surgical exploration is supported in the literature for patients who do not show improvement within 3 months of onset, immediate surgical exploration at 6 weeks is not indicated. Tendon transfers are indicated only if recovery fails to occur spontaneously or after surgical exploration of the AIN.
RECOMMENDED READINGS
12. Miller-Breslow A, Terrono A, Millender LH. Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am. 1990 May;15(3):493-6. PubMed PMID: 2348073.
13. Chi Y, Harness NG. Anterior interosseous nerve syndrome. J Hand Surg Am. 2010 Dec;35(12):2078-
80/. doi: 10.1016/j.jhsa.2010.08.018. Epub 2010 Oct 20. PubMed PMID: 20961706.
14. Sood MK, Burke FD. Anterior interosseous nerve palsy. A review of 16 cases. J Hand Surg Br. 1997 Feb;22(1):64-8. PubMed PMID: 9061529.
AIN syndrome can be present following blunt or penetrating trauma. It can also be seen in the absence of trauma, in which case there may be a prodrome of upper extremity discomfort, generalized fatigue, and/or fever. Clinical findings include weakness of the thumb interphalangeal (IP) joint and index DIP joint flexion, sometimes referred to as the “Playboy bunny sign.” Pronator quadratus weakness is also present; however, there is uncertainty as to the validity of manual muscle testing in determining pronator quadratus weakness. Electrodiagnostic studies demonstrate evidence of denervation of the muscles supplied by the AIN.
In the setting of acute trauma exploration, decompression and repair of the AIN is indicated early. In the case of a spontaneous and sudden onset of symptoms, especially when associated with other indications of an inflammatory process, a viral or inflammatory neuritis is much more likely. In these cases, multiple studies demonstrate a high incidence of spontaneous resolution over 6 to 12 months. Although systemic corticosteroids may be of benefit in the case of inflammatory neuritis, there are no data to support their use and no data to support the use of AIN corticosteroid injection. Although surgical exploration is supported in the literature for patients who do not show improvement within 3 months of onset, immediate surgical exploration at 6 weeks is not indicated. Tendon transfers are indicated only if recovery fails to occur spontaneously or after surgical exploration of the AIN.
RECOMMENDED READINGS
12. Miller-Breslow A, Terrono A, Millender LH. Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am. 1990 May;15(3):493-6. PubMed PMID: 2348073.
13. Chi Y, Harness NG. Anterior interosseous nerve syndrome. J Hand Surg Am. 2010 Dec;35(12):2078-
80/. doi: 10.1016/j.jhsa.2010.08.018. Epub 2010 Oct 20. PubMed PMID: 20961706.
14. Sood MK, Burke FD. Anterior interosseous nerve palsy. A review of 16 cases. J Hand Surg Br. 1997 Feb;22(1):64-8. PubMed PMID: 9061529.
QUESTION 93
of 100
Following an open reduction and internal fixation (Figures 99a and 99b), radiographs shown in Figures 99c and 99d reveal a nonreduced radial head. An attempted closed reduction of the radial head is unsuccessful. What is the best next step?

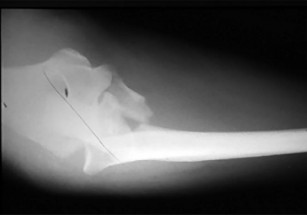





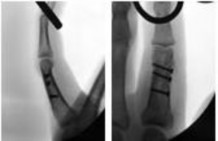
Following an open reduction and internal fixation (Figures 99a and 99b), radiographs shown in Figures 99c and 99d reveal a nonreduced radial head. An attempted closed reduction of the radial head is unsuccessful. What is the best next step?
1
Radial head excision
2
Removal of the plate from the ulna and revision osteosynthesis
3
Closed reduction and pin fixation of the radial head to the capitellum
4
Pin fixation of the radial head and reconstruction of the annular ligament
A comminuted proximal ulnar fracture is often plated in a shortened position, forcing the radial head into a nonanatomical position. Attempted reduction and pin fixation without addressing the length of the ulna often results in failure, even with a ligament reconstruct. Radial head excision is a salvage procedure. A helpful technique for comminuted proximal ulna fractures is to first pin the radial head in a reduced position and then plate the ulnar out to length.
RECOMMENDED READINGS
15. Heim U. [Combined fractures of the radius and the ulna at the elbow level in the adult. Analysis of 120 cases after more than 1 year]. Rev Chir Orthop Reparatrice Appar Mot. 1998 Apr;84(2):142-53. Review. French. PubMed PMID: 9775058.
16. Morrey BF: Surgical exposures of the elbow. In Morrey BF, ed. The Elbow and its Disorders. 2nd ed. Philadelphia, PA: WB Saunders, 1993:139-166.
17. Ring D, Jupiter JB. Reconstruction of posttraumatic elbow instability. Clin Orthop Relat Res. 2000 Jan;(370):44-56. Review. PubMed PMID: 10660701.
18. Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg. 1998 Jul-Aug;6(4):215-24. Review. PubMed PMID: 9682084.
**Question 100 of 100**
Figures 100a through 100c are the clinical photograph and radiographs of a 25-year-old, left-hand-dominant man who injured his left index finger. Which treatment option will most effectively allow satisfactory fracture alignment and maximize motion?
1. Buddy-taping to the long finger with an early range of motion (ROM) program
2. Closed reduction and static external fixation in extension
3. Open reduction and internal fixation (ORIF) with an early ROM program
4. Digital splinting for 4 weeks followed by a ROM program
_PREFERRED RESPONSE: 3- Open reduction and internal fixation (ORIF) with an early ROM program_
**DISCUSSION**
This patient has an oblique index proximal phalanx fracture with malrotation. Buddy-taping and digital splinting would not predictably maintain fracture reduction and would result in a malunion with rotational deformity and possible shortening. Closed reduction and spanning external fixation in extension would result in significant digital stiffness. ORIF (Figures 100d and 100e) followed by an early ROM program would allow anatomic fracture alignment and give this patient the best chance to regain the majority of motion in the shortest amount of time.
RECOMMENDED READINGS
19. [Pun WK, Chow SP, So YC, Luk KD, Ngai WK, Ip FK, Peng WH, Ng C, Crosby C. Unstable phalangeal fractures: treatment by A.O. screw and plate fixation. J Hand Surg Am. 1991 Jan;16(1):113-7. PubMed PMID: 1995665. ](http://www.ncbi.nlm.nih.gov/pubmed/1995665)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1995665)
20. [Kawamura K, Chung KC. Fixation choices for closed simple unstable oblique phalangeal and metacarpal fractures. Hand Clin. 2006 Aug;22(3):287-95. Review. PubMed PMID: 16843795. ](http://www.ncbi.nlm.nih.gov/pubmed/16843795)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16843795)
_This is the last question of the exam._
_GOOD LUCK_
RECOMMENDED READINGS
15. Heim U. [Combined fractures of the radius and the ulna at the elbow level in the adult. Analysis of 120 cases after more than 1 year]. Rev Chir Orthop Reparatrice Appar Mot. 1998 Apr;84(2):142-53. Review. French. PubMed PMID: 9775058.
16. Morrey BF: Surgical exposures of the elbow. In Morrey BF, ed. The Elbow and its Disorders. 2nd ed. Philadelphia, PA: WB Saunders, 1993:139-166.
17. Ring D, Jupiter JB. Reconstruction of posttraumatic elbow instability. Clin Orthop Relat Res. 2000 Jan;(370):44-56. Review. PubMed PMID: 10660701.
18. Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg. 1998 Jul-Aug;6(4):215-24. Review. PubMed PMID: 9682084.
**Question 100 of 100**
Figures 100a through 100c are the clinical photograph and radiographs of a 25-year-old, left-hand-dominant man who injured his left index finger. Which treatment option will most effectively allow satisfactory fracture alignment and maximize motion?
1. Buddy-taping to the long finger with an early range of motion (ROM) program
2. Closed reduction and static external fixation in extension
3. Open reduction and internal fixation (ORIF) with an early ROM program
4. Digital splinting for 4 weeks followed by a ROM program
_PREFERRED RESPONSE: 3- Open reduction and internal fixation (ORIF) with an early ROM program_
**DISCUSSION**
This patient has an oblique index proximal phalanx fracture with malrotation. Buddy-taping and digital splinting would not predictably maintain fracture reduction and would result in a malunion with rotational deformity and possible shortening. Closed reduction and spanning external fixation in extension would result in significant digital stiffness. ORIF (Figures 100d and 100e) followed by an early ROM program would allow anatomic fracture alignment and give this patient the best chance to regain the majority of motion in the shortest amount of time.
RECOMMENDED READINGS
19. [Pun WK, Chow SP, So YC, Luk KD, Ngai WK, Ip FK, Peng WH, Ng C, Crosby C. Unstable phalangeal fractures: treatment by A.O. screw and plate fixation. J Hand Surg Am. 1991 Jan;16(1):113-7. PubMed PMID: 1995665. ](http://www.ncbi.nlm.nih.gov/pubmed/1995665)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1995665)
20. [Kawamura K, Chung KC. Fixation choices for closed simple unstable oblique phalangeal and metacarpal fractures. Hand Clin. 2006 Aug;22(3):287-95. Review. PubMed PMID: 16843795. ](http://www.ncbi.nlm.nih.gov/pubmed/16843795)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16843795)
_This is the last question of the exam._
_GOOD LUCK_
