Score: 0%
ORTHOPEDIC MCQS ONLINE 015Spine
QUESTION 1
of 100
What is the most likely diagnosis?
What is the most likely diagnosis?
1
Degenerative disk disease
2
Disk herniation with spinal stenosis
3
Epidural and paraspinal abscess
4
Muscle strain
- Epidural and paraspinal abscess
QUESTION 2
of 100
Patients initially treated with intravenous (IV) antibiotics are at higher risk for failure of nonsurgical treatment in the setting of
Patients initially treated with intravenous (IV) antibiotics are at higher risk for failure of nonsurgical treatment in the setting of
1
obesity.
2
diabetes.
3
abscess extending over 3 vertebrae.
4
blood culture findings positive for coagulase-negative Staphylococci.
- diabetes.
QUESTION 3
of 100
Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?
Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?
1
Progressive weakness
2
C-reactive protein (CRP) level of 75
3
Increased low-back pain
4
White blood cell (WBC) count of 11
Epidural abscesses are potentially devastating. Nonsurgical care may be chosen for select patients. A baseline failure rate of 8.3% increases based on patient risk factors, which include a history of IV drug abuse, diabetes, age older than 65, CRP level higher than 115, WBC level higher than 12.5, and Staphylococcus aureus as the causative organism. Immunosuppression and abscess size are not significant risk factors for failure of nonsurgical care. Nonsurgical care may be regarded as "failed" if there is worsening of a patient's neurologic status. When nonsurgical care fails, delayed surgery is less successful at restoring motor function (vs early surgery).
RECOMMENDED READINGS
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Duarte RM, Vaccaro AR. Spinal infection: state of the art and management algorithm. Eur Spine J. 2013 Dec;22(12):2787-99. doi: 10.1007/s00586-013-2850-1. Epub 2013 Jun 12.
[Review. PubMed PMID: 23756630. ](http://www.ncbi.nlm.nih.gov/pubmed/23756630)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23756630)
RECOMMENDED READINGS
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Duarte RM, Vaccaro AR. Spinal infection: state of the art and management algorithm. Eur Spine J. 2013 Dec;22(12):2787-99. doi: 10.1007/s00586-013-2850-1. Epub 2013 Jun 12.
[Review. PubMed PMID: 23756630. ](http://www.ncbi.nlm.nih.gov/pubmed/23756630)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23756630)
QUESTION 4
of 100
Which factor is most important when attempting to prevent interbody graft subsidence?
Which factor is most important when attempting to prevent interbody graft subsidence?
1
End plate burring
2
Surface contact area
3
Bone quality
4
Use of rigid fixation
Osteoporosis can affect all aspects of spinal stability and is the most critical factor regarding spinal implant failure. Burring of the end plates may decrease strength of the interface with the uncovering of "softer" cancellous bone. Increasing the surface contact area may help prevent subsidence but is not as important as bone quality. Stress shielding through rigid fixation may lead to construct failure.
RECOMMENDED READINGS
Benzel E (ed): Biomechanics of Spine Stabilization. Rolling Meadows, IL, American Association of Neurological Surgeons, 2001, pp 446-447.
[Goldhahn J, Reinhold M, Stauber M, Knop C, Frei R, Schneider E, Linke B. Improved anchorage in osteoporotic vertebrae with new implant designs. J Orthop Res. 2006 May;24(5):917-25. PubMed PMID: 16583445. ](http://www.ncbi.nlm.nih.gov/pubmed/16583445)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16583445)
RECOMMENDED READINGS
Benzel E (ed): Biomechanics of Spine Stabilization. Rolling Meadows, IL, American Association of Neurological Surgeons, 2001, pp 446-447.
[Goldhahn J, Reinhold M, Stauber M, Knop C, Frei R, Schneider E, Linke B. Improved anchorage in osteoporotic vertebrae with new implant designs. J Orthop Res. 2006 May;24(5):917-25. PubMed PMID: 16583445. ](http://www.ncbi.nlm.nih.gov/pubmed/16583445)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16583445)
QUESTION 5
of 100
Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?
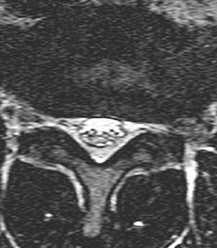
Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?
1
Posterior midline approach
2
Retroperitoneal approach
3
Far lateral approach
4
Transpsoas approach
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
[Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[View](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3175760)
[Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. ](http://www.ncbi.nlm.nih.gov/pubmed/7674015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7674015)
RECOMMENDED READINGS
[Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[View](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3175760)
[Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. ](http://www.ncbi.nlm.nih.gov/pubmed/7674015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7674015)
QUESTION 6
of 100
Which intervention most effectively prevents surgical-site infections following spine surgery?
Which intervention most effectively prevents surgical-site infections following spine surgery?
1
Bathing the day of surgery
2
Intravenous (IV) vancomycin
3
Preincision IV antibiotics
4
Vancomycin powder in wound
The use of IV antibiotics for prophylaxis of surgical-site infection is supported by Level 1 evidence in spine surgery. It has been given a "B" recommendation by the North American Spine Society. The use of specific bathing solutions the day of surgery may be beneficial, but the evidence in spine surgery is lacking. Similarly, evidence for use of vancomycin (either topically or IV) is not supported by high-level studies, although retrospective and basic science studies support topical vancomycin use.
RECOMMENDED READINGS
[Brown MD, Brookfield KF. A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine (Phila Pa 1976). 2004 May 15;29(10):1066-8. PubMed PMID: 15131430. ](http://www.ncbi.nlm.nih.gov/pubmed/15131430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15131430)
Diab M, Smucny M, Dormans JP, Erickson MA, Ibrahim K, Lenke LG, Sucato DJ, Sanders JO. Use and outcomes of wound drain in spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012 May 15;37(11):966-73. doi: 10.1097/BRS.0b013e31823bbf0b.
[PubMed PMID: 22037527. ](http://www.ncbi.nlm.nih.gov/pubmed/22037527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22037527)
[Evaniew N, Khan M, Drew B, Peterson D, Bhandari M, Ghert M. Intrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysis. Eur Spine J. 2014 May 18. [Epub ahead of print] PubMed PMID: 24838506. ](http://www.ncbi.nlm.nih.gov/pubmed/24838506)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24838506) Rubinstein E, Findler G, Amit P, Shaked I. Perioperative prophylactic cephazolin in spinal surgery. A double-blind placebo-controlled trial. J Bone Joint Surg Br. 1994 Jan;76(1):99-
[102/. PubMed PMID: 8300691. ](http://www.ncbi.nlm.nih.gov/pubmed/8300691)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8300691)
[Savage JW, Anderson PA. An update on modifiable factors to reduce the risk of surgical site infections. Spine J. 2013 Sep;13(9):1017-29. doi:10.1016/j.spinee.2013.03.051. Epub 2013 May 24. Review. PubMed PMID: 23711958. ](http://www.ncbi.nlm.nih.gov/pubmed/23711958)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23711958)
[Shaffer WO, Baisden JL, Fernand R, Matz PG; North American Spine Society. An evidence-based clinical guideline for antibiotic prophylaxis in spine surgery. Spine J. 2013 Oct;13(10):1387-92. doi: 10.1016/j.spinee.2013.06.030. Epub 2013 Aug 27. Review. PubMed PMID: 23988461. ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23988461)
RECOMMENDED READINGS
[Brown MD, Brookfield KF. A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine (Phila Pa 1976). 2004 May 15;29(10):1066-8. PubMed PMID: 15131430. ](http://www.ncbi.nlm.nih.gov/pubmed/15131430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15131430)
Diab M, Smucny M, Dormans JP, Erickson MA, Ibrahim K, Lenke LG, Sucato DJ, Sanders JO. Use and outcomes of wound drain in spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012 May 15;37(11):966-73. doi: 10.1097/BRS.0b013e31823bbf0b.
[PubMed PMID: 22037527. ](http://www.ncbi.nlm.nih.gov/pubmed/22037527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22037527)
[Evaniew N, Khan M, Drew B, Peterson D, Bhandari M, Ghert M. Intrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysis. Eur Spine J. 2014 May 18. [Epub ahead of print] PubMed PMID: 24838506. ](http://www.ncbi.nlm.nih.gov/pubmed/24838506)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24838506) Rubinstein E, Findler G, Amit P, Shaked I. Perioperative prophylactic cephazolin in spinal surgery. A double-blind placebo-controlled trial. J Bone Joint Surg Br. 1994 Jan;76(1):99-
[102/. PubMed PMID: 8300691. ](http://www.ncbi.nlm.nih.gov/pubmed/8300691)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8300691)
[Savage JW, Anderson PA. An update on modifiable factors to reduce the risk of surgical site infections. Spine J. 2013 Sep;13(9):1017-29. doi:10.1016/j.spinee.2013.03.051. Epub 2013 May 24. Review. PubMed PMID: 23711958. ](http://www.ncbi.nlm.nih.gov/pubmed/23711958)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23711958)
[Shaffer WO, Baisden JL, Fernand R, Matz PG; North American Spine Society. An evidence-based clinical guideline for antibiotic prophylaxis in spine surgery. Spine J. 2013 Oct;13(10):1387-92. doi: 10.1016/j.spinee.2013.06.030. Epub 2013 Aug 27. Review. PubMed PMID: 23988461. ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23988461)
QUESTION 7
of 100
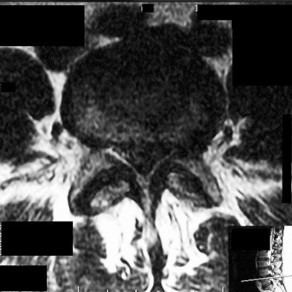
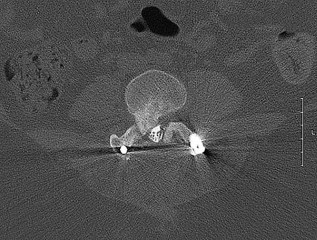
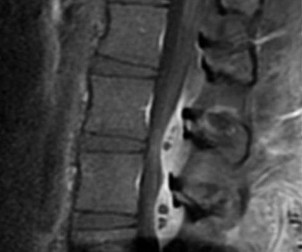
Figures 7a through 7d are the images of a 31-year-old obese woman who has a long history of low-back pain and intermittent bilateral lower extremity pain. Five days ago her symptoms increased markedly and she was given pain medications upon presentation to her primary care physician. Three days ago she noticed that her bed was wet upon awakening; she also had numbness and tingling in her peroneal area and lower extremities and weakness in her lower extremities. She is brought to your office in a wheelchair. Her examination reveals diminished sensation to light touch in the L4 to S4 dermatomes and 0-1/5 strength in all muscle groups in her bilateral lower
extremities with the exception of her hip flexors, hip adductors, and quadriceps, which are 5/5 in strength. She has decreased sphincter tone on rectal examination. You recommend immediate decompressive laminectomy. What is the likelihood she will regain bladder function after surgery?
A
B
C
D



Figures 7a through 7d are the images of a 31-year-old obese woman who has a long history of low-back pain and intermittent bilateral lower extremity pain. Five days ago her symptoms increased markedly and she was given pain medications upon presentation to her primary care physician. Three days ago she noticed that her bed was wet upon awakening; she also had numbness and tingling in her peroneal area and lower extremities and weakness in her lower extremities. She is brought to your office in a wheelchair. Her examination reveals diminished sensation to light touch in the L4 to S4 dermatomes and 0-1/5 strength in all muscle groups in her bilateral lower
extremities with the exception of her hip flexors, hip adductors, and quadriceps, which are 5/5 in strength. She has decreased sphincter tone on rectal examination. You recommend immediate decompressive laminectomy. What is the likelihood she will regain bladder function after surgery?
A
B
C
D
1
0% to 20%
2
21% to 40%
3
41% to 60%
4
61% to 80%
This patient has congenital and acquired spinal stenosis with multilevel disk protrusions that have both chronic (calcified) and acute components, resulting is multilevel cauda equina compression and acute cauda equina syndrome of more than 48 hours duration. Most studies indicate that patients who undergo decompression within 48 hours of symptom onset have a better prognosis for neurologic recovery than those who undergo decompression after 48 hours. Among patients with urinary incontinence, 1 study indicated that 43% remained incontinent at follow-up visits, but this study included a mix of early and late surgical patients. In another series of 44 patients with acute cauda equina syndrome, chronic bowel and bladder dysfunction were issues for 63% of those for whom surgery was delayed for more than 48 hours after symptom onset.
RECOMMENDED READINGS
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
[16/. PubMed PMID: 17224816. ](http://www.ncbi.nlm.nih.gov/pubmed/%2017224816)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2017224816)
[Ahn UM, Ahn NU, Buchowski JM, Garrett ES, Sieber AN, Kostuik JP. Cauda equina syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine (Phila Pa 1976). 2000 Jun 15;25(12):1515-22. PubMed PMID: 10851100. ](http://www.ncbi.nlm.nih.gov/pubmed/%2010851100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010851100) [Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine (Phila Pa 1976). 2000 Feb 1;25(3):348-51; discussion 352. PubMed PMID: 10703108. ](http://www.ncbi.nlm.nih.gov/pubmed/10703108)[View ](http://www.ncbi.nlm.nih.gov/pubmed/10703108)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10703108)
RECOMMENDED READINGS
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
[16/. PubMed PMID: 17224816. ](http://www.ncbi.nlm.nih.gov/pubmed/%2017224816)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2017224816)
[Ahn UM, Ahn NU, Buchowski JM, Garrett ES, Sieber AN, Kostuik JP. Cauda equina syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine (Phila Pa 1976). 2000 Jun 15;25(12):1515-22. PubMed PMID: 10851100. ](http://www.ncbi.nlm.nih.gov/pubmed/%2010851100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010851100) [Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine (Phila Pa 1976). 2000 Feb 1;25(3):348-51; discussion 352. PubMed PMID: 10703108. ](http://www.ncbi.nlm.nih.gov/pubmed/10703108)[View ](http://www.ncbi.nlm.nih.gov/pubmed/10703108)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10703108)
QUESTION 8
of 100
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
1
Apex of the curve is at T3
2
Apex of the curve is at T8
3
Apex of the curve is at L1
4
Apex of the curve is at L2
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
[Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. ](http://www.ncbi.nlm.nih.gov/pubmed/17945126)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17945126)
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
[Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. ](http://www.ncbi.nlm.nih.gov/pubmed/17945126)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17945126)
QUESTION 9
of 100
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)?
A
B
C D




Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)?
A
B
C D
1
Decreased blood loss
2
Less neural retraction
3
Improved neuroforaminal height
4
Lower fusion rates
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
[DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. ](http://www.ncbi.nlm.nih.gov/pubmed/18316711)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18316711)
[Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. ](http://www.ncbi.nlm.nih.gov/pubmed/24668350)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24668350)
[McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. ](http://www.ncbi.nlm.nih.gov/pubmed/15767888)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15767888)
RESPONSES FOR QUESTIONS 10 THROUGH 14
1. Postoperative deep surgical site infection
2. Proximal junctional kyphosis
3. Pedicle screw cut-out
4. Pseudarthrosis
5. Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
RECOMMENDED READINGS
[DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. ](http://www.ncbi.nlm.nih.gov/pubmed/18316711)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18316711)
[Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. ](http://www.ncbi.nlm.nih.gov/pubmed/24668350)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24668350)
[McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. ](http://www.ncbi.nlm.nih.gov/pubmed/15767888)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15767888)
RESPONSES FOR QUESTIONS 10 THROUGH 14
1. Postoperative deep surgical site infection
2. Proximal junctional kyphosis
3. Pedicle screw cut-out
4. Pseudarthrosis
5. Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
QUESTION 10
of 100
A 55-year-old man who has had multiple lumbar fusions during the last 10 years and a lumbar lordosis of 25 degrees notes difficulty standing upright without flexing his knees.
A 55-year-old man who has had multiple lumbar fusions during the last 10 years and a lumbar lordosis of 25 degrees notes difficulty standing upright without flexing his knees.
1
Postoperative deep surgical site infection
2
Proximal junctional kyphosis
3
Pedicle screw cut-out
4
Pseudarthrosis
5
Sagittal imbalance
- Sagittal imbalance
QUESTION 11
of 100
An 80-year-old woman with osteoporosis and thoracic kyphosis has a spinal fusion from T12-S1.
An 80-year-old woman with osteoporosis and thoracic kyphosis has a spinal fusion from T12-S1.
1
Postoperative deep surgical site infection
2
Proximal junctional kyphosis
3
Pedicle screw cut-out
4
Pseudarthrosis
5
Sagittal imbalance
- Pedicle screw cut-
QUESTION 12
of 100
A 65-year-old woman with diabetes has fever and erythema 2 weeks after undergoing instrumented spinal fusion.
A 65-year-old woman with diabetes has fever and erythema 2 weeks after undergoing instrumented spinal fusion.
1
Postoperative deep surgical site infection
2
Proximal junctional kyphosis
3
Pedicle screw cut-out
4
Pseudarthrosis
5
Sagittal imbalance
- Postoperative deep surgical site infection
QUESTION 13
of 100
A 60-year-old man with a pelvic incidence of 75 degrees undergoes an instrumented fusion for degenerative scoliosis from T11-S1, achieving a lumbar lordosis of 50 degrees.
A 60-year-old man with a pelvic incidence of 75 degrees undergoes an instrumented fusion for degenerative scoliosis from T11-S1, achieving a lumbar lordosis of 50 degrees.
1
Postoperative deep surgical site infection
2
Proximal junctional kyphosis
3
Pedicle screw cut-out
4
Pseudarthrosis
5
Sagittal imbalance
- Proximal junctional kyphosis
QUESTION 14
of 100
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
1
Postoperative deep surgical site infection
2
Proximal junctional kyphosis
3
Pedicle screw cut-out
4
Pseudarthrosis
5
Sagittal imbalance
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
[9/. PubMed PMID: 16166889.](http://www.ncbi.nlm.nih.gov/pubmed/16166889)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16166889)
[Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976). 2006 Sep 15;31(20):2359-66. PubMed PMID: 16985465.](http://www.ncbi.nlm.nih.gov/pubmed/16985465)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985465)
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
[9/. PubMed PMID: 16166889.](http://www.ncbi.nlm.nih.gov/pubmed/16166889)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16166889)
[Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976). 2006 Sep 15;31(20):2359-66. PubMed PMID: 16985465.](http://www.ncbi.nlm.nih.gov/pubmed/16985465)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985465)
QUESTION 15
of 100
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
1
there are no differences in functional outcome.
2
open diskectomy is associated with superior functional outcomes.
3
tubular diskectomy is associated with superior short- and long-term results.
4
tubular diskectomy is associated with inferior short-term results but superior long-term outcomes.
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183.](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142.](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183.](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142.](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
QUESTION 16
of 100
A 58-year-old man has had increasing midback pain for 8 weeks. Radiographs reveal mild osteopenia and mild disk degeneration but no fractures or lesions. An MRI of the spine reveals diskitis with a small-intensity signal within the spinal canal that is consistent with an epidural abscess at T11-12. The patient is neurologically intact but in significant pain. CT-guided biopsy of the disk space is positive for methicillin-sensitive Staphylococcus aureus. What is the most appropriate treatment?
A 58-year-old man has had increasing midback pain for 8 weeks. Radiographs reveal mild osteopenia and mild disk degeneration but no fractures or lesions. An MRI of the spine reveals diskitis with a small-intensity signal within the spinal canal that is consistent with an epidural abscess at T11-12. The patient is neurologically intact but in significant pain. CT-guided biopsy of the disk space is positive for methicillin-sensitive Staphylococcus aureus. What is the most appropriate treatment?
1
Intravenous (IV) antibiotics for 6 weeks and clinical observation
2
Observation and bracing alone
3
Laminectomy and posterior spinal fusion with IV antibiotics
4
Anterior spinal debridement and fusion with IV antibiotics
The treatment of spinal infections is variable. A diskitis in a patient with a mechanically stable spine without neurologic compromise is typically treated with needle biopsy/culture and appropriate IV antibiotics. Epidural abscess often is considered one of the true orthopaedic emergencies that necessitates surgical intervention. However, there is growing evidence that medical management can be appropriate to treat epidural abscesses in certain cases. In cases involving neurologic deterioration, surgical decompression, drainage, and systemic IV antibiotics is the treatment of choice. Medical management of spinal abscesses can be considered when a patient refuses surgical decompression; surgery is contraindicated because of high risk, pain, or
infection; or paralysis lasting longer than 24 to 36 hours results in a likely inability to reverse the paralysis. Patients who are neurologically intact may also be treated with medical management alone if they are stable and have an identifiable microorganism that can be observed closely to assess for neurologic deterioration. If neurologic changes are noted, surgical decompression and debridement and continued IV antibiotic therapy are appropriate.
RECOMMENDED READINGS
[Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006 Nov 9;355(19):2012-20. Review. PubMed PMID: 17093252.](http://www.ncbi.nlm.nih.gov/pubmed/17093252)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17093252)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683.](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. Review. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
[Siddiq F, Chowfin A, Tight R, Sahmoun AE, Smego RA Jr. Medical vs surgical management of spinal epidural abscess. Arch Intern Med. 2004 Dec 13-27;164(22):2409-12. PubMed PMID: 15596629. ](http://www.ncbi.nlm.nih.gov/pubmed/15596629)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15596629)
infection; or paralysis lasting longer than 24 to 36 hours results in a likely inability to reverse the paralysis. Patients who are neurologically intact may also be treated with medical management alone if they are stable and have an identifiable microorganism that can be observed closely to assess for neurologic deterioration. If neurologic changes are noted, surgical decompression and debridement and continued IV antibiotic therapy are appropriate.
RECOMMENDED READINGS
[Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006 Nov 9;355(19):2012-20. Review. PubMed PMID: 17093252.](http://www.ncbi.nlm.nih.gov/pubmed/17093252)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17093252)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683.](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. Review. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
[Siddiq F, Chowfin A, Tight R, Sahmoun AE, Smego RA Jr. Medical vs surgical management of spinal epidural abscess. Arch Intern Med. 2004 Dec 13-27;164(22):2409-12. PubMed PMID: 15596629. ](http://www.ncbi.nlm.nih.gov/pubmed/15596629)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15596629)
QUESTION 17
of 100
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
1
Perform an immediate wake-up test
2
Continue with the surgery and reassess in 5 minutes
3
Administer intravenous methylprednisolone
4
Ensure that mean arterial blood pressure is 80 or higher
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
[Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116091)
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
[Review. PubMed PMID: 21102290. ](http://www.ncbi.nlm.nih.gov/pubmed/21102290)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102290)
RECOMMENDED READINGS
[Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116091)
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
[Review. PubMed PMID: 21102290. ](http://www.ncbi.nlm.nih.gov/pubmed/21102290)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102290)
QUESTION 18
of 100
A
B
Figures 18a and 18b are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his followup visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?



A
B
Figures 18a and 18b are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his followup visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?
1
Nonsteroidal anti-inflammatory drugs (NSAIDS), physical therapy, and activity modification
2
Continued soft corset use
3
Thoracolumbosacral orthosis (TLSO) bracing
4
Posterior stabilization
The patient has previously undiagnosed ankylosing spondylitis. Radiographs reveal nonmarginal syndesmophytes throughout the lumbar spine. The CT scan reveals a nondisplaced 3-column fracture. Many patients with missed spinal injuries present in followup with neurologic worsening or progressive deformity. Fractures can often involve all 3 columns, including the posterior elements. In patients with ankylosing spondylitis, this represents an unstable injury and a high likelihood of displacement with nonsurgical treatment. Surgical treatment in the form of a posterior spinal fusion is indicated. Because the fracture is nondisplaced and the patient is neurologically intact, decompression via an anterior approach is not indicated. Bracing either with a TLSO brace or a soft corset will not provide sufficient stability for this fracture pattern. Physical therapy and NSAIDS are not indicated in this scenario.
RECOMMENDED READINGS
Hu SS, Ananthakrishnan D. Ankylosing spondylitis. In: Herkowitz HN, Garfin SR, eds. The Spine. 5th ed. Philadelphia, PA: Elsevier; 2006:763-761.
Blam OG, Cotler JM: Fractures in the stiff and osteoporotic spine. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction,. 3rd ed. Philadelphia, PA: Elsevier; 2003.
RECOMMENDED READINGS
Hu SS, Ananthakrishnan D. Ankylosing spondylitis. In: Herkowitz HN, Garfin SR, eds. The Spine. 5th ed. Philadelphia, PA: Elsevier; 2006:763-761.
Blam OG, Cotler JM: Fractures in the stiff and osteoporotic spine. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction,. 3rd ed. Philadelphia, PA: Elsevier; 2003.
QUESTION 19
of 100
A
B
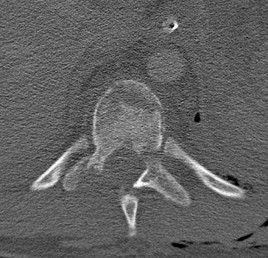
Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
A
B
Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
1
Axial load
2
Rotation
3
Extension
4
Distraction
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
[Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.](http://www.ncbi.nlm.nih.gov/pubmed/%0a16685239)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/%0a16685239)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%0a16685239)
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
[Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.](http://www.ncbi.nlm.nih.gov/pubmed/%0a16685239)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/%0a16685239)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%0a16685239)
QUESTION 20
of 100
A number of potential complications are associated with the direct lateral approach to the lumbar spine; which complication is most common?


A number of potential complications are associated with the direct lateral approach to the lumbar spine; which complication is most common?
1
Infection
2
Iliopsoas weakness
3
Injury to the aorta
4
Foot drop
Sofianos and associates examined the cases of 45 patients who underwent the lateral transpsoas approach and found that 18 of 45 patients (40%) experienced at least 1 complication. The most common complication was postsurgical weakness of the iliopsoas, which was an issue for 10 of 45 patients (22.2%). The second-most-common complication in this series was anterior thigh hypoesthesia. This occurred in 8 of 45 patients (17.8%). A series of 600 patients by Rodgers and associates noted that thigh pain and psoas weakness following a direct lateral approach to the lumbar spine were both "nearly universal" but almost "always transient."
RECOMMENDED READINGS
Sofianos DA, Briseño MR, Abrams J, Patel AA. Complications of the lateral transpsoas approach for lumbar interbody arthrodesis: a case series and literature review. Clin Orthop Relat Res. 2012 Jun;470(6):1621-32. doi: 10.1007/s11999-011-2088-3. Review. PubMed
[PMID: 21948287.](http://www.ncbi.nlm.nih.gov/pubmed/21948287)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21948287)
[Lee YP, Regev GJ, Chan J, Zhang B, Taylor W, Kim CW, Garfin SR. Evaluation of hip flexion strength following lateral lumbar interbody fusion. Spine J. 2013 Oct;13(10):1259-62. doi: 10.1016/j.spinee.2013.05.031. Epub 2013 Jul 12. PubMed PMID: 23856656. ](http://www.ncbi.nlm.nih.gov/pubmed/23856656)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23856656)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23856656)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23856656)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
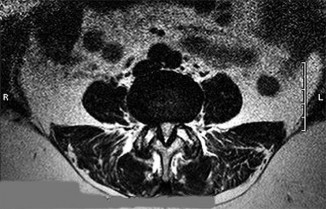
Figures 21a through 21c are the preoperative lateral standing radiograph, axial T2-weighted MR image at L4-5, and supine sagittal MR image of a 45-year-old woman who has had back and leg pain for 2 years. Treatment had included nonsteroidal anti-inflammatory drugs, physical therapy, and epidural corticosteroid injections. Her pain limited her activities of daily living; she could walk only 1 to 2 blocks before her pain became intolerable.
21A
B
C
RECOMMENDED READINGS
Sofianos DA, Briseño MR, Abrams J, Patel AA. Complications of the lateral transpsoas approach for lumbar interbody arthrodesis: a case series and literature review. Clin Orthop Relat Res. 2012 Jun;470(6):1621-32. doi: 10.1007/s11999-011-2088-3. Review. PubMed
[PMID: 21948287.](http://www.ncbi.nlm.nih.gov/pubmed/21948287)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21948287)
[Lee YP, Regev GJ, Chan J, Zhang B, Taylor W, Kim CW, Garfin SR. Evaluation of hip flexion strength following lateral lumbar interbody fusion. Spine J. 2013 Oct;13(10):1259-62. doi: 10.1016/j.spinee.2013.05.031. Epub 2013 Jul 12. PubMed PMID: 23856656. ](http://www.ncbi.nlm.nih.gov/pubmed/23856656)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23856656)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23856656)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23856656)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
Figures 21a through 21c are the preoperative lateral standing radiograph, axial T2-weighted MR image at L4-5, and supine sagittal MR image of a 45-year-old woman who has had back and leg pain for 2 years. Treatment had included nonsteroidal anti-inflammatory drugs, physical therapy, and epidural corticosteroid injections. Her pain limited her activities of daily living; she could walk only 1 to 2 blocks before her pain became intolerable.
21A
B
C
QUESTION 21
of 100
A lateral transpsoas interbody fusion with percutaneous pedicle screws was performed. When compared with those undergoing open laminectomy and fusion, this patient can expect
A lateral transpsoas interbody fusion with percutaneous pedicle screws was performed. When compared with those undergoing open laminectomy and fusion, this patient can expect
1
a longer hospital stay.
2
a higher complication rate.
3
higher risk for postoperative thigh pain.
4
no relief of lower extremity symptoms.
- higher risk for postoperative thigh pain.
QUESTION 22
of 100
The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain?
22A B

The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain?
22A B
1
Excessive retraction of the traversing nerve root
2
Bony overgrowth from the use of BMP protein in the disk space
3
Osteomyelitis with compression of the nerve roots
4
Inadequate decompression after surgery
Transient thigh pain after lateral, transpsoas interbody fusion is common and generally lasts for less than 3 months. Transpsoas interbody fusion with slip reduction can result in indirect spinal decompression and often obviates the need for a laminectomy for most patients. Complications with this approach are comparable to those experienced with open surgery, but the hospital stay is generally shorter.
Use of BMP in interbody devices has also become common. The images above show heterotopic bone growth into the spinal canal causing nerve compression. This complication is more commonly encountered after posterior lumbar interbody fusions.
RECOMMENDED READINGS
Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements.
[Spine (Phila Pa 1976). 2010 Dec 15;35(26 Suppl):S331-7. doi: 10.1097/BRS.0b013e3182022db0. PubMed PMID: 21160397. ](http://www.ncbi.nlm.nih.gov/pubmed/21160397)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21160397) Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011 Jul;15(1):11-8. doi: 10.3171/2011.2.SPINE10374. Epub 2011 Apr 8. PubMed PMID:
[21476801.](http://www.ncbi.nlm.nih.gov/pubmed/21476801)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21476801)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: a potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2). Spine J. 2008 Nov-Dec;8(6):1011-8. Epub 2007 Nov 26. PubMed PMID: 18037352.](http://www.ncbi.nlm.nih.gov/pubmed/18037352)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18037352)
[Chen NF, Smith ZA, Stiner E, Armin S, Sheikh H, Khoo LT. Symptomatic ectopic bone formation after off-label use of recombinant human bone morphogenetic protein-2 in transforaminal lumbar interbody fusion. J Neurosurg Spine. 2010 Jan;12(1):40-6. doi: 10.3171/2009.4.SPINE0876. PubMed PMID: 20043763.](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[View ](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)
Rouben D, Casnellie M, Ferguson M. Long-term durability of minimal invasive posterior transforaminal lumbar interbody fusion: a clinical and radiographic follow-up. J Spinal Disord Tech. 2011 Jul;24(5):288-96. doi:10.1097/BSD.0b013e3181f9a60a. PubMed PMID:
[20975594.](http://www.ncbi.nlm.nih.gov/pubmed/20975594)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20975594)
Use of BMP in interbody devices has also become common. The images above show heterotopic bone growth into the spinal canal causing nerve compression. This complication is more commonly encountered after posterior lumbar interbody fusions.
RECOMMENDED READINGS
Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements.
[Spine (Phila Pa 1976). 2010 Dec 15;35(26 Suppl):S331-7. doi: 10.1097/BRS.0b013e3182022db0. PubMed PMID: 21160397. ](http://www.ncbi.nlm.nih.gov/pubmed/21160397)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21160397) Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011 Jul;15(1):11-8. doi: 10.3171/2011.2.SPINE10374. Epub 2011 Apr 8. PubMed PMID:
[21476801.](http://www.ncbi.nlm.nih.gov/pubmed/21476801)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21476801)
[Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. ](http://www.ncbi.nlm.nih.gov/pubmed/21192221)[View](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21192221)
[Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: a potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2). Spine J. 2008 Nov-Dec;8(6):1011-8. Epub 2007 Nov 26. PubMed PMID: 18037352.](http://www.ncbi.nlm.nih.gov/pubmed/18037352)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18037352)
[Chen NF, Smith ZA, Stiner E, Armin S, Sheikh H, Khoo LT. Symptomatic ectopic bone formation after off-label use of recombinant human bone morphogenetic protein-2 in transforaminal lumbar interbody fusion. J Neurosurg Spine. 2010 Jan;12(1):40-6. doi: 10.3171/2009.4.SPINE0876. PubMed PMID: 20043763.](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[View ](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2020043763)
Rouben D, Casnellie M, Ferguson M. Long-term durability of minimal invasive posterior transforaminal lumbar interbody fusion: a clinical and radiographic follow-up. J Spinal Disord Tech. 2011 Jul;24(5):288-96. doi:10.1097/BSD.0b013e3181f9a60a. PubMed PMID:
[20975594.](http://www.ncbi.nlm.nih.gov/pubmed/20975594)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20975594)
QUESTION 23
of 100
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
1
Primary lumbar disk herniation
2
Adolescent idiopathic scoliosis
3
Cervical spondylotic myelopathy
4
No conditions; there are no official guidelines
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
[Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. ](http://www.ncbi.nlm.nih.gov/pubmed/23116090)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116090) [Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[View ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20858377)
[Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[View](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24688334)
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
[Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. ](http://www.ncbi.nlm.nih.gov/pubmed/23116090)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116090) [Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[View ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20858377)
[Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[View](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24688334)
QUESTION 24
of 100
A 56-year-old man has upper thoracic pain after undergoing stereotactic radiosurgery for a blastic metastatic lesion in the vertebral body of T5. He has normal alignment without collapse, but the tumor involves the entire vertebral body. Which factor increases this patient's risk for a pathologic fracture?
A 56-year-old man has upper thoracic pain after undergoing stereotactic radiosurgery for a blastic metastatic lesion in the vertebral body of T5. He has normal alignment without collapse, but the tumor involves the entire vertebral body. Which factor increases this patient's risk for a pathologic fracture?
1
Location of the lesion at T5
2
History of stereotactic radiation
3
Blastic nature of the tumor
4
Tumor involving all of the vertebral body
Criteria for spinal instability have been outlined by the Spine Oncology Study Group, which developed the Spinal Instability Neoplastic Score (SINS) criteria. Factors associated with lower risk for instability/fracture are location outside of a junctional level (the SINS criteria use C7-T2 as the junctional level),
blastic metastases, and no evidence of vertebral collapse (even with more than 50% involvement). Radiation has been associated with risk for pathologic fracture, and stereotactic radiation has been associated with risk for a spinal fracture.
RECOMMENDED READINGS
Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fourney DR. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010 Oct 15;35(22):E1221-9. doi: 10.1097/BRS.0b013e3181e16ae2. Review. PubMed
[PMID:20562730. ](http://www.ncbi.nlm.nih.gov/pubmed/20562730)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20562730)
[Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH, Bilsky MH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fisher CG. Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol. 2011 Aug 1;29(22):3072-7. doi:10.1200/JCO.2010.34.3897. Epub 2011 Jun 27. PubMed PMID: 21709187. ](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[at ](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21709187)
Rose PS, Laufer I, Boland PJ, Hanover A, Bilsky MH, Yamada J, Lis E. Risk of fracture after single fraction image-guided intensity-modulated radiation therapy to spinal metastases. J Clin Oncol. 2009 Oct 20;27(30):5075-9. doi: 10.1200/JCO.2008.19.3508. Epub 2009 Sep 8.
[PubMed PMID: 19738130 ](http://www.ncbi.nlm.nih.gov/pubmed/19738130)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19738130)
blastic metastases, and no evidence of vertebral collapse (even with more than 50% involvement). Radiation has been associated with risk for pathologic fracture, and stereotactic radiation has been associated with risk for a spinal fracture.
RECOMMENDED READINGS
Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fourney DR. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010 Oct 15;35(22):E1221-9. doi: 10.1097/BRS.0b013e3181e16ae2. Review. PubMed
[PMID:20562730. ](http://www.ncbi.nlm.nih.gov/pubmed/20562730)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20562730)
[Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH, Bilsky MH, Harrop JS, Fehlings MG, Boriani S, Chou D, Schmidt MH, Polly DW, Biagini R, Burch S, Dekutoski MB, Ganju A, Gerszten PC, Gokaslan ZL, Groff MW, Liebsch NJ, Mendel E, Okuno SH, Patel S, Rhines LD, Rose PS, Sciubba DM, Sundaresan N, Tomita K, Varga PP, Vialle LR, Vrionis FD, Yamada Y, Fisher CG. Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol. 2011 Aug 1;29(22):3072-7. doi:10.1200/JCO.2010.34.3897. Epub 2011 Jun 27. PubMed PMID: 21709187. ](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[at ](http://www.ncbi.nlm.nih.gov/pubmed/21709187)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21709187)
Rose PS, Laufer I, Boland PJ, Hanover A, Bilsky MH, Yamada J, Lis E. Risk of fracture after single fraction image-guided intensity-modulated radiation therapy to spinal metastases. J Clin Oncol. 2009 Oct 20;27(30):5075-9. doi: 10.1200/JCO.2008.19.3508. Epub 2009 Sep 8.
[PubMed PMID: 19738130 ](http://www.ncbi.nlm.nih.gov/pubmed/19738130)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19738130)
QUESTION 25
of 100
A
B
C
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?




A
B
C
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
1
Order a prostate-specific antigen (PSA) level
2
Perform a 2-level corpectomy and reconstruction with tissue sent for pathologic analysis
3
Fine-needle aspiration
4
Bone scan
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
QUESTION 26
of 100
Based on this patient's history and examination, what is the best next step?
Based on this patient's history and examination, what is the best next step?
1
Order a confirmatory erythrocyte sedimentation rate (ESR)
2
Obtain blood cultures
3
Initiate empiric broad-spectrum antibiotics
4
Perform surgical decompression
- Obtain blood cultures
QUESTION 27
of 100
Blood cultures reveal methicillin-sensitive Staphylococcus aureus (MSSA). The patient's examination remains unchanged. In addition to outpatient serial laboratory studies and weekly observation for neurologic deterioration, which of the following is the most appropriate for nonoperative treatment?
Blood cultures reveal methicillin-sensitive Staphylococcus aureus (MSSA). The patient's examination remains unchanged. In addition to outpatient serial laboratory studies and weekly observation for neurologic deterioration, which of the following is the most appropriate for nonoperative treatment?
1
Interventional radiology placement of an epidural drain
2
An 8-week course of intravenous (IV) vancomycin
3
An 8-week course of IV nafcillin
4
An 8-week course of oral amoxicillin
- An 8-week course of IV nafcillin
QUESTION 28
of 100
Clinical characteristics of patients who are ideal for a nonsurgical treatment trial (instead of surgery) include
Clinical characteristics of patients who are ideal for a nonsurgical treatment trial (instead of surgery) include
1
absence of neurologic deficits and MSSA infection.
2
normal blood pressure and normal heart rate.
3
negative blood cultures, cocaine abuse
4
normal blood pressure and normal heart rate
- absence of neurologic deficits and MSSA infection.
QUESTION 29
of 100
What would be the advantage of surgery for the patient described in this scenario?
What would be the advantage of surgery for the patient described in this scenario?
1
Shorter length of antibiotic therapy
2
Reduced mortality risk
3
Reduced risk for neurologic deterioration
4
Reduced risk for chronic pain
The MR image of the lumbar spine postgadolinium contrast shows a ring-enhancing fluid collection. Ring-enhancing lesions within the spinal canal on postgadolinium MR images are indicative of epidural abscess. It is important to obtain a culture-specific diagnosis to inform the choice of antibiotics and educate patients regarding the likelihood of failure for standalone antibiotic therapy. Infection with MSSA, age younger than 65 years, the absence of neurologic deficit, and lumbar abscess location are all factors that point toward a patient being a reasonable candidate for a trial of culture-specific IV antibiotics. In this case, nafcillin is a suitable treatment for MSSA. The antibiotic should be initiated and closely observed with serial labs (WBC, ESR, CRP, repeat blood cultures) to ensure that the patient responds appropriately to therapy and that neurologic deficits do not develop. In the setting of epidural abscess, surgery is performed to evacuate the abscess and reverse or prevent neurologic deterioration. In the current scenario in which sepsis is not an issue, scant high-quality evidence shows that surgical intervention influences risk for mortality or chronic pain following epidural abscess.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Adogwa O, Karikari IO, Carr KR, Krucoff M, Ajay D, Fatemi P, Perez EL, Cheng JS, Bagley CA, Isaacs RE. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014 Mar;20(3):344-9. doi: 10.3171/2013.11.SPINE13527. Epub 2013 Dec 20. Review.
[PubMed PMID: 24359002.](http://www.ncbi.nlm.nih.gov/pubmed/24359002)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24359002)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014
Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683.](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
Schoenfeld AJ. Spine infections. In: Cannada L, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2014: 737-747.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Adogwa O, Karikari IO, Carr KR, Krucoff M, Ajay D, Fatemi P, Perez EL, Cheng JS, Bagley CA, Isaacs RE. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014 Mar;20(3):344-9. doi: 10.3171/2013.11.SPINE13527. Epub 2013 Dec 20. Review.
[PubMed PMID: 24359002.](http://www.ncbi.nlm.nih.gov/pubmed/24359002)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24359002)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014
Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683.](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
Schoenfeld AJ. Spine infections. In: Cannada L, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2014: 737-747.
QUESTION 30
of 100
A
B
C
Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of
physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with
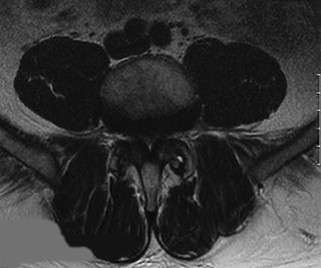


A
B
C
Figures 30a through 30c are the radiograph and MR images of a 54-year-old woman who has severe leg pain with walking. Her treatment has included 12 weeks of
physical therapy, anti-inflammatory medications, and narcotic pain relievers, and she is interested in surgery. Minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) is recommended. When compared with open TLIF, MIS TLIF is associated with
1
shorter hospital stay.
2
lower rates of fusion.
3
higher complication rates.
4
worse long-term outcomes.
MIS TLIF involves a steep learning curve but is associated with similar longterm outcomes as open TLIF, arguably comparable or possibly lower complication rates, and equivalent fusion rates. The major distinguishing feature comparing open to minimally invasive surgery for this and other spinal diagnoses has been shorter hospital stays.
RECOMMENDED READINGS
[Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. ](http://www.ncbi.nlm.nih.gov/pubmed/19478658)[View](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
[22453894/. ](http://www.ncbi.nlm.nih.gov/pubmed/22453894)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22453894)
[Lau D, Lee JG, Han SJ, Lu DC, Chou D. Complications and perioperative factors associated with learning the technique of minimally invasive transforaminal lumbar interbody fusion (TLIF). J Clin Neurosci. 2011 May;18(5):624-7. doi: 10.1016/j.jocn.2010.09.004. Epub 2011 Feb 23. PubMed PMID: 21349719. ](http://www.ncbi.nlm.nih.gov/pubmed/21349719)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21349719)
RECOMMENDED READINGS
[Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1385-9. doi: 10.1097/BRS.0b013e3181a4e3be. PubMed PMID: 19478658. ](http://www.ncbi.nlm.nih.gov/pubmed/19478658)[View](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19478658)
Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012 Nov;21(11):2265-70. doi: 10.1007/s00586-012-2281-4. Epub 2012 Mar 28. PubMed PMID:
[22453894/. ](http://www.ncbi.nlm.nih.gov/pubmed/22453894)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22453894)
[Lau D, Lee JG, Han SJ, Lu DC, Chou D. Complications and perioperative factors associated with learning the technique of minimally invasive transforaminal lumbar interbody fusion (TLIF). J Clin Neurosci. 2011 May;18(5):624-7. doi: 10.1016/j.jocn.2010.09.004. Epub 2011 Feb 23. PubMed PMID: 21349719. ](http://www.ncbi.nlm.nih.gov/pubmed/21349719)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21349719)
QUESTION 31
of 100
An orthopaedic surgeon is counseling a patient regarding risk for complications following lumbar fusion via a direct lateral approach. Surgery at which level is most likely to injure the lumbosacral plexus?
An orthopaedic surgeon is counseling a patient regarding risk for complications following lumbar fusion via a direct lateral approach. Surgery at which level is most likely to injure the lumbosacral plexus?
1
L1-2
2
L2-3
3
L3-4
4
L4-5
During the direct lateral approach, interbody fusion devices are inserted through a lateral window in the psoas muscle. To accomplish this, dilators and retractors are positioned at the posterior half of the disk space, and it must be noted that the lumbosacral plexus lies within the psoas muscle between the transverse process and vertebral body and departs distally at the medial edge of the psoas. Consequently, lateral interbody fusion poses risk for injury to the lumbosacral plexus. A cadaveric study demonstrated that the lumbosacral plexus progressively migrates from dorsal to ventral in the lumbar spine. Therefore, the plexus is most likely to be injured during an L4-L5 fusion because at this level the lumbosacral plexus is closest to the location at which dilators and retractors are placed.
A 2013 retrospective study by Le and associates followed 71 patients who underwent minimally invasive fusion via a lateral interbody approach. In this study, 54.9% (39/71) had immediate postsurgical ipsilateral iliopsoas or quadriceps weakness. Of these patients, the majority had resolution by 3 months (92.3%), and all had complete resolution by 2 years.
RECOMMENDED READINGS
Le TV, Burkett CJ, Deukmedjian AR, Uribe JS. Postoperative lumbar plexus injury after lumbar retroperitoneal transpsoas minimally invasive lateral interbody fusion. Spine (Phila Pa 1976). 2013 Jan 1;38(1):E13-20. doi: 10.1097/BRS.0b013e318278417c. PubMed PMID: 23073358.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23073358)
[Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J Neurosurg Spine. 2009 Feb;10(2):139-44. doi: 10.3171/2008.10.SPI08479. PubMed PMID: 19278328. ](http://www.ncbi.nlm.nih.gov/pubmed/19278328)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19278328)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/19278328)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19278328)
Knight RQ, Schwaegler P, Hanscom D, Roh J. Direct lateral lumbar interbody fusion for degenerative conditions: early complication profile. J Spinal Disord Tech. 2009 Feb;22(1):34-
[7/. doi: 10.1097/BSD.0b013e3181679b8a. PubMed PMID: 19190432.](http://www.ncbi.nlm.nih.gov/pubmed/19190432)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19190432)
A 2013 retrospective study by Le and associates followed 71 patients who underwent minimally invasive fusion via a lateral interbody approach. In this study, 54.9% (39/71) had immediate postsurgical ipsilateral iliopsoas or quadriceps weakness. Of these patients, the majority had resolution by 3 months (92.3%), and all had complete resolution by 2 years.
RECOMMENDED READINGS
Le TV, Burkett CJ, Deukmedjian AR, Uribe JS. Postoperative lumbar plexus injury after lumbar retroperitoneal transpsoas minimally invasive lateral interbody fusion. Spine (Phila Pa 1976). 2013 Jan 1;38(1):E13-20. doi: 10.1097/BRS.0b013e318278417c. PubMed PMID: 23073358.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23073358)
[Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J Neurosurg Spine. 2009 Feb;10(2):139-44. doi: 10.3171/2008.10.SPI08479. PubMed PMID: 19278328. ](http://www.ncbi.nlm.nih.gov/pubmed/19278328)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19278328)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/19278328)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19278328)
Knight RQ, Schwaegler P, Hanscom D, Roh J. Direct lateral lumbar interbody fusion for degenerative conditions: early complication profile. J Spinal Disord Tech. 2009 Feb;22(1):34-
[7/. doi: 10.1097/BSD.0b013e3181679b8a. PubMed PMID: 19190432.](http://www.ncbi.nlm.nih.gov/pubmed/19190432)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19190432)
QUESTION 32
of 100
Figure 32 shows the T2-weighted MR image through the L4-5 level of a 60-year-old man who has new-onset acute right lower-extremity pain and numbness and weakness in his right quadriceps muscle. The arrow in Figure 32 is pointing to which structure?
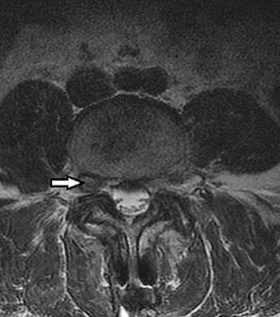
Figure 32 shows the T2-weighted MR image through the L4-5 level of a 60-year-old man who has new-onset acute right lower-extremity pain and numbness and weakness in his right quadriceps muscle. The arrow in Figure 32 is pointing to which structure?
1
Lumbar synovial cyst
2
Dorsal root ganglion
3
Herniated nucleus pulposus
4
Ligamentum flavum
The arrow is pointing to a structure of medium signal intensity that is equivalent to the nucleus pulposus on T2-weighted sequencing. This represents a foraminal disk herniation. A lumbar synovial cyst would display high-signal intensity on T2-weighted sequencing. Lumbar synovial cysts arise from the facet joints as a result of facet joint degeneration and may be a source of nerve root compression. The dorsal root ganglion is a collection of sensory nerve cell bodies and can be seen just dorsal and lateral to the disk herniation in Figure 32. The ligamentum flavum is located on the ventral
surface of the laminae and attaches between the laminae of adjacent vertebrae.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
Carrino JA, Morrison WB. Musculoskeletal imaging. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:119-136.
surface of the laminae and attaches between the laminae of adjacent vertebrae.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
Carrino JA, Morrison WB. Musculoskeletal imaging. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:119-136.
QUESTION 33
of 100
One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?
One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?
1
10% to 15%
2
30% to 35%
3
50% to 55%
4
70% to 75%
Dysphagia after anterior cervical diskectomy and fusion is a common, usually transient finding after anterior cervical approaches to the spine. While it has been reported to occur in up to 70% of patients 2 weeks following surgery, in most cases the symptoms quickly resolve. There is, however, a small subset of patients for whom symptoms of dysphagia will persist. Lee and associates prospectively studied the rate of dysphagia after anterior cervical diskectomy and fusion, reporting a 15% rate of dysphagia at 12 months, and 12% at 24 months. Phillips and associates analyzed the 2-year data from the PCM FDE clinical trial and found a 12.1% incidence of dysphagia in the ACDF arm.
RECOMMENDED READINGS
[Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study. Spine J. 2007 Mar-Apr;7(2):141-7. Epub 2007 Jan 22. PubMed PMID: 17321961. ](http://www.ncbi.nlm.nih.gov/pubmed/17321961)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17321961)
[Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004 Jul 1;29(13):1441-6. PubMed PMID: 15223936. ](http://www.ncbi.nlm.nih.gov/pubmed/15223936)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15223936)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15223936)
[Edwards CC 2nd, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST, Riew KD. Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am. 2004 Feb;86-A(2):251-6. PubMed PMID: 14960668. ](http://www.ncbi.nlm.nih.gov/pubmed/14960668)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14960668)
Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC. A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine (Phila Pa 1976). 2013 Jul 1;38(15):E907-18. doi: 10.1097/BRS.0b013e318296232f.
[Rihn JA, Kane J, Albert TJ, Vaccaro AR, Hilibrand AS. What is the incidence and severity of dysphagia after anterior cervical surgery? Clin Orthop Relat Res. 2011 Mar;469(3):658-65. PMID: 21140251.](http://www.ncbi.nlm.nih.gov/pubmed/21140251)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21140251)
RECOMMENDED READINGS
[Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study. Spine J. 2007 Mar-Apr;7(2):141-7. Epub 2007 Jan 22. PubMed PMID: 17321961. ](http://www.ncbi.nlm.nih.gov/pubmed/17321961)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17321961)
[Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004 Jul 1;29(13):1441-6. PubMed PMID: 15223936. ](http://www.ncbi.nlm.nih.gov/pubmed/15223936)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15223936)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15223936)
[Edwards CC 2nd, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST, Riew KD. Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am. 2004 Feb;86-A(2):251-6. PubMed PMID: 14960668. ](http://www.ncbi.nlm.nih.gov/pubmed/14960668)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14960668)
Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC. A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine (Phila Pa 1976). 2013 Jul 1;38(15):E907-18. doi: 10.1097/BRS.0b013e318296232f.
[Rihn JA, Kane J, Albert TJ, Vaccaro AR, Hilibrand AS. What is the incidence and severity of dysphagia after anterior cervical surgery? Clin Orthop Relat Res. 2011 Mar;469(3):658-65. PMID: 21140251.](http://www.ncbi.nlm.nih.gov/pubmed/21140251)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21140251)
QUESTION 34
of 100
What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?
What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?
1
MRI
2
Discography
3
CT discography
4
Radiography
Radiography is the best initial study. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain such as osteoporotic collapse, osteolytic collapse, and deformity also can be evaluated. The other tests may be beneficial and are more appropriate as later imaging options.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
3/. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:57-67.
Bess RS, Brodke DS. Degenerative disease of the lumbar spine. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:551-563.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
3/. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:57-67.
Bess RS, Brodke DS. Degenerative disease of the lumbar spine. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:551-563.
QUESTION 35
of 100
Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?
1
Transforming growth factor-beta (TGF-ß), bone morphogenetic protein-2 (BMP-2), latent membrane protein 1
2
Tissue inhibitor of matrix metallo-proteinase-1 (MMP-1), growth and development factor-5, noggin
3
Gremlin, MMP, biglycan
4
Tumor necrosis factor-alpha (TNF-a), Interleukin-1 (IL-1), MMP
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-a, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-ß, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
[Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18397957)
[Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. ](http://www.ncbi.nlm.nih.gov/pubmed/16298901)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16298901)
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
[Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18397957)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18397957)
[Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. ](http://www.ncbi.nlm.nih.gov/pubmed/16298901)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16298901)
QUESTION 36
of 100
A 45-year-old woman with a history of rheumatoid arthritis has C1-C2 instability with neurologic deterioration. Her posterior atlanto-dens interval is 10 mm. Which fixation technique will be the most biomechanically sound to facilitate fusion across the atlanto-axial junction?

A 45-year-old woman with a history of rheumatoid arthritis has C1-C2 instability with neurologic deterioration. Her posterior atlanto-dens interval is 10 mm. Which fixation technique will be the most biomechanically sound to facilitate fusion across the atlanto-axial junction?
1
Gallie fusion
2
Use of C1-C2 transarticular screws
3
Brooks fusion
4
Onlay grafting with a halo vest
C1-C2 transarticular screw fixation is 10-fold stiffer than wiring constructs, particularly in rotation; eliminates the need for postsurgical halo use; and is associated with reported fusion rates to a maximum of 100% for bilateral screws and 95% for unilateral fixation. All of the other fusion techniques mentioned are associated with a pseudarthrosis rate of at least 30%.
RECOMMENDED READINGS
[Stock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. J Bone Joint Surg Am. 2006 Jul;88(7):1642-9. PubMed PMID: 16841419. ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16841419)
[Sim HB, Lee JW, Park JT, Mindea SA, Lim J, Park J. Biomechanical evaluations of various c1-c2 posterior fixation techniques. Spine (Phila Pa 1976). 2011 Mar 15;36(6):E401-7. doi: 10.1097/BRS.0b013e31820611ba. PubMed PMID: 21372651. ](http://www.ncbi.nlm.nih.gov/pubmed/21372651)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21372651)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 43
Figure 37 is the lateral radiograph of a 71-year-old woman who has pain with ambulation that improves when she sits down. She had similar symptoms 2 years earlier when she underwent an L3-L5 posterior spinal fusion. Upon examination she has good range of hip and knee motion, 5/5 motor function, and normal sensation of her lower extremities. She has negative bilateral straight-leg raise findings and her knees slightly flex to stand upright
37
RECOMMENDED READINGS
[Stock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. J Bone Joint Surg Am. 2006 Jul;88(7):1642-9. PubMed PMID: 16841419. ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16841419)
[Sim HB, Lee JW, Park JT, Mindea SA, Lim J, Park J. Biomechanical evaluations of various c1-c2 posterior fixation techniques. Spine (Phila Pa 1976). 2011 Mar 15;36(6):E401-7. doi: 10.1097/BRS.0b013e31820611ba. PubMed PMID: 21372651. ](http://www.ncbi.nlm.nih.gov/pubmed/21372651)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21372651)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 43
Figure 37 is the lateral radiograph of a 71-year-old woman who has pain with ambulation that improves when she sits down. She had similar symptoms 2 years earlier when she underwent an L3-L5 posterior spinal fusion. Upon examination she has good range of hip and knee motion, 5/5 motor function, and normal sensation of her lower extremities. She has negative bilateral straight-leg raise findings and her knees slightly flex to stand upright
37
QUESTION 37
of 100
What is the most likely diagnosis considering this patient's history and examination?
What is the most likely diagnosis considering this patient's history and examination?
1
Metastatic disease of the spine
2
Neurogenic claudication
3
Degenerative joint disease of the hips
4
Degenerative scoliosis
- Neurogenic claudication
QUESTION 38
of 100
In addition to MR imaging, what is the most appropriate additional radiographic study at this time?
In addition to MR imaging, what is the most appropriate additional radiographic study at this time?
1
Mechanical axis of the lower extremities
2
Long-standing radiograph of the entire spine
3
Nuclear medicine: triple-phase bone scan
4
Hyperextension radiograph of the lumbar spine
- Long-standing radiograph of the entire spine
QUESTION 39
of 100
In addition to her planned primary procedure, how can the surgeon best improve this patient's lumbar lordosis?
In addition to her planned primary procedure, how can the surgeon best improve this patient's lumbar lordosis?
1
Placement of bilateral iliac screws
2
Use of an interbody strut at L5-S1
3
Extension of instrumentation to T11
4
Extension lumbosacral orthosis
- Use of an interbody strut at L5-S1
QUESTION 40
of 100
The patient is treated by another physician and undergoes the procedure shown in Figures 40a and 40b. She currently cannot stand upright. Spinopelvic measurements reveal her pelvic incidence to be 85 degrees and pelvic tilt to be 40 degrees. Her lordosis from T12-S1 is 35 degrees. Which additional surgical procedure should be considered?
40A
B

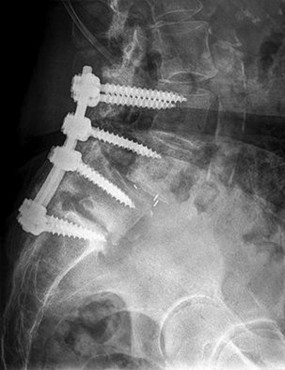
The patient is treated by another physician and undergoes the procedure shown in Figures 40a and 40b. She currently cannot stand upright. Spinopelvic measurements reveal her pelvic incidence to be 85 degrees and pelvic tilt to be 40 degrees. Her lordosis from T12-S1 is 35 degrees. Which additional surgical procedure should be considered?
40A
B
1
Single-level pedicle subtraction osteotomy
2
Single-level Smith-Petersen osteotomy
3
Instrumentation removal
4
Percutaneous fusion of the sacroiliac joints
- Single-level pedicle subtraction osteotomy
QUESTION 41
of 100
The patient's postsurgical radiographs reveal a sagittal vertical axis of +8 cm. In addition to the usual issues encountered during the early postsurgical period, what should the surgeon be most concerned about?
The patient's postsurgical radiographs reveal a sagittal vertical axis of +8 cm. In addition to the usual issues encountered during the early postsurgical period, what should the surgeon be most concerned about?
1
Instrumentation-related pain
2
Broken rod
3
Sacroiliac dissociation
4
Proximal junctional failure
- Proximal junctional failure
QUESTION 42
of 100
Bearing in mind her current condition as shown in Figures 40a and 40b, the surgeon should inform the patient and family that if she is to stand erect, she
Bearing in mind her current condition as shown in Figures 40a and 40b, the surgeon should inform the patient and family that if she is to stand erect, she
1
needs further spinal extensor strengthening.
2
will need to wear a spinal brace indefinitely.
3
will need another spinal surgery.
4
will need a spinal cord stimulator.
- will need another spinal surgery.
QUESTION 43
of 100
If additional posterior spinal surgery is performed to allow the patient to stand erect, the surgeon will need to advise the family about the risks of the procedure. In addition to risk for neurologic injury, what is the most likely complication?
If additional posterior spinal surgery is performed to allow the patient to stand erect, the surgeon will need to advise the family about the risks of the procedure. In addition to risk for neurologic injury, what is the most likely complication?
1
Substantial blood loss
2
Cerebral vascular accident
3
Degeneration of sacroiliac joints
4
Cervical spine stenosis
This case starts as standard degenerative spondylolisthesis but develops into a sagittal imbalance problem necessitating a major spinal procedure including
a pedicle subtraction osteotomy and extended posterior spinal instrumentation. Initially the patient had an L3-L5 posterior spinal fusion with a laminectomy and interbody fusion for an L4-L5 stenosis and degenerative spondylolisthesis. Two years after this procedure she is having difficult ambulation that improves with sitting. These symptoms are typical for neurogenic claudication associated with spinal stenosis. Adjacent segment degeneration leading to spinal stenosis is a common late complication associated with lumbar instrumented fusions, particularly in older patients. Figure 40b shows the adjacent segment degeneration at L5-S1 with the development of a degenerative spondylolisthesis. Degenerative spondylolisthesis is a radiographic sign of substantial degeneration of a disk space and is often associated with spinal stenosis. The primary procedure typically planned to address a degenerative spondylolisthesis is a laminectomy. An adjacent-level degenerative spondylolisthesis is typically instrumented and fused to the previous fusion construct.
The degeneration of the adjacent disk is also associated with a loss of disk height. A concern in this patient is the development of kyphosis at the L5-S1 disk space. Kyphosis at the lumbosacral junction can lead to sagittal imbalance issues. Spinal surgeons need to be aware of spinopelvic measurements to help prevent sagittal imbalance and proximal junctional failures. Improving the lumbar lordosis in this patient would necessitate restoration of the disk height at L5-S1. This can be accomplished with an interbody strut device placed either anteriorly or posteriorly via a posterolateral interbody approach at the time of the laminectomy.
This patient has undergone a posterior extension of her previous fusion without the addition of an interbody strut device. She now has further sagittal imbalance issues and an inability to stand erect without flexing her knees. This is a typical compensation posture that patients with significant sagittal imbalance acquire when trying to stand upright. Patients with sagittal imbalance are at increased risk for proximal junctional kyphosis or a more acute complication of proximal junctional failure.
The sagittal vertical axis is a plumb line dropped from C7 and should fall behind the hip joints and within 4 to 5 cm of the posterior corner of S1 (an easily identifiable radiographic marker). Pelvic incidence is a constant that is unique to each patient's spinopelvic anatomy. Pelvic incidence typically is within 10 degrees of the lumbar lordosis in an upright adult. Pelvic tilt (PT), on the other hand, can vary based on a patient's stance. PT is an indicator of the amount of compensation a patient has developed by retroverting their pelvis to stand upright. In an upright patient who is not compensating for loss of spinal sagittal alignment, the PT should be less than 20 degrees. In this case, the patient has a high PT and a significant lumbar lordosis/pelvic incidence mismatch with a significant positive sagittal imbalance (sagittal vertical axis of +8 cm). These are all indicators that a major spinal alignment procedure will be required to rebalance the spine. The use of posterior
osteotomies, such as a pedicle subtraction osteotomy, will be required if spinal realignment is planned. Pedicle subtraction osteotomies are considered 3-column osteotomies that remove the entire lamina, the facets, the pedicles (the posterior column), the underlying posterior vertebral wall and posterior vertebral body (middle column), and the underlying anterior vertebral body (anterior column) in a wedge fashion. Three-column osteotomies are associated with increased risk for neurologic injury and substantial blood loss. A Smith-Petersen osteotomy is a single-column posterior osteotomy that can provide a lesser amount of sagittal plane correction than pedicle subtraction osteotomy. A single-level Smith-Petersen osteotomy likely will not provide enough correction in this case.
RECOMMENDED READINGS
Lafage V, Schwab F, Vira S, Patel A, Ungar B, Farcy JP. Spino-pelvic parameters after surgery can be predicted: a preliminary formula and validation of standing alignment. Spine (Phila Pa 1976). 2011 Jun;36(13):1037-45. doi: 10.1097/BRS.0b013e3181eb9469. PubMed PMID:
[21217459/. ](http://www.ncbi.nlm.nih.gov/pubmed/21217459)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21217459)
Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2224-
[31/. doi: 10.1097/BRS.0b013e3181ee6bd4. Review. PubMed PMID: 21102297. ](http://www.ncbi.nlm.nih.gov/pubmed/21102297)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/21102297)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21102297)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102297)
a pedicle subtraction osteotomy and extended posterior spinal instrumentation. Initially the patient had an L3-L5 posterior spinal fusion with a laminectomy and interbody fusion for an L4-L5 stenosis and degenerative spondylolisthesis. Two years after this procedure she is having difficult ambulation that improves with sitting. These symptoms are typical for neurogenic claudication associated with spinal stenosis. Adjacent segment degeneration leading to spinal stenosis is a common late complication associated with lumbar instrumented fusions, particularly in older patients. Figure 40b shows the adjacent segment degeneration at L5-S1 with the development of a degenerative spondylolisthesis. Degenerative spondylolisthesis is a radiographic sign of substantial degeneration of a disk space and is often associated with spinal stenosis. The primary procedure typically planned to address a degenerative spondylolisthesis is a laminectomy. An adjacent-level degenerative spondylolisthesis is typically instrumented and fused to the previous fusion construct.
The degeneration of the adjacent disk is also associated with a loss of disk height. A concern in this patient is the development of kyphosis at the L5-S1 disk space. Kyphosis at the lumbosacral junction can lead to sagittal imbalance issues. Spinal surgeons need to be aware of spinopelvic measurements to help prevent sagittal imbalance and proximal junctional failures. Improving the lumbar lordosis in this patient would necessitate restoration of the disk height at L5-S1. This can be accomplished with an interbody strut device placed either anteriorly or posteriorly via a posterolateral interbody approach at the time of the laminectomy.
This patient has undergone a posterior extension of her previous fusion without the addition of an interbody strut device. She now has further sagittal imbalance issues and an inability to stand erect without flexing her knees. This is a typical compensation posture that patients with significant sagittal imbalance acquire when trying to stand upright. Patients with sagittal imbalance are at increased risk for proximal junctional kyphosis or a more acute complication of proximal junctional failure.
The sagittal vertical axis is a plumb line dropped from C7 and should fall behind the hip joints and within 4 to 5 cm of the posterior corner of S1 (an easily identifiable radiographic marker). Pelvic incidence is a constant that is unique to each patient's spinopelvic anatomy. Pelvic incidence typically is within 10 degrees of the lumbar lordosis in an upright adult. Pelvic tilt (PT), on the other hand, can vary based on a patient's stance. PT is an indicator of the amount of compensation a patient has developed by retroverting their pelvis to stand upright. In an upright patient who is not compensating for loss of spinal sagittal alignment, the PT should be less than 20 degrees. In this case, the patient has a high PT and a significant lumbar lordosis/pelvic incidence mismatch with a significant positive sagittal imbalance (sagittal vertical axis of +8 cm). These are all indicators that a major spinal alignment procedure will be required to rebalance the spine. The use of posterior
osteotomies, such as a pedicle subtraction osteotomy, will be required if spinal realignment is planned. Pedicle subtraction osteotomies are considered 3-column osteotomies that remove the entire lamina, the facets, the pedicles (the posterior column), the underlying posterior vertebral wall and posterior vertebral body (middle column), and the underlying anterior vertebral body (anterior column) in a wedge fashion. Three-column osteotomies are associated with increased risk for neurologic injury and substantial blood loss. A Smith-Petersen osteotomy is a single-column posterior osteotomy that can provide a lesser amount of sagittal plane correction than pedicle subtraction osteotomy. A single-level Smith-Petersen osteotomy likely will not provide enough correction in this case.
RECOMMENDED READINGS
Lafage V, Schwab F, Vira S, Patel A, Ungar B, Farcy JP. Spino-pelvic parameters after surgery can be predicted: a preliminary formula and validation of standing alignment. Spine (Phila Pa 1976). 2011 Jun;36(13):1037-45. doi: 10.1097/BRS.0b013e3181eb9469. PubMed PMID:
[21217459/. ](http://www.ncbi.nlm.nih.gov/pubmed/21217459)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21217459)
Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2224-
[31/. doi: 10.1097/BRS.0b013e3181ee6bd4. Review. PubMed PMID: 21102297. ](http://www.ncbi.nlm.nih.gov/pubmed/21102297)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/21102297)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21102297)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102297)
QUESTION 44
of 100
A 78-year-old athletic woman has a history of severe back pain without antecedent trauma. She was in the emergency department 2 days ago with a T12 compression fracture. A dual x-ray absorptiometry (DEXA) scan performed earlier this year revealed a T-score of -2.8. Her condition may be attributable to
A 78-year-old athletic woman has a history of severe back pain without antecedent trauma. She was in the emergency department 2 days ago with a T12 compression fracture. A dual x-ray absorptiometry (DEXA) scan performed earlier this year revealed a T-score of -2.8. Her condition may be attributable to
1
translocation of chromosomes X and 18.
2
variant of the EXT1 gene.
3
polymorphism of p53.
4
polymorphism of the COL1A1 gene.
The diagnosis is severe osteoporosis because this patient's T-score is lower than -2.5 on DEXA scan and her fragility fracture involves the T12 vertebra. Osteoporosis may be associated with polymorphisms of the COL1A1 gene. EXT1 is associated with multiple hereditary exostoses, and translocation X:18 is associated with synovial sarcoma. The gene p53 is associated with Li-Fraumeni syndrome and osteosarcoma.
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
[PubMed PMID: 24273577. ? ](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)
[Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24566004)
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
[PubMed PMID: 24273577. ? ](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2024273577)
[Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24566004)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24566004)
QUESTION 45
of 100
A
B
Figures 45a and 45b are the CT and MR spine images of an 82-year-old man who has a history of ankylosing spondylitis falls onto his back. He has no
neurologic deficits upon examination in the emergency department. What is the most appropriate next step?
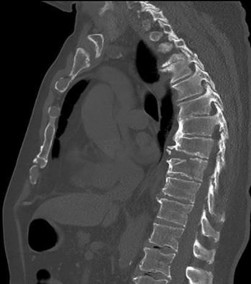

A
B
Figures 45a and 45b are the CT and MR spine images of an 82-year-old man who has a history of ankylosing spondylitis falls onto his back. He has no
neurologic deficits upon examination in the emergency department. What is the most appropriate next step?
1
Obtain upright radiographs
2
Thoracolumbar orthosis
3
Posterior stabilization and fusion
4
Laminectomy
Spinal fractures in patients with ankylosing spondylitis are unstable and generally necessitate surgical intervention. In a patient with a spinal fracture in the setting of ankylosing spondylitis, posterior instrumented fusion is an appropriate surgical procedure. Treatment with a thoracolumbar orthosis is not an option for patients with extension distraction injuries in the setting of an ankylosed spine because of risk for displacement. Similarly, simply checking upright radiographs is generally not advocated. Laminectomy alone is inappropriate for this patient because there is no cord compression and neurologic symptoms are absent. Stabilization is the treatment goal.
RECOMMENDED READINGS
[Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007 Apr 21;369(9570):1379-90. Review. PubMed PMID: 17448825.](http://www.ncbi.nlm.nih.gov/pubmed/17448825)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17448825)
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858) [Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. ](http://www.ncbi.nlm.nih.gov/pubmed/10432265)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432265) [Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. ](http://www.ncbi.nlm.nih.gov/pubmed/12296682)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12296682)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12296682)
RECOMMENDED READINGS
[Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007 Apr 21;369(9570):1379-90. Review. PubMed PMID: 17448825.](http://www.ncbi.nlm.nih.gov/pubmed/17448825)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17448825)
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858) [Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. ](http://www.ncbi.nlm.nih.gov/pubmed/10432265)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432265) [Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. ](http://www.ncbi.nlm.nih.gov/pubmed/12296682)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12296682)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12296682)
QUESTION 46
of 100
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of
A
B
C

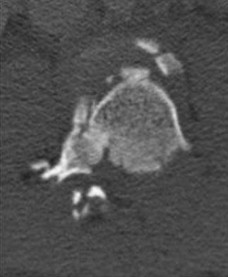

A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of
A
B
C
1
anterior reduction, stabilization, and fusion at L1-2.
2
anterior reduction, stabilization, and fusion at T12-L3.
3
posterior reduction, stabilization, and fusion at L1-2.
4
posterior reduction, stabilization, and fusion at T12-L4.
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
[Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[View](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15615508)
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
RECOMMENDED READINGS
[Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[View](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15615508)
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
QUESTION 47
of 100
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
1
Better clinical outcomes
2
Less blood loss
3
Less pseudarthrosis risk
4
Lower revision surgery rate
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
[Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. ](http://www.ncbi.nlm.nih.gov/pubmed/24981899)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24981899) [Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. ](http://www.ncbi.nlm.nih.gov/pubmed/22844053)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/22844053)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22844053)
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
[19411450/. ](http://www.ncbi.nlm.nih.gov/pubmed/19411450)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411450)
RESPONSES FOR QUESTIONS 48 THROUGH 50
1. Fracture displacement or subluxation leading to neurologic injury
2. Symptomatic epidural hematoma
3. Sepsis and death
4. Permanent nerve root injury and neurologic deficit
5. Loss of bowel or bladder control
6. Spinal cord injury
Select the complication listed above that most commonly is associated with the appropriate clinical scenario described below.
RECOMMENDED READINGS
[Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. ](http://www.ncbi.nlm.nih.gov/pubmed/24981899)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24981899) [Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. ](http://www.ncbi.nlm.nih.gov/pubmed/22844053)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/22844053)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22844053)
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
[19411450/. ](http://www.ncbi.nlm.nih.gov/pubmed/19411450)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19411450)
RESPONSES FOR QUESTIONS 48 THROUGH 50
1. Fracture displacement or subluxation leading to neurologic injury
2. Symptomatic epidural hematoma
3. Sepsis and death
4. Permanent nerve root injury and neurologic deficit
5. Loss of bowel or bladder control
6. Spinal cord injury
Select the complication listed above that most commonly is associated with the appropriate clinical scenario described below.
QUESTION 48
of 100
A 25-year-old man with a large central disk herniation at L4-5 with normal motor strength, perineal numbness, and difficulty urinating for 36 hours
A 25-year-old man with a large central disk herniation at L4-5 with normal motor strength, perineal numbness, and difficulty urinating for 36 hours
1
Fracture displacement or subluxation leading to neurologic injury
2
Symptomatic epidural hematoma
3
Sepsis and death
4
Permanent nerve root injury and neurologic deficit
5
Loss of bowel or bladder control
- Loss of bowel or bladder control
QUESTION 49
of 100
A 65-year-old man with ankylosing spondylitis has a fall from a standing height. He previously had minimal range of motion in his cervical spine, but now notices he is better able to extend his head. He is seen in the emergency department and released with a soft collar for use as needed.
A 65-year-old man with ankylosing spondylitis has a fall from a standing height. He previously had minimal range of motion in his cervical spine, but now notices he is better able to extend his head. He is seen in the emergency department and released with a soft collar for use as needed.
1
Fracture displacement or subluxation leading to neurologic injury
2
Symptomatic epidural hematoma
3
Sepsis and death
4
Permanent nerve root injury and neurologic deficit
5
Loss of bowel or bladder control
- Fracture displacement or subluxation leading to neurologic injury
QUESTION 50
of 100
A 74-year-old man with ankylosing spondylitis falls off a step stool and now has a minimally displaced T10-T11 extension-type fracture. He is initially treated with percutaneous pedicle screw fixation from T8-L1 and has good pain relief. The next day, however, he experiences increased back pain and loss of strength in his lower extremities.
A 74-year-old man with ankylosing spondylitis falls off a step stool and now has a minimally displaced T10-T11 extension-type fracture. He is initially treated with percutaneous pedicle screw fixation from T8-L1 and has good pain relief. The next day, however, he experiences increased back pain and loss of strength in his lower extremities.
1
Fracture displacement or subluxation leading to neurologic injury
2
Symptomatic epidural hematoma
3
Sepsis and death
4
Permanent nerve root injury and neurologic deficit
5
Loss of bowel or bladder control
Cauda equina syndrome, typically the result of severe central canal stenosis in the lower lumbar region, often is caused by a large central disk herniation. Symptoms include severe back or leg pain, perineal numbness, possible motor weakness, and initial urinary retention followed by an overflow incontinence. When bowel or bladder deficits are present, this is considered a surgical emergency because successful recovery is most likely if decompression occurs within the first 48 hours.
Ankylosing spondylitis can lead to progressive autofusion of the vertebrae and significant limitation in motion. Any sudden improvement in motion should be considered a fracture until proven otherwise. These fractures are commonly missed when using plain radiographs or even CT scan because minimal or no displacement often is noted. MR imaging can be useful to identify edema at
the fracture site. These fractures are typically very unstable and necessitate surgery to avoid displacement and potential neurologic injury.
Some fractures associated with ankylosing spondylitis can be effectively treated with percutaneous pedicle screw fixation. However, because of the highly vascular nature of some of these fractures, they pose risk for an epidural hematoma, potential neurologic deficit, and emergent decompression.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Mathews M, Bolesta MJ. Treatment of spinal fractures in ankylosing spondylitis. Orthopedics. 2013 Sep;36(9):e1203-8. doi: 10.3928/01477447-20130821-25. PubMed PMID: 24025014.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24025014)
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
[16/. PubMed PMID: 17224816. ](http://www.ncbi.nlm.nih.gov/pubmed/17224816)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17224816)
Ankylosing spondylitis can lead to progressive autofusion of the vertebrae and significant limitation in motion. Any sudden improvement in motion should be considered a fracture until proven otherwise. These fractures are commonly missed when using plain radiographs or even CT scan because minimal or no displacement often is noted. MR imaging can be useful to identify edema at
the fracture site. These fractures are typically very unstable and necessitate surgery to avoid displacement and potential neurologic injury.
Some fractures associated with ankylosing spondylitis can be effectively treated with percutaneous pedicle screw fixation. However, because of the highly vascular nature of some of these fractures, they pose risk for an epidural hematoma, potential neurologic deficit, and emergent decompression.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Mathews M, Bolesta MJ. Treatment of spinal fractures in ankylosing spondylitis. Orthopedics. 2013 Sep;36(9):e1203-8. doi: 10.3928/01477447-20130821-25. PubMed PMID: 24025014.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24025014)
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
[16/. PubMed PMID: 17224816. ](http://www.ncbi.nlm.nih.gov/pubmed/17224816)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17224816)
QUESTION 51
of 100
What is the chief mechanism of action of parathyroid hormone (PTH) in the treatment of patients with osteoporosis?
What is the chief mechanism of action of parathyroid hormone (PTH) in the treatment of patients with osteoporosis?
1
Reduces resorptive activity of osteoclasts
2
Inhibits receptor activator of nuclear factor kappa-B ligand
3
Stimulates osteoblastic bone formation
4
Acts as a selective estrogen modulator
Recombinant human PTH benefits patients with osteoporosis by stimulating osteoblastic bone formation and reducing osteoblastic apoptosis. Treatment reduces vertebral fractures by 65%. PTH analogs act similarly and reduce vertebral fractures by 47%. Bisphosphonates reduce the resorptive activity of
osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
RECOMMENDED READINGS
[Castro-Lionard K, Dargent-Molina P, Fermanian C, Gonthier R, Cassou B. Use of calcium supplements, vitamin D supplements and specific osteoporosis drugs among French women aged 75-85 years: patterns of use and associated factors. Drugs Aging. 2013 Dec;30(12):1029-38. doi: 10.1007/s40266-013-0121-9. PubMed PMID: 24114665. ](http://www.ncbi.nlm.nih.gov/pubmed/24114665)[View](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Papapoulos S, Makras P. Selection of antiresorptive or anabolic treatments for postmenopausal osteoporosis. Nat Clin Pract Endocrinol Metab. 2008 Sep;4(9):514-23. doi: 10.1038/ncpendmet0941. Review. PubMed PMID: 18714329. ](http://www.ncbi.nlm.nih.gov/pubmed/18714329)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18714329) [Zhang J, Delzell E, Curtis JR, Hooven F, Gehlbach SH, Anderson FA Jr, Saag KG. Use of pharmacologic agents for the primary prevention of osteoporosis among older women with low bone mass. Osteoporos Int. 2014 Jan;25(1):317-24. doi: 10.1007/s00198-013-2444-0. Epub 2013 Aug 28. PubMed PMID: 23982799. ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23982799)
osteoclasts and cause a dissociation of bone formation and resorption that favors bone formation and reduce vertebral fractures by 50% to 70%. Selective estrogen receptor modulators inhibit bone resorption and reduce vertebral fractures by 35%. Humanized monoclonal antibodies inhibit osteoclast formation and reduce vertebral fractures by 68%.
RECOMMENDED READINGS
[Castro-Lionard K, Dargent-Molina P, Fermanian C, Gonthier R, Cassou B. Use of calcium supplements, vitamin D supplements and specific osteoporosis drugs among French women aged 75-85 years: patterns of use and associated factors. Drugs Aging. 2013 Dec;30(12):1029-38. doi: 10.1007/s40266-013-0121-9. PubMed PMID: 24114665. ](http://www.ncbi.nlm.nih.gov/pubmed/24114665)[View](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24114665)
[Papapoulos S, Makras P. Selection of antiresorptive or anabolic treatments for postmenopausal osteoporosis. Nat Clin Pract Endocrinol Metab. 2008 Sep;4(9):514-23. doi: 10.1038/ncpendmet0941. Review. PubMed PMID: 18714329. ](http://www.ncbi.nlm.nih.gov/pubmed/18714329)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18714329) [Zhang J, Delzell E, Curtis JR, Hooven F, Gehlbach SH, Anderson FA Jr, Saag KG. Use of pharmacologic agents for the primary prevention of osteoporosis among older women with low bone mass. Osteoporos Int. 2014 Jan;25(1):317-24. doi: 10.1007/s00198-013-2444-0. Epub 2013 Aug 28. PubMed PMID: 23982799. ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23982799)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23982799)
QUESTION 52
of 100
A
B
Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?

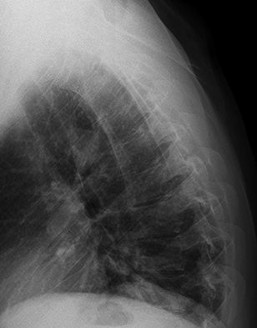
A
B
Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
1
Nonsteroidal medication and follow up as needed
2
Repeat radiographs in 1 week
3
MR imaging of the thoracic spine
4
Flexion-extension radiographs
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858)
[Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. ](http://www.ncbi.nlm.nih.gov/pubmed/8141015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8141015)
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858)
[Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. ](http://www.ncbi.nlm.nih.gov/pubmed/8141015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8141015)
QUESTION 53
of 100
A 70-year-old otherwise healthy woman is undergoing correction of thoracic kyphosis with spinal cord compression via a posterior approach. She receives an inhaled anesthetic, her mean arterial pressure is 93 mm Hg, and her core temperature is 37.2°C. Her spinal cord is being monitored with somatosensory-evoked potentials and transcranial motor-evoked potentials. She has very low amplitude and increased latency as detected by neurophysiologic monitoring. Which action should be taken?


A 70-year-old otherwise healthy woman is undergoing correction of thoracic kyphosis with spinal cord compression via a posterior approach. She receives an inhaled anesthetic, her mean arterial pressure is 93 mm Hg, and her core temperature is 37.2°C. Her spinal cord is being monitored with somatosensory-evoked potentials and transcranial motor-evoked potentials. She has very low amplitude and increased latency as detected by neurophysiologic monitoring. Which action should be taken?
1
A Stagnara wake-up test should be performed immediately.
2
The patient's mean arterial pressure should be increased immediately.
3
The anesthesia team should use propofol instead of isoflurane.
4
The patient's core temperature should be decreased to 35°C.
The use of halogenated inhaled anesthetic agents has been shown to abrogate the signals detected during neurophysiologic monitoring. Intravenous agents such as propofol should be used in favor of inhaled agents such as isoflurane and nitrous oxide. Neurophysiologic signals also can be dampened when hypotension and hypothermia are issues. In this case, the patient's mean arterial pressure and body temperature are within the range at which spinal cord blood flow and neurophysiologic monitoring may be optimized. A Stagnara wake-up test may be useful, but it poses risk. If there is another explanation for the patient's lack of signal, this test is not necessary.
RECOMMENDED READINGS
[Devlin VJ, Schwartz DM. Intraoperative neurophysiologic monitoring during spinal surgery. J Am Acad Orthop Surg. 2007 Sep;15(9):549-60. Review. PubMed PMID: 17761611. ](http://www.ncbi.nlm.nih.gov/pubmed/17761611)[View](http://www.ncbi.nlm.nih.gov/pubmed/17761611)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17761611)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17761611)
[Chen Z. The effects of isoflurane and propofol on intraoperative neurophysiological monitoring during spinal surgery. J Clin Monit Comput. 2004 Aug;18(4):303-8. PubMed PMID: 15779842. ](http://www.ncbi.nlm.nih.gov/pubmed/15779842)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15779842)
RECOMMENDED READINGS
[Devlin VJ, Schwartz DM. Intraoperative neurophysiologic monitoring during spinal surgery. J Am Acad Orthop Surg. 2007 Sep;15(9):549-60. Review. PubMed PMID: 17761611. ](http://www.ncbi.nlm.nih.gov/pubmed/17761611)[View](http://www.ncbi.nlm.nih.gov/pubmed/17761611)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17761611)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17761611)
[Chen Z. The effects of isoflurane and propofol on intraoperative neurophysiological monitoring during spinal surgery. J Clin Monit Comput. 2004 Aug;18(4):303-8. PubMed PMID: 15779842. ](http://www.ncbi.nlm.nih.gov/pubmed/15779842)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15779842)
QUESTION 54
of 100
A B
Figures 54a and 54b are the radiographs of a 21-year-old man who has a long history of thoracic back pain. His lumbar spine is asymptomatic. He has failed prolonged nonsurgical treatment. Surgical correction should consist of
A B
Figures 54a and 54b are the radiographs of a 21-year-old man who has a long history of thoracic back pain. His lumbar spine is asymptomatic. He has failed prolonged nonsurgical treatment. Surgical correction should consist of
1
anterior release and fusion at T4-10.
2
posterior instrumentation and fusion at T9-L5.
3
posterior instrumentation and fusion at T2-L2.
4
posterior instrumentation and fusion at T6-pelvis.
When planning surgical intervention for Scheuermann kyphosis, it is imperative that the instrumentation and fusion extend across the entirety of the deformity. Distally, this means extending across the first lordotic disk space. In this scenario, this disk is the L1-L2 disk, which means the fusion needs to extend to L2. Shorter and longer fusions are not necessary or appropriate.
RECOMMENDED READINGS
[Denis F, Sun EC, Winter RB. Incidence and risk factors for proximal and distal junctional kyphosis following surgical treatment for Scheuermann kyphosis: minimum five-year followup. Spine (Phila Pa 1976). 2009 Sep 15;34(20):E729-34. PubMed PMID: 19752692. ](http://www.ncbi.nlm.nih.gov/pubmed/19752692)[View](http://www.ncbi.nlm.nih.gov/pubmed/19752692)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19752692)
[Macagno AE, O'Brien MF. Thoracic and thoracolumbar kyphosis in adults. Spine (Phila Pa 1976). 2006 Sep 1;31(19 Suppl):S161-70. Review. PubMed PMID: 16946634. ](http://www.ncbi.nlm.nih.gov/pubmed/16946634)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/16946634)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16946634)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16946634)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 59
A 60-year-old woman has severe neck and back pain. She is relatively healthy but has diabetes and neuropathy involving her lower extremities. Her body mass index is 38. She has a history of spinal fusion performed by your colleague 3 years ago. At that time, she was treated for degenerative scoliosis of the lumbar spine with concomitant spinal stenosis. A 360-degree fusion was performed from L4-S1 with a posterior decompression from L2-S1 and a posterior instrumented fusion from T3 to the pelvis. On examination, she has reproducible pain and a visible kyphosis in the periscapular region. Neurologic examination findings are within normal limits, with the exception of lower-extremity dysesthesias related to her neuropathy. The patient states that she has been having progressive difficulty dressing herself and taking care of her apartment for several months. Plain radiographs and a standing scoliosis series demonstrate a solid fusion from the sacrum to T3 without evidence of hardware failure. There is focal collapse of the T2-T3 disk space and a proximal kyphosis involving the T2 vertebrae that is indicative of disk and ligamentous failure.
RECOMMENDED READINGS
[Denis F, Sun EC, Winter RB. Incidence and risk factors for proximal and distal junctional kyphosis following surgical treatment for Scheuermann kyphosis: minimum five-year followup. Spine (Phila Pa 1976). 2009 Sep 15;34(20):E729-34. PubMed PMID: 19752692. ](http://www.ncbi.nlm.nih.gov/pubmed/19752692)[View](http://www.ncbi.nlm.nih.gov/pubmed/19752692)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19752692)
[Macagno AE, O'Brien MF. Thoracic and thoracolumbar kyphosis in adults. Spine (Phila Pa 1976). 2006 Sep 1;31(19 Suppl):S161-70. Review. PubMed PMID: 16946634. ](http://www.ncbi.nlm.nih.gov/pubmed/16946634)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/16946634)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16946634)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16946634)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 59
A 60-year-old woman has severe neck and back pain. She is relatively healthy but has diabetes and neuropathy involving her lower extremities. Her body mass index is 38. She has a history of spinal fusion performed by your colleague 3 years ago. At that time, she was treated for degenerative scoliosis of the lumbar spine with concomitant spinal stenosis. A 360-degree fusion was performed from L4-S1 with a posterior decompression from L2-S1 and a posterior instrumented fusion from T3 to the pelvis. On examination, she has reproducible pain and a visible kyphosis in the periscapular region. Neurologic examination findings are within normal limits, with the exception of lower-extremity dysesthesias related to her neuropathy. The patient states that she has been having progressive difficulty dressing herself and taking care of her apartment for several months. Plain radiographs and a standing scoliosis series demonstrate a solid fusion from the sacrum to T3 without evidence of hardware failure. There is focal collapse of the T2-T3 disk space and a proximal kyphosis involving the T2 vertebrae that is indicative of disk and ligamentous failure.
QUESTION 55
of 100
The patient asks why the proximal kyphosis occurred. You indicate that she has several risk factors for this condition, including
The patient asks why the proximal kyphosis occurred. You indicate that she has several risk factors for this condition, including
1
her age, fusion to the sacrum, and upper instrumented vertebra at T3.
2
her age, 360-degree fusion, and obesity.
3
diabetes, history of neuropathy, and pelvic instrumentation.
4
upper instrumented vertebra at T3, obesity, and diabetes.
- her age, fusion to the sacrum, and upper instrumented vertebra at T3.
QUESTION 56
of 100
Considering her current symptoms, history, and examination findings, you believe that the most efficacious means with which to address this patient's junctional kyphosis is
Considering her current symptoms, history, and examination findings, you believe that the most efficacious means with which to address this patient's junctional kyphosis is
1
cervico-thoracic-lumbosacral orthosis to immobilize the kyphosed segment.
2
removal of the posterior instrumentation because she has had a successful fusion.
3
anteroposterior instrumented fusion at T2-3 to address the collapsed interspace.
4
revision posterior instrumentation with extension of the fusion to T1 to span the area of junctional kyphosis.
- revision posterior instrumentation with extension of the fusion to T1 to span the area of junctional kyphosis.
QUESTION 57
of 100
What are this patient's risk factors for postsurgical infection?
What are this patient's risk factors for postsurgical infection?
1
Presence of posterior spinal instrumentation
2
Anterior approach performed during the index procedure
3
Diabetes and obesity
4
Surgery performed in the thoracic spine
- Diabetes and obesity
QUESTION 58
of 100
Which complication is most frequently encountered after revision surgery to treat junctional kyphosis?
Which complication is most frequently encountered after revision surgery to treat junctional kyphosis?
1
Deep surgical-site infection
2
Pseudoarthrosis
3
Neurological injury
4
Adjacent segment degeneration
- Adjacent segment degeneration
QUESTION 59
of 100
During the revision surgical procedure, thoracic pedicle screws are placed. Following placement, triggered electromyography (EMG) is performed by stimulating the pedicle screw heads. During testing the right T2 pedicle screw head returns a threshold of 2 mA. What does this reading indicate?
During the revision surgical procedure, thoracic pedicle screws are placed. Following placement, triggered electromyography (EMG) is performed by stimulating the pedicle screw heads. During testing the right T2 pedicle screw head returns a threshold of 2 mA. What does this reading indicate?
1
The right T2 pedicle screw is well seated within the pedicle.
2
The right T2 pedicle screw has breached the pedicle wall and has violated the costovertebral junction.
3
There is a breach in the right T2 pedicle wall, but the screw is not in contact with a neural structure.
4
There is a breach in the right T2 pedicle and the screw is in contact with a neural structure.
This patient has developed a proximal junctional kyphosis following a long posterior fusion performed for treatment of degenerative lumbar scoliosis. Risk factors for proximal junctional kyphosis in the setting of instrumented fusions performed for degenerative scoliosis include advanced age, 360-
degree fusions, extension of fusion constructs to the sacrum, and upper instrumented vertebrae at the level of T1-3. The patient's junctional kyphosis is attributable to failure of the disk and ligamentous structures at T2-3 and would be graded as type I using the classification system of Yagi and associates. Most symptomatic proximal junctional kyphoses are treated with posterior extension of the fusion construct to a more proximal level spanning the kyphosed region. The use of orthoses or simple removal of instrumentation is unlikely to substantively impact symptoms or address the proximal kyphosis. Diabetes and obesity are known factors that increase risk for postsurgical infection following a spine fusion procedure. The most frequent complication following revision surgery for proximal junctional kyphosis, however, is the need for further surgery. In the study by Yagi and associates, 48% of patients who underwent revision surgery for proximal kyphosis developed further adjacent segment degeneration. In the proximal thoracic spine, where the pedicle may be narrow, triggered EMG testing of inserted pedicle screws may be used to assess for violation of the pedicle wall during insertion. In the setting of triggered EMG, thresholds exceeding 10 mA indicate a well-placed pedicle screw. Thresholds lower than 4 mA to 6 mA indicate that a screw is directly contacting a neural structure. Thresholds between 9 mA and 10 mA suggest that a breach of the pedicle may be present, but the screw is not contacting a neural structure.
RECOMMENDED READINGS
[Yagi M, Rahm M, Gaines R, Maziad A, Ross T, Kim HJ, Kebaish K, Boachie-Adjei O; Complex Spine Study Group. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity.Spine (Phila Pa 1976). 2014 May 1;39(10):E607-14. doi: 10.1097/BRS.0000000000000266. PubMed PMID: 24525992. ](http://www.ncbi.nlm.nih.gov/pubmed/24525992)[View](http://www.ncbi.nlm.nih.gov/pubmed/24525992)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24525992)
Cammarata M, Aubin CÉ, Wang X, Mac-Thiong JM. Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine (Phila Pa 1976). 2014 Apr 15;39(8):E500-7. doi: 10.1097/BRS.0000000000000222. PubMed
[PMID: 24480964. ](http://www.ncbi.nlm.nih.gov/pubmed/24480964)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24480964)
[Kim HJ, Lenke LG, Shaffrey CI, Van Alstyne EM, Skelly AC. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S144-64. doi: 10.1097/BRS.0b013e31826d611b. PubMed PMID: 22885829. ](http://www.ncbi.nlm.nih.gov/pubmed/22885829)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22885829) Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
[23578986/. ](http://www.ncbi.nlm.nih.gov/pubmed/23578986)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23578986)
Schoenfeld AJ. Spine infections. In: Cannada L, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2014: 737-747.
Schoenfeld AJ, Bono CM. Instrumented lumbar fusion. In: Flatow E, Colvin AC, eds. Atlas of Essential Orthopaedic Procedures. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2013: 611-616.
degree fusions, extension of fusion constructs to the sacrum, and upper instrumented vertebrae at the level of T1-3. The patient's junctional kyphosis is attributable to failure of the disk and ligamentous structures at T2-3 and would be graded as type I using the classification system of Yagi and associates. Most symptomatic proximal junctional kyphoses are treated with posterior extension of the fusion construct to a more proximal level spanning the kyphosed region. The use of orthoses or simple removal of instrumentation is unlikely to substantively impact symptoms or address the proximal kyphosis. Diabetes and obesity are known factors that increase risk for postsurgical infection following a spine fusion procedure. The most frequent complication following revision surgery for proximal junctional kyphosis, however, is the need for further surgery. In the study by Yagi and associates, 48% of patients who underwent revision surgery for proximal kyphosis developed further adjacent segment degeneration. In the proximal thoracic spine, where the pedicle may be narrow, triggered EMG testing of inserted pedicle screws may be used to assess for violation of the pedicle wall during insertion. In the setting of triggered EMG, thresholds exceeding 10 mA indicate a well-placed pedicle screw. Thresholds lower than 4 mA to 6 mA indicate that a screw is directly contacting a neural structure. Thresholds between 9 mA and 10 mA suggest that a breach of the pedicle may be present, but the screw is not contacting a neural structure.
RECOMMENDED READINGS
[Yagi M, Rahm M, Gaines R, Maziad A, Ross T, Kim HJ, Kebaish K, Boachie-Adjei O; Complex Spine Study Group. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity.Spine (Phila Pa 1976). 2014 May 1;39(10):E607-14. doi: 10.1097/BRS.0000000000000266. PubMed PMID: 24525992. ](http://www.ncbi.nlm.nih.gov/pubmed/24525992)[View](http://www.ncbi.nlm.nih.gov/pubmed/24525992)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24525992)
Cammarata M, Aubin CÉ, Wang X, Mac-Thiong JM. Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine (Phila Pa 1976). 2014 Apr 15;39(8):E500-7. doi: 10.1097/BRS.0000000000000222. PubMed
[PMID: 24480964. ](http://www.ncbi.nlm.nih.gov/pubmed/24480964)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24480964)
[Kim HJ, Lenke LG, Shaffrey CI, Van Alstyne EM, Skelly AC. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S144-64. doi: 10.1097/BRS.0b013e31826d611b. PubMed PMID: 22885829. ](http://www.ncbi.nlm.nih.gov/pubmed/22885829)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22885829) Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
[23578986/. ](http://www.ncbi.nlm.nih.gov/pubmed/23578986)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23578986)
Schoenfeld AJ. Spine infections. In: Cannada L, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2014: 737-747.
Schoenfeld AJ, Bono CM. Instrumented lumbar fusion. In: Flatow E, Colvin AC, eds. Atlas of Essential Orthopaedic Procedures. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2013: 611-616.
QUESTION 60
of 100
A
B
Figures 60a and 60b are the postmyelography CT images of a 62-year-old man who has had low-back and bilateral lower-extremity pain. His pain began approximately 1 year ago and there was no precipitating event. The location of the pain is in the lower lumbar region in the midline and it radiates into the buttocks and thighs bilaterally. The pain is exacerbated by standing and walking and relieved by forward spine flexion. He reports no pain while sitting or lying supine. Upright radiographs demonstrate 4 mm of anterolisthesis of L4 on L5. What is the most appropriate surgical procedure?


A
B
Figures 60a and 60b are the postmyelography CT images of a 62-year-old man who has had low-back and bilateral lower-extremity pain. His pain began approximately 1 year ago and there was no precipitating event. The location of the pain is in the lower lumbar region in the midline and it radiates into the buttocks and thighs bilaterally. The pain is exacerbated by standing and walking and relieved by forward spine flexion. He reports no pain while sitting or lying supine. Upright radiographs demonstrate 4 mm of anterolisthesis of L4 on L5. What is the most appropriate surgical procedure?
1
Microdiskectomy
2
Posterior decompression
3
Posterior decompression and fusion
4
Anterior lumbar interbody fusion
This patient radiographically has L4-5 degenerative stenosis and a low-grade spondylolisthesis. The axial images demonstrate a gap in the facet joint, more on the left than the right, which is highly suggestive of dynamic instability. Thus, this patient would most benefit from a laminectomy and fusion of L4-5. A microdiskectomy would not be helpful as this patient does not have a disk herniation. Patients undergoing posterior decompression alone experience an unacceptably high rate of recurrent stenosis and/or progression of spondylolisthesis. Early studies demonstrated that adding an intertransverse process fusion to posterior decompression significantly improved clinical outcomes. Anterior interbody fusion likely will not decompress the spinal canal sufficiently, though there is some thought that indirect decompression can be effective in some cases.
RECOMMENDED READINGS
[Frymoyer JW. Degenerative Spondylolisthesis: Diagnosis and Treatment. J Am Acad Orthop Surg. 1994 Jan;2(1):9-15. PubMed PMID: 10708989. Majid K, Fischgrund JS. Degenerative lumbar spondylolisthesis: trends in management. J Am Acad Orthop Surg. 2008 Apr;16(4):208-15. Review. PubMed PMID: 18390483. ](http://www.ncbi.nlm.nih.gov/pubmed/18390483)[View ](http://www.ncbi.nlm.nih.gov/pubmed/18390483)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18390483)
Carlisle E, Fischgrund JS. Lumbar spinal stenosis and degenerative spondylolisthesis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006: 299-317.
Puschak TJ, Sasso RC. Spondylolysis-spondylolisthesis. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:553-563.
RECOMMENDED READINGS
[Frymoyer JW. Degenerative Spondylolisthesis: Diagnosis and Treatment. J Am Acad Orthop Surg. 1994 Jan;2(1):9-15. PubMed PMID: 10708989. Majid K, Fischgrund JS. Degenerative lumbar spondylolisthesis: trends in management. J Am Acad Orthop Surg. 2008 Apr;16(4):208-15. Review. PubMed PMID: 18390483. ](http://www.ncbi.nlm.nih.gov/pubmed/18390483)[View ](http://www.ncbi.nlm.nih.gov/pubmed/18390483)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18390483)
Carlisle E, Fischgrund JS. Lumbar spinal stenosis and degenerative spondylolisthesis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006: 299-317.
Puschak TJ, Sasso RC. Spondylolysis-spondylolisthesis. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:553-563.
QUESTION 61
of 100
A 78-year-old man with ankylosing spondylitis sustains a minor fall. Shortly afterward he experiences sudden worsening of his chronic back pain and is brought to the emergency department by his caregiver. Radiographs and a CT scan of the spine do not show a clear fracture. What is the most appropriate next step?
A 78-year-old man with ankylosing spondylitis sustains a minor fall. Shortly afterward he experiences sudden worsening of his chronic back pain and is brought to the emergency department by his caregiver. Radiographs and a CT scan of the spine do not show a clear fracture. What is the most appropriate next step?
1
Nonsteroidal anti-inflammatory drugs
2
MRI of the spine
3
CT myelography
4
Flexion-extension plain films
Patients with ankylosing spondylitis are at high risk for occult fractures after low-energy injuries. Although radiographs and a CT scan do not demonstrate a spinal fracture in this patient, high risk for an unstable occult fracture necessitates further imaging with MRI to ensure that no fractures are missed. Although a CT scan is typically the primary imaging modality for workup of spine injuries in similar patients, CT and MRI complement each other and each detects fractures that are missed using the other modality. A CT myelogram might detect cord or root compression but would not aid in the diagnosis of an occult fracture. Nonsteroidal anti-inflammatory drugs are first-line treatment for idiopathic low-back pain. In a patient with ankylosing spondylitis at high risk for fracture, further workup is needed to rule out an occult fracture. Flexion and extension radiographs of the spine are inferior to MRI for evaluating occult fractures and ligamentous injuries. The primary concern for this patient remains an unstable spinal fracture, which necessitates an MRI of the spine before initiating a workup for other possible causes of his back pain.
RECOMMENDED READINGS
[Duane TM, Cross J, Scarcella N, Wolfe LG, Mayglothling J, Aboutanos MB, Whelan JF, Malhotra AK, Ivatury RR. Flexion-extension cervical spine plain films compared with MRI in the diagnosis of ligamentous injury. Am Surg. 2010 Jun;76(6):595-8. PubMed PMID: 20583514. ](http://www.ncbi.nlm.nih.gov/pubmed/20583514)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20583514)
[Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. ](http://www.ncbi.nlm.nih.gov/pubmed/12296682)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12296682)
Koivikko MP, Koskinen SK. MRI of cervical spine injuries complicating ankylosing spondylitis. Skeletal Radiol. 2008 Sep;37(9):813-9. doi: 10.1007/s00256-008-0484-x. Epub 2008 Apr
[18/. PubMed PMID: 18421455. ](http://www.ncbi.nlm.nih.gov/pubmed/18421455)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18421455)
[Wang YF, Teng MM, Chang CY, Wu HT, Wang ST. Imaging manifestations of spinal fractures in ankylosing spondylitis. AJNR Am J Neuroradiol. 2005 Sep;26(8):2067-76. PubMed PMID: 16155161. ](http://www.ncbi.nlm.nih.gov/pubmed/16155161)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16155161)
[Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[View ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18791749)
RECOMMENDED READINGS
[Duane TM, Cross J, Scarcella N, Wolfe LG, Mayglothling J, Aboutanos MB, Whelan JF, Malhotra AK, Ivatury RR. Flexion-extension cervical spine plain films compared with MRI in the diagnosis of ligamentous injury. Am Surg. 2010 Jun;76(6):595-8. PubMed PMID: 20583514. ](http://www.ncbi.nlm.nih.gov/pubmed/20583514)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20583514)
[Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. ](http://www.ncbi.nlm.nih.gov/pubmed/12296682)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12296682)
Koivikko MP, Koskinen SK. MRI of cervical spine injuries complicating ankylosing spondylitis. Skeletal Radiol. 2008 Sep;37(9):813-9. doi: 10.1007/s00256-008-0484-x. Epub 2008 Apr
[18/. PubMed PMID: 18421455. ](http://www.ncbi.nlm.nih.gov/pubmed/18421455)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18421455)
[Wang YF, Teng MM, Chang CY, Wu HT, Wang ST. Imaging manifestations of spinal fractures in ankylosing spondylitis. AJNR Am J Neuroradiol. 2005 Sep;26(8):2067-76. PubMed PMID: 16155161. ](http://www.ncbi.nlm.nih.gov/pubmed/16155161)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16155161)
[Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[View ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18791749)
QUESTION 62
of 100
A
B
C
Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?
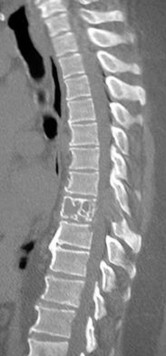

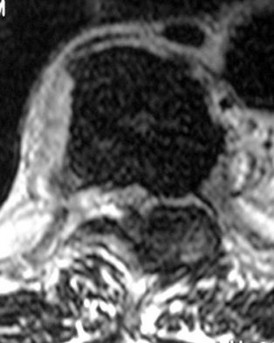
A
B
C
Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?
1
Thoracic tumor; CT-guided biopsy
2
Thoracic tumor; 3-phase bone scan
3
Thoracic discitis and osteomyelitis; CT-guided biopsy
4
Thoracic discitis and osteomyelitis; tagged white blood cell scan
The sagittal T2-weighted and axial T2-weighted images show a lesion within the T8 vertebral body that involves the posterior elements. There is an associated epidural component that results in compression of the spinal cord. The sagittal reconstructed CT image shows a lytic lesion within the T8 vertebral body. This pattern of vertebral body involvement with preservation
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
[Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. ](http://www.ncbi.nlm.nih.gov/pubmed/16304794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16304794)
[White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[View](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17030592)
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
[Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. ](http://www.ncbi.nlm.nih.gov/pubmed/16304794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16304794)
[White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[View](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17030592)
QUESTION 63
of 100
Misplaced pedicle screws are the most common complication associated with pedicle screw instrumentation. Many physicians use continuous electromyography (EMG) monitoring and direct stimulation of the screw to produce a peripheral EMG response. Which EMG stimulation minimum threshold indicates an accurately placed pedicle screw?
Misplaced pedicle screws are the most common complication associated with pedicle screw instrumentation. Many physicians use continuous electromyography (EMG) monitoring and direct stimulation of the screw to produce a peripheral EMG response. Which EMG stimulation minimum threshold indicates an accurately placed pedicle screw?
1
Higher than 20 mA
2
Higher than 15 mA
3
Higher than 10 mA
4
5 to 10 mA
A threshold of 15 mA or higher provides 98% confidence in accuracy of pedicle screw placement. If the EMG stimulation threshold is lower than 4 mA to 6 mA, the screw likely is in contact with the nerve root or dura. A threshold lower than 8 mA to 10 mA is associated with a breach in the pedicle cortex.
RECOMMENDED READINGS
Shen FH, Shaffrey CI, eds. Arthritis and Arthroplasty: The Spine. Philadelphia, PA: Saunders; 2010:141.
[Glassman SD, Dimar JR, Puno RM, Johnson JR, Shields CB, Linden RD. A prospective analysis of intraoperative electromyographic monitoring of pedicle screw placement with computed tomographic scan confirmation. Spine (Phila Pa 1976). 1995 Jun 15;20(12):1375-9. PubMed PMID: 7676335. ](http://www.ncbi.nlm.nih.gov/pubmed/7676335)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7676335)
RECOMMENDED READINGS
Shen FH, Shaffrey CI, eds. Arthritis and Arthroplasty: The Spine. Philadelphia, PA: Saunders; 2010:141.
[Glassman SD, Dimar JR, Puno RM, Johnson JR, Shields CB, Linden RD. A prospective analysis of intraoperative electromyographic monitoring of pedicle screw placement with computed tomographic scan confirmation. Spine (Phila Pa 1976). 1995 Jun 15;20(12):1375-9. PubMed PMID: 7676335. ](http://www.ncbi.nlm.nih.gov/pubmed/7676335)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7676335)
QUESTION 64
of 100
What is the most significant benefit of percutaneous transforaminal lumbar interbody fusion (TLIF) vs open posterior lumbar interbody fusion (PLIF)?
What is the most significant benefit of percutaneous transforaminal lumbar interbody fusion (TLIF) vs open posterior lumbar interbody fusion (PLIF)?
1
Preservation of the paraspinal muscle sleeve
2
Higher fusion rate
3
More measurable intraoperative blood loss
4
Improved ability to evacuate the disk space
Humphreys and associates in a retrospective review of TLIF vs PLIF found fusion rates, surgical time, and length of hospital stay were similar with both procedures. The only benefits associated with TLIF were less blood loss and preservation of the paraspinal muscle sleeve. Manos and associates in a cadaver study found no difference in the volume of disk material evacuated or the area of endplate exposed in either procedure.
RECOMMENDED READINGS
[Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001 Mar 1;26(5):567-71. PubMed PMID: 11242386. ](http://www.ncbi.nlm.nih.gov/pubmed/11242386)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11242386)
Manos R, Sukovich W, Weistroffer J: Transforaminal lumbar interbody fusion: Minimally invasive versus open disc excision and endplate preparation. Presented at the 12th International Meeting of Advanced Spine Techniques, Banff, Alberta, Canada, July 7-9, 2005.
RECOMMENDED READINGS
[Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001 Mar 1;26(5):567-71. PubMed PMID: 11242386. ](http://www.ncbi.nlm.nih.gov/pubmed/11242386)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11242386)
Manos R, Sukovich W, Weistroffer J: Transforaminal lumbar interbody fusion: Minimally invasive versus open disc excision and endplate preparation. Presented at the 12th International Meeting of Advanced Spine Techniques, Banff, Alberta, Canada, July 7-9, 2005.
QUESTION 65
of 100
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?
1
Anterior lumbar interbody fusion L4-5
2
L4-5 hemilaminotomy and diskectomy
3
Lumbar laminectomy L4-L5 posterior fusion
4
Lumbar laminectomy at L4-5
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
[Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487505)
[Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. ](http://www.ncbi.nlm.nih.gov/pubmed/2071615)[View](http://www.ncbi.nlm.nih.gov/pubmed/2071615)[ ](http://www.ncbi.nlm.nih.gov/pubmed/2071615)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2071615)
[Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. ](http://www.ncbi.nlm.nih.gov/pubmed/4089657)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4089657)
RESPONSES FOR QUESTIONS 66 THROUGH 69
1. Deep surgical-site infection
2. Adjacent segment degeneration
3. Pressure ulcers
4. Iatrogenic neurologic injury
5. Incidental durotomy
6. Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
[Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487505)
[Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. ](http://www.ncbi.nlm.nih.gov/pubmed/2071615)[View](http://www.ncbi.nlm.nih.gov/pubmed/2071615)[ ](http://www.ncbi.nlm.nih.gov/pubmed/2071615)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2071615)
[Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. ](http://www.ncbi.nlm.nih.gov/pubmed/4089657)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4089657)
RESPONSES FOR QUESTIONS 66 THROUGH 69
1. Deep surgical-site infection
2. Adjacent segment degeneration
3. Pressure ulcers
4. Iatrogenic neurologic injury
5. Incidental durotomy
6. Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
QUESTION 66
of 100
A 63-year-old woman who was treated with decompression and instrumented L4-L5 interbody fusion for degenerative spondylolisthesis demonstrates solid fusion on radiographs.
A 63-year-old woman who was treated with decompression and instrumented L4-L5 interbody fusion for degenerative spondylolisthesis demonstrates solid fusion on radiographs.
1
Deep surgical-site infection
2
Adjacent segment degeneration
3
Pressure ulcers
4
Iatrogenic neurologic injury
5
Incidental durotomy
- Adjacent segment degeneration
QUESTION 67
of 100
A 28-year-old obtunded man with a T12 burst fracture is treated in a thoracolumbosacral orthosis.
A 28-year-old obtunded man with a T12 burst fracture is treated in a thoracolumbosacral orthosis.
1
Deep surgical-site infection
2
Adjacent segment degeneration
3
Pressure ulcers
4
Iatrogenic neurologic injury
5
Incidental durotomy
- Pressure ulcers
QUESTION 68
of 100
A 42-year-old man with an L1 burst fracture, no neurologic deficit, and evidence of disruption of the posterior ligamentous complex as observed on MRI is treated with percutaneous stabilization without fusion.
A 42-year-old man with an L1 burst fracture, no neurologic deficit, and evidence of disruption of the posterior ligamentous complex as observed on MRI is treated with percutaneous stabilization without fusion.
1
Deep surgical-site infection
2
Adjacent segment degeneration
3
Pressure ulcers
4
Iatrogenic neurologic injury
5
Incidental durotomy
- Hardware failure
QUESTION 69
of 100
A 46-year-old man with a sacral chordoma is treated with sacrectomy.
A 46-year-old man with a sacral chordoma is treated with sacrectomy.
1
Deep surgical-site infection
2
Adjacent segment degeneration
3
Pressure ulcers
4
Iatrogenic neurologic injury
5
Incidental durotomy
Complications frequently occur following treatment for spinal disorders. Postsurgical morbidity may range from minor complications such as urinary tract infection to death. Wound infections are among the most commonly encountered complications following any surgical intervention; however, their incidence after spine surgery has been reported to be in the range of only 1% to 6%. Meanwhile, risk for adjacent segment degeneration, particularly following a fusion procedure performed with an interbody device, has been documented as high as 30%. Pressure ulcers can occur when spinal injuries are treated with rigid orthoses, especially in individuals who are immobile. Risk for pressure sores and decubiti is further elevated in patients who are obtunded and cannot communicate regarding pain levels and their need to mobilize. Hardware failure may occur following any instrumented spine procedure, but risk for this complication is elevated in the event of pseudarthrosis or in settings in which no fusion is performed.
In the recent work of Lee and associates, hardware failure was the only complication encountered among patients who were treated with percutaneous stabilization without fusion for thoracolumbar burst fractures. Similarly, iatrogenic neurologic injury may transpire in the setting of any spinal intervention (its incidence is rare). For example, in a large cohort of
more than 10000 patients undergoing surgical treatment for spondylolisthesis, acute neurologic injury was reported in only 0.8% of cases. Postsurgical wound infection, although relatively rare in cases of elective spine surgery, is common following large tumor resection such as sacrectomy performed for treatment of chordomas.
RECOMMENDED READINGS
[Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. ](http://www.ncbi.nlm.nih.gov/pubmed/24668350)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24668350)
Bransford RJ, Morgan RA. Thoracolumbar trauma. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:373-385.
[Lee JK, Jang JW, Kim TW, Kim TS, Kim SH, Moon SJ. Percutaneous short-segment pedicle screw placement without fusion in the treatment of thoracolumbar burst fractures: is it effective? comparative study with open short-segment pedicle screw fixation with posterolateral fusion. Acta Neurochir (Wien). 2013 Dec;155(12):2305-12; discussion 2312. doi: 10.1007/s00701-013-1859-x. Epub 2013 Sep 10. PubMed PMID: 24018981. ](http://www.ncbi.nlm.nih.gov/pubmed/24018981)[View](http://www.ncbi.nlm.nih.gov/pubmed/24018981)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24018981)
Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
[23578986/. ](http://www.ncbi.nlm.nih.gov/pubmed/23578986)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23578986)
[Sansur CA, Reames DL, Smith JS, Hamilton DK, Berven SH, Broadstone PA, Choma TJ, Goytan MJ, Noordeen HH, Knapp DR Jr, Hart RA, Zeller RD, Donaldson WF 3rd, Polly DW Jr, Perra JH, Boachie-Adjei O, Shaffrey CI. Morbidity and mortality in the surgical treatment of 10,242 adults with spondylolisthesis. J Neurosurg Spine. 2010 Nov;13(5):589-93. doi: 10.3171/2010.5.SPINE09529. PubMed PMID: 21039149. ](http://www.ncbi.nlm.nih.gov/pubmed/21039149)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/21039149)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21039149)
Dubory A, Missenard G, Lambert B, Court C. "En bloc" resection of sacral chordomas by combined anterior and posterior surgical approach: a monocentric retrospective review about 29 cases. Eur Spine J. 2014 Sep;23(9):1940-8. doi: 10.1007/s00586-014-3196-z. Epub 2014
[Jan 28. PubMed PMID: 24469886. ](http://www.ncbi.nlm.nih.gov/pubmed/24469886)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24469886)
In the recent work of Lee and associates, hardware failure was the only complication encountered among patients who were treated with percutaneous stabilization without fusion for thoracolumbar burst fractures. Similarly, iatrogenic neurologic injury may transpire in the setting of any spinal intervention (its incidence is rare). For example, in a large cohort of
more than 10000 patients undergoing surgical treatment for spondylolisthesis, acute neurologic injury was reported in only 0.8% of cases. Postsurgical wound infection, although relatively rare in cases of elective spine surgery, is common following large tumor resection such as sacrectomy performed for treatment of chordomas.
RECOMMENDED READINGS
[Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. ](http://www.ncbi.nlm.nih.gov/pubmed/24668350)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24668350)
Bransford RJ, Morgan RA. Thoracolumbar trauma. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:373-385.
[Lee JK, Jang JW, Kim TW, Kim TS, Kim SH, Moon SJ. Percutaneous short-segment pedicle screw placement without fusion in the treatment of thoracolumbar burst fractures: is it effective? comparative study with open short-segment pedicle screw fixation with posterolateral fusion. Acta Neurochir (Wien). 2013 Dec;155(12):2305-12; discussion 2312. doi: 10.1007/s00701-013-1859-x. Epub 2013 Sep 10. PubMed PMID: 24018981. ](http://www.ncbi.nlm.nih.gov/pubmed/24018981)[View](http://www.ncbi.nlm.nih.gov/pubmed/24018981)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24018981)
Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
[23578986/. ](http://www.ncbi.nlm.nih.gov/pubmed/23578986)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23578986)
[Sansur CA, Reames DL, Smith JS, Hamilton DK, Berven SH, Broadstone PA, Choma TJ, Goytan MJ, Noordeen HH, Knapp DR Jr, Hart RA, Zeller RD, Donaldson WF 3rd, Polly DW Jr, Perra JH, Boachie-Adjei O, Shaffrey CI. Morbidity and mortality in the surgical treatment of 10,242 adults with spondylolisthesis. J Neurosurg Spine. 2010 Nov;13(5):589-93. doi: 10.3171/2010.5.SPINE09529. PubMed PMID: 21039149. ](http://www.ncbi.nlm.nih.gov/pubmed/21039149)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/21039149)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21039149)
Dubory A, Missenard G, Lambert B, Court C. "En bloc" resection of sacral chordomas by combined anterior and posterior surgical approach: a monocentric retrospective review about 29 cases. Eur Spine J. 2014 Sep;23(9):1940-8. doi: 10.1007/s00586-014-3196-z. Epub 2014
[Jan 28. PubMed PMID: 24469886. ](http://www.ncbi.nlm.nih.gov/pubmed/24469886)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24469886)
QUESTION 70
of 100
An awake and alert patient with neck pain arrives at the emergency department after an automobile crash. Upon examination he is weak in the left deltoid and biceps muscles (3/5 strength). CT scans performed 2 hours after admission are shown in Figures 70a and 70b. His weakness deteriorates
to 1/5 strength in the upper and lower extremities. What is the most appropriate treatment?
A
B
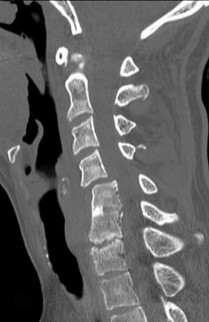

An awake and alert patient with neck pain arrives at the emergency department after an automobile crash. Upon examination he is weak in the left deltoid and biceps muscles (3/5 strength). CT scans performed 2 hours after admission are shown in Figures 70a and 70b. His weakness deteriorates
to 1/5 strength in the upper and lower extremities. What is the most appropriate treatment?
A
B
1
Immediate closed reduction in the intensive care unit while the patient is awake
2
Posterior spinal laminectomy and fusion with instrumentation
3
Anterior cervical diskectomy, corpectomy, and plating
4
High-dose methylprednisolone
Facet subluxation reduction may be performed in awake patients. Posterior spinal laminectomy and fusion can result in worsening neurologic status and is not recommended in this setting. Generally, corpectomy in the setting of facet subluxation is not recommended because it does not facilitate reduction or fully alleviate spinal cord compression. High-dose steroid use is not supported by current literature.
RECOMMENDED READINGS
[Fehlings MG, Perrin RG. The timing of surgical intervention in the treatment of spinal cord injury: a systematic review of recent clinical evidence. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S28-35; discussion S36. Review. PubMed PMID: 16685233. ](http://www.ncbi.nlm.nih.gov/pubmed/16685233)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/16685233)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16685233)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685233)
[Lee AS, MacLean JC, Newton DA. Rapid traction for reduction of cervical spine dislocations. J Bone Joint Surg Br. 1994 May;76(3):352-6. PubMed PMID: 8175833.](http://www.ncbi.nlm.nih.gov/pubmed/8175833)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/8175833)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8175833)
RECOMMENDED READINGS
[Fehlings MG, Perrin RG. The timing of surgical intervention in the treatment of spinal cord injury: a systematic review of recent clinical evidence. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S28-35; discussion S36. Review. PubMed PMID: 16685233. ](http://www.ncbi.nlm.nih.gov/pubmed/16685233)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/16685233)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16685233)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685233)
[Lee AS, MacLean JC, Newton DA. Rapid traction for reduction of cervical spine dislocations. J Bone Joint Surg Br. 1994 May;76(3):352-6. PubMed PMID: 8175833.](http://www.ncbi.nlm.nih.gov/pubmed/8175833)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/8175833)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8175833)
QUESTION 71
of 100
Pain emanating from the sacroiliac (SI) joint is best identified by which of the following maneuvers?

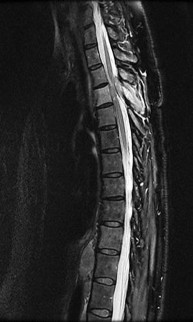
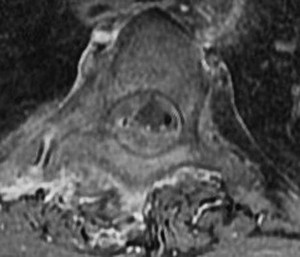
Pain emanating from the sacroiliac (SI) joint is best identified by which of the following maneuvers?
1
Reproduction of pain with the Gaenslen test
2
Reproduction of pain with the SI joint compression test
3
Presence of bone marrow edema on short tau inversion recovery sequence of MR images.
4
More than 75% pain reduction following fluoroscopically guided SI joint injection.
Though no gold standard exists, a reduction of concordant pain by at least 75 to 80% following an intra-articular, image-guided anesthetic injection is considered to be the most reliable method of identifying the SI joint as the cause of a patient's pain. Although provocation tests including the Gaenslen test, the compression test, thigh thrust, and Yeoman test are commonly used and can be helpful in diagnosing non-specific SI joint pain, individually they are not as reliable as the response to a diagnostic, anesthetic injection. Of note, the combination of all 4 manuevers has proven to be more useful than any one individual test. An MRI of the SI joint showing bony erosion and bone marrow edema suggests inflammatory arthritis and may not necessarily be associated with pain.
RECOMMENDED READINGS
Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine
[J. 2007 Oct;16(10):1539-50. Epub 2007 Jun 14. PubMed PMID: 17566796. ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17566796)
Visser LH, Nijssen PG, Tijssen CC, van Middendorp JJ, Schieving J. Sciatica-like symptoms and the sacroiliac joint: clinical features and differential diagnosis. Eur Spine J. 2013 Jul;22(7):1657-64. doi: 10.1007/s00586-013-2660-5. Epub 2013 Mar 2. PubMed PMID:
[23455949/. ](http://www.ncbi.nlm.nih.gov/pubmed/23455949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23455949)
[Weber U, Zubler V, Pedersen SJ, Rufibach K, Lambert RG, Chan SM, Ostergaard M, Maksymowych WP. Development and validation of a magnetic resonance imaging reference criterion for defining a positive sacroiliac joint magnetic resonance imaging finding in spondyloarthritis. Arthritis Care Res (Hoboken). 2013 Jun;65(6):977-85. doi: 10.1002/acr.21893. PubMed PMID: 23203670. ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203670)
CLINICAL SITUATION FOR QUESTION 72 THROUGH 75
Figures 72a through 72c are the sagittal CT scan and thoracic MR images of a 52-year-old woman with a history of pancreatic neuroendocrine tumor who has severe upper thoracic back pain despite receiving aggressive oral pain treatment. She has metastases in her liver, adrenal glands, and abdominal mesentery. The thoracic disease has been treated with conventional radiation. She continues to work her part-time job without experiencing signs or symptoms of myelopathy.
A B
C
RECOMMENDED READINGS
Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine
[J. 2007 Oct;16(10):1539-50. Epub 2007 Jun 14. PubMed PMID: 17566796. ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17566796)
Visser LH, Nijssen PG, Tijssen CC, van Middendorp JJ, Schieving J. Sciatica-like symptoms and the sacroiliac joint: clinical features and differential diagnosis. Eur Spine J. 2013 Jul;22(7):1657-64. doi: 10.1007/s00586-013-2660-5. Epub 2013 Mar 2. PubMed PMID:
[23455949/. ](http://www.ncbi.nlm.nih.gov/pubmed/23455949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23455949)
[Weber U, Zubler V, Pedersen SJ, Rufibach K, Lambert RG, Chan SM, Ostergaard M, Maksymowych WP. Development and validation of a magnetic resonance imaging reference criterion for defining a positive sacroiliac joint magnetic resonance imaging finding in spondyloarthritis. Arthritis Care Res (Hoboken). 2013 Jun;65(6):977-85. doi: 10.1002/acr.21893. PubMed PMID: 23203670. ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203670)
CLINICAL SITUATION FOR QUESTION 72 THROUGH 75
Figures 72a through 72c are the sagittal CT scan and thoracic MR images of a 52-year-old woman with a history of pancreatic neuroendocrine tumor who has severe upper thoracic back pain despite receiving aggressive oral pain treatment. She has metastases in her liver, adrenal glands, and abdominal mesentery. The thoracic disease has been treated with conventional radiation. She continues to work her part-time job without experiencing signs or symptoms of myelopathy.
A B
C
QUESTION 72
of 100
What is the best next step in managing her pain?
What is the best next step in managing her pain?
1
Additional conventional radiation
2
En bloc spondylectomy
3
Palliative spinal cord decompression and stabilization
4
Epidural steroid injection
- Palliative spinal cord decompression and stabilization
QUESTION 73
of 100
What is the most appropriate systemic therapy for this patient in the short term?
What is the most appropriate systemic therapy for this patient in the short term?
1
Bisphosphonate therapy
2
Monoclonal antibody against receptor activator of nuclear factor kappa beta ligand
3
Doxorubicin
4
Dexamethasone
- Dexamethasone
QUESTION 74
of 100
If surgery is chosen, what is the optimum procedure?
If surgery is chosen, what is the optimum procedure?
1
Transthoracic corpectomy followed by posterior instrumentation
2
Percutaneous pedicle screw stabilization
3
Costotransversectomy with posterior instrumentation
4
Posterior total en bloc spondylectomy
- Costotransversectomy with posterior instrumentation
QUESTION 75
of 100
What is the goal of surgical treatment in this scenario?
What is the goal of surgical treatment in this scenario?
1
To cure cancer
2
To prolong life
3
To relieve pain
4
To reverse neurologic symptoms
This patient has a metastatic neuroendocrine tumor. Surgical treatment should prioritize palliation of her symptoms. She has high-grade spinal cord compression without neurologic signs or symptoms. Steroids are beneficial for patients with high-grade spinal cord compression caused by tumors, and these drugs should be administered in the acute setting. This patient was appropriately initially treated with conventional radiation. However, she is not a candidate for further radiation because of spinal cord tolerance limits and insufficient clearance between the tumor and spinal cord. Consequently, stereotactic radiation is not an option.
The goal of surgical treatment of this tumor should be palliation of her symptoms rather than cure. A costotransversectomy approach offers the advantage of ventral and dorsal spinal cord access, which is necessary in this case. A sternotomy or transthoracic approach would offer ventral access, but dorsal access would be less than optimal.
RECOMMENDED READINGS
[Rose PS, Buchowski JM. Metastatic disease in the thoracic and lumbar spine: evaluation and management. J Am Acad Orthop Surg. 2011 Jan;19(1):37-48. Review. PubMed PMID: 21205766.](http://www.ncbi.nlm.nih.gov/pubmed/21205766)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21205766)
Rades D, Abrahm JL. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol. 2010 Oct;7(10):590-8. doi: 10.1038/nrclinonc.2010.137. Epub 2010 Aug
[31/. Review. PubMed PMID: 20808299. ](http://www.ncbi.nlm.nih.gov/pubmed/20808299)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20808299)
The goal of surgical treatment of this tumor should be palliation of her symptoms rather than cure. A costotransversectomy approach offers the advantage of ventral and dorsal spinal cord access, which is necessary in this case. A sternotomy or transthoracic approach would offer ventral access, but dorsal access would be less than optimal.
RECOMMENDED READINGS
[Rose PS, Buchowski JM. Metastatic disease in the thoracic and lumbar spine: evaluation and management. J Am Acad Orthop Surg. 2011 Jan;19(1):37-48. Review. PubMed PMID: 21205766.](http://www.ncbi.nlm.nih.gov/pubmed/21205766)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21205766)
Rades D, Abrahm JL. The role of radiotherapy for metastatic epidural spinal cord compression. Nat Rev Clin Oncol. 2010 Oct;7(10):590-8. doi: 10.1038/nrclinonc.2010.137. Epub 2010 Aug
[31/. Review. PubMed PMID: 20808299. ](http://www.ncbi.nlm.nih.gov/pubmed/20808299)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20808299)
QUESTION 76
of 100
An obtunded 80-year-old man was found alone in his apartment after an apparent fall. A CT scan performed in the emergency department shows that he has an extensile injury of an ankylosed cervical spine. The fracture extends across the ossified C5-C6 disk space and into the lamina of C5. There is 1.5 cm of widening between the C5 and C6 vertebrae anteriorly. The patient's family asks you about the long-term impact of the fracture on his functional capacity and survival. You advise them that patients with fractures of the cervical spine with ankylosing conditions have
An obtunded 80-year-old man was found alone in his apartment after an apparent fall. A CT scan performed in the emergency department shows that he has an extensile injury of an ankylosed cervical spine. The fracture extends across the ossified C5-C6 disk space and into the lamina of C5. There is 1.5 cm of widening between the C5 and C6 vertebrae anteriorly. The patient's family asks you about the long-term impact of the fracture on his functional capacity and survival. You advise them that patients with fractures of the cervical spine with ankylosing conditions have
1
An unknown prognosis until they can participate in an examination.
2
Higher rates of neurologic deficit and mortality than other same-age people.
3
Higher rates of neurologic deficit than other same-age people, but comparable mortality rates.
4
Similar rates of neurologic deficit and mortality as other same-age people.
Several studies have found that rates of neurologic deficit and mortality are higher for patients with ankylosing spondylitis and a spinal fracture than for age-matched controls. The 2011 work of Schoenfeld and associates, which directly compared patients with cervical fractures in ankylosed spines to age-and sex-matched controls who also had cervical fractures but no ankylosing condition, demonstrated that those with ankylosing spondylitis were at elevated risk for mortality for up to 2 years after sustaining a fracture. In a study by Westerveld and associates, the rate of neurologic deficit among patients with ankylosing spondylitis and a spinal fracture was 57.1% compared to 12.6% among controls.
RECOMMENDED READINGS
[Westerveld LA, van Bemmel JC, Dhert WJ, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014 May 1;14(5):729-40. doi: 10.1016/j.spinee.2013.06.038. Epub 2013 Aug 27. PubMed PMID: 23992936. ](http://www.ncbi.nlm.nih.gov/pubmed/23992936)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23992936)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23992936)
[Schoenfeld AJ, Harris MB, McGuire KJ, Warholic N, Wood KB, Bono CM. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011 Apr;11(4):257-64. doi: 10.1016/j.spinee.2011.01.018. Epub 2011 Mar 5. PubMed PMID: 21377938. ](http://www.ncbi.nlm.nih.gov/pubmed/21377938)[View ](http://www.ncbi.nlm.nih.gov/pubmed/21377938)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21377938)
RECOMMENDED READINGS
[Westerveld LA, van Bemmel JC, Dhert WJ, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014 May 1;14(5):729-40. doi: 10.1016/j.spinee.2013.06.038. Epub 2013 Aug 27. PubMed PMID: 23992936. ](http://www.ncbi.nlm.nih.gov/pubmed/23992936)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23992936)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23992936)
[Schoenfeld AJ, Harris MB, McGuire KJ, Warholic N, Wood KB, Bono CM. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011 Apr;11(4):257-64. doi: 10.1016/j.spinee.2011.01.018. Epub 2011 Mar 5. PubMed PMID: 21377938. ](http://www.ncbi.nlm.nih.gov/pubmed/21377938)[View ](http://www.ncbi.nlm.nih.gov/pubmed/21377938)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21377938)
QUESTION 77
of 100
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
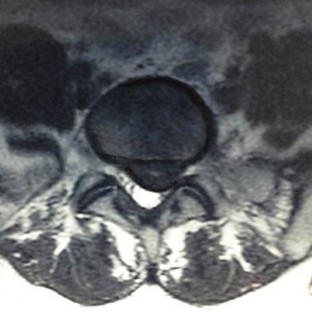
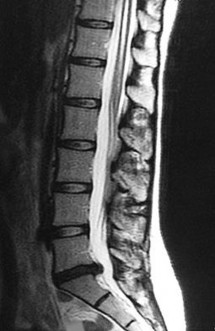
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
1
Saddle anesthesia, hyperreflexia, quadriceps weakness
2
Decreased motor function in the quadriceps and gastrocnemius, hyperreflexia,? and saddle anesthesia
3
More than 5 beats of clonus, saddle anesthesia, and bowel incontinence
4
Urinary retention, saddle anesthesia, and extensor hallucis longus weakness
Cauda equina syndrome is a lower-motor neuron deficit. Hyperreflexia, clonus, and other upper-motor neuron findings would not be seen. Saddle anesthesia, motor weakness, and neurogenic bladder are elements critical to the diagnosis of cauda equina syndrome.
RECOMMENDED READINGS
[Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. ](http://www.ncbi.nlm.nih.gov/pubmed/2936744)[View](http://www.ncbi.nlm.nih.gov/pubmed/2936744)[ ](http://www.ncbi.nlm.nih.gov/pubmed/2936744)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2936744)
[Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. ](http://www.ncbi.nlm.nih.gov/pubmed/18664636)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/18664636)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18664636)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18664636)
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
A B
RECOMMENDED READINGS
[Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. ](http://www.ncbi.nlm.nih.gov/pubmed/2936744)[View](http://www.ncbi.nlm.nih.gov/pubmed/2936744)[ ](http://www.ncbi.nlm.nih.gov/pubmed/2936744)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2936744)
[Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. ](http://www.ncbi.nlm.nih.gov/pubmed/18664636)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/18664636)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18664636)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18664636)
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
A B
QUESTION 78
of 100
Based on this patient's MR images, at which location would you expect to find altered sensation?
Based on this patient's MR images, at which location would you expect to find altered sensation?
1
Medial side of left leg
2
Medial side of left foot
3
Dorsum of left foot
4
Lateral aspect of left foot
- Lateral aspect of left foot
QUESTION 79
of 100
A minimally invasive diskectomy technique poses potential for
A minimally invasive diskectomy technique poses potential for
1
increased dural tear risk.
2
a lower success rate for relief of leg pain.
3
a lower overall complication rate.
4
a higher rate of recurrent disk herniation.
- increased dural tear risk.
QUESTION 80
of 100
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
1
less intraoperative blood loss.
2
an increased rate of recurrent disk herniation.
3
a shorter length of hospital stay.
4
a higher rate of surgical complications.
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
QUESTION 81
of 100
Figure 81 is a lateral thoracic spine radiograph of a 76-year-old man with a history of ankylosing spondylitis who falls and strikes his back. He has moderate thoracic discomfort. An initial examination does not reveal neurologic deficits. He is discharged home that day, but returns 3 days later with profound weakness in his legs. Which imaging study should have been obtained at his initial presentation?
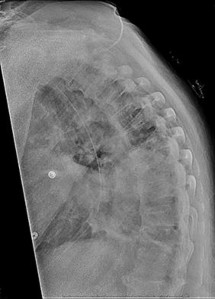
Figure 81 is a lateral thoracic spine radiograph of a 76-year-old man with a history of ankylosing spondylitis who falls and strikes his back. He has moderate thoracic discomfort. An initial examination does not reveal neurologic deficits. He is discharged home that day, but returns 3 days later with profound weakness in his legs. Which imaging study should have been obtained at his initial presentation?
1
Plain radiographs of the lumbar spine
2
Anteroposterior radiograph of the pelvis
3
CT scan of the thoracic spine
4
MRI of the brain

Patients with ankylosing spondylitis are at high risk for occult vertebral fractures that are not readily detectable on radiographs. The treating surgeon must have a high suspicion for fractures in these patients and pursue further imaging of the spine with CT and (often) MRI. Even among patients who are neurologically intact, fracture displacement and neurologic deterioration can occur if fractures are not recognized early and appropriately stabilized. Fractures in patients with ankylosing spondylitis are extremely unstable and are associated with high risk for delayed neurological deterioration. Although plain film imaging of the entire spine should be considered, occult fractures can easily be missed. Imaging of the sacroiliac joints can be helpful to establish the diagnosis of ankylosing spondylitis but would not identify an occult fracture of the vertebra in this patient.
RECOMMENDED READINGS
[Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. ](http://www.ncbi.nlm.nih.gov/pubmed/10432265)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432265) [Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005 Jul 15;30(14):E417-9. PubMed PMID: 16025019. ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16025019)
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and
[complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18791749)
RECOMMENDED READINGS
[Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. ](http://www.ncbi.nlm.nih.gov/pubmed/10432265)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432265) [Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005 Jul 15;30(14):E417-9. PubMed PMID: 16025019. ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16025019)
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and
[complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18791749)
QUESTION 82
of 100
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
1
Increasing coronal plane deformity
2
Increasing pain
3
Increasing sagittal balance
4
Invasiveness of the surgical procedure
In a retrospective review of 137 patients treated surgically and 153 patients treated nonsurgically for adult scoliosis, Bess and associates found that surgical treatment for patients younger than 50 years of age was driven by increased coronal plane deformity, and surgical treatment for older patients was mandated by pain and disability. They also concluded that age, comorbidities, and sagittal balance did not influence treatment decisions.
RECOMMENDED READINGS
[Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.](http://www.ncbi.nlm.nih.gov/pubmed/19752704)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19752704)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19752704)
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
RECOMMENDED READINGS
[Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.](http://www.ncbi.nlm.nih.gov/pubmed/19752704)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19752704)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19752704)
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
QUESTION 83
of 100
Figure 83 is the CT scan of a 36-year-old man who fell from a roof. Eight hours later at the emergency department he describes low-back pain with numbness and weakness in his bilateral lower extremity. A neurologic examination reveals 2/5 strength in his quadriceps and iliopsoas bilaterally, 2/5 strength in his right anterior tibialis and gastrocsoleus, and 1/5 strength in his left anterior tibialis and gastrocsoleus. Two hours later, strength in his lower extremities has diminished markedly. What is the best next step?

Figure 83 is the CT scan of a 36-year-old man who fell from a roof. Eight hours later at the emergency department he describes low-back pain with numbness and weakness in his bilateral lower extremity. A neurologic examination reveals 2/5 strength in his quadriceps and iliopsoas bilaterally, 2/5 strength in his right anterior tibialis and gastrocsoleus, and 1/5 strength in his left anterior tibialis and gastrocsoleus. Two hours later, strength in his lower extremities has diminished markedly. What is the best next step?
1
Intravenous (IV) methylprednisolone with a 30-mg/kg loading dose followed by continuous infusion of 5.4 mg/kg/hour for 24 hours
2
Immediate awake traction reduction
3
Emergent open reduction/decompression
4
Admission to the intensive care unit for fluid resuscitation followed by reduction/decompression when stable
Any progressive neurologic deficit requires emergent surgical intervention. Lumbar injuries cannot be reliably reduced with traction. Although IV steroids and management of mean arterial blood pressure are appropriate interventions for injuries in the region of the conus medullaris, steroids are only indicated when given within 8 hours of injury and are not appropriate as a sole means of management for progressive neurologic deficit.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
[Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[View](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15615508)
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
[Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[View](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15615508)
QUESTION 84
of 100
A 65-year-old woman undergoes a lumbar laminectomy for spinal stenosis at the L3-L4 level. The surgery and postsurgical course are uncomplicated. Eight weeks after surgery she has severe left anterior thigh, groin, and knee pain with ambulation and standing. Which condition is the most likely cause of her symptoms?
A 65-year-old woman undergoes a lumbar laminectomy for spinal stenosis at the L3-L4 level. The surgery and postsurgical course are uncomplicated. Eight weeks after surgery she has severe left anterior thigh, groin, and knee pain with ambulation and standing. Which condition is the most likely cause of her symptoms?
1
Epidural hematoma
2
Osteoarthritis of the hip
3
Miralgia paraesthetica
4
Facet joint pain
Disorders of the hip can mimic and/or coexist with lumbar spine disorders. The prevalence of hip pain lasting longer than 1 month in patients ages 65 to 74 years is 19%. There is often overlap between their respective signs and symptoms. In a patient with failed back surgery syndrome, hip pathology may have been present before back surgery and not recognized. Osteoarthritis of
the hip typically causes groin and anterior thigh pain. Meralgia paraesthetica is more likely to manifest immediately after surgery. Trochanteric bursitis usually affects the proximal lateral thigh and often can radiate to the distal thigh. Facet joint pain causes low-back pain that can be referred to the gluteal region. Epidural hematoma 6 weeks after surgery is highly unlikely.
RECOMMENDED READINGS
Bolt PM, Wahl MM, Schofferman J: The roles of the hip, spine, sacroiliac joint, and other structures in patients with persistent pain after back surgery. Seminars in Spine surgery 2008;20:14-19.
[Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;(419):280-4. PubMed PMID: 15021166. ](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[View](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15021166)
the hip typically causes groin and anterior thigh pain. Meralgia paraesthetica is more likely to manifest immediately after surgery. Trochanteric bursitis usually affects the proximal lateral thigh and often can radiate to the distal thigh. Facet joint pain causes low-back pain that can be referred to the gluteal region. Epidural hematoma 6 weeks after surgery is highly unlikely.
RECOMMENDED READINGS
Bolt PM, Wahl MM, Schofferman J: The roles of the hip, spine, sacroiliac joint, and other structures in patients with persistent pain after back surgery. Seminars in Spine surgery 2008;20:14-19.
[Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;(419):280-4. PubMed PMID: 15021166. ](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[View](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15021166)
QUESTION 85
of 100
Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve
A
B
C D




Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve
A
B
C D
1
resumption of full activity as soon as tolerated.
2
a brace.
3
anterior stabilization and fusion.
4
posterior stabilization and fusion.
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
RECOMMENDED READINGS
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16227897)
[Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15905761)
RESPONSES FOR QUESTIONS 86 THROUGH 89
1. Proximal junctional kyphosis (PJK)
2. Adjacent segment degeneration
3. Intraoperative neurological injury
4. Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
RECOMMENDED READINGS
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16227897)
[Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15905761)
RESPONSES FOR QUESTIONS 86 THROUGH 89
1. Proximal junctional kyphosis (PJK)
2. Adjacent segment degeneration
3. Intraoperative neurological injury
4. Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
QUESTION 86
of 100
A 68-year-old undergoes surgery for adult scoliosis with sagittal imbalance that necessitates a large kyphotic correction.
A 68-year-old undergoes surgery for adult scoliosis with sagittal imbalance that necessitates a large kyphotic correction.
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
- Proximal junctional kyphosis (PJK)
QUESTION 87
of 100
A 47-year-old man undergoes a 3-column osteotomy as part of scoliosis surgery. During closure, somatosensory-evoked potentials decrease.
A 47-year-old man undergoes a 3-column osteotomy as part of scoliosis surgery. During closure, somatosensory-evoked potentials decrease.
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
- Intraoperative neurological injury
QUESTION 88
of 100
A 35-year-old undergoes an L4/L5 posterior fusion for spondylolisthesis. Postsurgical radiographs reveal segmental kyphosis and overall sagittal imbalance.
A 35-year-old undergoes an L4/L5 posterior fusion for spondylolisthesis. Postsurgical radiographs reveal segmental kyphosis and overall sagittal imbalance.
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
- Adjacent segment degeneration
QUESTION 89
of 100
A 62-year-old woman undergoes a posterior laminectomy and fusion from L3 to S1. Postsurgical images show a pelvic incidence (PI) that is significantly larger than the lumbar lordosis (LL).
A 62-year-old woman undergoes a posterior laminectomy and fusion from L3 to S1. Postsurgical images show a pelvic incidence (PI) that is significantly larger than the lumbar lordosis (LL).
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
Sagittal balance is becoming increasingly important. PI should be roughly equal to LL. A PI larger than the LL has been associated with a higher incidence of PJK. PJK also is associated with larger sagittal balance corrections. Additional risk factors include higher presurgical thoracic kyphosis, higher postsurgical lordosis, osteoporosis, fusion below L2, and older (greater than 65 years old) patient age. The loss of somatosensory-evoked potentials during surgery, especially during osteotomy correction, is concerning for neurological injury and should be investigated. If no other cause for a change in signals can be identified, the correction should be lessened to take pressure off of the nerves.
RECOMMENDED READINGS
[Ghobrial GM, Thakkar V, Andrews E, Lang M, Chitale A, Oppenlander ME, Maulucci CM, Sharan AD, Heller J, Harrop JS, Jallo J, Prasad S. Intraoperative vancomycin use in spinal surgery: single institution experience and microbial trends. Spine (Phila Pa 1976). 2014 Apr 1;39(7):550-5. doi: 10.1097/BRS.0000000000000241. PubMed PMID: 24480966. ](http://www.ncbi.nlm.nih.gov/pubmed/24480966)[View](http://www.ncbi.nlm.nih.gov/pubmed/24480966)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24480966)
[Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116091)
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
[Review. PubMed PMID: 21102290. ](http://www.ncbi.nlm.nih.gov/pubmed/21102290)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102290)
[Kim HJ, Bridwell KH, Lenke LG, Park MS, Song KS, Piyaskulkaew C, Chuntarapas T. Patients with proximal junctional kyphosis requiring revision surgery have higher postoperative lumbar lordosis and larger sagittal balance corrections. Spine (Phila Pa 1976). 2014 Apr 20;39(9):E576-80. doi: 10.1097/BRS.0000000000000246. PubMed PMID: 24480958. ](http://www.ncbi.nlm.nih.gov/pubmed/24480958)[View](http://www.ncbi.nlm.nih.gov/pubmed/24480958)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24480958)
[Maruo K, Ha Y, Inoue S, Samuel S, Okada E, Hu SS, Deviren V, Burch S, William S, Ames CP, Mummaneni PV, Chou D, Berven SH. Predictive factors for proximal junctional kyphosis in long fusions to the sacrum in adult spinal deformity. Spine (Phila Pa 1976). 2013 Nov 1;38(23):E1469-76. doi: 10.1097/BRS.0b013e3182a51d43. PubMed PMID: 23921319. ](http://www.ncbi.nlm.nih.gov/pubmed/23921319)[View](http://www.ncbi.nlm.nih.gov/pubmed/23921319)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23921319)
[Radcliff KE, Kepler CK, Jakoi A, Sidhu GS, Rihn J, Vaccaro AR, Albert TJ, Hilibrand AS. Adjacent segment disease in the lumbar spine following different treatment interventions. Spine J. 2013 Oct;13(10):1339-49. doi: 10.1016/j.spinee.2013.03.020. Epub 2013 Jun 15. Review. PubMed PMID: 23773433. ](http://www.ncbi.nlm.nih.gov/pubmed/23773433)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23773433)
Lee JH, Kim JU, Jang JS, Lee SH. Analysis of the incidence and risk factors for the progression of proximal junctional kyphosis following surgical treatment for lumbar degenerative kyphosis: minimum 2-year follow-up. Br J Neurosurg. 2014 Apr;28(2):252-8. doi: 10.3109/02688697.2013.835369. Epub 2013 Dec 9. PubMed PMID: 24313308.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24313308)
RECOMMENDED READINGS
[Ghobrial GM, Thakkar V, Andrews E, Lang M, Chitale A, Oppenlander ME, Maulucci CM, Sharan AD, Heller J, Harrop JS, Jallo J, Prasad S. Intraoperative vancomycin use in spinal surgery: single institution experience and microbial trends. Spine (Phila Pa 1976). 2014 Apr 1;39(7):550-5. doi: 10.1097/BRS.0000000000000241. PubMed PMID: 24480966. ](http://www.ncbi.nlm.nih.gov/pubmed/24480966)[View](http://www.ncbi.nlm.nih.gov/pubmed/24480966)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24480966)
[Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23116091)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116091)
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
[Review. PubMed PMID: 21102290. ](http://www.ncbi.nlm.nih.gov/pubmed/21102290)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21102290)
[Kim HJ, Bridwell KH, Lenke LG, Park MS, Song KS, Piyaskulkaew C, Chuntarapas T. Patients with proximal junctional kyphosis requiring revision surgery have higher postoperative lumbar lordosis and larger sagittal balance corrections. Spine (Phila Pa 1976). 2014 Apr 20;39(9):E576-80. doi: 10.1097/BRS.0000000000000246. PubMed PMID: 24480958. ](http://www.ncbi.nlm.nih.gov/pubmed/24480958)[View](http://www.ncbi.nlm.nih.gov/pubmed/24480958)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24480958)
[Maruo K, Ha Y, Inoue S, Samuel S, Okada E, Hu SS, Deviren V, Burch S, William S, Ames CP, Mummaneni PV, Chou D, Berven SH. Predictive factors for proximal junctional kyphosis in long fusions to the sacrum in adult spinal deformity. Spine (Phila Pa 1976). 2013 Nov 1;38(23):E1469-76. doi: 10.1097/BRS.0b013e3182a51d43. PubMed PMID: 23921319. ](http://www.ncbi.nlm.nih.gov/pubmed/23921319)[View](http://www.ncbi.nlm.nih.gov/pubmed/23921319)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23921319)
[Radcliff KE, Kepler CK, Jakoi A, Sidhu GS, Rihn J, Vaccaro AR, Albert TJ, Hilibrand AS. Adjacent segment disease in the lumbar spine following different treatment interventions. Spine J. 2013 Oct;13(10):1339-49. doi: 10.1016/j.spinee.2013.03.020. Epub 2013 Jun 15. Review. PubMed PMID: 23773433. ](http://www.ncbi.nlm.nih.gov/pubmed/23773433)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23773433)
Lee JH, Kim JU, Jang JS, Lee SH. Analysis of the incidence and risk factors for the progression of proximal junctional kyphosis following surgical treatment for lumbar degenerative kyphosis: minimum 2-year follow-up. Br J Neurosurg. 2014 Apr;28(2):252-8. doi: 10.3109/02688697.2013.835369. Epub 2013 Dec 9. PubMed PMID: 24313308.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24313308)
QUESTION 90
of 100
A
B
Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?


A
B
Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?
1
Similar incidence of postsurgical neck pain with higher risk for radiculopathy recurrence at the same level
2
Higher incidence of postsurgical neck pain and radiculopathy recurrence at the same level
3
Higher incidence of postsurgical neck pain and adjacent-level radiculopathy
4
Lower incidence of adjacent segment degeneration and postsurgical neck pain
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
RECOMMENDED READINGS
[Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. ](http://www.ncbi.nlm.nih.gov/pubmed/17575617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17575617) Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
RECOMMENDED READINGS
[Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. ](http://www.ncbi.nlm.nih.gov/pubmed/17575617)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17575617) Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
QUESTION 91
of 100
A
B
C
Figures 91a through 91c are CT images of a 76-year-old man who was involved in a motor vehicle collision. Which of the following scenarios would pose a contraindication to closed reduction of this injury prior to MR imaging?
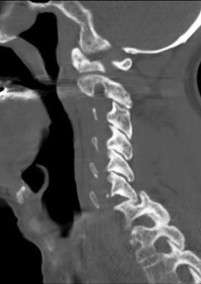

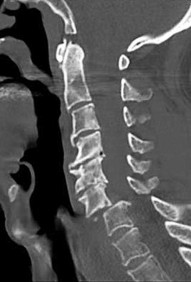
A
B
C
Figures 91a through 91c are CT images of a 76-year-old man who was involved in a motor vehicle collision. Which of the following scenarios would pose a contraindication to closed reduction of this injury prior to MR imaging?
1
American Spinal Injury Association Impairment Scale Grade B neurologic deficit
2
Nondisplaced frontal bone fracture
3
Obtunded status and a blood alcohol concentration higher than 0.2%
4
Presence of facet fractures
This patient has bilateral jumped facet joints at C6-7. Although MR imaging is useful for revealing disk herniations, cord injuries, and bony fragments, early closed reduction to restore anatomic alignment may be attempted prior to MR imaging because reduction will decrease pressure on the cord. There have been reports of catastrophic outcomes with closed reduction in patients who are intubated when disk fragments are pushed into the spinal cord. Consequently, closed reduction should be attempted only in awake and cooperative patients for whom neurologic status monitoring is possible. MR imaging is generally performed after reduction is attempted (successful or not).
RECOMMENDED READINGS
[Initial closed reduction of cervical spine fracture-dislocation injuries. Neurosurgery. 2002 Mar;50(3 Suppl):S44-50. Review. PubMed PMID: 12431286. ](http://www.ncbi.nlm.nih.gov/pubmed/12431286)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12431286) Radcliff K, Sonagli MA, Delasotta L, Singh N, Morrison E, Levine AM, Vaccaro AR. Cervical facet fractures and dislocations. In: Zigler JE, Eismont FJ, Garfin SR, Vaccaro AR, eds. Spine Trauma. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:441-464.
[Vaccaro AR, Falatyn SP, Flanders AE, Balderston RA, Northrup BE, Cotler JM. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine (Phila Pa 1976). 1999 Jun 15;24(12):1210-7. PubMed PMID: 10382247. ](http://www.ncbi.nlm.nih.gov/pubmed/10382247)[View ](http://www.ncbi.nlm.nih.gov/pubmed/10382247)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10382247)
[Wimberley DW, Vaccaro AR, Goyal N, Harrop JS, Anderson DG, Albert TJ, Hilibrand AS. Acute quadriplegia following closed traction reduction of a cervical facet dislocation in the setting of ossification of the posterior longitudinal ligament: case report. Spine (Phila Pa 1976). 2005 Aug 1;30(15):E433-8. PubMed PMID: 16094262. ](http://www.ncbi.nlm.nih.gov/pubmed/16094262)[View ](http://www.ncbi.nlm.nih.gov/pubmed/16094262)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16094262)
RECOMMENDED READINGS
[Initial closed reduction of cervical spine fracture-dislocation injuries. Neurosurgery. 2002 Mar;50(3 Suppl):S44-50. Review. PubMed PMID: 12431286. ](http://www.ncbi.nlm.nih.gov/pubmed/12431286)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12431286) Radcliff K, Sonagli MA, Delasotta L, Singh N, Morrison E, Levine AM, Vaccaro AR. Cervical facet fractures and dislocations. In: Zigler JE, Eismont FJ, Garfin SR, Vaccaro AR, eds. Spine Trauma. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:441-464.
[Vaccaro AR, Falatyn SP, Flanders AE, Balderston RA, Northrup BE, Cotler JM. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine (Phila Pa 1976). 1999 Jun 15;24(12):1210-7. PubMed PMID: 10382247. ](http://www.ncbi.nlm.nih.gov/pubmed/10382247)[View ](http://www.ncbi.nlm.nih.gov/pubmed/10382247)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10382247)
[Wimberley DW, Vaccaro AR, Goyal N, Harrop JS, Anderson DG, Albert TJ, Hilibrand AS. Acute quadriplegia following closed traction reduction of a cervical facet dislocation in the setting of ossification of the posterior longitudinal ligament: case report. Spine (Phila Pa 1976). 2005 Aug 1;30(15):E433-8. PubMed PMID: 16094262. ](http://www.ncbi.nlm.nih.gov/pubmed/16094262)[View ](http://www.ncbi.nlm.nih.gov/pubmed/16094262)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16094262)
QUESTION 92
of 100
Figures 92a through 92c are the radiographs of a 34-year-old man with low-back pain and an inability to walk upright. What is the appropriate surgical treatment?
A B C



Figures 92a through 92c are the radiographs of a 34-year-old man with low-back pain and an inability to walk upright. What is the appropriate surgical treatment?
A B C
1
Smith-Peterson osteotomies at T12-L1, L1-L2 and L2-3.
2
Vertebral column resection through a posterior approach
3
Anterior-posterior osteotomy
4
Pedicle subtraction osteotomy at L3
This patient has a marked fixed sagittal imbalance and a mild coronal imbalance. His fused sacroiliac joints indicate ankylosing spondylitis. Sufficient correction likely can be achieved with a pedicle subtraction osteotomy in the midlumbar spine. Smith-Petersen osteotomies necessitate flexibility of the anterior column, which is not associated with this diagnosis. Also, osteoclasis can result in vascular injuries. Vertebral column resection should not be needed in this case.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
[Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. ](http://www.ncbi.nlm.nih.gov/pubmed/11884909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884909)
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
[Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. ](http://www.ncbi.nlm.nih.gov/pubmed/11884909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884909)
QUESTION 93
of 100
During the approach to the lumbar spine for an L4-L5 anterior lumbar interbody fusion, which structure generally is found overlying the anterior surface of the L4 vertebra?
During the approach to the lumbar spine for an L4-L5 anterior lumbar interbody fusion, which structure generally is found overlying the anterior surface of the L4 vertebra?
1
Aorta
2
Right common iliac artery
3
Left common iliac vein
4
Right ureter
During an anterior approach to the L4-L5 disk space for anterior lumbar interbody fusion, meticulous exposure is paramount to allow for safe preparation of the disk space and subsequent arthrodesis. Although all of these structures can come into play during the exposure, the aorta lies anterior to the L4 vertebral body and bifurcates at this level. The vena cava bifurcates just distal to this. The ureters lie to both sides of the anterior spine. The right common iliac artery and the left common iliac vein originate after the bifurcation of the great vessels and lie caudal to the L4 vertebra.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:226-235.
Agur AMR, Lee MJ, eds. Grant's Atlas of Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:89.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:226-235.
Agur AMR, Lee MJ, eds. Grant's Atlas of Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:89.
QUESTION 94
of 100
What are the most likely examination findings of the patient with the images shown in Figures 94a and 94b?
A
B
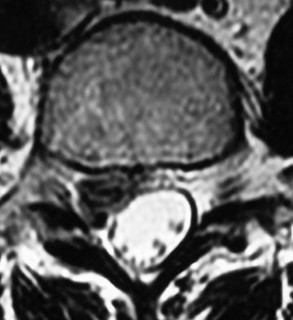

What are the most likely examination findings of the patient with the images shown in Figures 94a and 94b?
A
B
1
Diminished sensation over the distal anterior thigh and medial leg with quadriceps and anterior tibialis weakness and a diminished patellar tendon reflex on the left
2
Diminished sensation over the posterior leg, lateral leg, and plantar foot with weakness of plantar flexion and a diminished Achilles tendon reflex on the right
3
Diminished sensation over the lateral leg and dorsal foot with anterior tibialis and extensor hallucis longus and anterior tibialis weakness on the left 4- Diminished sensation over the lateral leg and dorsal foot with anterior tibialis and extensor hallucis longus and anterior tibialis weakness on the right
The findings on MR imaging reveal a right-sided L4-L5 disk extrusion with cephalad migration of the disk fragment. The axial image shows marked displacement of the traversing right L5 nerve root. The physical findings noted in Response 4 above are typical of a right L5 sensory and motor radiculopathy that would be associated with this level of disk extrusion. Although an extrusion at this level can affect the exiting L4 nerve root resulting in an L4 radiculopathy as described in Response 1, the findings described in this response are contralateral to the disk herniation and not likely to be present. The other responses describe findings associated with left and right S1 radiculopathy, which more typically are associated with an L5-S1 disk herniation/extrusion
RECOMMENDED READINGS
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Haak MH. History and physical examination. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:43-55.
RECOMMENDED READINGS
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Haak MH. History and physical examination. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:43-55.
QUESTION 95
of 100
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?


A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
1
Medical management with intravenous (IV) antibiotics and observation
2
CT-guided aspiration of the abscess before initiating antibiotics
3
Surgical decompression and IV antibiotics
4
Blood cultures and re-evaluation in 24 hours
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
QUESTION 96
of 100
Which factor is most important when making a decision regarding surgery with this patient?
Which factor is most important when making a decision regarding surgery with this patient?
1
Degree of kyphosis
2
Mechanism of injury
3
The patient's other injuries
4
The patient's bone quality
- The patient's other injuries
QUESTION 97
of 100
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
1
anterior corpectomy with percutaneous pedicle screw stabilization.
2
percutaneous pedicle screw stabilization.
3
posterior pedicle screw stabilization with fusion.
4
MRI.
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
[Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. ](http://www.ncbi.nlm.nih.gov/pubmed/16685232)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685232)
[Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. ](http://www.ncbi.nlm.nih.gov/pubmed/10065527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065527)
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.](http://www.ncbi.nlm.nih.gov/pubmed/24332321)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24332321)
RECOMMENDED READINGS
[Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. ](http://www.ncbi.nlm.nih.gov/pubmed/16685232)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685232)
[Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. ](http://www.ncbi.nlm.nih.gov/pubmed/10065527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065527)
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.](http://www.ncbi.nlm.nih.gov/pubmed/24332321)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24332321)
QUESTION 98
of 100
Surgical restoration of sagittal balance of an adult spinal deformity will have which effect on outcome?


Surgical restoration of sagittal balance of an adult spinal deformity will have which effect on outcome?
1
No effect
2
Improve leg-related symptoms but not back pain
3
Improve quality of life and back pain
4
Improve quality of life and leg-related symptoms
The influence of sagittal balance on outcomes following fusion-based procedures for degenerative conditions of the lumbar spine has only recently been appreciated. Restoration of sagittal spinal balance improves low-back-pain outcomes and quality of life. Sagittal spinal balance has not been shown to relieve neurogenic claudication attributable to spinal stenosis.
RECOMMENDED READINGS
[Li Y, Hresko MT. Radiographic analysis of spondylolisthesis and sagittal spinopelvic deformity. J Am Acad Orthop Surg. 2012 Apr;20(4):194-205. doi: 10.5435/JAAOS-20-04-194. Review. PubMed PMID: 22474089. ](http://www.ncbi.nlm.nih.gov/pubmed/22474089)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22474089)
[View ](http://www.ncbi.nlm.nih.gov/pubmed/20354466)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20354466)
CLINICAL SITUATION FOR QUESTIONS 99 AND 100
Figures 99a and 99b are MR images of a 59-year-old man with a history of intravenous (IV) drug abuse who arrives at the emergency department with malaise and fever. Upon admission, the patient's temperature is 38.9°C, his white blood cell count is 17000/µL (reference range [rr], 4500-11000/µL), his erythrocyte sedimentation rate is 98 mm/h (rr, 0-20 mm/h), and his C-reactive protein level is 45 mg/L (rr, 0.08-3.1 mg/L). He is admitted to the medical service to evaluate the source of his fevers. On hospital day 1, the patient reports weakness in his left arm and leg. Blood cultures are positive for methicillin-resistant Staphylococcus aureus.
A B
RECOMMENDED READINGS
[Li Y, Hresko MT. Radiographic analysis of spondylolisthesis and sagittal spinopelvic deformity. J Am Acad Orthop Surg. 2012 Apr;20(4):194-205. doi: 10.5435/JAAOS-20-04-194. Review. PubMed PMID: 22474089. ](http://www.ncbi.nlm.nih.gov/pubmed/22474089)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22474089)
[View ](http://www.ncbi.nlm.nih.gov/pubmed/20354466)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20354466)
CLINICAL SITUATION FOR QUESTIONS 99 AND 100
Figures 99a and 99b are MR images of a 59-year-old man with a history of intravenous (IV) drug abuse who arrives at the emergency department with malaise and fever. Upon admission, the patient's temperature is 38.9°C, his white blood cell count is 17000/µL (reference range [rr], 4500-11000/µL), his erythrocyte sedimentation rate is 98 mm/h (rr, 0-20 mm/h), and his C-reactive protein level is 45 mg/L (rr, 0.08-3.1 mg/L). He is admitted to the medical service to evaluate the source of his fevers. On hospital day 1, the patient reports weakness in his left arm and leg. Blood cultures are positive for methicillin-resistant Staphylococcus aureus.
A B
QUESTION 99
of 100
What is the most likely diagnosis?
What is the most likely diagnosis?
1
Central cord syndrome
2
Cerebrovascular stroke
3
Spinal epidural abscess
4
Guillain-Barre syndrome from IV drug abuse
- Spinal epidural abscess
QUESTION 100
of 100
What is the most appropriate treatment at this time?




What is the most appropriate treatment at this time?
1
IV steroids and antibiotics
2
IV antibiotics
3
Anterior decompression and fusion
4
Posterior laminectomy and instrumented fusion
Prompt diagnosis and treatment of patients with spinal epidural abscess is crucial to maintain and/or improve neurologic function. This clinical scenario stresses the importance of advanced imaging studies. It is also important to recognize the imaging features of spinal epidural abscess. T1-weighted gadolinium-enhanced images show ring enhancement with a central nonenhancing, low-signal area. In such a case, urgent decompression is indicated. Because of the location of the abscess, which is anterior to the spinal cord, an anterior decompression and reconstruction (ie, fusion) is probably the best treatment plan. Steroids are contraindicated in the presence of an epidural abscess. IV antibiotics alone will not adequately treat a patient with a neurological deficit. A posterior laminectomy and fusion will not safely allow access to the abscess.
RECOMMENDED READINGS
[Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg. 2004 May-Jun;12(3):155-63. Review. PubMed PMID: 15161168. ](http://www.ncbi.nlm.nih.gov/pubmed/15161168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15161168) [Ghobrial GM, Beygi S, Viereck MJ, Maulucci CM, Sharan A, Heller J, Jallo J, Prasad S, Harrop JS. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014 Aug;37(2):E1. doi: 10.3171/2014.6.FOCUS14120. PubMed PMID: 25081958. ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[View ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
This is the last question of the exam.
RECOMMENDED READINGS
[Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg. 2004 May-Jun;12(3):155-63. Review. PubMed PMID: 15161168. ](http://www.ncbi.nlm.nih.gov/pubmed/15161168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15161168) [Ghobrial GM, Beygi S, Viereck MJ, Maulucci CM, Sharan A, Heller J, Jallo J, Prasad S, Harrop JS. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014 Aug;37(2):E1. doi: 10.3171/2014.6.FOCUS14120. PubMed PMID: 25081958. ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[View ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
This is the last question of the exam.
