Score: 0%
ORTHOPEDIC MCQS ONLINE 015 TRAUMA
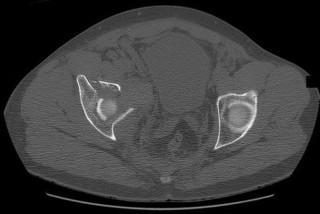
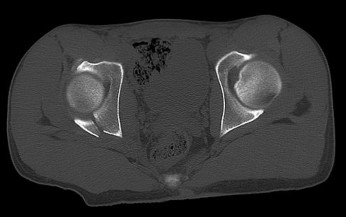
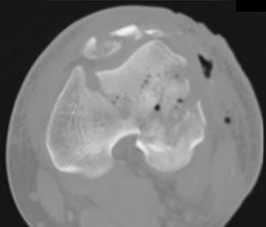
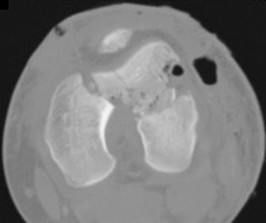
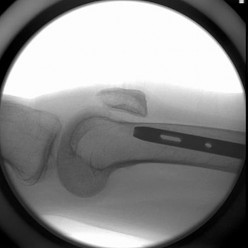
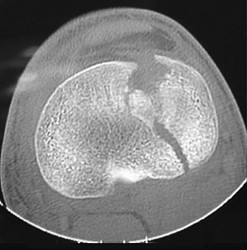
QUESTION 1
C



































1
C
2
/- Anterior column posterior hemitransverse
3
/- Anterior column
4
/- Anterior wall
5
/- Associated both-column
This is an anterior column fracture with dome impaction. The obturator oblique view and both CT images show disruption of the anterior column. Both CT images also reveal an intact posterior column, which eliminates anterior column posterior hemitransverse and associated both-column fracture types as correct responses. An anterior wall fracture would not extend up into the ilium.
RECOMMENDED READINGS
[Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res. 1980 Sep;(151):81-106. PubMed PMID: 7418327.](http://www.ncbi.nlm.nih.gov/pubmed/7418327)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7418327)
Beaulé PE, Dorey FJ, Matta JM. Letournel classification for acetabular fractures. Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am. 2003 Sep;85-A(9):1704-
[9/. PubMed PMID: 12954828.](http://www.ncbi.nlm.nih.gov/pubmed/12954828)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12954828)
CLINICAL SITUATION FOR QUESTIONS 39 THROUGH 41
Figure 39 is the standing radiograph of a 20-year-old college student who injures his foot while playing intramural football. Initial radiograph findings are reportedly normal, but 1 week after injury he still cannot bear weight. You see him in the clinic and note swelling of his foot and plantar ecchymosis.
of 101
A 53-year-old man is involved in a motor vehicle collision and sustains the closed distal femur fracture seen in Figures 54a and 54b. A precontoured distal femoral locking plate is selected for fixation. A locking construct should be used to
A B
- Low strain
of 101
A multifragmentary fracture pattern that is bridge plated, restoring length and alignment, and treated with a 12-hole locking plate with 4 bicortical locking screws placed on each side of the fracture
1) /- High strain
2) /- Low strain
- Low strain
of 101
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
1) /- High strain
2) /- Low strain
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
[Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. ](http://www.ncbi.nlm.nih.gov/pubmed/12463652)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/12463652)[ ](http://www.ncbi.nlm.nih.gov/pubmed/12463652)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12463652)
[Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.](http://www.ncbi.nlm.nih.gov/pubmed/21287837)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21287837)
of 101
The condition seen in Figure 60 is attributable to
1) /- improper nail placement.
2) /- wrong implant choice.
3) /- patient noncompliance.
4) /- radius of the curvature of the implant.
Cephallomedullary implants for treatment of proximal femur fractures have gained in popularity over the last decade. Although these implants have improved outcomes for certain fracture types, multiple complications are associated with this implant. Failure may occur secondary to implant design (for example, mismatch of curvature of the nail to the femur, which can result in distal anterior cortical perforation).
RECOMMENDED READINGS
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013 Jun;27(6):303-7. doi: 10.1097/BOT.0b013e318283f24f. PubMed PMID: 23287752.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23287752)
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000093. doi: 10.1002/14651858.CD000093.pub4. Review. Update
[in: Cochrane Database Syst Rev. 2010;(9):CD000093. PubMed PMID: 18646058. ](http://www.ncbi.nlm.nih.gov/pubmed/18646058)[View](http://www.ncbi.nlm.nih.gov/pubmed/18646058)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18646058)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18646058)
of 101
Figure 61 is the radiograph of a 42-year-old man who falls from a roof and sustains a right calcaneus fracture. His hindfoot is moderately swollen without skin wrinkling and the skin is intact and viable. Neurologic examination findings are normal and the dorsalis pedis pulse is strong and palpable. What is the best treatment plan at this time?
1) /- Immediate open reduction and internal fixation (ORIF) via an extensile lateral approach
2) /- Casting in a plantar-flexed position for 6 weeks
3) /- Splinting with follow-up in 10 to 14 days to check for resolution of swelling
4) /- Splinting with a repeat examination in 1 to 2 days
This patient has a displaced tuberosity of the calcaneus. A high rate of posterior skin breakdown is associated with these fracture types. The skin should be checked within 10 to 14 days when these fractures occur. The skin is swollen and not acutely at risk, so an immediate ORIF via an extensile lateral approach is not warranted. Immobilizing the ankle in a plantar-flexed position can take some tension off the posterior skin with this fracture type but should
not be definitive treatment. Splinting with repeat examination in 1 to 2 days is the preferred response because of the short follow-up for a repeat skin check. If the skin is at risk when a fracture of this type occurs, the ankle can be immobilized in plantar flexion to relieve tension on the skin. Immediate repair with either open or percutaneous techniques may be necessary if the skin remains at risk.
RECOMMENDED READINGS
[Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008 Aug;22(7):439-45. PubMed PMID: 18670282.](http://www.ncbi.nlm.nih.gov/pubmed/18670282)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18670282)
Schwartz AK, Brage ME, Laughlin RT, Stephen D. Foot injuries. In: Baumgartner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:453-468.
of 101
A 55-year-old active left-hand-dominant woman sustains a minimally displaced (less than 2 mm displaced) left proximal humerus fracture that involves fractures of the greater tuberosity and surgical neck. Her activities include tennis and golf. What is the best treatment for this patient?
1) /- Nonsurgical treatment
2) /- Percutaneous skeletal fixation
3) /- Open reduction and internal fixation
4) /- Total shoulder arthroplasty
Literature guiding indications for surgical vs nonsurgical treatment of proximal humerus fractures is not definitive. Many of the recommendations are based on older, nonrandomized series. Newer data suggest that surgical and nonsurgical treatment provide comparable results. Although surgical treatment is preferred for treatment of displaced fractures, fractures with minimal displacement are best managed without surgery.
RECOMMENDED READINGS
[Hauschild O, Konrad G, Audige L, de Boer P, Lambert SM, Hertel R, Südkamp NP. Operative versus non-operative treatment for two-part surgical neck fractures of the proximal humerus. Arch Orthop Trauma Surg. 2013 Oct;133(10):1385-93. doi:10.1007/s00402-013-1798-2. Epub 2013 Jul 3. PubMed PMID: 23820852.](http://www.ncbi.nlm.nih.gov/pubmed/23820852)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23820852)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23820852)
Bell J-R, Cadel ER. Shoulder trauma: Bone. In: Cannada LK, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:319-337.
of 101
A
B
C
Figures 63a through 63c are the radiographs of a 19-year-old woman who sustained injuries in a motorcycle collision. Which initial treatment will result in the best functional outcome and lowest pain scores at 2 years?
1) /- Open reduction and internal fixation (ORIF)
2) /- Closed reduction and percutaneous pinning
3) /- Nonsurgical management with closed reduction and casting
4) /- Primary arthrodesis of the first and second tarsometatarsal joints
Ligamentous injuries to the tarsometatarsal and intermetatarsal joints are commonly a result of high-energy mechanisms. These injuries have resulted in worse outcomes following ORIF than Lisfranc injuries, which involve fractures. Multiple injury patterns may occur, with some injuries involving mostly the ligamentous structures. Ligamentous Lisfranc injuries treated with primary arthrodesis have been shown to result in improved American Orthopaedic Foot & Ankle Society scores and lower Visual Analog Scale pain scores at 2-year follow-up than injuries treated with ORIF. ORIF with either plate or screw fixation has resulted in higher rates of secondary surgeries and lower functional scores. Nonsurgical management is not recommended for displaced injuries. Cast placement is recommended for patients with midfoot sprains with displacement of less than 2 mm. Nonanatomic reductions have been associated with poor results. Closed reduction and percutaneous pinning is unlikely to achieve an anatomic reduction and stable fixation.
RECOMMENDED READINGS
[Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583.](http://www.ncbi.nlm.nih.gov/pubmed/19796583)[View](http://www.ncbi.nlm.nih.gov/pubmed/19796583)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19796583)
[Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816. ](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[View](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16510816)
[Kuo RS, Tejwani NC, Digiovanni CW, Holt SK, Benirschke SK, Hansen ST Jr, Sangeorzan BJ. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. 2000 Nov;82-A(11):1609-18. PubMed PMID: 11097452. ](http://www.ncbi.nlm.nih.gov/pubmed/11097452)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11097452) [Nunley JA, Vertullo CJ. Classification, investigation, and management of midfoot sprains: Lisfranc injuries in the athlete. Am J Sports Med. 2002 Nov-Dec;30(6):871-8. PubMed PMID: 12435655. ](http://www.ncbi.nlm.nih.gov/pubmed/12435655)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12435655)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12435655)
of 101
A 36-year-old healthy man was thrown from a horse and sustained the injury shown in Figures 64a and 64b. His left buttock has a significant hematoma
with a "fluid wave," and the skin overlying the area is anesthetic (diminished sensation). How should this patient's injuries be treated?
A
B
1) /- Early open debridement of the hematoma and open reduction and internal fixation (ORIF) of the fracture with immediate wound closure
2) /- Aspiration and culture of the hematoma, delayed debridement of the hematoma, ORIF, and wound closure
3) /- Nonsurgical management of the wound and fracture
4) /- Early percutaneous debridement of the hematoma followed by delayed ORIF
The treatment of a pelvic and/or acetabular fracture associated with a Morel-Lavallee lesion is fraught with complications. The recommendations are to debride open followed by ORIF, closing only the fascia and leaving the remaining wound open, or performing a percutaneous debridement followed by delayed ORIF. Risk for wound breakdown and infection are higher with other treatment modalities. Cultures are not necessary because they can be positive, but are generally not the infecting organism if infection ensues. The posterior wall fracture pattern mandates surgical management, so nonsurgical management is not appropriate.
RECOMMENDED READINGS
[Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallee lesion. J Trauma. 1997 Jun;42(6):1046-51. PubMed PMID: 9210539.](http://www.ncbi.nlm.nih.gov/pubmed/9210539)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9210539)
[Tseng S, Tornetta P 3rd. Percutaneous management of Morel-Lavallee lesions. J Bone Joint Surg Am. 2006 Jan;88(1):92-6. PubMed PMID: 16391253. ](http://www.ncbi.nlm.nih.gov/pubmed/16391253)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16391253)
CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67
A 25-year-old man with a Gustilo IIIB open tibia fracture is treated with initial irrigation and debridement. Negative pressure wound therapy (NPWT) is initiated while awaiting definitive flap coverage. After 48 hours, the sponge is changed and erythema is noted at the wound edges.
of 101
What is the most likely cause of the erythema?
1) /- Acute bacterial infection
2) /- Allergic reaction to the sponge material
3) /- Mechanical irritation from contact of the sponge with intact skin
4) /- Skin necrosis from the original trauma
- Mechanical irritation from contact of the sponge with intact skin
of 101
What is the NPWT mechanism of action?
1) /- Increased blood flow to the wound
2) /- Increased antibiotic concentration in the wound
3) /- Angiogenic effect of sponge material on the wound bed
4) /- Thermal necrosis kills pathogens at the wound edges
- Increased blood flow to the wound
of 101
In which scenario is application of NPWT contraindicated?
1) /- Fasciotomy wound after compartment syndrome
2) /- Exposed bone after debridement
3) /- Surgical wound that cannot be closed because of tension
4) /- Surgical tumor bed after excision while awaiting final pathology and definitive closure
The most common complication associated with NPWT is a rash on the skin resulting from contact with a suction sponge. In a 2001 study by Webb and Schmidt, 2.2% of patients treated with NPWT had a rash that resolved within 48 hours. To minimize risk for this rash, care should be taken to avoid overlap of the sponge onto intact skin. If skin overlap is unavoidable, a lower-pressure setting should be used.
Acute bacterial infection is possible in this scenario, but there would likely be additional findings such as purulence in the wound itself. Similarly, an acute allergic reaction could be found within the wound and not just at the skin edge. Skin irritation from excessive adhesive plastic tension can result in blistering or shearing avulsion but not skin-edge erythema. Skin necrosis from the original trauma would result in skin-edge duskiness instead of erythema.
A study by Timmers and associates showed a statistically significant increase in microvascular blood flow to the skin under a sponge at subatmospheric pressures. Angiogenesis occurs in the area of the wound vacuum from the negative pressure and increased blood flow, not from the sponge material itself. There has been no indication that antibiotic concentration is increased in the setting of negative pressure therapy because antibiotics would be evacuated along with the fluid. NPWT does not result in increased temperatures that would kill pathogens.
NPWT is contraindicated in the setting of neoplasm because its effect on tumors is unknown. There is potential for increased angiogenesis in residual tumor cells, which could lead to recurrence or even metastasis. NPWT has been used safely and effectively for coverage of open fractures between initial debridement and definitive coverage. Fasciotomy wounds are frequently covered with NPWT dressings on a temporary basis with excellent results.
NPWT has been used to temporize wounds with exposed bone before flap coverage. Wounds with excessive tension frequently can be closed after short-term coverage with NPWT dressings.
RECOMMENDED READINGS
[Webb LX, Schmidt U. [Wound management with vacuum therapy]. Unfallchirurg. 2001 Oct;104(10):918-26. German. PubMed PMID: 11699301.](http://www.ncbi.nlm.nih.gov/pubmed/11699301)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11699301)
[Webb LX. New techniques in wound management: vacuum-assisted wound closure. J Am Acad Orthop Surg. 2002 Sep-Oct;10(5):303-11. PubMed PMID: 12374481. ](http://www.ncbi.nlm.nih.gov/pubmed/12374481)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/12374481)[ ](http://www.ncbi.nlm.nih.gov/pubmed/12374481)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12374481)
[Timmers MS, Le Cessie S, Banwell P, Jukema GN. The effects of varying degrees of pressure delivered bynegative-pressure wound therapy on skin perfusion. Ann Plast Surg. 2005 Dec;55(6):665-71. PubMed PMID: 16327472. ](http://www.ncbi.nlm.nih.gov/pubmed/16327472)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16327472)
CLINICAL SITUATION FOR QUESTIONS 68 AND 69
Figure 68 is the radiograph of a 17-year-old girl who is treated with closed reduction and percutaneous screw fixation for her displaced femoral neck fracture. Capsulotomy of the hip is not performed. After surgery, the patient is instructed to maintain touch-down weight-bearing status for 3 months.
of 101
Which technical error most likely could contribute to a poor outcome for this patient?
1) /- Failure to perform a capsulotomy
2) /- Failure to use a fixed-angle device
3) /- Failure to achieve reduction of the fracture
4) /- Failure to protect postoperative weight bearing
- Failure to achieve reduction of the fracture
of 101
The patient is at highest risk for which complication?
1) /- Postoperative infection
2) /- Heterotopic ossification
3) /- Malunion
4) /- Nonunion
The quality of femoral neck fracture reduction was the key outcome factor in a number of studies. Capsulotomy is performed when achieving open reduction of the femoral neck. In rare cases in which acceptable closed reduction is achieved capsulotomy has been advocated, but poor anatomic reduction is more likely to negatively influence the outcome. Although some biomechanical data suggest that fixed-angle implants may be advantageous, this has not been demonstrated in well-controlled clinical studies. If reduction is not achieved, protecting postoperative weight bearing is not likely to improve outcomes.
Failure to achieve anatomic reduction of the femoral neck frequently leads to nonunion and varus collapse. Postoperative infection and/or heterotopic ossification are not typically seen in closed reduction and percutaneous stabilization of femoral neck fractures. Nonunion is more common than malunion of displaced femoral neck fractures.
RECOMMENDED READINGS
[Duckworth AD, Bennet SJ, Aderinto J, Keating JF. Fixation of intracapsular fractures of the femoral neck in young patients: risk factors for failure. J Bone Joint Surg Br. 2011 Jun;93(6):811-6. doi: 10.1302/0301-620X.93B6.26432. PubMed PMID: 21586782. ](http://www.ncbi.nlm.nih.gov/pubmed/21586782)[View](http://www.ncbi.nlm.nih.gov/pubmed/21586782)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21586782)
[Yang JJ, Lin LC, Chao KH, Chuang SY, Wu CC, Yeh TT, Lian YT. Risk factors for nonunion in patients with intracapsular femoral neck fractures treated with three cannulated screws placed in either a triangle or an inverted triangle configuration. J Bone Joint Surg Am. 2013 Jan 2;95(1):61-9. doi: 10.2106/JBJS.K.01081. PubMed PMID: 23283374. ](http://www.ncbi.nlm.nih.gov/pubmed/23283374)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23283374)
[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23283374)
of 101
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?
1) /- Administer IV fluids and then reassess vital signs before making further decisions
2) /- Pelvic binder and IV fluids
3) /- Pelvic binder and immediate transfusion
4) /- Pelvic binder, IV fluids, type and cross-match, and then transfuse
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
1. /- Retrograde intramedullary (IM) nailing
2. /- Open reduction and internal fixation (ORIF) with screws alone
3. /- Locking condylar plate
4. /- Circular external fixation
5. /- Lateral and medial plates
Which treatment option listed is best for each patient described? of 101
71A
B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
1. /- Retrograde intramedullary (IM) nailing
2. /- Open reduction and internal fixation (ORIF) with screws alone
3. /- Locking condylar plate
4. /- Circular external fixation
5. /- Lateral and medial plates
PREFERRED RESPONSE: 3 - Locking condylar plate
of 101
72A
B
A 65-year-old polytrauma patient with the injury seen in Figures 72a and 72b
1) /- Retrograde intramedullary (IM) nailing
2) /- Open reduction and internal fixation (ORIF) with screws alone
3) /- Locking condylar plate
4) /- Circular external fixation
5) /- Lateral and medial plates
- Retrograde intramedullary (IM) nailing
of 101
32-year-old with the injury seen in Figures 73a and 73b
1) year-old with the injury seen in Figures 73a and 73b
2) /- Retrograde intramedullary (IM) nailing
3) /- Open reduction and internal fixation (ORIF) with screws alone
4) /- Locking condylar plate
5) /- Circular external fixation
- Locking condylar plate
of 101
74 A
B
25-year-old with the injury seen in Figures 74a and 74b
1) year-old with the injury seen in Figures 74a and 74b
2) /- Retrograde intramedullary (IM) nailing
3) /- Open reduction and internal fixation (ORIF) with screws alone
4) /- Locking condylar plate
5) /- Circular external fixation
Figures 71a through 71d reveal a severe intra-articular distal femur fracture that is best treated with ORIF with a locking condylar plate. A retrograde IM nail is not an ideal option for this application. Lateral and medial nonlocking plates have gone by the wayside in favor of locked plating and fixed-angle devices. External fixation will not allow for articular reconstruction and is best reserved for temporary stabilization of these fractures. Screws alone will not address this injury
Figures 72a and 72b reveal an extra-articular distal femur fracture that is best treated with an IM nail, which would also allow for earlier weight bearing. Screw fixation alone is inappropriate, and this does not necessitate medial and lateral plate fixation. Although a locking condylar plate could be used, blood loss in a polytrauma patient may be problematic. ?
Figures 73a and 73b show a comminuted supracondylar femur fracture with complex intra-articular involvement. This would be treated using the same application as seen in Figures 71a through 71d.
Figures 74a and 74b reveal a coronal plane fracture of the medial femoral condyle, which can be treated with screws alone.
RECOMMENDED READINGS
[Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. J Am Acad Orthop Surg. 2010 Oct;18(10):597-607. Review. PubMed PMID: 20889949.](http://www.ncbi.nlm.nih.gov/pubmed/20889949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20889949)
[Markmiller M, Konrad G, Südkamp N. Femur-LISS and distal femoral nail for fixation of distal femoral fractures: are there differences in outcome and complications? Clin Orthop Relat Res. 2004 Sep;(426):252-7. PubMed PMID: 15346082. ](http://www.ncbi.nlm.nih.gov/pubmed/15346082)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15346082)
[Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S, Benirschke SK. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005 Mar;87(3):564-9. PubMed PMID: 15741623. ](http://www.ncbi.nlm.nih.gov/pubmed/15741623)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/15741623)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15741623)
of 101
A
B
C
D
Figures 75a through 75d show the radiographs of an 85-year-old woman who fell from a step and sustained a right proximal femur fracture. Six months after surgery she has knee pain. What is the most likely cause of her pain?
1) /- Nail radius of curvature
2) /- Osteoarthrosis
3) /- Nonunion of fracture
4) /- Improper starting point for nail
Three cases of anterior distal femoral cortex penetration during intramedullary nailing for subtrochanteric fractures were documented by Ostrum and Levy in a 2005 study. Case 1 involved a Zimmer (Warsaw, Indiana) M/DN antegrade femoral nail, Case 2 involved a Stryker (Mahwah, New Jersey) long-stem Gamma nail, and Case 3 a DePuy Synthes (West Chester, Pennsylvania) titanium femoral nail with spiral blade locking. The anterior Zimmer nail penetration resulted in a displaced supracondylar fracture, which subsequently required revision. The Gamma nail as well as the DePuy Synthes nail were left impaled through the distal femoral cortex, and the subtrochanteric fractures went on to union. The anteroposterior radius of curvature for the Zimmer, long Gamma, and DePuy Synthes nails is 257 cm, 300 cm, and 150 cm, respectively. It is estimated that the radius of curvature of the femoral diaphyseal canal is 114 to 120 cm. It appears that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures. There is no evidence of osteoarthrosis on the radiographs. Although nonunion is possible, based on the radiographic findings it is more likely that this patient's pain is attributable to the curvature of the nail. The lateral image of the hip reveals an appropriate starting point for the device.
RECOMMENDED READINGS
[Ostrum RF, Levy MS. Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma. 2005 Oct;19(9):656-60. PubMed PMID: 16247312.](http://www.ncbi.nlm.nih.gov/pubmed/16247312)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16247312)
[Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004 Aug;18(7):410-5. PubMed PMID: 15289685. ](http://www.ncbi.nlm.nih.gov/pubmed/15289685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15289685)
RESPONSES FOR QUESTIONS 76 THROUGH 78
1. /- Nonsurgical treatment with closed reduction and immobilization
2. /- Early mobilization with physical therapy initiated within 2 weeks
3. /- Open reduction and internal fixation (ORIF) with locked implants
4. /- Use of supplemental bone graft or substitutes
5. /- Arthroplasty
6. /- Workup for osteoporosis and counseling
Which intervention listed is most appropriate to address each scenario described?
76A B
of 101
A 75-year-old man fell on his outstretched hand and sustained the fracture seen in Figures 76a and 76b. What is the preferred initial treatment?
1) /- Nonsurgical treatment with closed reduction and immobilization
2) /- Early mobilization with physical therapy initiated within 2 weeks
3) /- Open reduction and internal fixation (ORIF) with locked implants
4) /- Use of supplemental bone graft or substitutes
5) /- Arthroplasty
- Nonsurgical treatment with closed reduction and immobilization
of 101
In addition to the treatment plan, which intervention would also benefit this patient?
1) /- Nonsurgical treatment with closed reduction and immobilization
2) /- Early mobilization with physical therapy initiated within 2 weeks
3) /- Open reduction and internal fixation (ORIF) with locked implants
4) /- Use of supplemental bone graft or substitutes
5) /- Arthroplasty
- Workup for osteoporosis and counseling
of 101
78A
B
Figures 78a and 78b are the emergency department radiographs of an 83-year-old woman who tripped and braced herself against a wall; this was followed by shoulder pain. Which intervention would provide optimal treatment for this patient?
1) /- Nonsurgical treatment with closed reduction and immobilization
2) /- Early mobilization with physical therapy initiated within 2 weeks
3) /- Open reduction and internal fixation (ORIF) with locked implants
4) /- Use of supplemental bone graft or substitutes
5) /- Arthroplasty
Low-energy fractures in elderly patients typically are treated with nonsurgical care that involves early immobilization followed by early rehabilitation/therapy, especially when proximal humerus and distal humerus fractures are involved. Physical therapy should be initiated within the first 2 weeks. If surgery is needed ORIF is preferred for most fractures, but replacement may improve outcomes for unreconstructable fractures. The use of hemiarthroplasty vs reverse shoulder replacement is currently being debated.
For treatment of distal radius fractures in elderly patients, cast immobilization for about 6 weeks will allow for optimal fracture healing. This should be followed by aggressive therapy to improve range of motion and function. Moderately displaced fractures in elderly patients will result in satisfactory outcomes even though reduction may not be "anatomic."
RECOMMENDED READINGS
[Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. ](http://www.ncbi.nlm.nih.gov/pubmed/22159849)[View ](http://www.ncbi.nlm.nih.gov/pubmed/22159849)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/22159849)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22159849)
Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. doi: 10.1016/j.jse.2007.07.016. Epub 2008 Jan 22. PubMed
[PMID: 18207430. ](http://www.ncbi.nlm.nih.gov/pubmed/18207430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18207430)
Solberg BD, Moon CN, Franco DP, Paiement GD. Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome. J Orthop Trauma. 2009 Feb;23(2):113-9. doi: 10.1097/BOT.0b013e31819344bf. PubMed PMID:
[19169103/. ](http://www.ncbi.nlm.nih.gov/pubmed/19169103)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19169103)
RESPONSES FOR QUESTIONS 79 THROIUGH 83
1. /- Percutaneous screw fixation
2. /- Open reduction and internal fixation (ORIF) with a lateral plate
3. /- ORIF with a posteromedial plate
4. /- Dual plating
Which definitive surgical plan listed best addresses each injury pattern described?
of 101
83A
B
32-year-old with the injury pattern seen on the left lower extremity in CT images in Figures 83a and 83b
1) year-old with the injury pattern seen on the left lower extremity in CT images in Figures 83a and 83b
2) /- Percutaneous screw fixation
3) /- Open reduction and internal fixation (ORIF) with a lateral plate
4) /- ORIF with a posteromedial plate
5) /- Dual plating
In Figures 79a through 79c, CT images show a Schatzker IV medial tibial plateau fracture. This fracture is best treated with a medial incision and posteromedial plate, which will function as an antiglide or buttress plate. Percutaneous screw fixation is insufficient for this injury. Lateral fixation is not needed, and in many instances will not capture the medial fragment even with locking fixation. ?
In Figures 80a and 80b, the patient has a fairly well-aligned bicondylar tibial plateau fracture. The lateral joint is significantly depressed, necessitating open reduction and elevation with stabilization. The posteromedial fragment is often missed with single lateral locked plating and is best treated with a posteromedial plate. Percutaneous fixation does not address the joint depression.
In Figure 81, the patient has a classic split depression lateral tibial plateau fracture (Schatzker II). The joint must be reduced from a lateral approach and then supported and stabilized. Definitive ORIF with a lateral plate can be performed when appropriate.
In Figures 82a and 82b, the radiographs show a Schatzker I nondisplaced tibial plateau fracture that is amenable to percutaneous screw fixation if surgical intervention is required. The fracture pattern can be treated surgically, although, considering the comminution at the inferior aspect, late displacement could occur. The other surgical approaches mentioned are not required for this injury.
In Figures 83a and 83b, a lateral split depression tibial plateau fracture is noted (similar to the fracture seen in Figure 81). The same logic applies.
RECOMMENDED READINGS
[Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. ](http://www.ncbi.nlm.nih.gov/pubmed/%2019104303)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2019104303) [Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. ](http://www.ncbi.nlm.nih.gov/pubmed/%2016394164)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/%2016394164)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2016394164)
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi: 10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18317051)
[Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. ](http://www.ncbi.nlm.nih.gov/pubmed/22204013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22204013)
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
[18448992/. ](http://www.ncbi.nlm.nih.gov/pubmed/18448992)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18448992)
of 101
A 19-year-old man was in a motorcycle accident. He sustained a grade IIIB open tibia fracture with a wide zone of injury to the surrounding soft tissue and a closed-head injury. The patient was treated emergently with irrigation, debridement, and external fixation. What is the most accurate statement regarding long-term functional and financial outcomes?
1) /- Patients undergoing limb reconstruction are more satisfied.
2) /- Long-term functional outcomes are superior in the amputation group.
3) /- The percentage of patients who undergo amputation and return to work at 2 years is higher than the percentage of patients who undergo limb salvage who return to work at 2 years.
4) /- The cost of amputation is 3 times higher than the cost of limb reconstruction.
Lower Extremity Assessment Project data suggest that long-term functional outcomes and patient satisfaction at 7 years are equivalent between those
who undergo limb-salvage and primary amputations. Return to work is essentially the same between the 2 groups. The projected lifetime healthcare cost for patients treated with amputation is nearly 3 times higher than costs for those who are treated with limb-salvage procedures.
RECOMMENDED READINGS
[Busse JW, Jacobs CL, Swiontkowski MF, Bosse MJ, Bhandari M; Evidence-Based Orthopaedic Trauma Working Group. Complex limb salvage or early amputation for severe lower-limb injury: a meta-analysis of observational studies. J Orthop Trauma. 2007 Jan;21(1):70-6. PubMed PMID: 17211275. ](http://www.ncbi.nlm.nih.gov/pubmed/17211275)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17211275)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17211275)
[MacKenzie EJ, Jones AS, Bosse MJ, Castillo RC, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, Smith DG, Sanders RW, Jones AL, Starr AJ, McAndrew MP, Patterson BM, Burgess AR. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007 Aug;89(8):1685-92. PubMed PMID: 17671005. ](http://www.ncbi.nlm.nih.gov/pubmed/17671005)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17671005)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17671005)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17671005)
CLINICAL SITUATION FOR QUESTIONS 85 THROUGH 88
Figures 85a and 85b are the plain radiographs of a 38-year-old man who fell off the roof of a 2-story house and sustained an isolated injury to his right knee. Examination reveals a swollen leg with a knee effusion. The skin is intact, but there are some abrasions and an obvious deformity. His neurovascular examination reveals active dorsiflexion and plantar flexion with some pain and symmetric palpable pulses
85A
B
of 101
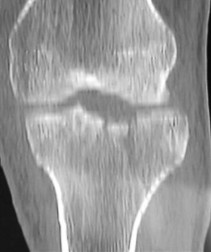
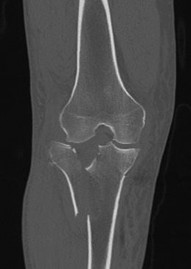
How would you best classify this injury according to the Schatzker classification?
1) /- Schatzker II
2) /- Schatzker IV
3) /- Schatzker V
4) /- Schatzker VI
- Schatzker VI
of 101
What is the best next step?
1) /- Obtain CT images.
2) /- Obtain ankle brachial indices.
3) /- Obtain oblique views.
4) /- Perform knee bridging external fixation.
- Perform knee bridging external fixation.
of 101
87A
B
C
.
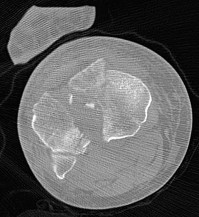
CT images are shown in Figures 87a through 87c. In addition to fixation of the tibial tubercle, what is the best treatment plan for this injury?
1) /- Medial and lateral incisions with dual plates
2) /- Midline incision with a lateral nonlocking plate
3) /- Midline incision with dual locking plates
4) /- Lateral incision with a lateral locking plate
- Medial and lateral incisions with dual plates
of 101
A medial plate is best used to treat tibial plateau fractures when there is
1) /- comminution of the lateral side.
2) /- posteromedial fracture fragment.
3) /- metaphyseal comminution.
4) /- a lateral open fracture.
The patient's plain radiographs demonstrate a bicondylar tibial plateau fracture with complete separation of the diaphysis from the epiphysis, making this a Schatzker VI injury. Clinically, the patient is neurovascularly intact with symmetric palpable pulses, and ankle brachial indices are not necessary.
There is significant lateral tibial plateau displacement with the lateral femoral condyle down into the plateau defect. Considering the swelling, abrasions, and severity of the injury, a bridging external fixator is warranted followed by CT imaging.
The ligamentotaxis will provide better definition of the injury and joint fragments and allow for soft-tissue rest and subsidence of the swelling for eventual surgical intervention. Oblique views will not add as much information as CT imaging, which will show the bicondylar nature of the injury and the proximal tibia essentially split centrally with the tubercle as a separate fragment. A midline incision with medial and lateral plating has fallen out of
favor secondary to wound-healing complications. Comminution of the metaphysis or the lateral side is not an absolute indication for a medial plate. Open lateral fractures can still be managed with a laterally based plate depending on the soft-tissue injury.
RECOMMENDED READINGS
[Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. ](http://www.ncbi.nlm.nih.gov/pubmed/19104303)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19104303) [Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: how does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma. 2007 May;21(5):301-6. PubMed PMID: 17485994. ](http://www.ncbi.nlm.nih.gov/pubmed/17485994)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17485994)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17485994)
[Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. ](http://www.ncbi.nlm.nih.gov/pubmed/16394164)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16394164)
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi:10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18317051)
[Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. PubMed PMID: 16882892. ](http://www.ncbi.nlm.nih.gov/pubmed/16882892)[View](http://www.ncbi.nlm.nih.gov/pubmed/16882892)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16882892)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16882892)
[Hall JA, Beuerlein MJ, McKee MD; Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:74-88. doi: 10.2106/JBJS.G.01165. PubMed PMID: 19255201. ](http://www.ncbi.nlm.nih.gov/pubmed/19255201)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19255201)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255201)
[Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. ](http://www.ncbi.nlm.nih.gov/pubmed/22204013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22204013)
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
[18448992/. ](http://www.ncbi.nlm.nih.gov/pubmed/18448992)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18448992)
CLINICAL SITUATION FOR QUESTIONS 89 THROUGH 91
Figures 89a and 89b are the radiographs of an 80-year-old woman who fell from a standing height.
A B
of 101
When treating this patient, it is important to be familiar with her
1) /- history of other fractures such as hip or distal radius fractures.
2) /- history of athletic participation.
3) /- marital and social status.
4) /- symptoms in the contralateral shoulder.
- history of other fractures such as hip or distal radius fractures.
of 101
When a fragility fracture is suspected, the workup should include
1) /- calcium and vitamin D levels.
2) /- a skeletal survey.
3) /- a bone scan.
4) /- urine analysis.
- calcium and vitamin D levels.
of 101
Use of long-term (at least 5 years) bisphosphonate medications for osteoporosis is associated with
1) /- increased risk for atypical femoral fractures.
2) /- increased risk for femoral neck fractures.
3) /- decreased risk for proximal humerus and wrist fractures.
4) /- decreased risk for mandible osteonecrosis.
Fragility or osteoporotic fractures are common in postmenopausal women and older men and include fractures of the proximal humerus and distal radius and hip and vertebral compression fractures. The most reliable predictor of a fragility fracture is a past fragility fracture; consequently, it is important to elicit history. Assessment of vitamin D and calcium levels is important when treating these patients because many of them have low levels.
Use of bisphosphonates for treatment of osteoporosis results in atypical femur fractures and a decrease in risk for fragility fractures (including hip fractures). There also are reports of osteonecrosis of the mandible with prolonged use of these drugs. Current medical literature suggests stopping these drugs after 3 to 5 years to allow bone remodeling.
RECOMMENDED READINGS
[Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. ](http://www.ncbi.nlm.nih.gov/pubmed/20842676)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/20842676)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20842676)
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone
[Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. ](http://www.ncbi.nlm.nih.gov/pubmed/23712442)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23712442)
CLINICAL SITUATION FOR QUESTIONS 92 THROUGH 95
A 23-year-old man is involved in a motorcycle collision and sustains a displaced transcervical femoral neck fracture with an associated open comminuted femoral shaft fracture.
of 101
The patient is hypotensive and requires resuscitation, laparotomy, and splenectomy. He improves immediately but continued resuscitation is needed and his lactate level is 6.2 (reference range, 5.0-15 mg/dL). What is the most appropriate next step?
1) /- Debridement of the open fracture wound and percutaneous fixation of the femoral neck fracture
2) /- Debridement of the open fracture wound and external fixation of the femur
3) /- Debridement of the open femur fracture, open reduction and internal fixation (ORIF) of the femoral neck via a Smith-Peterson approach, and external fixation of the femoral shaft
4) /- Closed cephalomedullary nailing of the femur
- Debridement of the open fracture wound and external fixation of the femur
of 101
A vertically oriented femoral neck fracture is unique because this pattern
1) /- is more commonly found in elderly patients.
2) /- favors bony union because the relatively longer fracture provides an increased surface area for healing.
3) /- is biomechanically advantageous because more compression occurs at
the fracture site.
4) /- is seen more commonly with associated femoral shaft fractures.
- is seen more commonly with associated femoral shaft fractures.
of 101
The patient undergoes fixation of the associated femoral neck and shaft fractures. The most appropriate fixation construct is a
1) /- piriformis entry reconstruction nail to fix both fractures.
2) /- long proximal femur locking plate to fix both fractures.
3) /- cannulated screw fixation of the femoral neck with retrograde nail fixation of the femoral shaft.
4) /- antegrade nail fixation of the femoral shaft with cannulated screw fixation placed around an antegrade nail.
- cannulated screw fixation of the femoral neck with retrograde nail fixation of the femoral shaft.
of 101
An anatomic reduction is obtained at the femoral neck. The most likely reason for development of avascular necrosis (AVN) in this scenario would be
1) /- an ORIF delay exceeding 24 hours because of hemodynamic ?instability.
2) /- an associated femur fracture.
3) /- patient age and mechanism of injury.
4) /- treatment with a closed reduction.
A damage-control approach is indicated for this patient. Debridement of the open fracture wound and rapid stabilization without an extensive surgical
approach are indicated. Rapid percutaneous fixation of the femoral neck would compromise long-term outcomes for this displaced fracture because obtaining a quality reduction and fixation construct is critical for the long-term outcome. This patient likely would not tolerate cephalomedullary nailing or open approaches very well at this time.
A vertically oriented (Pauwels 3) femoral neck fracture is more common in younger patients who sustain high-energy injuries. Because of the mechanism of injury, many of these patients have associated injuries. This is a biomechanically challenging fracture because the fracture is subject to shear forces rather than compression, making it inherently unstable. This type of fracture often necessitates different fixation strategies to counter shearing forces, such as use of a transversely oriented (Pauwels) screw to compress the fracture or a fixed-angle device.
The femoral neck fracture should be prioritized in this scenario. This does not necessarily mean that the femoral neck should be repaired first, but the strategy should emphasize optimal fixation of the femoral neck. It has been demonstrated that this is less successful when using a single implant to repair both fractures. It is possible to place femoral neck fixation around an antegrade femoral nail; however, it is much more likely that optimal fixation will be achieved with shaft fixation that does not obstruct placement of fixation for the femoral neck.
AVN is more common among physiologically young patients after femoral neck fractures. The higher energy of injury is a likely contributor. Closed reduction has not been shown to increase the risk for AVN when an anatomic reduction is obtained. A surgical delay of 24 hours does not cause AVN. Patients with associated femoral shaft fractures are not at increased risk for AVN; in fact, some studies have shown a relatively lower rate of AVN when a femoral neck fracture is associated with a femoral shaft fracture.
RECOMMENDED READINGS
Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-
[3 vertical femoral neck fractures. J Bone Joint Surg Am. 2008 Aug;90(8):1654-9. doi: 10.2106/JBJS.G.01353. PubMed PMID: 18676894. ](http://www.ncbi.nlm.nih.gov/pubmed/18676894)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18676894)
[Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures--an analysis of various internal fixation strategies. J Orthop Trauma. 2009 Apr;23(4):249-53. doi: 10.1097/BOT.0b013e3181a03675. PubMed PMID: 19318867. ](http://www.ncbi.nlm.nih.gov/pubmed/19318867)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19318867)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19318867)
[Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004 Aug;86-A(8):1711-6. PubMed PMID: 15292419. ](http://www.ncbi.nlm.nih.gov/pubmed/15292419)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15292419) [Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998 Mar-Apr;6(2):106-13. PubMed PMID: 9682073. ](http://www.ncbi.nlm.nih.gov/pubmed/9682073)[View ](http://www.ncbi.nlm.nih.gov/pubmed/9682073)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9682073)
[Upadhyay A, Jain P, Mishra P, Maini L, Gautum VK, Dhaon BK. Delayed internal fixation of fractures of the neck of the femur in young adults. A prospective, randomised study comparing closed and open reduction. J Bone Joint Surg Br. 2004 Sep;86(7):1035-40. PubMed PMID: 15446534. ](http://www.ncbi.nlm.nih.gov/pubmed/15446534)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15446534)
RESPONSES FOR QUESTIONS 96 THROUGH 99
1. /- Warfarin (Coumadin)
2. /- Dabigatran (Pradaxa)
3. /- Rivaroxaban (Xarelto)
4. /- Apixaban (Eliquis)
Match the appropriate oral anticoagulant listed with the description. of 101
This medication is a vitamin K antagonist and can be reversed.
1. /- Warfarin (Coumadin)
2. /- Dabigatran (Pradaxa)
3. /- Rivaroxaban (Xarelto)
4. /- Apixaban (Eliquis)
PREFERRED RESPONSE: 1 - Warfarin (Coumadin)
of 101
This medication, a direct thrombin inhibitor, may be excreted slowly in patients with renal insufficiency.
1) /- Warfarin (Coumadin)
2) /- Dabigatran (Pradaxa)
3) /- Rivaroxaban (Xarelto)
4) /- Apixaban (Eliquis)
- Dabigatran (Pradaxa)
of 101
This medication, a factor Xa inhibitor, offers the advantage of once-daily dosing.
1) /- Warfarin (Coumadin)
2) /- Dabigatran (Pradaxa)
3) /- Rivaroxaban (Xarelto)
4) /- Apixaban (Eliquis)
- Rivaroxaban (Xarelto)
of 101
This medication, a factor Xa inhibitor, currently is not approved for venous thromboembolism (VTE) prophylaxis.
1) /- Warfarin (Coumadin)
2) /- Dabigatran (Pradaxa)
3) /- Rivaroxaban (Xarelto)
4) /- Apixaban (Eliquis)
Warfarin has a long clinical track record and is well known among most physicians. It is a vitamin K antagonist that can be monitored with prothrombin time (INR) testing and reversed with vitamin K and fresh frozen plasma if needed. Newer oral anticoagulants are becoming more common and offer the advantage of being rapidly active without a need for monitoring. These oral anticoagulants are not reversible, which can complicate the treatment of patients who present with bleeding or require surgery. Dabigatran (Pradaxa) is a direct thrombin inhibitor that is approved for stroke prevention in atrial fibrillation. It is not reversible, and a surgical delay of 24 to 48 hours is recommended for all but emergent surgeries. A longer delay is recommended with renal insufficiency. Rivaroxaban (Xarelto) is an oral factor Xa inhibitor that is approved for atrial fibrillation and the treatment of VTE and deep vein thrombosis prophylaxis. It offers the advantage of daily dosing. It
is not reversible and a surgical delay of 36 to 48 hours is recommended. Apixaban (Eliquis) is another factor Xa inhibitor for which twice-daily dosing is required. It is currently approved for stroke prevention in atrial fibrillation, and a surgical delay of 36 to 48 hours is recommended.
RECOMMENDED READINGS
[Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013 May;88(5):495-511. doi: 10.1016/j.mayocp.2013.03.006. Review. Erratum in: Mayo Clin Proc. 2013 Jul;88(7):777. PubMed PMID: 23639500. ](http://www.ncbi.nlm.nih.gov/pubmed/23639500)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23639500) [Alquwaizani M, Buckley L, Adams C, Fanikos J. Anticoagulants: A Review of the Pharmacology, Dosing, and Complications. Curr Emerg Hosp Med Rep. 2013 Apr 21;1(2):83-97. Print 2013 Jun. PubMed PMID: 23687625. ](http://www.ncbi.nlm.nih.gov/pubmed/23687625)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23687625)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23687625)
CLINICAL SITUATION FOR QUESTIONS 100 AND 101
A 55-year-old woman slipped on ice while getting out of her car and sustained the injury shown in Figure 100.
of 101
Which material is preferred to fill the metaphyseal defect during open reduction and internal fixation?
1) /- Recombinant human bone morphogenetic protein (BMP)-2
2) /- BMP-7
3) /- Calcium phosphate
4) /- Polymethylmethacrylate
- Calcium phosphate
of 101
What is the primary mechanism of degradation of calcium phosphate cement?
1) /- Macrophage-mediated degradation
2) /- Osteoclast-mediated degradation
3) /- Giant-cell-mediated degradation
4) /- Dissolution by interstitial fluid
To treat depressed tibial plateau fractures, surgeons must elevate the depressed segments, which results in a metaphyseal bone void. This void can be filled with multiple materials, including autograft and allograft bone. The addition of BMP-2 or BMP-7 is not recommended to fill contained bone defects. These materials are indicated for application between bone and soft tissue and they do not provide the volume or strength to fill closed defects. Calcium phosphates have been use to fill these voids, demonstrating improved strength and resistance to subsidence when compared to autograft. Although polymethylmethacrylate is commonly used to fill bone voids in patients with cancer, it is not preferred in the setting of acute fracture because of the exothermic reaction that may compromise local bone healing. Although hydroxyapatite may be degraded by macrophage and giant-cell-mediated processes, the calcium phosphate degrades mainly by an osteoclast-mediated method. The calcium phosphate is not soluble in interstitial fluid, so simple dissolution does not occur.
RECOMMENDED READINGS
Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P 3rd, Einhorn TA, Buckley R, Leighton R, Russell TA, Larsson S, Bhandari M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J Bone Joint Surg Am. 2008 Jun;90(6):1186-
[96/. doi: 10.2106/JBJS.G.00241. PubMed PMID: 18519310. ](http://www.ncbi.nlm.nih.gov/pubmed/18519310)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18519310)
[Goff T, Kanakaris NK, Giannoudis PV. Use of bone graft substitutes in the management of tibial plateau fractures. Injury. 2013 Jan;44 Suppl 1:S86-94. doi: 10.1016/S0020-1383(13)70019-6. PubMed PMID: 23351879. ](http://www.ncbi.nlm.nih.gov/pubmed/23351879)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23351879)
[Jensen SS, Aaboe M, Pinholt EM, Hjørting-Hansen E, Melsen F, Ruyter IE. Tissue reaction and material characteristics of four bone substitutes. Int J Oral Maxillofac Implants. 1996 Jan-Feb;11(1):55-66. PubMed PMID: 8820123. ](http://www.ncbi.nlm.nih.gov/pubmed/8820123)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8820123)
Schnettler R, Stahl JP,Alt V, Pavlidis T, Dingeldein E, Wenisch S. Calcium phosphate-based bone substitutes. Europ J Trauma 2004;30(4):219-229.
This is the last question of the exam.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
of 101
A multifragmentary fracture pattern that is bridge plated, restoring length and alignment, and treated with a 12-hole locking plate with 4 bicortical locking screws placed on each side of the fracture
1) /- High strain
2) /- Low strain
- Low strain
of 101
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
1) /- High strain
2) /- Low strain
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
[Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. ](http://www.ncbi.nlm.nih.gov/pubmed/12463652)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/12463652)[ ](http://www.ncbi.nlm.nih.gov/pubmed/12463652)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12463652)
[Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.](http://www.ncbi.nlm.nih.gov/pubmed/21287837)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21287837)
of 101
The condition seen in Figure 60 is attributable to
1) /- improper nail placement.
2) /- wrong implant choice.
3) /- patient noncompliance.
4) /- radius of the curvature of the implant.
Cephallomedullary implants for treatment of proximal femur fractures have gained in popularity over the last decade. Although these implants have improved outcomes for certain fracture types, multiple complications are associated with this implant. Failure may occur secondary to implant design (for example, mismatch of curvature of the nail to the femur, which can result in distal anterior cortical perforation).
RECOMMENDED READINGS
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013 Jun;27(6):303-7. doi: 10.1097/BOT.0b013e318283f24f. PubMed PMID: 23287752.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23287752)
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000093. doi: 10.1002/14651858.CD000093.pub4. Review. Update
[in: Cochrane Database Syst Rev. 2010;(9):CD000093. PubMed PMID: 18646058. ](http://www.ncbi.nlm.nih.gov/pubmed/18646058)[View](http://www.ncbi.nlm.nih.gov/pubmed/18646058)[ ](http://www.ncbi.nlm.nih.gov/pubmed/18646058)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18646058)
of 101
Figure 61 is the radiograph of a 42-year-old man who falls from a roof and sustains a right calcaneus fracture. His hindfoot is moderately swollen without skin wrinkling and the skin is intact and viable. Neurologic examination findings are normal and the dorsalis pedis pulse is strong and palpable. What is the best treatment plan at this time?
1) /- Immediate open reduction and internal fixation (ORIF) via an extensile lateral approach
2) /- Casting in a plantar-flexed position for 6 weeks
3) /- Splinting with follow-up in 10 to 14 days to check for resolution of swelling
4) /- Splinting with a repeat examination in 1 to 2 days
This patient has a displaced tuberosity of the calcaneus. A high rate of posterior skin breakdown is associated with these fracture types. The skin should be checked within 10 to 14 days when these fractures occur. The skin is swollen and not acutely at risk, so an immediate ORIF via an extensile lateral approach is not warranted. Immobilizing the ankle in a plantar-flexed position can take some tension off the posterior skin with this fracture type but should
not be definitive treatment. Splinting with repeat examination in 1 to 2 days is the preferred response because of the short follow-up for a repeat skin check. If the skin is at risk when a fracture of this type occurs, the ankle can be immobilized in plantar flexion to relieve tension on the skin. Immediate repair with either open or percutaneous techniques may be necessary if the skin remains at risk.
RECOMMENDED READINGS
[Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008 Aug;22(7):439-45. PubMed PMID: 18670282.](http://www.ncbi.nlm.nih.gov/pubmed/18670282)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18670282)
Schwartz AK, Brage ME, Laughlin RT, Stephen D. Foot injuries. In: Baumgartner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:453-468.
of 101
A 55-year-old active left-hand-dominant woman sustains a minimally displaced (less than 2 mm displaced) left proximal humerus fracture that involves fractures of the greater tuberosity and surgical neck. Her activities include tennis and golf. What is the best treatment for this patient?
1) /- Nonsurgical treatment
2) /- Percutaneous skeletal fixation
3) /- Open reduction and internal fixation
4) /- Total shoulder arthroplasty
Literature guiding indications for surgical vs nonsurgical treatment of proximal humerus fractures is not definitive. Many of the recommendations are based on older, nonrandomized series. Newer data suggest that surgical and nonsurgical treatment provide comparable results. Although surgical treatment is preferred for treatment of displaced fractures, fractures with minimal displacement are best managed without surgery.
RECOMMENDED READINGS
[Hauschild O, Konrad G, Audige L, de Boer P, Lambert SM, Hertel R, Südkamp NP. Operative versus non-operative treatment for two-part surgical neck fractures of the proximal humerus. Arch Orthop Trauma Surg. 2013 Oct;133(10):1385-93. doi:10.1007/s00402-013-1798-2. Epub 2013 Jul 3. PubMed PMID: 23820852.](http://www.ncbi.nlm.nih.gov/pubmed/23820852)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23820852)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23820852)
Bell J-R, Cadel ER. Shoulder trauma: Bone. In: Cannada LK, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:319-337.
of 101
A
B
C
Figures 63a through 63c are the radiographs of a 19-year-old woman who sustained injuries in a motorcycle collision. Which initial treatment will result in the best functional outcome and lowest pain scores at 2 years?
1) /- Open reduction and internal fixation (ORIF)
2) /- Closed reduction and percutaneous pinning
3) /- Nonsurgical management with closed reduction and casting
4) /- Primary arthrodesis of the first and second tarsometatarsal joints
Ligamentous injuries to the tarsometatarsal and intermetatarsal joints are commonly a result of high-energy mechanisms. These injuries have resulted in worse outcomes following ORIF than Lisfranc injuries, which involve fractures. Multiple injury patterns may occur, with some injuries involving mostly the ligamentous structures. Ligamentous Lisfranc injuries treated with primary arthrodesis have been shown to result in improved American Orthopaedic Foot & Ankle Society scores and lower Visual Analog Scale pain scores at 2-year follow-up than injuries treated with ORIF. ORIF with either plate or screw fixation has resulted in higher rates of secondary surgeries and lower functional scores. Nonsurgical management is not recommended for displaced injuries. Cast placement is recommended for patients with midfoot sprains with displacement of less than 2 mm. Nonanatomic reductions have been associated with poor results. Closed reduction and percutaneous pinning is unlikely to achieve an anatomic reduction and stable fixation.
RECOMMENDED READINGS
[Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583.](http://www.ncbi.nlm.nih.gov/pubmed/19796583)[View](http://www.ncbi.nlm.nih.gov/pubmed/19796583)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19796583)
[Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816. ](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[View](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16510816)
[Kuo RS, Tejwani NC, Digiovanni CW, Holt SK, Benirschke SK, Hansen ST Jr, Sangeorzan BJ. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. 2000 Nov;82-A(11):1609-18. PubMed PMID: 11097452. ](http://www.ncbi.nlm.nih.gov/pubmed/11097452)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11097452) [Nunley JA, Vertullo CJ. Classification, investigation, and management of midfoot sprains: Lisfranc injuries in the athlete. Am J Sports Med. 2002 Nov-Dec;30(6):871-8. PubMed PMID: 12435655. ](http://www.ncbi.nlm.nih.gov/pubmed/12435655)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12435655)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12435655)
of 101
A 36-year-old healthy man was thrown from a horse and sustained the injury shown in Figures 64a and 64b. His left buttock has a significant hematoma
with a "fluid wave," and the skin overlying the area is anesthetic (diminished sensation). How should this patient's injuries be treated?
A
B
1) /- Early open debridement of the hematoma and open reduction and internal fixation (ORIF) of the fracture with immediate wound closure
2) /- Aspiration and culture of the hematoma, delayed debridement of the hematoma, ORIF, and wound closure
3) /- Nonsurgical management of the wound and fracture
4) /- Early percutaneous debridement of the hematoma followed by delayed ORIF
The treatment of a pelvic and/or acetabular fracture associated with a Morel-Lavallee lesion is fraught with complications. The recommendations are to debride open followed by ORIF, closing only the fascia and leaving the remaining wound open, or performing a percutaneous debridement followed by delayed ORIF. Risk for wound breakdown and infection are higher with other treatment modalities. Cultures are not necessary because they can be positive, but are generally not the infecting organism if infection ensues. The posterior wall fracture pattern mandates surgical management, so nonsurgical management is not appropriate.
RECOMMENDED READINGS
[Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallee lesion. J Trauma. 1997 Jun;42(6):1046-51. PubMed PMID: 9210539.](http://www.ncbi.nlm.nih.gov/pubmed/9210539)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9210539)
[Tseng S, Tornetta P 3rd. Percutaneous management of Morel-Lavallee lesions. J Bone Joint Surg Am. 2006 Jan;88(1):92-6. PubMed PMID: 16391253. ](http://www.ncbi.nlm.nih.gov/pubmed/16391253)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16391253)
CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67
A 25-year-old man with a Gustilo IIIB open tibia fracture is treated with initial irrigation and debridement. Negative pressure wound therapy (NPWT) is initiated while awaiting definitive flap coverage. After 48 hours, the sponge is changed and erythema is noted at the wound edges.
of 101
What is the most likely cause of the erythema?
1) /- Acute bacterial infection
2) /- Allergic reaction to the sponge material
3) /- Mechanical irritation from contact of the sponge with intact skin
4) /- Skin necrosis from the original trauma
- Mechanical irritation from contact of the sponge with intact skin
of 101
What is the NPWT mechanism of action?
1) /- Increased blood flow to the wound
2) /- Increased antibiotic concentration in the wound
3) /- Angiogenic effect of sponge material on the wound bed
4) /- Thermal necrosis kills pathogens at the wound edges
- Increased blood flow to the wound
of 101
In which scenario is application of NPWT contraindicated?
1) /- Fasciotomy wound after compartment syndrome
2) /- Exposed bone after debridement
3) /- Surgical wound that cannot be closed because of tension
4) /- Surgical tumor bed after excision while awaiting final pathology and definitive closure
The most common complication associated with NPWT is a rash on the skin resulting from contact with a suction sponge. In a 2001 study by Webb and Schmidt, 2.2% of patients treated with NPWT had a rash that resolved within 48 hours. To minimize risk for this rash, care should be taken to avoid overlap of the sponge onto intact skin. If skin overlap is unavoidable, a lower-pressure setting should be used.
Acute bacterial infection is possible in this scenario, but there would likely be additional findings such as purulence in the wound itself. Similarly, an acute allergic reaction could be found within the wound and not just at the skin edge. Skin irritation from excessive adhesive plastic tension can result in blistering or shearing avulsion but not skin-edge erythema. Skin necrosis from the original trauma would result in skin-edge duskiness instead of erythema.
A study by Timmers and associates showed a statistically significant increase in microvascular blood flow to the skin under a sponge at subatmospheric pressures. Angiogenesis occurs in the area of the wound vacuum from the negative pressure and increased blood flow, not from the sponge material itself. There has been no indication that antibiotic concentration is increased in the setting of negative pressure therapy because antibiotics would be evacuated along with the fluid. NPWT does not result in increased temperatures that would kill pathogens.
NPWT is contraindicated in the setting of neoplasm because its effect on tumors is unknown. There is potential for increased angiogenesis in residual tumor cells, which could lead to recurrence or even metastasis. NPWT has been used safely and effectively for coverage of open fractures between initial debridement and definitive coverage. Fasciotomy wounds are frequently covered with NPWT dressings on a temporary basis with excellent results.
NPWT has been used to temporize wounds with exposed bone before flap coverage. Wounds with excessive tension frequently can be closed after short-term coverage with NPWT dressings.
RECOMMENDED READINGS
[Webb LX, Schmidt U. [Wound management with vacuum therapy]. Unfallchirurg. 2001 Oct;104(10):918-26. German. PubMed PMID: 11699301.](http://www.ncbi.nlm.nih.gov/pubmed/11699301)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11699301)
[Webb LX. New techniques in wound management: vacuum-assisted wound closure. J Am Acad Orthop Surg. 2002 Sep-Oct;10(5):303-11. PubMed PMID: 12374481. ](http://www.ncbi.nlm.nih.gov/pubmed/12374481)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/12374481)[ ](http://www.ncbi.nlm.nih.gov/pubmed/12374481)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12374481)
[Timmers MS, Le Cessie S, Banwell P, Jukema GN. The effects of varying degrees of pressure delivered bynegative-pressure wound therapy on skin perfusion. Ann Plast Surg. 2005 Dec;55(6):665-71. PubMed PMID: 16327472. ](http://www.ncbi.nlm.nih.gov/pubmed/16327472)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16327472)
CLINICAL SITUATION FOR QUESTIONS 68 AND 69
Figure 68 is the radiograph of a 17-year-old girl who is treated with closed reduction and percutaneous screw fixation for her displaced femoral neck fracture. Capsulotomy of the hip is not performed. After surgery, the patient is instructed to maintain touch-down weight-bearing status for 3 months.
of 101
Which technical error most likely could contribute to a poor outcome for this patient?
1) /- Failure to perform a capsulotomy
2) /- Failure to use a fixed-angle device
3) /- Failure to achieve reduction of the fracture
4) /- Failure to protect postoperative weight bearing
- Failure to achieve reduction of the fracture
of 101
The patient is at highest risk for which complication?
1) /- Postoperative infection
2) /- Heterotopic ossification
3) /- Malunion
4) /- Nonunion
The quality of femoral neck fracture reduction was the key outcome factor in a number of studies. Capsulotomy is performed when achieving open reduction of the femoral neck. In rare cases in which acceptable closed reduction is achieved capsulotomy has been advocated, but poor anatomic reduction is more likely to negatively influence the outcome. Although some biomechanical data suggest that fixed-angle implants may be advantageous, this has not been demonstrated in well-controlled clinical studies. If reduction is not achieved, protecting postoperative weight bearing is not likely to improve outcomes.
Failure to achieve anatomic reduction of the femoral neck frequently leads to nonunion and varus collapse. Postoperative infection and/or heterotopic ossification are not typically seen in closed reduction and percutaneous stabilization of femoral neck fractures. Nonunion is more common than malunion of displaced femoral neck fractures.
RECOMMENDED READINGS
[Duckworth AD, Bennet SJ, Aderinto J, Keating JF. Fixation of intracapsular fractures of the femoral neck in young patients: risk factors for failure. J Bone Joint Surg Br. 2011 Jun;93(6):811-6. doi: 10.1302/0301-620X.93B6.26432. PubMed PMID: 21586782. ](http://www.ncbi.nlm.nih.gov/pubmed/21586782)[View](http://www.ncbi.nlm.nih.gov/pubmed/21586782)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21586782)
[Yang JJ, Lin LC, Chao KH, Chuang SY, Wu CC, Yeh TT, Lian YT. Risk factors for nonunion in patients with intracapsular femoral neck fractures treated with three cannulated screws placed in either a triangle or an inverted triangle configuration. J Bone Joint Surg Am. 2013 Jan 2;95(1):61-9. doi: 10.2106/JBJS.K.01081. PubMed PMID: 23283374. ](http://www.ncbi.nlm.nih.gov/pubmed/23283374)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/23283374)
[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23283374)
of 101
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?
1) /- Administer IV fluids and then reassess vital signs before making further decisions
2) /- Pelvic binder and IV fluids
3) /- Pelvic binder and immediate transfusion
4) /- Pelvic binder, IV fluids, type and cross-match, and then transfuse
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
1. /- Retrograde intramedullary (IM) nailing
2. /- Open reduction and internal fixation (ORIF) with screws alone
3. /- Locking condylar plate
4. /- Circular external fixation
5. /- Lateral and medial plates
Which treatment option listed is best for each patient described? of 101
71A
B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
1. /- Retrograde intramedullary (IM) nailing
2. /- Open reduction and internal fixation (ORIF) with screws alone
3. /- Locking condylar plate
4. /- Circular external fixation
5. /- Lateral and medial plates
PREFERRED RESPONSE: 3 - Locking condylar plate
of 101
72A
B
A 65-year-old polytrauma patient with the injury seen in Figures 72a and 72b
1) /- Retrograde intramedullary (IM) nailing
2) /- Open reduction and internal fixation (ORIF) with screws alone
3) /- Locking condylar plate
4) /- Circular external fixation
5) /- Lateral and medial plates
- Retrograde intramedullary (IM) nailing
of 101
32-year-old with the injury seen in Figures 73a and 73b
1) year-old with the injury seen in Figures 73a and 73b
2) /- Retrograde intramedullary (IM) nailing
3) /- Open reduction and internal fixation (ORIF) with screws alone
4) /- Locking condylar plate
5) /- Circular external fixation
- Locking condylar plate
of 101
74 A
B
25-year-old with the injury seen in Figures 74a and 74b
1) year-old with the injury seen in Figures 74a and 74b
2) /- Retrograde intramedullary (IM) nailing
3) /- Open reduction and internal fixation (ORIF) with screws alone
4) /- Locking condylar plate
5) /- Circular external fixation
Figures 71a through 71d reveal a severe intra-articular distal femur fracture that is best treated with ORIF with a locking condylar plate. A retrograde IM nail is not an ideal option for this application. Lateral and medial nonlocking plates have gone by the wayside in favor of locked plating and fixed-angle devices. External fixation will not allow for articular reconstruction and is best reserved for temporary stabilization of these fractures. Screws alone will not address this injury
Figures 72a and 72b reveal an extra-articular distal femur fracture that is best treated with an IM nail, which would also allow for earlier weight bearing. Screw fixation alone is inappropriate, and this does not necessitate medial and lateral plate fixation. Although a locking condylar plate could be used, blood loss in a polytrauma patient may be problematic. ?
Figures 73a and 73b show a comminuted supracondylar femur fracture with complex intra-articular involvement. This would be treated using the same application as seen in Figures 71a through 71d.
Figures 74a and 74b reveal a coronal plane fracture of the medial femoral condyle, which can be treated with screws alone.
RECOMMENDED READINGS
[Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. J Am Acad Orthop Surg. 2010 Oct;18(10):597-607. Review. PubMed PMID: 20889949.](http://www.ncbi.nlm.nih.gov/pubmed/20889949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20889949)
[Markmiller M, Konrad G, Südkamp N. Femur-LISS and distal femoral nail for fixation of distal femoral fractures: are there differences in outcome and complications? Clin Orthop Relat Res. 2004 Sep;(426):252-7. PubMed PMID: 15346082. ](http://www.ncbi.nlm.nih.gov/pubmed/15346082)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15346082)
[Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S, Benirschke SK. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am. 2005 Mar;87(3):564-9. PubMed PMID: 15741623. ](http://www.ncbi.nlm.nih.gov/pubmed/15741623)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/15741623)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15741623)
of 101
A
B
C
D
Figures 75a through 75d show the radiographs of an 85-year-old woman who fell from a step and sustained a right proximal femur fracture. Six months after surgery she has knee pain. What is the most likely cause of her pain?
1) /- Nail radius of curvature
2) /- Osteoarthrosis
3) /- Nonunion of fracture
4) /- Improper starting point for nail
Three cases of anterior distal femoral cortex penetration during intramedullary nailing for subtrochanteric fractures were documented by Ostrum and Levy in a 2005 study. Case 1 involved a Zimmer (Warsaw, Indiana) M/DN antegrade femoral nail, Case 2 involved a Stryker (Mahwah, New Jersey) long-stem Gamma nail, and Case 3 a DePuy Synthes (West Chester, Pennsylvania) titanium femoral nail with spiral blade locking. The anterior Zimmer nail penetration resulted in a displaced supracondylar fracture, which subsequently required revision. The Gamma nail as well as the DePuy Synthes nail were left impaled through the distal femoral cortex, and the subtrochanteric fractures went on to union. The anteroposterior radius of curvature for the Zimmer, long Gamma, and DePuy Synthes nails is 257 cm, 300 cm, and 150 cm, respectively. It is estimated that the radius of curvature of the femoral diaphyseal canal is 114 to 120 cm. It appears that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures. There is no evidence of osteoarthrosis on the radiographs. Although nonunion is possible, based on the radiographic findings it is more likely that this patient's pain is attributable to the curvature of the nail. The lateral image of the hip reveals an appropriate starting point for the device.
RECOMMENDED READINGS
[Ostrum RF, Levy MS. Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma. 2005 Oct;19(9):656-60. PubMed PMID: 16247312.](http://www.ncbi.nlm.nih.gov/pubmed/16247312)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16247312)
[Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004 Aug;18(7):410-5. PubMed PMID: 15289685. ](http://www.ncbi.nlm.nih.gov/pubmed/15289685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15289685)
RESPONSES FOR QUESTIONS 76 THROUGH 78
1. /- Nonsurgical treatment with closed reduction and immobilization
2. /- Early mobilization with physical therapy initiated within 2 weeks
3. /- Open reduction and internal fixation (ORIF) with locked implants
4. /- Use of supplemental bone graft or substitutes
5. /- Arthroplasty
6. /- Workup for osteoporosis and counseling
Which intervention listed is most appropriate to address each scenario described?
76A B
of 101
A 75-year-old man fell on his outstretched hand and sustained the fracture seen in Figures 76a and 76b. What is the preferred initial treatment?
1) /- Nonsurgical treatment with closed reduction and immobilization
2) /- Early mobilization with physical therapy initiated within 2 weeks
3) /- Open reduction and internal fixation (ORIF) with locked implants
4) /- Use of supplemental bone graft or substitutes
5) /- Arthroplasty
- Nonsurgical treatment with closed reduction and immobilization
of 101
In addition to the treatment plan, which intervention would also benefit this patient?
1) /- Nonsurgical treatment with closed reduction and immobilization
2) /- Early mobilization with physical therapy initiated within 2 weeks
3) /- Open reduction and internal fixation (ORIF) with locked implants
4) /- Use of supplemental bone graft or substitutes
5) /- Arthroplasty
- Workup for osteoporosis and counseling
of 101
78A
B
Figures 78a and 78b are the emergency department radiographs of an 83-year-old woman who tripped and braced herself against a wall; this was followed by shoulder pain. Which intervention would provide optimal treatment for this patient?
1) /- Nonsurgical treatment with closed reduction and immobilization
2) /- Early mobilization with physical therapy initiated within 2 weeks
3) /- Open reduction and internal fixation (ORIF) with locked implants
4) /- Use of supplemental bone graft or substitutes
5) /- Arthroplasty
Low-energy fractures in elderly patients typically are treated with nonsurgical care that involves early immobilization followed by early rehabilitation/therapy, especially when proximal humerus and distal humerus fractures are involved. Physical therapy should be initiated within the first 2 weeks. If surgery is needed ORIF is preferred for most fractures, but replacement may improve outcomes for unreconstructable fractures. The use of hemiarthroplasty vs reverse shoulder replacement is currently being debated.
For treatment of distal radius fractures in elderly patients, cast immobilization for about 6 weeks will allow for optimal fracture healing. This should be followed by aggressive therapy to improve range of motion and function. Moderately displaced fractures in elderly patients will result in satisfactory outcomes even though reduction may not be "anatomic."
RECOMMENDED READINGS
[Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. ](http://www.ncbi.nlm.nih.gov/pubmed/22159849)[View ](http://www.ncbi.nlm.nih.gov/pubmed/22159849)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/22159849)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22159849)
Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. doi: 10.1016/j.jse.2007.07.016. Epub 2008 Jan 22. PubMed
[PMID: 18207430. ](http://www.ncbi.nlm.nih.gov/pubmed/18207430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18207430)
Solberg BD, Moon CN, Franco DP, Paiement GD. Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome. J Orthop Trauma. 2009 Feb;23(2):113-9. doi: 10.1097/BOT.0b013e31819344bf. PubMed PMID:
[19169103/. ](http://www.ncbi.nlm.nih.gov/pubmed/19169103)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19169103)
RESPONSES FOR QUESTIONS 79 THROIUGH 83
1. /- Percutaneous screw fixation
2. /- Open reduction and internal fixation (ORIF) with a lateral plate
3. /- ORIF with a posteromedial plate
4. /- Dual plating
Which definitive surgical plan listed best addresses each injury pattern described?
of 101
83A
B
32-year-old with the injury pattern seen on the left lower extremity in CT images in Figures 83a and 83b
1) year-old with the injury pattern seen on the left lower extremity in CT images in Figures 83a and 83b
2) /- Percutaneous screw fixation
3) /- Open reduction and internal fixation (ORIF) with a lateral plate
4) /- ORIF with a posteromedial plate
5) /- Dual plating
In Figures 79a through 79c, CT images show a Schatzker IV medial tibial plateau fracture. This fracture is best treated with a medial incision and posteromedial plate, which will function as an antiglide or buttress plate. Percutaneous screw fixation is insufficient for this injury. Lateral fixation is not needed, and in many instances will not capture the medial fragment even with locking fixation. ?
In Figures 80a and 80b, the patient has a fairly well-aligned bicondylar tibial plateau fracture. The lateral joint is significantly depressed, necessitating open reduction and elevation with stabilization. The posteromedial fragment is often missed with single lateral locked plating and is best treated with a posteromedial plate. Percutaneous fixation does not address the joint depression.
In Figure 81, the patient has a classic split depression lateral tibial plateau fracture (Schatzker II). The joint must be reduced from a lateral approach and then supported and stabilized. Definitive ORIF with a lateral plate can be performed when appropriate.
In Figures 82a and 82b, the radiographs show a Schatzker I nondisplaced tibial plateau fracture that is amenable to percutaneous screw fixation if surgical intervention is required. The fracture pattern can be treated surgically, although, considering the comminution at the inferior aspect, late displacement could occur. The other surgical approaches mentioned are not required for this injury.
In Figures 83a and 83b, a lateral split depression tibial plateau fracture is noted (similar to the fracture seen in Figure 81). The same logic applies.
RECOMMENDED READINGS
[Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. ](http://www.ncbi.nlm.nih.gov/pubmed/%2019104303)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2019104303) [Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. ](http://www.ncbi.nlm.nih.gov/pubmed/%2016394164)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/%2016394164)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2016394164)
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi: 10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18317051)
[Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. ](http://www.ncbi.nlm.nih.gov/pubmed/22204013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22204013)
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
[18448992/. ](http://www.ncbi.nlm.nih.gov/pubmed/18448992)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18448992)
of 101
A 19-year-old man was in a motorcycle accident. He sustained a grade IIIB open tibia fracture with a wide zone of injury to the surrounding soft tissue and a closed-head injury. The patient was treated emergently with irrigation, debridement, and external fixation. What is the most accurate statement regarding long-term functional and financial outcomes?
1) /- Patients undergoing limb reconstruction are more satisfied.
2) /- Long-term functional outcomes are superior in the amputation group.
3) /- The percentage of patients who undergo amputation and return to work at 2 years is higher than the percentage of patients who undergo limb salvage who return to work at 2 years.
4) /- The cost of amputation is 3 times higher than the cost of limb reconstruction.
Lower Extremity Assessment Project data suggest that long-term functional outcomes and patient satisfaction at 7 years are equivalent between those
who undergo limb-salvage and primary amputations. Return to work is essentially the same between the 2 groups. The projected lifetime healthcare cost for patients treated with amputation is nearly 3 times higher than costs for those who are treated with limb-salvage procedures.
RECOMMENDED READINGS
[Busse JW, Jacobs CL, Swiontkowski MF, Bosse MJ, Bhandari M; Evidence-Based Orthopaedic Trauma Working Group. Complex limb salvage or early amputation for severe lower-limb injury: a meta-analysis of observational studies. J Orthop Trauma. 2007 Jan;21(1):70-6. PubMed PMID: 17211275. ](http://www.ncbi.nlm.nih.gov/pubmed/17211275)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17211275)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17211275)
[MacKenzie EJ, Jones AS, Bosse MJ, Castillo RC, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, Smith DG, Sanders RW, Jones AL, Starr AJ, McAndrew MP, Patterson BM, Burgess AR. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007 Aug;89(8):1685-92. PubMed PMID: 17671005. ](http://www.ncbi.nlm.nih.gov/pubmed/17671005)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17671005)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17671005)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17671005)
CLINICAL SITUATION FOR QUESTIONS 85 THROUGH 88
Figures 85a and 85b are the plain radiographs of a 38-year-old man who fell off the roof of a 2-story house and sustained an isolated injury to his right knee. Examination reveals a swollen leg with a knee effusion. The skin is intact, but there are some abrasions and an obvious deformity. His neurovascular examination reveals active dorsiflexion and plantar flexion with some pain and symmetric palpable pulses
85A
B
of 101
How would you best classify this injury according to the Schatzker classification?
1) /- Schatzker II
2) /- Schatzker IV
3) /- Schatzker V
4) /- Schatzker VI
- Schatzker VI
of 101
What is the best next step?
1) /- Obtain CT images.
2) /- Obtain ankle brachial indices.
3) /- Obtain oblique views.
4) /- Perform knee bridging external fixation.
- Perform knee bridging external fixation.
of 101
87A
B
C
.
CT images are shown in Figures 87a through 87c. In addition to fixation of the tibial tubercle, what is the best treatment plan for this injury?
1) /- Medial and lateral incisions with dual plates
2) /- Midline incision with a lateral nonlocking plate
3) /- Midline incision with dual locking plates
4) /- Lateral incision with a lateral locking plate
- Medial and lateral incisions with dual plates
of 101
A medial plate is best used to treat tibial plateau fractures when there is
1) /- comminution of the lateral side.
2) /- posteromedial fracture fragment.
3) /- metaphyseal comminution.
4) /- a lateral open fracture.
The patient's plain radiographs demonstrate a bicondylar tibial plateau fracture with complete separation of the diaphysis from the epiphysis, making this a Schatzker VI injury. Clinically, the patient is neurovascularly intact with symmetric palpable pulses, and ankle brachial indices are not necessary.
There is significant lateral tibial plateau displacement with the lateral femoral condyle down into the plateau defect. Considering the swelling, abrasions, and severity of the injury, a bridging external fixator is warranted followed by CT imaging.
The ligamentotaxis will provide better definition of the injury and joint fragments and allow for soft-tissue rest and subsidence of the swelling for eventual surgical intervention. Oblique views will not add as much information as CT imaging, which will show the bicondylar nature of the injury and the proximal tibia essentially split centrally with the tubercle as a separate fragment. A midline incision with medial and lateral plating has fallen out of
favor secondary to wound-healing complications. Comminution of the metaphysis or the lateral side is not an absolute indication for a medial plate. Open lateral fractures can still be managed with a laterally based plate depending on the soft-tissue injury.
RECOMMENDED READINGS
[Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. ](http://www.ncbi.nlm.nih.gov/pubmed/19104303)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19104303) [Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: how does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma. 2007 May;21(5):301-6. PubMed PMID: 17485994. ](http://www.ncbi.nlm.nih.gov/pubmed/17485994)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17485994)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17485994)
[Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. ](http://www.ncbi.nlm.nih.gov/pubmed/16394164)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16394164)
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi:10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18317051)
[Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. PubMed PMID: 16882892. ](http://www.ncbi.nlm.nih.gov/pubmed/16882892)[View](http://www.ncbi.nlm.nih.gov/pubmed/16882892)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16882892)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16882892)
[Hall JA, Beuerlein MJ, McKee MD; Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:74-88. doi: 10.2106/JBJS.G.01165. PubMed PMID: 19255201. ](http://www.ncbi.nlm.nih.gov/pubmed/19255201)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19255201)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19255201)
[Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. ](http://www.ncbi.nlm.nih.gov/pubmed/22204013)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22204013)
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
[18448992/. ](http://www.ncbi.nlm.nih.gov/pubmed/18448992)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18448992)
CLINICAL SITUATION FOR QUESTIONS 89 THROUGH 91
Figures 89a and 89b are the radiographs of an 80-year-old woman who fell from a standing height.
A B
of 101
When treating this patient, it is important to be familiar with her
1) /- history of other fractures such as hip or distal radius fractures.
2) /- history of athletic participation.
3) /- marital and social status.
4) /- symptoms in the contralateral shoulder.
- history of other fractures such as hip or distal radius fractures.
of 101
When a fragility fracture is suspected, the workup should include
1) /- calcium and vitamin D levels.
2) /- a skeletal survey.
3) /- a bone scan.
4) /- urine analysis.
- calcium and vitamin D levels.
of 101
Use of long-term (at least 5 years) bisphosphonate medications for osteoporosis is associated with
1) /- increased risk for atypical femoral fractures.
2) /- increased risk for femoral neck fractures.
3) /- decreased risk for proximal humerus and wrist fractures.
4) /- decreased risk for mandible osteonecrosis.
Fragility or osteoporotic fractures are common in postmenopausal women and older men and include fractures of the proximal humerus and distal radius and hip and vertebral compression fractures. The most reliable predictor of a fragility fracture is a past fragility fracture; consequently, it is important to elicit history. Assessment of vitamin D and calcium levels is important when treating these patients because many of them have low levels.
Use of bisphosphonates for treatment of osteoporosis results in atypical femur fractures and a decrease in risk for fragility fractures (including hip fractures). There also are reports of osteonecrosis of the mandible with prolonged use of these drugs. Current medical literature suggests stopping these drugs after 3 to 5 years to allow bone remodeling.
RECOMMENDED READINGS
[Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. ](http://www.ncbi.nlm.nih.gov/pubmed/20842676)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/20842676)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20842676)
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone
[Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. ](http://www.ncbi.nlm.nih.gov/pubmed/23712442)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23712442)
CLINICAL SITUATION FOR QUESTIONS 92 THROUGH 95
A 23-year-old man is involved in a motorcycle collision and sustains a displaced transcervical femoral neck fracture with an associated open comminuted femoral shaft fracture.
of 101
The patient is hypotensive and requires resuscitation, laparotomy, and splenectomy. He improves immediately but continued resuscitation is needed and his lactate level is 6.2 (reference range, 5.0-15 mg/dL). What is the most appropriate next step?
1) /- Debridement of the open fracture wound and percutaneous fixation of the femoral neck fracture
2) /- Debridement of the open fracture wound and external fixation of the femur
3) /- Debridement of the open femur fracture, open reduction and internal fixation (ORIF) of the femoral neck via a Smith-Peterson approach, and external fixation of the femoral shaft
4) /- Closed cephalomedullary nailing of the femur
- Debridement of the open fracture wound and external fixation of the femur
of 101
A vertically oriented femoral neck fracture is unique because this pattern
1) /- is more commonly found in elderly patients.
2) /- favors bony union because the relatively longer fracture provides an increased surface area for healing.
3) /- is biomechanically advantageous because more compression occurs at
the fracture site.
4) /- is seen more commonly with associated femoral shaft fractures.
- is seen more commonly with associated femoral shaft fractures.
of 101
The patient undergoes fixation of the associated femoral neck and shaft fractures. The most appropriate fixation construct is a
1) /- piriformis entry reconstruction nail to fix both fractures.
2) /- long proximal femur locking plate to fix both fractures.
3) /- cannulated screw fixation of the femoral neck with retrograde nail fixation of the femoral shaft.
4) /- antegrade nail fixation of the femoral shaft with cannulated screw fixation placed around an antegrade nail.
- cannulated screw fixation of the femoral neck with retrograde nail fixation of the femoral shaft.
of 101
An anatomic reduction is obtained at the femoral neck. The most likely reason for development of avascular necrosis (AVN) in this scenario would be
1) /- an ORIF delay exceeding 24 hours because of hemodynamic ?instability.
2) /- an associated femur fracture.
3) /- patient age and mechanism of injury.
4) /- treatment with a closed reduction.
A damage-control approach is indicated for this patient. Debridement of the open fracture wound and rapid stabilization without an extensive surgical
approach are indicated. Rapid percutaneous fixation of the femoral neck would compromise long-term outcomes for this displaced fracture because obtaining a quality reduction and fixation construct is critical for the long-term outcome. This patient likely would not tolerate cephalomedullary nailing or open approaches very well at this time.
A vertically oriented (Pauwels 3) femoral neck fracture is more common in younger patients who sustain high-energy injuries. Because of the mechanism of injury, many of these patients have associated injuries. This is a biomechanically challenging fracture because the fracture is subject to shear forces rather than compression, making it inherently unstable. This type of fracture often necessitates different fixation strategies to counter shearing forces, such as use of a transversely oriented (Pauwels) screw to compress the fracture or a fixed-angle device.
The femoral neck fracture should be prioritized in this scenario. This does not necessarily mean that the femoral neck should be repaired first, but the strategy should emphasize optimal fixation of the femoral neck. It has been demonstrated that this is less successful when using a single implant to repair both fractures. It is possible to place femoral neck fixation around an antegrade femoral nail; however, it is much more likely that optimal fixation will be achieved with shaft fixation that does not obstruct placement of fixation for the femoral neck.
AVN is more common among physiologically young patients after femoral neck fractures. The higher energy of injury is a likely contributor. Closed reduction has not been shown to increase the risk for AVN when an anatomic reduction is obtained. A surgical delay of 24 hours does not cause AVN. Patients with associated femoral shaft fractures are not at increased risk for AVN; in fact, some studies have shown a relatively lower rate of AVN when a femoral neck fracture is associated with a femoral shaft fracture.
RECOMMENDED READINGS
Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-
[3 vertical femoral neck fractures. J Bone Joint Surg Am. 2008 Aug;90(8):1654-9. doi: 10.2106/JBJS.G.01353. PubMed PMID: 18676894. ](http://www.ncbi.nlm.nih.gov/pubmed/18676894)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18676894)
[Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures--an analysis of various internal fixation strategies. J Orthop Trauma. 2009 Apr;23(4):249-53. doi: 10.1097/BOT.0b013e3181a03675. PubMed PMID: 19318867. ](http://www.ncbi.nlm.nih.gov/pubmed/19318867)[View ](http://www.ncbi.nlm.nih.gov/pubmed/19318867)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19318867)
[Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004 Aug;86-A(8):1711-6. PubMed PMID: 15292419. ](http://www.ncbi.nlm.nih.gov/pubmed/15292419)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15292419) [Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998 Mar-Apr;6(2):106-13. PubMed PMID: 9682073. ](http://www.ncbi.nlm.nih.gov/pubmed/9682073)[View ](http://www.ncbi.nlm.nih.gov/pubmed/9682073)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9682073)
[Upadhyay A, Jain P, Mishra P, Maini L, Gautum VK, Dhaon BK. Delayed internal fixation of fractures of the neck of the femur in young adults. A prospective, randomised study comparing closed and open reduction. J Bone Joint Surg Br. 2004 Sep;86(7):1035-40. PubMed PMID: 15446534. ](http://www.ncbi.nlm.nih.gov/pubmed/15446534)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15446534)
RESPONSES FOR QUESTIONS 96 THROUGH 99
1. /- Warfarin (Coumadin)
2. /- Dabigatran (Pradaxa)
3. /- Rivaroxaban (Xarelto)
4. /- Apixaban (Eliquis)
Match the appropriate oral anticoagulant listed with the description. of 101
This medication is a vitamin K antagonist and can be reversed.
1. /- Warfarin (Coumadin)
2. /- Dabigatran (Pradaxa)
3. /- Rivaroxaban (Xarelto)
4. /- Apixaban (Eliquis)
PREFERRED RESPONSE: 1 - Warfarin (Coumadin)
of 101
This medication, a direct thrombin inhibitor, may be excreted slowly in patients with renal insufficiency.
1) /- Warfarin (Coumadin)
2) /- Dabigatran (Pradaxa)
3) /- Rivaroxaban (Xarelto)
4) /- Apixaban (Eliquis)
- Dabigatran (Pradaxa)
of 101
This medication, a factor Xa inhibitor, offers the advantage of once-daily dosing.
1) /- Warfarin (Coumadin)
2) /- Dabigatran (Pradaxa)
3) /- Rivaroxaban (Xarelto)
4) /- Apixaban (Eliquis)
- Rivaroxaban (Xarelto)
of 101
This medication, a factor Xa inhibitor, currently is not approved for venous thromboembolism (VTE) prophylaxis.
1) /- Warfarin (Coumadin)
2) /- Dabigatran (Pradaxa)
3) /- Rivaroxaban (Xarelto)
4) /- Apixaban (Eliquis)
Warfarin has a long clinical track record and is well known among most physicians. It is a vitamin K antagonist that can be monitored with prothrombin time (INR) testing and reversed with vitamin K and fresh frozen plasma if needed. Newer oral anticoagulants are becoming more common and offer the advantage of being rapidly active without a need for monitoring. These oral anticoagulants are not reversible, which can complicate the treatment of patients who present with bleeding or require surgery. Dabigatran (Pradaxa) is a direct thrombin inhibitor that is approved for stroke prevention in atrial fibrillation. It is not reversible, and a surgical delay of 24 to 48 hours is recommended for all but emergent surgeries. A longer delay is recommended with renal insufficiency. Rivaroxaban (Xarelto) is an oral factor Xa inhibitor that is approved for atrial fibrillation and the treatment of VTE and deep vein thrombosis prophylaxis. It offers the advantage of daily dosing. It
is not reversible and a surgical delay of 36 to 48 hours is recommended. Apixaban (Eliquis) is another factor Xa inhibitor for which twice-daily dosing is required. It is currently approved for stroke prevention in atrial fibrillation, and a surgical delay of 36 to 48 hours is recommended.
RECOMMENDED READINGS
[Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013 May;88(5):495-511. doi: 10.1016/j.mayocp.2013.03.006. Review. Erratum in: Mayo Clin Proc. 2013 Jul;88(7):777. PubMed PMID: 23639500. ](http://www.ncbi.nlm.nih.gov/pubmed/23639500)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23639500) [Alquwaizani M, Buckley L, Adams C, Fanikos J. Anticoagulants: A Review of the Pharmacology, Dosing, and Complications. Curr Emerg Hosp Med Rep. 2013 Apr 21;1(2):83-97. Print 2013 Jun. PubMed PMID: 23687625. ](http://www.ncbi.nlm.nih.gov/pubmed/23687625)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/23687625)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23687625)
CLINICAL SITUATION FOR QUESTIONS 100 AND 101
A 55-year-old woman slipped on ice while getting out of her car and sustained the injury shown in Figure 100.
of 101
Which material is preferred to fill the metaphyseal defect during open reduction and internal fixation?
1) /- Recombinant human bone morphogenetic protein (BMP)-2
2) /- BMP-7
3) /- Calcium phosphate
4) /- Polymethylmethacrylate
- Calcium phosphate
of 101
What is the primary mechanism of degradation of calcium phosphate cement?
1) /- Macrophage-mediated degradation
2) /- Osteoclast-mediated degradation
3) /- Giant-cell-mediated degradation
4) /- Dissolution by interstitial fluid
To treat depressed tibial plateau fractures, surgeons must elevate the depressed segments, which results in a metaphyseal bone void. This void can be filled with multiple materials, including autograft and allograft bone. The addition of BMP-2 or BMP-7 is not recommended to fill contained bone defects. These materials are indicated for application between bone and soft tissue and they do not provide the volume or strength to fill closed defects. Calcium phosphates have been use to fill these voids, demonstrating improved strength and resistance to subsidence when compared to autograft. Although polymethylmethacrylate is commonly used to fill bone voids in patients with cancer, it is not preferred in the setting of acute fracture because of the exothermic reaction that may compromise local bone healing. Although hydroxyapatite may be degraded by macrophage and giant-cell-mediated processes, the calcium phosphate degrades mainly by an osteoclast-mediated method. The calcium phosphate is not soluble in interstitial fluid, so simple dissolution does not occur.
RECOMMENDED READINGS
Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P 3rd, Einhorn TA, Buckley R, Leighton R, Russell TA, Larsson S, Bhandari M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J Bone Joint Surg Am. 2008 Jun;90(6):1186-
[96/. doi: 10.2106/JBJS.G.00241. PubMed PMID: 18519310. ](http://www.ncbi.nlm.nih.gov/pubmed/18519310)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18519310)
[Goff T, Kanakaris NK, Giannoudis PV. Use of bone graft substitutes in the management of tibial plateau fractures. Injury. 2013 Jan;44 Suppl 1:S86-94. doi: 10.1016/S0020-1383(13)70019-6. PubMed PMID: 23351879. ](http://www.ncbi.nlm.nih.gov/pubmed/23351879)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23351879)
[Jensen SS, Aaboe M, Pinholt EM, Hjørting-Hansen E, Melsen F, Ruyter IE. Tissue reaction and material characteristics of four bone substitutes. Int J Oral Maxillofac Implants. 1996 Jan-Feb;11(1):55-66. PubMed PMID: 8820123. ](http://www.ncbi.nlm.nih.gov/pubmed/8820123)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8820123)
Schnettler R, Stahl JP,Alt V, Pavlidis T, Dingeldein E, Wenisch S. Calcium phosphate-based bone substitutes. Europ J Trauma 2004;30(4):219-229.
This is the last question of the exam.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
