Orthopedic Upper Extrem Review | Dr Hutaif General Orth -...
Updated: Feb 2026
56 Views
Key Medical Takeaway
In this comprehensive guide, we discuss everything you need to know about ORTHOPEDIC MCQS ONLINE 014 UPPER EXTREMITY. An arthroscopic Bankart repair is a minimally invasive surgical procedure performed to treat shoulder instability, specifically a Bankart lesion. This injury involves the detachment of the labrum from the anterior glenoid rim after a shoulder dislocation. The procedure reattaches the torn labrum and tightens the joint capsule, aiming to restore shoulder stability and prevent future dislocations through small incisions.
Table of Contents
Score: 0%
ORTHOPEDIC MCQS ONLINE 014 UPPER EXTREMITY
QUESTION 1
..A 45-year-old man who had gout in his foot 2 years ago has a 3-day history of elbow pain without an injury. The pain is diffuse, constant, and worse with any movement. Examination shows motion from 20 degrees to 90 degrees. There is no erythema around his elbow, he has no fever, and a sensory and motor examination of his arm is unremarkable.
Radiographs only show an effusion. The patient’s uric acid level is within defined limits. What is the next diagnostic step?
1
Elbow joint aspiration
2
MRI scan
3
Splint for 2 weeks and repeat examination
4
Sedimentation rate and C-reactive protein level
DISCUSSION…The best way to make the diagnosis is to aspirate the fluid from the joint and send it to the laboratory for a cell count and crystal search. This will allow for the diagnosis of an infection, gout, or pseudogout. An MRI scan will confirm the examination finding of an effusion, but it will not reveal the cause of an inflammatory effusion. If the patient has chronic gout, an MRI scan or ultrasound can aid in diagnosis if gout tophi are seen. A splint will help relieve the pain from the effusion and the effusion may resolve on its own, but it will not contribute to a diagnosis.
Sedimentation rate and C-reactive protein level will help to rule out an infection, but they are not as diagnostic as an aspiration.
- Elbow joint aspiration
QUESTION 2
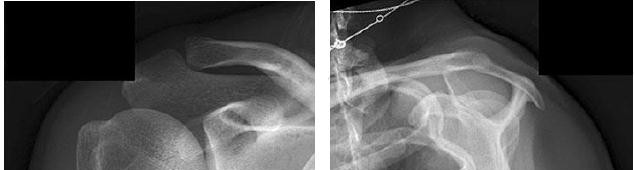
..A 65-year-old man who underwent an uncomplicated reverse total shoulder arthroplasty (rTSA) to treat rotator cuff arthropathy 2 years ago has a routine follow-up visit in your clinic. A radiograph at 2-year followup is shown in Figure 2. He denies shoulder pain and dysfunction and constitutional symptoms, and his clinical examination findings are benign. Based upon the present radiologic evaluation, what is the next most appropriate step?
1
Revision rTSA
2
Conversion to hemiarthroplasty
3
Continued observation
4
Infection work-up with screening labs and joint aspiration **DISCUSSION..** Based upon the patient’s clinical examination and symptoms, continued observation is appropriate. The remaining options are not indicated. The radiograph reveals scapular notching, one of the more common complications specific to rTSA. Notching is caused by repeated contact between the humeral component and/or humerus and the inferior pillar of the scapular neck. Generation of particulate debris from this interaction can result in osteolysis with the potential for screw and
base plate failure. The overall incidence of notching has been reported to be between 51% and 96%. This nearly ubiquitous finding has been attributed to implant positioning, altered glenoid and humeral anatomy, and duration of implantation. Recent studies that indicate increased lateral offset, increased glenosphere size, and inferior positioning of the base plate may reduce the incidence of scapular notching.
- Continued observation
QUESTION 3
..A 61-year-old right-hand-dominant woman sustains a fall down 3 stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm.
What is the most appropriate treatment?
1
Open reduction internal fixation with transosseous sutures
2
Arthroscopic fixation using a suture bridge technique
3
Nonsurgical treatment with early passive range of motion
4
Nonsurgical treatment with sling immobilization for 4 weeks
DISCUSSION..Greater tuberosity fractures and rotator cuff tears associated with a traumatic dislocation are more commonly seen in women older than age 60. Greater tuberosity fractures that are displaced less than 5 mm in the general population and less than 3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range of motion is important to avoid the complication of stiffness.
- Nonsurgical treatment with early passive range of motion
QUESTION 4
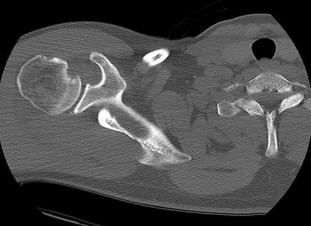
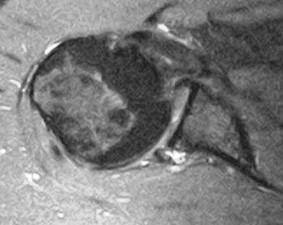
..A 30-year-old man with diabetes sustained an acute posterior dislocation of his right shoulder after a seizure event that required emergency department reduction. You initially treat him with a sling for 4 weeks and then refer him for outpatient therapy. During his therapy sessions, the patient admits to pain and instability symptoms during range of motion exercises. Repeat examination indicates a positive posterior load-shift test and apprehension with adduction and internal rotation of the shoulder. His CT and MRI scans are shown in Figures 4a and 4b. What is the most appropriate next step in treating his injury?
1
Brief period of immobilization and reinitiation of therapy
2
Open posterior capsular shift with labral repair
3
Arthroscopic capsulolabral repair with subscapularis and lesser tuberosity transfer
4
Resurfacing arthroplasty with labral repair
DISCUSSION..Posterior glenohumeral dislocations are much less common than anterior glenohumeral dislocations, with a prevalence of 1.1 per 100,000 per year. There is a bimodal distribution with a peak in young men (2.4 men to 1 woman) and a second peak in elderly people with a more equivalent gender ratio. Posterior dislocations most commonly result from trauma, with
the remainder of events secondary to seizure activity. According to Robinson and associates, age younger than 40 years, dislocation during a seizure, and a large Hill-Sachs lesion were all predictive of recurrent instability. Concomitant injuries associated with posterior shoulder dislocations include capsulolabral tears, fractures, and rotator cuff tears. Imaging studies in this patient indicate a reverse Hill-Sachs lesion with a corresponding posterior labral tear. Because of his persistent mechanical symptoms, continued immobilization and therapy is not appropriate. An open capsular shift with labral repair alone would not address symptoms related to an engaging Hill-Sachs lesion. Based upon the patient’s age, activity level, and percentage of humeral head involvement, a resurfacing arthroplasty is not recommended. Historically, the Zuckerman procedure, lesser tuberosity transfer, has been used to address symptomatic reverse Hill-Sachs lesions (20% to 40% humeral head involvement) associated with posterior shoulder dislocations. Modifications of this technique such as arthroscopic transfer of the subscapularis tendon without posterior capsulorrhaphy have proven beneficial.
- Arthroscopic capsulolabral repair with subscapularis and lesser tuberosity transfer
CLINICAL SITUATION FOR QUESTIONS 5 AND 6
A 40-year-old riveter who works in a manufacturing plant experiences gradual onset of anterior shoulder pain that started 4 months ago, and he now has a constant ache in his shoulder. His pain wakes him at night and is worsened by lifting anything at shoulder height. He does not have any radiation of pain, and neck motion does not aggravate his pain. He stopped doing riveting work 1 month ago, but the pain did not improve.
Examination shows normal motion and strength, a positive impingement sign, and tenderness over the anterior greater tuberosity. His sulcus sign is negative, and his Yergason and speed test findings are negative. He has normal scapular mechanics.
QUESTION 5
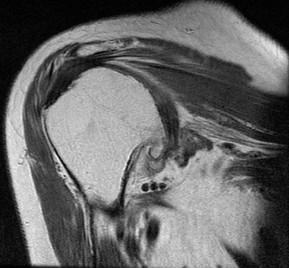
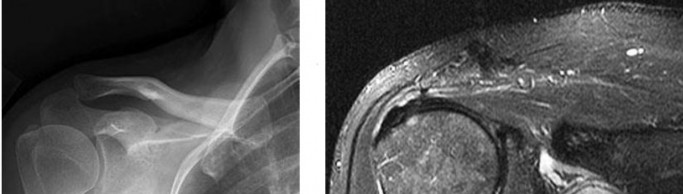
..He started physical therapy while continuing light duty at work. Eight weeks later, his pain remained unchanged. An MRI scan is shown in Figure 5. What histologic changes are likely to be found in the supraspinatus
tendon?
1
Disorganized collagen fibers with mucoid degeneration
2
Disorganized collagen fibers and acute inflammatory
3
Normal tendon fibers infiltrated with capillary proliferation
4
Normal tendon fibers infiltrated with acute inflammatory cells
DISCUSSION..This patient has impingement syndrome based on the history and examination. The best way to confirm the diagnosis is by performing a subacromial injection with lidocaine, which is also called a Neer impingement test. If the
pain is relieved, the patient’s pain is coming from the subacromial space. An MRI scan would not confirm the diagnosis of impingement, although it can aid in diagnosis of other causes of anterior shoulder pain such as a rotator cuff tear. This patient has normal rotator cuff strength, so that diagnosis is less likely. A radiograph can show acromial morphology, which would support the diagnosis of impingement, but it does not rule out impingement if the radiograph findings are normal. Ultrasound would not support the diagnosis of impingement, but, like an MRI scan, it can reveal pathologies other than impingement. The MRI scan shows a supraspinatus tendon with changes consistent with tendinopathy, which is defined by disorganized collagen fibers with mucoid degeneration on the microscopic level. Although there are always exceptions, most tendinopathy occurs without inflammatory cells or capillary proliferation.
- Subacromial injection with lidocaine
PREFERRED RESPONSE: 1- Disorganized collagen fibers with mucoid degeneration
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
A 26-year-old man has the chief complaint of right shoulder instability. He underwent an uncomplicated arthroscopic Bankart repair following an injury sustained while playing high school football. His condition was stable for 7 years, but he redislocated his shoulder in a fall 6 months ago. He describes weekly anterior instability events that he can reduce on his own. Radiographs reveal a located glenohumeral joint, but a Hill-Sachs lesion is noted. A CT scan reveals a 20% anteroinferior glenoid deficiency and a Hill-Sachs lesion involving 20% of the humeral head.
QUESTION 6
..What is the most likely predictor of postsurgical pain following a coracoid transfer procedure for recurrent shoulder instability?
1
Suboptimal graft placement
2
Pain before surgery
3
Progression of osteoarthritis
4
Previous surgical treatment
DISCUSSION…Recurrent glenohumeral instability with anteroinferior glenoid bone loss is best treated with a coracoid transfer. Schmid and associates reported on 49 patients with these lesions and recurrent instability who underwent coracoid transfer procedures. Good and excellent outcomes were reported in 88% of patients, and there were no instances of recurrent instability.
With anteroinferior glenoid bone loss, capsular procedures—whether open or arthroscopic—are unlikely to provide stability. Remplissage is a procedure designed to address Hill-Sachs lesions rather than glenoid defects. The absolute indications to treat Hill-Sachs lesions surgically include a lesion associated with a humeral head fracture, a lesion involving more than 30% of the humeral head with chronic instability, and reverse Hill-Sachs lesions involving more than 20% of
the articular surface with symptoms of posterior instability. Lesions involving 20% to 35% with or without engagement on examination are relative indications, as are lesions exceeding 10% that do not remain centered in the glenoid following arthroscopic stabilization.
In Schmid and associates’ series of coracoid transfers for recurrent instability and anterior glenoid deficiency, patients who reported pain before surgery were 20 times more likely to have pain after surgery that compromised the functional outcome. Optimal graft placement correlated with better functional outcomes and less progression of arthrosis, but not with pain. Consequently, poor graft position, arthritis progression, and prior surgical treatment are not as consistently predictive of pain after surgery.
- Coracoid transfer
P R: 4- A lesion involving 40% of the humeral head with recurrent glenohumeral instability PREFERRED RESPONSE: 2- Pain before surgery
QUESTION 7
..A 45-year-old woman with diabetes has a 3-month history of left shoulder pain and motion loss unrelated to trauma. She previously underwent treatment with nonsteroidal anti-inflammatory medication and a home stretching program, experiencing minimal relief of her symptoms. Examination reveals loss of passive external rotation, abduction, and forward elevation without reduction in strength. Radiograph findings are normal. What is the most appropriate next step?
1
MRI scan
2
Cortisone injection therapy with continued physical therapy (PT)
3
Closed manipulation under anesthesia
4
Arthroscopic release with manipulation under anesthesia
DISCUSSION..Based upon the duration of symptoms and clinical presentation, this patient would benefit from cortisone injection therapy and continued PT. Adhesive capsulitis is most commonly an idiopathic process that results in joint pain and loss of motion from capsular contracture. It affects approximately 2% to 5% of the general population. The process typically affects middle-age women. There are secondary causes such as previous trauma and fractures as well as associated medical conditions such as diabetes, stroke, and cardiac and thyroid disease. Debate remains as to whether there is a genetic predisposition for the development of adhesive capsulitis despite increased frequency noted in twin studies. Although the underlying etiology and pathophysiology are not well understood, the consensus is that synovial inflammation and capsular fibrosis result in pain and joint volume loss. It is hypothesized that in patients with diabetes, an increased rate of glycosylation and cross-linking of the shoulder capsule raises the incidence of frozen shoulder. For this patient, history reveals a short course of symptoms that did not improve with nonsurgical modalities. Clinically, the patient has reduced passive range of motion, particularly with external and internal rotation and forward elevation. Radiographs are usually obtained to exclude other causes of shoulder pain such as glenohumeral arthrosis, malignancy, calcific tendonitis, impingement, and acromioclavicular degeneration. If pain and stiffness persist beyond 6 months, closed manipulation may be an option. Complications associated with this modality may include
humerus fracture, dislocation, hematoma, rotator cuff and labral tears, and brachial plexus injury. Some surgeons advocate arthroscopic capsular release to allow for examination of concomitant pathology and controlled release of capsular tissue, with the potential for reduced required force when performing the manipulation portion of the procedure. This modality may be appropriate after an initial treatment with PT. Controversy remains as to whether posterior capsular release should be performed routinely because studies have shown outcomes to be similar with anterior and combined approaches. Therapy should be initiated early after intervention, with some surgeons advocating admission to the hospital with inpatient therapy for pain management and compliance.
- Cortisone injection therapy with continued physical therapy (PT)
QUESTION 8
..A 42-year-old woman has a posterior elbow dislocation. Closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Further treatment should consist of
1
early mobilization only.
2
surgical repair or reconstruction of the lateral collateral ligament (LCL) and the medial collateral ligament (MCL).
3
active range of motion in a hinged brace with a range of 30 degrees to 120 degrees.
4
application of a hinged external fixator with early mobilization.
DISCUSSION…This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the MCL is intact and the LCL is disrupted or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction, application of a hinged external fixator may be considered.
- early mobilization only.
RESPONSES FOR QUESTIONS 12 THROUGH 16
QUESTION 9
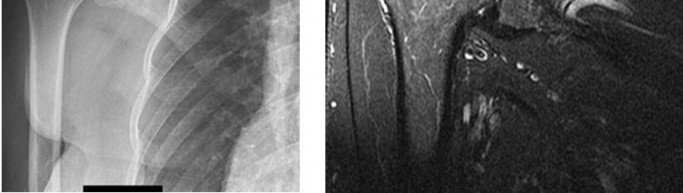
..The fracture seen in Figure 17 is most likely associated with injury to what ligamentous structure?
1
Inferior glenohumeral ligament
2
Acromioclavicular (AC) ligaments
3
Coracoclavicular ligaments
4
Coracoacromial ligament
DISCUSSION..The radiograph shows an extra-articular distal clavicle fracture lateral to the clavicular attachment point of the
coracoclavicular ligaments (conoid and trapezoid). However, unlike a scenario featuring a typical Neer type I fracture, the interval between coracoid and clavicle is clearly widened and there is marked fracture displacement. It is clear that the coracoclavicular ligaments must also be torn. The inferior glenohumeral ligament is important to glenohumeral joint stability, but has no effect on the relationship between clavicle and scapula. The AC ligaments are thickenings of the AC joint capsule. They have been shown to be responsible for 90% of anteroposterior stability of the AC joint. The coracoclavicular ligaments are responsible for 77% of stability for superior translation (as in this case). The coracoacromial ligament connects 2 parts of the scapula (coracoids and acromion) and is part of the arch that supports the rotator cuff.
- Coracoclavicular ligaments
QUESTION 10
…A 36-year-old right-hand-dominant man fell from his motorcycle and sustained the acute right upper extremity injury seen in Figure 18. At surgery, an open reduction and internal fixation of the ulna is performed along with attempted open reduction of the radiocapitellar joint. However, the radial head is slightly subluxed in flexion and redislocates with elbow extension below 90 degrees. What is the most appropriate treatment at this time?
1
Radial head resection
2
Casting in 90 degrees of flexion for 3 weeks, followed by reassessment of elbow stability
3
Repair of the annular ligament
4
Revision open reduction and internal fixation of the ulnar fracture
DISCUSSION…This case is a variant of a type I Monteggia fracture according to the Bado classification with a segmental ulna fracture. In some cases, the radial head subluxation can be subtle, and missing this would lead to a poor outcome. In this case, the anterior radial head dislocation is obvious, but the segmental nature of the ulna fracture makes anatomic reduction difficult. The radial head usually spontaneously reduces once the ulna is anatomically reduced, and no surgical treatment to the lateral side is required. When this is not the case, a lateral approach and incision of the annular ligament may be required for reduction. If an open reduction of the radial head is unsuccessful, the problem is almost always residual malalignment of the ulna. Therefore, casting and annular ligament repair will not improve reduction. A radial head resection would eliminate the nonconcentric contact between radial head and capitellum, but would not be an appropriate treatment for this young patient who has an acute, correctable fracture deformity.
- Revision open reduction and internal fixation of the ulnar fracture
QUESTION 11
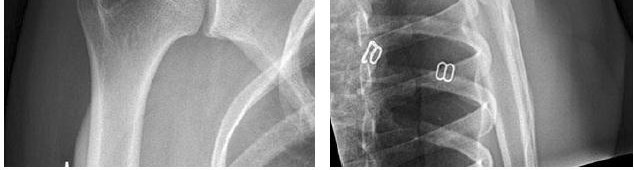
..Figure 19 is the radiograph of a 45-year-old right-hand-dominant man who has had a 2-day history of right shoulder pain, weakness, and a deformity involving the clavicle region after a fall from a scaffold during work activities. He was previously evaluated by his primary care physician and another orthopaedist. He has sought a second opinion regarding his treatment options. What is the most appropriate treatment for his injury?
1
Sling immobilization with continued observation
2
Open reduction and plate fixation
3
Open reduction, plate fixation, and application of an external bone stimulator
4
External fixation
DISCUSSION..Midshaft clavicle fractures are relatively common and account for 3% to 10% of all adult fractures. Historical studies regarding nonsurgical treatment of displaced clavicle fractures indicated a low nonunion rate approaching 1%. Contemporary studies, however, suggest that the nonunion rate is much higher, reaching 15% to 20% with corresponding loss of shoulder strength and residual deficits at 6 months from date of injury. A recent meta-analysis by McKee and associates comparing nonsurgical treatment with a sling and surgical treatment with plate fixation concluded that initial fixation of displaced midshaft clavicle fractures demonstrated a positive effect
on pain reduction at 3 weeks and improved Disabilities of the Arm, Shoulder, and Hand (DASH) scores at 6 weeks and 3 months after surgery. The choice of fixation remains a matter of debate because both plate and pin fixation have been used to achieve clavicle union. Intramedullary fixation of clavicle fractures historically has demonstrated an increased risk for pin tract infections and hardware removal attributable to local irritation from the implant. External bone stimulator use has not proven beneficial in effecting a reduction of nonunion rates. The most common complications noted with surgical intervention included local hardware irritation and wound infection.
- Open reduction and plate fixation
QUESTION 12
..A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
1
Bushing wear
2
Infection
3
Aseptic component loosening
4
Component fracture
DISCUSSION..TEA has been described for posttraumatic arthritis of the elbow and typically involves a young patient population with multiple previous operations on the affected elbow. Morrey and Schneeberger found aseptic component loosening to be uncommon (fewer than 10% of patients), and usually occurs more than 10 years after surgery. Prosthetic fracture, usually of the ulnar component, is also a late-term finding. Infection is the most common mode of early failure, but usually occurs within the first 5 years and has an overall rate of approximately 5%. Bushing wear has been reported as the most common cause of mechanical TEA failure in this population at intermediate-term followup.
- Bushing wear
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
A 21-year-old rugby player has had the sensation of shoulder instability while making tackles for 3 years. Two years ago, he had an arthroscopic Bankart repair and capsulorrhaphy that used 3 suture anchors after dislocating his shoulder while making a tackle. This procedure required an emergency department sedated reduction. After this dislocation, he had paresthesias in his arm and a sense of weakness. His numbness eventually resolved. He did well after surgery until 2 weeks ago, when he again felt his shoulder dislocate while tackling and had an emergency department reduction.
QUESTION 13
..Numbness after his first dislocation was related to
1
intrasurgical traction on the musculocutaneous nerve.
2
residual interscalene blockade.
3
ulnar neuropathy after sling use.
4
sensory axillary nerve palsy from his dislocation.
DISCUSSION..Several studies have demonstrated the equivalency of arthroscopic Bankart repair to open surgery, but most studies have also demonstrated increased recurrence rates in patients who participate in collision sports such as rugby. Revision surgery with arthroscopy is unlikely to be durable, and in patients who have large glenoid defects, a coracoid process transfer (Latarjet or Bristow) is the preferred surgical treatment. Arthroplasty would not be indicated in a young and active patient.
- His activity levels after surgery
PREFERRED RESPONSE: 4- sensory axillary nerve palsy from his dislocation.
QUESTION 14
…The patient underwent an uneventful arthroscopic repair and did well until 1 year later when she crashed during a race. She tore her anterior cruciate ligament (ACL) and underwent reconstruction. Followup after her successful ACL reconstruction reveals complaints of new shoulder pain and posterior instability from using crutches after her ACL surgery. A new MRI scan is shown in Figure 24. What factors are most likely associated
with this patient’s recurrence?
1
Gender
2
Age
3
Sport
4
Bone loss
DISCUSSION…Nonsurgical treatment for a first-time traumatic dislocation may not be effective in a young, athletic patient; moreover, a Bankart lesion may be present in 70% of all traumatic subluxations. A period of immobilization in external rotation may decrease the risk for recurrence, but only if the patient is placed in a brace immediately and complies with the treatment. Return to play may be possible after 2 weeks of immobilization, provided the patient undergoes appropriate range of motion, cuff strengthening, and scapular stabilization exercises. Among athletes in 1 study, 80% were able to finish the season, but 40% experienced episodes of subluxation or recurrent dislocation prior to the end of the season.
The rate of recurrence after arthroscopic stabilization should be lower than 10% and may be equivalent to open repair for most patients. Bone loss remains the primary indication for open procedures, as coracoid transfers or other bone-grafting operations may be needed to reconstruct the glenoid if more than 20% of its surface area is missing. Furthermore, collision athletes may fare better with open surgery than arthroscopic options. Bone loss remains the most significant factor for recurrence across many studies. Glenoid bone loss may be present in 20% of primary dislocations and 70% of recurrent dislocations. Age younger than 30 has a high correlation with recurrence. Although men may be almost twice as likely as women to have a recurrent dislocation, age seems to be the most reliable patient-related risk factor for recurrence. Thermal capsulorrhaphy has not proven to be effective and carries a high risk for complication. More recent studies have found equal recurrence rates between open and arthroscopic Bankart repair, with a greater loss of motion in patients who underwent open repair. Longitudinal studies have demonstrated that 40% to 50% are likely to develop arthritis after a shoulder dislocation; however, recurrent dislocation seems to be the most important factor for early development of arthritis, while age younger than 25 may be protective. Postcapsulorrhaphy arthropathy may be more associated with open repairs or those that severely limit external rotation.
- that 2 weeks of immobilization followed by therapy may allow her to return to finish the season.
PREFERRED RESPONSE: 2- arthroscopic Bankart repair. PREFERRED RESPONSE: 2- Age
QUESTION 15
..What is the best next step?
1
Physical therapy
2
CT scan
3
Arthroscopic capsular release
4
Arthroscopic Bankart repair
DISCUSSION..The patient has a posterior glenohumeral dislocation, as evidenced by the overlap on the initial radiograph. While posterior dislocations are rare, they can be overlooked. A CT scan will accurately show the lesion prior to a trip to the operating room. If a simple closed reduction is performed acutely and the arm is stable after the reduction, no further intervention may be needed and treatment can be successful with a 2-week period of immobilization for defects involving less than 30% of the humeral head. However, in this scenario, open reduction is likely and stabilization may require a modified McLaughlin procedure or other intervention to fill in the humeral defect.
Younger male patients, those with a large humeral head defect, and those with seizure disorder may be at highest risk for recurrence. For treatment of chronic posterior dislocations, it may be necessary to perform shoulder arthroplasty to restore stability.
Stiffness is attributable to articular incongruity; therefore, physical therapy and capsular release are inappropriate.
..A 40-year-old right-hand-dominant construction worker has a 3-month history of right shoulder weakness secondary to a fall from a ladder at work. He underwent nonsurgical treatment with anti-inflammatory medication, cortisone injections, and therapy, with minimal relief of his symptoms. A subsequent MRI scan indicates a 1-cm full-thickness supraspinatus tendon tear. He has been referred to your clinic for discussion of surgical intervention. The patient's nurse case manager is concerned that he may not be able to return to his preinjury level of activity at work, even with surgical intervention. You tell the nurse case manager that, on average, the patient will
1
be at increased risk for infection compared to patients without a Worker’s Compensation claim.
2
have significant functional improvement after rotator cuff repair that is less robust than that of patients without a Worker’s Compensation claim.
3
have pain relief that is equivalent to that of patients without a Worker’s Compensation claim.
4
return to work without restrictions within a 3-month time frame.
DISCUSSION..Many factors have been associated with less-than-favorable outcomes following rotator cuff repair such as tear size, age at time of intervention, gender, fatty degeneration of rotator cuff musculature, and Worker’s Compensation status. Henn and associates performed a prospective study regarding rotator cuff repairs in a cohort of 125 patients to assess the factors that may affect outcome as measured with the Simple Shoulder Test (SST), Disabilities of the Arm, Shoulder, and Hand (DASH), Short Form-36 (SF-36), and Visual Analog Pain Scale (VAS). When confounding factors were controlled, Worker’s Compensation status was an independent predictor of poorer DASH scores. With the use of historical controls, Bhatia and associates concluded that the vast majority (89%) of workers who underwent an arthroscopic rotator cuff repair returned to their preoperative level of work at a mean time of 7.6 months. There was a trend toward decreased return to full duty with increased work demands before surgery (light, medium, and heavy duty), but this result did reach statistical significance. Alcohol consumption (more than 6 drinks per week) was the only factor to demonstrate an association with postoperative restricted work duty and increased rotator cuff repair failure. There is no evidence to support increased infection rates for rotator cuff repair in Worker’s Compensation patients.
- have significant functional improvement after rotator cuff repair that is less robust than that of patients without a Worker’s Compensation claim.
QUESTION 17
..A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
1
Scratching the opposite shoulder
2
Pushing off an ipsilateral chair armrest to assist in standing up
3
Tying shoelaces on the contralateral foot
4
Brushing hair
DISCUSSION…Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder implanted with the deltopectoral approach; dislocation of the prosthesis is exceedingly rare if the superior approach is employed. The arm position implicated in reverse total shoulder instability is
extension, adduction, and internal rotation, such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
- Pushing off an ipsilateral chair armrest to assist in standing up
QUESTION 18
..When performing an ulnar nerve decompression at the elbow, the surgeon must be aware of the
1
median nerve as it crosses the surgical field 6 cm proximal to the medial epicondyle.
2
medial antebrachial cutaneous nerve as it crosses the field 3 cm distal to the medial epicondyle.
3
anterior antebrachial cutaneous nerve as it crosses the field at the medial epicondyle.
4
posterior antebrachial cutaneous nerve that crosses the field 2 cm distal to the medial epicondyle.
DISCUSSION..The medial antebrachial cutaneous and medial brachial cutaneous are nerves that can be injured during ulnar nerve decompression at the elbow. The medial antebrachial cutaneous nerve crosses the surgical field at an average of 3.1 cm distal to the medial epicondyle. The medial brachial cutaneous nerve crosses the field 7 cm proximal to the medial epicondyle and arborizes into 2 to 3 terminal branches. Because the surgical approach involves dissection on the medial side, the posterior antebrachial cutaneous nerve is distant from the exposure. Although the median nerve potentially can be located in the deep dissection of a submuscular transposition, it is considered distant to an in situ decompression.
- medial antebrachial cutaneous nerve as it crosses the field 3 cm distal to the medial epicondyle.
QUESTION 19
..Figure 33 is the radiograph of a 27-year-old bicyclist who crashes. He has an isolated and closed injury. He is neurovascularly intact in the upper extremity. The lateral fragment is displaced inferiorly by
1
gravity.
2
the trapezius.
3
the biceps.
4
the pectoralis minor.
DISCUSSION…Open reduction and internal fixation with a plate and screw construct have been demonstrated to reduce nonunion rate and improve outcomes compared to sling immobilization for displaced clavicle fractures. Neurovascular injury and infection risk increase, however, with surgery. In the upright position, the weight of the extremity inferiorly displaces the lateral segment.
- gravity.
QUESTION 20
..Placement of the most distal interlocking screw seen in the Figures 34a and 34b radiographs most likely resulted in what motor weakness?
1
Elbow flexion
2
Thumb interphalangeal (IP) extension
3
Index proximal IP flexion
4
Index metacarpophalangeal (MCP) abduction
DISCUSSION..The most distal locking screw in this intramedullary nail construct was placed from anterior to posterior, passing through the distal portion of the biceps and brachialis muscle bellies. The median nerve, along with the brachial artery, is at risk as it lies between these 2 muscles. Malrotation of the nail, producing a more anteromedial starting point for the screw, can lead to a path that intersects with the nerve. Blunt dissection and soft-tissue protection is warranted with this screw placement. Median nerve injury would affect innervations of the flexor digitorum superficialis and
profundus to the index finger (among other motors). Although the dissection violates the muscle belly of these 2 elbow flexors, measurable weakness is not typically seen. The radial nerve has already provided function to triceps (elbow extension) proximal to this level and lies sufficiently lateral to be more of a concern with a lateral screw placement (thumb IP extension). The ulnar nerve (index MCP abduction) is further medial at this level and would be at considerably lower risk than the median.
- Index proximal IP flexion
QUESTION 21
..One week after closed reduction of a primary anterior shoulder dislocation, a 25-year-old athlete should be counseled that
1
recurrence rate is reduced with 4 weeks of immobilization instead of 2 weeks of immobilization.
2
age at the time of injury is the most consistent risk factor for recurrent instability.
3
a majority of patients in this age group will elect to have surgery for recurrent instability.
4
after an in-season return to sports, his likelihood of choosing surgery after the season is 25%.
DISCUSSION..In a study by Sachs and associates, age younger than 25 years at the time of presentation was found to be the strongest predictor of recurrent instability. In this age group (20-to 29-year-olds), only 14% elected to proceed with surgery. After an in-season return to sports, about 50% of patients in this same study chose to proceed with surgery after completing the season. Immobilization in a sling for longer than 2 weeks has no effect on future instability.
- age at the time of injury is the most consistent risk factor for recurrent instability.
CLINICAL SITUATION FOR QUESTIONS 36 THROUGH 39
A 65-year-old man experienced 6 years of worsening shoulder pain. Examination demonstrates stiffness and crepitus with range of motion, but full rotator cuff strength in all planes. Radiographs show advanced shoulder osteoarthritis, and an MRI scan ordered by the patient's primary care physician shows an intact rotator cuff.
QUESTION 22
..At what point of glenoid retroversion is there risk for component perforation of the glenoid vault with traditional high side reaming and standard component implantation?
1
5 degrees
2
10 degrees
3
15 degrees
4
20 degrees
DISCUSSION..Posterior glenoid wear is the most common pattern seen in typical glenohumeral arthritis. Central wear can also be seen, but it is less common and anterior wear is least common. TSA is the gold standard for surgical treatment of glenohumeral osteoarthritis. Multiple comparative studies between hemiarthroplasty and total shoulder arthroplasty demonstrate advantages of TSA regarding pain relief and most functional parameters. Shoulder hemiarthroplasty with meniscal interposition has been described for young patients with glenohumeral arthritis, but outcomes at intermediate-term followup have been inferior to those of TSA. Reverse TSA is contraindicated in patients with an intact rotator cuff. Proprionobacterium acnes and Staphylococcus species are the most common pathogens causing deep infection after TSA. In a recent long-term follow-up study of total shoulder infections, male gender and younger patient age were significantly associated with a higher infection risk. Other comorbidities and indications for TSA were not predictive.
Posterior glenoid wear results in increased retroversion and erosion of the bony vault, which can compromise component fixation. Iannotti and associates reported on 13 patients with varying degrees of glenoid deformity. At 20 degrees of retroversion, optimal glenoid component placement after eccentric reaming was associated with glenoid vault perforation.
- Posterior wear
PREFERRED RESPONSE: 3- Total shoulder arthroplasty (TSA) PREFERRED RESPONSE: 2- Male gender
PREFERRED RESPONSE: 4- 20 degrees
QUESTION 23
..A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
1
Open reduction internal fixation (ORIF) with parallel plates
2
ORIF with orthogonal plates and iliac crest bone grafting
3
Total elbow arthroplasty (TEA)
4
Closed reduction and percutaneous pinning
DISCUSSION..TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF to TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared to ORIF. TEA was also likely to result in a lower resurgical rate; one-quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA vs ORIF in 24 elderly women. TEA outcomes were again superior to ORIF at a minimum of 2 years of followup. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed reduction and percutaneous pinning studies have not been published on the adult population.
- Total elbow arthroplasty (TEA)
QUESTION 24
..A 67-year-old man with right shoulder osteoarthritis remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder before surgery shows eccentric posterior glenoid wear with 10 degrees of retroversion. What is the appropriate treatment of this glenoid bone loss?
1
Implantation of the glenoid component in 10 degrees of retroversion
2
Hemiarthroplasty
3
Eccentric reaming of glenoid
4
Posterior glenoid bone graft
DISCUSSION..Total shoulder arthroplasty (TSA) is superior to hemiarthroplasty for primary osteoarthritis. The most common complication of TSA is glenoid loosening and malposition, which are common causes of glenoid failure. Glenoid malposition decreases the glenohumeral contact area and subsequently increases contact pressures. Altering the stem version to accommodate glenoid retroversion does not appropriately address soft-tissue balancing. A retroversion of less than 12 degrees to 15 degrees can be corrected with eccentric reaming without excessively compromising glenoid bone stock and risking glenoid vault penetration by the glenoid component. Posterior glenoid bone grafting may be considered for glenoid retroversion exceeding 15 degrees.
- Eccentric reaming of glenoid
QUESTION 25
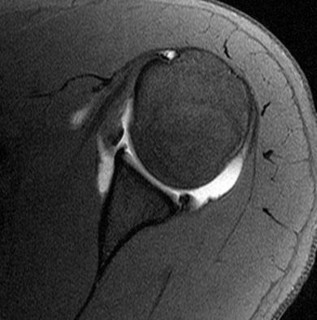
..Figure 42 is the MRI scan of a 52-year-old active man who fell from a ladder 6 weeks ago and sustained an isolated glenohumeral dislocation that was reduced in the emergency department. He wore his sling for about 2 weeks and arrived at your clinic today after referral by his primary care doctor. Examination reveals sensation intact throughout his hand, forearm, and shoulder girdle. Belly press examination findings are normal, but painful. He has tenderness to palpation on the anterior shoulder and a painful speed test. Rotator cuff repair associated with tenotomy of the indicated structure will result in what condition when compared to tenodesis of the same structure?
1
Decreased strength in forward elevation
2
Increased external rotation
3
Cosmetic deformity
4
Earlier fatigability with pronation
DISCUSSION..Patients with subluxation of the biceps tendon and full-thickness tears of the subscapularis require treatment of the biceps tendon. Studies have shown there is increased likelihood for cosmetic “Popeye” deformity after tenotomy when compared to tenodesis, but there is little or no functional
deficit associated with tenotomy. In other studies, there have been findings of supination strength reduction in patients with tenotomy compared to those with tenodesis.
- Cosmetic deformity
QUESTION 26
..A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
1
loss of elbow extensor power.
2
implant dislocation.
3
implant malposition.
4
development of heterotopic ossification.
DISCUSSION..Numerous approaches can be used to implant a total elbow arthroplasty. The Morrey approach identifies, transposes, and protects the ulnar nerve, and then subperiosteally reflects the triceps off the ulna. The sleeve of tissue is very thin distally, and the triceps need to be meticulously repaired at the time of closure. Implant dislocation and malposition are less likely with an extensile approach, and dislocation is unlikely with a semiconstrained implant. The development of heterotopic ossification is unrelated to the surgical approach used for elbow arthroplasty.
- loss of elbow extensor power.
CLINICAL SITUATION FOR QUESTIONS 44 AND 45
A 19-year-old hockey player returns home from college over holiday break and experiences multiple recurrent dislocations only 1 year after an arthroscopic stabilization.
QUESTION 27
..The treating physician opted to perform a Latarjet coracoid transfer. What is the primary mechanism of stability?
1
Capsular reinforcement by the coracoacromial ligament
2
Dynamic sling created by the conjoint tendon
3
Increased glenoid depth
4
Subscapularis tenodesis
DISCUSSION…Because bone loss is likely the biggest risk factor for this patient’s recurrence, a CT arthrogram will provide the most accurate representation of the defect. An arthrogram enhances the ability to evaluate the capsule and ligamentous attachments that may have a role in recurrent instability. Collision athletes may have a lower recurrence rate with open surgery. The Latarjet coracoid transfer achieves its primary stability through the increased glenoid surface area that the bone block provides.
..A 45-year-old woman has a 3-month history of left shoulder pain. She has tried 2 months of physical therapy focused on rotator cuff strengthening without experiencing relief. A subacromial corticosteroid injection fails to provide lasting relief. Examination reveals no atrophy or winging. She has anterior and posterior shoulder tenderness, full symmetric forward elevation and abduction, and pain with maximal passive forward elevation. She has pain with internal rotation in 90 degrees of forward elevation.
She has an increased distance between the antecubital fossa and coracoid process with cross chest adduction compared to the contralateral side. No weakness is appreciated. Radiographs reveal a type II acromion. What is the best next step?
1
Posterior capsular stretching
2
Arthroscopic subacromial decompression
3
Diagnostic acromioclavicular (AC) joint injection
4
MRI scan
DISCUSSION…This patient’s examination is consistent with posterior capsular tightness, which can mimic impingement. Four weeks of posterior capsular stretches will likely improve motion and pain. Surgical treatment should be considered only after failure of a dedicated stretching program. An AC joint injection would help differentiate this condition from AC joint arthritis, but in light of the radiographic findings, arthritis is unlikely. An MRI scan likely will not change the initial treatment at this point.
- Posterior capsular stretching
CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 49
A 13-year-old pitcher reports the immediate onset of medial elbow pain after throwing a pitch. Upon examination, the patient is tender to palpation at the medial epicondyle and has pain and instability with valgus testing of the elbow.
QUESTION 29
..If the patient were a college pitcher with a similar presentation and examination, what structure would most likely be injured?
1
Ulnar collateral ligament
2
Pronator teres
3
Ligament of Struthers
4
Lateral collateral ligament
DISCUSSION…The patient has an acute avulsion fracture of the medial epicondyle, which can occur in response to the valgus load placed on the elbow while throwing. Diagnosis is confirmed by radiograph, with comparison views of the uninjured elbow to evaluate for physeal closure vs injury. In older pitchers, the ulnar collateral ligament fails rather than the bone of the medial epicondyle.
Advanced imaging may be necessary to confirm the diagnosis of an ulnar collateral ligament injury and/or bony injury.
- Plain radiographs of both elbows PREFERRED RESPONSE: 1- To evaluate for apophyseal injury PREFERRED RESPONSE: 1- Ulnar collateral ligament
QUESTION 30
..A 21-year-old college swimmer presents with an inability to compete for longer than 1 year because of right shoulder pain and subjective symptoms of instability despite physical therapy. Recent radiographs and an MRI scan of her shoulder demonstrate an intact labral complex. Her symptoms are reproduced with sulcus testing and load and shift maneuvers in both anterior and posterior directions. What is the most appropriate next treatment step?
1
Continued physical therapy
2
Open capsular shift
3
Arthroscopic capsulolabral shift
4
Thermal capsulorrhaphy
DISCUSSION..In this scenario, the patient has already failed therapy. An MRI scan did not indicate recurrent injury to the labrum. The open capsular shift procedure initially popularized by Neer and modified by Wirth and Rockwood allows surgeons to reduce joint volume by imbricating the patulous inferior capsule through an anterior axillary-based incision. Through this anterior approach, concomitant injuries such as a humeral avulsion of the glenohumeral ligament, Bankart lesions, and subscapularis tears may be addressed. Multidirectional instability (MDI) of the shoulder is defined as symptomatic instability in more than 1 direction. Both dynamic (rotator cuff, periscapular muscles) and static stabilizers (glenoid, labrum, and joint capsule) impart stability to the glenohumeral joint. In this patient, the examination may indicate a positive sulcus sign, increased humeral head translation in more than 1 direction with the load-and-shift test, and generalized hyperlaxity such as elbow, knee, and metacarpophalangeal joint hyperextension.
Radiographs may infrequently reveal glenoid dysplasia and bone loss. MRI arthrogram imaging may demonstrate a redundant capsule without specific injury to the labral complex. Initial management of MDI involves therapy with a focus on rotator cuff and periscapular muscle strengthening. Arthroscopic capsulorrhaphy may be a viable option but is not indicated in this scenario based upon lack of injury to the labrum. As with the open capsular shift, care must be taken when performing an arthroscopic plication to avoid overreduction and subsequent shoulder stiffness. Thermal caspulorrhaphy has been abandoned as a treatment option because of high failure rate (60%) and risk for chondrolysis and axillary nerve injury.
- Open capsular shift
QUESTION 31
..What is the most appropriate treatment if instability is present at the time of evaluation?
1
TEA
2
Distal humeral replacement arthroplasty
3
Arthroscopic release with debridement
4
Soft-tissue interposition arthroplasty
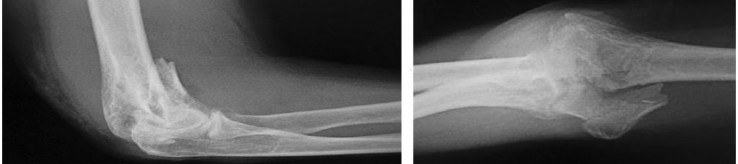
DISCUSSION..The radiographs reveal ulnohumeral arthrosis with relative sparing of the radiocapitellar articulation secondary to underlying osteoarthritis. Arthrosis of the elbow joint in this
young and active patient presents a treatment dilemma for the surgeon. Interposition arthroplasty allows for improved function with pain relief and no weight-lifting restrictions, as required with TEA. This option is an intermediate procedure that preserves bone stock and allows for conversion to a TEA if necessary. Conventional TEA would provide pain relief with improved range of motion, but activity limitation and lifetime weight restrictions make this an undesirable option. Arthroscopic debridement is not an option, considering the previous failure from this modality. Contraindications for soft-tissue interposition arthroplasty include elbow instability, active infection, and pain without motion loss. Common complications associated with this procedure include instability, infection, ulnar neuropathy, bone resorption, and heterotopic bone formation.
physical therapy and nonsteroidal anti-inflammatory medications.
2
open biopsy of the lesion for permanent section.
3
manipulation under anesthesia.
4
shoulder arthroscopy.
DISCUSSION..Calcific tendinitis of the shoulder is a deposition of calcium carbonate apatite crystals into the structure of the rotator cuff tendon. The crystalline form appears to progress throughout the clinical disease process, demonstrating increasing matured stoichiometric apatite deposition during the resorptive phase. MRI can be difficult to interpret because the signal of the calcific lesion is frequently similar to that seen in normal supraspinatus tendon. Plain radiographs remain the gold standard for diagnosis. Ultrasound can be a useful ancillary study to determine the location and size of the lesion. Primary management of calcific tendinitis starts with nonsurgical treatment including physiotherapy and injections, if indicated. Mixed results have been reported with extracorporeal shock wave therapy. Surgical removal with repair of the tendon in larger lesions remains the definitive treatment when nonsurgical modalities fail. Subacromial decompression may improve pain relief in patients who require surgery; however, patients with decompression may take longer to fully recover.
- isointense signal to the rotator cuff. PREFERRED RESPONSE: 1- calcium carbonate apatite.
PREFERRED RESPONSE: 1- physical therapy and nonsteroidal anti-inflammatory medications.
QUESTION 33
..Figure 59 is the MRI scan of a 30-year-old fire fighter who dislocated his left shoulder during work activities. His shoulder was reduced in the emergency department. After 8 weeks of physical therapy, he continues to have apprehension when lifting and pushing the fire hose back into the truck. He has normal rotator cuff strength and a negative sulcus sign. What treatment option will allow this patient to return to work as soon as possible?
1
Strengthening in physical therapy
2
Anterior labral repair
3
Posterior labral repair
4
Coracoid transfer
DISCUSSION..The MRI scan shows a posterior labral tear, which is contributing to his posterior instability. If a patient does not improve after 8 weeks of physical therapy, the therapy likely will not correct his or her instability. Activities that involve internal rotation of the shoulder and adduction will put the shoulder at most risk for posterior dislocation or subluxation. The patient elevates his risk when he pushes fire hoses into the truck repetitively, which further supports the diagnosis
of posterior instability attributable to a posterior labral tear. An anterior labral repair or a coracoid transfer would not treat posterior instability.
- Posterior labral repair
CLINICAL SITUATION FOR QUESTIONS 60 AND 61
A 10-year-old left-hand-dominant baseball pitcher has had left elbow pain for 6 weeks. His pain primarily is located medially, and he states that it is worst during the late cocking/early acceleration phase of his pitch. Recently he noticed that he is not able to throw as fast as usual. He decreased his pitch count by half during the last 2 weeks without significant improvement in his symptoms. When he is not pitching, he does not have significant pain. Radiographs show widening of the medial epicondyle physis.
QUESTION 34
..What biomechanical forces and pathology most likely underlie this patient’s pain and injury?
1
Acute avulsion of the medial epicondyle attributable to valgus stress
2
Chronic weakening of the ulnar collateral ligament attributable to chronic tension forces
3
Chronic compressive forces on the medial epicondyle leading to fragmentation
4
Chronic tension forces of valgus overload on the medial epicondyle leading to physeal separation
DISCUSSION..The medial epicondyle ossification center is first seen at 5 to 6 years of age and is the last to fuse at age 15 to 16. The capitellum first appears at age 1 to 2. The radial epicondylar epiphysis appears at 2 to 4 years. The trochlea appears at age 8 to 10; the olecranon appears at approximately age 10. The lateral epicondylar epiphysis is the last to appear at age 12.
Repetitive tensile stress on the medial epicondyle is caused by the flexor-pronator mass and the ulnar collateral ligament. This chronic valgus microtrauma eventually can lead to apophysitis and/or stress fracture. In the skeletally immature athlete, tension across the medial elbow produces a physeal injury rather than a ligamentous injury. Based upon the history, this is a repetitive overuse injury and not an acute injury.
- Appears at 5 to 6 years, fuses at 15 to 16 years
PREFERRED RESPONSE: 4- Chronic tension forces of valgus overload on the medial epicondyle leading to physeal separation
QUESTION 35
..A 35-year-old man fell off of a roof and sustained an extra-articular supracondylar elbow fracture. He had normal sensation in all fingers after the injury and before undergoing surgery to repair the fracture. The ulnar nerve was not transposed, but it was inspected prior to wound closure. Ten days after surgery, the patient has numbness in his small finger and is unable to cross his fingers. His elbow range of motion is between 40 degrees and 100 degrees. What is the next appropriate treatment step?
1
Elbow splint at 40 degrees at night for 6 weeks
2
Electromyography (EMG)
3
Exploration of the ulnar nerve and transposition
4
Observation
DISCUSSION..This patient has an early postsurgical ulnar nerve palsy. The causes of this injury are laceration of the nerve during surgery, entrapment of the nerve in the fracture or hardware, or traction injury during surgery. If the orthopaedic surgeon is sure that the nerve was not lacerated at the end of the case or entrapped in the hardware, then the nerve is probably intact and will recover. Observation is the best treatment in this case because the nerve was checked before wound closure. Elbow splinting has not been shown to help with postsurgical nerve recovery. EMG findings may not be accurate this early in the injury.
- Observation
QUESTION 36
..A 54-year-old pipefitter falls from a ladder at work and dislocates his nondominant shoulder. His MRI scan shows supraspinatus and infraspinatus tears with retraction to the glenoid. He cannot actively raise his arm away from his side. He denies prior shoulder symptoms before his fall. Three weeks of physical therapy have failed to improve his function. You and the patient decide to proceed with surgical repair. Which is a risk factor for a poor outcome?
1
The patient’s age
2
The patient’s gender
3
Work-related injury
4
Acute nature of the tear
DISCUSSION…Several studies have demonstrated that patients with work-related injuries do not do as well as those whose injuries are not work-related after repair of the rotator cuff. This patient’s age and gender are not negative prognostic indicators. The acute nature of the tear does not lead to an inferior outcome.
- Work-related injury
RESPONSES FOR QUESTIONS 64 THROUGH 68
QUESTION 37
..If nonsurgical treatment has failed, what surgical procedure will best reduce the risk for recurrent instability?
1
Diagnostic shoulder arthroscopy with labral repair
2
Diagnostic shoulder arthroscopy with open capsular shift
3
Diagnostic shoulder arthroscopy with coracoid transfer
4
Diagnostic shoulder arthroscopy with thermal capsulorrhaphy
DISCUSSION…If nonsurgical treatment has failed in the revision setting, the amount of bone loss should be quantified. The current standard for quantification of glenoid bone loss is CT scan with or without digital subtraction of the humeral head. An initial diagnostic arthroscopy may permit calculation of glenoid bone loss. The glenoid bare-spot method popularized by Lo and associates provides a reliable estimate of bone loss. Percentage of bone loss is calculated by subtracting the distance from the anterior rim to the bare spot from the posterior rim-bare spot distance divided by twice the posterior rim-bare spot distance. The critical limits of glenoid bone loss are based on a combination of cadaveric and clinical reports. Nonsurgical management may still be a reasonable choice with less than 20% glenoid bone loss in low-demand individuals, patients with high surgical risk secondary to medical comorbidities, and voluntary dislocators. When addressing recurrent anterior instability of the shoulder, it is imperative to assess both soft-tissue and bone injury.
Particular attention must be paid to glenoid and humeral head deficiencies. Patient-specific demands should be considered when discussing treatment options. In a high-demand patient such as this contact athlete, surgical treatment is appropriate. In general, if glenoid bone loss is less than 15%, a soft-tissue stabilization procedure may be all that is necessary. In those with 15% to 25% bone loss, arthroscopic stabilization with bone fragment incorporation may be performed if local bone is available. In the setting of a high-demand patient with no local bone for repair, coracoid transfer, iliac crest bone autograft, or distal tibial allograft is appropriate. With more than 25% bone loss, the glenoid deficiency must be addressed. In this scenario, the athlete demonstrates more than 25% bone loss involving the anteroinferior glenoid. This deficiency must be addressed to restore stability to the glenohumeral joint. In a high-demand patient (contact athlete), augmentation with iliac crest bone graft, distal tibial allograft, or a coracoid transfer procedure is appropriate if local bone is not available.
- CT scan
PREFERRED RESPONSE: 3- Diagnostic shoulder arthroscopy with coracoid transfer
QUESTION 38
..A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
1
Midsubstance tear of the lateral ulnar collateral ligament
2
Proximal avulsion of the ulnar collateral ligament
3
Proximal avulsion of the lateral ulnar collateral ligament
4
Distal bony avulsion of the ulnar collateral ligament from the sublime tubercle
DISCUSSION..Classic posterior elbow dislocations result from a posterolateral rotatory mechanism, whereby the hand is fixed (typically on the ground) while the weight of the body creates a valgus and external rotation moment on the elbow. This results first in tearing of the lateral collateral ligament that proceeds medially through the anterior and posterior joint capsules, ending with potential involvement of the ulnar collateral ligament (but this is not universal). McKee and associates assessed the lateral soft-tissue injury pattern of elbow dislocations with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding.
Midsubstance tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
- Proximal avulsion of the lateral ulnar collateral ligament
QUESTION 39
..A 25-year-old man is planning to have an elbow contracture release. His elbow range of motion is 40 degrees to 90 degrees of flexion. He has no heterotopic ossification. His ring and small fingers become numb as his elbow approaches his flexion endpoint. There is no evidence of instability of the ulna-humeral or radioulnar joints. To achieve the best possible outcome, the surgeon should
1
include postsurgical elbow continuous passive motion (CPM).
2
perform the surgery open.
3
decompress the ulnar nerve.
4
release the anterior band of the medial collateral ligament.
DISCUSSION..The patient is exhibiting signs of ulnar neuropathy. The surgeon should be sure to decompress and possibly transpose the ulnar nerve, if unstable, to prevent worsening neuropathy after surgery. CPM has not been shown to be of benefit after contracture release. Equal success rates have been shown for open and arthroscopic contracture releases. The anterior band of the medial collateral ligament is important to maintain valgus stability of the elbow. The posterior band can be released to improve flexion without increasing concern for elbow instability.
- decompress the ulnar nerve.
QUESTION 40
..Figures 78a and 78b are the radiographs of a 47-year-old right-hand-dominant woman who has a 3-month history of gradually progressive right shoulder pain. She reports no previous trauma, but does report pain at night and with activity such as weight training. Examination demonstrates active and passive range of motion to be 110 degrees forward elevation, external rotation to 20 degrees, and internal rotation to the sacrum. The next treatment step should include
1
an MRI of the shoulder.
2
a physical therapy referral for rotator cuff strengthening and proprioceptive exercise.
3
a home stretching program and corticosteroid injection.
4
arthroscopic glenohumeral capsular release.
DISCUSSION..This patient has idiopathic adhesive glenohumeral stiffness. Most patients with this condition are women between 40 and 60 years of age with no specific mechanism of onset.
Patients typically develop pain, at which point the disease is marked by significant inflammation. This patient is likely in the second stage of the disease, marked by inflammation and early fibrosis of the joint capsule, leading to joint stiffness. Associated conditions include diabetes mellitus and hypothyroidism, although there is no explainable cause for most cases. The most appropriate treatment step at this stage is an intra-articular glenohumeral corticosteroid injection, most often in conjunction with either a supervised or home-based capsular stretching program. Physical therapy that prioritizes toward rotator cuff strengthening is more appropriate for patients with isolated subacromial impingement syndrome and may worsen symptoms in patients with stiff shoulders. An MRI scan likely would not alter initial treatment for patients who are stiff at presentation.
Arthroscopic glenohumeral capsular release is reserved for those patients who fail initial attempts at nonsurgical management and remain functionally limited.
- a home stretching program and corticosteroid injection.
RESPONSES FOR QUESTIONS 79 THROUGH 82
QUESTION 41
..Figures 83a and 83b are the radiographs of a 53-year-old otherwise healthy homemaker who had a syncopal episode and sustained a ground-level fall and injury to her right elbow. She presently admits to right elbow pain, swelling, and an inability to bend her elbow. What is the best initial treatment for this injury?
1
Closed reduction with immobilization
2
Closed reduction with percutaneous pinning
3
Open reduction, bicolumnar fixation with plate and screws
4
Open reduction, bicolumnar fixation with Kirschner wires
DISCUSSION..The radiographs and CT scans indicate a comminuted and displaced intra-articular fracture of the distal humerus. Rigid internal fixation with bicolumnar orthogonal or parallel plating is the treatment of choice for most fractures of the distal humerus that involve the joint surface.
Closed reduction and variations thereof will not yield a stable environment for healing. To achieve
adequate exposure for fixation, a chevron olecranon osteotomy is the preferred approach. Disadvantages associated with this approach include complications such as nonunion of the osteotomy site and intra-articular adhesions. Prominent hardware may need to be removed during a secondary procedure, and intraoperative conversion to an elbow arthroplasty may be limited.
The most common complications after open reduction and internal fixation include elbow stiffness, nonunion (2%-10%), and ulnar neuropathy (0%-12%).
- Open reduction, bicolumnar fixation with plate and screws
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 87
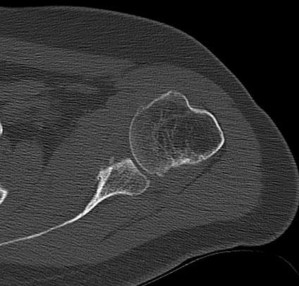
Figure 84 is the glenoid CT scan of a 20-year-old man who dislocated his shoulder anteriorly while playing football. He had persistent instability 2 months after the injury, but he did not have a sulcus sign or posterior instability. He underwent an arthroscopic Bankart repair with 4 bioabsorbable anchors with simple sutures through the labrum and capsule.
He did not have an engaging Hill-Sachs lesion, the rotator cuff was unremarkable, and the capsule was not torn from the humerus. After surgery, he did well for 6 months until he jumped into a lake and again dislocated his shoulder anteriorly. He says his shoulder no longer felt stable after his reduction.
QUESTION 42
..What is the most common late complication of the revision procedure for this patient?
1
Glenohumeral arthritis
2
Bone graft absorption
3
Anterior ligament attenuation
4
Rotator cuff tear
DISCUSSION..The CT scan shows bone loss exceeding 20% on the anterior glenoid, which is the most likely reason the arthroscopic Bankart repair failed. One study showed that using 3 or fewer anchors increases risk for failure; 4 anchors were used in this patient, so that is not the likely cause of failure. The patient returned to full activity 6 months after surgery, which is the usual time needed to regain full strength in the shoulder and ensure complete labrum healing. Suture configuration has not been shown to affect failure rates. The patient did not have signs of multidirectional instability such as a sulcus sign on examination, instability without a labral tear, or excessive translation of the humeral head posteriorly on examination. This patient has recurrent instability due to glenoid bone loss, so the procedure of choice would need to restore the anterior bone to the glenoid. The coracoid transfer procedure uses the coracoid for bone restoration, but iliac crest bone graft would be appropriate as well. An open Bankart repair, arthroscopic capsular plication, or a revision arthroscopic repair are all soft-tissue procedures, which do not correct the bone loss. Braces may work to allow a patient to finish a season before having surgery, but will not allow a return to activities of daily living without instability. The most common complication of the coracoid transfer is a loss of external rotation. The rate of recurrent instability is low. Most patients regain all of their internal rotation. The technique for the coracoid transfer splits the subscapularis muscle, so a tear of the muscle is rare. Axillary or musculocutaneous nerve palsies are rare after this procedure, but can occur if the nerves are not protected and mobilized during the dissection of the conjoint tendon. The most common long-term complication is early arthritis of the glenohumeral joint. Most cases of arthritis are asymptomatic and appear on follow-up radiographs. The graft rarely absorbs, and tears of the rotator cuff are uncommon with this procedure and infection is rare. Anterior ligament attenuation is uncommon, and some surgeons do not even repair the anterior labrum or capsule because this can lead to a loss of external rotation after surgery.
- Coracoid transfer
PREFERRED RESPONSE: 1- Loss of external rotation PREFERRED RESPONSE: 1- Glenohumeral arthritis
QUESTION 43
..Complete transection of the ulnar nerve at the elbow will result in
1
loss of sensation on the ulnar side of the index finger.
2
weakness with thumb extension.
3
weakness with elbow flexion.
4
weakness with finger abduction.
DISCUSSION..Ulnar nerve lesions manifest with weakness in the finger abductor muscles. There will be loss of interossei muscle function as well as the third and fourth lumbricals. Extensor pollicis longus function is based on the posterior interosseous nerve (radial), not the ulnar. The index
finger has sensation from the median nerve distribution. Elbow flexion strength is not dependent on the ulnar nerve.
- weakness with finger abduction.
QUESTION 44
..Figures 91a through 91d are the radiographs of an 86-year-old man who lives independently who has fallen down the stairs. He has an isolated elbow injury. What treatment option is most likely to offer the most rapid return of function and pain relief?
1
Open reduction and internal fixation (ORIF)
2
Cast treatment for 4 weeks followed by static splinting
3
Percutaneous pinning
4
Total elbow arthroplasty (TEA)
DISCUSSION...Advantages of TEA for fracture in elderly patients include preservation of the extensor mechanism, early mobilization, and avoiding complications of fixation; however, there are lifetime activity limitations and risk for loosening over time. Reoperation rates may be lower, functional outcomes improved, and results more predictable for TEA than ORIF in elderly populations. Cast treatment leads to unacceptable rates of stiffness and disability. Percutaneous fixation does not provide rigid enough fixation in the adult population.
- Total elbow arthroplasty (TEA)
QUESTION 45
…A 68-year-old right-hand-dominant man underwent a right total shoulder arthroplasty (TSA) 3 months ago. He was started on passive range of motion and started active motion 6 weeks after surgery. He notes that he fell onto his outstretched right arm 2 weeks ago but did not seek care. His primary symptom is poor active elevation of the right shoulder. His right shoulder motion has active elevation of 45 degrees, passive elevation of 140 degrees, 95-degree external rotation, and internal rotation to L3. His left shoulder has active and passive elevation of 160 degrees, external rotation of 70 degrees, and internal
rotation to T12. The right shoulder radiographs show a concentric total shoulder arthroplasty with no fractures or other abnormalities. What is the most appropriate treatment at this point?
1
Reassurance and a review of his rehabilitation program with an emphasis on deltoid strengthening
2
Open repair of the subscapularis tendon
3
Latissimus dorsi tendon transfer
4
Revision to reverse TSA
DISCUSSION..This patient had a fall approximately 2½ months following a TSA. He now has poor active elevation but good passive motion and external rotation exceeding that of the contralateral shoulder. Rupture of the subscapularis tendon, which would have been released and repaired intrasurgically, would be the primary concern in this scenario. In the native shoulder treated surgically for instability, subscapularis failure can produce pain, weakness of abdominal press and lumbar pushoff, apprehension, and frank instability. Further delay in treatment of the tendon failure with therapy is not indicated because this will lead to further muscle atrophy and adhesions to the scapula and overlying brachial plexus. Augmentation or replacement with a transfer of the superior portion of the pectoralis major muscle is sometimes required. Transfer of the pectoralis minor muscle is also described. However, latissimus dorsi transfer is described for irreparable supraspinatus deficiency. Revision to a reverse TSA can be considered as a salvage of a persistently unstable shoulder, but will not be the primary treatment for this shoulder if radiograph findings are normal.
- Open repair of the subscapularis tendon
QUESTION 46
..Figure 93 is the radiograph of a 72-year-old woman. Treatment includes fixation of the ulna. What options are recommended for the radius?
1
Radial head replacement to restore radiocapitellar contact
2
Radial head excision because there is no risk for posterolateral instability
3
Percutaneous fixation to avoid the risk for stiffness after surgery
4
Allograft reconstruction to prevent capitellar erosion
DISCUSSION..Prosthetic replacement is an appropriate option in cases of a nonreconstructable fracture to restore the radiocapitellar contact. Most complex fractures are associated with instability;
therefore, it is advisable to consider open reduction and internal fixation or radial head replacement when the injury involves a dislocation or fracture of the ulna. Simple radial head excision may be a viable option for a comminuted fracture without instability or associated ulnar fracture. When the radial head is replaced, caution must be exercised to avoid overstuffing the joint because this can lead to stiffness from impingement, capitellar erosion, loss of flexion, or synovitis.
- Radial head replacement to restore radiocapitellar contact
CLINICAL SITUATION FOR QUESTIONS 94 THROUGH 96
Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
QUESTION 47
..A common postoperative radiographic observation associated with your surgery in an asymptomatic patient is
1
implant fracture. 2- suture anchor dislodgement.
2
scapular notching. 4- acromial fracture.
DISCUSSION..The patient has anterior superior instability. This condition is caused by a combination of rotator cuff insufficiency and loss of coracoacromial arch integrity. The only known way to restore shoulder function in this scenario is to implant a rTSA. The device works by converting the translational force of the deltoid into a rotational force, resulting in restoration of forward elevation of the shoulder. Performing a rotator cuff repair or arthroscopic debridement will not address this biomechanical problem. TSA will also not change this biomechanical problem.
The poor motion and function are not a result of synovitis or pain because an injection with local anesthetic has eliminated the pain and serves as a useful test to determine if rTSA is the only viable solution. If the patient can achieve near-normal function with a local anesthetic challenge, rTSA is overtreatment. Scapular notching is a long-term concern for implant longevity because it represents bone loss under the baseplate of the glenoid component. This loss of support can lead to catastrophic failure of the device. Implant fracture, acromial fracture, and dislodgement of suture anchors are not likely to be asymptomatic in a non-Charcot joint.
- reverse total shoulder arthroplasty (rTSA).
PREFERRED RESPONSE: 1- prosthesis is designed to convert the translational force of the deltoid to rotational motion.
PREFERRED RESPONSE: 3- scapular notching.
QUESTION 48
..What complication following total elbow arthroplasty poses more risk for a 60-year-old man with osteoarthritis than for a man of the same age with rheumatoid arthritis?
1
Aseptic loosening of a linked implant
2
Instability of an unlinked implant
3
Triceps rupture
4
Wound dehiscence
DISCUSSION..Patients with elbow osteoarthritis tend to be active and are often involved in manual occupations that place greater demands on a total elbow implant. Such patients are most often treated with nonprosthetic options because of concerns about prosthetic longevity. As a result, few cases of primary osteoarthritis are included in published studies. However, complications such as stem fracture and aseptic loosening appear to be more common in this population than in any other subgroup, including revision patients. The poor soft-tissue quality associated with rheumatoid arthritis leads to a high-risk ligamentous attenuation and is a general contraindication to use of an unlinked implant. The same poor soft tissue leads to a higher rate of triceps insufficiency and wound dehiscence.
- Aseptic loosening of a linked implant
QUESTION 49
..Figure 99a is the radiograph of a 48-year-old woman 8 months after initial treatment of an injury. She initially was placed in a sling and progressive rehabilitation followed. She now has refractory pain but normal range of movement and strength. The current radiograph is shown in Figure 99b. The most appropriate next treatment step is
1
Resumption of sling immobilization
2
Open reduction and internal fixation
3
Application of a bone stimulator and rest from exacerbating activities
4
Application of a figure-of-8 brace





DISCUSSION..The radiographs reveal an atrophic nonunion of the midshaft of the clavicle. The treatment of acute, displaced midshaft clavicle fractures in adults continues to evolve, with several reports advocating early surgical intervention. Although many fractures heal, symptomatic delayed unions or nonunions occur and may eventually require treatment. In this case, further sling immobilization or use of a figure-of-8 brace is unlikely to lead to fracture consolidation at 8 months after the injury. Although use of an electrical bone stimulator may be attractive, there is no conclusive data suggesting its efficacy in promoting healing of a displaced clavicular nonunion.
Most authors advocate treatment with open reduction internal plate fixation. Controversy exists as to the need for allograft or autograft bone augmentation.
- Open reduction and internal fixation
QUESTION 50
..A 75-year-old woman sustained a 4-part fracture dislocation of the proximal humerus with a comminuted humeral head. You decide to perform a reverse total shoulder replacement because of her age and activity level. This will be your first reverse total shoulder replacement. It is common practice in your hospital for an industry representative to be present when new implants are brought into the operating room. What information are you required to disclose?
1
This is an experimental procedure.
2
You have no financial relationship with the implant company.
3
There will be an implant company representative in the room.
4
The hospital will lose money because of the cost of the implant.
DISCUSSION..Current recommendations from the American Orthopaedic Association Orthopaedic Institute of Medicine are that the patient be notified if an industry representative is going to be present in the operating room. This surgery is not experimental for this indication, and Medicare currently covers the surgery for patients with appropriate indications. Court cases have demonstrated that surgeon-related factors can be litigated (such as surgeon experience), but there are no current requirements to disclose this. Surgeons are not required to disclose cost and compensation information to their patients.
- There will be an implant company representative in the room.
RESPONSES FOR QUESTIONS 101 THROUGH 104
QUESTION 51
..Figures 105a and 105b are the radiograph and MRI scan of a 45-year-old woman with fibromyalgia that causes chronic neck and scapula pain. She has had new-onset lateral shoulder pain for 1 year. She has tenderness throughout her shoulder, back, and neck; a positive Hawkins impingement sign; and pain with resisted elevation. She tried physical therapy for 12 weeks and the pain is worse. What is the next appropriate treatment step for her shoulder pain?
1
Subacromial injection
2
Referral to pain management
3
Arthroscopic removal of a calcium deposit
4
Arthroscopic subacromial decompression






DISCUSSION…The radiographs show a calcium deposit in the supraspinatus tendon. The MRI scan shows a small black signal in the supraspinatus tendon without a tear of the tendon. These findings are consistent with calcific tendonitis. A subacromial injection will help distinguish between the pain from the calcific tendonitis and the chronic fibromyalgia. Pain management is an option after an injection is done for diagnostic purposes. Surgery should not be considered until the diagnosis is confirmed because it will not be successful if the shoulder pain is attributable to the patient’s fibromyalgia.