Here are the crucial details you must know about Ace Orthopedic MCQs: ESR in Hip & Knee Revisions. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are essential for evaluating pain after total hip arthroplasty. Drawing an erythrocyte sedimentation rate (ESR) and CRP helps assess for inflammation or infection, which are critical considerations in the differential diagnosis. These tests are part of the basic workup before recommending revision surgery for post-operative pain.
Table of Contents
Score: 0%
Ace Orthopedic MCQs: ESR in Hip & Knee Revisions
QUESTION 1
Cementless knee replacements are associated with
1
increased risk for revision.
2
increased wear of the polyethylene insert.
3
increased infection risk.
4
significantly higher Knee Society Scores (KSS).
Many published series comparing cementless to cemented knee replacements show no difference in KSS or infection risk, but data in several registries demonstrate a significant increase in the revision rates for cementless knees. Although no difference in poly wear occurred, loosening of the tibial component was the most common cause of failure. PREFERRED RESPONSE: 1
QUESTION 2
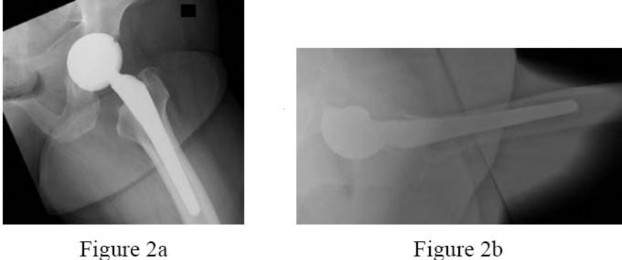
Figures 2a and 2b are the radiographs of a 56-year-old woman who has groin pain and decreased function 15 months after a total hip replacement using the posterolateral approach. Findings from the workup for infection are negative and physical examination localizes pain to the hip joint. Records show the patient underwent total hip surgery with a metal-on-metal bearing.
The patient undergoes cup revision to a more optimal position using a 36-mm metal-polyethylene bearing. Abductor muscle damage from gross metal debris and inflammation are encountered during surgery. After cup revision, repair of abductors, and hip brace use for several weeks, the patient has no more pain.Several months after surgery, the patent returns with a history of multiple hip dislocations that have proven refractory to treatment including hip precautions, bracing, and exercise. Radiographs perfectly positioned components; the patient has no pain, and examination under anesthesia shows show hip instability.
---
Before recommending revision total hip arthroplasty, what other step(s) should be included in the workup?
1
Aspiration of the hip joint and diagnostic injection of an anesthetic
2
Draw an erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
3
Three-phase bone scan of the hip
4
Lumbar spine radiographs
The differential diagnosis of pain after a total hip arthroplasty encompasses a number of etiologies, but the question is directed to a basic and essential part of the workup (ie, definitively considering and ruling in or out the possibility of deep sepsis). Radiographs may point to other, obvious sources of pain, but the orthopaedic surgeon must not overlook the possibility that deep sepsis is the predominant cause of the symptoms. Accordingly, ESR and CRP are logical next steps in the workup in this clinical scenario. Radiographs show increased anteversion of the metal socket, and pain etiologies can include psoas irritation, hip instability, or adverse tissue reaction to metal debris generated by suboptimal implant position leading to higher bearing contact stresses and/or impingement. Once other common etiologies of hip pain have been excluded such as deep infection or lumbar pathology, the most likely cause of hip symptoms should be considered. Here the evidence points to a malpositioned acetabular component. Systemic ion dissemination may occur in this patient but will not produce hip pain. Head-neck taper corrosion can generate metallic debris, but a more likely source of local metallic debris is edge loading or impingement of the metal-metal bearing. Leg length inequality can be distressing to a patient but will usually not result in hip pain. Component malposition is the best answer. Among the spectrum of clinical presentations following failed metalmetal total hip replacements, abductor damage from localized inflammation is one finding that can lead to hip instability. A reasonable treatment option is to repair the abductors as best as possible, with augmentation of soft-tissue repair using graft tissue, a large-diameter femoral head, and a constrained polyethylene liner. This is a challenging clinical scenario because chronic hip instability with deficient abductors is difficult to control and is an indication for the use of constrained components. Revision to a larger head and increased leg lengths will not address the underlying cause of instability. Hip resection is not necessary because this is not a septic total hip.
QUESTION 3
Figures 2a and 2b are the radiographs of a 56-year-old woman who has groin pain and decreased function 15 months after a total hip replacement using the posterolateral approach. Findings from the workup for infection are negative and physical examination localizes pain to the hip joint. Records show the patient underwent total hip surgery with a metal-on-metal bearing.
The patient undergoes cup revision to a more optimal position using a 36-mm metal-polyethylene bearing. Abductor muscle damage from gross metal debris and inflammation are encountered during surgery. After cup revision, repair of abductors, and hip brace use for several weeks, the patient has no more pain.Several months after surgery, the patent returns with a history of multiple hip dislocations that have proven refractory to treatment including hip precautions, bracing, and exercise. Radiographs perfectly positioned components; the patient has no pain, and examination under anesthesia shows show hip instability.
---
Before this patient’s most recent revision surgery, her symptoms were most likely related to
1
systemic metal ion debris.
2
component malposition.
3
leg length inequality.
4
Head-neck taper corrosion.
The differential diagnosis of pain after a total hip arthroplasty encompasses a number of etiologies, but the question is directed to a basic and essential part of the workup (ie, definitively considering and ruling in or out the possibility of deep sepsis). Radiographs may point to other, obvious sources of pain, but the orthopaedic surgeon must not overlook the possibility that deep sepsis is the predominant cause of the symptoms. Accordingly, ESR and CRP are logical next steps in the workup in this clinical scenario. Radiographs show increased anteversion of the metal socket, and pain etiologies can include psoas irritation, hip instability, or adverse tissue reaction to metal debris generated by suboptimal implant position leading to higher bearing contact stresses and/or impingement. Once other common etiologies of hip pain have been excluded such as deep infection or lumbar pathology, the most likely cause of hip symptoms should be considered. Here the evidence points to a malpositioned acetabular component. Systemic ion dissemination may occur in this patient but will not produce hip pain. Head-neck taper corrosion can generate metallic debris, but a more likely source of local metallic debris is edge loading or impingement of the metal-metal bearing. Leg length inequality can be distressing to a patient but will usually not result in hip pain. Component malposition is the best answer. Among the spectrum of clinical presentations following failed metalmetal total hip replacements, abductor damage from localized inflammation is one finding that can lead to hip instability. A reasonable treatment option is to repair the abductors as best as possible, with augmentation of soft-tissue repair using graft tissue, a large-diameter femoral head, and a constrained polyethylene liner. This is a challenging clinical scenario because chronic hip instability with deficient abductors is difficult to control and is an indication for the use of constrained components. Revision to a larger head and increased leg lengths will not address the underlying cause of instability. Hip resection is not necessary because this is not a septic total hip.
QUESTION 4
Figures 2a and 2b are the radiographs of a 56-year-old woman who has groin pain and decreased function 15 months after a total hip replacement using the posterolateral approach. Findings from the workup for infection are negative and physical examination localizes pain to the hip joint. Records show the patient underwent total hip surgery with a metal-on-metal bearing.
The patient undergoes cup revision to a more optimal position using a 36-mm metal-polyethylene bearing. Abductor muscle damage from gross metal debris and inflammation are encountered during surgery. After cup revision, repair of abductors, and hip brace use for several weeks, the patient has no more pain.Several months after surgery, the patent returns with a history of multiple hip dislocations that have proven refractory to treatment including hip precautions, bracing, and exercise. Radiographs perfectly positioned components; the patient has no pain, and examination under anesthesia shows show hip instability.
---
After revision surgery, this patient’s total hip remains unstable and unresponsive to nonsurgical treatment.What is the most appropriate surgical option?
1
Trochanteric advancement
2
Revision to a constrained polyethylene liner
3
Revision to the largest head size and increase leg length
4
Resection with repeat abductor repair, with staged reimplantation
The differential diagnosis of pain after a total hip arthroplasty encompasses a number of etiologies, but the question is directed to a basic and essential part of the workup (ie, definitively considering and ruling in or out the possibility of deep sepsis). Radiographs may point to other, obvious sources of pain, but the orthopaedic surgeon must not overlook the possibility that deep sepsis is the predominant cause of the symptoms. Accordingly, ESR and CRP are logical next steps in the workup in this clinical scenario. Radiographs show increased anteversion of the metal socket, and pain etiologies can include psoas irritation, hip instability, or adverse tissue reaction to metal debris generated by suboptimal implant position leading to higher bearing contact stresses and/or impingement. Once other common etiologies of hip pain have been excluded such as deep infection or lumbar pathology, the most likely cause of hip symptoms should be considered. Here the evidence points to a malpositioned acetabular component. Systemic ion dissemination may occur in this patient but will not produce hip pain. Head-neck taper corrosion can generate metallic debris, but a more likely source of local metallic debris is edge loading or impingement of the metal-metal bearing. Leg length inequality can be distressing to a patient but will usually not result in hip pain. Component malposition is the best answer. Among the spectrum of clinical presentations following failed metalmetal total hip replacements, abductor damage from localized inflammation is one finding that can lead to hip instability. A reasonable treatment option is to repair the abductors as best as possible, with augmentation of soft-tissue repair using graft tissue, a large-diameter femoral head, and a constrained polyethylene liner. This is a challenging clinical scenario because chronic hip instability with deficient abductors is difficult to control and is an indication for the use of constrained components. Revision to a larger head and increased leg lengths will not address the underlying cause of instability. Hip resection is not necessary because this is not a septic total hip.
QUESTION 5
A 67-year-old active man returns for routine follow up 12 years after hip replacement. He has no hip pain.Radiographs revealed a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components were perfectly positioned. Six months later, comparison radiographs show an increase in the size of the osteolytic lesion. A CT scan shows a well-described lesion that is 3 cm at its largest diameter and is localized around 1 screw hole with an eccentric femoral head. What treatment is appropriate,assuming well-fixed cementless total hip components exist?
1
Revision of the polyethylene liner, removal of the screw, and debridement of the osteolytic lesion with or without bone grafting
2
Revision of the acetabular component to a newer design without screws
3
Removal of the screw, revision of the polyethylene liner, and stem cell injection into the lytic lesion
4
Removal of the offending screw from the metal socket and placement of a new polyethylene liner in the existing socket
With a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected with liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings during revision surgery. Here, complete cup revision is not warranted considering the appropriate implant position. Beaule and associates reviewed 83 consecutive patients (90 hips) in which a well-fixed acetabular component was retained in clinical scenarios such as the one described; no hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, or if the osteolytic lesion is not amenable to debridement through the screw hole,acetabular component revision may be indicated.
QUESTION 6
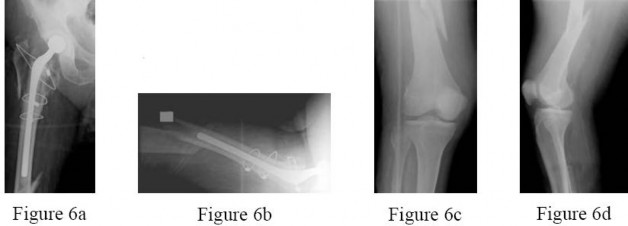
A 70-year-old man underwent removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. He was in a nursing home receiving intravenous antibiotics 3 weeks after surgery when he tripped and fell. Examination shows swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in Figures 6a through 6d. What is the most appropriate treatment for the fracture below the implant? ---
1
Balanced traction to address concern regarding persistent infection with reoperation
2
Open reduction and internal fixation of the fracture with a lateral plate and screws
3
Removal of the articulating spacer and revision to a longer-stem antibiotic-loaded articulating spacer
4
Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because it can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks to delay surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Additionally, removing the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate because it would be premature to reimplant this man’s hip while he is still receiving treatment for his deep-hip infection. PREFERRED RESPONSE: 2
QUESTION 7
What antithrombotic agent is a selective factor I0a inhibitor?
1
Warfarin
2
Low-molecular-weight heparin
3
Rivaroxaban
4
Aspirin
Rivaroxaban is a selective factor I0a inhibitor. Aspirin is a cyclooxygenase inhibitor. Low-molecularweight heparin is a nonspecific anticoagulant. Warfarin is a vitamin K antagonist and reduces production of clotting factors II, VII, IX, and X. PREFERRED RESPONSE: 3
QUESTION 8
What is the difference between annealed (below the melting temperature) and remelted highly crossedlinked polyethelyne?
1
Annealing results in lower potential for oxidation in vivo.
2
Annealing results in less change to mechanical properties and strength compared to remelting.
3
Remelting of polyethylene eliminates the potential for oxidation.
4
Remelting of the polyethylene removes the remaining free radicals and makes the polyethylene stronger.
Polyethylene is remelted to remove free radicals that formed during the radiation process for cross-linking. The disadvantage of remelting polyethylene is that it reduces the mechanical properties of the material.Annealing of polyethylene maintains its mechanical properties
but is less effective at removing free radicals, leaving the polyethylene more susceptible to oxidation. However, both annealed and remelted polyethylene have shown in vivo oxidation.
QUESTION 9
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic disease as recommended by the 2011 AAOS Clinical Practice Guideline,Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty,include
1
use of mechanical prophylaxis (eg, pneumatic calf compressors) while in the hospital.
2
oral warfarin with a goal INR between 2.0 and 3.0.
3
low-dose warfarin for 3 weeks postsurgically beginning 48 hours after surgery.
4
no prophylaxis because this patient already is partially anticoagulated secondary to her liver disease.
The 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty, recommends the use of mechanical prophylaxis for patients at increased risk for bleeding (including those with liver disease or hemophilia). This recommendation is the consensus of the workgroup that established these guidelines because there was insufficient evidence to justify a stronger recommendation in this clinical scenario. The other responses use no prophylaxis or pharmacological prophylaxis. Pharmacological prophylaxis is not recommended in patients who are at increased risk for bleeding.
---
QUESTION 10
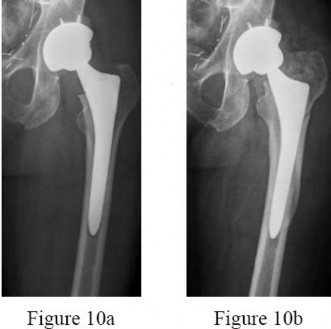
A healthy, active 72-year-old man tripped and fell, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 10a. A radiograph taken after the fall is shown in Figure 10b. He was unable to bear weight and was brought to the emergency department. Examination revealed a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin was intact without abrasions or lacerations. What is the most appropriate treatment?
1
Open reduction and cerclage fixation of the fracture
2
Open reduction and revision of the femoral implant to a long cemented stem
3
Open reduction and revision of the femoral implant to a long fluted and tapered uncemented
stem
4
Application of balanced traction and surgery after the ecchymosis has resolved
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock(Vancouver type B2). The most appropriate treatment is fixation of the fracture along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable.
Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice
listed and the most appropriate response. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site; this would pose risk for nonunion at the fracture, and overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem. PREFERRED RESPONSE: 3
QUESTION 11
A 78-year-old active woman who weighs 227 pounds has a long history of type 2 diabetes mellitus and had a total knee replacement 15 years ago. She underwent revision arthroplasty for loose components.After surgery, she fell and now has a 35-degree extensor lag with a high-riding patella on the lateral radiographic view. When attempting to surgically repair the torn extensor, gross purulence is found,leading to a resection with an antibiotic cement spacer. Enterococcus bacteria are recovered on cultures a few days later; this species is resistant to several antibiotics. The wound drains for 3 weeks and then heals with continued redness, pain, and swelling despite intravenous antibiotics. What is the most effective longterm treatment for this patient?
1
Knee fusion
2
Primary extensor repair with a hinged total knee
3
Revision total knee with extensor mechanism allograft
4
Repeat debridement and chronic antibiotic suppression
Arthrodesis may be the most satisfactory long-term option for this elderly, obese patient even though all knee motion will be lost. The other options presented are associated with unpredictable results and higher failure rates. PREFERRED RESPONSE: 1
QUESTION 12
A 65-year-old woman with type 2 diabetes mellitus and hypertension who underwent an index total knee arthroplasty (TKA) 1 year ago has a knee aspirate culture positive methicillin-resistant Staphylococcus aureus periprosthetic joint infection after 2 days of increasing pain and swelling. She states her knee“never felt right.” Her erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels are elevated. Radiographs reveal well-fixed, appropriately positioned components.
What is the most appropriate treatment?
1
Open debridement, poly exchange, and intravenous (IV) antibiotics
2
Two-stage exchange arthroplasty
3
Arthroscopic debridement
4
Resection arthroplasty
This patient has had a painful knee joint since surgery, and it is possible this is a chronic infection. In this setting, a 2-stage reimplantation procedure is most appropriate. There is no role for arthroscopic debridement and resection arthroplasty is not indicated. During the second stage, it is important to obtain cultures to confirm successful eradication of the infection. If there is clinical suspicion for persistent joint infection, an intraoperative frozen section can be indicated, but gram stain is useful. Aspiration and culture prior to the intraoperative culture should be obtained after the patient has not been taking the antibiotic for a minimum of 2 weeks. ESR and CRP trends are more valuable than the actual numbers in this setting. Finally, leukocyte-labeled imaging has no role in this setting.
QUESTION 13
A 65-year-old woman with type 2 diabetes mellitus and hypertension who underwent an index total knee arthroplasty (TKA) 1 year ago has a knee aspirate culture positive methicillin-resistant Staphylococcus aureus periprosthetic joint infection after 2 days of increasing pain and swelling. She states her knee“never felt right.” Her erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels are elevated. Radiographs reveal well-fixed, appropriately positioned components.
The patient undergoes a successful first stage that includes removal of implants and placement of an articulating spacer. IV antibiotics are administered for 6 weeks. Appropriate clinical management for this patient includes
1
leukocyte-labeled imaging.
2
reimplantation surgery only after her ESR and CRP values are within defined limits.
3
obtaining an intraoperative culture at the time of 2-stage exchange.
4
obtaining intraoperative gram stain at the time of the 2-stage exchange.
This patient has had a painful knee joint since surgery, and it is possible this is a chronic infection. In this setting, a 2-stage reimplantation procedure is most appropriate. There is no role for arthroscopic debridement and resection arthroplasty is not indicated. During the second stage, it is important to obtain cultures to confirm successful eradication of the infection. If there is clinical suspicion for persistent joint infection, an intraoperative frozen section can be indicated, but gram stain is useful. Aspiration and culture prior to the intraoperative culture should be obtained after the patient has not been taking the antibiotic for a minimum of 2 weeks. ESR and CRP trends are more valuable than the actual numbers in this setting. Finally, leukocyte-labeled imaging has no role in this setting.
QUESTION 14
A 77-year-old man who had right total knee replacement surgery 2½ years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3 and 120 degrees. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
1
Knee aspiration for culture
2
CT scan of the knee to assess implant rotation
3
Indium, technetium-sulfur colloid scan of the knee
4
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) labs
This patient’s history and physical findings are concerning for deep infection. Inflammatory markers (ESR and CRP) should first be obtained, and, if levels are elevated, proceed to knee aspiration for synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection, rarely is helpful, and is not cost effective. A CT scan to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection and when infection has been excluded.
QUESTION 15
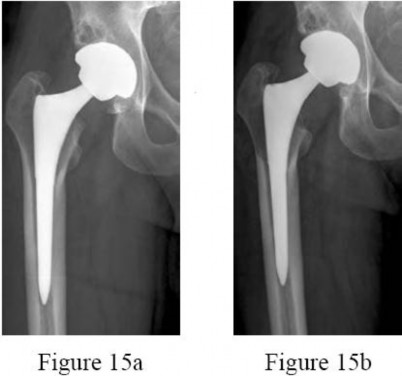
Figures 15a and 15b are the 6-week postsurgical anteroposterior hip radiograph and current radiograph of a 54-year-old avid hiker who returns for routine follow-up 3 years after an uncomplicated uncemented modular metal-on-metal hip replacement. He reports mild activity-related aching diffusely around the right hip region, but does not feel restricted with his activities. Examination reveals no local tenderness, a well-healed incision, and mild discomfort at the extremes of rotation. An erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are obtained, showing 9 mm/h (reference range, 0-20 mm/h) and 2.0 mg/L (reference range, 0.08-3.1 mg/L), respectively. What is the etiology of the radiographic finding? ---
1
Osteolysis secondary to metal particle wear (an adverse reaction to metal debris)
2
Osteolysis secondary to loosening of the femoral implant
3
Metastatic lesion to the proximal femur
4
Deep periprosthetic joint infection
The radiograph shows a large area of osteolysis involving the proximal femur. The implants appear solidly fixed on radiographs and, in the absence of symptoms, it is unlikely the implants are loose or infected. Although infection or metastatic disease is a possibility, the normal ESR and CRP values make the diagnosis of deep infection unlikely. The most likely cause for the radiographic findings is wear from metal particles resulting in an adverse local tissue response and osteolysis.
QUESTION 16
What risk factor is associated with a poor prognosis after revision of a failed metal-on-metal resurfacing hip arthroplasty to total hip arthroplasty?
1
Femoral neck fracture
2
Osteonecrosis of the femoral head
3
Aseptic loosening of the femoral component
4
Pseudotumor formation
Recent clinical series have focused on the high complication rates and problems resulting from revision cases with pseudotumor formation. Pseudotumors are probably related to very high levels of cobalt and chrome particulate wear debris. The underlying etiology most likely is edge wear or impingement that destroys the congruity of the articulation. Revision surgery was quite difficult in one series, particularly if there were large amounts of soft-tissue destruction or nerve involvement. There was a high re-revision rate, often resulting from recurrent pseudotumors with large amounts of debris that could not be removed with the initial revision. The other causes of revision that can cause failure of the femoral resurfacing component can be easily revised with a femoral stem component, and results can be nearly as favorable as with a primary hip replacement.
QUESTION 17
Ten-year follow-up studies of total hip replacements performed with modern alumina ceramic femoral heads and acetabular liners show what outcomes?
1
Low incidence of osteolysis, squeaking noise, and ceramic head fractures
2
Same incidence of osteolysis as metal-polyethylene total hips of the same design
3
Higher incidence of osteolysis in hips that make audible noises in vivo
4
Elimination of ceramic head fractures resulting from use of improved biomaterials
Ten-year follow-up data have been published from a number of clinical centers worldwide that describe the outcomes of total hip arthroplasties performed with third-generation alumina ceramic bearings (metalpolyethylene control hips often were included in the same series). These studies show no osteolysis around well-fixed metal components, and a small incidence of revision surgery to address bearing noise (squeaking) or ceramic femoral head fracture. Newer ceramic materials are associated with satisfactory outcomes in terms of elimination of wear-mediated osteolysis, but problems such as bearing noise and catastrophic femoral head failure have not been eliminated even though the risk for these complications is small and much improved compared to risk associated with earlier generations of ceramic bearings. PREFERRED RESPONSE: 1
QUESTION 18
When do most symptomatic thromboembolic events occur after undergoing total joint arthroplasty?
1
On the day of surgery
2
Within the first week after surgery
3
Between 1 week and 6 weeks after surgery
4
More than 3 months after surgery
Most clinical venous thromboembolism events occur between the second and sixth weeks after surgery. It is estimated that 10% of patients are readmitted to the hospital within the first 3 months after total hip or knee arthroplasties. Most pulmonary events on the day of surgery are related to fat embolism or cardiac events. PREFERRED RESPONSE: 3
QUESTION 19
What effect does morbid obesity (body mass index [BMI] higher than 40) have on total knee arthroplasty outcomes?
1
No difference in functional outcome
2
Complication rates are similar to those experienced by nonobese patients
3
Revision rates are similar to those experienced by nonobese patients
4
More postoperative radiolucent lines
Patients with a BMI higher than 40 are more likely than nonobese patients to have radiolucent lines on postoperative radiographs. These patients have a higher rate of complications, inferior survivorship with a higher rate of revision, and poorer function scores.
QUESTION 20
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
1
Wound vacuum-assisted closure dressing
2
IV antibiotics for 6 weeks flowed by long term oral antibiotics
3
Irrigation and debridement and polyethylene exchange
4
Two-stage debridement and reconstruction
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone may suppress the infection but will not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a 2-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture can be done presurgically and may help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the 2-stage reconstruction, however. PREFERRED RESPONSE: 4
QUESTION 21
A 66-year-old woman had fever, chills, and increasing pain in her right hip. She underwent a total hip arthroplasty using large-head metal-on-metal articulation 4 years earlier without complications. Her hip pain began about 1 month ago following several days of productive cough that her primary care physician had diagnosed as a viral illness. She had elevated serology with an erythrocyte sedimentation rate of 70mm/h (reference range, 0-20 mm/h) and C-reactive protein of 3.5 mg/L (reference range, 0.08-3.1 mg/L).There is no radiographic evidence of loosening or adverse bone remodeling around the hip arthroplasty.What is the most appropriate course of action?
1
Hip aspiration
2
Metal artifact reduction sequence (MARS) MRI
3
Initiate intravenous antibiotics
4
Assess serum metal trace element levels
This patient has a history and laboratory values highly suggestive of infection following her upperrespiratory-tract infection. Hip aspiration is the most appropriate work-up in this acute setting. Metal ion level assessment is not useful in the workup for acute infection. A MARS MRI scan would be less effective in diagnosing infection than hip aspiration. Empirical use of antibiotics is not appropriate. PREFERRED RESPONSE: 1
QUESTION 22
When comparing arthroscopic lavage and knee debridement to placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
1
Reliable and durable pain relief
2
No significant benefit for chronic osteoarthritis
3
Up to 75% pain relief for 2 months, then variable response
4
Three-month measurable pain relief, followed by recurrence
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, when knee osteoarthritis of indeterminate cause is treated with arthroscopic lavage and debridement, no discernable benefit has been found to offset the risk of surgery. Effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple time points between 1 week and 2 years after surgery. PREFERRED RESPONSE: 2
QUESTION 23
A 57-year-old woman reported pain 1 year after total knee arthroplasty (TKA). The pain was characterized as a sharp catching anterior pain that was aggravated by rising from a chair or climbing stairs. Physical examination revealed a mild effusion and a range of motion of 2 to 130 degrees with patellar crepitus. Symptoms were reproduced by resisted knee extension. Radiographs showed a wellaligned posterior-stabilized TKA without evidence of component loosening.
What is the most likely cause of this patient’s pain?
1
Patella clunk syndrome
2
Flexion gap instability
3
Polyethylene wear
4
Femoral component malrotation
Patella clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45 degrees of flexion to 30 degrees from full extension. It characteristically occurs in posterior stabilized total knees and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also be a
cause of a painful total knee arthroplasty, but is less common in posterior stabilized implants. Femoral component malrotation can be a cause of pain attributable to flexion gap imbalance or patella tracking problems. Polyethylene wear would be unlikely after just 1 year. Patella clunk syndrome can usually be successfully addressed with arthroscopic synovectomy and recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy, but will not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patella clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
QUESTION 24
A 57-year-old woman reported pain 1 year after total knee arthroplasty (TKA). The pain was characterized as a sharp catching anterior pain that was aggravated by rising from a chair or climbing stairs. Physical examination revealed a mild effusion and a range of motion of 2 to 130 degrees with patellar crepitus. Symptoms were reproduced by resisted knee extension. Radiographs showed a wellaligned posterior-stabilized TKA without evidence of component loosening.
What is the recommended treatment for this patient?
1
Physical therapy
2
Arthroscopic synovectomy
3
Tibial insert revision
4
Femoral component revision
Patella clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45 degrees of flexion to 30 degrees from full extension. It characteristically occurs in posterior stabilized total knees and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also be a
cause of a painful total knee arthroplasty, but is less common in posterior stabilized implants. Femoral component malrotation can be a cause of pain attributable to flexion gap imbalance or patella tracking problems. Polyethylene wear would be unlikely after just 1 year. Patella clunk syndrome can usually be successfully addressed with arthroscopic synovectomy and recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy, but will not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patella clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
QUESTION 25
is the anteroposterior hip radiograph of a 74-year-old healthy and active man who was seen in the office 18 months after a primary uncemented total hip replacement with a history of 3 hip dislocations.The last dislocation occurred 1 week ago and he was treated in the emergency department with a closed reduction and application of a hip abduction brace. ---
All episodes of dislocation occurred when bending forward. Aside from the episodes of dislocation, his hip functions well. Examination revealed a normal gait with good abductor strength and pain-free hip movement. What is the most appropriate next treatment step?
1
Prescribe physical therapy to work on abductor strengthening and reinforce hip position
precautions.
2
Recommend revision of the acetabular component to change cup position and increase the
head and liner size.
3
Recommend revision of the head and liner to a larger size using an elevated or oblique liner.
4
Continue use of the hip abduction brace for 6 weeks and follow with physical therapy.
This patient has had 3 hip dislocations since his hip replacement, and the radiograph shows an underanteverted cup. He will likely continue to dislocate and surgery is indicated. The anteroposterior radiograph indicates that the cup is vertically oriented and not anteverted. His acetabular component is malpositioned and should be revised to provide the highest likelihood for success. A simple head and liner exchange with a malpositioned implant is less
likely to succeed. Additionally, the radiograph shows sufficient acetabular bone stock medial to the cup. The addition of acetabular revision caries a low risk for increased morbidity and will allow a large cup with a larger femoral head with sufficient polyethylene thickness. PREFERRED RESPONSE: 2
QUESTION 26
A 67-year-old man who underwent an uncomplicated hip arthroplasty 9 years ago has had a 1-week history of groin pain with movement. Radiographs reveal a well-positioned, well-fixed cementless arthroplasty with mild eccentricity of the femoral head within the polyethylene. His serum C-reactive protein (CRP) level is 3.0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate(ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?
1
Aspiration of the hip to rule out an infectious process
2
Complete blood count with differential
3
Observation
4
Bone scan
Both CRP and ESR results are negative, so aspiration of the hip to rule out periprosthetic hip infection is not recommended. The pain may be the result of a noninfectious process such as polyethylene wear with lysis or a muscle strain. A bone scan is of limited value, as is any further bloodwork. If the symptoms continue, further imaging may be of value.
QUESTION 27
Cryotherapy has been demonstrated to achieve what effect after total knee replacement?
1
Decreased transfusion requirement
2
Improved pain, swelling, and analgesia
3
Improved range of motion at the time of discharge
4
Better long-term knee range of motion
In a meta-analysis of randomized controlled trials on the efficacy of cryotherapy after total knee arthroplasty, patients treated with cryotherapy had less blood loss but no difference in transfusion requirements. There was better range of motion at the time of discharge from the hospital. There was no improvement in pain, swelling, or analgesia requirements. Patients treated with cryotherapy did not have better long-term range of motion. PREFERRED RESPONSE: 3
QUESTION 28
Compared to retention of the native patella in primary total knee arthroplasty, routine patella resurfacing is associated with
1
no patellar complications.
2
an increased occurrence of anterior knee pain.
3
a decreased patellar fracture rate.
4
a decreased risk for revision surgery.
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in large joint registries. In addition, the retention of the native patella results in a 5.7 revision surgery rate in patients with anterior knee pain. PREFERRED RESPONSE: 4
QUESTION 29
What clinical outcome is associated with total hip replacements that have metalmetal bearings (compared to total hip replacements with metal-polyethylene bearings)?
1
Soft-tissue sarcomas
2
Similar revision rates at 5 years
3
Increased nephrotoxicity
4
Pseudotumors
Patients with metal-metal total hip bearings have higher levels of cobalt and chromium in the bloodstream,but systemic migration of wear debris from total hip bearings is also common to total hip arthroplasties with polyethylene bearings. There is no direct evidence that patients with
metal-metal total hip arthroplasties experience a higher incidence of cancer. Chromosome abnormalities have been detected in patients with metal-metal hip bearings, and the clinical consequences of this finding remain unknown.
Also, pseudotumors can form around the periprosthetic joint space in response to localized metal ion debris and the host inflammatory response, although these tumors are not specific for failed metalmetal total hip arthroplasties. Metal-on-metal hip replacements have higher revision rates compared to conventional hip replacements in multiple registry studies. Although metal-on-metal articulations have not been shown to cause renal failure, they are not recommended in patients with chronic renal insufficiency. PREFERRED RESPONSE: 4
QUESTION 30
A 55-year-old man with unilateral osteoarthritis of the hip underwent a total hip arthroplasty using cementless fixation. The acetabular cup was 52 mm and the femoral head was 28 mm and made of cobaltchromium alloy. The bearing surface was made of annealed highly cross-linked polyethylene, with an estimated thickness of 6.5 mm. What should the orthopaedic surgeon tell the patient regarding wear of the bearing surface?
1
A highly cross-linked polyethylene bearing has superior wear characteristics compared to a conventional polyethylene bearing.
2
A highly cross-linked polyethylene bearing has similar wear characteristics compared to a conventional polyethylene bearing.
3
The incidence of osteolysis is expected to be higher with highly cross-linked polyethylene than with conventional polyethylene.
4
The volumetric wear rate would be lower if a 36-mm femoral head were used.
DISCUSSION-In a prospective, randomized clinical trial of 100 patients undergoing cementless total hip arthroplasties,the investigators compared highly crossed-linked polyethylene to conventional polyethylene. All of the femoral heads were 28 mm. The mean follow-up was 6.8 years. The mean head penetration was 0.003 mm/year for the highly cross-linked polyethylene group in comparison to 0.051 mm/year for the conventional polyethylene group (P =
.006). The improved wear is seen with larger-diameter heads as well. The volumetric wear rate of highly cross-linked polyethylene is equivalent to slightly higher with a larger head than a 28-mm head. Incidence of periarticular osteolysis is lower with highly cross-linked polyethylene.
QUESTION 31
A 49-year-old active man has groin pain 3 years after undergoing an uneventful total hip replacement using a cobalt-chrome femoral head articulating against a cobalt-chrome acetabular insert. The pain intensifies with activity and travels down his thigh. Examination and radiographic evaluation are not particularly helpful; there is no evidence of spinal or vascular disease. What is the next step in the evaluation of this patient?
1
A 3-phase bone scan
2
Measurement of synovial metal ions levels
3
Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and possible hip aspiration
4
Bearing exchange to a metal-polyethylene combination
ESR, CRP, and possible hip aspiration is the most logical next step even though at some point, bearing exchange may emerge as the ultimate treatment for a metal-metal adverse reaction in this patient. But the initial workup of a patient with a painful total hip that was otherwise functioning well must include the differential diagnosis of infection, which must be excluded with an appropriate laboratory workup, clinical history, and hip aspiration. The latter study may also help to diagnose a reaction to the metal bearing;cobalt and chromium levels in the aspirate can be investigated, and the color and quantity of the aspirate can be examined along with the cell count. Serum levels of metal ions at this stage could be both helpful and difficult to interpret.
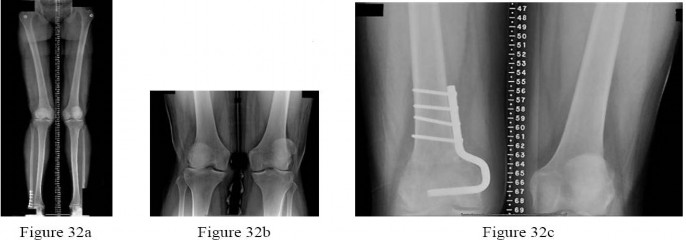
QUESTION 32
are the radiographs of a 25-year-old woman whose pain has progressed during the last several years to pain with any activity and pain at night. What is the most appropriate treatment? ---
1
Proximal tibial osteotomy
2
Distal femoral osteotomy
3
Lateral unicompartmental arthroplasty
4
Total knee arthroplasty
This patient is a good candidate for a joint-preserving procedure. Her symptoms and radiographic findings reveal valgus malalignment of the knee with narrowing of the lateral joint space. The alignment can be corrected with a varus-producing distal osteotomy as shown in Figure 32c.
Most patients do not proceed to knee arthroplasty for at least 10 years after this procedure. Osteotomy is preferred over partial or total knee arthroplasty because of the patient’s young age. Varus proximal tibial osteotomy would result in joint line obliquity. PREFERRED RESPONSE: 2
QUESTION 33
What is the plasma half-life of warfarin?
1
1 to 2 hours
2
4 to 6 hours
3
12 to 18 hours
4
36 to 42 hours
Warfarin, which is dosed daily, can take 72 to 96 hours to reach therapeutic levels. It has a plasma halflife of 36 to 42 hours. Low-molecular heparins have a plasma half-life of 4 to 5 hours, and fondaparinux has a half-life of 17 to 21 hours. Warfarin will not affect the International Normalized Ratio (INR) until 2 to 3 days after it is given. Patients on chronic warfarin therapy should have treatment stopped 3 to 5 days before elective surgery to allow the INR to normalize.
QUESTION 34
An orthopaedic surgeon noticed a displaced calcar fracture during stem insertion when performing total hip arthroplasty using cementless fixation. What is the most appropriate course of action?
1
Intraoperative exploration to determine the extent of the fracture
2
Use of a longer stem without fixation of the calcar fracture
3
Complete insertion of the stem and measures to protect the patient against full weight bearing for 4 weeks
4
Removal of the stem, internal fixation of the fracture, and definitive reconstruction at a later stage after the fracture has healed
Calcar fractures can occur with both cemented and cementless stem fixation during surgery. The dista extent of the fracture must be identified either by direct visualization or intraoperative radiograph prior to fixation or implantation of the femoral component. The recommended treatment is to fix the calcar fracture with cerclage wires/cables to restore the mechanical stability of the femoral metaphysis. The same stem can be inserted successfully. The majority of these fractures unite without adverse stem fixation problems.
QUESTION 35
A 48-year-old woman had an 8-month history of spontaneous onset of left medial knee pain. She was otherwise healthy with an unremarkable past medical history. Prior to the onset of knee pain, she jogged,played tennis, and golfed regularly. She wished to remain active. Examination showed a fit woman witha BMI of 26, a stable left knee with full range of motion, and some mild medial joint line tenderness.Radiograph results were normal. An MRI scan showed diffuse grade 3 and a focal area of grade 4 chondromalacia on the medial femoral condyle. The medial meniscus had a degenerative signal but no tear. The remainder of the knee showed no additional pathology. What is the most appropriate initial treatment?
1
Lateral heal wedge
2
Low-impact aerobic exercises
3
Glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day
4
Arthroscopic debridement and microfracture of the focal area of grade 4 chondromalacia to reduce risk for progression
This patient has early medial compartmental osteoarthritis of her knee. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), there is Level 1 evidence and an “A” recommendation for the use of low-impact aerobic exercises. The guideline also has “A” recommendations with Level 1 evidence indicating that glucosamine and chondroitin should not be prescribed and that arthroscopic debridement not be performed in the absence of symptoms of a meniscal tear or loose body. Lateral heal wedge is not appropriate; the AAOS guideline provides a “B” recommendation with Level 2 evidence indicating that a lateral heal wedge not be prescribed.
---
QUESTION 36
is the postoperative photograph of a patient who underwent a total knee arthroplasty 10 days after surgery. Knee aspiration suggests a Streptococcus infection.
1
Stop physical therapy and institute oral antibiotics.
2
Stop physical therapy and institute intravenous (IV) antibiotics.
3
Open irrigation and debridement, polyethylene spacer exchange, and IV antibiotics
4
Remove components and insert an antibiotic spacer.
_For each question below, please select the most appropriate treatment from the list above._
An acute postoperative infection during the first 2 to 4 weeks should be treated with a return to the operating room for open irrigation and debridement of the wound. Polyethylene spacer exchange aides in washing out the entire knee joint. IV antibiotics are also indicated in this situation. To address persistent wound drainage, there is no role for oral or IV antibiotics alone. Removal of the arthroplasty components is recommended for infections after the initial 2- to 4-week postoperative period.
However,several recent publications demonstrate a failure rate higher than 50% when the organism is a methicillinresistant Staphylococcus aureus. Six weeks after surgery, this scenario is no longer considered an acute postoperative infection, and most authors recommend a 2-stage protocol with removal of components and placement of an antibiotic-impregnated cement spacer and 4 to 6 weeks of IV antibiotics.
QUESTION 37
Seven weeks after total knee replacement surgery, a patient has a painful swollen knee. Knee aspiration reveals coagulase-negative Staphylococcus aureus.
1
Stop physical therapy and institute oral antibiotics.
2
Stop physical therapy and institute intravenous (IV) antibiotics.
3
Open irrigation and debridement, polyethylene spacer exchange, and IV antibiotics
4
Remove components and insert an antibiotic spacer.
_For each question below, please select the most appropriate treatment from the list above._
An acute postoperative infection during the first 2 to 4 weeks should be treated with a return to the operating room for open irrigation and debridement of the wound. Polyethylene spacer exchange aides in washing out the entire knee joint. IV antibiotics are also indicated in this situation. To address persistent wound drainage, there is no role for oral or IV antibiotics alone. Removal of the arthroplasty components is recommended for infections after the initial 2- to 4-week postoperative period.
However,several recent publications demonstrate a failure rate higher than 50% when the organism is a methicillinresistant Staphylococcus aureus. Six weeks after surgery, this scenario is no longer considered an acute postoperative infection, and most authors recommend a 2-stage protocol with removal of components and placement of an antibiotic-impregnated cement spacer and 4 to 6 weeks of IV antibiotics.
QUESTION 38
What is the difference in outcome when comparing high tibial osteotomy (HTO) to total knee arthroplasty(TKA)?
1
TKA has a longer recovery period than HTO.
2
HTO provides more complete pain relief than TKA.
3
HTO is more reliable in older patients than TKA.
4
HTO outcomes among thin, active, young patients who undergo this procedure approach outcomes associated with TKA.
The ideal candidate for HTO is a thin, active person with a stable knee, unicompartmental knee symptoms,and age younger than 60. TKA offers a shorter recovery period and more complete pain relief than HTO.TKA is believed to be more reliable than HTO for patients older than age 60. PREFERRED RESPONSE: 4
---
QUESTION 39
is a radiograph of a 72-year-old man who underwent an open reduction and internal fixation of a right femoral neck fracture. After 3 months he started to develop pain, and during the next 8 months hecomplained of progressive pain and shortening of the hip. What is the most appropriate treatment?
1
Girdlestone
2
Total hip replacement
3
Hardware removal
4
Hardware removal with revision open reductions and internal fixation
Even though a relatively short amount of time has passed since the index surgery, this patient has developed significant osteonecrosis that has caused collapse of the bony structures and the hardware prominent. Total hip replacement gives the most efficient pain relief. Hardware removal with or without re-
reduction does not provide reliable pain relief. A girdlestone does not allow the patient to function. PREFERRED RESPONSE: 2
---
QUESTION 40
is the radiograph of a 68-year-old woman who has right knee pain that is limiting her activity and severe preoperative valgus deformity. During total knee arthroplasty, what pathologic features are typically encountered?
1
Lateral femoral hypoplasia
2
Internal rotation of the tibia relative to the femur
3
Medial patella tracking
4
Tight medial collateral ligament
In patients with severe valgus deformity, problems frequently encountered include looseor attenuated medial collateral ligament, tight lateral retinaculum and lateral ligamentous structures (lateral collateral,posterolateral corner), atrophic lateral femoral condyle, lateral patella tracking, and external rotation of the tibia relative to the femur. The hypoplastic lateral condyle can cause internal rotation of the anteroposterior cutting block if the posterior condyler line is used for rotational alignment. The medial soft tissues are typically attenuated and stretched. PREFERRED RESPONSE: 1
QUESTION 41
A 72-year-old man with previous total hip arthroplasty developed hip pain of 1 month’s duration. He underwent dental work 6 weeks ago. Aspiration showed a white blood cell count of > 6000 cells/µL (reference range, 4500-11000/µL) and presence of gram-positive cocci in clusters on gram stain. The orthopaedic surgeon recommended urgent debridement and irrigation. The components were judged to be stable with regard to fixation, and the surgeon elected to retain the implants.
What is this patient’s prognosis for infection resolution?
1
Good because it is a gram-positive organism
2
Good because it is an acute infection
3
Poor because it is a gram-positive organism
4
Poor because it is a late infection
This is a late infection of at least 4 weeks symptomatic duration that most probably is hematogenous in etiology. This is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7 years of follow-up. In one study of 50 infections attributable to MRSA or methicillin-resistant Staphylococcus epidermidis organisms treated with a 2-stage protocol, the failure rate was 21%. Patients who experienced successful infection treatment had lower functional outcome measures using the WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index), UCLA (University of California Los Angeles) activity, and Oxford-12 scores, however.
QUESTION 42
A 72-year-old man with previous total hip arthroplasty developed hip pain of 1 month’s duration. He underwent dental work 6 weeks ago. Aspiration showed a white blood cell count of > 6000 cells/µL (reference range, 4500-11000/µL) and presence of gram-positive cocci in clusters on gram stain. The orthopaedic surgeon recommended urgent debridement and irrigation. The components were judged to be stable with regard to fixation, and the surgeon elected to retain the implants.
The patient had a final culture that revealed methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommended the 2-stage protocol including the use of an antibiotic-cement spacer,what is the most likely prognosis for this patient?
1
Better functional outcome in comparison to infections from sensitive organisms
2
Same functional outcome as infections from sensitive organisms
3
Same prognosis for eradication of infection as infections from sensitive organisms
4
Poorer prognosis for eradication of infection compared to infection from sensitive organisms
This is a late infection of at least 4 weeks symptomatic duration that most probably is hematogenous in etiology. This is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7 years of follow-up. In one study of 50 infections attributable to MRSA or methicillin-resistant Staphylococcus epidermidis organisms treated with a 2-stage protocol, the failure rate was 21%. Patients who experienced successful infection treatment had lower functional outcome measures using the WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index), UCLA (University of California Los Angeles) activity, and Oxford-12 scores, however.
QUESTION 43
A 59-year-old active woman underwent elective total hip replacement using a posterior approach. She had minimal pain and was discharged to home 2 days after surgery. Four weeks later she dislocated her hip while shaving her legs. She underwent a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
1
Observation and patient education regarding hip dislocation precautions
2
Revision to a larger-diameter femoral head
3
Revision to a constrained acetabular component
4
Application of a hip orthosis for 3 months
First-time early dislocations are often successfully treated without revision surgery, especially when there is no component malalignment. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful, but is usually reserved for patients with recurrent dislocations. Question 43
QUESTION 44
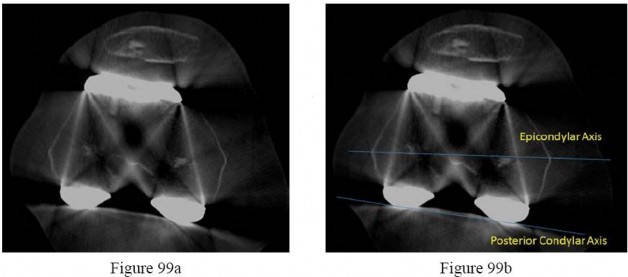
Patellar pain, subluxation, or dislocation after total knee arthroplasty can result from which of the following component orientations?
1
Internal rotation of the tibial component
2
Lateralization of the tibial component
3
Lateralization of the femoral component
4
External rotation of the femoral component
Internal rotation of the components of a total knee arthroplasty, both the tibial and femoral components,can lead to symptoms ranging from patellar pain to dislocation. Most researchers agree that proper external rotation of the femoral component is parallel or nearly so to the femoral epicondylar axis with the knee in the 90-degree flexed position. Proper rotational positioning of the tibial component places the midportion of the tibial component rotationally aligned within the medial one-third of the tibial tubercle.Internal rotation of the tibial component causes relative lateralization of the tibial tubercle and the extensor mechanism. Lateralization of the femoral component moves the trochlear groove laterally. Lateralization of the tibial component moves the tibial tubercle medially, which may be beneficial to patellar tracking.PREFERRED RESPONSE: 1
QUESTION 45
How does the risk for periprosthetic infection after total knee arthroplasty compare to risk for infection after total hip arthroplasty?
1
Higher in primary arthroplasty
2
Lower in primary arthroplasty
3
Lower in revision arthroplasty
4
Equivalent in both primary and revision arthroplasty
Risk for periprosthetic infection is higher in the knee (1%-2%) than it is in the hip (0.3%-1.3%). The risk for infection is higher after revision joint replacement surgery compared to primary joint replacement surgery. Osteoarthritis is not associated with a higher risk for periprosthetic infection, but certain inflammatory conditions such as rheumatoid arthritis and psoriatic arthritis place patients at higher risk for postoperative infection. PREFERRED RESPONSE: 1
QUESTION 46
What factor is associated with a higher risk for dislocation after total hip arthroplasty?
1
Male gender
2
Previous hip surgery
3
A direct lateral surgical approach
4
Metal-on-metal bearing surfaces
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase risk for this complication. Previous hip
surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose lower risk for dislocation. PREFERRED RESPONSE: 2
QUESTION 47
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
1
Posterior capsulorrhaphy
2
Use of a jumbo cup
3
Use of a lateralized liner
4
Use of a larger femoral head diameter
When addressing recurrent dislocation after total hip arthroplasty, surgical considerations that must be addressed include approach, soft-tissue tension, component positioning, impingement, head size, and acetabular liner profile. These considerations most often involve tensioning or augmentation of soft tissues, as in capsulorrhaphy or trochanteric advancement; correction of malpositioned components; use of larger femoral head sizes that increase motion before impingement; improving the head-to-neck ratio; and increasing femoral offset. The use of a larger-diameter acetabular component may lead to soft-tissue overgrowth around the liner, causing impingement and increasing the risk for recurrent dislocation. PREFERRED RESPONSE: 2
QUESTION 48
Viscosupplementation (hyaluronan) achieves what effect in treatment of osteoarthritis pain of the knee?
1
Alters the natural history of osteoarthritis
2
No improvement in validated outcomes
3
Rebuilds articular cartilage
4
Beneficial for treating early-to-moderate osteoarthritis
Hyaluronan is a high-molecular-weight polysaccharide. Hyaluronan has been shown effective in treating patients with early-to-moderate osteoarthritis. Hyaluronan products differ in method of production, molecular weight biologic characteristics, and pharmacologic properties.
Hyaluronan has not been shown to rebuild articular cartilage or alter the natural history of osteoarthritis. PREFERRED RESPONSE: 4
QUESTION 49
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. He has developed hip pain gradually during the last 4 months.Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. There is no periarticular osteolysis.
What is the most appropriate management of this condition?
1
Continue to observe with repeat radiographs in 6 months.
Serum cobalt and chromium levels and metal-reduction MRI scan
Controversies remain with regard to the best approach for treating patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection no differently than patients with non-MOM hip arthroplasties.
Obtaining serum trace element levels is recommended. If the levels are high, cross-sectional imaging should be obtained to determine if there is any pseudotumor or tissue necrosis around the hip arthroplasty.
Hip aspiration should be considered if there is concern for infection and if erythrocyte sedimentation rate and C-reactive protein are elevated. Aseptic lymphocytic vasculitis-associated lesions have been identified as occurring around MOM hip arthroplasties. Histologic features are predominantly tissue necrosis with infiltration of lymphocytes and plasma cells.
QUESTION 50
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. He has developed hip pain gradually during the last 4 months.Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. There is no periarticular osteolysis.
The patient developed a large intra-articular and intrapelvic pseudotumor. What predominant histological features are present in such a lesion?
1
Polymorphonuclear leukocytes
2
Extracellular metal-wear debris
3
Cement particles within the macrophages
4
Lymphocytes and plasma cells
Controversies remain with regard to the best approach for treating patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection no differently than patients with non-MOM hip arthroplasties.
Obtaining serum trace element levels is recommended. If the levels are high, cross-sectional imaging should be obtained to determine if there is any pseudotumor or tissue necrosis around the hip arthroplasty.
Hip aspiration should be considered if there is concern for infection and if erythrocyte sedimentation rate and C-reactive protein are elevated. Aseptic lymphocytic vasculitis-associated lesions have been identified as occurring around MOM hip arthroplasties. Histologic features are predominantly tissue necrosis with infiltration of lymphocytes and plasma cells.
QUESTION 51
A 72-year-old man was scheduled for left total knee replacement. He has a history of hypertension and deep venous thrombosis (DVT) in his right lower extremity after an ankle fracture 2 years ago that was treated nonsurgically. The patient asked about the recommended types of DVT prophylaxis or investigations. Based on the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty, what is an acceptable option?
1
Six weeks of acetylsalicylic acid postsurgically beginning the evening of surgery
2
Six weeks of low-molecular-weight heparin beginning the morning after surgery
3
Routine duplex scans of both lower extremities before hospital discharge to ensure the patient has not developed another DVT
4
Use of pneumatic calf compressors on both lower extremities while in the hospital and 4 weeks of warfarin starting the evening of surgery
The 2011 AAOS guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty, recommends the combined use of mechanical and pharmacological prophylaxis in patients who have a history of previous thromboembolism. This recommendation is a consensus opinion of the work group that established these guidelines because there is no other reliable evidence for this clinical scenario. There is strong evidence against the use of routine duplex scans in patients undergoing hip and knee replacement. The remaining two responses are less appropriate because they do not include the use of mechanical prophylaxis immediately after surgery. PREFERRED RESPONSE: 4
QUESTION 52
What has been identified as a risk factor for total knee arthroplasty failure after previous high tibial osteotomy?
1
Body mass index higher than 35
2
Female gender
3
Preoperative stiffness
4
Advanced age
Increased weight, male gender, young age at the time of total knee arthroplasty, laxity, and limb malalignment preoperatively have been identified as risk factors for early failure for total knee Arthroplasty following high tibial osteotomy. PREFERRED RESPONSE: 1
QUESTION 53
What limits indications for the use of constrained liners?
1
Association with periprosthetic fracture
2
Technical difficulty associated with insertion
3
High costs associated with their use
4
High failure rates associated with their use
Because of reports of relatively high failure rates associated with constrained liners, indications are limited to continued instability after appropriate component position or deficient abductor mechanism and instability. Neither cost nor technical insertion issues are relevant with regard to indications for use.Periprosthetic fractures are not associated with constrained liner usage. PREFERRED RESPONSE: 4
QUESTION 54
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has Factor V Leiden following an episode of pulmonary embolism. What are this patient’s risk factors for thromboembolic disease?
1
Type of surgery, age, and BMI
2
Type of surgery, hypercholesterolemia, and age
3
Age, BMI, and hypercholesterolemia
4
BMI, type of surgery, and hypercholesterolemia
Risk stratification is one of the most critical clinical evaluations before undergoing total joint arthroplasty.Many factors have been identified to increase risk for venous thromboembolism (VTE). The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states,myocardial infarction, congestive heart failure, family history of VTE, and hormonal replacement therapy.Hypercholesterolemia is not a risk factor for thromboembolic disease. PREFERRED RESPONSE: 1
QUESTION 55
An otherwise healthy 79-year-old man underwent a total hip arthroplasty 5 years ago. He has had a 48-hour history of groin and thigh pain and malaise. Examination reveals pain with internal motion of thehip. Radiographs show well-fixed, appropriately positioned components.
What serum inflammatory marker has the highest correlation with periprosthetic joint infection?
1
C-reactive protein
2
Serum white blood cell count
3
Erythrocyte sedimentation rate
4
Interleukin 6 (IL-6)
Although CRP and ESR can be elevated in the setting of infection, IL-6 has been shown to have the highest correlation with infection. Serum white blood cell count has been shown to be ineffective in correlating with periprosthetic joint infection. Given the history, it is likely this patient has an acute hematogenous infection. Appropriate steps including initiation of intravenous antibiotics after cultures have been obtained and medical optimization with treatment consisting of irrigation and debridement with head and liner exchange. There is no role for an indium scan or a repeat aspiration in the presence of an elevated ESR, CRP, and IL-6. There is no role for arthroscopic debridement in this case.
QUESTION 56
An otherwise healthy 79-year-old man underwent a total hip arthroplasty 5 years ago. He has had a 48-hour history of groin and thigh pain and malaise. Examination reveals pain with internal motion of thehip. Radiographs show well-fixed, appropriately positioned components.
Serum blood work reveals markedly elevated erythrocyte sedimentation rate (ESR), C-reactive protein(CRP), and IL-6 levels. Cultures from a hip aspirate reveal a low virulence staph epidermis. What is the next appropriate step in management?
1
Arthroscopic debridement
2
Reaspiration to confirm that the organism is not a contaminant
3
Indium scan to evaluate for infection
4
Irrigation and debridement and head and liner exchange
Although CRP and ESR can be elevated in the setting of infection, IL-6 has been shown to have the highest correlation with infection. Serum white blood cell count has been shown to be ineffective in correlating with periprosthetic joint infection. Given the history, it is likely this patient has an acute hematogenous infection. Appropriate steps including initiation of intravenous antibiotics after cultures have been obtained and medical optimization with treatment consisting of irrigation and debridement with head and liner exchange. There is no role for an indium scan or a repeat aspiration in the presence of an elevated ESR, CRP, and IL-6. There is no role for arthroscopic debridement in this case.
QUESTION 57
A 70-year-old man complains of symptomatic medial knee pain that has become progressively worse during the past year. An MRI scan reveals a complex posterior horn medial meniscus tear with associated medial and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable symptom relief?
1
High tibial osteotomy
2
Total knee replacement
3
Unicondylar knee replacement
4
Arthroscopic partial menisectomy
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus, but not osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for singlecompartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee. PREFERRED RESPONSE: 2
QUESTION 5
A 68-year-old man reports hip pain 15 years after successful cementless total hip arthroplasty.Radiographs show 3 mm of linear wear of the modular acetabular liner and a retro-acetabular osteolytic lesion. Both the titanium femoral and acetabular components appear to be well fixed. The orthopaedic surgeon recommends revision of the acetabular liner and femoral head. This patient is at increased risk for
1
dislocation.
2
periprosthetic fracture.
3
infection.
4
progressive osteolysis.
Isolated acetabular liner revision is frequently performed in cases of liner wear and periprosthetic osteolysis in the absence of acetabular component loosening. Many reports have documented an increased incidence of dislocation following this type of revision surgery. This dislocation rate can be reduced by using a larger-diameter femoral head at the time of revision. If the acetabular component is loose or malpositioned, it should be revised. If the locking mechanism is damaged, then a replacement liner may be cemented into the well-fixed shell. Numerous studies have shown that many osteolytic lesions will reduce in size or heal without bone grafting, and removal of the source of wear debris will arrest the progression of osteolysis. The risk for periprosthetic fracture and infection are lower than risk for dislocation in this setting. PREFERRED RESPONSE: 1
QUESTION 59
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain.Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
1
glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day.
2
weight loss through dietary management and low-impact aerobic exercises.
3
arthroscopic debridement and lavage.
4
a valgus-directing brace.
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee(Non-Arthroplasty), Level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day and arthroscopic debridement and lavage). PREFERRED RESPONSE: 2
QUESTION 60
show the intraoperative photograph, anteroposterior radiograph, and axial MRI scan of a 63-year-old man who had right groin pain 18 months after undergoing an uncemented right total hip replacement using a modular femoral neck implant and a metal-on-polyethylene bearing. His laboratory studies revealed an erythrocyte sedimentation rate of 8 mm/h (reference range, 0-20 mm/h) and C-reactive protein level of 5.4 mg/L (reference range, 0.08-3.1 mg/L). A preoperative aspiration revealed cultures that were negative for infection. A cell could not be obtained for evaluation because the cells were “degenerative.” At the time of surgery the joint fluid was turbid in appearance; the periarticular tissues appeared avascular and tan/beige in color. An intraoperative frozen section was negative for acute inflammation. The implants were solidly fixed to bone. The cause of this patient’s symptoms and the intraoperative findings most likely are attributable to ---
1
“backside” polyethylene wear.
2
metal debris.
3
soft-tissue sarcoma.
4
iliopsoas tendonitis.
Metal debris has caused an adverse local soft-tissue response in this scenario. The laboratory studies are all negative for infection. The MRI scan shows a large soft-tissue mass that is posterior to the hip and originating from the hip joint. The dysvascular appearance of the tissues is typical for an adverse tissue response to metal. Even though the bearing is polyethylene, the modular junctions created sufficient metal debris to cause the reaction. Figures 60d and 60e show metal debris inside of the removed femoral head and corrosion of the modular neck. The other diagnoses are not consistent with this clinical presentation. PREFERRED RESPONSE: 2
QUESTION 61
The range of knee mobility after total knee replacement is multifactorial and dependent upon implant design, surgical implantation accuracy, and patient-specific variables. What total knee implant design is associated with the most knee flexion after total knee replacement?
1
Highly conforming articular surface geometry
2
Higher-flexion femoral component design manufactured to allow the most knee flexion
3
Posterior cruciate-stabilized implant, with or without a higher flexion manufacturing modification
4
Posterior cruciate-retaining design with a mobile bearing, custom implanted based on CT scan Data
A posterior cruciate-stabilized implant has the best support in the literature in terms of the most favorable range of motion after knee arthroplasty, regardless of whether the femoral component is designed with a higher flexion variation. The higher flexion design is a manufacturing variation that is intended to increase motion by clearing the posterior condyles in flexion. Although the knee may not gain more flexion, this design allows for more safety in deep flexion. The long-term outcomes of increased stresses on the polyethylene are not known, however. By itself, a higher-flexion design does not lead to increased knee mobility. The effects of mobile bearings, custom CT scan-based knee implantation, and highly conforming designs on ultimate knee range of motion are uncertain.
QUESTION 62
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
1
Increased ductility
2
Increased wettability
3
Diminished fatigue strength
4
Decreased resistance to abrasive wear
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been identified as causing implant failure in most recent clinical trials, but remain the most important mechanical issues associated with current material processing methods. PREFERRED RESPONSE: 3
QUESTION 63
What factor is associated with a high risk for developing pseudotumors after metal-on-metal hip resurfacing?
1
Large-diameter components
2
Age 40 or older for men
3
Age 40 or younger for women
4
Diagnosis of primary osteoarthritis
The recent experience of a large clinical cohort revealed the most likely risk factors as female gender, age younger than 40, small components, and the diagnosis of hip dysplasia causing osteoarthritis. Failure was least likely among men and procedures involving larger components. These data have prompted some authors to caution against use in women and to primarily target candidates who are men younger than age 50. Small components may be more prone to failure because of malpositioning and edge loading, which have been noted to be more common in dysplasia cases.
QUESTION 64
---
Figure 64 is the radiograph of a 77-year-old woman with a painful total hip arthroplasty (THA) who had surgery 15 years ago. Preoperative laboratory studies reveal a C-reactive protein (CRP) of 4 mg/L(reference range, 0.08-3.1 mg/L). Her serum white blood cell (WBC) count and differential values are within defined limits, and her erythrocyte sedimentation rate (ESR) is 35 mm/h (reference range, 0-20mm/h).
What is the next appropriate step in management of the patient?
1
Labeled WBC scan
2
MRI scan of the hip to evaluate for fluid collection
3
Revision THA with gram stain and multiple cultures
4
Aspiration with cell count and differential and culture
Aspiration is appropriate in the setting of a failed total joint replacement when ESR and CRP are elevated,even with a normal systemic WBC count. A MRI scan of the hip is not useful in this setting. A labeled WBC scan is of no additional value when an aspiration of the hip is planned. Although multiple cultures should be obtained at the time of revision THA, preoperative aspiration is appropriate in this case. Most acetabular revisions can be accomplished with a cementless hemispherical component.
Supplemental fixation with screws is indicated. In this patient, the acetabular rim and columns are intact and the first choice is a cementless hemispherical component. Bilobed components have an unacceptably high failure rate and are not indicated when the acetabular rim is intact. A cemented all-polyethylene shell is not likely to achieve adequate long-term fixation with the sclerotic acetabular bone. An antiprotrusio device is indicated in the setting of severe bone loss or pelvic discontinuity. An antiprotrusio cage is the best choice in the setting of a pelvic discontinuity that has the capacity to heal. If the discontinuity does not have the capacity to heal, it can be treated in distraction with an acetabular allograft supported by a cage or custom triflange component. A large porous cup is not likely to achieve stable fixation and will require removal of more acetabular bone. A cemented acetabular component will not achieve adequate stability or fixation in the absence of additional support. Resection arthroplasty would not be the first choice in a potentially reconstructable situation. PREFERRED RESPONSE: 3
QUESTION 65
---
Figure 64 is the radiograph of a 77-year-old woman with a painful total hip arthroplasty (THA) who had surgery 15 years ago. Preoperative laboratory studies reveal a C-reactive protein (CRP) of 4 mg/L(reference range, 0.08-3.1 mg/L). Her serum white blood cell (WBC) count and differential values are within defined limits, and her erythrocyte sedimentation rate (ESR) is 35 mm/h (reference range, 0-20mm/h).
At the time of revision THA, the acetabular defect is confined to a contained cavitary defect in the dome. Anterior and posterior columns are intact, as is the rim. What is the most appropriate acetabular reconstruction?
1
Bilobed or “double bubble” acetabular component
2
Cementless acetabular hemisphere with multiple screws
3
Cemented all-polyethylene shell
4
Antiprotrusio cage device
Aspiration is appropriate in the setting of a failed total joint replacement when ESR and CRP are elevated,even with a normal systemic WBC count. A MRI scan of the hip is not useful in this setting. A labeled WBC scan is of no additional value when an aspiration of the hip is planned. Although multiple cultures should be obtained at the time of revision THA, preoperative aspiration is appropriate in this case. Most acetabular revisions can be accomplished with a cementless hemispherical component.
Supplemental fixation with screws is indicated. In this patient, the acetabular rim and columns are intact and the first choice is a cementless hemispherical component. Bilobed components have an unacceptably high failure rate and are not indicated when the acetabular rim is intact. A cemented all-polyethylene shell is not likely to achieve adequate long-term fixation with the sclerotic acetabular bone. An antiprotrusio device is indicated in the setting of severe bone loss or pelvic discontinuity. An antiprotrusio cage is the best choice in the setting of a pelvic discontinuity that has the capacity to heal. If the discontinuity does not have the capacity to heal, it can be treated in distraction with an acetabular allograft supported by a cage or custom triflange component. A large porous cup is not likely to achieve stable fixation and will require removal of more acetabular bone. A cemented acetabular component will not achieve adequate stability or fixation in the absence of additional support. Resection arthroplasty would not be the first choice in a potentially reconstructable situation. PREFERRED RESPONSE: 3
QUESTION 66
---
Figure 64 is the radiograph of a 77-year-old woman with a painful total hip arthroplasty (THA) who had surgery 15 years ago. Preoperative laboratory studies reveal a C-reactive protein (CRP) of 4 mg/L(reference range, 0.08-3.1 mg/L). Her serum white blood cell (WBC) count and differential values are within defined limits, and her erythrocyte sedimentation rate (ESR) is 35 mm/h (reference range, 0-20mm/h).
During the revision, a large anterior column defect secondary to reaming is noted. At the time of impaction of the acetabular component, a loss of resistance is noted and the shell is unstable. After removing the shell, a fracture through the posterior column is noted. What is the most appropriate course of action?
1
Resection arthroplasty
2
Distraction of the fracture with a large porous acetabular component
3
Acetabular antiprotrusio cage with screw fixation
4
Revision of the acetabular component with allograft and a cemented socket
Aspiration is appropriate in the setting of a failed total joint replacement when ESR and CRP are elevated,even with a normal systemic WBC count. A MRI scan of the hip is not useful in this setting. A labeled WBC scan is of no additional value when an aspiration of the hip is planned. Although multiple cultures should be obtained at the time of revision THA, preoperative aspiration is appropriate in this case. Most acetabular revisions can be accomplished with a cementless hemispherical component.
Supplemental fixation with screws is indicated. In this patient, the acetabular rim and columns are intact and the first choice is a cementless hemispherical component. Bilobed components have an unacceptably high failure rate and are not indicated when the acetabular rim is intact. A cemented all-polyethylene shell is not likely to achieve adequate long-term fixation with the sclerotic acetabular bone. An antiprotrusio device is indicated in the setting of severe bone loss or pelvic discontinuity. An antiprotrusio cage is the best choice in the setting of a pelvic discontinuity that has the capacity to heal. If the discontinuity does not have the capacity to heal, it can be treated in distraction with an acetabular allograft supported by a cage or custom triflange component. A large porous cup is not likely to achieve stable fixation and will require removal of more acetabular bone. A cemented acetabular component will not achieve adequate stability or fixation in the absence of additional support. Resection arthroplasty would not be the first choice in a potentially reconstructable situation. PREFERRED RESPONSE: 3
QUESTION 67
a is the radiograph of a 78-year-old woman who has a recent history of increasing thigh pain 12 years after undergoing total hip arthroplasty. Figure 67b is the radiograph after she fell and was unable to ambulate. What is the most appropriate treatment? ---
1
Application of a femoral cable plate
2
Application of cerclage-wired double allograft femoral struts
3
Femoral revision with an uncemented long stem
4
Femoral revision with a cemented long-stem prosthesis
Surgical treatment of periprosthetic fractures of total hip replacement with a loose implant and progressive bone loss is associated with a high complication rate. Recent literature would favor the use of long “Wagner-type” stems that have a long distal taper that may optimally engage the remaining femoral shaft isthmus. Plating options are problematic because the ability to use screws with the plate is limited by the intramedullary stem. Use of long distally fixed stems circumvents this problem by enhancing fracture and healing and creating a long-term prosthetic solution in these most difficult cases.
QUESTION 68
What criterion is most reliable when attempting to establish a diagnosis of chronic periprosthetic joint infection (PJI) of the hip and knee?
1
Positive bone scan
2
Elevated erythrocyte sedimentation rate (ESR)
3
Elevated serum white blood cell (WBC) count
4
Aspiration with > 2500 WBC per mm3
Aspiration with a cell count in the joint fluid that yields a WBC higher than 2500 per mm3 is consistent with infection. ESR and C-reactive protein should be obtained when evaluating a patient for PJI. Joint aspiration should be performed for patients being investigated for PJI when CRP and/or ESR values are outside defined limits. PREFERRED RESPONSE: 4
QUESTION 69
A 70-year-old man is scheduled to undergo bearing surface revision for wear and osteolysis 10 years after cementless total hip arthroplasty. The femoral head is 28 mm alumina-oxide ceramic material. The components are in good position, and there is no evidence of fixation loosening of either component by radiograph or preoperative bone scan. What outcome is associated with isolated polyethylene exchange?
1
Reduced risk for future wear and osteolysis with a larger femoral head
2
Reduced risk for future wear and osteolysis with a cobalt chrome femoral head
3
Similar risk for dislocation compared to primary total hip arthroplasty
4
Increased risk for dislocation compared to primary total hip arthroplasty
The major complication associated with polyethylene exchange is postoperative dislocation. Maloney and associates noted a dislocation rate of 11% in a study of 35 hips after such revision. Boucher and associates reported a 25% rate of dislocation in a study of 25 patients. Larger femoral heads result in higher volumetric wear in contrast to smaller-diameter heads. Stem revision is not indicated because there is no fixation loosening. Moreover, stem biomaterial has no effect on polyethylene wear.
QUESTION 70
A healthy, active 68-year-old woman had a total hip arthroplasty 3 months ago. She has been to the emergency department with a posterior dislocation 3 times during the last 2 months. Plain radiographs and a CT scan confirm that the acetabular component is oriented in 5 degrees of retroversion and 55 degrees of abduction. What is the most appropriate treatment?
1
Revision of the femoral and acetabular components
2
Maximizing head-neck ratio and increasing head length
3
Acetabular component revision
4
Closed reduction with an abduction brace and reinforcement of hip precautions
Acetabular malposition can lead to recurrent instability. When this cause is confirmed, reorientation of the component can lead to successful revision surgery. Revision of the femoral component may not be necessary if the acetabular component is repositioned. Increasing length and maximizing head-neck ratio cannot make up for component malposition. There is no role for nonsurgical treatment in the setting of recurrent instability with component malposition in an active, healthy patient. PREFERRED RESPONSE: 3
QUESTION 71
A 55-year-old woman with history of HIV infection is scheduled for revision total knee arthroplasty to address instability. The index surgery was done 3 years ago. What is the white blood cell (WBC) count threshold in the synovial fluid for an infection diagnosis? 1/. 100000
2/. 25000
3/. 2500
4/. 250
1
Option 1
2
Option 2
3
Option 3
4
Option 4
Numerous centers have published data supporting the use of synovial fluid WBC level as one of the most accurate diagnostic criterion for infection in total joint arthroplasty. The threshold ranges between 2000 and 3000 WBC/mL. The sensitivity and specificity have been demonstrated to be higher than 90%. PREFERRED RESPONSE: 3
QUESTION 72
What is the most common complication after a total hip replacement done through the anterior (Smith-Peterson) approach?
1
Lateral femoral cutaneous nerve injury
2
Heterotopic ossification
3
Femoral nerve palsy
4
Anterior dislocation
Responses 2, 3, and 4 can occur after anterior-approach total hip replacement, but their incidence is much lower than that of thigh numbness, which is associated with injury to the lateral femoral cutaneous nerve. This injury is usually clinically inconsequential. Goulding and associates investigated the incidence of lateral femoral cutaneous nerve injury after anterior hip replacement using self-administered questionnaires to assess sensory deficits and various functional scores for up to 1 year after surgery. Among patients, 81% reported some alteration in thigh sensation, but functional scores did not show any limitations. Symptoms also decreased over time and only a small number of patients reported complete resolution. Also, hip injections administered from the anterior direction risk injury to the lateral femoral cutaneous nerve. Patients undergoing anterior total hip replacement should be counseled about this specific risk before surgery. PREFERRED RESPOE: 1
QUESTION 73
is the anteroposterior pelvis radiograph of a 58-year-old woman who reported chronic hip pain and a clunking sensation 18 months after hip surgery. Laboratory test findings are negative for infection.What is the most appropriate treatment? ---
1
Revision total hip arthroplasty
2
Trochanteric bursa injection
3
Acetabular component revision
4
A course of physical therapy
The radiograph shows a metal-on-metal hip resurfacing arthroplasty. The acetabular component is malpositioned in excessive abduction, which may explain the clunking symptoms and be allowing the joint to subluxate. The best option is to convert this failed surface replacement to a conventional total hip arthroplasty. Metal-on-metal bearings pose risk for synovitis, metallosis, and adverse tissue reactions, particularly when the acetabular component is malpositioned, resulting in edge loading (this patient’s situation). Acetabular revision is possible, but would leave the patient with a metal-on-metal bearing and higher risk for failure attributable to a metal debris reaction and a damaged femoral head component. PREFERRED RESPONSE: 1
QUESTION 74
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
1
Staphylococcus epidermidis
2
Streptococcus viridans
3
Propionibacterium acnes
4
Staphylococcus aureus
Staphylococcus aureus is the most common organism cultured in early (fewer than 4 weeks postoperative)periprosthetic infections. Methicillin-resistant Staphylococcus aureus is becoming a more common pathogen in certain patient populations. B-hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. Staphylococcus epidermidis, Streptococcus viridans,and Propionibacterium acnes are more commonly found in late (> 4 weeks postoperative) infections. PREFERRED RESPONSE: 4
QUESTION 75
Figures 75a through 75c are the radiographs and CT scan of a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when she actively flexed her hip. She had trouble walking up stairs and getting out of her car.
---
What is the most likely diagnosis?
1
Trochanteric bursitis
2
Femoral component loosening
3
Iliopsoas tendonitis
4
Acetabular component loosening
There are a number of possible causes of groin pain after total hip replacement, but an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated,diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms, or in any patient with a metal-on-metal bearing. This patient’s symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT scan show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning is indicated. Fluoroscopic-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well-positioned, then iliopsoas tenotomy should be considered.
QUESTION 76
Figures 75a through 75c are the radiographs and CT scan of a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when she actively flexed her hip. She had trouble walking up stairs and getting out of her car.
---
This patient failed a course of appropriate nonsurgical treatment. What is the next step in definitive treatment?
1
Acetabular component revision
2
Femoral component revision
3
Acetabular liner exchange
4
Trochanteric bursectomy
There are a number of possible causes of groin pain after total hip replacement, but an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated,diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms, or in any patient with a metal-on-metal bearing. This patient’s symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT scan show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning is indicated. Fluoroscopic-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well-positioned, then iliopsoas tenotomy should be considered.
QUESTION 77
A 72-year-old woman returns 3 weeks after a right total knee replacement. She has been experiencing increasing pain, swelling, and decreasing range of motion during the last 10 days. Examination shows the knee to be more swollen and warm than what is typical at 3 weeks after surgery. The knee feels stable,but she has diffuse tenderness and range of motion is between 15 and 85 degrees. What is the most appropriate investigation(s) to diagnose the etiology of her current problem?
1
Radiographs of the knee
2
Radiographs, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP)
3
Radiographs, ESR, CRP, and knee aspiration
4
No investigations are needed; reassure the patient that her findings are typical at this point
Although the differential diagnosis of her symptoms is broad at this point, the description of symptoms and findings are concerning for postsurgical infection. Regardless of other possible causes, infection needs to be investigated. This question is directed at the most appropriate investigations for the diagnosis of deep infection in the early postsurgical time period. Radiographs should be obtained to rule out mechanical causes. Although the CRP should be trending to normal by 3 to 4 weeks, ESR will likely be elevated secondary to the surgery and difficult to interpret. However, baseline laboratory studies are helpful in the event that follow-up laboratory studies are required. An aspiration for culture and cell count should also be obtained; however, it should be recognized that the normal synovial cell count values during the early postsurgical period (fewer than 6 weeks) are much higher than in the chronic setting. In a study by Bedair and associates, the synovial white blood cell count (WBC) was found to be most useful in predicting infection in patients fewer than 6 weeks after surgery. All but 1 of 19 infected patients had a synovial WBC higher than or equal to 10700 cells/µl, and all but 1 of 127 noninfected knees had a synovial WBC of < 27800 cells/µl. Mean synovial cell counts were 96000 (3520-570000) cells/µl for the infected group, and 4200 (0-41000) cells/µl for the noninfected group. Using receiver operating characteristic curves, these authors learned that the optimal synovial WBC cutoff was 27800 cells/µl,giving 84% sensitivity, 99% specificity, and positive and negative predictive values of 94% and 98%,respectively. Synovial cell differential was less useful with the optimal value of 89% neutrophils, giving a sensitivity of 84% and specificity of 69%. In the chronic setting, a synovial WBC count of > ~3000 cells/µl and percentage of neutrophils > 65% is considered suspicious for infection. PREFERRED RESPONSE: 3
QUESTION 78
What is the most effective method to increase range of motion to impingement during total hip arthroplasty?
1
Increase neck length with a skirted component
2
Increase femoral head diameter
3
Decrease femoral neck offset
4
Use an elevated lip liner
Femoral heads with neck skirts impinge early and have less range of motion. Increased femoral neck offset lengths have been shown to have better range of motion. Elevated lip liners increase the distance the femoral head has to travel to become dislocated, but they reduce the overall range of motion to impingement. Increasing the diameter of the femoral head when the diameter of the femoral neck remains the same increases the range of motion to impingement and hip stability. PREFERRED RESPONSE: 2
QUESTION 79
What factor is associated with high wear and elevated serum metal ion levels after metal-on-metal resurfacing hip arthroplasty?
1
Retroversion of the femoral component
2
Acetabular anteversion more than 20 degrees
3
Acetabular inclination more than 50 degrees
4
Recurrent dislocation of the hip prosthesis
Early failure of metal-on-metal hip resurfacing has been attributed to abnormal wear related to impingement or malalignment. A high level of acetabular inclination over the Lewinnek safe zone of 50 degrees has been associated with high levels of chrome and cobalt ions. This may be related to the fact that wear may be increased by the uncoverage of the implant, although evidence to
prove this conclusion is anecdotal. Additionally, periprosthetic fluid collections and soft-tissue masses have been found in these cases. The other component positions would not necessarily be associated with impingement or wear. PREFERRED RESPONSE: 3
QUESTION 80
are the anteroposterior and lateral radiographs taken 8 months after revision of an aseptically loose acetabular component of an 81-year-old man who has mild cognitive impairment but is medically healthy. A 32-mm femoral head with metal-on-polyethylene was used at the time of revision.He has a history of numerous subluxation events and 2 dislocations requiring closed reduction since the cup revision. An abduction brace was prescribed after the first dislocation. The hip functions well apart from the episodes of instability. Erythrocyte sedimentation rate and C-reactive protein values are within defined limits. What is the most appropriate treatment for his recurrent instability? ---
1
Reinforce the use of an abduction brace when he is out of bed
2
Prescribe physical therapy focusing on abductor strengthening and reinforce hip precautions
3
Revision of the acetabular implant
4
Revision of the head and liner to a larger bearing size
This patient has had numerous episodes of instability and has difficulty remembering his position of risk.He has tried an abduction brace without success. Surgery is indicated for this patient. The 32-mm head appears small in the cup, indicating a very large acetabular component for which one could use a much larger bearing. There is no need for cup revision because the implant is well positioned and not loose. PREFERRED RESPONSE: 4
QUESTION 81
After undergoing elective knee arthroplasty, which risk factor is most likely to cause a symptomatic pulmonary embolus?
1
Female gender
2
Previous knee surgery
3
High preadmission blood glucose
4
History of coronary artery disease
Diabetes mellitus and high blood glucose levels have been shown to increase risk for perioperative complications and symptomatic pulmonary embolism in patients undergoing arthroplasty. Other risk factors include a body mass index higher than 30 and bilateral knee arthroplasty. Neither coronary artery disease, previous knee surgery, nor female gender has been shown to increase risk. PREFERRED RESPONSE: 3
QUESTION 82
A 72-year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
1
Revision using a proximal femoral replacement prosthesis
2
Revision using a long-stem femoral prosthesis along with cerclage fixation
3
Open reduction internal fixation using a locking plate with strut graft
4
Protected weight bearing with abduction bracing
A Vancouver type B-2 periprosthetic fracture pattern (between the lesser trochanter and the tip of the femoral component) frequently compromises stem fixation. This patient’s stem fixation status was not stable because the stem was inserted only 3 weeks before the fracture occurred. The most effective treatment for Vancouver type B-2 fractures is revision with a long stem to achieve distal diaphyseal fixation, along with fixation of the fracture using cables or wires with or without strut graft based on the quality and quantity of the bone stock. PREFERRED RESPONSE: 2
QUESTION 83
Figure 83a is the radiograph of a previously active patient with pain in her lower lumbar spine region and lateral hip 6 months after a cementless hip arthroplasty. What is the most likely cause of this patient’s symptoms? ---
1
Increased hip joint offset
2
Increased leg length
3
Increased hip joint offset and leg length
4
Increased leg length but no increase in offset
The patient has an approximate 1-cm increase in leg length and a 1-cm increase in offset (Figure 83b). A transischial line intersecting the lesser trochanters shows a 1.14-cm difference in leg length. The lateral distance from the pubic midline to the medial femoral neck shows a difference in lateral offset of 1.1 cm.This has resulted in pelvic obliquity and an apparent leg length discrepancy in addition to a true leg length discrepancy. PREFERRED RESPONSE: 3
QUESTION 84
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers,acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, significant risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and also raising risk for nerve injury. Which technique is used to overcome this problem?
1
Subtrochanteric osteotomy with femoral shortening
2
Use of an offset femoral component
3
Use of a lateralized liner
4
Extended trochanteric osteotomy
DISCUSSION-When significant lengthening of a dysplastic hip will occur because a high dislocation is relocated into a significantly lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening,and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoralshortening.
QUESTION 85
Figures 85a and 85b are the radiographs of an 81-year-old woman who is brought to the emergency department after tripping and landing on her right knee. She had a right total knee replacement 8 years before this injury. The replacement had functioned well, but now she cannot bear weight and examination shows swelling and an abrasion over the patella. Neurovascular examination is unremarkable. What is the most appropriate treatment? ---
1
Urgent open reduction and internal fixation using cerclage cables
2
Urgent closed, and possible open, reduction and internal fixation using a lateral periarticular locking screw plate
3
Wait for the patellar abrasion to heal, and then proceed with revision of her knee replacement to a distal femoral replacement.
4
Wait for the patellar abrasion to heal, and then proceed with revision of her femoral component using a long-stemmed femoral revision stem.
This patient has a periprosthetic distal femoral fracture above a well-fixed femoral implant. This is a long spiral fracture and revision of her implant is not required. The level of the fracture is suitable for fixation. The most reliable fixation method is use of a locking screw plate. Cerclage fixation with cables is insufficient for this fracture. Surgery does not need to be delayed for healing of the patellar abrasion because the surgical approach is distant to the abrasion.
QUESTION 86
A 65-year-old woman has had 6 months of activity-related pain in her 15-year-old hip replacement.Her radiograph reveals an eccentric position of the ball head within the acetabulum. She has minimal periacetabular osteolysis, and her uncemented acetabular and femoral components are well fixed. What is the most appropriate treatment?
1
Revision of the acetabular component with retention of the femoral component
2
Revision of both acetabular and femoral components
3
Liner and ball head exchange
4
Observation
Well-fixed components in the presence of minimal osteolysis and a worn acetabular polyethylene liner in a symptomatic patient should be treated with liner and ball head exchange.
Revision of either or both of the well-fixed and otherwise well-functioning components is unnecessary
and introduces the possibility for additional complications. Observation is a suboptimal choice considering that significant wear is seen and the patient is symptomatic. PREFERRED RESPONSE: 3
QUESTION 87
When compared to a general population of patients undergoing knee arthroplasty, patients with ankylosing spondylitis are at higher risk for developing what condition?
1
Stiffness and ossification
2
Infection
3
Component loosening
4
No heightened risk; they can expect the same outcome as patients with primary osteoarthritis

---
Patients with ankylosing spondylitis experience pain relief and improved function after total knee replacement, but a number of studies have shown an increased risk for knee stiffness and heterotopic ossification in this subgroup. Patients should be advised that their underlying condition could make them more likely to experience this complication. PREFERRED RESPONSE: 1
QUESTION 88
Figure 88 is the radiograph of an 84-year-old man who had bilateral total knee replacements 14 years ago. For 3 years he has had pain and swelling in his right knee. Radiographs reveal a progressive valgus deformity of the knee. The patient wants to return to full function and ambulate throughout his household with minimal surgical risk.
Which of the following descriptions best characterizes the polyethylene particles liberated from this patient’s knee in comparison to wear particles found in a patient who undergoes total hip arthroplasty?
1
Smaller and less reactive
2
Smaller and more reactive
3
Larger and less reactive
4
Larger and more reactive
The particles isolated from the knee are larger and less reactive. Wear in a total knee replacement prosthesis differs from that in a total hip replacement. Wear is the result of pitting and delamination; there are not submicron wear debris particles as one would find in the hip. Because of this patient’s age and medical risks, polyethylene exchange is the best decision. The components appear to be well-fixed, and progressive valgus deformity is caused by asymmetric polyethylene wear. Revision total knee Arthroplasty is not expected to be necessary.
_**CLINICAL SITUATION FOR QUESTIONS 90 AND 91**_
A 76-year-old woman underwent an uncomplicated total knee arthroplasty (TKA) 7 years ago. She has had a 4-month history of pain and swelling. Radiographs reveal a global large lucency under the tibial component. Comparison of older radiographs reveals gross migration and subsidence of the tibial component. Further testing reveals an elevated erythrocyte sedimentation rate and C-reactive protein level, as well as a synovial white blood cell count > 15000 cells/µL. Synovial fluid cultures are negative for bacterial growth at 48 hours.
QUESTION 89
Figure 88 is the radiograph of an 84-year-old man who had bilateral total knee replacements 14 years ago. For 3 years he has had pain and swelling in his right knee. Radiographs reveal a progressive valgus deformity of the knee. The patient wants to return to full function and ambulate throughout his household with minimal surgical risk.
What is the most appropriate treatment for this condition?
1
Revision of both the femoral and tibial components
2
Polyethylene exchange
3
Tibia component revision
4
Osteotomy
The particles isolated from the knee are larger and less reactive. Wear in a total knee replacement prosthesis differs from that in a total hip replacement. Wear is the result of pitting and delamination; there are not submicron wear debris particles as one would find in the hip. Because of this patient’s age and medical risks, polyethylene exchange is the best decision. The components appear to be well-fixed, and progressive valgus deformity is caused by asymmetric polyethylene wear. Revision total knee Arthroplasty is not expected to be necessary.
_**CLINICAL SITUATION FOR QUESTIONS 90 AND 91**_
A 76-year-old woman underwent an uncomplicated total knee arthroplasty (TKA) 7 years ago. She has had a 4-month history of pain and swelling. Radiographs reveal a global large lucency under the tibial component. Comparison of older radiographs reveals gross migration and subsidence of the tibial component. Further testing reveals an elevated erythrocyte sedimentation rate and C-reactive protein level, as well as a synovial white blood cell count > 15000 cells/µL. Synovial fluid cultures are negative for bacterial growth at 48 hours.
QUESTION 90
A 76-year-old woman underwent an uncomplicated total knee arthroplasty (TKA) 7 years ago. She has had a 4-month history of pain and swelling. Radiographs reveal a global large lucency under the tibial component. Comparison of older radiographs reveals gross migration and subsidence of the tibial component. Further testing reveals an elevated erythrocyte sedimentation rate and C-reactive protein level, as well as a synovial white blood cell count > 15000 cells/µL. Synovial fluid cultures are negative for bacterial growth at 48 hours.
What is the most appropriate next step?
1
Synovial fluid gram stain
2
Tissue samples sent for culture and frozen section
3
Revision of both components with antibiotic cement and stems
4
Removal of the tibial component and retention of the femoral component if well fixed and appropriately positioned
In this scenario, suspicion for a periprosthetic joint infection is high. The synovial fluid WBC count
is elevated and the synovial fluid culture result may be a false negative. The AAOS Clinical Practice Guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, recommends strongly against the use of gram stain and strongly in favor of multiple culture and frozen sections to aid in the diagnosis of infection. Considering the chronicity of the infection, removal of both components is indicated.
QUESTION 91
A 76-year-old woman underwent an uncomplicated total knee arthroplasty (TKA) 7 years ago. She has had a 4-month history of pain and swelling. Radiographs reveal a global large lucency under the tibial component. Comparison of older radiographs reveals gross migration and subsidence of the tibial component. Further testing reveals an elevated erythrocyte sedimentation rate and C-reactive protein level, as well as a synovial white blood cell count > 15000 cells/µL. Synovial fluid cultures are negative for bacterial growth at 48 hours.
Frozen sections reveal 17 neutrophils per high-power field. What is the most appropriate definitive surgical treatment associated with the highest chance for successful eradication of infection?
1
Irrigation and debridement with tibial revision
2
Irrigation and debridement with placement of an intra-articular antibiotic pump
3
Resection arthroplasty with placement of an antibiotic spacer
4
One-stage exchange
In this scenario, suspicion for a periprosthetic joint infection is high. The synovial fluid WBC count
is elevated and the synovial fluid culture result may be a false negative. The AAOS Clinical Practice Guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, recommends strongly against the use of gram stain and strongly in favor of multiple culture and frozen sections to aid in the diagnosis of infection. Considering the chronicity of the infection, removal of both components is indicated.
QUESTION 92
A 68-year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck with final implant insertion. What is the most appropriate treatment?
1
Removal of the press-fit implant and cementing of the same femoral stem
2
Removal of the uncemented femoral component and placement of a revision modular taperfluted femoral stem
3
Removal of the implant, placement of a cerclage cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
4
Final seating of the uncemented femoral component without additional measures
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction. Several studies indicate that proximal cerclage wiring is adequate to create“barrel hoop” stability of the proximal femur. Braided cables offer superior stability compared to twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
QUESTION 93
The pharmacokinetics of which deep venous thrombosis (DVT) prophylactic agent are affected by liver function and dietary intake?
1
Dalteparin
2
Warfarin
3
Fondaparinux
4
Enoxaparin
Warfarin is an oral vitamin K antagonist that is rapidly absorbed from the gastrointestinal tract. It accumulates in the liver, where it is metabolized and excreted. The pharmacokinetics of warfarin can be affected by certain drugs or disease states that influence liver function. Fondaparinux is a synthetic factor Xa inhibitor that is eliminated through the kidneys. Both Dalteparin and Enoxaparin are low-molecularweight heparins that activate antithrombin and inhibit factors Xa and IIa. Like Fondaparinux, they are eliminated through the kidneys and should be used with caution in patients with kidney disease.
---
QUESTION 94
is the radiograph of a patient who underwent component removal, insertion of an antibiotic spacer, and recent completion of 6 weeks of intravenous antibiotic therapy. The patient’s C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) have decreased and are now within defined limits.The skin is supple and the patient has a range of motion between 10 and 70 degrees. What is the mostappropriate next step?
1
Two weeks off of antibiotics (antibiotic holiday), followed by knee joint aspiration
2
Continued observation for 6 months after surgery to make sure the infection has resolved
3
Joint aspiration for culture and cell count at the time of completion of IV antibiotic therapy
4
Antibiotic spacer exchange
The situation described here is consistent with a successful treatment for deep infection. If the patient’s knee aspiration reveals no organisms and the CRP and ESR trend toward normal, the patient is a candidate for a second-stage revision knee arthroplasty. A 2-week antibiotic holiday is necessary to obtain accurate culture results either with aspiration or soft-tissue specimens at the time of second-stage revision TKA.There is no evidence that waiting for up to 6 months provides a lower
recurrence rate, and there may be long-term problems with a spacer left in place for 6 months, such as breakage, instability, or loosening. PREFERRED RESPONSE: 1
QUESTION 95
What factor is associated with decreased range of motion to impingement?
1
Skirted modular femoral head
2
Trapezoidal neck geometry
3
Vertical cup inclination of 40 to 55 degrees
4
Anteversion of 10 to 20 degrees of both the stem and cup
The use of modular femoral stems and acetabular implants have increased the number of head, neck,and liner designs, but the features of recent designs can cause intra-articular prosthetic impingement within the arc of motion required to perform daily activities. Impingement may lead to limited motion,increased wear, osteolysis, and subluxation or dislocation. Minimizing impingement involves avoiding skirted heads, matching the femoral head with an appropriate acetabular implant, maximizing the headto-neck ratio and, when possible, using a chamfered acetabular liner and a trapezoidal, rather than circular, neck cross-section. Computer modeling studies indicate the optimal cup position is 45 to 55 degrees’ abduction. Angles < 55 degrees require anteversion of 10 to 20 degrees of both the stem and cup to minimize risk for impingement and dislocation. However, wear or instability may occur with cup inclination exceeding 50 degrees. PREFERRED RESPONSE: 1
QUESTION 96
A 68-year-old woman undergoes an uncomplicated total knee replacement through a midline incision that is extended distally to join a previous incision from a high-tibial osteotomy done 12 years previously.Despite relief of pain and appropriate knee mobility at 2 weeks, drainage continues from the distal part of the wound. What are the most appropriate next step(s) in treatment?
1
Oral cephalexin while the wound heals
2
Vacuum suction drain applied over the draining part
3
Intravenous antibiotics and reassess the knee in 24 hours
4
Urgent open debridement of the knee, cultures, and evaluation of inflammatory laboratory data
Drainage from a knee after arthroplasty can be ominous; here, a previous incision was made for an osteotomy, possibly compromising wound healing. At 2 weeks, persistent wound drainage is not expected and warrants urgent attention with surgical debridement, cultures, and a baseline check of inflammatory laboratory data. Intravenous antibiotics can be started while awaiting cultures, but oral or intravenous antibiotics alone are not sufficient and a vacuum drain is not indicated in this situation. PREFERRED RESPONSE: 4
QUESTION 97
What infection-control measure has been shown to have the most notable impact in reducing surgical-site infections?
1
Intravenous antibiotic administration within 1 hour of surgical incision
2
Screening and decolonization of patients colonized with methicillin-resistant Staphylococcus aureus
3
Horizontal laminar flow
4
Use of enclosed body exhaust suits
Timely administration of prophylactic antibiotics is the most important factor shown to decrease surgicalsite infections. The use of horizontal laminar flow and body exhaust suits has not been shown to significantly affect infection rates. PREFERRED RESPONSE: 1
QUESTION 98
Three years after undergoing a metal-on-polyethylene total hip arthroplasty, a 72-year--old woman develops pain with weight bearing and rest. Hip flexion and internal rotation is associated with pain.Radiographs show no evidence of loosening. What is the most appropriate next step in this evaluation?
1
Bone scan
2
White blood cell (WBC) count
3
Labeled white cell scan
4
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels
The ESR is a sensitive serologic indicator of inflammation; however, it is less specific for infection. Other noninfectious conditions may cause an elevated ESR. The CRP is a specific indicator of infection, which may be transiently elevated after uncomplicated total hip arthroplasty, but usually returns to a normal range within 1 to 2 weeks of surgery. If both the ESR and CRP are elevated, there is a high likelihood that a painful hip replacement is infected, and joint aspiration is indicated. Serum WBC is not a reliable indicator of periprosthetic infection, with a sensitivity of only 20%. Bone scan typically demonstrates increased technetium uptake for several years after hip arthroplasty, which is not specific for infection. A labeled white cell scan is useful to rule out infection, but less helpful to detect the presence of infection. PREFERRED RESPONSE: 4
QUESTION 99
is a CT scan at the level of the distal femur and femoral component. What is the orientation of the femoral component in the CT scan? ---
1
Properly rotated
2
Internally rotated
3
Externally rotated
4
Excessive flexion
A CT scan with metal artifact reduction is a useful study to evaluate femoral component rotation. Proper rotation would show that the transepicondylar line and posterior condylar line are parallel. Figure 99b shows that the femoral component is internally rotated compared to the femoral epicondylar axis. PREFERRED RESPONSE: 2
QUESTION 100
A 68-year-old woman with a 9-year history of type II diabetes is seen 11 weeks after an uncemented left total hip replacement. When seen 6 weeks after surgery, some mild erythema and induration at the distal incision was noted, but no drainage. She states that drainage started 2 weeks ago. Examination shows turbid drainage coming from the distal third of the incision with mild surrounding erythema. Hip range of motion causes mild discomfort. Investigations reveal an erythrocyte sedimentation rate of 45 mm/h(reference range, 0-20 mm/h) and C-reactive protein of 54 mg/L (reference range, 0.08-3.1 mg/L). A rapid polymerase chain reaction of the swabbed fluid is positive for methicillin-resistant Staphylococcus aureus.Hip aspiration under fluoroscopy is attempted but no fluid is obtained. What is the most appropriate treatment?
1
Debridement of the skin and superficial tissues
2
Debridement and removal of the implants and insertion of an antibiotic spacer
3
Debridement of superficial and deep tissues including the joint with exchange of the modular head and liner
4
Prescription for sulfamethoxazole and trimethoprim (Bactrim DS), 1 tablet, twice daily for 14 days, and then re-evaluate the patient
This case illustrates the treatment choices to address a postsurgical deep infection at 11 weeks postsurgery.Considering the progression of symptoms and persistent drainage, one needs to assume the infection is deep. Wound drainage beginning at 9 weeks after surgery is unlikely to be the result of a superficial infection. The absence of fluid on the attempted aspiration may occur in situations in which a sinus tract allows most of the fluid to escape the joint. Injection of contrast could confirm the presence of a sinus tract. Debridement and removal of the implants and insertion of an antibiotic spacer are most appropriate because the results of a single debridement at 11 weeks with a resistant organism are poor for curing or controlling infection. The use of antibiotics alone or a superficial debridement is inadequate in this setting.