
Question 26
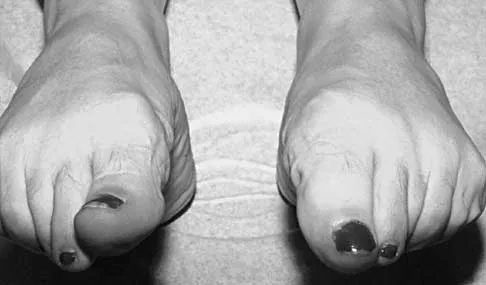
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?


Explanation
The patient has necrotizing fasciitis, a rare and sometimes fatal disease that has many different etiologies. Signs that this is not a normal infection are the worsening clinical symptoms despite IV antibiotics and the systemic symptoms. He needs urgent surgical care before he becomes completely septic and unstable. He needs very aggressive debridement of his tissues. Hyperbaric oxygen and immunoglobulins are only anecdotally helpful, and would only be used after surgery. Fontes RA, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
References:
- Ozalay M, Ozkoc G, Akpinar S, et al: Necrotizing soft-tissue infection of a limb: Clinical presentation and factors related to mortality. Foot Ankle Int 2006;27:598-605.
Question 27
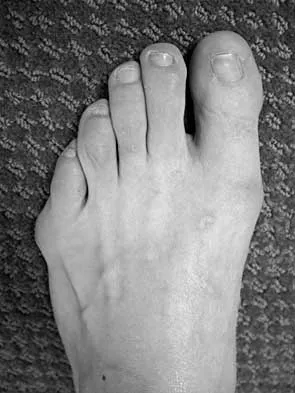
A 17-year-old girl with Charcot-Marie-Tooth disease reports the development of progressive instability when walking on uneven surfaces. Her involved heel is positioned in varus when viewed from behind. Examination reveals that she walks on the outer border of the involved foot. She has full passive motion of the ankle and hindfoot joints. She is able to dorsiflex the ankle against resistance. The heel varus fully corrects with the Coleman block test. Standing radiographs reveal a cavus deformity with valgus of the forefoot. She would like to avoid using an ankle-foot orthosis. What is the best surgical option?


Explanation
This deformity is early in the disease process. The foot is still flexible, as evidenced by correction with the Coleman block test. A simple dorsiflexion osteotomy of the first metatarsal should provide a plantigrade foot. More complex osteotomies are required later in the disease process when the foot is not flexible and the deformity does not correct with the Coleman block test. The patient may also require a tibialis anterior transfer later in the disease process but not at the present time. Richardson EG (ed): Orthopaedic Knowledge Upate: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-144.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Coughlan MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 525-557.
Question 28
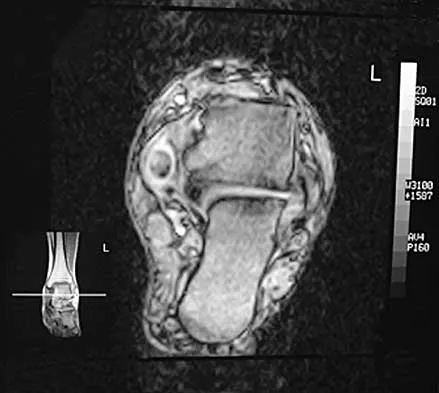
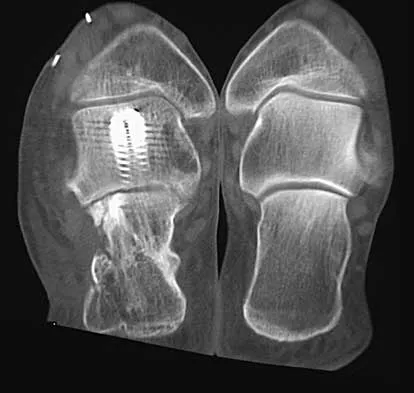
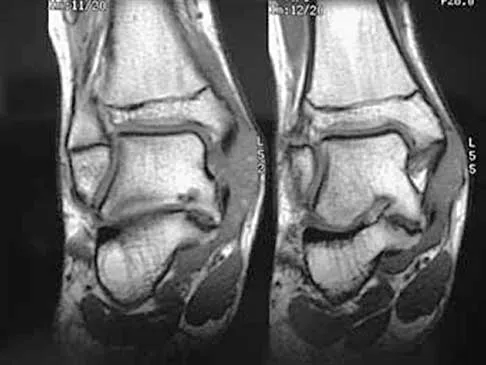
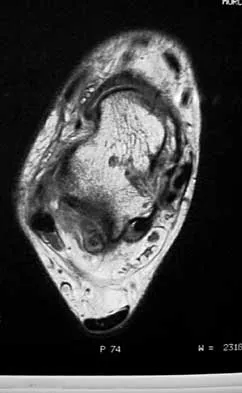
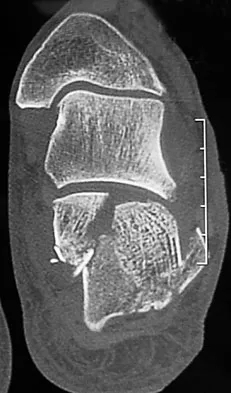
A 58-year-old man with type 1 diabetes mellitus is seen in the emergency department and he reports a 3-day history of a red swollen foot but no history of trauma. Examination reveals that the skin is intact, and the patient has discomfort with passive range of motion at the ankle, hindfoot, and midfoot joints. He denies any fever. Laboratory studies show a WBC count of 7,800/mm3, an erythrocyte sedimentation rate of 40 mm/h, a C-reactive protein level of 23, and a serum glucose of 100. A radiograph and MRI scans are shown in Figures 16a through 16c. What is the next most appropriate step in management?




Explanation
16b 16c Whereas it is difficult to distinguish between cellulitis, septic joint, osteomyelitis, and early Eichenholtz stage 1 Charcot, the presence of a fracture in the absence of ulcerations with a normal WBC count and serum glucose strongly indicates that the described symptoms are due to an early Charcot process alone. A technetium Tc 99m scan alone would not be helpful; however, the addition of a sulfur colloid marrow scan or indium In 111 scan may be more specific to rule out infection, though it is not warranted here. Total contact casting with non-weight-bearing or limited weight bearing during Eichenholtz stage 1 when the foot is warm, erythematous, and swollen is advised to help prevent deformity. Alternatively, stabilization with pneumatic bracing may also be considered. While some authors have proposed early fixation or arthrodesis for Eichenholtz stage 1, the gold standard is still total contact casting with no to limited weight bearing until the swelling resolves and evidence of consolidation is seen on radiographs. Trepman E, Nihal A, Pinzur MS: Current topics review: Charcot neuropathy of the foot and ankle. Foot Ankle Int 2005;26:46-63. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 123-134.
References:
- Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 29
Which of the following conditions is not associated with an increased risk of developing Achilles tendinopathy?


Explanation
Diabetes mellitus, obesity, and exposure to steroids have all been associated with the development of Achilles tendinopathy. In addition, Achilles tendinopathy has been associated with a history of hormone replacement therapy and the use of oral contraceptives. Quinolone antibiotics have also been linked to Achilles tendinopathy. Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy. Foot Ankle Int 2006;27:952-959.
References:
- Holmes GB, Mann RA, Well L: Epidemiological factors associated with rupture of the Achilles tendon. Contemp Orthop 1991;23:327-331.
Question 30
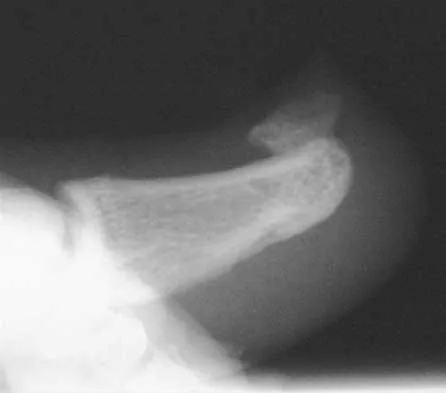
Figures 17a through 17c show the radiographs of a 38-year-old man following a motorcycle accident. The posterior portion of the talus extruded through a posterolateral wound. The extruded talar body is visible in the wound along with some road debris. Management should now consist of surgical irrigation, debridement, and






Explanation
17b 17c The extruded talus should be placed in sterile bacitracin solution, irrigated thoroughly, gently debrided, and immediately replanted in the OR. Open reduction and internal fixation of the talar fracture may be attempted immediately depending on the soft-tissue envelope, or delayed after soft-tissue stabilization with an external fixator. A retrospective study of 19 patients with an extruded talus reported that 12 patients had no subsequent surgery after definitive fixation, 7 had subsequent procedures, and 2 patients developed infections that were treated successfully at an average of 42-month follow-up. Successful outcome in this series was attributed to multiple debridements, soft-tissue stabilization, and primary wound closure. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424. Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.
References:
- Marsh JL, Saltzman CL, Iverson M, et al: Major open injuries of the talus. J Orthop Trauma 1995;9:371-376.
Question 31
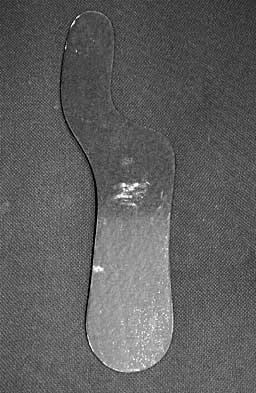
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?



Explanation
18b The patient has a malunion of an attempted open reduction of a Lisfranc dislocation. The pain occurs during the terminal stance phase of gait as load is being transferred from the hindfoot to the forefoot. The bending moment can be best neutralized with shoe modification with a cushioned heel and rocker sole, which best unloads the tarsal-metatarsal junction. Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
References:
- Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 58-63.
Question 32
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?



Explanation
Differentiating between a midfoot sprain and Lisfranc diastasis is critical in the management of the athlete with an acute injury to the midfoot. Greater than 2 mm of displacement between the first and second metatarsals on a weight-bearing radiograph is an indication for anatomic reduction with internal fixation of the tarsometatarsal joints. If no subluxation is noted, treatment should consist of a non-weight-bearing cast for 6 weeks, followed by a gradual return to activity. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
References:
- Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 33
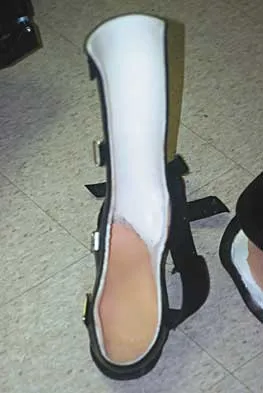
A 36-year-old woman is wearing an ankle-foot orthosis for a foot drop secondary to spastic hemiplegia following a postpartum stroke 2 years ago. Knee and hip motion and strength are within normal ranges. She has undergone multiple rounds of physical therapy but has seen no improvement over the past several months. No improvement has been recorded by electromyography (EMG) studies over the past year. Examination reveals a 5-degree plantar flexion contracture with clonus, heel varus, and compensatory knee hyperextension when standing. She has 4/5 power in the tibialis anterior and gastrocnemius soleus complex with resistance testing. Everters are 2/5 to resistance testing. EMG gait studies show that the tibialis anterior demonstrates activity during both swing and stance phase that is increased during swing phase. Premature firing of the triceps surae is noted when positioning the foot in equinus prior to floor contact. What is the most appropriate management?
Explanation
The patient has a dynamic varus deformity secondary to spasticity of the tibialis anterior during stance phase with inverter/everter imbalance. The patient still has active motion of the tibialis anterior; therefore, an out-of-phase posterior tibial tendon transfer should not be performed. The same is true of the Bridle procedure. Transfer of the posterior tibialis in this patient may also result in subsequent planovalgus deformity. Lengthening of the Achilles tendon through a percutaneous tenotomy will restore dorsiflexion and decrease clonus from the stretch response. If adequate dorsiflexion is not obtained intraoperatively, then posterior tibialis tendon lengthening may be considered. A split tibialis anterior tendon transfer to the lateral cuneiform, or, transfer of the entire tendon to the cuneiform should correct the varus component and compensate for the weakened peroneals. Yamamoto H, Okumura S, Morita S, et al: Surgical correction of foot deformities after stroke. Clin Orthop Relat Res 1992;282:213-218. Piazza SJ, Adamson RL, Moran MF, et al: Effects on tensioning errors in split transfers of tibialis anterior and posterior tendons. J Bone Joint Surg Am 2003;85:858-865.
References:
- Morita S, Muneta T, Yamamoto H, et al: Tendon transfers for equinovarus deformed foot caused by cerebrovascular disease. Clin Orthop Relat Res 1998;350:166-173.
Question 34
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?




Explanation
19b Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome. Acupuncture would be expected to be of limited benefit. Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.
References:
- Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 182-183.
Question 35
What is the most frequent complication of percutaneous repair of an acute Achilles tendon rupture?


Explanation
Sural nerve entrapment is the major risk of percutaneous repair. A small mini-open technique with a suture guide can obviate that issue. Re-rupture rates after surgical repair are approximately 3%. Infection and wound problems are rarely encountered with percutaneous repair; they are issues with open repair. Aracil J, Pina A, Lozano JA, et al: Percutaneous suture of Achilles tendon ruptures. Foot Ankle 1992;13:350-351. Sutherland A, Maffulli N: A modified technique of percutaneous repair of the ruptured Achilles tendon. Oper Orthop Traumatol 1998;10:50-58.
References:
- Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170.
Question 36
A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?

Explanation
Weinstein reported on 31 patients (45 feet) with congenital metatarsus adductus followed for an average of 33 years. Twenty-nine feet had moderate to severe deformities treated with manipulation and casting with a 90% success rate. In a young child, surgery is not indicated until nonsurgical management has failed. In patients 2 to 4 years of age, tarsometatarsal capsulotomies are indicated, whereas multiple metatarsal osteotomies are reserved for recalcitrant deformities in children older than 4 years of age. Mild or moderate metatarsus adductus that is passively correctable will resolve without treatment. Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988. Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus. J Pediatr Orthop 1999;19:49-50.
References:
- Weinstein SL: Bristol-Myers Squibb/Zimmer award for distinguished achievement in orthopaedic research. Long-term follow-up of pediatric orthopaedic conditions: Natural history and outcomes of treatment. J Bone Joint Surg Am 2000;82:980-990.
Question 37
A 34-year-old man has had a 13-month history of an equinovarus deformity of the foot and ankle after a motorcycle accident. His foot and ankle are flexible, but bracing has become uncomfortable. Active dorsiflexion and eversion are absent. What is the most appropriate treatment?



Explanation
Arthrodesis of any of the ankle or hindfoot joints should be reserved for fixed deformities or end-stage degenerative arthritis. Achilles tendon lengthening is necessary to correct the equinus and to improve dorsiflexion-plantar flexion balance. Similarly, transfer of the posterior tibialis tendon reduces both plantar flexion and inversion torque. Hansen ST: Function Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 442-447.
References:
- Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106.
Question 38
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?



Explanation
20b Triplane fractures generally occur in children who are near skeletal maturity. The injury is generally caused by a supination external rotation mechanism. The number of fracture fragments present (two or three) depends on what part of the physes is closed at the time of injury. Articular congruity is the major concern in the management of these injuries since the patient has almost reached skeletal maturity. The goal is to restore articular congruity to minimize the development of posttraumatic arthritis. Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765. Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
References:
- Spiegel PG, Mast JW, Cooperman DR, et al: Triplane fractures of the distal tibial epiphysis. Clin Orthop Relat Res 1984;188:74-89.
Question 39
A 75-year-old woman reports foot pain and states that her foot has become progressively "flatter" in the past 3 years. Custom inserts and physical therapy have failed to provide relief. Examination reveals a flexible hindfoot and mild heel cord contracture. The patient is able to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 21a through 21d. What is the most appropriate surgical management?



Explanation
21b 21c 21d The patient has end-stage midfoot arthritis, with a secondary flatfoot deformity through the midfoot. The ability to perform a single limb heel rise indicates that the posterior tibial tendon is functioning, and the weight-bearing radiographs show normal calcaneal pitch and talar head coverage, thus confirming that the flatfoot deformity is isolated to the midfoot. Therefore, the most appropriate treatment is medial column arthrodesis and heel cord lengthening. The other listed procedures are not indicated because they are used in the management of adult flatfoot from posterior tibial tendon insufficiency. Toolan BC: Midfoot arthrodesis: Challenges and treatment alternatives. Foot Ankle Clin 2002;7:75-93.
References:
- Horton GA, Olney BW: Deformity correction and arthrodesis of the midfoot with a medial plate. Foot Ankle 1993;14:493-499.
Question 40
A 52-year-old woman who underwent cheilectomy 1 year ago for hallux rigidus now reports continued pain in the first metatarsophalangeal joint. She did not have any incision healing problems, and has not had any fevers, erythema, or drainage. Which of the following procedures will provide the best combination of pain relief and function?

Explanation
All but the Moberg osteotomy are capable of providing pain relief; however, arthrodesis offers the best long-term results and restores weight bearing and propulsion function to the first ray. Machacek F Jr, Easley ME, Gruber F, et al: Salvage of a failed Keller resection arthroplasty. J Bone Joint Surg Am 2004;86:1131-1138.
References:
- Myerson MS, Schon LC, McGuigan FX, et al: Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Question 41
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?



Explanation
The sural nerve runs with the small saphenous vein on the posterior leg just lateral to the Achilles tendon. It is formed by contributions from both the tibial and common peroneal nerves and provides sensation on the dorso-lateral aspect of the foot. Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
References:
- Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 42
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?




Explanation
23b The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case. Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction. Foot Ankle Clin 2007;12:137-151.
References:
- Migues A, Solari G, Carrasco NM, et al: Repair of talar neck nonunion with indirect corticocancellous graft technique: A case report and review of the literature. Foot Ankle Int 1996;17:690-694.
Question 43
What type of physical therapy is most effective for chronic noninsertional Achilles tendinopathy?


Explanation
Eccentric gastrocsoleus strengthening (especially with heavy loads) consistently has been shown to be superior in the management of Achilles tendinopathy. Decreases in pain and increases in strength have been demonstrated despite the frequently refractory nature of this condition. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 91-102.
References:
- Vora AM, Myerson MS, Oliva F, et al: Tendinopathy of the main body of the Achilles tendon. Foot Ankle Clin 2005;10:293-308.
Question 44
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?


Explanation
This is an example of tethering of the flexor hallucis longus/flexor digitorum longus (FHL/FDL) to the fracture site. Additional time and/or physical therapy and bracing would not be expected to be of benefit. Release of the FHL and FDL from the fracture site or retromalleolar lengthening will address the posttraumatic claw toe deformity and Achilles tendon lengthening will address the mild equinus. Posterior tibial tendon transfer is not appropriate as the patient demonstrates a normal heel rise. Midfoot releases and hallux fusion are also not indicated. Feeny MS, Williams RL, Stephens MM: Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-338.
References:
- Clawson DK: Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-48.
Question 45
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
Explanation
The ankle dorsiflexor muscles have been denervated for too long a period to expect reinnervation to be successful. Even if the extensor hallucis longus tendon was functional, it is unlikely to have sufficient strength to achieve dynamic ankle dorsiflexion. The tibialis posterior tendon transfer has been shown to predictably achieve these goals in a high percentage of patients. Successful ankle fusion is likely to fail with time due to the development of forefoot equinus. Pinzur MS, Kett N, Trilla M: Combined anteroposterior tibial tendon transfer in post-traumatic peroneal palsy. Foot Ankle 1988;8:27l-275.
References:
- Lipscomb P, Sanchez J: Anterior transplantation of the posterior tibial tendon for persistant palsy of the common peroneal nerve. J Bone Joint Surg Am 1961;43:60-66.
Question 46
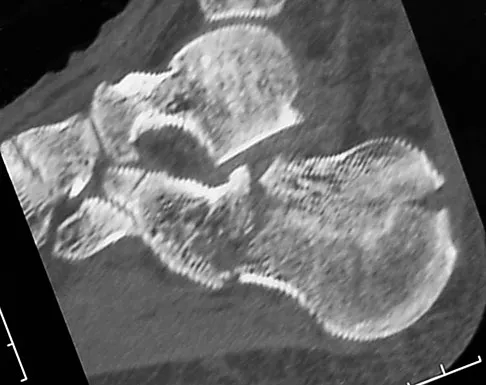
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?





Explanation
24b 24c 24d 24e The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
References:
- Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 47
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?


Explanation
A flexor digitorum longus transfer, while not as strong as the peroneals, improves the tendon balance and maintains hindfoot mobility. Subtalar fusion is a salvage procedure. Posterior tibial tendon transfer compromises inversion strength and arch height. Functional absence of the peroneals results in an imbalance that could lead to forefoot varus. Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
References:
- Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 48
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?

Explanation
Ultrasound is best at imaging abrupt changes in the density of adjacent tissue and therefore is best at imaging wood in the soft tissues of the foot. Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
References:
- Jacobson JA, Powell A, Craig JG, et al: Wooden foreign bodies in soft tissue: Detection at US. Radiology 1998;206:45-48.
Question 49
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Explanation
The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean. Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res 2003;408:86-91.
References:
- Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.
Question 50
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
The most frequently described entrapment of the deep peroneal nerve is the anterior tarsal tunnel syndrome. This syndrome refers to entrapment of the deep peroneal nerve under the inferior extensor retinaculum. Entrapment can also occur as the nerve passes under the tendon of the extensor hallucis brevis. Compression by underlying dorsal osteophytes of the talonavicular joint and an os intermetatarseum (between the bases of the first and second metatarsals) have previously been described in runners. Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
References:
- Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Finish Exam?
You cannot change answers after submitting.
