Understanding Multiple Epiphyseal Dysplasia: Orthopedic Cases
Patient Presentation & History
This Grand Rounds presentation focuses on a challenging case involving Multiple Epiphyseal Dysplasia (MED) and its orthopedic implications.
Patient Demographics: A 28-year-old male.
Chief Complaint: The patient presented with a five-year history of progressive bilateral hip pain, predominantly worse on the right side. This pain significantly impacted his activities of daily living (ADLs), including ambulation, stair climbing, and prolonged standing. He reported a noticeable, worsening Trendelenburg gait.
Past Medical History: The patient was diagnosed with Multiple Epiphyseal Dysplasia at five years of age following evaluation for short stature, gait abnormalities, and chronic joint pain. Genetic testing subsequently confirmed a mutation in the COMP gene, consistent with an autosomal dominant form of MED (Fairbank type). He reported a childhood history of chronic, intermittent pain in his knees and ankles, though no specific interventions beyond conservative management were required previously. There was no history of prior hip surgery. No other significant medical comorbidities were noted. He is a non-smoker and reports occasional alcohol consumption.
Family History: His mother has a history of mild short stature and early-onset osteoarthritis affecting multiple joints, though she was never formally diagnosed with MED. This history is suggestive of a familial pattern of the disorder.
Mechanism of Injury: There was no acute traumatic event preceding the exacerbation of hip pain. The onset of symptoms was insidious and characterized by gradual progression of pain and functional limitation.
Clinical Examination
A thorough orthopedic examination was performed.
General Observations: The patient exhibited mild short stature (160 cm). Inspection revealed broad and flattened joint contours, particularly evident in the knees and ankles. His gait analysis demonstrated a bilateral Trendelenburg pattern, more pronounced on the right, with a compensatory lurch and significantly decreased stride length.
Right Hip Examination:
*
Inspection:
Noted apparent shortening of the right lower extremity, accompanied by a subtle external rotation deformity. Significant atrophy of the gluteal musculature was observed.
*
Palpation:
Localized tenderness was elicited over the greater trochanter and anterior joint line. There was no palpable warmth or erythema, suggesting an absence of acute inflammatory or infectious processes.
*
Range of Motion (ROM):
Markedly restricted and painful passive and active range of motion was noted.
* Flexion: 70 degrees (normal typically 120-130 degrees)
* Extension: 0 degrees (normal typically 10-20 degrees)
* Abduction: 5 degrees (normal typically 40-50 degrees)
* Adduction: 15 degrees (normal typically 20-30 degrees)
* Internal Rotation: 0 degrees (normal typically 30-40 degrees)
* External Rotation: 30 degrees (normal typically 40-50 degrees)
A fixed flexion contracture of 20 degrees was identified on Thomas test. A positive Faber test further indicated hip joint pathology.
*
Neurological Assessment:
Sensation was intact to light touch and pinprick throughout the right lower extremity (L2-S1 dermatomes). Motor strength was 5/5 across all major muscle groups (hip flexors, extensors, abductors, adductors, knee flexors/extensors, ankle dorsi/plantar flexors). Deep tendon reflexes (patellar and Achilles) were 2+ and symmetrical. No pathological reflexes were present.
*
Vascular Assessment:
Distal pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were palpable, strong, and symmetrical bilaterally. Capillary refill was brisk in all digits of the right foot.
Left Hip Examination:
The left hip was less symptomatic but also demonstrated significant restriction, though marginally better than the right.
* ROM: Flexion 90 degrees, extension 5 degrees, abduction 15 degrees, adduction 20 degrees, internal rotation 10 degrees, external rotation 35 degrees. A mild flexion contracture was present.
Other Joints: Mild valgus deformity was observed in both knees. Examination of the ankles revealed flattened talar domes. Range of motion in the knees and ankles was mildly restricted with palpable crepitus, consistent with widespread epiphyseal involvement and early degenerative changes.
Imaging & Diagnostics
Initial Radiographs (Bilateral Hips with pelvis AP and frog-leg lateral views):
The initial radiographic series provided critical insights into the extent of the patient's skeletal dysplasia and secondary degenerative changes.
*
Key Findings:
*
Severe bilateral coxa magna and coxa plana:
The femoral heads were significantly enlarged in overall diameter but profoundly flattened, demonstrating irregular ossification. The femoral necks appeared short and broad.
*
Acetabular Dysplasia:
Both acetabula exhibited shallow morphology, consistent with dysplasia. Sclerotic changes and subchondral cyst formation were evident in the weight-bearing areas.
*
Joint Space Narrowing:
There was complete obliteration of the superior and anterior joint spaces bilaterally, indicative of severe osteoarthritis.
*
Osteophytes:
Extensive peripheral osteophyte formation was observed circumferentially around both femoral heads and acetabular margins.
*
Subchondral Sclerosis:
Diffuse subchondral sclerosis was apparent, reflecting the chronic degenerative process.
*
Overall Impression:
These features were pathognomonic for severe secondary osteoarthritis resulting from chronic epiphyseal dysplasia.
*
*
This image displays an anteroposterior radiograph of the pelvis, illustrating the characteristic findings of advanced bilateral hip osteoarthritis in the setting of Multiple Epiphyseal Dysplasia, specifically exhibiting irregular and flattened femoral heads (coxa plana) and broadened femoral necks (coxa magna), coupled with severe joint space narrowing and acetabular remodeling.
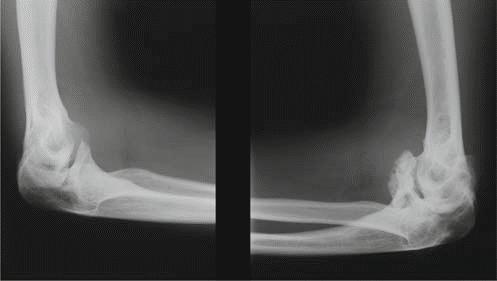
Additional Radiographs (Knees and Ankles):
To assess the widespread nature of MED, radiographs of other commonly affected joints were obtained.
*
Knees:
Revealed widened and irregular epiphyses of the distal femora and proximal tibiae. Patella alta was noted. Significant joint space narrowing was observed in the patellofemoral and medial tibiofemoral compartments. Mild valgus deformity was confirmed.
*
Ankles:
Demonstrated flattened and irregular talar domes, contributing to a widened ankle mortise and evidence of subtalar arthritis.
*

*
This image typically represents an anteroposterior view of the knee, showcasing the irregular and flattened epiphyses, potentially widened and disorganized growth plates (if skeletally immature), and early degenerative joint changes consistent with the manifestations of Multiple Epiphyseal Dysplasia.
Computed Tomography (CT) Scan of Pelvis and Hips:
*
Indications:
A CT scan was considered imperative for precise delineation of residual bone stock, detailed assessment of femoral head and acetabular morphology in three dimensions, evaluation for large subchondral cysts, and invaluable assistance in preoperative planning for total hip arthroplasty (THA). This was especially critical due to the severe anatomical distortion associated with MED.
*
Findings:
The CT scan confirmed the severe acetabular and femoral head deformities. Large femoral head osteophytes were prominent, and significant superior bone loss was noted in the acetabulum. Increased femoral anteversion was also identified. The medullary canals of the femora appeared relatively narrow compared to typical adult anatomy, a common feature in certain forms of skeletal dysplasia.
*
*
This image illustrates a computed tomography reconstruction, likely a three-dimensional volume rendering, providing intricate detail of the complex osseous architecture of the pelvis and hips. Such imaging is invaluable for assessing dysplastic changes, bone stock deficiencies, and precise component planning essential for successful total hip arthroplasty in challenging cases.
Magnetic Resonance Imaging (MRI) of Hips:
*
Indications:
While not always a primary requirement for end-stage osteoarthritis, MRI was briefly considered to definitively rule out other concurrent soft tissue pathologies or avascular necrosis (AVN) of the femoral head, which can sometimes present similarly or coexist in younger patients. However, given the unequivocal radiographic and CT findings of severe osteoarthritis secondary to MED, the diagnostic utility for
surgical planning
was deemed limited in this specific scenario.
*
Findings (expected, if performed):
An MRI would likely demonstrate extensive cartilage loss, subchondral edema, synovial hypertrophy (synovitis), and potential labral degeneration or absence. It would confirm the absence of AVN.
Templating:
Meticulous templating was performed utilizing both calibrated radiographs and detailed CT reconstructions. Due to the severe coxa magna and plana, specific attention was directed towards selecting an appropriate femoral component size and offset, as well as optimizing acetabular component position. The goals were to ensure stable fixation, restore limb length, and re-establish the hip center of rotation, which is often superiorly migrated in dysplastic acetabula. The potentially narrow femoral medullary canal necessitated careful assessment of stem fit and length, with a cautious approach to femoral reaming, often starting with smaller reamers.
Differential Diagnosis
| Feature | Multiple Epiphyseal Dysplasia (MED) | Spondyloepiphyseal Dysplasia (SED) Congenita / Tarda | Legg-Calvé-Perthes Disease (LCPD) (late sequelae) | Achondroplasia (for comparative understanding of dysplasias) |
|---|---|---|---|---|
| Genetic Basis | Heterogeneous; mutations in COMP , COL9A1/2/3 , DTDST , SLC26A2 , MATN3 , GDF5 , etc. Primarily autosomal dominant, some autosomal recessive forms. | SED Congenita: COL2A1 gene (autosomal dominant). SED Tarda: TRPV4 or SEDL (X-linked recessive, some autosomal dominant). | Idiopathic avascular necrosis of the femoral head occurring in childhood. Primarily a local ischemic event, not a genetic dysplasia in itself, though genetic predispositions are studied. | Mutation in FGFR3 gene (autosomal dominant), typically a de novo mutation in 80% of cases. |
| Primary Anatomic Effect | Diffuse, symmetrical involvement of epiphyses and growth plates across multiple joints (hips, knees, ankles, shoulders, wrists). Cartilage defects. | Spine & Epiphyses . Characterized by disproportionate short stature with a short trunk. Significant impact on vertebral bodies (platyspondyly) and often severe epiphyseal abnormalities. | Localized to the femoral head initially (unilateral or bilateral, usually asymmetrical). Later sequelae include femoral head deformity (coxa magna, plana), pistol grip deformity, and secondary osteoarthritis. | Predominantly affects long bone diaphyses due to impaired enchondral ossification, leading to rhizomelic (proximal) limb shortening. Minimal direct epiphyseal dysgenesis. |
| Radiographic Hallmarks | Irregular, fragmented, flattened, and often delayed ossification of multiple epiphyses. Characteristic coxa plana and coxa magna . Early-onset osteoarthritis. Small, irregular carpal bones. Mild vertebral endplate abnormalities may be present in some types. | Platyspondyly (flattened vertebral bodies), odontoid hypoplasia, pear-shaped or ovoid vertebral bodies. Delayed epiphyseal ossification. Flattened epiphyses (e.g., knee, hip). | Early: Femoral head sclerosis and fragmentation. Later: Enlarged, flattened, and irregular femoral head (coxa plana/magna), metaphyseal cysts, lateral subluxation, widening of the femoral neck. | Shortened long bones with metaphyseal flaring ("trumpet-shaped" bones). Broad and short phalanges ("trident hand"). Normal trunk length. Lumbar lordosis. Macrocephaly. |
| Clinical Presentation | Joint pain (hips, knees, ankles, spine) typically presenting in childhood or adolescence. Waddling gait (Trendelenburg) is common. Mild to moderate short stature. Early-onset osteoarthritis (3rd-5th decade, often earlier). Good intelligence. | Disproportionate short stature (short trunk dwarfism). Early progressive joint degeneration. Scoliosis, kyphosis, and often atlantoaxial instability due to odontoid hypoplasia (particularly SED congenita). Vision and hearing impairment can occur. | Limp, hip/knee/thigh pain in childhood (typically 4-10 years). Limited hip range of motion, especially abduction and internal rotation. Later: stiff hip, limited ROM, progressive osteoarthritis, and leg length discrepancy. | Disproportionate short stature, macrocephaly, midface hypoplasia, frontal bossing, exaggerated lumbar lordosis. Normal intelligence. Can have spinal stenosis. |
| Spine Involvement | Generally mild or absent. Some specific genetic types (e.g., MED due to DTDST or SLC26A2 ) may present with more prominent spinal involvement, including flattened vertebral bodies, but typically less severe than SED. | Significant and defining : Severe platyspondyly, severe kyphoscoliosis, and crucial odontoid hypoplasia with risk of atlantoaxial instability, potentially leading to neurological compromise. | No direct primary spinal involvement. Secondary spine issues like scoliosis can occur due to gait abnormalities or leg length discrepancy. | Significant: Severe lumbar spinal stenosis (especially in the thoracolumbar region), exaggerated lumbar lordosis. Potential for kyphosis. |
| Treatment Challenges | Premature osteoarthritis necessitates joint arthroplasty at a significantly younger age. Atypical anatomy (flattened epiphyses, short broad necks, shallow acetabula, narrow canals) complicates component sizing and positioning. Joint preservation strategies often limited. | Requires complex spinal fusion for instability/deformity. Arthroplasty for severe peripheral joint OA. High risk of neurological complications related to spinal issues. Requires careful management of atlantoaxial instability. | Containment strategies (bracing, osteotomy) in childhood to preserve femoral head sphericity. Later: osteotomy to improve joint congruence, or total hip arthroplasty for end-stage OA. Managing residual deformity and leg length. | Management of spinal stenosis often requires laminectomy/decompression. Limb lengthening procedures are controversial and complex. Management of associated hydrocephalus. |
Surgical Decision Making & Classification
Indications for Surgery:
The patient's severe, debilitating hip pain, coupled with significant functional limitation (manifesting as a pronounced Trendelenburg gait and inability to perform ADLs without severe discomfort), and the unequivocal radiographic evidence of end-stage osteoarthritis in the right hip, rendered him an appropriate candidate for surgical intervention. Conservative management, including NSAIDs, activity modification, and physical therapy, had been attempted for several years with diminishing efficacy. The progressive nature of the disease and the patient's relatively young age, desiring an active lifestyle, further supported the decision for a definitive surgical solution.
Why Operative vs. Non-Operative:
*
Non-Operative Management:
This typically includes analgesics (NSAIDs, acetaminophen), physical therapy aimed at maintaining range of motion and strengthening periarticular muscles, and activity modification to reduce joint stress. Intra-articular injections (corticosteroids or viscosupplementation) may offer temporary symptomatic relief. However, for end-stage degenerative changes as demonstrated by this patient's imaging, non-operative measures are primarily palliative. They do not halt disease progression, restore native joint function, or correct significant anatomical deformities.
*
Operative Management:
Total Hip Arthroplasty (THA) is the recognized gold standard for end-stage hip osteoarthritis. In patients with MED, THA addresses the primary issues of intractable pain, substantially improves functional mobility, and corrects significant biomechanical deformities. While technically challenging due to altered anatomy, THA offers the most predictable and durable relief in these complex cases.
Classification Systems (Relevant to MED & OA):
1.
Multiple Epiphyseal Dysplasia Classification:
While a detailed genetic classification of MED exists (e.g., MED type 1 related to
COMP
mutation, type 2 to
COL9A2
, etc.), for an orthopedic surgeon planning arthroplasty, the
phenotypic presentation
and its specific implications for surgical technique are more immediately relevant. This patient presented with classical features of a dominant MED variant (specifically Fairbank type), characterized by severe coxa plana and coxa magna, leading to profound premature osteoarthritis.
2.
Osteoarthritis Classification (e.g., Tönnis Classification):
This is a radiographic classification system for hip osteoarthritis severity (Grade 0-3). This patient's hip radiographs, showing complete joint space narrowing, subchondral sclerosis, and large osteophytes, would classify as Tönnis Grade 3, indicating severe osteoarthritis. This classification informs the decision for arthroplasty.
3.
Acetabular Bone Loss Classification (e.g., Paprosky Classification):
While primarily used in revision THA, the principles of assessing acetabular bone loss are crucial in primary THA for dysplastic hips. Severe dysplasia often leads to deficiencies in host bone stock, particularly superiorly and anteriorly. Understanding these potential deficiencies guides the selection of the acetabular component (e.g., standard vs. high-offset, augmented cups, or custom implants) and dictates the approach to reaming and fixation.
*

*
This image would typically represent a pre-operative templating overlay or digital planning screenshot for total hip arthroplasty. It illustrates measurements of the acetabulum and femur, potential implant sizes and positions, projected osteotomy levels, and assessment of limb length and offset restoration, all crucial steps for navigating the complex anatomy encountered in Multiple Epiphyseal Dysplasia.
Surgical Technique / Intervention
Procedure: Right Total Hip Arthroplasty (THA)
- Anesthesia: General endotracheal anesthesia was administered, supplemented with a multimodal pain management approach including an epidural catheter for post-operative analgesia and a periarticular nerve block.
- Patient Positioning: The patient was carefully positioned in the left lateral decubitus position on a standard operating table. All bony prominences were meticulously padded to prevent pressure injuries. An axillary roll was utilized, and appropriate limb supports ensured stability and prevented nerve compression.
- Surgical Approach: A standard posterior approach was chosen. This approach offers excellent visualization of both the acetabulum and the proximal femur, which is advantageous in cases of severe anatomical distortion as seen in MED. It allows for comprehensive assessment of posterior osteophytes and facilitates soft tissue releases often required in stiff, dysplastic hips. While a direct anterior approach (DAA) could offer some advantages in terms of recovery, the unpredictable anatomy and need for extensive releases in a dysplastic hip typically favor approaches providing maximal exposure.
- Incision: A curvilinear skin incision was made, centered over the greater trochanter and extending proximally and distally, adhering to typical surgical landmarks.
-
Dissection and Exposure:
- The incision was carried through the skin and subcutaneous tissue. The fascia lata was incised, and a portion was typically harvested for later capsular repair if needed, though primary capsular repair is often achievable.
- The gluteus maximus fibers were split, and the short external rotators (piriformis, superior and inferior gemelli, obturator internus) were identified. These muscles, along with the posterior capsule, were sharply released from their insertions on the greater trochanter. The tendons were tagged with sutures for meticulous repair at closure.
- Careful and systematic release of the posterior capsule and often extensive, hypertrophic osteophytes was required to adequately dislocate the severely dysplastic and often ankylosed femoral head. This step demands patience to prevent iatrogenic fracture.
- Femoral Osteotomy: A high neck osteotomy was performed with an oscillating saw, typically at the base of the femoral neck, to facilitate dislocation and subsequent reaming. The excised femoral head, often flattened and enlarged, was retrieved and sent for histopathological examination.
-
Acetabular Preparation:
- Identification of True Acetabulum: This is arguably the most critical and challenging step in dysplastic hips. The true acetabular floor, often more medially situated and surrounded by significant osteophytes or a false acetabulum formed superiorly, must be precisely identified. Palpation of the teardrop and careful use of fluoroscopy or specific anatomical landmarks (e.g., transverse acetabular ligament, anterior inferior iliac spine) are paramount.
- Reaming: Progressive reaming of the acetabulum was initiated, carefully directed towards the true hip center of rotation. Fluoroscopic guidance was frequently employed to confirm proper depth, inclination (target 40-45 degrees), and anteversion (target 15-20 degrees). Given the inherently shallow nature of the dysplastic acetabulum, controlled medialization of the reamer was utilized to maximize host bone coverage and achieve a stable foundation. In this specific case, careful reaming and medialization proved sufficient for host bone coverage without requiring bone grafting or augmented components.
- Component Insertion: A porous-coated, hemispherical cementless acetabular component (e.g., 52mm diameter) was impacted into the prepared acetabulum. Additional security was achieved by inserting multiple cancellous screws through dedicated holes in the cup, ensuring robust primary stability.
-
Femoral Preparation:
- Broaching: The femoral canal was progressively broached. Due to the known potential for narrow or abnormally shaped medullary canals in patients with MED, initial broaching was performed with smaller sizes and advanced slowly and carefully to prevent iatrogenic femoral fracture. Fluoroscopy was used periodically to confirm correct broach alignment, version, and depth within the canal.
-

- This image would likely be an intraoperative photograph or a surgical schematic depicting the prepared acetabulum and reamed femoral canal during total hip arthroplasty. It highlights the surgical field after osteotomy and preparation, illustrating the readiness for definitive implant insertion, and the careful attention required for bone stock management in dysplastic hips.
- Trial Reduction: Trial components (e.g., a size 9 trial stem, a +0 offset trial femoral head, and a 36mm trial head diameter) were inserted. A trial reduction was performed to meticulously assess limb length, femoral offset, joint stability (anterior, posterior, superior), and the overall range of motion. Adjustments, such as changing stem size, neck length, or head offset, were made as needed to optimize biomechanics, address any pre-existing leg length discrepancies, and ensure adequate soft tissue tension. Restoring proper leg length and femoral offset is critical to improve abductor function and minimize dislocation risk.
- Definitive Femoral Stem Insertion: A cementless, proximally coated femoral stem (e.g., Corail® size 9) was impacted into the prepared femoral canal. Correct version and alignment were verified before final seating.
- Definitive Femoral Head and Liner Insertion: A ceramic femoral head (36mm diameter) was carefully seated onto the taper of the femoral stem. A cross-linked polyethylene liner was then securely locked into the acetabular shell.
- Final Reduction & Stability Assessment: The hip was definitively reduced. Rigorous testing for stability was performed throughout a full range of motion, assessing for any signs of impingement or potential dislocation risk. The soft tissue tension was confirmed to be appropriate.
-

- This image would typically be an intraoperative fluoroscopic image or a post-reduction radiograph taken in the operating theatre. It visually confirms the successful implantation of the total hip components, demonstrating proper alignment, restored leg length, and appropriate femoral offset immediately after the definitive reduction of the hip joint.
- Closure: The short external rotators and posterior capsule were meticulously repaired using robust non-absorbable sutures to enhance posterior stability. The fascia lata, subcutaneous tissue, and skin were then closed in anatomical layers.
- Blood Loss: Estimated blood loss was minimal (approximately 200 ml).
- Intraoperative Complications: No intraoperative complications such as iatrogenic fracture, neurovascular injury, or component malpositioning were encountered.
- Specimen Pathology: The resected femoral head was sent for pathological examination, which confirmed severe degenerative joint disease with extensive cartilage loss and subchondral bone remodeling, consistent with osteoarthritis secondary to MED. No specific features of tumor or infection were noted.
-
- This image presents a post-operative anteroposterior pelvis radiograph, clearly demonstrating the well-positioned cementless total hip arthroplasty components on the right side. The image confirms restoration of the hip's center of rotation, appropriate limb length, and optimal component alignment, indicative of a successful primary arthroplasty.
Post-Operative Protocol & Rehabilitation
The post-operative and rehabilitation protocol was designed to optimize recovery, minimize complications, and restore function, while being mindful of the unique considerations in a patient with MED.
-
Immediate Post-Operative Period (Day 0-3):
- Pain Management: A multimodal analgesia regimen was continued, including epidural/nerve blocks, scheduled oral opioids, NSAIDs (if not contraindicated), and acetaminophen, to effectively manage post-surgical pain and facilitate early mobilization.
- Mobilization: The patient was encouraged to ambulate out of bed with assistance (walker) on Post-Operative Day 0 or 1. Weight-bearing as tolerated (WBAT) was permitted from the outset, promoting early joint motion and preventing stiffness.
- Thromboprophylaxis: Chemical prophylaxis (e.g., low molecular weight heparin) was initiated pre-operatively and continued for 4-6 weeks post-operatively, combined with mechanical prophylaxis (sequential compression devices), to mitigate the risk of deep vein thrombosis (DVT) and pulmonary embolism (PE).
- Hip Precautions: Standard posterior hip precautions (avoiding hip flexion beyond 90 degrees, adduction past the midline, and internal rotation) were strictly enforced for a minimum of 6 weeks. This was critical to minimize the risk of dislocation, especially given the posterior surgical approach and the altered anatomy.
- Physiotherapy: Initial physiotherapy focused on gentle active and passive range of motion exercises within the hip precaution limits, isometric strengthening of hip abductors and extensors, transfer training, and gait training with the walker.
-
Early Rehabilitation (Weeks 1-6):
- Outpatient Physiotherapy: The patient transitioned to an outpatient physiotherapy program. The focus intensified on progressive strengthening of the hip musculature (gluteal muscles, quadriceps, hamstrings), improving gait mechanics, and gradually increasing endurance.
- Range of Motion: Gradual and controlled increase in active and passive range of motion was encouraged, always respecting hip precautions.
- Activity Progression: The patient continued to use a walker or crutches, with progression to a single cane as stability and confidence improved. Light activities of daily living were encouraged, avoiding strenuous activities.
-
Mid-Term Rehabilitation (Weeks 6-12):
- Progression: Depending on clinical progress and surgeon assessment, hip precautions were gradually discontinued. This decision was based on adequate soft tissue healing, muscle strength, and patient adherence.
- Strengthening and Conditioning: More advanced strengthening exercises were introduced, including resistance training. Proprioceptive training and balance exercises were emphasized to further improve stability and coordination.
- Return to Activity: A gradual return to light recreational activities was permitted, with guidance from the physiotherapist.
-
Long-Term Rehabilitation (Beyond 12 Weeks):
- Maintenance: Patients are encouraged to maintain a lifelong home exercise program to preserve strength and flexibility.
- Return to Sport/High-Impact Activities: High-impact activities (e.g., running, jumping sports) and contact sports are generally discouraged after THA, particularly in younger patients and those with underlying bone conditions, due to increased risk of implant wear, loosening, and periprosthetic fracture. Low-impact activities such as swimming, cycling, and walking are highly encouraged.
- Follow-up: Regular clinical and radiographic follow-up appointments were scheduled (e.g., at 6 weeks, 3 months, 6 months, 1 year, then annually). These appointments monitor for component stability, signs of aseptic loosening, osteolysis, or other potential complications.
-

- This image typically represents a follow-up radiograph at 6-12 months post-total hip arthroplasty, demonstrating stable components with evidence of good bony ingrowth (for cementless implants), maintained joint space, and no signs of loosening, migration, or progressive osteolysis, indicating a favorable long-term outcome.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Clinical Suspicion: Always maintain a high index of suspicion for underlying skeletal dysplasia, such as MED, in young patients presenting with premature, severe, often bilateral, and symmetrical osteoarthritis, especially affecting the hips, knees, and ankles. A positive family history is a strong indicator.
- Genetic Confirmation: While not always mandatory for immediate surgical decision-making in end-stage disease, genetic testing can definitively confirm the diagnosis of MED and differentiate it from other dysplasias. This is crucial for accurate prognosis, family counseling, and understanding potential systemic manifestations.
-
Comprehensive Pre-operative Planning is Paramount:
- Advanced Imaging: Calibrated plain radiographs are the starting point. However, CT scans are invaluable for 3D visualization of the complex dysplastic anatomy, precise assessment of bone stock deficiencies (especially in the acetabulum), identification of the true acetabular floor, and guidance for component sizing and placement. MRI may offer insights into soft tissue structures but is often less critical than CT for bony templating in end-stage OA.
- Meticulous Templating: Digital or manual templating helps anticipate challenges such as significant bone loss, difficulty in identifying the true hip center of rotation, need for offset restoration, and potential leg length discrepancies.
-
Managing Dysplastic Anatomy During Surgery:
- Acetabulum: Dysplastic acetabula are often shallow, hypoplastic, and can be retroverted. The goal is to medialise the hip center of rotation as much as safely possible to reduce joint reaction forces and improve the abductor moment arm. Ensure adequate host bone coverage for cementless components. Bone grafting or custom acetabular components may be necessary for severe superior or medial deficiencies.
- Femur: Patients with MED typically present with coxa plana and coxa magna, characterized by enlarged, flattened femoral heads and short, broad femoral necks. The medullary canal can be narrow or irregularly shaped, necessitating smaller broaches and stems, or potentially custom femoral stems. Be prepared for increased femoral anteversion.
- Soft Tissue Considerations: Expect significant contractures, especially in long-standing cases. Extensive soft tissue releases may be required to achieve adequate range of motion, prevent impingement, and facilitate dislocation and reduction.
- Component Selection: While cementless components are generally favored in younger patients due to their longevity, careful assessment of bone quality and potential canal morphology is essential. In cases of compromised bone stock, hybrid or cemented constructs may be a more prudent choice.
- Restoring Biomechanics: Precise restoration of limb length and femoral offset is critical for optimizing gluteal abductor function, eliminating the Trendelenburg gait, and minimizing the risk of post-operative dislocation. Intraoperative fluoroscopy or specific leg length measuring devices can be highly beneficial.
- Expected Outcomes: THA in MED patients generally yields excellent pain relief and significant functional improvement. However, due to the younger age at surgery, potentially higher activity levels, and altered bone mechanics, component longevity may be reduced compared to primary THA in non-dysplastic patients.
- Multidisciplinary Approach: Consider collaboration with geneticists for definitive diagnosis and counseling, rheumatologists for systemic management, and pain management specialists for refractory pain.
Pitfalls:
- Underestimation of Anatomical Distortion: Failure to fully appreciate the severity and complexity of the dysplastic anatomy pre-operatively can lead to significant intraoperative challenges, malpositioning of components, and ultimately suboptimal functional outcomes.
- Inadequate Acetabular Coverage/Fixation: Incorrect identification of the true acetabulum or inadequate preparation can result in insufficient host bone coverage for the acetabular component, increasing the risk of early aseptic loosening, migration, and osteolysis.
- Iatrogenic Femoral Fracture: Aggressive reaming or broaching within an abnormally shaped or narrow femoral canal can lead to iatrogenic femoral fracture, particularly in the dense, often stiff dysplastic bone. Careful, slow, and incremental broaching is essential.
- Neurovascular Injury: Extensive soft tissue releases, particularly around the posterior aspect of the hip and near the true acetabular floor, increase the risk of injury to the sciatic nerve, femoral nerve, or major vascular structures. Meticulous dissection and careful retraction are paramount.
- Uncorrected Leg Length Discrepancy: Failure to accurately restore limb length can result in persistent gait abnormalities, compensatory spinal issues, and significant patient dissatisfaction. This requires meticulous pre-operative planning and intra-operative verification.
- Post-operative Dislocation: The risk of dislocation can be higher if soft tissue tension is inadequate, component version is suboptimal, or if significant pre-existing contractures are not fully released. Strict adherence to hip precautions is crucial initially.
- Periprosthetic Fracture: Dysplastic bone can be inherently weaker and more brittle, predisposing to periprosthetic fractures both intraoperatively (during stem insertion) and postoperatively following minor trauma.
- Premature Component Loosening/Wear: Younger age at surgery, higher activity demands, and altered stress distribution in dysplastic bone can lead to accelerated polyethylene wear and earlier aseptic loosening of components, potentially necessitating earlier revision surgery.
- Ignoring Other Joint Involvement: MED is a systemic condition affecting multiple epiphyses. While focusing on the primary surgical site (e.g., hip), it is crucial to remain cognizant of other affected joints (knees, ankles, spine) that may develop progressive osteoarthritis requiring future intervention.
- Incomplete Correction of Deformity: Simply implanting components without adequately correcting underlying biomechanical deformities (e.g., severe femoral anteversion or acetabular retroversion) can compromise the long-term success and functional outcome of the arthroplasty.
Clinical & Radiographic Imaging

