As a highly respected Academic Orthopedic Surgeon and Medical Educator, I present an exhaustive review of Ellis-Van Creveld (EVC) syndrome, focusing on its critical orthopedic and oral manifestations relevant to surgical management. This guide is tailored for orthopedic surgeons, residents, and medical students, emphasizing high-yield clinical and surgical principles.
Introduction & Epidemiology
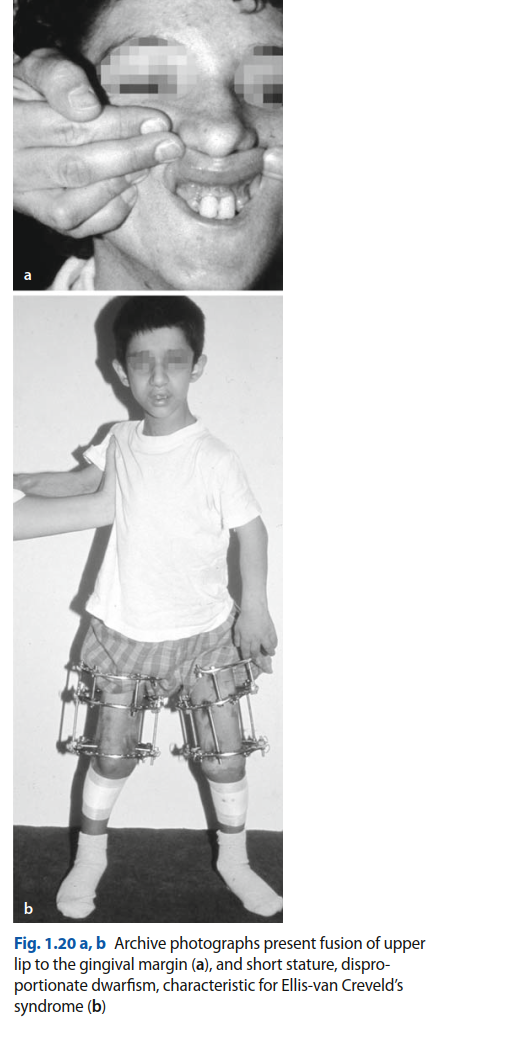
Ellis-Van Creveld (EVC) syndrome, also known as chondroectodermal dysplasia, is a rare, autosomal recessive osteochondrodysplasia characterized by a distinct constellation of clinical features primarily affecting the skeletal, oral, and cardiovascular systems. First described by Richard W. B. Ellis and Simon Van Creveld in 1940, the syndrome is a multisystemic disorder with variable expressivity.
The genetic basis of EVC lies in mutations within the EVC and EVC2 genes, located adjacently on chromosome 4p16. These genes encode proteins that play a crucial role in the Hedgehog signaling pathway, a fundamental regulator of embryonic development, particularly in limb, heart, and craniofacial patterning. Disruption of this pathway leads to the characteristic developmental anomalies observed in affected individuals.
Epidemiologically, EVC syndrome is rare, with an estimated incidence ranging from 1 in 60,000 to 1 in 200,000 live births globally. However, specific populations exhibit a significantly higher prevalence due to founder effects and consanguinity, most notably among the Old Order Amish population in Lancaster County, Pennsylvania, where the incidence can be as high as 1 in 5,000 live births. This clustering provides valuable cohorts for genetic and clinical studies.
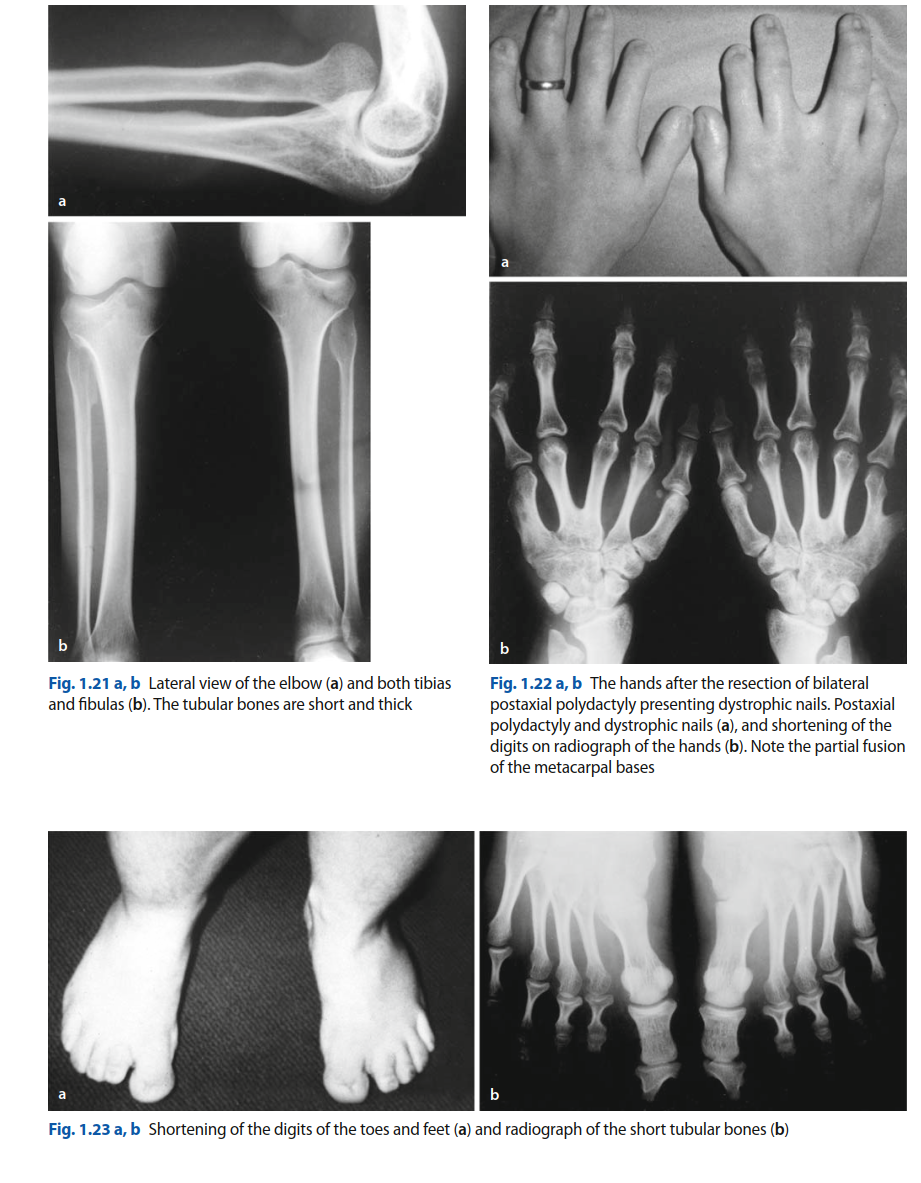
The clinical spectrum of EVC syndrome is broad, encompassing short-limbed dwarfism (mesomelic and acromelic types), postaxial polydactyly of both hands and feet, characteristic ectodermal dysplasias affecting nails and teeth, and a high incidence of congenital cardiac defects, most commonly an atrial septal defect (ASD). Oral manifestations include natal or neonatal teeth, supernumerary frenula, hypoplastic or dysplastic enamel, and abnormal dentition. Given its multisystemic nature, effective management necessitates a multidisciplinary approach involving orthopedics, oral and maxillofacial surgery, cardiology, pediatrics, and genetics. This review will delve specifically into the orthopedic and oral aspects amenable to surgical intervention, providing a comprehensive reference for clinical practice.
Surgical Anatomy & Biomechanics
A thorough understanding of the distinct anatomical and biomechanical alterations in EVC syndrome is paramount for effective surgical planning and execution. The skeletal and oral anomalies present unique challenges and considerations.
Skeletal Dysplasia
The skeletal abnormalities in EVC syndrome are primarily characterized by mesomelic and acromelic short-limbed dwarfism, meaning the middle (forearm, lower leg) and distal (hands, feet) segments of the limbs are disproportionately short compared to the proximal segments. This is a crucial distinction from rhizomelic dwarfism (proximal limb shortening).
- Long Bones: The tibia, fibula, radius, and ulna are typically hypoplastic and shortened, leading to significant limb length discrepancies. The overall bone architecture can be robust, but growth plates may show irregularities, including cone-shaped epiphyses, particularly in the phalanges and metacarpals.
-
Polydactyly:
Postaxial polydactyly of the hands (often on the ulnar side) and feet is a hallmark feature, present in nearly all affected individuals. This can range from a rudimentary skin tag to a fully formed extra digit, often with its own metacarpal/phalangeal components and neurovascular supply. The presence and morphology of the extra digit significantly impact hand function, grip, and shoe wear.
- Genu Valgum: A common angular deformity, genu valgum (knock-knees), often develops due to disproportionate growth of the medial and lateral femoral or tibial physes, compounded by altered biomechanics of gait in short-statured individuals. This can lead to patellofemoral pain, early degenerative changes, and functional impairment.
- Hip Dysplasia: Acetabular shallowing and varying degrees of femoral head abnormalities are frequently observed, contributing to hip instability, subluxation, or frank dislocation. The biomechanics of the hip joint are compromised, potentially leading to pain and accelerated osteoarthritis if untreated.
- Radial Head Dislocation: Persistent anterior or posterior dislocation of the radial head is a recognized feature, affecting elbow range of motion and often leading to a characteristic elbow deformity. While often asymptomatic in early life, it can become painful or functionally limiting with age.
- Carpal and Tarsal Anomalies: Carpal fusions, particularly of the capitate and hamate, are common, leading to reduced wrist mobility. Similar fusions can occur in the tarsal bones, affecting foot mechanics.
- Thoracic Cage: A narrow, short thorax with short ribs is characteristic, especially in severe cases, which can compromise pulmonary function and predispose to recurrent respiratory infections, particularly in infancy. This has significant implications for anesthetic management.
- Spine: Scoliosis or kyphosis can occur, though less consistently than limb deformities. Spinal involvement is typically mild, but should be screened for.
Oral Manifestations
The oral cavity is significantly affected in EVC syndrome, often presenting unique challenges for feeding, speech, and dental hygiene.
- Alveolar Ridge Fusion: A distinctive feature is the fusion of the anterior maxillary alveolar ridge to the upper lip, creating a shallow oral vestibule and potentially contributing to a median pseudo-cleft of the upper lip. This significantly restricts lip mobility and makes oral hygiene difficult.
- Natal/Neonatal Teeth: The presence of teeth at birth (natal) or within the first month of life (neonatal) is common. These teeth are often premature, hypoplastic, and poorly anchored, posing risks of aspiration, tongue ulceration (Riga-Fede disease), and irritation to the mother during breastfeeding.
- Supernumerary Frenula: Multiple or hypertrophied frenula, particularly the labial frenulum, are frequently observed. These can further restrict lip movement and contribute to diastema or malocclusion.
- Dental Hypoplasia/Dysplasia: Enamel hypoplasia, small or conical teeth (microdontia), and partial anodontia (missing teeth) are common. These teeth are prone to early caries and increased sensitivity.
- Malocclusion: A combination of jaw size discrepancies, abnormal tooth morphology, and premature tooth eruption often leads to significant malocclusion.
-
Gingival Hyperplasia:
Generalized gingival hyperplasia can be present, contributing to difficulties with oral hygiene and increasing susceptibility to periodontal disease.
Cardiac Considerations
While not directly part of the surgical anatomy for orthopedic or oral procedures, the high incidence of congenital heart disease (50-60%), predominantly atrial septal defect (ASD), is a critical anatomical and physiological consideration. A single common atrium is also observed. The presence and severity of cardiac anomalies significantly impact perioperative risk and anesthetic management. A detailed cardiology assessment is mandatory prior to any surgical intervention.
Indications & Contraindications
Surgical intervention in Ellis-Van Creveld syndrome is typically indicated to address functional impairment, pain, progressive deformity, or significant cosmetic concerns. A careful risk-benefit analysis is essential, considering the systemic nature of the syndrome and potential anesthetic challenges.
Orthopedic Indications for Surgery
-
Polydactyly Excision:
- Functional impairment: Interference with grip, shoe wear, or pain from pressure.
- Cosmetic concerns: Significant psychosocial impact, especially in visible areas like hands.
- Progressive deformity: If the extra digit is contributing to deformity of adjacent digits.
-
Limb Lengthening:
- Significant short stature: When disproportionate shortening of limbs severely impacts ambulation, ability to perform activities of daily living (ADLs), or quality of life. Typically considered for discrepancies greater than 5 cm or global short stature in adolescence.
- Severe psychosocial impact: Addressing body image issues and integration into society.
-
Correction of Angular Deformities (e.g., Genu Valgum):
- Progressive deformity: Valgus angles exceeding 15-20 degrees in the knee that are progressing.
- Symptomatic gait disturbance: Pain, limping, instability.
- Risk of degenerative arthritis: To preserve joint longevity and function.
-
Clubfoot Correction:
- Recurrent or rigid deformity: After initial conservative management (e.g., Ponseti method) fails to achieve or maintain correction.
- Severe equinovarus: Significant functional limitation for ambulation.
-
Hip Dysplasia Management:
- Persistent subluxation or dislocation: To restore joint congruity and prevent premature degenerative arthritis.
- Acetabular index: Specific age-dependent radiological criteria (e.g., >30 degrees in infancy).
- Pain or Trendelenburg gait: Functional impairment.
-
Radial Head Reduction/Stabilization:
- Symptomatic: Pain, limited range of motion (pronation/supination).
- Progressive elbow dysfunction: Impairment of ADLs.
Oral Indications for Surgery
-
Extraction of Natal/Neonatal Teeth:
- Risk of aspiration: Due to mobility and poor anchorage.
- Irritation/Trauma: To the infant's tongue (Riga-Fede disease) or mother's breast during feeding.
- Feeding difficulties: Impaired latch or suckling.
-
Frenulectomy/Frenectomy:
- Impaired lip mobility: Affecting feeding, speech development, or oral hygiene.
- Contribution to malocclusion or diastema: If interfering with orthodontic treatment or tooth alignment.
-
Release of Alveolar-Lip Synechiae:
- Impaired feeding: Inability to create a proper seal for suckling.
- Speech impediments: Due to restricted lip movement.
- Poor oral hygiene: Inability to effectively clean the teeth and gingiva.
-
Cleft Palate Repair (if present):
- Standard indications for cleft palate repair to facilitate feeding, speech, and prevent recurrent otitis media.
Contraindications
Absolute and relative contraindications must be carefully considered for any surgical procedure in EVC syndrome patients.
- Severe Cardiac Compromise: Untreated, large atrial septal defects with significant shunting, pulmonary hypertension, or complex single ventricle physiology represent a major anesthetic and surgical risk. Cardiology clearance is paramount.
- Severe Respiratory Compromise: Significant pulmonary hypoplasia or restrictive lung disease due to a narrow thorax, active respiratory infections, or a history of recurrent pulmonary complications.
- Uncontrolled Systemic Infection: Any active infection, particularly if near the surgical site.
- Severe Nutritional Deficiencies: Poor healing and increased complication rates.
- Anesthetic Risks: Unmanageable difficult airway, severe reactions to anesthetic agents.
- Lack of Clear Functional Benefit: Procedures primarily for cosmetic reasons may be contraindicated if surgical risks are high, especially in very young or medically fragile patients.
- Patient/Family Refusal: After comprehensive discussion of risks and benefits.
Operative vs. Non-Operative Indications
The decision between operative and non-operative management often involves a shared decision-making process with the family, considering the child's overall health, severity of the anomaly, and potential for long-term functional improvement versus surgical morbidity.
| Feature/Condition | Operative Indication | Non-Operative Indication |
|---|---|---|
| Postaxial Polydactyly | Symptomatic (pain, irritation with shoe/glove wear), significant functional impairment, severe cosmetic concern, bony articulation. | Asymptomatic skin tag, rudimentary digit without bony articulation, minimal functional or cosmetic impact. |
| Short Stature (Limb) | Severe functional impairment (gait, ADLs), significant limb length discrepancy (>5cm), psychosocial distress unresponsive to conservative measures. | Mild shortening, patient/family preference against extensive procedures, high surgical risk, poor bone quality. |
| Genu Valgum | Progressive deformity (>15-20 degrees), symptomatic gait disturbance, risk of early degenerative arthritis, failed guided growth. | Mild deformity (<15 degrees), asymptomatic, observation in growing child (especially if physes are open), guided growth (hemiepiphysiodesis) as a less invasive option. |
| Hip Dysplasia | Persistent subluxation/dislocation after non-operative treatment, acetabular index >30-35 degrees (age-dependent), pain, Trendelenburg gait. | Mild dysplasia, stable subluxation amenable to bracing (Pavlik harness in infancy), asymptomatic. |
| Clubfoot | Recurrent/rigid deformity after serial casting (Ponseti method), significant residual adduction/varus, functional impairment. | Initial presentation, flexible deformity, amenable to Ponseti method or gentle stretching/bracing. |
| Radial Head Dislocation | Symptomatic (pain, significantly limited ROM), progressive functional impairment. | Asymptomatic, minimal functional limitation. |
| Natal/Neonatal Teeth | Risk of aspiration, trauma to tongue/mother's breast, significant mobility. | Stable, asymptomatic, no risk of aspiration. |
| Alveolar-Lip Synechiae | Impaired feeding, speech, oral hygiene, significant restriction of lip movement. | Mild, no functional impairment, patient/family preference. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial in EVC syndrome, necessitating a highly coordinated multidisciplinary approach.
Multidisciplinary Team
A comprehensive team ensures all aspects of the patient's complex needs are addressed:
*
Orthopedic Surgeon:
Primary surgeon, responsible for skeletal corrections.
*
Oral & Maxillofacial Surgeon/Pediatric Dentist:
Manages oral anomalies.
*
Cardiologist:
Essential for pre-operative cardiac evaluation and risk stratification for ASD or other cardiac defects.
*
Anesthesiologist (Pediatric):
Critical for airway management, intraoperative monitoring, and pain control, particularly given potential difficult airway and cardiac shunts.
*
Pediatrician:
General medical optimization and co-morbidity management.
*
Geneticist:
Provides counseling and confirms diagnosis.
*
Physical & Occupational Therapists:
For pre- and post-operative rehabilitation planning.
*
Social Worker/Child Life Specialist:
Supports the family and child through the surgical journey.
Cardiac Evaluation
This is arguably the most critical pre-operative step. All patients with EVC syndrome require:
*
Echocardiography:
To define the type and severity of congenital heart disease (ASD, VSD, single atrium, etc.).
*
Cardiology Consultation:
To assess surgical risk, optimize cardiac function, and determine the need for prophylactic antibiotics if an unrepaired cardiac defect is present. Severe pulmonary hypertension or uncorrected large shunts may contraindicate elective surgery.
Respiratory Evaluation
Given the potential for a narrow thorax and restricted lung volumes, a thorough respiratory assessment is vital:
*
Baseline Pulmonary Function Tests:
(Age-appropriate) if concern for restrictive lung disease.
*
Anesthesia Consultation:
To anticipate and plan for a potentially difficult airway (due to micrognathia or abnormal facial anatomy), restricted chest wall excursion, and potential need for post-operative respiratory support. Equipment for difficult intubation (fiberoptic bronchoscope, LMA) should be readily available.
Imaging
- Plain Radiographs: Long bone series, hand and foot films, pelvis, and spine to characterize skeletal deformities, assess bone age, and identify carpal/tarsal fusions. Essential for surgical planning (e.g., osteotomy angles, fixation length).
- CT/MRI: May be indicated for complex joint deformities (e.g., hip, elbow) or limb length discrepancies if detailed 3D anatomy is required for pre-operative planning of osteotomies or fixation.
- Dental Radiographs: For oral anomalies to assess tooth eruption, root morphology, and presence of supernumerary teeth.
Specific Considerations
- Blood Loss: Procedures such as limb lengthening osteotomies or complex angular corrections can involve significant blood loss. Type and cross-match should be performed, and blood products made available.
- Bone Quality: While bone quality in EVC is generally normal, healing may be prolonged. Consideration of bone graft substitutes or osteoinductive agents may be prudent for certain osteotomies.
- Skin and Nail: Ectodermal dysplasia can manifest as thin, fragile skin or dysplastic nails, requiring careful tissue handling and wound closure.
- Consent: Detailed discussion with parents/guardians about the multisystemic nature, potential complications, and realistic outcomes, especially for limb lengthening which is a prolonged and arduous process.
Patient Positioning
Positioning varies based on the specific surgical procedure but always requires meticulous attention to prevent pressure sores, nerve palsies, and ensure adequate surgical access:
*
Supine:
Common for lower limb procedures (e.g., genu valgum correction, tibial lengthening, hip procedures). Ensure head and neck are neutral, arms adducted, and pressure points padded.
*
Lateral Decubitus:
For certain hip or femoral procedures.
*
Prone:
Rarely for EVC, but if spinal deformity requires it, careful attention to respiratory mechanics is needed due to narrow thorax.
*
Hand/Foot Surgery:
Upper limb procedures often utilize a hand table; lower limb procedures require appropriate limb holders.
Given the potential for joint laxity or altered joint mechanics, careful and gradual positioning is necessary to avoid iatrogenic injury.
Detailed Surgical Approach / Technique
This section will outline key surgical techniques commonly employed in managing orthopedic and oral manifestations of Ellis-Van Creveld syndrome.
1. Polydactyly Excision (Postaxial Hand Polydactyly)
Postaxial polydactyly, often involving the small finger side, is a frequent indication. The surgical technique depends on the morphology (rudimentary skin tag vs. fully articulated digit).
Pre-Operative:
- Careful clinical assessment and radiographs to determine bone and joint involvement, presence of shared neurovascular bundles, and intrinsic muscle attachments.
- Marking: The planned incision line should be meticulously marked with the limb in a functional position, accounting for skin redundancy and potential scar contracture.
Surgical Steps:
- Anesthesia: General anesthesia is typical for pediatric patients. Upper extremity block (e.g., axillary block) can provide excellent post-operative analgesia.
- Tourniquet: Apply a pneumatic tourniquet to the upper arm and exsanguinate the limb to ensure a bloodless field.
- Incision: For a fully formed supernumerary digit, a racquet-shaped or elliptical incision is typically made around its base, extending proximally along the border of the digit to be retained. For rudimentary tags, a simple elliptical excision may suffice.
-
Dissection:
- Carefully dissect soft tissues, identifying and ligating any neurovascular bundles supplying only the supernumerary digit. Preserve the neurovascular structures of the adjacent, functional digit.
- Identify and excise any accessory tendons, or if a shared extensor/flexor tendon is present, release the portion going to the accessory digit and repair the remaining tendon to the retained digit.
- For digits with bony articulation (e.g., an accessory metacarpal or phalanx), disarticulate it from its base or perform an osteotomy at the junction of the accessory and main bone. Remove any cartilaginous rests or abnormal ossicles.
-
Soft Tissue Reconstruction:
- If collateral ligaments of the retained digit were disrupted, repair them using fine non-absorbable sutures.
- If intrinsic muscles were involved, reattach them to the remaining structures to restore function and prevent deviation.
- The aim is to reconstruct a stable, functional fifth ray (or appropriate ray) without residual deformity.
-
Closure:
- Achieve meticulous hemostasis.
- Close the subcutaneous layer with fine absorbable sutures.
- Close the skin with non-absorbable sutures (e.g., 6-0 nylon) to ensure a neat scar.
- Dressing and Splinting: Apply a sterile dressing and a light protective splint (e.g., plaster slab) to immobilize the digit for 2-3 weeks, protecting the repair and promoting healing.
2. Distal Femoral Valgus Osteotomy (for Genu Valgum)
This procedure corrects genu valgum by realigning the mechanical axis of the limb, often performed as a medial opening wedge or lateral closing wedge osteotomy.
Pre-Operative:
- Full-length standing radiographs (scanograms) to measure mechanical axis deviation, femoral valgus angle (FVA), and identify the apex of the deformity.
- Surgical planning involves templating on radiographs to determine the osteotomy level, wedge size, and plate placement.
Surgical Steps (Lateral Closing Wedge Technique):
- Anesthesia: General anesthesia. Epidural catheter for post-operative pain management is highly beneficial.
- Positioning: Supine on a radiolucent table, with affected limb draped free for manipulation and imaging. A lateral bump under the hip can facilitate access.
-
Approach:
- A straight lateral incision, approximately 8-10 cm long, centered over the distal femur, proximal to the lateral epicondyle.
- Dissect through subcutaneous tissue. Identify and protect the iliotibial band.
- Internervous Plane: The approach can be made between the vastus lateralis (anterior) and the lateral intermuscular septum (posterior). Reflect the vastus lateralis anteriorly off the femur.
- Expose the lateral aspect of the distal femur. Protect the common peroneal nerve posteriorly and popliteal vessels medially.
-
Osteotomy:
- Place a guide wire (e.g., K-wire) perpendicular to the femoral shaft axis, approximately 1.5-2 cm proximal to the physis (if open) or articular cartilage.
- Make the first osteotomy cut using an oscillating saw, parallel to the guide wire, extending about two-thirds of the way across the femur.
- Insert a second guide wire proximally, angled to create the desired wedge (calculated pre-operatively). Make the second osteotomy cut converging with the first, again about two-thirds across.
- Crucial: Preserve the medial periosteum and a small medial cortical hinge to maintain stability and prevent iatrogenic fracture.
- Remove the bone wedge. Gradually close the osteotomy, using intraoperative fluoroscopy to confirm correction of the mechanical axis.
-
Fixation:
- Apply a pre-contoured locking plate (e.g., a lateral distal femoral locking plate) to the lateral aspect of the femur.
- Secure the plate with locking screws, ensuring adequate purchase in both proximal and distal fragments. Dynamic compression may be used if appropriate.
-
Closure:
- Irrigate the wound thoroughly.
- Close deep fascial layers and vastus lateralis.
- Subcutaneous and skin closure.
- Post-Operative: Apply a soft dressing; a knee immobilizer may be used, though often not necessary with stable internal fixation.
3. Tibial Lengthening (Monorail External Fixator)
Limb lengthening for significant short stature is a complex and protracted process.
Pre-Operative:
- Detailed assessment of limb length discrepancy, neurovascular status, and joint mobility.
- Patient and family education regarding the long duration of treatment, potential complications, and intensive rehabilitation.
- Templating for fixator placement and osteotomy level.
Surgical Steps (Overview):
- Anesthesia: General anesthesia. Consider epidural for analgesia.
- Positioning: Supine, affected limb draped free.
-
Fixator Application:
- Apply a monorail external fixator (e.g., LRS, Orthofix) to the tibia, ensuring pins are placed meticulously to avoid neurovascular structures and growth plates. Proximal and distal fixation blocks are secured with multiple half-pins or wires.
- The fixator is positioned parallel to the mechanical axis of the tibia.
-
Corticotomy (Percutaneous or Mini-Open):
- Make a small incision over the metaphyseal-diaphyseal junction of the tibia (e.g., proximal or distal).
- Internervous Plane: No true internervous plane; carefully dissect through skin, subcutaneous tissue, and periosteum.
- Using an osteotome or small oscillating saw, perform a low-energy corticotomy, preserving the periosteal sleeve as much as possible to facilitate osteogenesis. The fibula must also be osteotomized (or distal tibiofibular syndesmosis released) to allow for tibial lengthening.
- Closure: Small skin incisions are closed. Pin sites are dressed.
-
Post-Operative Protocol (Distraction Osteogenesis):
- Latency Phase: 5-7 days of rest to allow initial callus formation.
- Distraction Phase: Begin distraction at 1 mm per day (e.g., 0.25 mm x 4 times daily) until the desired length is achieved. This is a crucial phase requiring close monitoring for neurovascular compromise, pain, and pin site infections.
- Consolidation Phase: Once length is achieved, the fixator remains in place while the regenerate bone matures and consolidates. Weight-bearing is progressively increased. This phase can be several months long (often 1.5-2 times the distraction time).
- Fixator Removal: Once consolidation is complete (radiographic evidence of corticalization across three cortices), the fixator is removed.
4. Oral Procedures: Natal/Neonatal Teeth Extraction & Frenulectomy
These are typically minor oral surgical procedures but require careful attention in this population.
Pre-Operative:
- Clinical examination of the oral cavity.
- Assessment of tooth mobility, aspiration risk.
- Evaluation of frenulum hypertrophy and its impact.
- For infants, ensure adequate feeding and hydration status.
Surgical Steps:
- Anesthesia: Local anesthesia (lidocaine with epinephrine) is typically sufficient for older children. For infants, local anesthetic with or without light sedation is preferred, often in an operating room setting due to aspiration risk and need for airway control.
-
Natal/Neonatal Teeth Extraction:
- If the tooth is highly mobile and poses an aspiration risk, gentle extraction using small dental forceps is performed.
- These teeth often have rudimentary root formation, making extraction straightforward.
- Achieve hemostasis with local pressure and gauze. Sutures are rarely needed.
-
Frenulectomy:
- For hypertrophied labial frenula, infiltrate with local anesthetic.
- Clamp the frenulum with a hemostat, then incise with a scalpel or electrocautery above and below the clamp.
- Excise the excess tissue.
- Primary closure with fine absorbable sutures (e.g., 5-0 chromic gut) can be performed, or the wound may be left to heal by secondary intention, especially if electrocautery is used.
- Carefully avoid damage to adjacent salivary ducts or structures.
-
Alveolar-Lip Synechiae Release:
- Infiltrate the fibrous band with local anesthetic.
- Incise the fibrous band transversely to release the tension between the lip and the alveolar ridge.
- Close the defect longitudinally with absorbable sutures to prevent re-adhesion. A Z-plasty or V-Y plasty may be considered for more complex cases to improve vestibular depth.
- Post-Operative: Soft diet, good oral hygiene, and pain management with acetaminophen.
Complications & Management
Given the systemic nature of Ellis-Van Creveld syndrome, patients are susceptible to a range of surgical complications, requiring vigilance and prompt management.
Orthopedic Complications
-
Infection:
- Pin site infection (External Fixators): Common (up to 80% minor, 10-20% major in lengthening). Management includes meticulous pin site care, oral antibiotics for superficial infections, and debridement/pin exchange for deeper or resistant infections.
- Deep Surgical Site Infection: Rare but serious. Requires surgical debridement, intravenous antibiotics, and potentially removal of hardware if the infection persists.
-
Nonunion/Delayed Union:
(Especially in limb lengthening or osteotomies)
- Incidence: Varies, but 5-20% in limb lengthening.
- Management: Prolonged immobilization, extended external fixation, bone grafting (autograft or allograft), osteoinductive agents (e.g., BMPs), or internal fixation (exchange nailing) for nonunions. Gradual distraction parameters may need adjustment.
- Neurovascular Injury: Rare but catastrophic. Careful surgical technique, intraoperative monitoring, and prompt recognition/repair are paramount.
- Re-deformity: The underlying growth plate pathology can lead to recurrence of angular deformities or limb length discrepancy. Management may involve repeat osteotomy, guided growth techniques (hemiepiphysiodesis), or further lengthening procedures.
- Joint Stiffness/Contractures: Common post-lengthening, especially of the ankle or knee. Requires aggressive physical therapy, dynamic splinting, and sometimes percutaneous tenotomies or capsulotomies.
- Hardware-related complications: Screw breakage, plate loosening, soft tissue irritation from implants. May require hardware removal or revision.
- Uneven Lengthening: In limb lengthening, differential growth of two bones (e.g., tibia and fibula) can occur, requiring secondary procedures.
Oral Complications
- Bleeding: Post-extraction or post-frenulectomy. Managed with local pressure, hemostatic agents, or suturing.
- Infection: Oral infections are rare but can occur. Managed with oral antibiotics and local drainage if an abscess forms.
- Recurrence of Frenula/Synechiae: Due to scar contracture. May require repeat surgery, sometimes with Z-plasty or V-Y plasty for more durable release.
- Damage to Adjacent Structures: Injury to salivary ducts or tooth buds during frenulectomy or extraction. Careful technique and anatomical knowledge are key.
- Speech or Feeding Issues: Can persist or worsen if surgical correction is inadequate or if underlying muscle dysfunction is significant. May require ongoing speech and occupational therapy.
General/Systemic Complications
- Cardiac Events: Given the high prevalence of ASD, cardiac arrhythmia, heart failure exacerbation, or paradoxical embolism can occur. Pre-operative optimization and meticulous intraoperative cardiac monitoring by an experienced anesthesiologist are essential.
- Respiratory Compromise: Due to a narrow thorax and potential pulmonary hypoplasia, patients are at increased risk for atelectasis, pneumonia, and respiratory failure, especially post-operatively. Careful airway management, early mobilization, and chest physiotherapy are vital.
- Difficult Airway: Micrognathia and other craniofacial anomalies can make intubation challenging. Requires experienced anesthesiologists and appropriate equipment (fiberoptic scope).
- Anesthetic Reactions: As with any patient, allergic reactions or adverse drug effects can occur.
Complications & Salvage Strategies
| Complication | Incidence | Salvage Strategy / Management |
|---|---|---|
| Orthopedic | ||
| Pin Site Infection (Ex-fix) | High (up to 80% minor, 10-20% major) | Aggressive local cleaning, oral antibiotics for superficial infection. Debridement, pin removal/exchange for severe/deep infection. |
| Nonunion/Delayed Union | Varies (5-20% in lengthening) | Prolonged fixation, bone grafting (autograft/allograft), osteoinductive agents (BMPs), focused ultrasound, internal fixation (e.g., exchange nailing) once distraction completed. |
| Neurovascular Injury | Low (<1%) | Intraoperative identification and immediate repair. Post-operative neurological assessment, urgent re-exploration if symptoms arise. |
| Re-deformity | Varies (5-15% after correction) | Repeat osteotomy, guided growth (hemiepiphysiodesis), further lengthening/correction with external fixation, bracing. |
| Joint Stiffness/Contractures | Common post-lengthening | Intensive physical therapy, dynamic splinting, serial casting, surgical release (e.g., tenotomies, capsulectomies). |
| Oral/Dental | ||
| Post-extraction Bleeding | Low | Local pressure, hemostatic agents (gelatin sponge, topical thrombin), suturing of extraction site. |
| Post-operative Infection | Low | Oral antibiotics, drainage if abscess formation. |
| Recurrence of Frenula/Synechiae | Varies | Repeat frenulectomy, consideration of Z-plasty or V-Y plasty for improved vestibular depth and reduced recurrence. |
| General/Systemic | ||
| Cardiac Event (due to ASD) | Dependent on severity; 50-60% incidence | Pre-operative cardiology clearance and optimization. Intraoperative vigilant monitoring, appropriate anesthetic management for shunting lesions. Post-operative cardiac support as needed. |
| Respiratory Compromise | Increased risk | Pre-operative pulmonary assessment. Experienced pediatric anesthesiologist. Careful airway management. Post-operative ventilatory support, chest physiotherapy, early mobilization. |
| Difficult Airway | Increased risk | Experienced anesthesiologist, availability of fiberoptic bronchoscope, LMA, surgical airway readiness. Careful pre-operative assessment for micrognathia. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of successful outcomes in Ellis-Van Creveld syndrome, requiring a dedicated and often prolonged multidisciplinary effort.
Orthopedic Rehabilitation
- Pain Management: Crucial for early mobilization and participation in therapy. A multimodal approach including regional blocks (epidural, nerve blocks), oral analgesics (NSAIDs, opioids), and muscle relaxants is often employed.
-
Physical Therapy (PT):
- Range of Motion (ROM): Initiated early to prevent stiffness and contractures, especially around joints affected by lengthening or osteotomy. Passive and active ROM exercises, continuous passive motion (CPM) machines may be used.
- Strengthening: Progressive resistance exercises to restore muscle strength lost during immobilization or due to disuse.
- Gait Training: For lower extremity procedures, progressive weight-bearing protocols, balance training, and gait re-education are essential once bone healing permits. Use of assistive devices (crutches, walker) is guided by the surgeon and therapist.
- External Fixator Care: Meticulous pin site care is taught to the patient and family to prevent infection. Education on proper turning of distraction nuts.
- Occupational Therapy (OT): For hand procedures (e.g., polydactyly excision), OT focuses on restoring fine motor skills, grip strength, and dexterity. Splinting for protection and scar management.
- Serial Radiographs: Regular radiographic follow-up is necessary to monitor bone healing, alignment, and regenerate bone quality, particularly during distraction osteogenesis. Adjustments to weight-bearing and therapy are made based on these findings.
- Bracing/Orthotics: Custom orthoses or braces may be required to maintain correction, support joints, or aid in ambulation during the rehabilitation phase and potentially long-term.
Oral Rehabilitation
- Diet Modification: Post-extraction or frenulectomy, a soft diet is typically recommended for a few days to a week to promote healing.
- Oral Hygiene: Emphasize meticulous oral hygiene with soft toothbrushes and appropriate rinses. Patients and families are educated on specific cleaning techniques, especially in areas of prior synechiae or frenulum release.
- Pain Management: Acetaminophen or ibuprofen for discomfort.
- Speech Therapy: If speech impediments are present pre-operatively or persist post-operatively (e.g., after release of alveolar-lip synechiae or cleft palate repair), speech therapy is crucial for articulation and phonation development.
- Regular Dental Follow-up: Long-term follow-up with a pediatric dentist/oral surgeon is essential for managing dental anomalies, monitoring eruption, addressing malocclusion, and preventing caries. Orthodontic intervention may be needed as the child grows.
Multidisciplinary Long-Term Follow-up
Patients with Ellis-Van Creveld syndrome require lifelong, integrated care due to the multisystemic nature of their condition.
*
Orthopedics:
Regular assessment for growth, potential recurrence of deformities, joint health, and late complications.
*
Dentistry/Oral & Maxillofacial Surgery:
Ongoing dental care, orthodontic management, and monitoring for recurrent oral anomalies.
*
Cardiology:
Continued monitoring of cardiac health, especially for those with unrepaired or complex cardiac defects.
*
Genetics:
Ongoing counseling for the family and patient, especially as they approach reproductive age.
*
Physical and Occupational Therapy:
As needed for functional gains, adaptation, and maintenance of mobility.
*
Psychosocial Support:
Essential for patients and families coping with a chronic condition and its impact on daily life.
Summary of Key Literature / Guidelines
Ellis-Van Creveld syndrome, while rare, has been well-documented in the medical literature, with key publications guiding clinical practice. The overarching theme in modern management is a multidisciplinary, patient-centered approach.
Early descriptions by Ellis and Van Creveld laid the foundation for recognizing the clinical triad of chondrodysplasia, ectodermal dysplasia, and polydactyly. Subsequent genetic discoveries identifying mutations in the EVC and EVC2 genes have significantly advanced our understanding of the molecular pathology, providing a basis for genetic counseling and future therapeutic research.
Key Literature Highlights:
- Clinical Characterization: Numerous case series and reviews have detailed the wide spectrum of orthopedic manifestations, including the specific types of polydactyly, long bone shortening, and angular deformities. These studies emphasize the need for early diagnosis and tailored surgical planning.
-
Orthopedic Management:
- Polydactyly: Consensus generally supports early surgical excision of supernumerary digits, particularly if they are well-formed or functionally impairing. Techniques have evolved to focus on functional and cosmetic outcomes, emphasizing careful soft tissue and joint reconstruction.
- Limb Lengthening: Reports on limb lengthening in EVC syndrome, often utilizing external fixators (Ilizarov, monorail systems), demonstrate that significant length gains are achievable, improving ambulation and quality of life. However, these studies also highlight the prolonged treatment duration and high complication rates, underscoring the need for careful patient selection and dedicated rehabilitation.
- Angular Deformities: Guided growth techniques (e.g., hemiepiphysiodesis with 8-plates) have become a less invasive option for correcting genu valgum in growing children, potentially avoiding osteotomies or delaying them until skeletal maturity.
- Hip Dysplasia: Management follows principles for developmental dysplasia of the hip, ranging from bracing in infancy to periacetabular or femoral osteotomies in older children.
- Oral and Dental Management: Dental literature emphasizes the importance of early intervention for natal/neonatal teeth to prevent aspiration and trauma. Management of supernumerary frenula and alveolar-lip synechiae is crucial for feeding, speech, and oral hygiene. Long-term orthodontic and restorative dental care are essential to address hypoplastic enamel and malocclusion.
- Cardiac Management: Seminal pediatric cardiology texts and guidelines consistently stress the high prevalence of ASD and the need for comprehensive pre-operative cardiac evaluation for any surgical procedure in EVC patients. The timing and necessity of ASD repair itself are guided by standard cardiology protocols.
- Multidisciplinary Approach: Reviews uniformly advocate for a coordinated, multidisciplinary team approach involving orthopedics, dentistry, cardiology, genetics, pediatrics, and rehabilitation specialists. This integrated care model is considered the standard for optimizing outcomes and addressing the complex needs of these patients throughout their lives.
Guidelines and Evolving Concepts:
While no specific "EVC syndrome" surgical guidelines exist from major orthopedic societies, management typically follows general principles for osteochondrodysplasias, adapted to the specific anatomical and physiological considerations of EVC.
*
Genetic Counseling:
Increasingly, genetic testing and counseling are integral to diagnosis and family planning, providing critical information regarding recurrence risk.
*
Research Directions:
Ongoing research focuses on understanding the precise role of the
EVC
and
EVC2
genes in Hedgehog signaling and bone development, with potential future avenues for targeted pharmacological interventions to improve growth and bone health.
In conclusion, Ellis-Van Creveld syndrome demands a comprehensive, tailored surgical and medical strategy. Surgeons treating these patients must possess a deep understanding of the syndrome's unique orthopedic and oral pathologies, be prepared for potential systemic complications, and collaborate seamlessly within a multidisciplinary team to achieve the best possible functional and quality-of-life outcomes.
