Orthopedic Cases Achondroplasia: Essential Insights & Management
Patient Presentation & History
A 35-year-old male, known to have achondroplasia, presented to the emergency department following a high-energy mechanism of injury (pedestrian struck by motor vehicle). The patient reported immediate, severe pain in his left distal thigh and knee, with an inability to bear weight. He was an unrestrained pedestrian struck by a vehicle traveling approximately 40 mph, sustaining a direct impact to his left lower extremity. The patient denied loss of consciousness, head injury, or abdominal pain.
His medical history was significant for achondroplasia, diagnosed in infancy. Comorbidities included chronic lumbar spinal stenosis, managed conservatively with physical therapy and NSAIDs, and a history of recurrent otitis media in childhood, resulting in mild conductive hearing loss. He had no prior orthopedic surgeries or significant fractures. He was a non-smoker, rarely consumed alcohol, and was otherwise healthy with no known allergies.
On initial ATLS assessment, the patient was hemodynamically stable. Airway was patent, breathing unlabored, circulation stable. Neurological assessment revealed he was alert and oriented. Priority was then given to focused secondary survey, particularly the injured extremity.
Clinical Examination
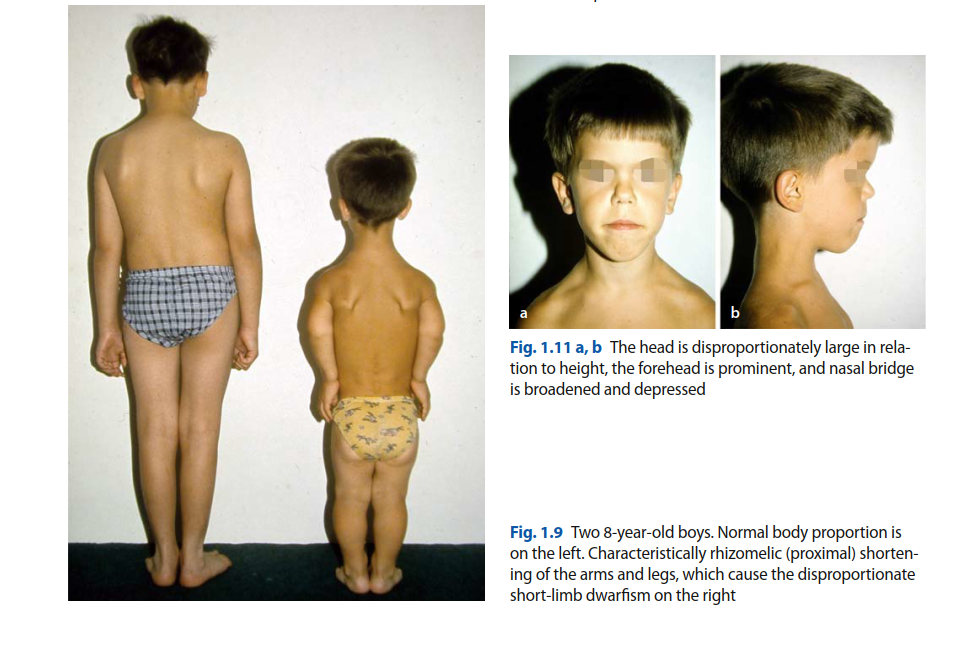
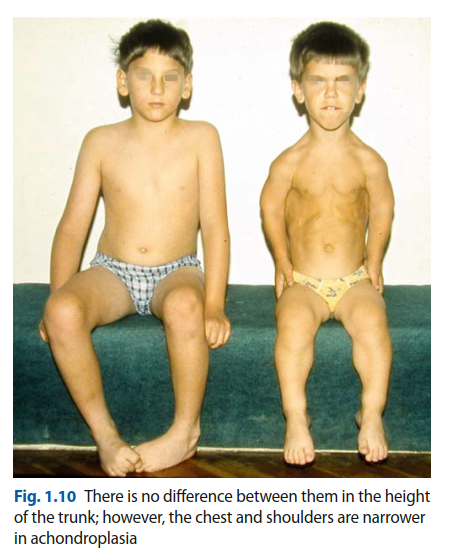
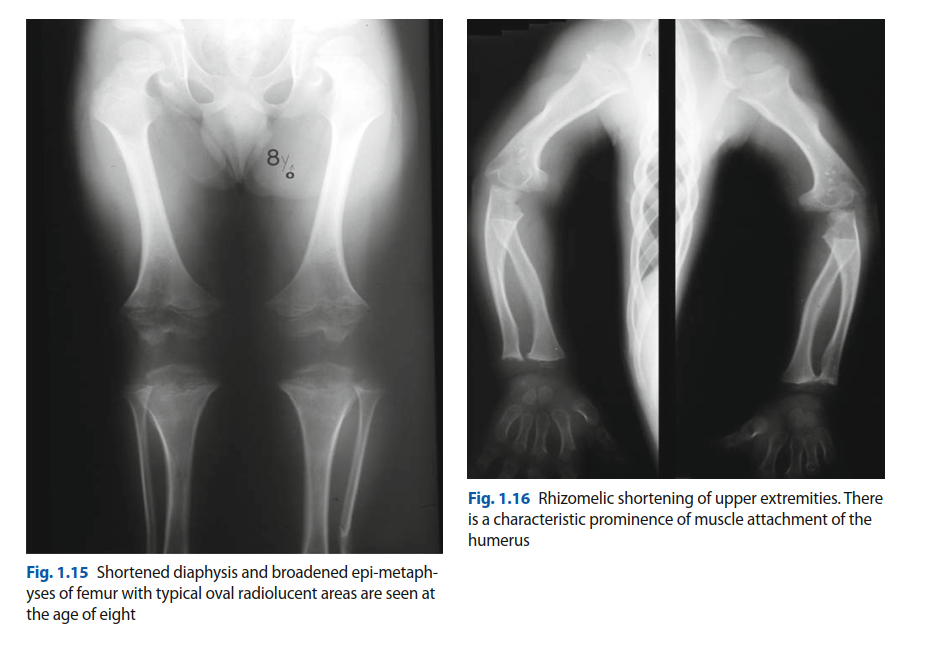
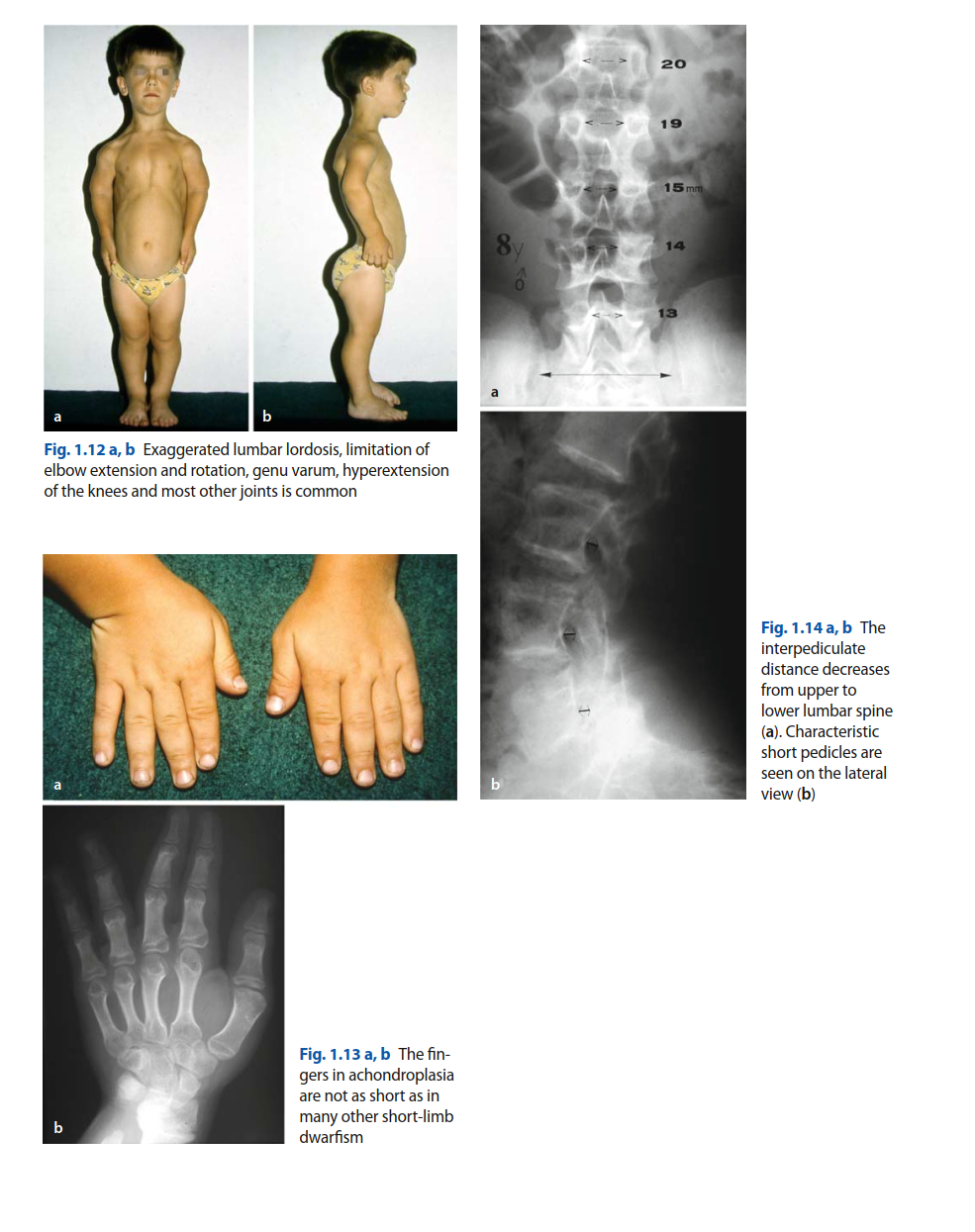
Upon examination, the patient presented with characteristic features of achondroplasia, including short stature (approximately 130 cm), macrocephaly, midface hypoplasia, and rhizomelic limb shortening, particularly pronounced in the femurs and humeri. He exhibited mild thoracolumbar kyphosis and a compensatory lumbar lordosis, which is common in his condition.
The left lower extremity demonstrated a gross varus deformity of the distal thigh and knee, with apparent shortening. There was significant swelling and ecchymosis involving the distal femur and knee joint, making detailed palpation challenging. The skin integrity was intact, with no open wounds or signs of impending soft tissue compromise. Palpation revealed exquisite tenderness over the distal femur, with palpable crepitus indicative of a displaced fracture.
Range of motion of the knee was severely restricted due to pain and mechanical block; any attempt at movement elicited guarding. Pre-injury, the patient had a documented knee flexion of 0-130 degrees and elbow extension deficit of 15 degrees, typical for achondroplasia.
Neurovascular assessment of the left foot and ankle was critical. Dorsalis pedis and posterior tibial pulses were palpable and strong, with brisk capillary refill in the toes. Sensory examination revealed intact sensation to light touch in the superficial peroneal, deep peroneal, saphenous, and sural nerve distributions. Motor function of the ankle and toes was intact, though voluntary movement was limited by pain. No signs of compartment syndrome were present acutely. The opposite extremity examination was unremarkable.
Imaging & Diagnostics
Initial radiographs of the left femur and knee were obtained in the emergency department.
These views confirmed a complex, comminuted intra-articular distal femoral fracture. Specifically, the images demonstrated a highly displaced, multifragmentary fracture of both femoral condyles extending into the metaphysis. The fracture pattern was consistent with a Müller AO/OTA 33-C3 injury, indicating a complete articular fracture with severe comminution. Significant coronal and sagittal plane displacement of the condylar fragments was noted. The overall limb alignment was disrupted, with varus angulation and shortening.
Further advanced imaging, including a computed tomography (CT) scan of the left femur and knee, was immediately performed to delineate the articular involvement, assess comminution, and aid in pre-operative planning.
The CT scan confirmed the 33-C3 classification, revealing multiple articular fragments involving both medial and lateral femoral condyles, with extension into the intercondylar notch. A significant metaphyseal void was identified secondary to the comminution. Three-dimensional (3D) reconstructions were invaluable for understanding the complex fracture geometry and planning the surgical approach and reduction strategy.
The CT scan also highlighted specific anatomical challenges inherent to achondroplasia:
*
Short, bowed femur:
The overall length of the femur was significantly reduced, and there was a subtle anterior bowing, which would impact plate contouring and length selection.
*
Metaphyseal flaring:
While achondroplastic bones are generally shorter, the metaphyseal area often demonstrates prominent flaring, while the diaphyseal canal can be relatively narrow.
*
Narrow intramedullary canal:
The CT confirmed a significantly narrower intramedullary canal compared to an average-statured individual, making intramedullary nailing a potentially difficult or unsuitable option without reaming.
Pre-operative templating was performed meticulously using calibrated radiographs and CT reconstructions. Given the altered bone morphology, standard adult-sized implants were unlikely to be appropriate. We specifically templated for shorter lateral distal femoral locking plates and considered smaller diameter screws if cortical thickness proved insufficient for standard-sized hardware. The anticipated screw lengths for distal and proximal fixation were carefully estimated.
Laboratory investigations were unremarkable, including a complete blood count, basic metabolic panel, coagulation profile, and type and crossmatch.
Differential Diagnosis
While the diagnosis of a distal femur fracture in this high-energy trauma setting was straightforward, considering potential alternative traumatic injuries around the knee is prudent in any polytrauma patient. The unique anatomical context of achondroplasia also influences how these injuries might present or be managed.
| Feature | Distal Femur Fracture (AO/OTA 33-C3) in Achondroplasia | Proximal Tibia Fracture (AO/OTA 41-C) | Knee Dislocation (Multiligamentous Injury) | Patellar Fracture / Extensor Mechanism Rupture |
|---|---|---|---|---|
| Pain Location | Distal thigh, knee joint. | Proximal tibia, knee joint. | Diffuse knee pain, often instability. | Anterior knee pain, supra/infrapatellar. |
| Deformity | Gross deformity of distal thigh/knee, shortening, rotational component. | Gross deformity of proximal leg/knee, shortening, varus/valgus, often open. | Marked instability, potential gross deformity; often spontaneously reduced. | Palpable defect (rupture), inability to extend knee (fracture with displacement). |
| Swelling | Significant hemarthrosis, soft tissue swelling around distal femur. | Significant hemarthrosis, soft tissue swelling around proximal tibia. | Rapid, significant hemarthrosis, may mask underlying vascular/nerve injury. | Localized swelling, ecchymosis over patella. |
| Mechanism | High-energy axial load with valgus/varus/rotational component; direct impact. | High-energy axial load with valgus/varus/rotational component; direct impact. | High-energy rotational or hyperextension/hyperflexion force. | Direct impact to patella, forceful quadriceps contraction against resistance. |
| Palpable Instability | Often present at fracture site; knee joint may be stable unless articular fracture extends. | Often present at fracture site; knee joint may be stable unless articular fracture extends. | Marked laxity in multiple planes (AP, varus/valgus, rotation) on stress examination. | Patellar mobility compromised; abnormal high-riding patella (quads rupture). |
| Imaging Findings | Fracture lines involving femoral condyles/metaphysis. Displacement, comminution. | Fracture lines involving tibial plateau/metaphysis. Displacement, comminution. | Normal bone alignment (post-reduction). Avulsion fractures may be present; MRI shows ligament injury. | Fracture lines in patella; avulsion from tibia/quadriceps on X-ray. |
| Vascular Injury Risk | Moderate (popliteal artery injury possible with severe displacement). | Moderate (popliteal artery injury possible with severe displacement). | High (popliteal artery injury in 30-50% of cases, even with spontaneous reduction). | Low. |
| Neurological Injury Risk | Moderate (peroneal nerve, less common than tibial plateau). | Moderate (peroneal nerve is highly vulnerable). | High (peroneal nerve is most commonly injured). | Low. |
| Achondroplasia Considerations | Short, thick bones, bowed femurs, narrow IM canal, specific hardware challenges. | Short, thick bones, bowed tibias, specific hardware challenges. | Ligamentous laxity can be a pre-existing factor; altered biomechanics. | Patellar tracking issues common; altered lever arm. |
Surgical Decision Making & Classification
The patient's distal femoral fracture was classified as a Müller AO/OTA 33-C3, denoting a complete articular fracture that is multifragmentary. This classification signifies severe articular involvement and comminution, requiring meticulous anatomical reduction and stable internal fixation to restore joint congruity and knee function.
Indications for Surgical Intervention:
1.
Displaced Intra-articular Fracture:
The severe displacement of the articular fragments necessitated operative intervention to restore joint surface congruity and prevent early post-traumatic arthritis.
2.
Unstable Fracture:
The high-energy mechanism and multifragmentary nature rendered the fracture inherently unstable, precluding non-operative management.
3.
Potential for Malunion/Nonunion:
Without stable fixation, the risk of malunion with resulting limb deformity and functional impairment, or nonunion, would be unacceptably high.
4.
Patient Factors:
The patient's relatively young age and desire for optimal functional recovery favored aggressive surgical management.
Challenges Unique to Achondroplasia in Surgical Planning:
*
Anatomical Aberrations:
*
Short Limb Length:
The significantly shorter femur limits the available diaphyseal segment for plate fixation and impacts overall limb length restoration strategies.
*
Bowing Deformities:
The characteristic anterior and sometimes varus/valgus bowing of the femur necessitates careful plate contouring or selection of pre-contoured plates that can accommodate this morphology.
*
Narrow Intramedullary Canal:
Standard intramedullary nails are often too large for the narrow diaphyseal canal of achondroplastic long bones, ruling out IM nailing as a primary option for distal femur fractures without extensive reaming. Plate fixation is generally preferred for distal femur fractures in achondroplasia.
*
Metaphyseal Flaring:
While the metaphysis can be wide, the specific geometry may make standard plate application challenging, requiring precise positioning to ensure adequate screw purchase.
*
Bone Quality:
While cortices can be thick, the overall bone architecture and mechanical properties can vary, requiring attention to screw purchase and fixation strength.
*
Hardware Selection:
Standard adult implants are often too long or too wide. Meticulous pre-operative templating with attention to implant length, width, and screw trajectory is crucial. Pediatric-sized implants or custom plates might be considered in specific circumstances, though off-the-shelf distal femoral locking plates can often be utilized if length is adequate.
*
Patient Positioning:
The patient's short stature, macrocephaly, and pre-existing thoracolumbar kyphosis/lordosis associated with spinal stenosis require special attention during positioning on the operating table to prevent iatrogenic neural compromise, airway issues, or pressure injuries. A vacuum beanbag or specialized pediatric positioning aids might be necessary.
*
Anesthesia Considerations:
The presence of spinal stenosis (both foramen magnum and lumbar) raises concerns regarding neuraxial anesthesia (epidural/spinal) and necessitates careful airway management planning with the anesthesiology team due to potential for difficult intubation.
Pre-operative Planning:
Our planning involved:
1.
Detailed Review of Imaging:
Scrutiny of CT scans with 3D reconstructions to fully grasp the fracture configuration, identify key articular fragments, and determine the optimal sequence of reduction.
2.
Templating:
Precise templating on radiographs and CT images using digital planning software. This guided the selection of a specific lateral distal femoral locking plate system (e.g., LISS or NCB plates) and helped estimate the appropriate length of the plate and individual screws. We ensured the plate length would allow for adequate bicortical fixation in the diaphyseal segment.
3.
Surgical Approach:
Planned a standard extensile lateral approach (e.g., modified Swashbuckler or a long lateral parapatellar approach) to allow for direct visualization and reduction of the articular surface.
4.
Anesthesia Consultation:
Discussed the patient's spinal history and airway with the anesthesia team to formulate a safe anesthetic plan.
Surgical Technique / Intervention
The patient was transferred to the operating room, and under general endotracheal anesthesia, positioned supine on a radiolucent table. Special care was taken to support the patient's head in neutral alignment with a donut pillow to mitigate any potential spinal cord compromise from the known foramen magnum stenosis. A small bump was placed under the ipsilateral hip to facilitate the lateral approach and allow free access for intraoperative fluoroscopy in both AP and lateral planes. The limb was draped free.
Surgical Approach:
A standard extensile lateral approach to the distal femur was utilized. A longitudinal incision was made, centered over the distal femur, extending from approximately 10 cm proximal to the joint line distally to the lateral epicondyle. The fascia lata was incised, and a subvastus approach was employed to expose the lateral aspect of the distal femur. If visualization of the articular surface proved inadequate, a limited arthrotomy via a lateral parapatellar approach would have been considered, but direct visualization through the fracture fragments proved sufficient initially.
Reduction Techniques:
1.
Articular Reduction First:
The paramount step for a 33-C3 fracture. The goal was to meticulously reconstruct the articular surface of the femoral condyles. Using small pointed reduction clamps, bone hooks, and k-wires, the displaced articular fragments were anatomically reduced under direct visualization and fluoroscopic guidance. This involved careful manipulation of the condylar fragments to restore the trochlear groove and intercondylar notch.
2.
Temporary Fixation:
Once anatomical articular reduction was achieved, it was maintained with multiple K-wires placed in non-obstructing positions to avoid future screw paths. Small, fully threaded cancellous screws were then placed across the articular fragments for stable interfragmentary compression.
3.
Restoration of Length, Alignment, and Rotation (LAR):
With the articular block reconstructed, attention shifted to reducing this block to the femoral metaphysis and diaphysis. Gross length was restored by applying gentle longitudinal traction. Varus/valgus and rotational alignment were assessed clinically and confirmed fluoroscopically. Provisional reduction was held with large pointed reduction clamps spanning the articular block to the femoral shaft, followed by additional K-wires. The pre-existing subtle femoral bowing was accounted for during alignment restoration.
Fixation Construct:
A pre-contoured lateral distal femoral locking plate (e.g., LCP Distal Femoral Plate System) was selected based on our templating, opting for a shorter length than typically used in an average-statured adult to accommodate the patient's limb length.
1.
Plate Application:
The plate was meticulously positioned on the lateral aspect of the distal femur, ensuring it was centered and parallel to the mechanical axis of the femur. Fluoroscopy was used to confirm optimal plate placement relative to the articular surface distally and the femoral shaft proximally.
2.
Distal Fixation:
Multiple variable-angle locking screws were inserted into the femoral condyles through the plate, ensuring appropriate length and trajectory to achieve strong purchase within the articular block without violating the knee joint or contra-cortical penetration. The locking nature of the screws provided angular stability, crucial in comminuted metaphyseal zones.
3.
Proximal Fixation:
The diaphyseal segment was fixed with a minimum of four bicortical locking screws, achieving an adequate working length to provide robust fixation to the femoral shaft. Care was taken to ensure the screws obtained good purchase in the thick achondroplastic cortices.
4.
Bone Grafting:
Given the significant metaphyseal comminution and potential for defects, structural allograft chips were gently packed into any remaining metaphyseal voids to promote bone healing.
Final Assessment:
Prior to wound closure, final fluoroscopic images were taken in AP, lateral, and oblique views to confirm anatomical reduction of the articular surface, appropriate alignment of the limb, and satisfactory hardware placement.
The knee joint was put through a full range of motion to ensure no mechanical impingement of hardware and to assess knee stability. The tourniquet was deflated, and hemostasis was achieved.
Wound Closure:
The surgical site was copiously irrigated. The vastus lateralis and fascia lata were closed in layers using absorbable sutures. The subcutaneous tissue and skin were closed in a standard fashion. A sterile dressing was applied, and a long-leg knee brace was placed with the knee in 20 degrees of flexion for initial protection.
Post-Operative Protocol & Rehabilitation
The post-operative protocol was designed to balance fracture stability with early, protected range of motion, taking into account the unique biomechanics and potential challenges in an achondroplastic patient.
Initial Phase (Days 0-6 Weeks)
- Weight Bearing: Strict non-weight bearing (NWB) on the operative left lower extremity for the first 6-8 weeks. This was crucial for articular healing and metaphyseal bone consolidation given the complexity of the fracture.
- Immobilization: A hinged knee brace was maintained, locked from 0 to 30 degrees of flexion for the first 2 weeks, protecting against varus/valgus stress.
- Pain Management: Multimodal approach including scheduled NSAIDs (if no contraindications), acetaminophen, and opioid analgesics as needed, with a strong emphasis on opioid-sparing strategies.
- DVT Prophylaxis: Standard chemical prophylaxis (e.g., subcutaneous enoxaparin) was initiated on post-operative day 1 and continued for 6 weeks, combined with mechanical prophylaxis (SCDs).
-
Physical Therapy (PT) & Occupational Therapy (OT):
- CPM Machine: Initiated on post-operative day 1, with a gradual increase in range of motion (ROM) as tolerated, progressing from 0-30 degrees to 0-90 degrees by week 6, as comfort allowed.
- Isometric Exercises: Quadriceps sets, gluteal sets, and ankle pumps to maintain muscle tone and promote circulation.
- Patellar Mobilizations: Gentle patellar glides to prevent stiffness.
- Upper Extremity Strengthening: To prepare for crutch ambulation.
- Transfer Training: Training for safe transfers without weight bearing on the affected limb.
- Wound Care: Daily dressing changes and monitoring for signs of infection. Sutures were removed at 2 weeks post-op.
Intermediate Phase (Weeks 6-12)
- Radiographic Assessment: Follow-up radiographs at 6 weeks were performed to assess early signs of fracture healing (callus formation, bridging bone).
-
Weight Bearing Progression:
- If radiographic healing was adequate and pain was minimal, progression to touch-down weight bearing (TDWB) (approximately 10-15 kg) was initiated, using crutches.
- Gradual progression to partial weight bearing (PWB) as tolerated, guided by clinical pain and further radiographic evidence of healing.
- Immobilization: The knee brace ROM was gradually increased, aiming for functional ROM (e.g., 0-110 degrees) by week 12. The brace could be unlocked for exercises and removed for showering.
-
Physical Therapy:
- Progressive ROM: Continued emphasis on regaining full knee flexion and extension.
- Strengthening: Introduction of closed kinetic chain exercises (e.g., mini-squats, leg presses against light resistance), hamstring curls, hip abduction/adduction exercises.
- Proprioception and Balance Training: Single-leg stance (NWB initially, then PWB) on stable surfaces.
- Gait Training: Focus on normal gait pattern with assistive devices.
- Achondroplasia Specific Considerations: Given the patient's pre-existing limited joint ROM (e.g., elbow extension deficit), it was emphasized that achieving pre-injury knee ROM was the primary goal, rather than aiming for supra-physiological ranges. Close monitoring for exacerbation of lumbar spinal stenosis symptoms during exercise was also crucial.
Advanced Phase (Weeks 12-24 and Beyond)
- Radiographic Assessment: Further radiographs at 12 and 16 weeks to confirm consolidation.
- Weight Bearing: Progression to full weight bearing (FWB) without assistive devices, as tolerated and confirmed by solid radiographic union.
-
Physical Therapy:
- Advanced Strengthening: Progressive resistance exercises, plyometrics (if appropriate), agility drills.
- Functional Training: Return to activities of daily living (ADLs), work-specific tasks, and recreational activities.
- Cardiovascular Conditioning: Cycling, swimming (non-impact activities).
- Long-term Follow-up: Regular clinical and radiographic follow-up for 1-2 years to monitor for hardware complications, malunion, nonunion, and the development of post-traumatic arthritis. Consideration for hardware removal after 18-24 months if symptoms warrant and fracture is fully healed.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Pre-operative Planning is Paramount: For any complex fracture, but especially in achondroplasia, detailed pre-operative planning with CT/3D reconstructions is non-negotiable. It allows for accurate fracture mapping, identification of key fragments, and an informed surgical strategy.
- Templating is ESSENTIAL: Do not assume standard adult implants will fit. Achondroplastic long bones have unique dimensions (shorter length, narrow intramedullary canals, specific bowing patterns, altered metaphyseal flare). Meticulous templating for plate length, width, and screw lengths is critical to prevent implant mismatch and ensure adequate fixation. Consider pediatric-sized implants if necessary.
- Prioritize Articular Reduction: For intra-articular fractures (AO/OTA 33-C3), anatomical reduction of the joint surface is the primary goal to minimize the risk of post-traumatic arthritis. Use direct visualization, small fragments clamps, and temporary K-wires.
- Robust Fixation: Utilize a stable, angularly-stable construct, such as a lateral locking plate, which is biomechanically well-suited for distal femur fractures and can compensate for potentially weaker bone stock or short fixation segments. Ensure adequate working length and strong bicortical purchase.
- Patient Positioning Awareness: Be acutely aware of the patient's underlying achondroplastic features, particularly potential foramen magnum stenosis or lumbar spinal stenosis. Meticulous positioning, cervical spine precautions, and adequate padding are crucial to prevent iatrogenic nerve injury or pressure sores. Discuss with anesthesia regarding airway and neuraxial anesthesia considerations.
- Early, Controlled Range of Motion: While maintaining protection for fracture healing, initiation of early, controlled ROM exercises is vital to prevent stiffness, especially in joints already prone to some degree of stiffness or contracture in achondroplasia.
- Multimodal Pain Management: Implement a comprehensive pain management strategy to facilitate early mobilization and minimize opioid reliance.
Pitfalls
- Underestimating Anatomical Variations: Failure to appreciate the distinct bone morphology (short, bowed, narrow IM canal) of achondroplasia can lead to incorrect implant selection, malpositioning, and ultimately, suboptimal fixation or intraoperative complications.
- Inadequate Templating: Attempting to use standard adult implants without proper pre-operative templating can result in plates that are too long (causing impingement or needing excessive bending), too wide, or screws that are too long/short, leading to joint penetration, poor purchase, or soft tissue irritation.
- Compromising Articular Reduction: Accepting a suboptimal articular reduction in a complex intra-articular fracture significantly increases the risk of early post-traumatic arthritis and long-term functional impairment.
- Insufficient Fixation: Inadequate number of screws, poor screw purchase, or choosing an unstable construct can lead to hardware failure, loss of reduction, and nonunion, especially in comminuted fractures or potentially compromised bone quality.
- Neglecting Systemic Comorbidities: Ignoring the potential impact of spinal stenosis, airway challenges, or other systemic issues associated with achondroplasia during surgical planning and execution can lead to severe perioperative complications.
- Aggressive or Overly Conservative Rehabilitation: Pushing rehabilitation too aggressively without radiographic evidence of healing can risk hardware failure or loss of reduction. Conversely, being overly cautious can lead to significant joint stiffness and prolonged recovery. Tailor the protocol to individual fracture healing.
- Failure to Detect Associated Injuries: In high-energy trauma, always consider associated ligamentous injuries, especially in the knee, or potential neurovascular compromise, even if initially masked by obvious fracture. A thorough post-reduction clinical and imaging assessment is crucial.
