Orthopedic Board Review MCQs: Adult Reconstruction & Trauma - Part 98
Key Takeaway
This page offers Part 98 of a comprehensive orthopedic board review. It's an interactive MCQ set designed for orthopedic surgeons and residents preparing for OITE/ABOS/AAOS certification. Featuring 100 high-yield, verified questions covering Arthroplasty, Fracture, Hip, Knee, it provides essential exam preparation in both study and exam modes.
About This Board Review Set
This is Part 98 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 98
This module focuses heavily on: Arthroplasty, Fracture, Hip, Knee.
Sample Questions from This Set
Sample Question 1: Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?...
Sample Question 2: -An 8-1/2-month-old male infant who has developmental dysplasia of the hip was treated in a Pavlick harness for 3 months. At follow-up, examination of the hip reveals full flexion and extension and abduction to 80 degrees. Figure 41a shows ...
Sample Question 3: Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?...
Sample Question 4: -What do the bone scan findings represent?...
Sample Question 5: Treatment should now include...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?

Explanation
internal fixation in the acute phase (6 to 8 hours) or sub-acute phase (2 to 3 days) is difficult.
Question 2
- An 8-1/2-month-old male infant who has developmental dysplasia of the hip was treated in a Pavlick harness for 3 months. At follow-up, examination of the hip reveals full flexion and extension and abduction to 80 degrees. Figure 41a shows an AP arthrogram and Figure 41b an arthrographic view in flexion and abduction. Management should now consist of
Explanation
Question 3
Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293.
McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.
Kumar PJ, McPherson EJ, Dorr LD, et al: Rehabilitation after total knee arthroplasty: A comparison of 2 rehabilitation techniques. Clin Orthop 1996;331:93-101.
Question 4
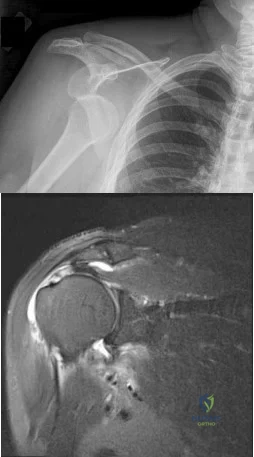
-What do the bone scan findings represent?
Explanation
The bone scan shows no uptake of the tracer, which indicates osteonecrosis. The MRI scan of the shoulder reveals sepsis with a focus on osteomyelitis. A CT scan will not add more useful information and will delay treatment. A sequestrum is a piece of dead bone that has become separated from normal/solid bone during the osteonecrosis process. It appears as a radiopacity on plain radiograph. The involucrum is new bone formed by an elevated periosteum and can be seen on radiograph.
Heterotopic ossification appears as radiopacity within the soft tissues. Late recognition of pediatric shoulder sepsis has been reported, and damage to the joint can be extensive. Septic joints are one of the few true orthopaedic emergencies. The methodology of drainage in shoulder sepsis is controversial (aspiration vs open drainage vs arthroscopic lavage), but the joint must be drained and sterilized to prevent cartilage damage.
Question 5
Treatment should now include
Explanation
Extensive laminectomy in patients with degenerative spondylolisthesis does result in postoperative instability. In the study by White and Wiltse, further subluxation did occur in 66 percent of patients who were operated on for degenerative spondylolisthesis , whereas it was observed in only 2 percent of the spondylolisthesis or disc patients who did not have
spondylolisthesis postoperatively. The extent of decompression and facet removal must be limited in the patient with degenerative spondylolisthesis or a fusion of the transverse processes included as part of the treatment. Internal fixation devices have been used in these circumstances to prevent further subluxation while the fusion is consolidating. Wiltse outlined some guidelines for spinal fusion in spinal stenosis: (1) the patient who is less than sixty years old and had degenerative spondylolisthesis with a total loss of posterior stability due to removal of the articular processes (a one-level fusion of the transverse processes); (2) the patient who is less than fifty-five and had a midline decompression for degenerative spondylolisthesis with facet preservation; and
(3) the patient who is less than fifty years old with isthmic spondylolisthesis, if the posterior elements have been removed. Simple degenerative spinal stenosis seldom requires a fusion, even if all posterior stability has been lost. The problem with obtaining a successful spinal fusion is real and conditions are less than optimum in these instances.
Question 6
Which of the following postoperative rehabilitation techniques causes minimal rotator cuff muscle activation? Review Topic
Explanation
Question 7
Figure 56 is the MR image of a 20-year-old Division I baseball pitcher who has a 1-month history of medial elbow pain in his throwing arm. He also notes a decrease in both control and pitching velocity. An examination reveals tenderness at the medial epicondyle that is exacerbated with valgus elbow stress. The strongest indication for ulnar collateral ligament (UCL) reconstruction is
Explanation
All responses represent findings that may be associated with chronic UCL insufficiency. Responses 1 and 3 reflect injury to the UCL itself. In most patients, particularly young patients, UCL reconstruction should not be considered until an appropriate trial of nonsurgical measures has failed. This trial should include, at a minimum, 6 weeks of throwing abstinence followed by rehabilitation to address pitching mechanics and shoulder motion deficits and core strengthening. Although the decision to enter the MLB draft may influence surgical decision making, a pitcher with a 1-month history of elbow symptoms should attempt nonsurgical therapy before making a surgical decision that is not based on clinical data.
Question 8
A 56-year-old male presents to your office with a primary complaint of pain in his lower back that extends down his left leg when he walks. He states he rides a stationary bike without pain, but he has severe pain walking more than two blocks. On exam he has 5/5 strength in all major muscle groups, and his sensation is intact to light touch in all dermatomes. He has no upper motor neuron signs. The pain has been going on for about a year, and he has had no improvement with physical therapy or anti-inflammatory medication. Figure A is an upright lateral radiograph of his lumbar spine. Figures B is his sagittal MRI, and Figure C is an axial image through L4/5. Assuming this patient is going to undergo surgery, what is most important in ensuring longterm symptomatic relief? Review Topic

Explanation
Degenerative spondylolisthesis occurs when there is anterior translation of one vertebral body (most commonly L4) on another vertebral body (most commonly L5). When this occurs, there can be compression of the traversing/caudal (L5) nerve root in the lateral recess. Because of the instability associated with this diagnosis, a fusion is needed to preserve longterm outcomes.
Kornblum et al., reported on the outcomes of 47 patients with degenerative spondylolisthesis at an average follow-up of 7 years and 8 months. Excellent to good results were reported in 86% of patients with a solid arthrodesis compared to 56% of patients with a pseudarthrosis.
Weinstein et al., reported the 4-year data from the SPORT study and found that patients with degenerative spondylolisthesis treated with surgery had statistically significant improvements in health related quality of life scores compared to those treated non-operatively.
Figure A is an upright lateral radiograph of the lumbar spine in which a degenerative spondylolisthesis of L4 on L5 is identified. Figure B is a sagittal T2 MRI re-demonstrating the spondylolisthesis as well as spinal stenosis. FIgure C is the axial image through L4/5 demonstrating spinal stenosis; additionally, a left sided facet cyst can be seen.
Illustration A and B are the postoperative films from the same patient after he underwent an L4/5 posterior decompression and instrumented fusion.
Incorrect
(SBQ13PE.7) A 45-year-old HIV-positive homeless man presents with increasing low back pain for the last three weeks. He now reports difficulty ambulating, fever, and loss of appetite. He denies bowel and bladder symptoms. He denies any symptoms radiating into his buttock or legs. On physical exam he has in obvious discomfort with standing which worsens in the forward flexion position. He has a normal motor and sensory exam in his lower extremities. Blood cultures are performed which come back negative. What would be the most next appropriate step in treatment? Review Topic

Broad spectrum antibiotics
Isoniazid, rifampin, and pyrazinamide therapy
CT guided biopsy with cultures
Technetium bone scan
Anterior corpectomy with a retroperitoneal approach, strut grafting and instrumentation
The clinical presentation is consistent with spondylodiscitis. Although the patient has risk factors for spinal tuberculosis, a CT guided biopsy should be performed to establish a diagnosis.
There is an increasing incidence of TB in United States due to increasing immunocompromised population from HIV. 15% of patients with TB will have extrapulmonary involvement. 5% of all TB patients have spine involvement. With any type of spondylodiscitis the infectious organism must be identified with blood cultures or a biopsy prior to initiating treatment.
Khoo et al. emphasize with the recent global pandemic of human immunodeficiency virus, the number of tuberculosis and secondary spondylitis cases is again increasing at an alarming rate. They report that medical treatment alone remains the cornerstone of therapy for the majority of Pott disease cases. Surgical intervention should be limited primarily to cases of severe or progressive deformity and/or neurological deficit.
Hadjipavlou et al. performed a retrospective study of 101 cases of spondylodiscitis. They found Staphylococcus aureus was the main organism. Infection elsewhere was the most common predisposing factor. Leukocyte counts were elevated in 42.6% of spondylodiscitis cases. The erythrocyte sedimentation rate was elevated in all cases of epidural abscess.
Figure A shows lumbar radiograph with a radiolucent lesion in L2 with mild loss of disc height of the L2/3 level. Figure B shows a T2-weighted MRI showing a lesion involving the L2/3 disc spaced and extending into the L2 vertebral body.
Incorrect Answers:
Question 9
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
Explanation
8 • American Academy of Orthopaedic Surgeons
DISCUSSION: Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
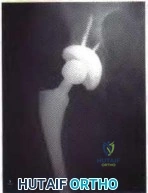
Figure 3a Figure 3b
Question 10
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Explanation
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 11
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991,
pp 1712-1718.
Question 12
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis? Review Topic

Explanation
Question 13
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
Question 14
A 62-year-old man complains of shoulder pain for 2 years. He has had 1 course of intra-articular sodium hyaluronate and 6 weeks of physical therapy with little relief. Examination reveals diminished arm flexion and abduction secondary to pain. Radiographs of his shoulder are shown in Figures A and B. According to the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines, what is the next best step? Review Topic

Explanation
TSA is indicated for cases of end-stage GH OA. It is preferred to hemiarthroplasty. It is contraindicated in cases with insufficient glenoid bone stock (glenoid wear to the level of the coracoid), rotator cuff arthropathy or irreparable cuff tears and deltoid dysfunction. It provides good pain relief and has good survival at 10 years (>90%).
Radnay et al. performed a systematic review involving 1952 patients comparing TSA with humeral head replacement (HHR). They found that TSR provided greater pain relief, range of motion, patient satisfaction, and had lower revision rates. They recommend TSA over HHR for GH OA.
Izquierdo et al. described the AAOS Clinical Practice Guidelines (CPG) regarding treatment of GH OA. This is summarized in Illustration A.
Figures A and B show end-stage GH OA with large osteophytes and subchondral sclerosis. There is significant glenoid wear and posterior subluxation (Walch B glenoid deformity). Illustration A is a table summarizing the AAOS CPG on treatment of GH OA. Illustration B shows a CTA humeral component. It is not paired with a glenoid component.
Incorrect Answers:
Question 15
-The Coleman block test is used to test for
Explanation

Question 16
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 17
Which of the following antibiotics is contraindicated in children?
Explanation
REFERENCE: Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 18
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 19
An 8-year-old girl has had a painless enlarging mass of insidious onset in the left thigh for the past 3 weeks. Her mother denies any history of trauma, fever, or disease. Examination reveals a nontender, mobile mass in the left medial thigh. Her gait is normal. Figures 25a through 25d show the frog-lateral radiograph, the axial and coronal T1-weighted MRI scans, and the axial T2-weighted MRI scan. Biopsy results reveal a nonrhabdomyosarcoma soft-tissue sarcoma. The most appropriate treatment should consist of
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, p 757.
Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 605.
Question 20
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament.
REFERENCES: Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 21
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results? Review Topic

Explanation
Question 22
A 63-year-old male, with history of myocardial infarction, presents with buttock and leg pain. He states the pain is worse when climbing stairs, and is absent when walking down a hill. He reports when walking on a flat surface the pain begins after roughly 50 meters, but if he stops walking and remains standing upright, the pain resolves after a few minutes. He denies any leg pain when sitting and driving a car. These symptoms are most consistent with: Review Topic
Explanation
Vascular claudication refers to the pain, aching or fatigue of the muscles of the buttocks, thigh and/or calf that occurs with exertion, and is related to a failure to meet muscular oxygen requirements, usually caused by peripheral vascular disease impeding blood flow to the peripheral muscles.
Neurogenic claudication is the classic symptom caused by lumbar spinal stenosis. Neurogenic claudication classically presents with bilateral buttock pain with upright activities, but seems to improve by postural changes that flex the lumbar spine. These posture changes are thought to increase the cross sectional area of the central canal, which relieves pressure on the affected area.
Issack et al. reviewed degenerative lumbar spinal stenosis. They state that patients with vascular claudication will have similar symptoms of leg cramping, whether ambulating or riding a stationary bicycle. In comparison, patients with neurogenic
claudication have diminished symptoms of claudication while positioned seated.
Young et al. reviewed the use of lumbar epidural/transforaminal steroids for managing spinal disease. They report that two thirds of acute low back pain episodes resolve within 7 weeks, so the utility and practice patterns regarding the timing and number of epidural/transforaminal steroid injections is usually based on expert opinion, rather than high level research evidence.
Illustration A shows an angiogram of a patients with normal (left) vs abnormal (right) arterial vasculature. Illustration B shows the typical MRI of a patient with spinal stenosis.
Incorrect
Question 23
A 41-year-old woman has medial-sided knee pain and varus deformity. Her radiographic findings are consistent with isolated medial compartment osteoarthritis. Her pain persists despite nonsurgical therapy. A medial-sided, opening-wedge osteotomy with locking plate fixation is performed. What factor is most associated with delayed union or nonunion of the osteotomy?
Explanation
Many factors can lead to delayed union or nonunion after medial opening-wedge high tibial osteotomy; the factor most associated with delayed union or nonunion is smoking. Other factors include obesity and unstable lateral hinge fractures, but to a lesser extent. An accelerated weight-bearing protocol has no effect on union. The use of locking screws should increase construct stability and is not associated with osteotomy delayed union or nonunion.

Question 24
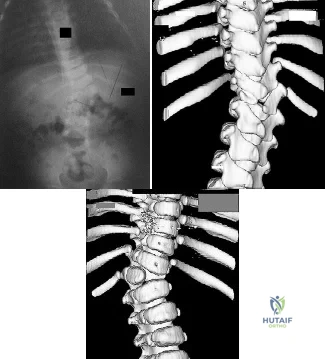
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35°. Neurologic examination is normal. Management should consist of
Explanation
REFERENCES: Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767.
Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Farley FA, Song KM, Birch JG, Browne R: Syringomyelia and scoliosis in children. J Pediatr Orthop 1995;15:187-192.
Question 25
When performing a radioscapholunate (RSL) fusion for posttraumatic radiocarpal arthritis, excision of the distal pole of the scaphoid will cause a decrease in
Explanation
RSL arthrodesis is a motion-sparing option for posttraumatic radioscaphoid or radiolunate arthritis when the midcarpal joint is preserved. Preserving the midcarpal joint allows the dart-thrower motion to remain. Mühldorfer-Fodor and associates reported that the rates of nonunion for RSL fusion were reduced by excision of the distal pole of the scaphoid. Multiple studies have shown increased radial and ulnar deviation with excision of the distal pole of the scaphoid; excision of the triquetrum further increases the radial-ulnar arc of motion. Bain and associates and Pervaiz and associates reported increased wrist
flexion-extension arcs with distal scaphoid and triquetrum excisions in cadaveric models; other authors have reported no difference.
Question 26
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?
Explanation
REFERENCES: Robinson CM, Aderinto J: Posterior shoulder dislocations and
fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.
Question 27
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include
Explanation
REFERENCES: Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
LeGay D, Petrie DP, Alexander DI: Flexion-distraction injuries of the lumbar spine and associated abdominal trauma. J Trauma 1990;30:436-444.
Question 28
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
Explanation
Question 29
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 30
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete? Review Topic
Explanation
Question 31
A 19-year-old football player is taken off the field because of fatigue. Examination reveals a rash shown in Figure A. Oral examination reveals findings shown in Figure B. Posterior cervical glands are palpable. A mass is palpable in the left upper quadrant. Which of the following is true regarding the most likely diagnosis? Review Topic
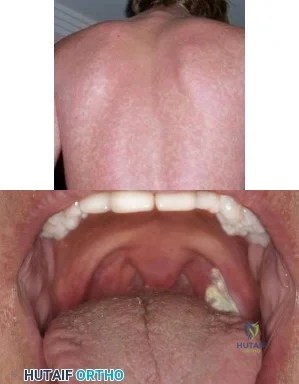
Explanation
IM is caused by the Epstein-Barr virus (EBV). Annual incidence is 1-3% in college freshmen. It is characterized by Hoagland's triad (fever, pharyngitis, lymphadenopathy). Some have rash and splenomegaly. Splenic rupture is rare (0.1-0.2% of patients). It is caused by sudden increase in portal venous pressure from a simple Valsalva maneuver or from external trauma. The risk of rupture is highest in the first 3 weeks of illness.
Putukian et al. reviewed IM and athletic participation. They recommend return to LIGHT activity after 3 weeks from symptom onset when the athlete is afebrile, has a good energy level, and does not have any significant associated abnormalities. They recommend returning to CONTACT sports after at least 3 weeks when the athlete has no remaining clinical symptoms, is afebrile, and has a normal energy level.
Jaworski et al. discussed infectious diseases in athletes. They state that splenic rupture occurs because of lymphocytic infiltration that distorts the support structure of the spleen, leading to fragility. They recommend return to light, non-contact activities once the athlete is afebrile and appropriately hydrated, fatigue has improved, and a minimum period of 3 weeks has passed from symptom onset.
Figure A shows a petechial rash, which can be seen in IM. Amoxicillin increases the risk of rash. Figure B shows unilateral exudative pharyngitis. The left tonsil is
covered
by
a
white
exudate/pseudomembrane.
Incorrect
Question 32
A workers' compensation carrier for a local manufacturing company requests a second opinion on a 59-year-old man who sustained a crush injury to his foot and leg at work 6 months ago. His leg and foot were pinned between a forklift and a wall when an employee he was supervising lost control of the forklift. The employer suspects that the injured worker is malingering because the treating physician released him to work, but he has not returned to work. Which of the following elements of your history will best help you determine that the injured worker does not want to return to work out of fear of a confrontation with the employee he was supervising?
Explanation
Question 33
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
REFERENCES: Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120.
Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
Question 34
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
REFERENCES: Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Mansat P: Surgical treatment of the rheumatoid elbow. Joint Bone Spine 2001;68:198-210.
Question 35
A 23-year-old man sustains a unilateral jumped facet with an isolated cervical root injury in a motor vehicle accident. Acute reduction results in some initial improvement of his motor weakness. Over the next 48 hours, examination reveals ipsilateral loss of pain and temperature sensation in his face, limbs, and trunk, as well as nystagmus, tinnitus, and diplopia. What is the most likely etiology for these changes?
Explanation
REFERENCES: Young PA, Young PH: Basic Clinical Neuroanatomy. Baltimore, MD, Williams and Wilkins, 1997, pp 242-243.
Hauop JS, et al: The cause of neurologic deterioration after acute cervical spinal cord injury. Spine 2001;26:340-346.
Veras LM, Pedraza-Gutierrez S, Castellanos J, Capellades J, Casamitjana J, Rovira-Canellas A: Vertebral artery occlusion after acute cervical spine trauma. Spine 2000;25:1171-1177.
Question 36
A 32-year-old woman is ejected from her vehicle in a motor vehicle accident. She has a distant history of pacemaker implantation for an unknown arrthymia. She complains of neck pain. Examination reveals midline cervical tenderness but no neurological deficit. CT scans of her cervical spine are shown in Figures A and B. She requires an emergency laparotomy for a splenic injury. Regarding her cervical spine, what is the next best step? Review Topic
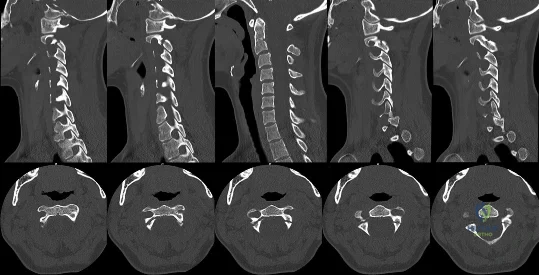
Explanation
Traditional hangman's fractures (execution by hanging) are hyperextension-distraction injuries, severing the spinal cord. Motor vehicle accidents/falls are caused by hyperextension-compression, and neurologic injury is uncommon because the fracture fragments separate, decompressing the spinal canal. The Levine-Edwards classification is most commonly used. Type II fractures have disruption of the posterior longitudinal ligament, and Type III have bilateral facet joint dislocation.
Pryputniewicz et al. reviewed axis fractures. They advocate rigid collar or halo immobilization as initial treatment for hangman's fractures, and surgery for fusion failures or irreducible fractures or repeatedly unstable fractures during initial bracing. For unstable fractures or failure of external immobilization, surgical options include C2-C3 ACDF and dorsal C1-C3 fusion.
Jackson et al. reviewed upper cervical spine injuries. They advocate collar immobilization for Types I and IA fractures, gentle reduction and halo vest immobilization for 6-8weeks for Types II and IIA fractures, and open reduction and wiring/plating (depending on the integrity of the facets/lamina) for Type III fractures.
Li et al. performed a systematic review of hangman fractures. They advocate nonrigid external immobilization for stable Type I and Type II injuries, rigid immobilization for Type IIa and III fractures, and surgery for Levine-Edwards Type IIA and III fractures with significant dislocation or possibility for late instability.
Figure A is a composite of sagittal CT scan images through left facet and pars, dens, and right facet and pars. There is no facet dislocation. Figure B is a composite of sequential axial CT scan images showing bilateral pars interarticularis fracture. Illustration A is the Effendi classification. Illustration B is the Levine-Edwards classification.
Incorrect Answers:
Question 37
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman’s sign. What is the most appropriate treatment plan?
Explanation
REFERENCES: Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: Two to seventeen-year follow-up. J Bone Joint Surg Am 1998;80:941-951.
Ferguson RJ, Caplan LR: Cervical spondylotic myelopathy. Neurol Clin 1985;3:373-382.
Herkowitz HN: A comparison of anterior cervical fusion, cervical laminectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine 1988;13:774-780.
Question 38
A 78-year-old athletic woman has a history of severe back pain without antecedent trauma. She was in the emergency department 2 days ago with a T12 compression fracture. A dual x-ray absorptiometry (DEXA) scan performed earlier this year revealed a T-score of -2.8. Her condition may be attributable to
Explanation
The diagnosis is severe osteoporosis because this patient's T-score is lower than -2.5 on DEXA scan and her fragility fracture involves the T12 vertebra. Osteoporosis may be associated with polymorphisms of the COL1A1 gene. EXT1 is associated with multiple hereditary exostoses, and translocation X:18 is associated with synovial sarcoma. The gene p53 is associated with Li-Fraumeni syndrome and osteosarcoma.
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
PubMed PMID: 24273577. ? View Abstract at PubMed
Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? View Abstract at PubMed
Question 39
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 40
Figure 24 shows the radiograph of a 36-year-old volleyball player with right hip pain. What is the cause of the pain?
Explanation
REFERENCES: Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
Question 41
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of
Explanation
REFERENCES: Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Cain JE Jr, Lauerman WC, Rosenthal HG, Broom MJ, Jacobs RR: The histomorphologic sequence of dural repair: Observations in the canine model. Spine 1991;16:S319-S323.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 42
Which laboratory findings would most support a diagnosis of prosthetic joint infection (PJI) in a hip or knee arthroplasty performed 3 weeks ago?
Explanation
The diagnosis of acute PJI is associated with different criteria than the diagnosis of a chronic PJI. There is no agreed-upon threshold for ESR during the acute period (6 weeks) following total joint arthroplasty. The CRP threshold is higher during the acute period (100 mg/L vs 10 mg/L for a chronic infection). The threshold for synovial fluid analysis for an acute PJI is 10000 cells/µL and more than 90% PMN neutrophils vs 3000 cells/µL and more than 80% PMN neutrophils for a chronic infection.

Question 43
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
REFERENCES: Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Barber CL, Click J, Britt BT: Complications of ankle arthroscopy. Foot Ankle 1990;10:263-266.
Question 44
Which of the following factors is most likely to be associated with prolonged survival of total knee arthroplasty?
Explanation
REFERENCES: Rand JA, Ilstrup DM: Survivorship analysis of total knee arthroplasty: Cumulative rates of survival of 9200 total knee arthroplasties. J Bone Joint Surg Am 1991;73:397-409.
Stern SH, Insall JN: Posterior stabilized prosthesis: Results after follow-up of nine to twelve years. J Bone Joint Surg Am 1992;74:980-986.
Knutson K, Lindstrand A, Lidgren L: Survival of knee arthroplasties: A nation-wide multicentre investigation of 8000 cases. J Bone Joint Surg Br 1986;68:795-803.
Question 45
- What factor is most commonly associated with malignant transformation of a giant cell tumor?
Explanation
Question 46
Which of the following agents have been shown to reduce the incidence of skeletal events in patients with multiple myeloma?
Explanation
REFERENCES: Berenson JR: Bisphosphonates in multiple myeloma. Cancer 1997;15:1661-1667.
Berenson JR, Lichtenstein A, Porter L, et al: Efficacy of pamidronate in reducing skeletal events in patients with advanced multiple myeloma: Myeloma Aredia Study Group. N Engl J Med 1996;334:488-493.
Question 47
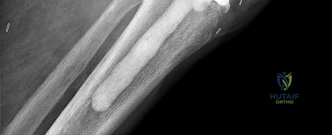
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus? Review Topic

Explanation
Question 48
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of
Explanation
REFERENCES: Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
Hensinger RN, DeVito PD, Ragsdale CG: Changes in the cervical spine in juvenile rheumatoid arthritis. J Bone Joint Surg Am 1986;68:189-198.
Question 49
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of
Explanation
REFERENCES: Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
Question 50
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 51
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
REFERENCE: Stewart AF: Clinical practice: Hypercalcemia associated with cancer. N Engl J of Med 2005;352:373-379.
Question 52
A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values show a WBC count of 11,400/mm3 and an erythrocyte sedimentation rate of 52mm/h. What is the most appropriate action? Review Topic
Explanation
susceptibility to antibiotics, and implant stability. An MRI scan to evaluate for a rotator cuff tear is not indicated at this time.
Question 53
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of
Explanation
REFERENCES: Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Curtis RJ Jr, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 991-1032.
Question 54
A 74-year-old patient is seen for follow-up 6 weeks after undergoing a total shoulder arthroplasty for glenohumeral osteoarthritis. The patient missed the 2-week follow-up appointment and is currently wearing a sling. The incision is well healed with no signs of breakdown. Examination reveals that passive range of motion is forward elevation of 90 degrees, external rotation at the side 0 degrees, and internal rotation up the back is to the level of the greater trochanter. A radiograph shows no signs of fracture or dislocation. What is the next most appropriate management for this patient? Review Topic
Explanation
Question 55
03

Explanation

The Essex-Lopresti reduction technique is a useful method for the treatment of tongue type calcaneal fractures. With this technique, a steinman pin is inserted percutaneously into the posterior facet fragment. This pin is then used to disimpact the fragment and reduce the fracture.
Question 56
A college athlete has a knee injury requiring surgery. He has acne, gynecomastia, and well-developed muscles related to the use of anabolic steroids. What association with steroid use is concerning for surgery and anesthesia? Review Topic
Explanation
Question 57
A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
Explanation
REFERENCES: Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370.
Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Stephens DC: Myositis and fascitis, in Root RK (ed): Clinical Infectious Diseases, ed 1. Oxford, England, Oxford Press University, 1999, pp 769-770.
Question 58
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has
Explanation
Question 59
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
Explanation
REFERENCE: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 60
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 61
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Explanation

Question 62
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy? Review Topic
Explanation
diabetes mellitus, have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category, there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 63
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?
Explanation
REFERENCES: Ghalambor N, Warner JJP: Arthroscopic capsular release: Evolution of the technique and its applications. Tech Shoulder Elbow Surg 2000;1:52-60.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 64
Figures 1 through 3 demonstrate the radiographs obtained from a 45-year-old construction worker who has wrist pain, loss of motion, and loss of strength. Nonsurgical measures have failed, and the patient requests surgery. What is the best surgical option for this patient?

Explanation
This patient has a physically demanding occupation. His radiographs show a long-standing nonunion with avascular necrosis and collapse of the proximal pole. This condition is referred to as a scaphoid nonunion advanced collapse wrist (SNAC). He has advanced arthritis of the capitolunate joint, but the radiolunate joint is preserved. The best option for him would be scaphoid excision with four-corner fusion. Proximal row carpectomy, would be incorrect because of the advanced arthritis of the capitolunate joint. This procedure relies on normal cartilage/joint articulation of the capitate as well as of the lunate fossa of the distal radius. Proximal pole scaphoid excision alone would not address the advanced arthritis of the capitolunate joint. Scaphoid fixation with bone grafting would not address the midcarpal arthritis and advanced proximal pole collapse.
Question 65
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
Explanation
REFERENCES: Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction.
Foot Ankle Clin 2007;12:137-151.
Migues A, Solari G, Carrasco NM, et al: Repair of talar neck nonunion with indirect corticocancellous graft technique: A case report and review of the literature. Foot Ankle Int 1996;17:690-694.
Question 66
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of
Explanation
REFERENCE: Fitzgerald RH Jr: Infected total hip arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:249-262.
Question 67
View Abstract at PubMed Figures 87a and 87b are sagittal and coronal MR images of the affected elbow of a 36-year-old man who has a history of painful mechanical symptoms in his dominant arm when extending his elbow in full supination. What is the most likely cause of his painful snapping? A B

Explanation
The MRI studies show a radiocapitellar plica. This anomalous structure has been associated with symptomatic snapping. Lacertus fibrosis contracture will not cause painful snapping. An intra-articular pathology such as loose bodies is not present on these imaging studies. Olecranon fossa impingement causes posterior pain in extension and is not shown in the images.
RECOMMENDED READINGS
Antuna SA, O'Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001 May;17(5):491-5. PubMed 11337715. View Abstract at PubMed
Ruch DS, Papadonikolakis A, Campolattaro RM. The posterolateral plica: a cause of refractory lateral elbow pain. J Shoulder Elbow Surg. 2006 May-Jun;15(3):367-70. PubMed PMID: 16679240. View Abstract at PubMed
Question 68
An MRI scan
Explanation
Question 69
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis?

Explanation
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 70
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Explanation
REFERENCES: Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Bellier G, Dupont JY, Larrain M, et al: Lateral discoid menisci in children. Arthroscopy 1989;5:52-56.
Question 71
A 23-year-old male reports a firm, immobile mass behind his tibia that creates pain when he walks long distances or uses stairs. He reports no night pain or constitutional symptoms. His WBC, LDH, and Alkaline phosphatase are normal. Radiographs are shown in Figures A and B. A T1 MRI is shown in Figure C. What is the next most appropriate step in management?

Explanation
Osteochondromas are benign lesions, and therefore treatment is dictated by the severity of the symptoms they produce, the skeletal maturity of the patient, and concern for malignant transformation. If the symptoms are tolerable, excision is delayed until patient reaches skeletal maturity or for as long as possible due to increased risk of recurrence. In a more symptomatic skeletally immature patient, marginal excision is performed. Depending on the location, an additional concern for these patients is periarticular deformity or limb length inequality after removal. In skeletally mature patients, marginal excision is the treatment with very low risk of local recurrence. Concern for malignant transformation, found in less than 1% of patients, is an indication for wide resection.
Gitelis et al. discussed osteochondromas addressing general characteristics, presentation, and management options. Nonsurgical management is used in asymptomatic patients with no concern for malignant degeneration. Surgical excision is indicated in patients who have pain, interference with joint function, or impingement of the mass on neurovascular structures. These symptomatic tumors are usually treated with marginal resection, but there is the option of intralesional excision in skeletally mature patients. If there is concern for malignant degeneration, wide resection is performed for all patients.
Figure A and B are radiographs of an osteochondroma in which the cortex of the lesion and the underlying cortex are continuous. Figure C is a sagittal cut of a T1-weighted MRI image showing the high signal features of fatty marrow extending from the medullary canal of the tibia up into the bony stock of the pedunculated osteochondroma.
Incorrect Answers:
A 51-year-old female with known metastatic breast cancer presents with acute right thigh pain and inability to bear weight. A radiograph is shown in Figure A. A biopsy is performed that confirms metastatic breast cancer. What is the next step in management?

Local radiation therapy
Intramedullary nailing only
Intramedullary nailing and chemotherapy
Intramedullary nailing, radiation therapy to the tumor site, and chemotherapy
Intramedullary nailing, radiation therapy to the entire femur, and chemotherapy
This patient is presenting with biopsy proven metastatic breast cancer and a pathological fracture. The treatment in this situation is intramedullary nailing with postoperative radiation therapy to the entire femur and chemotherapy.
Due to the process of placing the intramedullary nail, the treating surgeon contaminates the ENTIRE femur with breast cancer. The surrounding area is already contaminated with tumor cells from the fracture, however. While the intramedullary nail will stabilize the pathological fracture, it does nothing to control the local progression of breast cancer in this patient's leg. Local radiotherapy will not only improve the local control of disease but it will palliate the patient's cancer related pain.
Weber et al review bone metastasis to the femur and propose valuable treatment pearls for clinical decision making and the biology which prevents cancer bearing bones to heal properly despite appropriate mechanical stabilization.
Swanson et al review the role of the orthopaedic surgeon in evaluating and treating metastatic bone disease, paying close attention to the necessity to obtain a tissue diagnosis in the event of presumed metastatic disease PRIOR to proceeding with any treatment plan.
All of the following locations are common sites for giant cell tumor of bone to occur EXCEPT?
Posterior elements of the spine
Distal femur
Sacrum
Distal radius
Proximal tibia
As reviewed by Robert Turcotte in the referenced article, the most common locations for giant cell tumor of bone to occur are about the distal femur/proximal tibia, distal radius, and the sacrum. The spine is an uncommon location for giant cell tumors, and when they occur, they usually occur in the vertebral body, not the posterior elements. In the axial skeleton, the sacrum is a common location for giant cell tumor of bone. Outside of the sacrum, giant
cell tumor of bone is characteristically an epiphyseal/metaphyseal lesion. As discussed in the in vitro study by Gortzak et al, treatment of giant cell tumor of bone includes aggressive intralesional curettage augmented with adjuvant treatment like hydrogen peroxide, argon beam, liquid nitrogen, or phenol. Due to the morbidity of the surgical treatment, and the less than perfect long term outcome, adjuvant therapy with an antibody against RANKL called denosumab is currently being investigated in multiple centers across North America as described by Thomas et al in their phase 2 study. Denosumab inhibits osteoclast mediated osteolysis and treatment is associated with improved bone stock and sclerosis of the GCT lesions. While denosumab doesn't obviate the need for surgical excision, the resulting surgical procedure is less extensive and early data may suggest a decreased risk of local recurrence.
While giant cell tumor of bone is a benign condition, there is a small chance for pulmonary seeding of giant cell metastases. This occurs in somewhere between 2-5% of patients with primary giant cells and occurs more often in patients with recurrent disease.
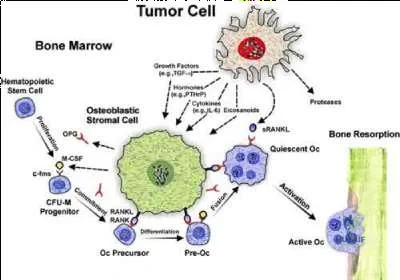
A 59-year-old female presents with a metastatic spinal tumor and has a lytic lesion in the T12 vertebral body. The process of bone resorption in her lytic lesion is mediated by
Direct resorption of bone by tumor cells
Neoangiogenesis of the vertebral body
Macrophage-mediated bony destruction
Tumor induced activation of osteoclasts
Necrosis of the vertebral body
Metastatic tumors are thought to induce osteolysis not by direct resorption of bone (remember only osteoclasts can destroy bone) but rather by releasing osteoclastogenic inflammatory cytokines.
Okeefe et al present a Level 5 review that states TNFa, RANKL, IL-1b, and IL-6 are osteoclastogenic inflammatory cytokins. Among these, RANKL is the most
notable and important cytokine. It binds to RANK, a surface receptor, and initiates osteoclastogenesis.
Goltzman presents a Level 5 review of the skeletal manifestations of malignancy. They report that by binding and neutralizing RANKL, osteoprotegrin (OPG) can diminish the production of functioning osteoclasts, and this factor has been shown to block bone resorption that is associated with malignancy.
Illustration A is a schematic representation of tumor-cell induced osteolysis.
Patients with which of the following conditions have the highest incidence of malignant tumor?
Single enchondroma
Single osteochondroma
Multiple hereditary exostosis
Ollier's disease
Maffucci's syndrome
Of all the listed cartilage lesions, patients with Maffucci's syndrome have the highest risk of malignant tumor - estimated to be 100% over the lifetime of the patient.
Single enchondromas and osteochondromas have a 1% risk of malignant transformation. Multiple hereditary exostosis patients have approximately a 10 % life time risk of malignant transformation. Ollier's disease is one of multiple enchondromas and carries a 30% risk of malignant transformation ( Illustration A) while Maffucci's syndrome is multiple enchondromas with hemangiomas (Illustration B). Maffucci's is also associated with a large number of other malignancies—particularly, pancreatic and hepatic adenocarcinoma, mesenchymal ovarian tumors, brain tumors such as glioma and astrocytoma, and various kinds of sarcomas.
While patients with enchondromas and osteochondromas do have a slight elevation in the risk for malignant transformation, it is not as great as those patients with Ollier's disease or Maffucci's syndrome. Distinguishing enchondromas from low grade chondrosarcomas can be done by looking at radiograph features such as the degree of endosteal scalloping on radiographs and the clinical presence of pain, both associated with low grade chondrosarcomas.
Ryzewicz et al review the diagnosis, pathology, and recommended treatment for patients with benign cartilage lesions. They recommend periodic follow-up even for the most benign lesions to track for malignant degeneration.

A 44-year-old male reports a mass at his right iliac crest that bothers him when he wears a belt. He denies constitutional symptoms

and has no bowel function disturbance. His ESR and CRP are normal. His chest CT is normal. Pelvis radiograph, CT, and MRI images are shown in Figures A-D. A biopsy is performed with histology shown in Figure E. What is the next most appropriate step in management?
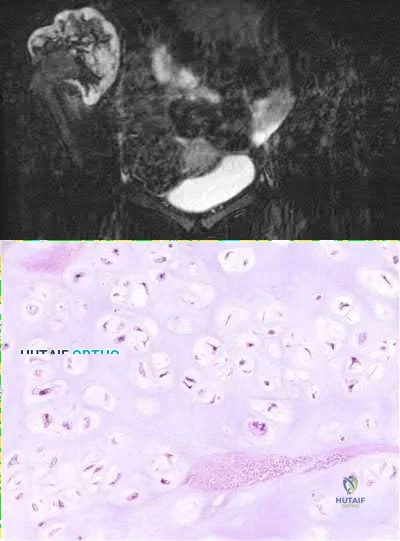
Repeat CT scan in 3 months
Neoadjuvant radiation followed by marginal surgical resection followed by adjuvant chemotherapy 3 . Marginal surgical resection
Wide surgical resection
Neoadjuvant chemotherapy followed by marginal surgical resection followed by adjuvant chemotherapy
The history, imaging, and biopsy is consistent with chondrosarcoma and is appropriately treated with wide surgical resection. Chondrosarcoma is a malignant tumor of cartilaginous origin. It can be a primary lesion but may also develop from a preexisting cartilaginous lesion (e.g., osteochondroma, enchondroma). On plain radiographs, chondrosarcoma is typically visualized as a destructive, lytic lesion. Extension into surrounding soft tissues is frequently seen and delineated well on MRI. The characteristic chondroid matrix (rings
and arcs) can be seen on radiographs (70%), and better visualized by CT. The histology generally demonstrates enlarged, pleomorphic chondrocytes with multinucleated lacunae.
Level 4 evidence by Lee et al reviewed 227 patients with chondrosarcoma with an average follow-up of 6 years. They found that “patients who had had a resection with wide margins (margins extending outside the reactive zone) had a longer duration of survival than did those who had had a so-called marginal resection (margins extending outside the tumor but within the reactive zone) or an intralesional resection (margins within the lesion) (p < 0.04)."
Sixty Gy is a typical radiation dose for which of the following indications?
Prevention of post-operative heterotopic ossification
Neoadjuvant radiation therapy for a high-grade chondrosarcoma
Adjuvant radiation therapy for a high-grade osteosarcoma
Adjuvant radiation therapy for a soft-tissue sarcoma
Palliative therapy for a painful adenocarcinoma metastasis in the thoracic spine
Sixty Gy (or 6000 cGy) is a typical radiation dose for adjuvant radiation therapy for a soft-tissue sarcoma.
External beam radiotherapy plays a major role in the treatment of soft-tissue sarcomas following limb salvage surgery. Radiation doses can vary between 45 and 65 Gy. Any dose of XRT compromises wound healing, but especially those of 45 Gy (delayed healing) and 60 Gy (not expected to heal).
Incorrect Answers:
Question 72
Figures 115a and 115b are the radiograph and intraoperative view of the femoral taper junction of a 68-year-old man who has left groin pain 8 years after undergoing total hip arthroplasty (THA). He has a mild limp and mild pain with active and passive range of motion. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. His serum cobalt level is 5.3 ppb and serum chromium level is 3.4 ppb. In addition to exchanging the acetabular insert, what is the best surgical procedure for this patient?
Explanation
This patient has symptomatic severe pelvic and femoral osteolysis occurring after a metal-on-metal bearing THA. Bearing surface wear and taper wear (corrosion) are debris sources contributing to osteolysis, and both sources should be addressed at surgery. Current recommendations are to not remove a stable cementless femoral component unless the taper is damaged so badly that a new ball will not lock on the taper. There have been reports of repeat local tissue reactions when a new cobalt chromium ball is placed on a taper with corrosion damage. The current recommendation is to minimize the amount of cobalt at the taper junction, and this can be done by avoiding a cobalt chromium ball in favor of a titanium taper sleeve on the damaged taper with a ceramic ball on the new sleeve. Use of a ceramic head on a previously used trunnion poses risk for fracture of the ceramic head.
Question 73
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm 3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
REFERENCES: Del Beccaro MA, Champoux AN, Bockers T, Mendelman PM: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Annals Emerg Med 1992;21:1418-1422.
Kehl DK: Developmental coxa vara, transient synovitis, and idiopathic chondrolysis of the hip, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1035-1058.
Question 74
0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Explanation
Question 75
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 76
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 77
The main arterial supply to the humeral head is provided by which of the following arteries?
Explanation
REFERENCES: Brooks CH, Revell WJ, Heatley FW: Vascularity of the humeral head after proximal humeral fractures: An anatomical cadaver study. J Bone Joint Surg Br 1993;75:132-136.
Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 78
The condition seen in Figure 60 is attributable to

Explanation
Cephallomedullary implants for treatment of proximal femur fractures have gained in popularity over the last decade. Although these implants have improved outcomes for certain fracture types, multiple complications are associated with this implant. Failure may occur secondary to implant design (for example, mismatch of curvature of the nail to the femur, which can result in distal anterior cortical perforation).
RECOMMENDED READINGS
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013 Jun;27(6):303-7. doi: 10.1097/BOT.0b013e318283f24f. PubMed PMID: 23287752.
View Abstract at PubMed
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000093. doi: 10.1002/14651858.CD000093.pub4. Review. Update
in: Cochrane Database Syst Rev. 2010;(9):CD000093. PubMed PMID: 18646058. View Abstract at PubMed
Question 79
Figures 82a through 82c show the radiograph and 3-dimensional (3-D) CT scans of a 2-year-old boy whose scoliosis has progressed 15 degrees during the past year. The child is clinically healthy. He has been walking since 11 months of age. An MRI scan of the entire spine revealed no other anomalies. What additional study is indicated? Review Topic
Explanation
Question 80
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon’s) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include
Explanation
REFERENCES: Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 81
A 12-year-old girl is seen after tripping and twisting her ankle earlier in the morning. She had immediate pain and swelling and was unable to bear weight. Radiographs are shown in Figures 80a through 80c. Appropriate treatment should consist of which of the following? Review Topic

Explanation
Question 82
A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
Explanation
REFERENCES: Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56.
O’Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
Question 83
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 84
A 38-year-old woman has persistent elbow pain but is unable to recall a specific traumatic event. Examination reveals that the patient exhibits apprehension when the elbow is placed in valgus with forearm supination and axial loading. Because of chronicity and failure to respond to nonsurgical management, what is the most appropriate treatment? Review Topic
Explanation
Question 85
Randomized controlled trials can be designed in several ways. Which of the following study designs refers to a randomized controlled trial in which two interventions are compared within the same study group?
Explanation
Question 86
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
Explanation
REFERENCES: Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45.
Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369.
McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.
Brundage SI, McGhan R, Jurkovich GJ, et al: Timing of femur fracture fixation: Effect on outcome in patients with thoracic and head injuries. J Trauma 2002;52:299-307.
Question 87
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 88
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?
Explanation
REFERENCES: Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Robert M, Khouri N, Carlioz H, et al: Fractures of the proximal tibial metaphysis in children: Review of a series of 25 cases. J Pediatr Orthop 1987;7:444-449.
Question 89
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to 3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results show no signs of infection, so a single-stage procedure is preferred.
Question 90
positive skin-test response to CSD skin-test antigen; 3) characteristic lymph node lesions; and 4) negative laboratory investigation for unexplained lymphadenopathy. Treatment consists of azithromycin, ciprofloxacin, doxycycline, or multiple other antibiotics, all of which have been used successfully. Radiation therapy and chemotherapy would be reserved for malignant diseases and would not be appropriate in this setting. Treatment is necessary for this infectious entity; therefore, observation or physical therapy is not indicated.
Explanation
A 56-year-old right hand dominant male presents to your office complaining of right thumb pain worsened with pincer grip and using his mobile phone. He is a writer, and is having difficulty holding his pen. Radiographs from this visit are shown in Figure A. Compared with trapeziectomy alone, which of the following treatment options is likely to result in superior pain relief and improvement of key-pinch strength?

Trapeziometacarpal corticosteroid injection followed by aggressive occupational therapy
Trapeziectomy with interpositional palmaris longus arthroplasty
Trapeziectomy, interpositional arthroplasty, and palmar oblique ligament reconstruction using flexor carpi radialis autograft
Partial trapeziectomy with capsular interpositional arthroplasty
None of the above CORRECT ANSWER: 5
This patient has symptomatic basal joint arthritis with radiographic evidence of pantrapezial arthritis. Simple trapeziectomy has been shown to provide pain relief and improvement of key-pinch strength that is comparable to trapeziectomy plus interpositional arthroplasty.
Definitive surgical management of basal joint arthritis commonly involves excision of the diseased trapezium with concomitant interpositional arthroplasty at the carpometacarpal joint in an effort to mantain the height of the metacarpal. This is commonly done with flexor carpi radialis (FCR) or palmaris longus (PL) autograft. Recent studies have called into question the need for interpositional arthroplasty, suggesting that excision of the trapezium alone can provide non-inferior results.
Davis et. al. randomized 183 symptomatic trapeziometacarpal joints to one of three procedures: trapeziectomy alone, trapeziectomy with palmaris longus interpositional arthroplasty, or trapeziectomy with FCR interpositional arthroplasty and reconstruction of the palmar oblique ligament. For all patients, the thumb metacarpal was percutaneously pinned to the distal pole of the scaphoid to maintain the height of the digit. Patients were evaluated at three and 12 months post-operatively. At both time-points, they found no difference between groups with respect to subjective accounts of pain, function, stiffness, and weakness. Objective measures of thumb key-pinch strength were no different at either time point. The authors concluded that there may be no benefit to ligament reconstruction or tendon interposition in
the short term.
Li et. al. performed a systematic review of four randomized controlled trials and two systematic reviews to evaluate outcomes of trapeziectomy with and without LRTI for treatment of basal joint osteoarthritis. In their review, there were no statistically significant differences in post-op grip strength, pinch strength, visual analog pain scores, DASH scores, and complications. The authors concluded that both procedures produced similar clinical results.
Raven et. al. performed a retrospective analysis of 54 patients who underwent one of three procedures for basal joint osteoarthritis: resection arthroplasty, trapeziectomy with tendon interposition, or trapeziometacarpal arthrodesis.
The authors found resection arthroplasty to be a simple procedure with longterm results pain and functional outcomes comparable to trapeziectomy with tendon interposition.
Naram et. al. retrospectively reviewed 200 patients who underwent simple trapeziectomy with or without LRTI and with or without Kirschner wire stabilization, or a Weilby ligament reconstruction. They found that patients undergoing trapeziectomy with LRTI or a Weilby procedure had a greater incidence of complications compared to trapeziectomy alone, including infection and reoperation.
Figure A is a plain radiograph demonstrating pantrapezial arthritis with the thumb trapeziometacarpal joint being most significantly affected.
Incorrect Answers:
A 31-year-old patient has had a left medial elbow mass for 1 month. The mass has been increasing in size and has now become very painful and erythematous. MRI scans are shown in Figures 76a and 76b. Laboratory studies show an erythrocyte sedimentation rate of 49 mm/h (normal 0 to 20 mm/h) and C-reactive protein level of 23 mg/L (normal 0 to 0.3 mg/L). Histology showed lymphoid tissue and multiple necrotizing granulomas. What organism is responsible for this clinical picture?
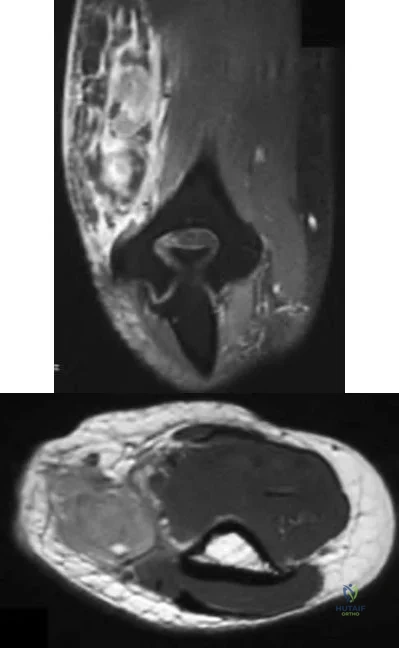
Borrelia burgdorferi
Trichophyton tonsurans
Bartonella henselae
Mycobacterium avium
Corynebacterium minutissimum
Cat scratch disease (CSD) is an important diagnosis for the orthopaedic surgeon to consider in the differential diagnosis of soft-tissue masses adjacent to epitrochlear or cervical lymph nodes. It is a soft-tissue tumor simulator and a high index of suspicion is necessary in all patients with upper extremity or head and neck adenopathy and a history of cat exposure. Although generally not required for diagnosis, cross-sectional imaging will reveal a mass with surrounding edema in an area of lymphatic drainage. A peripheral blood sample can be tested for Bartonella henselae - the offending organism with this diagnosis. Classically the histology of these lesions when biopsied will show multiple necrotizing granulomas. Mycobacterium avium is the only other organism that would demonstrate a granulomatous reaction and the location is classic for CSD. Borrelia burgdorferi is associated with Lyme disease.
Mycobacterium avium may be a source of immunocompromised infections in HIV patients. Trichophyton tonsurans and corynebacterium minutissimum are not associated with orthopaedic diseases.
A 45-year-old woman has a painful mass in the dorsum of the right wrist. It is firm and nontender to palpation. She states it has slowly gotten bigger over the past 3 years. You suspect a dorsal wrist ganglion. What is the most definitive way to confirm this diagnosis?
Observe it for 1 year to see if it changes dramatically in size.
Obtain a gadolinium enhanced MRI scan.
Obtain radiographs, looking for scapholunate joint degenerative changes.
Perform a needle aspiration and send the aspirate for cytologic examination.
Apply direct firm manual pressure over the mass to see if it can be ruptured.
Dorsal wrist ganglions are synovial cysts that arise most frequently from the scapholunate joint. They often extend between the extensor digitorum communis and extensor pollicis longus tendons at the wrist. Aspiration of the cyst is both oncologically safe if done appropriately and also the easiest way to definitively confirm the diagnosis. Clear, yellow viscous fluid/gel is most often aspirated. Cytologic evaluation is mandatory to exclude myxoid neoplasms.
Because the lesion has been present for 3 years, further observation is not warranted. The classic presentation, physical examination findings, and location make MRI and radiographs unnecessary. Manual rupture of the mass is not recommended.
A 28-year-old man fell while ice skating 6 months ago and has had ulnar-sided wrist pain ever since. The patient's wrist radiograph is shown in Figure A and a CT scan is shown in Figure B. What is the most appropriate treatment?

Scapholunate ligament repair
Excision of the hook hamate
Excision of the pisiform
Open reduction internal fixation of the hamate
Open reduction internal fixation of the pisiform
Based on clinical history and imaging shown, this patient has developed a pisiform fracture nonunion. Treatment of symptomatic nonunions of the pisiform is by pisiformectomy
Fractures of the pisiform are rare. They often occur in conjunction with injuries to the distal radius or carpus. Non-operative management with cast immobilization in 30 degrees of wrist flexion is the first line of treatment.
Symptomatic nonunions are treated with pisiformectomy.
Palmieri et al. performed pisiformectomies on 21 patients who had pisiform area pain that was refractory to conservative management. Patients had a history of painful union or nonunion of pisiform fractures, arthritis or FCU tendonitis. In all cases, wrist strength and mobility was retained.
Lam et al. reviewed the effect of pisiform excision on wrist function in patients with piso-triquetral dysfunction. After an average follow up of 65 months, 75%
of patients had complete relief of pisiform area symptoms. No differences in grip, wrist motion, strength or power were found in comparison to the contralateral side.
Figure A shows an oblique radiograph of a pisiform fracture nonunion. Figure B shows an axial CT scan sequence of the wrist. A pisiform fracture nonunion is identified with subtle comminution. The pisotriquetral joint appears to be congruent.
Incorrect Answers
A 32-year-old woman jammed her ring finger. Figures 77a and 77b show radiographs of the finger after a closed reduction. Which of the following interventions, if done correctly, is likely to result in the best possible final clinical outcome?

Early removal of a splint and application of continuous passive motion
Application of dynamic extension bracing after the first week
Maintaining reduction of the middle phalanx on the condyles of the proximal phalanx with dynamic external fixation
Open reduction and anatomic restoration of the middle phalanx articular surface
Surgical advancement of the volar plate into the middle phalanx base
The most important determinant in the final clinical outcome in proximal interphalangeal (PIP) joint fracture locations is the maintenance of the PIP joint alignment on the lateral view. This can sometimes be done with just extension block splinting, sometimes the fracture requires dynamic external fixation, and sometimes the fracture requires open reduction or volar plate arthroplasty. Good function can be the result in the setting of an incongruent middle phalanx base as long as the PIP joint alignment is maintained.
Continuous passive motion has not been shown to be of benefit. Whereas dynamic external fixation in a flexed position is a very good treatment, dynamic extension bracing will just precipitate loss of PIP joint reduction and is therefore not indicated. Whereas open reduction of the articular surface is theoretically desirable, it is generally impossible in the setting of the comminution of the volar middle phalanx base. Furthermore, open reduction and internal fixation by itself does not guarantee that the PIP joint alignment will be maintained, and typically it causes finger stiffness given the extensive surgical approach. Likewise, volar plate arthroplasty is a surgery of last resort and requires careful attention to PIP joint alignment before joint pinning. In this case, with characteristics of comminution, dynamic external fixation is the preferred choice.
A 20-year-old woman sustained a laceration to her volar forearm 4 cm proximal to the wrist flexion crease. She has numbness in the thumb, index, and middle fingers. After microscopic repair of the median nerve, 2 weeks of splinting, and commencement of a hand therapy program, the patient is most likely to require what secondary operation 6 months after the injury?
Tenolysis of the profundus tendons at the wrist
Nerve transfer of the ulnar motor nerve to the median motor nerve
Opponensplasty with the extensor indicis
Open carpal tunnel release
Transfer of the extensor digiti minimi to the first dorsal interosseous tendon
The patient sustained a laceration of the median nerve in what would be considered a low median nerve injury. Standard treatment entails exploration and microscopic repair of the median nerve. With a good quality nerve repair in a young adult, return of some sensory function (albeit reduced compared with the normal nerve) is usual. Return of motor function to the thenar muscles is more unpredictable. If the patient begins a therapy program within a few weeks after nerve repair, it is unlikely that tenolysis of the profundus tendons would be required. An open carpal tunnel release would be unlikely to change functional return. The patient would not be expected to have lost first dorsal interosseous function after a median nerve laceration because this muscle is innervated by the ulnar nerve. A neurotization procedure for low median nerve palsy has been described, but it consists of transfer of the distal anterior interosseous nerve into the median nerve motor fascicles, not transfer of the ulnar nerve. Therefore, the most likely secondary procedure required in this scenario is an opponensplasty procedure to improve thumb opposition.
What is the most efficient pressure for use with negative pressure wound therapy?
25 mm Hg
75 mm Hg
125 mm Hg
300 mm Hg
500 mm Hg CORRECT ANSWER: 3
In animal and clinical studies, a range of pressures between 50 mm Hg to 500 mm Hg were tested; the most efficient pressure was 125 mm Hg, resulting in a fourfold increase in blood flow, 63% increase in granulation tissue with continuous pressure, and 103% increase in granulation tissue with intermittent pressure. When 125 mm Hg pressures were compared with either those less than 50, or those greater than 250, there was a decrease in granulation tissue in swine models.
Figures 125a and 125b are the current radiographs of a 52-year-old man who sustained an injury to his dominant wrist 8 weeks ago. He is an alcoholic and does not remember the details of how he injured it. Paperwork showing what treatment he received at an
urgent care facility indicates that he was given a splint for his "sprained wrist." Examination reveals the pain is getting better, but there is persistent swelling and range of motion is very limited.
Recommended treatment at this time should consist of

discontinuation of the splint and commencement of a regimen of hand therapy.
casting for an additional 2 weeks and reassessment of the fracture healing at that time.
open reduction and internal fixation of the injury.
proximal row carpectomy.
wrist arthrodesis.
The injury represents a very uncommon presentation of a perilunate injury pattern. Whereas these injuries are sometimes overlooked on initial radiographic studies, they are usually recognized much sooner. In this case of a late presenting perilunate injury in a patient that is not entirely responsible, a proximal row carpectomy represents the best treatment option. Open reduction and internal fixation is generally not successful because of cartilage degeneration and contracture that has developed in the interim. No further splinting or casting is indicated, and neglecting the injury would be indicated only if the patient refused any further treatment. Wrist arthrodesis is generally indicated only as a salvage procedure if a proximal row carpectomy is unsuccessful.
A 47-year-old woman sustained a nondisplaced distal radius fracture 6 months ago and is unable to extend her thumb. When performing reconstruction using the extensor indicis proprius to the extensor pollicis longus transfer, tension is ideally determined by securing the tendons in what manner?
In maximum tension with the wrist and thumb in extension
In maximum tension with the wrist and thumb in neutral
In maximum tension with the wrist and thumb in flexion
According to the tenodesis effect with wrist flexion and extension
According to functional testing with the patient awake under local anesthesia
Extensor pollicis longus rupture can result from distal radius fractures. Synergistic tendon transfer can be achieved using the extensor pollicis longus as the motor donor. Whereas different schemes for achieving optimal tension are available, the most reliable method is to tension the repair under local anesthesia while asking the patient to perform thumb flexion and extension. Tendon transfer tension can be adjusted accordingly to achieve maximum extension without compromising active flexion range. Other methods of tensioning are estimates at best, and maximum tensioning in patients without neuromuscular disease is rarely used in tendon transfers.
Which of the following substances is likely to cause the most soft-tissue damage in the long term if injected into a fingertip under
high pressure?
Grease
Latex paint
Water
Oil-based paint
Chlorofluorocarbon-based refrigerant
This type of injury represents a difficult problem in hand surgery. The factors that most determine outcome after high-pressure injection injuries into the fingertip include: involvement of the tendon sheath, extent of proximal spread of the injected substance, pressure setting, and delay to surgical treatment.
The other factor that likely is most important is the type of substance injected. Water and latex-based paints are least destructive. Grease and chlorofluorocarbon-based substances are intermediate, but aggressive surgical debridement can restore reasonable function. Oil-based paints are highly inflammatory and can cause such chronic inflammation such that amputation may be the only reasonable treatment option despite early aggressive surgical treatment.
A 37-year-old woman has right-hand numbness and tingling. Based on the history and examination, carpal tunnel syndrome is suspected, and electrodiagnostic tests also point to the same diagnosis. The patient has worn night splints for the last 8 weeks with continued persistent symptoms. What is the next most appropriate step in management?
Continue the night splinting for 1 additional month.
Continue the night splinting for 3 more months.
Switch to full-time splinting and reevaluate in 1 month.
Switch to full-time splinting for 3 more months.
Perform carpal tunnel release.
Various nonsurgical management options exist for carpal tunnel syndrome (local and oral steroids, splinting, and ultrasound). All effective or potentially effective nonsurgical forms of management have measureable effects on symptoms within 2 to 7 weeks of the initiation of treatment. If a treatment is not effective within that time frame, a different treatment option should be
chosen. In this case, continued splinting is unlikely to improve symptoms and steroid injection or surgery is indicated.
A 46-year-old man sustains an injury to his left index finger while cleaning his paint gun with paint thinner. Examination reveals a small puncture wound at the pulp. The finger is swollen. What is the next most appropriate step in management?
Elevation and observation
Surgical debridement and lavage
Infiltration with corticosteroids
Infiltration with a neutralizing agent
Administration of antibiotics
High-pressure injection injuries are associated with a high risk of amputation. The risk of amputation is highest with organic solvents. The presence of infection and the use of steroids do not impact the amputation rate.
Amputation risk is lower if surgical debridement is performed within 6 hours. Elevation and observation would delay necessary care. Neutralizing agents may be used in specific situations, such as hydrofluoric acid exposure or chemotherapeutic agent extravasation, but in high pressure paint thinner injection, the best outcome is achieved through early surgical lavage.
A 54-year-old woman who has a history of undergoing left trapezium excision with ligament reconstruction and tendon interposition using the entire flexor carpi radialis performed by another surgeon, now reports left basilar thumb pain. Examination reveals pain and subluxation of the carpometacarpal joint with axial loading. The metacarpophalangeal joint hyperextends to 60 degrees, but radiographs show intact joint space. What is the best option to improve function?
Bracing with a hand-based thumb spica splint
Pinning of the carpometacarpal joint
Pinning of the carpometacarpal and metacarpophalangeal joints
Carpometacarpal revision stabilization
Carpometacarpal revision stabilization and metacarpophalangeal joint fusion
The patient previously underwent ligament reconstruction and tendon interposition. However, the previous surgeon failed to address metacarpophalangeal joint hyperextension, which leads to adduction contracture and collapse of the basilar joint. With the basilar joint causing pain and instability, repeat ligament reconstruction should be performed. Splinting alone is unlikely to resolve instability problems. Because the flexor carpi radialis was used, the next option is to use the abductor pollicis longus.
Additionally, the severe metacarpophalangeal joint hyperextension should be corrected by fusion. Simple pinning is unlikely to provide long-term stability when this degree of hyperextension exists.
When evaluating a patient with suspected purulent flexor tenosynovitis in the thumb, the distal forearm and little finger are found to be swollen as well. The most likely anatomic explanation is the existence of a potential space in which of the following?
Through the carpal tunnel
Across the midpalmar space
Communicating with the subcutaneous tissue
Superficial to the distal antebrachial fascia
Between the fascia of the pronator quadratus and flexor digitorum profundus conjoined tendon sheaths
Pyogenic flexor tenosynovitis is an infection within the flexor tendon sheath that can involve the fingers or thumb. The tendon sheaths begin at the metacarpal neck level and extend to the distal interphalangeal joint. In the little finger and the thumb, the sheaths usually communicate with the ulnar and radial bursae, respectively. The potential space of communication, Parona's space, lies between the fascia of the pronator quadratus muscle and flexor digitorum profundus conjoined tendon sheaths. Infection tracking through this space presents as a horseshoe abscess.
Which of the following proximal phalanx fractures can most reliably be treated with a closed reduction and avoidance of surgical measures?
Midshaft transverse diaphyseal fracture with 30 degrees of angulation
Long spiral diaphyseal fracture with 15 degrees of malrotation
Open fracture with skin loss and exposed extensor tendon
Distal condylar intra-articular fracture with minimal displacement
Proximal metaphyseal fracture location with 30 degrees of dorsal tilting
Proximal phalanx fractures are very common, but care must be taken to understand which injuries are reliably treated with nonsurgical measures, and which ones are prone to clinically symptomatic malunion without surgical treatment. The proximal metaphyseal location is a problematic fracture to get reduced with closed measures, and due to the forces of the extensor apparatus, is prone to collapse into the original deformity. Imaging is also frequently difficult because of the overlap of the other fingers and frequently the true angulation is underappreciated. With 30 degrees of angulation, consideration should be given to surgical treatment. Long oblique/spiral fractures with malrotation are also most reliably treated with multiple lag screws, because maintaining the reduction with nonsurgical measures is unreliable, and can lead to significant functional problems in the form of crossover of the fingers with gripping. Open fractures with skin loss clearly are treated with surgical measures. Distal condylar fractures with minimal displacement are another fracture pattern that have a high rate of loss of reduction when treated nonsurgically. Like most articular fractures, they are best treated with anatomic reduction and rigid internal fixation. By comparison, closed midshaft transverse diaphyseal fractures can usually be anatomically reduced and held in this position with closed measures.
Figure 3 shows an arthroscopic view of the radiocarpal joint from the 3-4 portal, looking volarly and radially (Sc=scaphoid, R=Radius). What structure is marked by the asterisk?
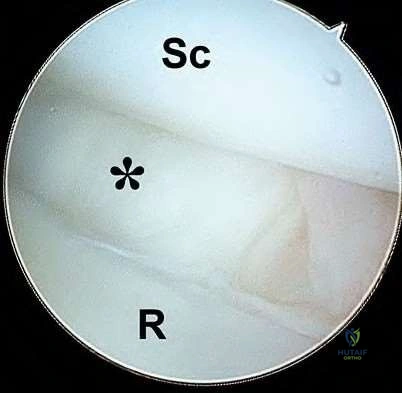
Radioscaphocapitate ligament
Scapholunate ligament
Palmar oblique ligament
Dorsal intercarpal ligament
Triangular fibrocartilage complex (TFCC)
The radioscaphocapitate ligament is a volar capsular structure running obliquely from the radial styloid to the scaphoid waist, ultimately inserting on the proximal radial aspect of the capitate. The radioscaphocapitate ligament is important in preventing ulnar translocation of the carpus. The scapholunate ligament is located intra-articularly, between the scaphoid and lunate. The dorsal intercarpal ligament is a dorsal structure, and not visible during routine wrist arthroscopy. The palmar oblique ligament connects the first and second metacarpal bases. The TFCC is visible during wrist arthroscopy between the radius and ulna.
A 22-year-old man reports a 2-week history of a burning pain along the dorsoradial aspect of the distal forearm. The pain radiates to the dorsum of the thumb. Examination reveals tenderness and reproduction of symptoms with percussion 8 cm proximal to the radial styloid. Reproduction of symptoms also occurs with forearm pronation
and ulnar deviation of the wrist. No discrete sensory deficit is noted and electrodiagnostic studies are normal. Nonsurgical management consisting of rest, splinting, and anti-inflammatory medications for 6 weeks has failed to provide relief. Treatment should now consist of decompression of the
lateral antebrachial cutaneous nerve in the interval between the abductor pollicis longus and the extensor pollicis brevis in the forearm.
lateral antebrachial cutaneous nerve in the interval between the brachioradialis and the extensor carpi radialis longus in the distal forearm.
radial sensory nerve in the interval between the extensor carpi radialis longus and the extensor carpi radialis brevis in the distal forearm.
radial sensory nerve in the interval between the brachioradialis and the extensor carpi radialis longus in the distal forearm.
radial sensory nerve in the interval between the brachioradialis and the extensor carpi radialis brevis in the distal forearm.
Wartenberg's syndrome, or compression of the sensory branch of the radial nerve, occurs in the interval between the brachioradialis and the extensor carpi radialis longus approximately 8 cm proximal to the radial styloid. There may be history of repetitive wrist/forearm circumduction activity (ie, knitting) or of wearing a tight wristwatch or jewelry. It can occur in patients who have been handcuffed. Typical clinical findings are pain, paresthesia, and/or hypesthesia in the dorsoradial aspect of the wrist and hand in the distribution of the radial sensory nerve. There is often a positive Tinel's sign over the compression site. Hypesthesia may be present in the distribution of the radial sensory nerve which is typically on the dorsal aspect of the first dorsal web space and dorsum of the thumb; however, with overlap in the distribution of the superficial radial nerve and the lateral cutaneous nerve of the forearm this may not always be present. Surgical management consists of release of the nerve as it exits the interval between the brachioradialis and the extensor carpi radialis longus in the distal forearm.
A 55-year-old woman with rheumatoid arthritis reports that she awoke with an inability to flex the interphalangeal joint of her thumb. Figure 8 shows an intraoperative finding. What is the most appropriate surgical treatment?

Primary repair of the tendon
Tendon reconstruction with the palmaris longus tendon
Tendon reconstruction using a transfer of the flexor digitorum profundus (FDP) of the ring finger
Thumb metacarpophalangeal fusion
End-to-side repair of the flexor pollicis longus to the FDP of the index finger
The patient has sustained a chronic flexor pollicis longus rupture (Mannerfelt lesion). The injury is most likely a result of tendinopathy and attritional rupture of the tendon secondary to synovitis and bony osteophytosis at the scaphotrapeziotrapezoid joint. Because of the attritional injury and inherent tendinopathy, primary repair is unlikely to be successful. Among the options listed, tendon graft reconstruction with the palmaris longus tendon is the most appropriate treatment. Tendon reconstruction is possible with the flexor digitorum profundus of the index finger, not the flexor digitorum profundus of the ring finger. If osteophytes are encountered, these should be debrided.
Thumb interphalangeal fusion is an option, but metacarpophalangeal fusion is not beneficial. End-to-side repair of the flexor pollicis longus to the FDP of the index finger is not appropriate and would sacrifice needed function of the index finger.
Figures A and B show the initial radiographs of a 27-year-old snow boarder who fell backward onto his left outstretched hand. Which of the following most accurately describes the sequence of events that occurred during this injury?

Lunotriquetral ligament failure followed by distal row dissociation, scaphoid extension, scaphoid failure, and dorsal dislocation of the carpus
Volar dislocation of the lunate followed by scaphoid extension, scaphoid failure, lunotriquetral failure, and distal row dissociation
Dorsal intercarpal ligament failure followed by distal row dissociation, scaphoid failure, lunotriquetral ligament failure, and dorsal dislocation of the carpus
Short radiolunate ligament failure followed by volar dislocation of the lunate, lunotriquetral ligament failure, scaphoid failure, and distal row dissociation
Scaphoid extension followed by scaphoid failure, distal row dissociation, lunotriquetral ligament failure, and dorsal dislocation of the carpus
As described by Mayfield and associates, the typical sequence of events referred to as "progressive perilunar instability" that result in a volar
perilunate dislocation are as follows: scaphoid extension, followed by opening of the space of Poirer, scaphoid failure, and distal row dissociation, which in turn lead to hyperextension of the triquetrum, lunotriquetral ligament failure, and finally dorsal dislocation of the carpus. The lunate remains in the lunate fossa in a perilunate fracture-dislocation but is dislocated in a lunate dislocation. The short radiolunate and dorsal intercarpal ligaments typically remain intact.
Which of the following is the most consistently proposed tendon transfer for radial nerve palsy?
Pronator teres to extensor carpi radialis brevis
Brachioradialis to extensor carpi radialis brevis
Flexor carpi radialis to extensor digitorum communis
Palmaris longus to extensor pollicis longus
Flexor digitorum superficialis to abductor pollicis longus and extensor pollicis brevis
Whereas there are many variations of tendon transfers for radial nerve palsy, the most consistently proposed tendon transfer is the pronator teres to extensor carpi radialis brevis. The brachioradialis is innervated by the radial nerve so that is not an option. The flexor digitorum superficialis, flexor carpi radialis, and flexor carpi ulnaris are appropriate options to transfer to the extensor digitorum communis. The palmaris longus is not always present. A transfer to the abductor pollicis longus and extensor pollicis brevis may not be necessary if the extensor pollicis longus is rerouted to allow for abduction of the first ray.
A patient has severe cubital tunnel syndrome and marked wasting of the intrinsic muscles of the hand. Why is the little finger held in an abducted position?
Accessory slip of the extensor digiti minimi attaching to the abductor digiti minimi tendon
Tetanic contraction of the abductor digiti minimi
Radial collateral ligament insufficiency of the fifth metacarpophalangeal (MCP) joint
Unopposed pull of the flexor digitorum profundus
Muscle innervation from a Martin-Gruber anastomosis
A Wartenberg's sign, where the little finger is held in an abducted position, is associated with an ulnar nerve palsy. This happens when there is an accessory slip of the extensor digiti minimi, which is innervated by the radial nerve, crossing ulnar to the center of the MCP joint to attach to the tendon of the abductor digiti minimi and the proximal phalanx. The abductor digiti minimi and the volar interosseous muscles are both innervated by the ulnar nerve; therefore, there is no tetanic contraction of the abductor digiti minimi.
Unopposed pull of the flexor digitorum profundus results in excess flexion of the proximal interphalangeal and distal interphalangeal joints of the hand as seen with a clawing-type deformity. A Martin-Gruber anastomosis, which is a neural connection between the ulnar and median nerves in the forearm, cannot explain this finger position.
Figure 38 shows the radiograph of a 41-year-old man who reports ulnar palmar pain, decreased sensibility and tingling in the ring and little fingers, and a grating sensation in the ulnar fingers with motion. He reports that he sustained a fall on an outstretched hand 6 months ago. What is the most appropriate treatment option?

Ulnar gutter cast
Short arm cast
Carpal tunnel release
Decompression of Guyon's canal
Excision of a fractured hook of hamate
Excision of a fractured hook of hamate is the most appropriate management. The patient has a hook of hamate fracture with ulnar nerve compression and irritation of the flexor tendons by the fracture surfaces; this puts the tendons at risk for rupture. Cast treatment will most likely not gain union of the fracture and will not address the nerve or tendon problems. Decompression of Guyon's canal alone will not address the tendon issue.
A 25-year-old man was involved in an altercation. Examination reveals loss of active extension of the middle finger metacarpophalangeal (MCP) joint. A diagnosis of sagittal band rupture is made. Which of the following is considered the key diagnostic finding?
Extensor lag of 30 degrees
Extensor lag of 60 degrees
Positive Bunnell intrinsic tightness test
Ability to maintain active extension of the interphalangeal joints
Ability to maintain MCP extension after passive extension
In sagittal band rupture, the extensor tendon may subluxate into the valley between the metacarpal heads. The patient will not be able to actively extend the MCP joint from a flexed position with the subluxated tendon, but will be able to maintain MCP extension after it has been passively extended. Extensor lags can have other etiologies other than extensor digitorum communis subluxation such as tendon laceration or rupture, posterior interosseous nerve palsy, but in these conditions, patients cannot maintain MCP extension. Active interphalangeal extension can be achieved with the intrinsic muscles that are not affected by sagittal band rupture.
What is the effect of shortening of metacarpal fractures?
Causes the greatest degree of extensor lag in the index finger
Causes the greatest degree of extensor lag in the little finger
Results in an average extensor lag of 7 degrees for every 2 mm of shortening
Results in an average extensor lag of 14 degrees for every 2 mm of
shortening
Has no effect on grip strength
Cadaveric models have demonstrated a 7-degree extensor lag for every 2 mm of metacarpal shortening, with the amount of lag increasing in a linear fashion. There was no statistical difference in the amount of lag in regard to the digit involved. Based on muscle length-tension relationships, cadaveric models have also been used to demonstrate an 8% loss of power secondary to decreased interosseous force generation with 2 mm of shortening. Because the intrinsic muscles of the hand contribute anywhere from 40% to 90% of grip strength, decreased interosseous force generation secondary to metacarpal shortening will invariably cause a decrease in grip strength.
A 22-year-old motorcyclist sustains open fractures to the left radial shaft and second and third metacarpals with exposed extensor tendon and bone. The fractures are approached via the dorsal open wounds of the forearm and hand with no additional incisions made. The radiograph and clinical photograph of the remaining defect in the hand are shown in Figures 55a and 55b. The remaining wound can be most appropriately covered with which of the following?

Split-thickness skin grafting
Posterior interosseous rotational flap
Radial forearm rotational flap
Groin flap
Free lateral arm flap CORRECT ANSWER: 3
After adequate debridement, there is exposed bone, tendon, and hardware. Split-thickness skin grafting over exposed tendon will not have a viable bed to support the graft. The tendons would not have healthy surrounding tissue, resulting in poor tendon gliding. The dorsal wound has disrupted the posterior interosseous artery that runs in the septum between the extensor digiti minimi and the extensor carpi ulnaris. Following the reconstructive ladder, the radial forearm rotational flap accomplishes wound coverage with a local flap rather
than a groin flap (a distant flap) or a lateral arm flap (microvascular free tissue transfer).
What is the effect of performing a flexor tenosynovectomy with an open carpal tunnel release for idiopathic carpal tunnel syndrome?
Increased risk of nerve injury
Improved postoperative finger flexion
No added long-term clinical benefit versus open carpal tunnel release alone
Increased postoperative pain
Decreased recurrence of carpal tunnel syndrome
In patients with idiopathic carpal tunnel syndrome, flexor tenosynovectomy has not been shown to change the clinical outcome compared with open carpal tunnel release alone. This has been demonstrated in a randomized clinical trial of open carpal tunnel release with or without flexor tenosynovectomy. There has also been no evidence to suggest there is an added risk to performing the flexor tenosynovectomy. At time of surgery, the gross or histologic appearance of the flexor tenosynovium does not correlate with preoperative symptoms nor with clinical outcomes. The histology of the tenosynovium has been shown to be that of fibrosis in a setting of chronic inflammatory changes and no evidence of an acute inflammatory process exists. There may be an added role for flexor tenosynovectomy in non-idiopathic carpal tunnel syndrome such as in patients with renal disease or diabetes.
Figures 69a and 69b show the radiographs of a 62-year-old man with severe radially sided wrist pain. Management has consisted of wrist splinting, nonsteroidal anti-inflammatory drugs, and activity modification, but he continues to have pain and reports difficulty sleeping. What is the most appropriate treatment for this patient?

Arthroscopic debridement
Open reduction and internal fixation
Scaphoid nonvascularized bone graft and screw fixation
Scaphoid vascularized bone graft and screw fixation
Scaphoid excision and 4-corner fusion
Scaphoidectomy and 4-bone fusion is the most appropriate management based on the choices available. The patient has arthritic changes of SNAC (scaphoid nonunion advanced collapse) wrist, stage III. Stage I is at the radial styloid, stage II is at the radioscaphoid joint, and stage III is at the midcarpal joint. Arthroscopic debridement is not appropriate in patients with arthrosis.
Attempting to achieve scaphoid union is only appropriate if there is no arthrosis or the changes are classified as stage I where radial styloidectomy can be performed.
A 7-year-old boy is referred to your office 3 months after jamming his finger while playing basketball. Examination reveals 40 degrees of active and passive motion at the proximal interphalangeal (PIP) joint. The PIP joint is stable to radial and ulnar stressing. Radiographs are shown in Figures 76a and 76b. What is the most appropriate management?

Observation
Corrective osteotomy
Ostectomy
Hand therapy for aggressive stretching
Dynamic splinting CORRECT ANSWER: 3
The most appropriate management is an ostectomy, or resection of the bone in the subcondylar fossa region. This is a malunion where the subcondylar fossa is blocked by malaligned bone. Because it is a bony block to motion, stretching or dynamic splinting will be of no benefit. The physis of the proximal phalanx is proximal, making remodeling of a fracture at the distal end very
unlikely. A corrective osteotomy has a risk of osteonecrosis of the very small distal fragment.
Figure 78 shows the clinical photograph of a patient who injured his finger while playing football. He cannot actively flex the distal interphalangeal joint of the ring finger. Which of the following is the most accurate statement regarding the injury shown?

The tendon is attached to the avulsed fragment from the distal phalanx.
There is no difference in time sensitivity in an acute injury whether or not the tendon has retracted into the palm.
In a chronic (> 3 months) case of flexor digitorum profundus (FDP) avulsion, the FDP should be tenodesed to the flexor digitorum sublimis (FDS).
If the FDP is advanced more than 1.5 cm, there is a risk for quadriga effect.
The method of repair does not affect repair gapping or strength of the tendon repair.
Overadvancement of the FDP tendon is one of the causes of the quadriga effect. Relative shortening of an FDP tendon decreases the excursion of the neighboring FDP tendons because they originate from a common muscle belly. The patient reports a weak grasp. Answer 1 is not correct because there can be a fracture and the tendon can avulse off of the fracture fragment (Trumble JHS-A 1992). Whether the tendon has retracted into the palm or not does matter because retraction into the palm allows pulleys to collapse and contract and it also means that the vinculae have been stripped off of the tendon.
Regarding answer 3, in chronic cases where the FDS is intact and strong, many patients may be better off with a sublimis finger and no FDP reconstruction that could, in the worst case scenario, worsen a functional proximal interphalangeal joint. Regarding the repair method, there is recent
research showing method of repair (button vs anchor), suture type, and method do affect the biomechanical properties of the repair.
A 44-year-old woman with cubital tunnel syndrome and associated ulnar nerve subluxation with elbow flexion has failed to respond to nonsurgical management. Which of the following statements is most acccurate regarding in situ simple decompression of the nerve compared with subcutaneous anterior transposition?
Patients undergoing anterior transposition have improved motor outcomes.
Patients undergoing anterior transposition have improved sensory outcomes
Patients undergoing simple decompression have improved motor outcomes.
Patients undergoing simple decompression have improved sensory outcomes.
No differences in outcome are likely between treatment types.
Recent reports comparing outcomes of surgical treatment of ulnar nerve compression at the elbow have demonstrated no differences in outcome between simple decompression and anterior transposition. The presence of subluxation of the ulnar nerve was not a contraindication to in situ decompression in the study by Keiner and associates.
What anatomic structure must be excised when performing a volar plate arthroplasty of the proximal interphalangeal joint?
Central slip
Collateral ligament
Checkrein ligament
Triangular ligament
Flexor digitorum superficialis insertion
The collateral ligament must be excised or released from the proximal phalanx to allow gliding of the middle phalanx on the articular surface of the proximal phalanx. Failure to do so may prevent this gliding motion and make the middle phalanx just hinge on the proximal phalanx.
Figures 97a and 97b show a clinical photograph and radiograph of a patient who has a history of repeated drainage from the lesion. What is the preferred surgical treatment?

Excision of the lesion alone
Removal of the osteophyte alone
Distal interphalangeal joint fusion
Excision of the mass and osteophyte removal
Removal of the mass and skin with skin grafting
The patient has a mucoid cyst. Whereas many of these lesions are associated with osteoarthritis, the best surgical treatment of the lesions in patients who have little or no pain is typically excision of the mass with osteophyte removal. Studies have shown that osteophyte excision helps minimize the risk of recurrence. Distal interphalangeal joint fusion is reserved for patients with pain and more advanced radiographic arthritis. Excision of the lesion alone is a less favorable option than excision of the mass and osteophyte removal. The lesion is independent of the skin and thus, skin removal with the mass is unnecessary.
Which of the following structures cannot be seen during standard radiocarpal arthroscopy?
Scapholunate ligament
Lunotriquetral ligament
Radioscaphocapitate ligament
Extensor carpi ulnaris tendon
Superficial insertion of the triangular fibrocartilage complex (TFCC)
The extensor carpi ulnaris tendon is located in an extra-articular position, and as such, cannot be seen during arthroscopy. Wrist arthroscopy is a useful technique for evaluation and treatment of radiocarpal and midcarpal maladies. During standard radiocarpal arthroscopy, the scapholunate and lunotriquetral ligaments can be easily visualized. The superficial TFCC is seen overlying the ulnar head. Volarly, the radioscaphocapitate ligament can be seen as a discrete band of the capsule.
A 20-year-old skateboarder fell 6 months ago and has had radial-sided wrist pain since. His radiograph upon presentation to your office is shown in figure A. What is the most appropriate treatment at this time?

four corner fusion
long arm thumb spica cast
wrist arthroscopy to evaluate intercarpal ligaments
open reduction internal fixation with autologous bone graft
wrist arthrodesis CORRECT ANSWER: 4
This patient has a scaphoid waist fracture nonunion. Several studies indicate that scaphoid nonunions left untreated have a determined course of collapse and progressive arthritis (scaphoid nonunion advanced collapse - SNAC). Per Markiewitz et al, the standard treatment of scaphoid nonunions is open reduction internal fixation with bone graft; non-operative treatment is not appropriate. Proximal row carpectomy and wrist fusion are salvage procedures reserved for patient that has an advanced scaphoid nonunion, collapse and wrist arthritis.
Figures 112a and 112b show the radiographs of a 28-year-old motorcyclist who sustained a closed hand injury in a collision. What is
the most appropriate definitive treatment?

Closed reduction and a hand/forearm cast in the intrinsic plus position
Closed reduction and a hand splint
Primary fusion of the carpometacarpal joints
Closed versus open reduction and internal fixation
Closed reduction and external fixation
Closed versus open reduction and internal fixation is the most appropriate treatment. The radiographs show fracture-dislocations of all five carpometacarpal joints. These injuries are extremely unstable and not amenable to closed (splint or cast) treatment only. External fixation may be warranted in an open, contaminated injury. Fusion would be an option if this were a chronic, painful condition on presentation.
What additional procedure should be done when performing a radioscapholunate fusion for posttraumatic arthrosis following a distal radius fracture?
Excision of the triquetrum and distal pole of the scaphoid
Anterior interosseous neurectomy
Fascial interposition arthroplasty of the capitolunate joint
Sectioning of the dorsal intercarpal ligament
Ulnar shortening osteotomy
Excision of the triquetrum and distal pole of the scaphoid frees up the midcarpal joint, improving radial deviation and the flexion-extension arc of motion of the wrist. This offers an alternative to complete wrist arthrodesis for posttraumatic arthrosis of the radiocarpal joint. An anterior interosseous neurectomy is believed to decrease some pain transmission from the wrist but because the fusion is done dorsal, cutting this volar structure is not routinely done. Fascial interposition is not needed because the capitolunate should be preserved in posttraumatic radiocarpal arthrosis. Sectioning of the dorsal intercarpal ligament would provide no benefit. If the triquetrum is excised, then an ulnar shortening osteotomy is unnecessary.
Apert's syndrome is caused by a mutation in what gene?
Fibroblast growth factor receptor 2 (FGFR2)
Fibroblast growth factor receptor 3 (FGFR3)
Collagen type II alpha 1 chain (COL2A1)
SED late (SEDL)
Fibrillin
Apert's syndrome (acrocephalosyndactyly type 1) is characterized by anomalies of the cranium, hands, and feet. Mutations in the FGFR2 gene cause Apert syndrome.
Anderson et al report that in Apert's syndrome there is widespread anomalies of the feet, with defects including both predictable dysmorphic changes and progressive fusions of the skeletal components during skeletal maturity.
Incorrect Answers:
2: Achondroplasia is related to abnormalities in the FGFR3, not FGFR2.
3: SED congenita is caused by mutations in COL2A1 (type II collagen alpha 1 chain) on chromosome 12. These result in abnormal type II collagen.
4:The X-linked form of SED tarda is caused by mutation in SEDL (SED late)
gene.
5: Marfan syndrome is caused by defects in the fibrillin gene.
What is the most important measure to take to reduce the risk of frostbite of the toes while hiking in extreme temperatures?
Stop often for recovery breaks.
Drink enough warm liquids.
Reduce thermal heat loss from shoes.
Use triple socks.
Adequately "carbo load" before the start.
Several studies showed the most reliable method to reduce the risk of cold exposure injury is to reduce thermal heat loss. This can be done with a combination of protective socks and shoes, and reducing moisture in the shoes.
Figures 45a through 45e are the MRI scans, gross specimen, and histology of the specimen of a 19-year-old man who has an enlarging mass in the second interspace. He reports forefoot pain that is worse with athletic activity. Radiographs show erosive changes of the third metatarsal head. What is the most common complication associated with incomplete excision?
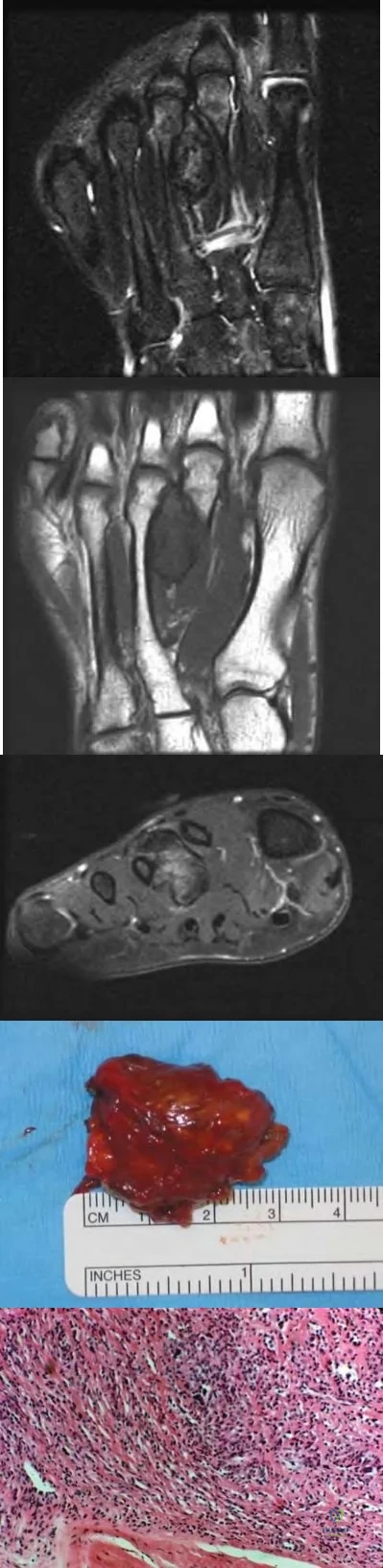
Metastatic disease
Malignant degeneration
Recurrence
Pathologic fracture
Infection
Giant cell tumor of the tendon sheath often arises from the synovial lining of tendon sheaths. This lesion is frequently found in the hand and foot. The lesion is slow growing and can invade adjacent structures. In the foot, wearing shoes or increased activity can cause pain. Incomplete or piecemeal excision can lead to recurrence.
A 42-year-old construction worker presents with pain in his right wrist. A current radiograph of the wrist is shown in Figure A. He reports that rotating activities, such as turning a screw driver, are bothersome and the pain is preventing him from working. A current MRI reveals a TFCC tear, and nonsurgical treatment has failed to provide relief. Treatment should now consist of:

Repair of the ulnar styloid nonunion
Darrach resection of the distal ulna
Complete ulnar head resection
Ulnar hemiresection arthroplasty and TFCC reconstruction/repair
Isolated arthroscopic TFCC reconstruction
The clinical presentation is consistent with DRUJ arthritis in a heavy laborer. Of the options listed, ulnar hemiresection arthroplasty with concurrent TFCC reconstruction or repair would be the most appropriate treatment.
While there are multiple treatment options, the ulnar hemiresection arthroplasty with concurrent TFCC reconstruction or repair is considered most appropriate in heavy laborers, as it would likely resolve the pain and enable them to return to work sooner. The TFCC should be intact when performing an ulnar hemiresection arthroplasty to prevent distal ulna instability with forearm rotation. One could also consider performing a Suave-Kapandji procedure. This procedure creates a distal radioulnar fusion and an ulnar pseudarthrosis proximal to the fusion site through which rotation can occur. The advantage is that the ulnocarpal joint is not sacrificed, and a stable wrist is created.
Scheker et al reported on the outcome of ulnar shortening performed on 32 wrists with early osteoarthritis of the DRUJ. The postoperative wrist ratings were 7/32 excellent, 11/32 good, 9/32 fair, 5/32 poor, with plate irritation being the most frequent postoperative complication.
Figure A is a radiograph showing significant DRUJ arthritis. Illustration A shows ulnar hemiresection arthroplasty. Illustration B shows a Darrach procedure.
Illustration C shows a Sauve-Kapandji procedure. Illustration D is a treatment schematic of TFCC reconstruction.
Incorrect Answers:

Figures 113a and 113b are the radiographs of a 7-year-old girl who was evaluated for a visible elbow deformity by a foster parent. She thought the child fell, but her history was vague. On physical examination, a large prominence was seen over the posterolateral elbow, and the girl lacks the terminal 20 degrees of elbow extension. She has 75 degrees of elbow pronation and supination. She was nontender on examination. What is the most appropriate next treatment step?

Child abuse workup
Closed reduction
Open reduction with possible osteotomy
Observation CORRECT ANSWER: 4
The most appropriate management of this condition is observation. The patient most likely has a congenital dislocation of the radial head, although this may also represent a posttraumatic deformity. The absence of findings on physical examination speaks against an acute injury. The appearance of the radial head reveals the typical findings of a congenital dislocation, namely the convex appearance of the proximal radial articular surface. These children typically have very functional range of motion and do not require treatment unless they are symptomatic. There is nothing in this child's history to suggest abuse.
The most common mechanism of injury to the triangular fibrocartilage complex (TFCC) involves
wrist extension and forearm pronation.
wrist extension and forearm supination.
wrist flexion and forearm pronation.
wrist flexion and forearm supination.
axial load in ulnar deviation.
TFCC tears are common in athletes. As the athlete braces for a fall, the wrist is most commonly in an extended position and the forearm is pronated.
A 28-year-old woman fell on her right wrist while rollerblading 6 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Arthroscopy of the wrist
CT of the wrist
Bilateral PA clenched fist radiograph
Electromyography and nerve conduction velocity studies
AP and lateral radiographs of the forearm
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool.
Figures 12a through 12c show the radiographs of a 28-year-old professional baseball player who has ulnar-sided wrist pain and
numbness and tingling in the fourth and fifth digits for the past 6 weeks. Management should consist of

cast immobilization.
bone stimulation and splinting.
ulnar nerve exploration.
open reduction and internal fixation.
excision of the fragment.
Hook of the hamate fractures typically occur as a result of direct force from swinging a bat, golf club, or racket. Pain is localized to the hypothenar eminence. The injury is best seen on a carpal tunnel view. CT will confirm the diagnosis. Chronic cases can be associated with neuropathy of the ulnar nerve. Excision of the hook through the fracture site usually yields satisfactory results, allowing the athlete to return to competition.
A 40-year-old right-handed professional football player reports persistent right wrist pain after falling during a game 5 days ago. A radiograph is shown in Figure 21. Management should consist of

immobilization in a short arm thumb spica cast.
immobilization in a long arm thumb spica cast.
arthroscopic repair and percutaneous pinning.
open repair and percutaneous pinning.
dorsal capsulodesis.
The radiograph reveals an increased distance between the scaphoid and the lunate, which is indicative of scapholunate disassociation. A ring sign is also present, which represents the distal pole of the scaphoid viewed end on in a palmarly flexed position. In the acute setting, the scapholunate can be repaired. Open repair and percutaneous pinning is the treatment of choice. Dorsal capsulodesis is performed in the chronic setting if such an injury is initially missed.
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Acute tendon repair
DIP joint extension splinting for 6 weeks
DIP and proximal interphalangeal joint extension splinting for 6 weeks
Buddy taping to the middle finger for 2 weeks
Early range-of-motion exercises and return to play as pain permits
Flexor digitorum profundus rupture or “rugger jersey finger” often occurs in the ring finger after the player misses a tackle and catches the digit on the shirt of the opposing player. Surgical repair is required for zone I-type injuries.
A 65-year-old right-hand-dominant man has a 5 year history of progressive right wrist pain. He relates spraining his wrist playing football in college, but otherwise has had no prior traumatic injury. He is a pack per day smoker. An AP radiograph of the wrist is shown in Figure A. Wrist immobilization, anti-inflammatory medications, and injections have failed to provide relief. Which appropriate surgical treatment option offers the lowest risk of postoperative complications?

Radial styloidectomy
Total wrist arthroplasty
Proximal row carpectomy
Scaphoid excision with four-corner fusion
Complete radiocarpal arthrodesis
Proximal row carpectomy (PRC) and scaphoid excision with four-corner fusion are both appropriate surgical treatment options for stage II scapholunate advanced collapse (SLAC) wrist; however PRC is associated with fewer postoperative complications, particularly in active smokers.
Scapholunate interosseous ligament disruption leads to abnormal wrist biomechanics and degenerative arthritis. This progression follows a predictable pattern termed scapholunate advanced collapse. In stage II disease where the entire radioscaphoid articulation is affected but the capitolunate articulation is spared, both proximal row carpectomy (PRC) and scaphoid excision with four-corner fusion offer long-term pain relief while preserving wrist motion and grip strength. Scaphoid excision with four-corner fusion has a higher rate of complications owing to nonunion, hardware issues, and dorsal impingement from malunion. PRC is not recommended in the setting of capitolunate arthritis (stage III).
Tomaino, et al. retrospectively compared PRC and limited intercarpal arthrodesis with scaphoid excision (LWF) at a mean of 5.5 years postoperatively in 24 symptomatic SLAC wrists. They noted good pain relief, grip strength, and function in all but 3 patients having undergone PRC - one of whom required revision to wrist arthrodesis (these patients had symptomatic capitate arthrosis). They concluded that in wrists without capitolunate arthritis, PRC had the benefit of being technically easier to perform, did not require prolonged postoperative immobilization, and avoided the risk of nonunion associated with LWF; however it was not an appropriate surgical option in stage III SLAC wrists with capitolunate involvement.
Strauch reviewed the evaluation and treatment of SLAC and SNAC (scaphoid nonunion advanced collapse) wrists. Treatment options for SLAC wrist include four-corner fusion, capitolunate arthrodesis, PRC, radial styloidectomy, wrist denervation, and complete radiocarpal fusion. Excision of the distal ununited scaphoid fragment is an additional option in the setting of SNAC wrist. He additionally highlights current controversies between PRC vs. four-corner fusion.
Figure A shows an AP radiograph with stage II SLAC wrist. The entire radioscaphoid articulation is arthritic with sparing of the capitolunate surface.
Illustration A shows the modified Watson classification of scapholunate advanced collapse.
Incorrect Answers:

A 25-year-old male presents to the clinic with a painful, enlarging mass at the volar radial wrist. He initially noticed the mass 6 months ago after he hurt his wrist golfing. Figure A shows a clinical photograph of the patient's wrist. Radiographs are unremarkable. An ultrasound of the mass is shown in Figure B. Surgical excision is planned. Which of the following is the most appropriate type of resection and histologic finding?

Intralesional excision; synovial cells with mucin accumulation
Incision & drainage; polymorphonuclear cells
Wide excision; histiocytes with frequent giant cells
Marginal excision; synovial cells with mucin accumulation
Intralesional excision; histiocytes with frequent giant cells
The patient presents with a volar wrist ganglion cyst. Surgical treatment consists of marginal excision. Histologic analysis demonstrates synovial cells with mucin accumulation.
Ganglion cysts are the most commonly presenting masses in the hand. These cysts consist of a synovial cell lining filled with mucin. Dorsal wrist ganglion cysts originate from the scapholunate interval and are more common than volar wrist ganglions, which typically originate from the scapho-trapezio-
trapezoidal joint articulation. Ganglion cysts can cause pain related to mass effect. Ultrasound can help differentiate these masses from vascular malformations or other tumors; ganglion cysts present as homogenous anechoic masses with well-defined borders.
Mayerson, et al. reviewed the diagnosis and management of soft-tissue masses. They highlight the typical presentation of ganglion cysts, which wax and wane in size and transilluminate with a pen light. The authors concluded that MRI is diagnostic if there remains any uncertainly after history and clinical exam.
Head et al compared surgical excision versus needle aspiration of 2,239 adult wrist ganglions in a meta-analysis of 35 studies. Surgical excision resulted in a 76% reduction in recurrence compared to aspiration. Mean recurrence for arthroscopic excision (6%), open surgical excision (21%) and aspiration (59%) and mean complication rate for arthroscopic excision (4%) open surgical excision (14%) and aspiration (3%) were also determined. Data from arthroscopic excision was limited but is a promising technique. Open surgical excision has a significantly lower recurrence rate as compared to aspiration.
Figure A shows a clinical photo of a volar wrist ganglion cyst. Figure B shows the ultrasound image of a volar wrist ganglion cyst.
Incorrect Answers:

A 27-year-old man falls on his hand at work. He notices an immediate deformity of his ring finger. Radiographs are provided in Figure A. Which of the following is the most appropriate initial treatment?

Closed reduction, buddy taping, and early motion to prevent stiffness
Closed reduction and full time extension splinting
Open reduction and repair of the central slip of the extensor tendon
Open reduction and repair of the volar plate
Amputation and immediate return to work
The radiograph demonstrates a volar PIP dislocation. The central slip of the extensor tendon is frequently ruptured and will lead to a boutonneire deformity if left untreated. The PIP must be immobilized in extension to allow the extensor mechanism to heal. Immobilization in extension should be maintained for 6 weeks to allow soft tissue healing. Open reduction and repair of the central slip would be the appropriate treatment for a developing boutonneire deformity that presents in a subacute or chronic time basis.
Illustrations A and B demonstrate a schematic and clinical photo of central slip disruption and secondary deformity with PIP flexion and DIP hyperextension (Boutonniere Deformity).
Posner et al reviewed 7 patients with chronic palmar dislocations of the PIP joint who were treated with open reduction and reconstruction of the extensor mechanism. All patients acheived satisfactory range of motion and the authors concluded that this technique is preferable to arthrodesis.
Peimer et al reviewed 15 patients with palmar dislocations of the PIP joint. Twelve of the fifteen were evaluated on a delayed basis (average 11 weeks following injury) and underwent open reduction and surgical repair of the extensor tendon. Three of the fifteen were seen earlier following injury and were treated with closed reduction and pinning. All fifteen patients acheived satisfactory clinical outcomes although finger range of motion was not fully recovered in any case.
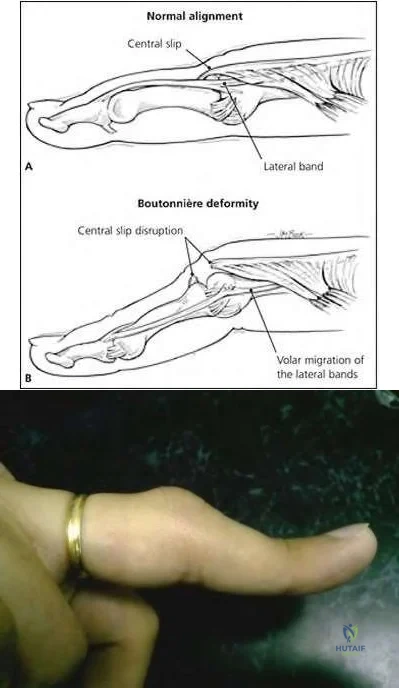
Figure A is of a 22-year-old male college basketball player presents for evaluation of a right index finger deformity. He reports a fall during a game 8 weeks ago, with resultant deformity to the index finger. He "popped it back in" and returned to play. Physical exam is most likely to demonstrate:

Inability to passively extend the PIP joint to neutral, able to passively flex and extend the DIP joint
With the PIPJ flexed, resistance to PIPJ extension causes the DIPJ to become supple
Dorsal subluxation of the PIP joint, able to passively flex and extend DIP joint
With the PIPJ flexed, resistance to PIPJ extension causes the DIPJ to become rigid
Inability to actively flex the DIP joint, able to actively flex the PIP and the MCP joints
The patient presents with a Boutonniere deformity secondary to a traumatic central slip disruption in the setting of volar PIP joint dislocation. Physical exam will demonstrate a positive Elson's test, which is described in answer 4.
The digital extensor mechanism consists of the central slip and two lateral bands, all of which arise from the extensor digitorum communis (EDC) tendon. Flexion of the PIP joint puts the central slip on tension, and volarly subluxes the lateral bands causing them to become slack. Tension on the central slip causes extension of the PIP joint, with concomitant dorsal shift of the lateral bands which help to bring the DIP joint into extension.
In 1986, Elson described his physical examination maneuver for diagnosis closed rupture of the central slip. With the hand resting on the edge of a table, the PIP joint is flexed to 90 degrees over the table edge, and the patient is asked to extend the digit against resistance. Active extension of the middle phalanx can only be observed with an intact central slip, and the adjacent lateral bands will remain slack which allows the DIP joint to remain flail. In central slip ruptures, effort to extend the middle phalanx will be accompanied
by DIP rigidity/extension as the lateral bands are forced to contribute to extension.
Rubin et. al. performed a cadaveric study evaluating the efficacy of physical examination maneuvers to identify acute ruptures of the central slip. They
found that Elson’s test was the only maneuver that could discern central slip integrity in both tested scenarios: 1) pre-boutonniere deformity with division of the central slip and 2) passively correctible boutonniere deformity caused by division of the central slip, the triangular ligament, and the oblique fibers of the extensor expansion.
Figure A is a clinical image of an index finger with boutonniere deformity. Video A is a short demonstration of how to perform the Elson test.
Incorrect answers:
A 25-year-old woman presents to the clinic after knife injury to the volar aspect of her long finger 2 weeks ago. She is evaluated and diagnosed with tendon rupture of the flexor digitorum profundus (FDP). What finding on examination can be expected in this patient?
With passive wrist extension, extension remains at the distal interphalangeal joint
With passive wrist extension, extension remains at the proximal interphalangeal joint
With passive wrist flexion, extension is limited at the distal interphalangeal joint
With passive wrist flexion, flexion remains at the distal interphalangeal joint
With passive wrist flexion, flexion remains at the proximal interphalangeal joint
With an FDP rupture, physical exam would likely reveal loss of flexion at the DIP joint both actively and passively with wrist extension.
When the wrist is in extension, flexor tendons are stretched and should result in flexion at the DIP (FDP) and PIP (FDS) joints. The FDP tendon is responsible for flexion of the DIP joint, and this joint would remain extended during normal tenodesis on passive wrist exam. Inversely, with extensor tendon injuries, there may be a loss of digit extension with passive wrist flexion.
Strickland presents a review article (Part 1) on flexor tendon injuries discussing clinical presentation and repair techniques. A commonly tested concept is that tendon repair is proportional to the number of core sutures, and currently recommended repair includes at least 4 core sutures for strength with epitendinous suture to aid in gliding and provide some strength.
Kamal et al. present current evidence regarding flexor tendon injuries, reviewing examination, repair, and rehab. They note that to date there still remains heterogeneity in treatment patterns and no clear standard of care. Rehab options include no motion, early active range of motion, and controlled passive range of motion. The authors note that early loading may lead to improved strength.
Illustration A depicts the usual tenodesis effect of the digits where passive extension of the wrist produces flexion of the fingers.
Incorrect Answers:

A 20-year-old college football lineman sustains an injury to his index finger during a game. A radiograph of the hand is demonstrated in Figure A. What is the mechanism of injury and most common reason for unsuccessful closed reduction?

Hyperextension mechanism causes the metacarpal head to button hole between the flexor tendon and the lumbrical
Hyperextension mechanism causes volar plate avulsion and entrapment dorsal to the metacarpal head
Rotational mechanism causes the metacarpal head to button hole between the flexor tendon and the lumbrical
Hyperflexion mechanism causes volar plate avulsion and entrapment dorsal to the metacarpal head
Hyperflexion mechanism causes the metacarpal head to button hole between the flexor tendon and the lumbrical
Irreducible dorsal metacarpophalangeal (MP) joint dislocations occur from a hyperextension moment, which causes volar plate displacement and incarceration dorsal to the metacarpal head.
MP joint dislocations are most commonly dorsal and occur with hyperextension injuries. Simple dislocations are reducible with wrist flexion (to relax the intrinsic muscles) and direct palpation over the proximal phalanx base.
Complex dislocations occur with interposition of the volar plate. When irreducible, open reduction is required.
Afifi et al. performed a cadaver study defining the anatomy surrounding irreducible dorsal index MP joint dislocations. They found that of all local structures, only release of the volar plate allowed for reduction of the MP joint. They concluded that volar plate interposition dorsal to the metacarpal head was responsible for irreducible MP joint dislocations.
Bohart et al. describe 9 patients with irreducible dorsal MP joint dislocations (5 thumbs and 4 index fingers). A dorsal approach was performed in each case to allow for reduction of the volar plate. A stable MP joint was achieved in each case. They advocate for a dorsal approach, which minimizes the risk of iatrogenic injury to the neurovascular bundles, which are displaced volarly by the metacarpal head.
Figure A shows an oblique radiograph of the hand demonstrating a dorsal dislocation of the index MP joint. Illustration A provides a schematic of both a simple and a complex dorsal MP joint dislocation. In the case of a complex dislocation, the volar plate avulses from its origin and becomes entrapped dorsal to the metacarpal head.
Incorrect Responses:
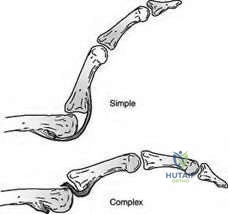
A 3-year-old patient presents to clinic with her parents for the chest wall anomaly seen in Figure A. What other congenital disorder is associated with this syndrome?

Flexible pes planovalgus
Syndactyly
Polydactyly
Macrodactyly
Accessory navicular CORRECT ANSWER: 2
The figure shows an individual with Poland's Syndrome, as demonstrated by the absent sternoclavicular head of the pectorals major. Syndactyly and symbrachydactyly is often seen, in addition to hypoplasia and shortening of the fingers.
Poland's Syndrome, or Poland anomaly/sequence, is thought to be caused by disruption of the subclavian artery in utero, causing various hypoplastic anomalies of the upper extremity. These are typically ipsilateral ranging from aplasia of the sternocostal head of the pectorals major, radio-ulnar synostosis, symbrachydactyly and other limb hypoplasias, or syndactyly of the central digits. Syndactyly is often simple and either complete or incomplete. It is addressed surgically early on, with the chest wall deformities needing reconstruction and muscle transfers closer to sexual maturity. Thoracic, cardiovascular, and genitourinary anomalies may also be present.
Catena et al. proposed a new classification system for Poland Syndrome based on the degree of clinical severity of the entire upper extremity. The classification type increased with more proximal involvement up the upper extremity. This new system may help guide treatment as is takes into account the functional state of the rest of the upper extremity and not just the hand, as previous systems have.
Ireland et al. analyzed 43 consecutive cases of Poland's Syndrome. All cases involved congenital aplasia and syndactyly which was typically simple and incomplete. The thumb can be involved putting it the same plane as the fingers. Anomalies were more frequently seen on the right side. They noted favorable outcomes with surgical correction by syndactyly release initiated by 1 year, with some requiring periodic revision releases, while others required an amputation producing a three-fingered hand.
Figure A shows an absent stenocostal head of the pec major. Only the right side is involved. Illustrations A-C show pre-op and post-op digital release of an individual with syndactyly
Incorrect Answers:
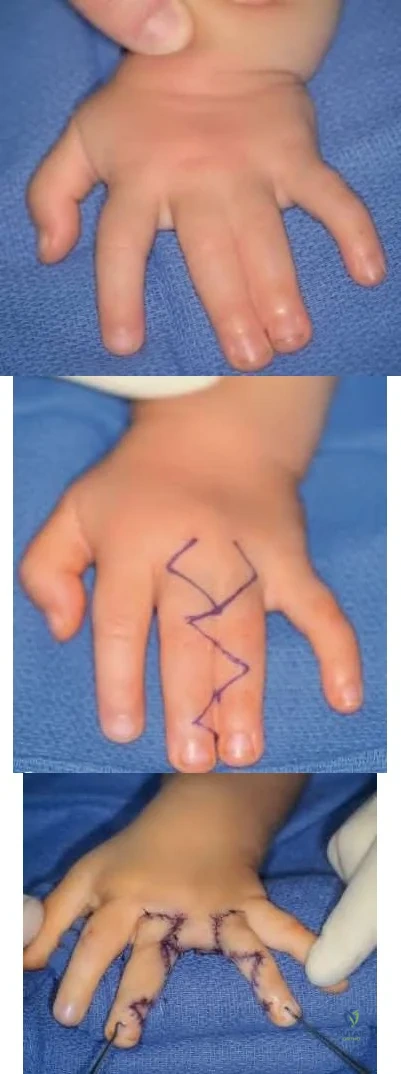
A 32-year-old man sustains an injury to his left thumb. Examination in the ER demonstrates a 2x4 cm wound on the dorsal thumb overlying the proximal phalanx with exposed tendon and bone. What is the most appropriate option for soft tissue coverage?
Cross-finger flap
Moberg advancement flap
Full-thickness skin graft
First dorsal metacarpal artery flap
V-Y advancement CORRECT ANSWER: 4
The first dorsal metacarpal artery flap (Kite flap) is the most appropriate soft tissue coverage option for dorsal thumb wounds that disrupt vascularized tissue overlying the extensor tendon and bone (including the epidermis, dermis, subcutaneous tissue, and tenosynovium) when primary closure is not possible.
Kite flaps are based off of the first dorsal metacarpal artery, which overlies the index finger metacarpal. It offers a pedicle length up to 7 cm and can reliably cover soft tissue defects up to 3x5 cm in area. Given its location, it is appropriate for the treatment of thumb wounds including those to the web space, dorsum, and volar pulp, particularly when injury compromised the vascularity of the wound bed. It can be modified to include both dorsal branches of the proper digital nerve, thereby conferring sensibility to the covered wound. The donor site can subsequently be covered with a full-thickness skin graft.
Rehim et al. reviewed local flaps of the hand. They offer treatment options and appropriate indications based upon the anatomic location and size of the wound within the hand. They conclude that when there are no clinical limitations, local flaps provide ideal soft tissue coverage and function for hand wounds based upon the local anatomy without the need for more complex free tissue transfers.
Eberlin et al. review soft tissue coverage options in the hand. They present four clinical cases and offer one established and one non-traditional surgical treatment option for each. They recommend the first dorsal metacarpal artery flap as an established treatment option in a case of thumb volar pulp injury as it offers contour restoration as well as sensibility when the digital nerves are included with the vascular pedicle.
Illustration A demonstrates a large dorsal thumb soft-tissue injury that is treated with first dorsal metacarpal artery flap coverage and full-thickness skin grafting to cover the donor site.
Incorrect Answers:

A 65-year-old man complains of numbness and tingling in the thumb, index, and long fingers of his dominant right hand for 3 months. An EMG demonstrates prolonged median sensory latency and low amplitude compound muscle action potentials with fibrillations in the abductor pollicis brevis. What is the most appropriate treatment option and the rate of continued symptoms at 1 year after treatment?
Splinting and corticosteroids; 5%
Open carpal tunnel release; 20%
Splinting and corticosteroids; 30%
Endoscopic carpal tunnel release; 2%
Open carpal tunnel release; 5%
The most appropriate treatment of carpal tunnel syndrome (CTS) with EMG evidence of denervation is surgical release. The rate of residual symptoms at 1 year is approximately 20%.
The American Association of Electrodiagnostic Medicine (AAEM) criteria delineates CTS severity by EMG. Mild CTS is purely sensory. Moderate disease demonstrates prolonged sensory and motor latencies. Severe disease progresses to involve muscle denervation. Mild and moderate CTS may be treated with carpal tunnel release following failure of nonoperative treatment; however, early operative treatment is supported for severe disease to limit further denervation. Patients experience significant improvement in
symptoms; however, recovery is prolonged and persistent symptoms may be present in ~20% at 1 year.
Kronlage et al. compared changes in numbness and pain following carpal tunnel release in 47 patients with moderate and 48 patients with severe CTS diagnosed on EMG. At 1 year or longer, 1 (2%) patient with moderate disease had continued symptoms compared to 9 (19%) of patients with severe CTS. They concluded that patients with severe CTS experience significant reductions in symptoms following carpal tunnel release; however, recovery may be prolonged or incomplete at 1 year postop.
Ono et al. performed a systematic review of 25 studies reporting outcomes for the treatment of carpal tunnel syndrome. They noted an increasing trend towards recommending earlier surgery for CTS with or without median nerve denervation. They conclude that this differed from the 2007 AAOS guidelines, which recommended early surgery only in the setting of muscle denervation.
Incorrect Answers:
A 23-year-old man presents with chronic, progressive right wrist pain. He remembers falling onto an outstretched hand 2 years ago. Radiographs, CT scans and a T1-weighted coronal MRI are shown in Figures A through E. No bleeding was identified at surgery. In addition to surgical stabilization, what is the next best step?

Corticocancellous autograft inserted through a dorsal approach
Pedicled distal radius graft inserted through a dorsal approach
Pedicled distal radius graft inserted through a volar approach
Free vascularized femoral bone graft inserted through a dorsal approach
Free vascularized femoral bone graft inserted through a volar approach
This patient has an old scaphoid waist fracture with nonunion, proximal pole avascular necrosis (AVN), and carpal collapse. Optimal treatment is with a free vascularized medial femoral condyle (MFC) graft through a volar approach.
Where there is proximal pole AVN, union was achieved in 88% of patients with a vascularized graft versus 47% with screw and nonvascularized wedge bone graft fixation. The 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) pedicle graft leads to union rates of 71% for scaphoid nonunions and 50% for AVN. The risk for failure is higher when there is DISI or humpback deformity (underscoring the need to restore scaphoid geometry). The MFC graft uses a pedicle from the descending genicular artery or the superomedial genicular artery when the descending genicular artery is not present. The volar approach is preferred as it allows correction of the humpback deformity and anastomosis of the MFC pedicle to the radial artery.
Jones et al. retrospectively compared 2 vascularized bone grafts for treatment of scaphoid waist nonunions with proximal pole AVN and carpal collapse. 4 of
10 nonunions treated with distal radial pedicle graft healed at 19 weeks. 12 of 12 nonunions treated with free vascularized medial femoral condyle (MFC) graft healed at median of 13 weeks. Rate of union was higher, and time to healing was shorter for the MFC graft. They recommend the MFC vascularized bone graft for treatment of scaphoid waist nonunion with proximal pole AVN and carpal collapse.
Figures A, B, C and D are PA and lateral radiographs and coronal and sagittal CT images showing scaphoid waist nonunion with carpal collapse and osteonecrosis of the proximal pole, respectively. Figure E is a T1-weighted coronal image shows diffusely decreased signal within the proximal pole.
Illustrations A and B show harvest and inlay of the 1,2 ICSRA graft. Illustration C shows the MFC graft.
Incorrect Answers:
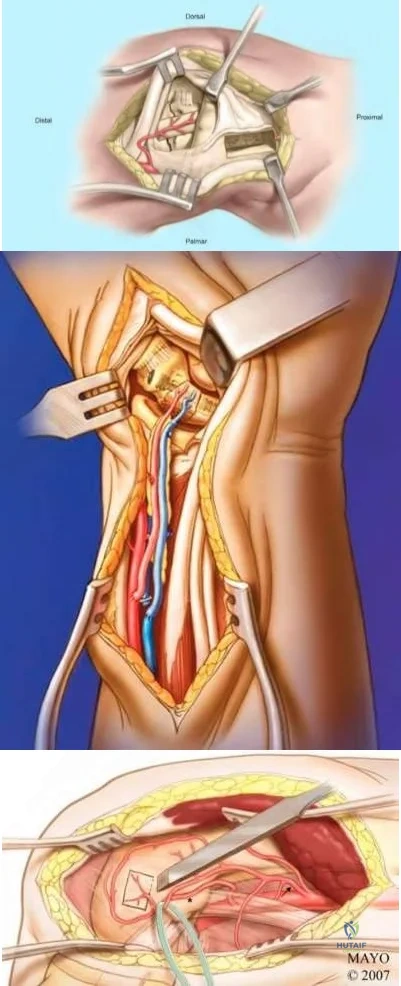
A 38-year-old female develops pain and pallor in all the digits of the right hand daily. Her symptoms have progressed over 2 years despite avoiding direct cold exposure and multiple medications including nifedipine. Recently she has developed the lesions seen Figure A. Workup for underlying disease by her rheumatologist was negative. She is a candidate for Botuninum toxin A injections. What is the physiologic effect of botulinum toxin in the hand for her condition?

Improving proprioception in the fingers and hand by binding to postsynaptic acetylcholine receptors
Improving digital perfusion by cleaving pre-synaptic SNAREs and preventing the release of acetylcholine
Decreasing glabrous skin sensation by reducing hyperexcitability of voltage dependent calcium channels
Strengthening the intrinsic muscles by increasing hyperexcitability of voltage dependent calcium channels
Increasing sympathetic innervation by cleaving pre-synaptic SNAREs and preventing the release of acetylcholine
The patient is displaying Raynaud's Disease with the development of ulcerations from chronic vasoconstriction. Botulinum toxin has been shown to increase the blood supply throughout the hand through the its well-known mechanism of pre-synaptic SNARE cleavage.
Botulinum toxin cleaves the pre-synaptic SNAREs (soluble NSF attachment potion receptor) and prevents the release of acetylcholine from the intracellular vesicles. This has been used for multiple medical purposes, including vasospastic disorders. Raynaud's Disease is characterized by idiopathic vasospasm of the digital arteries without known underlying cause. Usually afflicting pre-menopausal women, it begins with pain and pallor in the digits, typically affecting the bilateral hands. Avoiding cold environments and tobacco are the mainstays of treatment, with calcium-channel blockers being the most common medication used. When these and other medications fail, botulinum toxin injections have been shown to be of benefit by relieving vasoconstriction and decreasing ischemia and pain.
Neumeister et al. reviewed the application of botulinum toxin A and individuals with Raynaud's Disease and Syndrome. They showed marked increases (up to 300%) in digital perfusion in patients receiving these injections into the common digital vessel at the level of the palm. They concluded the mechanisms for this response are likely multifactorial, involving central and systemic effects on neurotransmitters involved in chronic pain pathways, local digital vessel tone, and sympathetic innervation.
Iodio et al. reviewed all clinical studies regarding the use of bootulinum toxin A in raynaud's. There was high variability among the studies in terms of dosage and application method, but all studies reported favorable patient outcomes and some showed improved healing of ulcerations. These studies are promising but are limited due to study design and lack of standardization of botulinum toxin application.
Figure A shows non-infected ulcerations in the digits, common in progressive raynaud's disease.
Illustration A shows ischemic digits due to Raynaud's Syndrome. Illustration B is the same hand after botulinum toxin A injection. Illustration C is a laser doppler of a hand both pre- and post-injection perfusion of botulinum toxin A in an individual with Raynaud's Disease. Illustration D depicts the recommended method of injection, placing 10 units of botulinum around the common digital vessel at the level of the palm.
Incorrect Answers: There is no shown effect on digital proprioception, skin sensation, muscle strengthening.
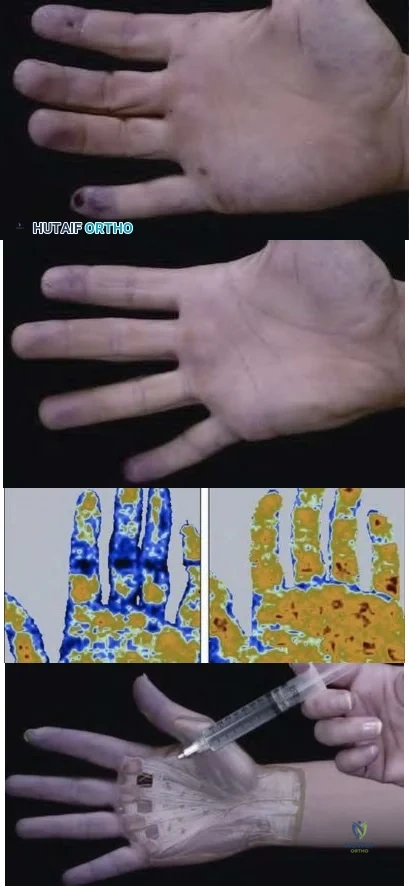
A 27-year-old male injures his thumb during a fall onto an outstretched hand. He has pain at the MCP joint and difficulty grasping objects between the thumb and index finger. He undergoes surgery with the planned incision shown in Figure A. What muscle and corresponding nerve innervates the structure that blocks reduction of the ligament shown in Figure B?
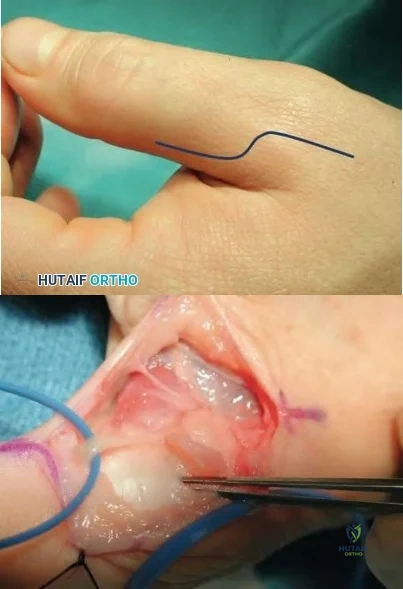
Opponens pollicis, median nerve
Flexor pollicis brevis, ulnar nerve
Adductor pollicis, ulnar nerve
Abductor pollicis brevis, median nerve
Adductor pollicis, median nerve
The patient has an ulnar collateral ligament injury. The structure that blocks reduction of the ligament is the adductor pollicis aponeurosis, which is innervated by the ulnar nerve.
Thumb ulnar collateral ligament injuries occur after a radially directed force on an extended thumb, stressing the ulnar collateral ligament, dorsal capsule and volar plate. The thumb should be radiographed before stress exam if the history warrants so as not to displace a possible bony avulsion. Exam includes valgus stress on the thumb at 0 and 30 degrees of flexion to test the accessory and proper collateral ligaments respectively. With complete rupture of both ligaments, a bump over the ulnar thumb MCP joint may be palpated, signifying a Stener lesion. The ligament usually tears at the distal insertion and displaces proximal and superficial to the adductor aponeurosis. The dorsal capsule and volar plate may also be injured.
Bean et al. evaluated the biomechanics of non-anatomic reconstruction of the ulnar collateral ligaments in cadaveric specimens. They showed that 2mm of volar displacement of the ligament origin will allow for 10 degrees more radial deviation than anatomic placement will. This highlights the need for anatomic reconstruction and that deviation from this will alter joint kinematics.
Figure A shows a planned incision over the ulnar aspect of the thumb MCP joint
Fibure B shows a Stener lesion that is migrated proximally compared to the aponeurosis which is marked by the forceps
Illustration A depicts the retraction of the collateral ligament proximal to the aponeurosis
Illustration B shows a T1 MR coronal image showing a distal avulsion of the UCL and the Stener lesion, denoted by the asterisk, and the arrow pointing to the aponeurosis
Incorrect Answers:

An otherwise healthy 5-year-old female is brought to your office for the deformity shown in Figures A and B. Only the small digit of the left hand is involved and it may be fully flexed, but there is limited passive extension. What is the next best step in treatment?
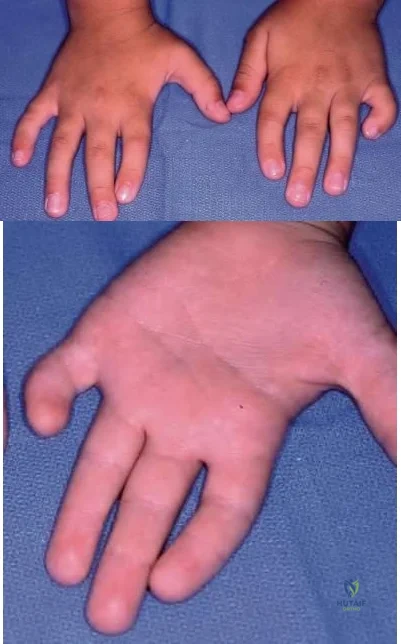
Observation and reassurance
Nighttime extension splinting and stretching regimen
Nighttime extension splinting and stretching regimen with full genetic workup
FDS transfer to radial lateral band
FDS split with transfer of limbs to A2 pulley and central tendon hood
The patient described has isolated camptodactyly with a mild flexion contracture. The best next step in treatment is to begin a stretching and splinting regimen.
Camptodactyly is a nontraumatic flexion deformity isolated to the proximal interphalangeal joint, typically involving the small finger. This is often seen
bilaterally and sporadically, although many congenital disorders are associated. Many underlying anatomical structures have been implicated in the pathogenesis of this condition, with various surgical techniques having been described to address these. If this condition remains untreated, adjacent joint involvement can develop, with MCP hyperextension seen most commonly.
Intrinsic-plus splinting of the hand with passive stretching exercises should be initiated first. Surgery is usually reserved in cases of failed splinting or significant contractures approaching 60 degrees.
Comer et al. reviewed the complications of campylodactly. Most common complications were progression or failed improvement of both PIP contracture and MP hyperextension, isolated PIP postoperative residual stiffness, and bony remodeling of proximal phalanx head preventing full extension. They note inconsistent results after surgical correction which supports early detection and conservative modalities as the mainstay of treatment, focusing heavily on a stretching program and night splinting.
Rhee et al. reviewed outcomes of passive stretching for isolated camptodactyly flexion contractures in a series of children under the age of three years. They showed marked improvement of contracture deformity in all children across all levels of severity, though to less extent with more severe deformities.
Figures A and B demonstrate early contracture of the left small finger. Illustration A is a radiograph showing maintenance of articular congruity.
Incorrect Answers:

A collegiate rower complains of dorsal wrist pain for 6 weeks refractory to NSAIDs and bracing. Maximal tenderness is palpated on the dorsoradial forearm approximately 5 cm proximal to the wrist. Pain is exacerbated with resisted wrist extension. Radiographs are unremarkable. A steroid injection should be directed into the compartment containing which of the following structures?
APL and EPB tendons
ECRL and ECRB tendons
EPL tendon
APL and ECRB tendons
Brachoradialis tendon CORRECT ANSWER: 2
The clinical scenario is consistent with intersection syndrome, a inflammatory response to overuse at the site of the second dorsal compartment crossing under the first dorsal compartment approximately 5 cm proximal to the wrist. An anatomical depiction is provided in illustration A. Injections of the second dorsal compartment, which includes ECRL and ECRB, may relieve symptoms
and quell inflammation. Intersection must be differentiated from DeQuervain's syndrome, which is tenosynovitis of the first dorsal compartment. Injections of the first dorsal compartment, which includes APL and EPB, are part of the treatment algorithm for Dequervain's. Wood et al summarizes the evaluation and treatment of sports-related wrist injuries. Grundberg et al demonstrates the pathologic abnormality of intersection syndrome is stenosing tenosynovitis of the second compartment explaining the rationale behind steroid injections into the sheath.
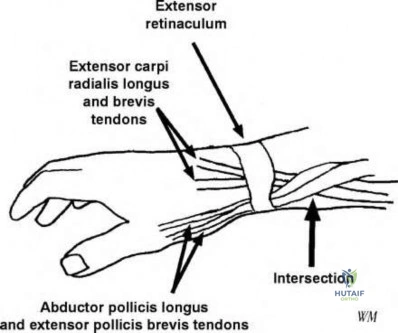
A 42-year-old chef has finally been transferred to the hand specialist 15 hours after injuring his non-dominant hand index finger with a butcher's knife as seen in figure A. He has kept the finger with him, which has been wrapped in saline-soaked gauze and placed on ice. What is the best reason the finger tip should not be replanted?

The replanted digit will likely have poor function due to the delay in care
Possible malingering
The replanted digit will likely have poor function due to the local anatomy
Patient age
Workers compensation patients will have worse outcomes
Single digit amputations proximal to the insertion of the flexor digitorum superficialis (FDS), in generally have poor function and severe stiffness following replantation.
Replantation between the FDS insertion and the distal palmar crease (zone 2 flexor tendon injuries) has historically led to poor results due to stiffness at the proximal interphalangeal joint, decreased sensation in the finger, and tendon adhesions between the FDP and slips of the FDS. Furthermore, outcome studies have demonstrated patients with index finger amputations through this region are more likely to bypass their stiff index finger and utilize their long finger for most tasks. However, amputation of multiple digits through zone 2 would be considered for replantation.
Urbaniak et al performed a retrospective case series of 59 patients who
underwent finger (thumb excluded) replantation for traumatic amputation. They found the functional results were most dependent on level of amputation and patients with amputation proximal to the insertion of the FDS had significantly decreased PIP motion. They concluded that replantation through zone 2 is seldom indicated due to severe stiffness.
Boulas et al reviewed digital replantation and recommend initial treatment should consist of wrapping amputated parts in moistened gauze and placing on ice. Sharp and clean amputations are considered more viable candidates for replantation due to limited damage to the replantation junction compared to crush injuries. Additionally, they state the patients with major psychiatric disorders or those that are unable to comply with postoperative protocols should also be considered poor candidates for replantation.
Figure A demonstrates an amputation through the left index finger proximal phalanx with no evidence of comminution or crush injury. Illustration A demonstrates the flexor tendon zones.
Incorrect Answers:
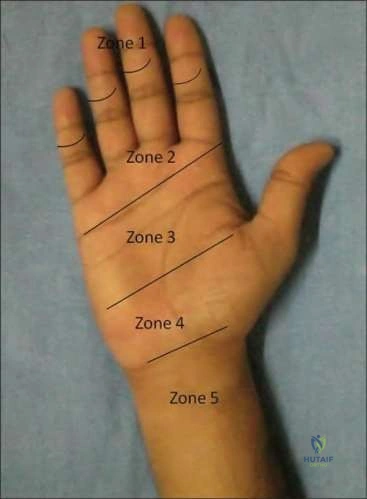
A patient sustains an acute, closed injury to his index finger. The clinical appearance of the finger is shown in Figure A. The patient is asked to extend the finger against resistance, with the PIP joint in 90 degrees of flexion. You note that PIP joint extension was weak, with hyperextension and restricted passive flexion of the DIP joint. When planning to treat this injury non-operatively which active joint motion is encouraged?
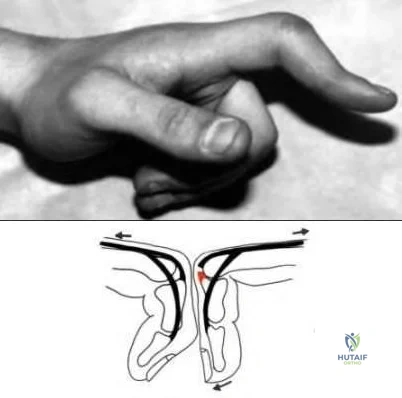
DIP flexion
MCP flexion
MCP extension
PIP extension
PIP flexion CORRECT ANSWER: 1
This patient has sustained a central slip injury. Treatment consists of full time extension splinting of the PIP joint for 5 weeks with active DIP motion (flexion) encouraged.
A central slip injury, or a zone 3 extensor tendon injury, is characterized by PIP flexion and DIP extension (boutonniere deformity). This is most often caused by a rupture of the central slip over the PIP joint caused by a laceration, a traumatic avulsion, or capsular distension in rheumatoid arthritis. A rupture of the central slip causes the extrinsic extension mechanism from the EDC to be lost and prevents extension at the PIP joint. This allows the lumbricals' pull to become unopposed, causing PIP flexion and DIP extension. The examination maneuver described in the question stem is the Elson Test. It is the most reliable way to diagnose a central slip injury before the deformity is present. Non-operative treatment may be undertaken if the injury is closed and presents acutely. The PIP is splinted in full extension for 5 weeks. Active DIP extension and flexion in the splint is encouraged to avoid contraction of the oblique retinacular ligament.
Posner et al. describe the diagnosis and treatment of finger deformities following injuries to the extensor tendon mechanism. They suggest that treatment of a boutonniere deformity depends on its stage. For the acute injury (within the first 2 weeks), immobilization of the proximal interphalangeal joint in full extension for 5 weeks using a static splint that permits active and passive flexion of the DIP joint is usually effective.
Figure A is a clinical photograph demonstrating an index finger with the classic boutonniere deformity of flexion at the PIP joint and hyperextension of the DIP joint. Figure B is a diagram showing the Elson test. When the central slip is intact, there is no hyperextension of the distal phalanx. When the central slip is disrupted, the distal phalanx can hyperextend due to the function of the tight lateral bands.
Incorrect Answers:
A 25-year-old male is stabbed in the proximal volar forearm while fighting in a bar. He presents to the ED with a 1 cm wound and moderate oozing of blood. On exam, he has normal sensation throughout all distributions in his hand, normal radial and ulnar pulses, and a normal tenodesis effect. He is unable to actively flex his index finger DIP joint. Which muscle will also likely not function as a result of his injury?
Flexor digitorum brevis
Flexor carpi radialis
Flexor carpi ulnaris
Flexor pollicis longus
Pronator teres CORRECT ANSWER: 4
The patient has sustained a laceration of the anterior interosseous nerve (AIN), which is a branch of the median nerve and innervates the flexor pollicis longus, pronator quadratus, and the flexor digitorum profundus to the index and long fingers. An intact tenodesis effect signifies that all of his tendons are structurally intact.
The AIN can be injured by a penetrating injury or chronic compression. It
arises from the dorsoradial aspect of the median nerve distal to the elbow. It then passes between the FPL and FDP to lie on the anterior interosseous membrane en route to the pronator quadratus and wrist capsule (Illustration A). Compression sites of the AIN include the deep head of the pronator teres, FDS arcade, edge of the lacertus fibrosus, an accessory head of the FPL, or other accessory muscles of the forearm (FDS, FDP, FCR). In this particular scenario of an acute, penetrating AIN injury, exploration and primary end-to-end suture repair is appropriate.
Rodner et al. review AIN syndrome and stress the importance of ruling out a tendon rupture, which can present similarly and can be differentiated by testing the patient's tenodesis effect. Non-traumatic AIN syndrome is usually the result of a neuritis, similar to Parsonage-Turner Syndrome (brachial plexus neuritis), and may have similar triggers such as viral infection or autoimmune disease. They recommend a prolonged period of observation (~12 months; in the absence of an obvious compressive or space-occupying lesion) due to high rates of spontaneous recovery at about one year.
Park et al. report on 11 patients that underwent surgical exploration for spontaneous AIN syndrome at an average of 7.8 months. The most common compressive structure was a fibrous band of the FDS, however, four patients had no obvious compressive structure, emphasizing the importance of at least six months of conservative treatment.
Incorrect answers:
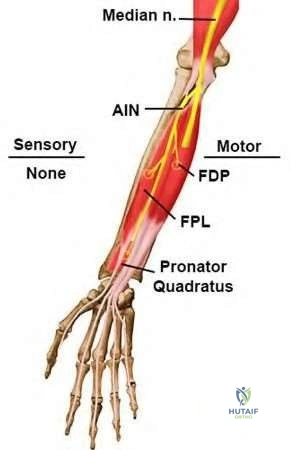
A 38-year-old female presents with 8 months of gradual weakness of her right hand. She denies paresthesias, numbness, and pain in the right upper extremity. She has compensatory thumb interphalangeal flexion during key pinch and intact two point discrimination. She has a negative Tinel's sign at the wrist and elbow. Electromyography (EMG) shows normal sensory conduction velocities but delayed motor conduction to the first dorsal interosseous muscle. Figure A and B show MRI images of pre and post contrast, respectively. Ultrasound is shown in Figure C. What is the next best step?
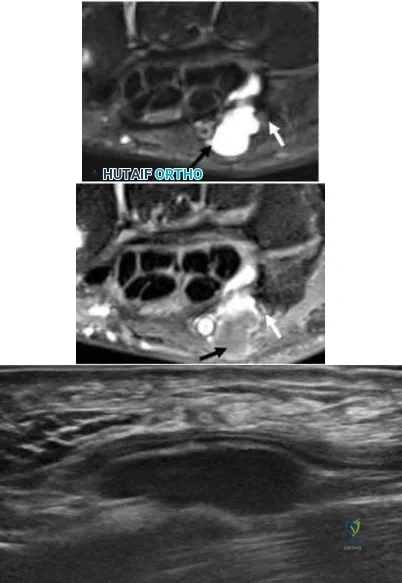
Biopsy of the mass
Cyst excision
MRI of cervical spine
Excision of the hook of hamate
Cubital tunnel release CORRECT ANSWER: 2
The patient has pure motor symptoms from ulnar nerve compression by a ganglion cyst at Guyon's canal. The next best treatment is excision of the ganglion cyst.
Atraumatic compression of the ulnar nerve at Guyon's canal is caused by a ganglion cyst 80% of the time. Compression may present with mixed motor and sensory or pure motor symptoms. With purely motor compression the deep branch of the ulnar nerve is affected resulting in weakness of adductor pollicis. Subsequent loss of metacarpophalangeal flexion and adduction leads to a positive Froment's sign with compensatory thumb IP flexion. Pure motor compression will result in normal sensory examination and intact two point discrimination as sensory branches are unaffected. EMG will localize decreased velocities at the wrist. When neurologic symptoms are present, cyst excision is recommended. Ganglion cysts in this location often arise from the pisohamate joint and excision of the stalk is important to prevent recurrence.
Wang et al. retrospectively investigated the outcomes of 9 patients with
ganglion cysts with symptomatic compression of the deep branch of the ulnar nerve. At a mean follow-up of 23 months they found all patients had improved grip and tip pinch strength. They conclude that surgical intervention can lead to satisfactory outcomes.
Shen et al review the imaging findings possible in patients with ulnar neuropathy. They present a case of a patient with ulnar neuropathy secondary to a ganglion cyst in guyon's canal.
Maroukis et al. review the history of the clinical anatomy of Guyon's canal. They conclude that the three zone theory helped simplify the complex anatomy of ulnar nerve compression at Guyon's canal.
Figure A (Shen et al) shows a T2 fat saturation MRI of a well circumscribed lesion (black arrow) with homogeneous fluid signal intensity at Guyon's canal compressing the ulnar nerve (white arrow). Figure B (Shen et al) shows a post contrast T1 fat saturation MRI showing rim enhancement consistent with a cyst (black arrow) and compression of the ulnar nerve (white arrow). Figure C shows an longitudinal ultrasound view of a anechoic well defined structure consistent with a cyst. Illustration A shows the areas of potential ulnar nerve compression in Guyon's canal. Illustration B shows a table with potential causes for compression at each zone and expected symptoms.
Incorrect Answers:
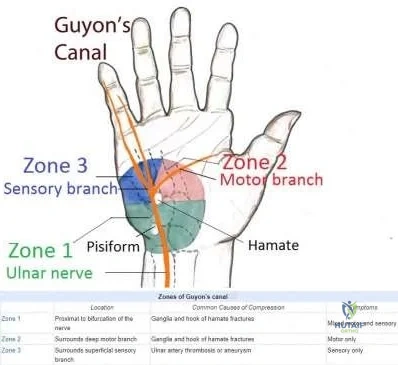
A 20-year-old male presents to clinic for evaluation of right wrist pain. He fell playing flag football about 6 weeks ago. He initially had significant pain but since it slowly improved he did not seek immediate treatment. His improvement has now plateaued. Figures A and B are x-rays, and figures C and D select CT scan images of his right wrist. What is the best treatment option?

Percutaneous screw fixation
Open reduction internal fixation through a volar approach
Open reduction internal fixation through a dorsal approach
Open reduction internal fixation with bone grafting through a volar approach
Open reduction internal fixation with bone grafting through a dorsal approach
The patient presents with a displaced right scaphoid waist fracture with cyst formation. The best treatment would open reduction internal fixation (ORIF) with bone grafting through a volar approach.
The surgical management of scaphoid fracture depends on location and characteristics of the fracture as well as time from injury. Displaced distal pole and waist fractures are typically approached from the volar side, especially if there is a humpback deformity; the proximal pole is more easily accessed from the dorsal side. Injuries with significant comminution or cyst formation due to extended time to treatment are often augmented with bone graft. There is controversy as to the use of vascularized bone graft in nonunion cases.
Rettig et al. reported on fourteen patients undergoing acute surgical fixation for displaced scaphoid waist fractures. Thirteen patients united and regained functional wrist range of motion and grip strength. They advocate for early
operative intervention in these fractures.
Raskin et al. describe the utility of the dorsal approach for proximal pole scaphoid fractures. They report good fracture visualization and the ability to bone graft through the same incision with successful union in a majority of cases.
Pinder et al. reviewed the literature on management of scaphoid nonunions. They found no difference in use of nonvascularized or vascularized bone graft, choice of approach, or use of Kirschner wires versus screw fixation.
Figures A and B are postero-anterior lateral right wrist radiographs with a displaced scaphoid waist fracture and mild humpback deformity. Figures C and D are coronal and sagittal CT cuts, respectively, demonstrating cyst formation and better showing the humpback deformity.
Incorrect Answers:
A 53-year-old white male presents with contractures of his ring finger and lesions over the dorsum of his hand. On examination of the lesions, they are subcutaneous, solid, and firm lesions measuring about 5 mm in diameter. They are located over the dorsum of the PIP joints of his ring and long finger. They become more mobile while the joint is in neutral and less mobile when the joint is in flexion. He also has a 5 degree flexion contracture his ring finger MCP joint. Examination of his palm reveals a palpable cord over the volar ring finger. His neurovascular examination is normal. The appearance of the dorsum of his hand is seen in Figure A. What is the next most appropriate step in treatment?

Collagenase injection and resection of dorsal finger lesions
Collagenase injection without resection of dorsal finger lesions
Observation and follow up
Surgical resection/fasciectomy and resection of dorsal finger lesions
Surgical resection/fasciectomy without resection of dorsal finger lesions
This patient has mild Dupuytren's disease with associated dorsal Dupuytren nodules, which may be observed.
Dupuytren’s disease is a proliferative disorder characterized by fascial nodules and contractures of the hand. It is autosomal dominant with variable penetrance. It exhibits a 2:1 male to female ratio and is classically seen in Caucasian males of northern European descent. The main pathology of
Dupuytren’s disease is excessive myofibroblast proliferation and altered collagen matrix composition lead to thickened and contracted palmar fascia. Surgical intervention is often indicated in cases of ≥30° of MCP contracture or any PIP contracture (usually >15°).
Rayan et al report that dorsal Dupuytren's nodules are a subcutaneous, solid, firm, well-defined, tumor-like mass or a nodule 3 mm in diameter or larger, located over the dorsum of the PIP joint. It is seldom painful and becomes more mobile while the joint is in neutral position and less mobile during joint flexion.
Black et al report that diseased tissue is referred to as nodules or cords. The Dupuytren nodule is a palpable subcutaneous lump that may be fixed to the skin. Cords are highly organized collagen structures arranged in parallel with a relatively hypocellular matrix. Cords are predominantly composed of collagen III while normal palmar fascia is predominantly collagen I.
Figure A is a picture of a dorsal Dupuytren's nodule. Incorrect Answers:
at this time. The dorsal finger lesions should not be resected.
A 37-year-old man has a 2-year history of increasing right wrist pain that is worse at night and aggravated by activity. He denies systemic symptoms, history of trauma, or recent weight loss. On physical exam he has tenderness over the dorsal radiocarpal joint. Radiographs of the right wrist are shown in Figure A. Which of the following imaging studies would be most sensitive for determining the stage of this patient's underlying condition?

Ultrasound
Angiography
CT scan of the wrist
Clenched fist AP radiograph of wrist
Bone scan of the wrist CORRECT ANSWER: 3
The clinical presentation of dorsal radiocarpal wrist pain is suggestive of Kienbock’s disease. Figure A shows an AP radiograph of the right wrist with
evidence of lunate sclerosis with no obvious collapse. The imaging study most sensitive for identifying early lunate collapse in Kienbock's disease is CT scanning of the wrist.
Kienbock’s disease is defined by avascular necrosis of the lunate. It is classified into 4 stages under the Lichtman Classification. In stage 1, plain radiographs appear normal and magnetic resonance imaging is required for diagnosis. MRI is useful for detecting early disease when sclerosis is not evident on plain film radiographs. In stage 2, plain radiographs and/or CT scan images will show sclerosis of the lunate but no evidence of collapse. In stage 3, radiographs and/or CT scan images will show lunate collapse. For stage 4, radiographs show degenerative changes to the adjacent carpus and intercarpal joints.
Imaeda et al. examined the use of MRI for the diagnosis and staging of Kienbock's disease. They found that MRI was most sensitive in detecting early focal loss of signal intensity in the lunate on T1-weighted images. This was a key diagnostic feature in early stages of Kienböck's disease when plain radiographs appear normal.
Cross et al. reviewed the latest concepts for diagnosis, staging, and management of Keinbock's disease. They suggest that computed tomography (CT) or tomography will better characterize lunate necrosis and trabecular destruction once collapse or sclerosis has occurred in late stage disease.
Illustration A is a collection of CT scanning images that show osteonecrosis of the lunate. The blue arrow shows lunate flattening and sclerosis. The red double arrow shows a loss of lunate height and the yellow shows fragmentation of the bone.
Incorrect Answers:
widening of the scapholunate interval.

Each of the following are indications for microvascular replantation EXCEPT?
Thumb amputation
Index finger amputation in a child
Through wrist amputation
Long finger amputation through the proximal phalanx
Mid-palm amputation of all four fingers
As reviewed by Soucacos, there are several major indications for single digit replantation: 1) Level of the amputation is distal to the insertion of FDS. 2) Amputations at the level of the distal phalanx. 3) Ring avulsion injuries involving both the dorsal and palmar skin and blood supply in an isolated finger, as long as FDS is intact. 4) Any amputation in a child. 5) Thumb amputation. Replantation of a single digit, which is amputated at the level of the proximal phalanx or at the PIP joint, particularly in avulsion or crush injury is contra-indicated. Soucacos also discusses appropriate surgical teams, transport, and other related issues surrounding a "transplant team."
All of the following are predictive findings for correctly diagnosing carpal tunnel syndrome EXCEPT:
Abnormal hand diagram
Abnormal Semmes-Weinstein testing in wrist-neutral position
Positive median nerve compression test (Durkan's sign)
Presence of night pain
Loss of small digit adduction (Wartenberg sign)
All of the listed physical exam findings, except for loss of small digit adduction (Wartenberg sign), has been found to be predictive for diagnosing carpal tunnel syndrome.
Szabo et al in a Level 3 study used a regression model to analyze the most predictive factors for correctly diagnosing carpal tunnel syndrome (CTS). Their analysis found that with an abnormal hand diagram, abnormal sensibility by Semmes-Weinstein testing in wrist-neutral position, a positive Durkan's test, and night pain, the probability that carpal tunnel syndrome will be correctly diagnosed is 0.86. They found the tests with the highest sensitivity were Durkan's compression test (89%), Semmes-Weinstein testing after Phalen's maneuver (83%), and hand diagram scores (76%). Night pain was a sensitive symptom predictor (96%). The most specific tests were the hand diagram (76%) and Tinel's sign (71%). The authors concluded that the addition of electrodiagnostic tests did not increase the diagnostic power of the combination of these 4 clinical tests, and proceeding with surgical release is appropriate even if the EMG is normal.
Wartenberg sign is persistent abduction and extension of the small digit when a patient is asked to adduct the digits and is seen in cubital tunnel syndrome, but not carpal tunnel syndrome.
Illustration V demonstrate the Durkan's Compression test for carpal tunnel syndrome.
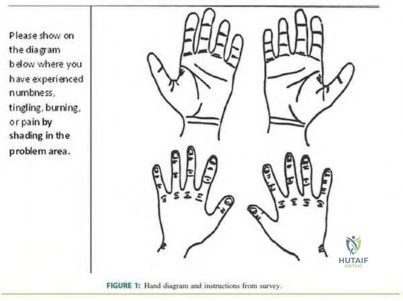
Extrinsic imbalance from splinting a crushed hand with metacarpophalangeal joint extension causes what characteristic hand deformity?
Distal interphalangeal joint extension
Ulnar subluxation of the metacarpophalangeal joints
Proximal interphalangeal joint extension
Proximal interphalangeal joint flexion
Swan-neck deformity CORRECT ANSWER: 4
Failure to splint the hand in an intrinsic positive position leads to increased extrinsic finger flexor tension, leading the DIP and PIP joints to have an increasing flexion position. Illustration A and B show a clinical image and illustration of intrinsic minus hand.
von Schroeder et al present a Level 5 review of hand crush injuries. They conclude that early diagnosis and treatment is critical, but the functional outcome is often poor with associated Volkmann's contracture.
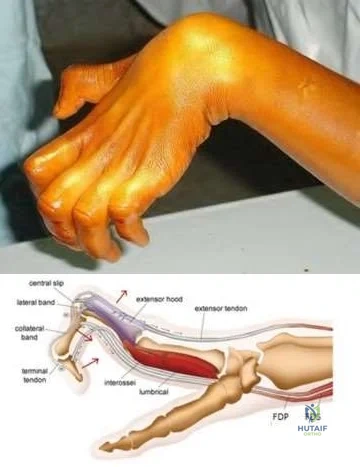
Axon regeneration almost always occurs following a Sunderland second-degree nerve injury because which anatomic structure is not injured?
Epineurium
Endoneurium
Perineurium
Myelin sheath
Schwann cell CORRECT ANSWER: 2
Following a Sunderland second-degree injury, axon regeneration is possible because the endoneurium is intact.
There are two classification schemes for peripheral nerve injuries, which include the Seddon and the Sunderland systems. Under the Sunderland
classification, a second-degree injury is considered a part of the axonotmesis spectrum. The endoneurium, perineurium and epineurium are still intact. This enables complete functional recovery.
Lee et al. review the pathophysiology and evaluation of peripheral nerve injuries. They note that in Sunderland type two injuries, there is physiologic disruption of the axons. Because the endoneurium is still intact, axons are able to regenerate. This process takes months.
Illustration A is a schematic of the various stages of peripheral nerve injury. Incorrect Answers
Sunderland type 2 injury, axon regeneration is possible because of an intact endoneurium.
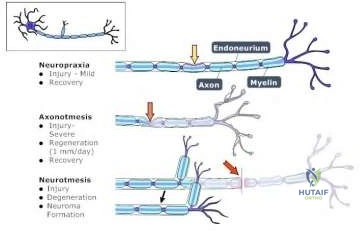
A 29-year-old intravenous drug user undergoes irrigation and debridement of a ring finger abscess. After adequate eradication of the infection, he is left with the skin defect shown in Figure A. What is the most appropriate treatment at this time?

Local woundcare and healing by secondary intention
V-Y advancement flap
Thenar flap
Moberg flap
Cross-finger flap CORRECT ANSWER: 5
Based on the location of the lesion, a cross-finger flap would be most appropriate.
Cross finger flaps are indicated in patients > 30 years of age when the lesion is a volar oblique finger tip lacerations or a volar proximal finger lesions. The advantage is it leads to less stiffness.
Martin et al review the treatment options available for digit injuries. They report treatment of fingertip injuries is a continuous focus of controversy among hand and orthopaedic surgeons. Different treatment options have been described, depending on the affected segment and finger, type of lesion, gender and age of the patient, location, size, and depth of the defect.
Fassler et al reviews the proper management of fingertip injuries discussing variables such as the severity of soft tissue loss and whether bone is exposed.
Incorrect Answers:
A 4-year-old boy sustains a flexor tendon laceration in Zone 2 of his 4th digit when he attempts to grab a knife. Optimal surgical management and postoperative rehabilitation consists of:
2 strand core suture technique and gentle active flexion and extension exercises with wrist in extension
2 strand core suture technique and cast immobilization for 8 weeks
4 strand core suture technique and gentle active flexion and extension exercises with wrist in extension
4 strand core suture technique and cast immobilization for 4 weeks
4 strand core suture technique and cast immobilization for 8 weeks
4 strand core suture technique and cast immobilization for 4 weeks is the preferred postoperative rehabiltation in a 4 year old child.
Ordinarily, adult flexor tendon repair postoperative rehab protocols call for early light active digital flexion with wrist in gentle flexion as long as the tendon has been repaired with a 4 or 6 strand core suture technique and strong epitendinous suture. However, this method cannot succeed without the cooperation of a mature and motivated patient. Children or the mentally disabled are often lacking some of these prerequisites. Therefore, a flexor tendon repair in a child should be treated like a flexor tendon repair with interposed graft in an adult. Immobilization for a minimum of 3 – 4 weeks with a posterior molded plaster splint or cast from the tips of the fingers to just above the elbow. Wrist is flexed 35 degrees, MCPs flexed 60 – 70 degrees and IP joints relaxed in extension. Active motion can be started after the cast is removed at 4 weeks.
A 45-year-old male sustained a fall onto his right wrist 2 weeks ago. A radiograph is shown in figure A. What joint is first affected if left untreated with subsequent development of a SLAC (scapholunate advanced collapse) wrist?

Capitolunate joint
Radioscaphoid
Radioulnar
Radiolunate
STT (scaphotrapezotrapezoidal)
The clinical presentation is consistent with a SLAC wrist. The radioscaphoid joint is the first to be affected in this process.
The radiographs of the right wrist demonstrate a scapholunate dissociation, as evidenced by an increased scapholunate joint space, referred to as scapholunate diastasis (abnormal when the gap is greater than 2 mm and increased from the opposite extremity and other intercarpal spaces).
If left untreated, the wrist may progress to a "SLAC" wrist, as originally described by Watson and Ballet in 1984, which is the most common form of wrist arthritis. The repetitive sequence of degenerative changes is based on and caused by articular alignment problems between the scaphoid, the lunate and the radius.
Kuo et al. review the stages of SLAC wrist. They report stage I SLAC wrist involves changes limited to an area of abnormal contact between the abnormally rotated scaphoid and the radial styloid. In stage II the remaining radioscaphoid joint is affected, as persistent abnormal load transfer and shear across the cartilaginous surfaces leads to degeneration of the proximal scaphoid facet. In stage III, the dorsally translated capitate migrates proximally into the widened scapholunate interval, and degenerative changes occur at the capitolunate joint. The relative congruency of the radiolunate joint in all positions of lunate rotation due to the spherical shape of the lunate facet preserves this articulation, and at all stages of SLAC wrist the radiolunate joint is not involved. The lunate is congruently loaded in every position and, thus, highly resistant to degenerative changes.
Illustration A below shows the stages of involvement in the SLAC wrist.
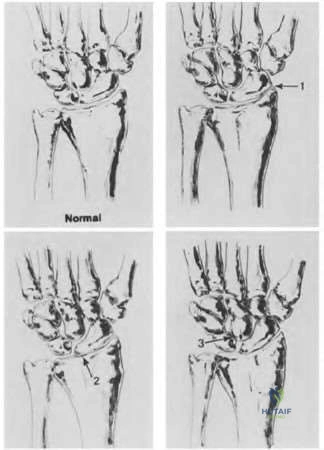
Question 91
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD,
Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 92
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability? Review Topic
Explanation
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy.
Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability.
Park et al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
Question 93
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?

Explanation
Question 94
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
REFERENCE: O’Rourke M, Callaghan J, Goetz D, Sullivan P, Johnson R: Osteolysis associated with a cemented modular posterior cruciate substituting total knee design. J Bone Joint Surgery Am 2002;84:1362-1371.
Question 95
The patient does well initially but returns for the 4-month postsurgical evaluation with ongoing stiffness and pain despite going to physical therapy twice weekly and working on motion at home. She is unable to bear weight comfortably. What is the best next step?
Explanation
In a skeletally immature patient with OCD and minor symptoms, the lesion can be observed and healing obtained with activity limitations if the cartilage is stable (but this cannot be determined radiographically or clinically). Activity restriction and serial follow-up are appropriate if an MRI reveals a stable lesion. MRI is indicated when there is concern that a lesion may be unstable. Surgical treatment depends on MRI findings.
Observation is recommended for OCD lesions in growing patients for 6 months because healing has been observed. Early surgical procedures, although they may be needed in the future, are not appropriate for patients with well-controlled symptoms.
If symptoms continue for longer than 6 months, arthroscopic drilling is not indicated for unstable OCD. The appropriate treatment is OCD fixation. Debridement is not appropriate with a stable lesion.
Evaluation of the fixation and stability of the lesion with advanced imaging after weight bearing and therapy initiation is the most appropriate option. Manipulating the knee without determining whether the stiffness is attributable to subsidence of the fixation or mechanical block is not appropriate. After 4 months, aspiration of a hematoma (if still present) would not yield much benefit. More therapy is not likely to be useful when a patient is attending therapy regularly and working on a home program.

Question 96
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 97
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.
Question 98
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
Explanation

Question 99
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Explanation
REFERENCES: Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br
2001;83:954-962.
Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 100
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?

Explanation
