Orthopedic Board Review MCQs: Arthroplasty, Spine & Pediatrics | Part 78
Key Takeaway
This page offers Part 78 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review. Authored by Dr. Mohammed Hutaif, it features 100 high-yield MCQs, formatted like real exams. Designed for orthopedic residents and surgeons, this quiz provides verified questions and detailed explanations to optimize board certification exam preparation.
About This Board Review Set
This is Part 78 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 78
This module focuses heavily on: Arthroplasty, Hip, Infection, Knee, Scoliosis.
Sample Questions from This Set
Sample Question 1: The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following? Review Topic...
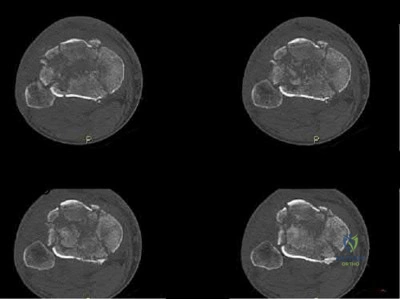
Sample Question 2: A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of...
Sample Question 3: A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynami...
Sample Question 4: In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?...
Sample Question 5: Ayear-oldwomanisreferredforevaluationofapainfulkneereplacement.Sheunderwenttotalkneearthroplasty(TKA)morethan1yearagowithoutperioperativecomplicationsbuthashadconsistentpain sincethesurgery.Thepatient’spreoperativeradiographsandpostoperativ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following? Review Topic
Explanation
(SBQ13PE.87) A 4-week-old child is suspected to have classic arthrogryposis, also known as amyoplasia. Clinical examination and hip ultrasound reveal a unilateral, non-reducible, hip dislocation. What do you recommend to reduce the hip? Review Topic
Pavlik harness application
Semi-rigid abduction brace application
Skeletal traction
Early closed reduction and spica casting
Delayed open reduction with or without pelvic and femoral osteotomy
Delayed open reduction with or without pelvic and femoral osteotomy is recommended in the management of unilateral hip deformities associated with amyoplassia. This procedure should be performed at 6-9 months of age. In order to proceed with reduction, there must be a reasonable arc of flexion/extension and active movement of the lower limbs.
Amyoplasia is the most common recognizable form of arthrogryposis. It most commonly occurs as a sporadic symmetric contracture syndrome that is characterized by symmetrical limb involvement, normal to above-average intelligence, and often a midline facial hemangioma. Approximately 80% of children with amyoplasia will have involvement of the hip ranging from soft tissue contractures to unilateral or bilateral hip dislocations.
Bevan et al. reviewed arthrogryposis. They state that open hip reduction is recommended for the management of unilateral dislocation. There is more controversy with regard to the treatment of bilateral hip dislocations. Open reduction can be performed by a medial or anterolateral approach, with or without pelvic and
femoral osteotomy. This procedure is generally delayed for 6-9 months to facilitate the procedure.
Bernstein et al. also reviewed arthrogryposis. They state that the term 'arthrogryposis' encompasses a broad spectrum of diseases, all with the common phenotype of multiple congenital contractures.
Illustration A shows the characteristic features of an infant with severe arthrogryposis. Note the internal rotation of the shoulders, elbow and knee hyperextension, flexed and ulnarly deviated wrists, flexed finger, external rotation of hips and bilateral clubfeet.
Incorrect answers:
Question 2
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of
Explanation
not indicated.
REFERENCES: Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Question 3
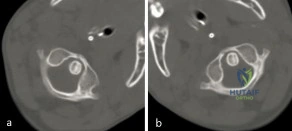
A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynamic computed tomographic (CT) was obtained and shown in Figure A. Panel (a) shows an axial image with maximal rotation to the left. Panel (b) shows an axial image with maximal rotation to the right. What is the most appropriate next step in management? Review Topic
Explanation
Common causes of Atlantoaxial rotatory displacement (AARD) include infection, trauma, and recent neck surgery. Diagnosis is challenging and is best confirmed with dynamic CT (CT with the head turned maximally to either side and at neutral). If the symptoms are acute (less than 7 days) then initial treatment with a soft collar and anti-inflammatory medications is indicated. If the condition has been present for more than a week, more aggressive treatment with halter traction (present 1 week to 1 month) or halo traction (present for 1-3 months) is indicated. If nonoperative modalities fail, the condition has been present for > 3 months, or the patient has neurologic deficits, then posterior C1-C2 fusion is indicated.
Copley et al discuss the evaluation and treatment of various congenital and traumatic conditions of the pediatric cervical spine. They report that the underlying mechanism of Atlantoaxial rotatory displacement (AARD) is inflammation and spasm which can be caused by infection, prior surgery, trauma, and rheumatoid arthritis.
Subach et al reviewed at 20 children with atlantoaxial rotatory subluxation. They found that of the 20 patients treated overall, conservative management failed in 6 (30%), and they required posterior fusion because of recurrence of the atlantoaxial rotatory subluxation or unsuccessful reduction. The major factor predicting the failure of conservative management was the duration of subluxation before initial reduction. Patients with long-standing subluxation were more likely to experience recurrence and require surgery.
Figure A shows an asymmetric placed odontoid within the ring of C1. There is an increased distance from the odontoid to the right arch of C1 which is fixed and minimally changes with maximal rotation to the left. This radiographic finding is indicative of fixed subluxation. Illustration A further demonstrates this.
Incorrect
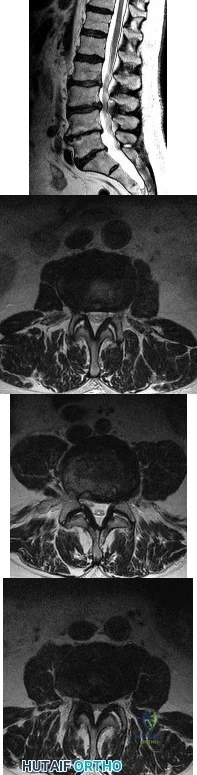
(SBQ12SP.1) A 65-year-old female with a history of breast cancer presents with bilateral buttock and leg pain that is worse with walking and improves with sitting. In addition, she reports that she feels unsteady on her feet and requires holding the railing when going up and down stairs. On physical exam she is unable to complete a tandem gait and has hip flexion weakness, ankle dorsiflexion weakness, and ankle plantar flexion weakness. Her reflex exam shows 3+ bilateral patellar reflexes. Radiographs and an MRI are shown in Figure A and B. What is the next most appropriate step in management. Review Topic

Lumbar epidural injection
Physical therapy with core strengthening and anti-inflammatory medications as needed
Lumbar decompression
Lumbar decompression and fusion
MRI of the cervical and thoracic spine
The clinical scenario is consistent with a patient with symptoms of degenerative spondylolisthesis AND symptoms of myelopathy. Myelopathy must be ruled out by performing an MRI of the cervical and thoracic spine.
Tandem stenosis occurs in approximately 5 to 25% of patients. Because of the stepwise progressive nature of myelopathy, treatment of myelopathy often takes precedence over lumbar spinal stenosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies. Both the upward babinski reflex and the presence of clonus were found to be very non-sensitive (13%). The most sensitive provacative test was found to be the Hoffman sign (59%).
Salvi et al. reviewed the classic presentations for cervical myelopathy including demographics, history, and physical exam findings (the inability to preform a tandem gait, hyperreflexia, an abnormal babinksi and hoffman reflex, the inability to preform rapid movements and bilateral muscle weakness). Additionally they identify other potential causes for myelopathy, including multiple sclerosis, amyotrophic lateral sclerosis, multifocal motor neuropathy, and Guillain-Barre´syndrome.
Maezawa et al. showed that gait analysis can identify a pattern in patients with myelopathy. Patients with severe myelopathy have a characteristic gait with hyperextension of the knee in the stance phase without plantar flexion of the ankle in the swing phase. They also have decreased walking speed and stride length with a prolonged stance phase.
Figure A and B show a classic degenerative spondylolisthesis.
Incorrect Answers:
Question 4
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Explanation
require surgery.
REFERENCES: Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am
2000;82:685-693.
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 5
A year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 6
A 10-year-old girl was thrown over the handlebars of her bicycle and landed directly on her left shoulder. She was treated with a figure-of-8 strap and analgesics. Follow-up examination 2 weeks later reveals that the lateral end of the clavicle is superiorly dislocated relative to the acromion. A radiograph of the shoulder shows calcification lateral to the coracoid process at the level of the acromion, and the clavicle is superiorly displaced. Management should consist of
Explanation
REFERENCES: Falstie-Jensen S, Mikkelsen P: Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br 1982;64:368-369.
Havranek P: Injuries of the distal clavicular physis in children. J Pediatr Orthop 1989;9:213-215.
Question 7
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?
Explanation
REFERENCES: Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207.
Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 8
A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.
The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts.
The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 9
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
Explanation
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail,
residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
Question 10
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb’s point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change? Review Topic
Explanation
Question 11
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 12
Figure 10 shows patellar radiographs of a 68-year-old woman who underwent bilateral total knee arthroplasty 2 months ago. Following a recent fall onto the left side, she now reports anterior pain in the left knee. A CT scan shows that the femoral and tibial components are appropriately externally rotated and radiographs show acceptable axial alignment and no evidence of loosening. What is the most appropriate treatment option?
Explanation
If the components are determined to be in satisfactory position, soft-tissue procedures can be pursued. Lateral retinacular release is usually the first soft-tissue procedure used to improve patellofemoral mechanics. In this patient, the patellar fracture fragment is so small that it can be excised. Distal realignment is not usually used as the first line of treatment for patellar maltracking following TKA.
REFERENCES: Fehring TK, Christie MJ, Lavemia C, et al: Revision total knee arthroplasty: Planning, management, and controversies. Instr Course Lect 2008;57:341-363.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
Question 13
15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature), erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin. Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Explanation
Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
Segmentally comminuted ulnar fracture
Simple diaphyseal fracture of the humerus
Transverse midshaft displaced clavicle fracture
Periprosthetic femur fracture distal to a well-fixed total hip arthroplasty
Schatzker 2 fracture of the tibia with severe joint depression and comminution
Locking screw fixation is a relatively new option in the armamentarium of orthopaedic surgeons treating fractures. The understanding of the biomechanics, implications to healing, and optimal indications and surgical techniques is still in evolution. A periprosthetic proximal femur fracture with a stable prosthesis is best treated with open reduction and internal fixation with locking proximal fixation with or without cerclage cables. Diaphyseal fractures treated with compression plating or bridge plating can be treated well with conventional implants unless osteoporosis is severe. An AO/OTA B-type partial articular fracture is also better suited to standard buttress plating with periarticular rafting lag screws. Locking fixation is not always required for a transverse displaced midshaft clavicle fracture.
What is the post-amplification product of reverse transcription polymerase chain reaction (RT-PCR)?
RNA
DNA
Protein
Mitochondria
Immunoglobulins
Reverse transcription polymerase chain reaction (RT-PCR) is a variant of polymerase chain reaction (PCR) used in molecular biology to generate many copies of a DNA sequence from fragments of RNA. The RNA strand is first reverse transcribed into its DNA complement, followed by amplification of the resulting DNA using polymerase chain reaction. Polymerase chain reaction amplifies short segments of DNA by using the temperature stable DNA polymerase enzyme.
A 63-year-old woman falls from standing and lands on her right hand. She complains of deformity and wrist pain. Radiographs are provided in Figure A. Following closed reduction, the patient inquires whether she has osteoporosis and if she is likely to have another fracture. In counselling the patient, which of the following is the strongest predictor for a future fracture from low energy trauma?
Bone mineral density T-score < -2.5
Low vitamin D levels
Family history of osteoporosis
History of a prior fragility fracture
Ten year history of oral prednisone use
Each of the answer choices is a risk factor for subsequent fragility fracture, but patient history of a prior fragility fracture is the strongest predictor.
Bouxsein et al reviews the proper care, diagnosis, and prevention of fragility fractures. History of a fragility fracture is the greatest predictor of a future fracture from low energy trauma. Appropriate care includes not only treatment of the fracture itself, but also proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology. Evaluation includes bone densitometry, lab testing of Vitamin D and calcium.
A T-score compares your bone density to the optimal peak bone density for your gender. It is reported as number of standard deviations below the average. A T-score of -1 to -2.5 is considered osteopenia, and a risk for developing osteoporosis. A T- score of less than -2.5 is diagnostic of osteoporosis.
Long-term alendronate (Fosamax) use for osteoporosis has been associated
with which of the following?
Scurvy
Detached retina
Uterine carcinoma
Osteonecrosis of the femoral head
Diaphyseal femoral insufficiency fractures
Alendronate is a bisphosphonate that inhibits the ruffled border of the osteoclast. When used long term, this class of medication prevents the normal bone remodeling process. Long-term use has recently been shown to be associated with insufficiency fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with
uterine cancer or a detached retina.
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Hepatic
Renal
Respiratory
Gastrointestinal
Polylactic acid suture and suture anchors are popular bioabsorbable orthopaedic implants. This material undergoes hydrolysis of the ester background in vivo. Resulting lactic acid enters the tricarboxylic acid (Krebs)
cycle and is excreted as carbon dioxide by the lungs. Polyglycolic acid and poly(p- dioxanone) may also be excreted by the kidneys.
A patient sustains a grade III medial collateral ligament injury. One year later, when compared to collagen in an uninjured ligament, an increase is likely in the
gross number of fibers.
proportion of type III fibers.
cross-linking.
mass and diameter of fibers.
Studies on animal models have shown that there is a change in collagen fiber type and distribution early in the healing process. There is a higher portion of type III fibers than in
normal ligament initially, but this ratio returns to normal about 1 year after the injury occurs. Healing ligaments show an increased number of collagen fibers, but the number of mature collagen cross-links is
45% of predicted value after 1 year. There is also a decrease in the mass and diameter of the collagen fibers.
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Bone morphogenetic protein (BMP)/SMAD pathway
Receptor activator of nuclear factor kappa beta (RANK)/RANK ligand (RANKL) pathway
Wnt/Beta-catenin (ß-catenin) pathway
Parathyroid hormone (PTH) pathway
Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the ß-catenin. The unphosphorylated ß-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, ß- catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/ß- catenin pathway. The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation. BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
During endochondral ossification of the growth plate, the process that most contributes to the longitudinal growth of long bones is
chondrocyte apoptosis.
chondrocyte hypertrophy.
chondrocyte proliferation.
growth plate matrix synthesis.
The growth plate is divided into 5 distinct zones: reserve, proliferative, maturation, hypertrophy, and vascular invasion. During growth-plate chondrocyte hypertrophy, intracellular volume and an increase in chondrocyte height are responsible for most growth of long bones. Other factors that contribute to bone growth are chondrocyte proliferation and matrix synthesis, but to a lesser degree than chondrocyte hypertrophy. Growth plate chondrocytes undergo programmed cell death (apoptosis) after hypertrophy
takes place.
Bacterial resistance to tetracycline is confirmed by ribosome protection, tetracycline modification, and
altered RNA polymerase.
altered membrane binding protein.
increased drug efflux.
DNA gyrase mutation.
Mutations of bacterial DNA gyrase can decrease the effectiveness of quinolones. Altered membrane-binding protein is observed with resistance to ?
-lactam antibiotics. Tetracyclines are antibiotics that inhibit bacterial growth by stopping protein synthesis. Three specific mechanisms of tetracycline
resistance have been identified: increased tetracycline efflux, ribosome protection, and tetracycline modification. Alteration of RNA polymerase is found in resistance to rifampin.
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge- shaped
vertebrae. What name is associated with this process?
Hooke's law
Kirchhoff's law
Wolff's law
Heuter-Volkmann principle
The Heuter-Volkmann principle shows that bone placed in longitudinal tension will tend to stimulate longitudinal growth, and that compressive longitudinal forces inhibit longitudinal growth, making this response the best choice. Hooke's law relates to stress being proportional to strain and is not directly related to bone growth. Kirchhoff's laws apply to electrical circuit design. Wolff's law states that bone remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
A tendon repair is thought to be weakest during which phase of tendon healing?
Inflammatory
Proliferation
Maturation
Remodeling
Healing after a tendon repair or rupture has the following stages: inflammatory, cellular proliferation, and remodeling. During the inflammatory phase, neutrophils and macrophages migrate into the injury site and release chemotactic factors that recruit fibroblasts. A tendon is thought to be weakest
5 to 21 days after repair, which coincides with the inflammatory phase. During the proliferative phase, inflammatory cells secrete cytokines and growth
factors (platelet-derived growth factor, insulin-like growth factor, bone morphogenetic protein (BMP)-12 and BMP 13, and transforming growth factor- beta) that promote differentiation of fibroblasts. Fibrosis and decreased cellularity are the hallmarks of the remodeling stage.
A 4-year-old boy has bilateral genu varum and is in the fifth percentile for height for his age. A younger sister has less severe genu varum. Radiographs reveal physeal cupping and widening on both the distal femur and proximal tibia. Laboratory studies show sodium 145 mEq/L (reference range, 136-142 mEq/L), potassium 4.0 mEq/L (reference range, 3.5-5.0 mEq/L), calcium 9.0 mg/dL (reference range, 8.2-10.2 mg/dL), phosphorous 2 mg/dL (reference range, 4-
Question 14
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
REFERENCES: Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 961-990.
Question 15
Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?
Explanation
Epidural abscesses are potentially devastating. Nonsurgical care may be chosen for select patients. A baseline failure rate of 8.3% increases based on patient risk factors, which include a history of IV drug abuse, diabetes, age older than 65, CRP level higher than 115, WBC level higher than 12.5, and Staphylococcus aureus as the causative organism. Immunosuppression and abscess size are not significant risk factors for failure of nonsurgical care. Nonsurgical care may be regarded as "failed" if there is worsening of a patient's neurologic status. When nonsurgical care fails, delayed surgery is less successful at restoring motor function (vs early surgery).
RECOMMENDED READINGS
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 16
A 12-year-old Little League pitcher reports lateral elbow pain and “catching.” Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of Review Topic

Explanation
Question 17
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
Explanation
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
Question 18
A 34-year-old woman who is a professional skier (Figure 42)
Explanation

Question 19
Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
Explanation
Question 20
When using the direct lateral (or Hardinge) approach for hip arthroplasty, three muscles are detached from the femur. In addition to the vastus lateralis, they include the
Explanation
REFERENCES: Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Hardinge K: The direct lateral approach to the hip. J Bone Joint Surg Br 1982;64:17-19.
Question 21
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 2-49.
Question 22
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
REFERENCES: Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567.
Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 23
Figure 82 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment? Review Topic

Explanation
Question 24
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of
Explanation
REFERENCES: Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Healy WL, Lo TC, DeSimone AA, et al: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Question 25
A 64-year-old woman sustains a fracture to her distal femur 5 years after undergoing total knee arthroplasty. When choosing between locked femoral plating and retrograde femoral nailing, which factor is important to consider based on this patient’s surgical record?
Explanation
Treatment of periprosthetic supracondylar femoral fractures is complex and may involve the use of a retrograde intramedullary femoral nail or locked or unlocked femoral plate. Knowledge of certain measurements specific to the model of the implant, specifically to the minimal intercondylar distance and the position of the notch on the femoral component in relation to the intramedullary canal, is crucial when choosing a retrograde nail over a locked femoral plate. Although the surgical approach, presence of an anterior femoral notch, and previous tourniquet time are interesting to consider, none of these factors would preclude the ability to proceed with femoral intramedullary nailing.

CLINICAL SITUATION FOR QUESTIONS 128 THROUGH 130
Figure 128 is the radiograph of a 78-year-old nursing home resident who has hypertension and peripheral vascular disease. He has developed acute severe hip pain 20 years after undergoing a cementless total hip arthroplasty (THA) and subsequent revision for instability. He was previously ambulatory with a walker and now can no longer ambulate. His erythrocyte sedimentation rate is 8 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein level is
Question 26
Of all the pelvic ring injury types, anteroposterior compression type III pelvic ring injuries have the highest rate of which of the following?

Explanation
Question 27
Figure 3a shows the preoperative radiograph of a 5-year-old girl who achieved complete correction with valgus osteotomies. Figure 3b shows a radiograph obtained 2 years later. What is the cause of the recurrent deformity on the right side?
Explanation
REFERENCES: Brooks WC, Gross RH: Genu varum in children: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:326-335.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
pp 840-950.
Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1068-1073.
Question 28
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
REFERENCES: American College of Surgeons Committee on Trauma. Advanced Trauma Life Support Course. Instructor’s Manual. Chicago, IL, American College of Surgeons, 1984.
Eichelberger MR, Randolph JG: Pediatric trauma: An algorithm for diagnosis and therapy. J Trauma 1983;23:91-97.
Question 29
reduced the risk of nonvertebral fractures by 35 percent at the 20-µg dose and by 40 percent at the 40-µg dose and reduced the risk of nonvertebral fragility fractures by 53 and 54 percent, respectively
Explanation
Stoffel et al review the biomechanics of locking bridge plate constructs. The working distance is the most important determinant of axial stiffness and torsional rigidity.
Decreasing the distance from the plate to the bone, using a longer plate, and increasing the number of screws used also increased stiffness.
Egol et al reviews and compares the biomechanics of locked plates and conventional nonlocked plates. Locked plates are most indicated for diaphyseal- metaphyseal junction fractures in osteoporotic bone, severely comminuted fractures, indirect fracture reduction, and fractures where anatomical constraints prevent plating on the tension side of the bone. Conventional nonlocked plates are the fixation of choice for periarticular
fractures that require anatomic reduction, and nonunions that require compression to enhance healing.
A 47-year-old man complains of long standing pain involving the right index, middle, and ring fingers. A clinical image is shown in Figure A. A radiograph is provided in Figure B. Which of the following is the most likely diagnosis?
Gout
Osteoarthritis
Rheumatoid arthritis
Septic arthritis
Psoriatic arthritis
The clinical presentation and radiograph are consistent with psoriatic arthritis. Figure A shows a swollen "sausage digit" (dactylitis) and nail pitting (onychodystrophy)characteristic of this condition. Figure B demonstrates the classic "pencil-in-cup" radiographic deformity seen in DIP arthritis, a common orthopaedic manifestation of psoriatic arthritis. Psoriatic arthritis affects 5 to
10% of patients with psoriasis of the skin. However, the spectrum of
symptoms varies greatly from mild and self-limiting to destructive arthritis. It most commonly affects the hands and feet, but can also involve the spine and sacroiliac joints. Primary treatment is medicinal with NSAIDS, methotrexate, and TNF-alpha inhibitors.
High infection rates have been reported with surgical intervention. Illustration A is an closer image depicting psoriatic onychodystrophyis. Illustration B illustrates a "pencil-in- cup" deformity.
Which of the following study designs represent a level III evidence study?
Prospective, randomized controlled trial
Retrospective case-control study
Retrospective case series
Prospective cohort study
Expert opinion
The practice of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. Therapeutic study hierarchy of evidence has been established to better analyze studies in a reproducible fashion. Level I studies include well- designed randomized controlled prospective studies (RCT). Level II include
lower quality designed prospective RCT as well as prospective cohort studies. Level III include retrospective cohort studies and case-control studies. Level IV include case series. Level V include case reports, expert opinion, and personal observation. This is summarized in illustration A. The referenced article by Brighton et al is a review of how the level of evidence has evolved and how the different levels can carry varied amounts of impact on clinical treatments and future research.
A prosthetic polycentric knee with hydraulic swing control is chosen for a very active 63-year-old transfemoral amputee. All of the following appropriately describe the features of this prosthesis EXCEPT:
Flexes in a controlled manner
Variable cadence
Ability to walk at a moderately fast pace
Knee center of rotation is fixed anterior to the line of weight bearing
Weighs more than a constant friction knee that has a manual extension locking mechanism
A polycentric knee has a variable, not fixed, center of rotation. When the center of rotation is posterior to the line of weight bearing it allows control in the stance phase, but makes flexion more difficult. However, when the center of rotation is anterior to the line of weight bearing, flexion is improved but control is sacrificed. An example of this prosthesis is shown in illustration A.
The piston mechanism in the hydraulic knee allows variable cadence by changing resistance to knee flexion. This prosthesis also flexes in a controlled manner by limiting excessive flexion and by extending earlier in the gait cycle.
The polycentric knee with hydraulic swing control is best for active patients who prefer greater utility and variability but it does weigh more than the constant-friction knee hinge that has a manual extension locking mechanism.
The review articles by Michael and Friel review the prescription options for lower extremity prostheses.
Level 1 evidence has shown vitamin C reduces the incidence of reflex sympathetic dystrophy (RSD) or complex regional pain syndrome type I (CRPS) in patients with which of the following?
Tarsal tunnel syndrome
Distal radius fractures
Carpal tunnel syndrome
Cervical radiculopathy from herniated nucleus pulposis
Ankle fractures Corrent answer: 2
Two different prospective, double-blind studies performed by the same institution have shown that vitamin C administration is associated with a lower risk of RSD (i.e CRPS) after wrist fractures. Vitamin C is thought to reduce
lipid peroxidation, scavenge free hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability.
The first trial by Zollinger was published in Lancet and included 115 adults with 119 fractures treated with conservative management. They found that RSD/CRPS occurred in four (7%) wrists in the vitamin C group (500mg daily for 50 days) and 14 (22%) in the placebo group.
The second trial by Zollinger published in JBJS included 317 adult patients sustaining 328 distal radius fractures treated conservatively. They had allocated treatment groups to 200mg, 500mg, or 1500mg vitamin C dosages
for 50 days. RSD/CRPS occurrence was 4.2% in the 200mg group, 1.8% in the 500mg group, and 1.7% in the 1500mg group and thus the 500mg dosage for
50 days was recommended at the conclusion of the study. Patients making early cast- related complaints to their provider had a higher incidence of developing RSD/CRPS.
It should also be noted that a recent double blinded randomized controlled trial by Ekrol et al found no statistical significant benefit of Vitamin C on the outcome of distal radius fractures.
Which of the following best describes the mechanism by which osteoprotegerin (OPG) plays a role in RANKL-mediated osteoclast bone resorption?
inhibits RANKL-mediated osteoclast bone resorption by directly binding to RANKL
inhibits RANKL-mediated osteoclast bone resorption by directly binding to the RANK receptor on osteoclasts
stimulates RANKL-mediated osteoclast bone resorption by directly binding to RANKL
stimulates RANKL-mediated osteoclast bone resorption by directly binding to the
RANK receptor on osteoclasts
stimulates RANKL-mediated osteoclast bone resorption by directly binding to PTH
Osteoclastic bone resorption is the final common mechanism for osteolysis, whether due to a pathologic lytic lesion, macrophage activation in particle wear, or normal remodeling. The RANKL mechanism controls the coupling of osteoblast and osteoclast activation.
RANKL is expressed from osteoblasts and bone-marrow stromal cells. When RANKL binds to the RANKL receptor (receptor/activator of NF-[kappa]B) on the cell membrane of osteoclasts) it
stimulates differentiation from osteoclast progenitor cells to mature osteoclasts. Mature osteoclasts proceed with osteoclastic bone resporption. Osteoprotegerin (OPG) acts as a decoy receptor by binding to RANKL and blocking the interaction between RANKL and the RANK-receptor and consequently inhibiting osteoclast formation and activation.
The reference by Clohisy et al reviews recent developments in our understanding of the cellular and molecular events regulating osteoclast- mediated bone resorption and discusses the role of the RANKL pathway in several disease states, including osteolysis associated with inflammatory arthritis and cancer-induced bone loss.
The reference by Goater et al studied the potential of OPG gene therapy by evaluating the ability of transfected synoviocytes expressing OPG to prevent wear debris-induced osteoclastogenesis. They found a decrease in the amount of bone resorption in mice with the transfected OPG gene. The RANKL pathway is shown in Illustration A below and further described in the linked video.
Level 1 evidence has shown Low-intensity Pulsed Ultrasound Stimulation (LIPUS) decreased the time to fracture union in all of the the following injuries EXCEPT?
Radius shaft fracture
Distal radius fracture
Tibia shaft fracture treated with casting
Tibia shaft fracture treated with reamed intramedullary nailing
Scaphoid fracture
Tibia shaft fractures treated with reamed intramedullary nailing do not have Level 1 evidence supporting adjunctive LIPUS treatment. Low-intensity pulsed ultrasound (LIPUS) "bone stimulators" deliver 30mW/cm2 pulsed-waves via an external device over the fracture site.
The meta-analysis by Busse et al found 6 randomized, controlled trials evaluating LIPUS. They concluded that low-intensity pulsed ultrasound treatment may significantly reduce the time to fracture healing for fractures treated nonoperatively.
The metanalysis cites that Emami et al found no benefit to LIPUS treatment on intramedullary fixed tibial fractures. Injuries described in the metaanalysis as having positive benefits from LIPUS include radius shaft(Cook et al), distal radius(Kristiansen et al), scaphoid(Mayr et al), and tibia treated with casting (Heckman et al).
The Level 1 study by Heckman et al of 67 patients found a significant decrease in the time to clinical healing in tibia fractures treated with casting and no serious complications with its use.
A 58-year-old Jehovah's Witness male presents with severe right hip pain due to osteoarthritis. He has failed exhaustive physical therapy, steroid injections, and activity modifications, and now wishes to proceed with a right total hip arthroplasty. During the procedure, there is profound blood loss with associated hypotension. Which of the following is generally the most preferred method for treating the patient's acute intraoperative anemia?
Iron supplementation
Subcutaneous erythropoietin administration
ABO-matched allogeneic blood transfusion
Continuous tranexamic acid infusion
Use of cell salvage
The patient has experienced a greater than expected blood loss during the procedure and has developed hemodynamic instability as a result. Given that the patient is a Jehovah's Witness, the use of a cell salvage (Cell Saver) is most preferred method for treating the patient's acute blood loss anemia.
Signficant intraoperative blood loss is a risk associated with major orthopedic procedures such as joint arthroplasty, and spine, tumor, and trauma surgeries. The most effective method of mitigating this risk is by maintaining good hemostasis during the procedure.
Tranexamic acid (TXA), cell saver, and allogeneic blood transfusion are adjunctive modalities to limit and address excessive intraoperative blood loss. Patients who are Jehovah's Witnesses are generally not amenable to allogeneic blood transfusions but can often be transfused with their own blood. The use of intraoperative cell saver allows for the recycling of the patient's own blood that is obtained with suction, and this can then be used later to transfuse the patient. However, this should be discussed with the patient pre- operatively, as some Jehovah's witnesses may be amenable to allogenic blood transfusion or conversely be opposed to cell saver.
Moonen et al. reviewed perioperative blood management in elective orthopedic surgery procedures. The authors stated that the gold standard for preventing intraoperative blood loss was by maintaining adequate hemostasis and dissecting through anatomically correct tissue planes. They proposed the use
of pre-operative erythropoietin and iron supplementation, pre-operative autologous blood donation, platelet-rich plasmapheresis, hypotensive epidural anesthesia, and intra- operative cell saving as adjunctive blood loss management modalities. The authors concluded that allogenic blood transfusion should be based on physiologic variables, risks of disease transmission, and patient preference.
Imai et al. performed a retrospective study of intraoperative and postoperative blood loss in patients undergoing primary total hip arthroplasty that were treated with either a control or TXA at various time points in the perioperative period. They found that patients who received TXA either 10 minutes prior to surgery or 6 hours after the original dose had a significant decrease in periopreative blood loss. Postoperative blood loss was significantly decreased
in all patients that received TXA. The authors concluded that TXA is an effective adjunct for minimizing blood loss during arthroplasty procedures.
Incorrect Answers:
According to the 2008 National Osteoporosis Foundation Guidelines for Pharmacologic Treatment of Osteoporosis, when are bisphosphonates indicated for the treatment or prevention of osteoporosis?
DEXA T-score between -1.0 and -2.5
FRAX calculated 10-year hip fracture risk of >3%
FRAX calculated 10-year risk of major osteoporosis-related fracture of
>10%
The 2008 National Osteoporosis Foundation Guidelines for Pharmacologic Treatment of Osteoporosis suggests that pharmacologic treatment should be considered for a DEXA T-score between -1.0 and -2.5 at the femoral neck/spine AND 10-year risk of hip fracture ≥ 3%.
Osteoporosis affects more than 12 million Americans per year, with the burden falling heaviest on postmenopausal women. Because of decreased bone strength, patients with osteoporosis are susceptible to fragility fractures. With no additional risk factors, a 65- year-old Caucasian woman has an estimated
10% 10-year risk of a fragility fracture. FRAX (World Health Organization Fracture Risk Assessment Tool) calculates 10-year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility
fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. discussed the utility of the FRAX tool as an assessment modality for prediction of fracture risk. The authors advocated for treatment with osteopenia (T-score of
-1.0 to -2.5) combined with either a ten-year risk of hip fracture >= 3% or a ten-year risk of major osteoporosis-related fracture
of >= 20% as calculated by FRAX. They also discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive therapy and may help identify patients at high risk for fracture.
Cosman et al. review the 2008 National Osteoporosis Foundation guidelines and support that pharmacologic treatment for osteoporosis should be considered if patients are postmenopausal women or men > 50 years of age AND meet one of the following criteria: have a prior hip or vertebral fracture, a T score -2.5 or less at the femoral neck or spine, OR a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture
greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%. They conclude that DEXA scans should be repeated every 1-2 years if patients are undergoing pharmacologic treatment.
Gass et al. review the epidemiology and tiered management strategy for osteoporosis. They discuss the first line prevention, treatment of secondary causes of osteoporosis, and finally pharmacologic interventions, all in an effort to mitigate fracture risk and the burden that osteoporotic fractures on the health care system.
Illustrations:
Illustration A outlines the variables taken into account in the FRAX score calculator.
Incorrect answers:
ADDITIONALLY has either a ten-year risk of hip fracture >= 3% or a ten-year risk of major osteoporosis-related fracture of >= 20% (or both) as calculated by the FRAX tool.
>20% as calculated by the FRAX tool in order to meet the criterion set forth in the 2008 National Osteoporosis Foundation guidelines. Combined with documented osteopenia (T- score of -1.0 to -2.5), bisphosphonate therapy would be indicated.
>20% as calculated by the FRAX tool in order to meet the criterion set forth in the 2008 National Osteoporosis Foundation guidelines.
Which of the following bone graft substitutes has the fastest resorption characteristics?
Calcium sulfate
Tricalcium phosphate
Hydroxyapatite
Fibular allograft
Cortical iliac crest autograft
Of the three bone graft substitutes listed (calcium sulfate, tricalcium phosphate, and hydroxyapatite), calcium sulfate has the fastest resorption characteristics. Fibular allograft and cortical iliac crest autograft are not considered bone graft substitutes.
Calcium sulfate, tricalcium phosphate, and hydroxyapatite are all "osteoconductive" bone graft substitutes, meaning that these implants provide a surface and structure that facilitates the attachment, migration, proliferation, differentiation and survival of osteogenic stem and progenitor cells. Each has different chemical, macro- and microstructural properties. Calcium sulfate (plaster of Paris) is a low-molecular weight soluble compound that must be implanted adjacent to viable periosteum to work. It is reabsorbed by a
process of dissolution over a period of 5-7 weeks.
Jamali, et al., found that calcium sulphate was completely reabsorbed by 6 weeks. Tricalcium phosphate has compressive strength similar to cancellous bone, but is brittle and weak under tension and shear. It undergoes reabsorbtion via dissolution and fragmentation over 6-18 months; unfortunately less bone volume is produced than tricalcium phosphate absorbed. For this reason, it is used clinically as an adjunct with other less
absorbable substitutes.
Moore et al discuss that hydroxyapatite forms the principle mineral content of bone. Synthetically, it is available in ceramic and non-ceramic forms as porous or solid, blocks or granules. HA has good compressive strength, but is weak in tension and shear and brittle making it fracture-prone in shock loading. Ceramic HA preparations are resistant to absorption in vivo, which occurs at 1-
2% per year. Non-ceramic HA is more readily absorbed.
Which of the following techniques increases strength and stability to an external fixation construct?
Unicortical pin fixation
Decreasing total pin separation distance
Increased working distance from the pin to fracture site
Decreasing the distance between the bone and the construct
Using smaller diameter pins
There are several methods that can be used to increase the strength of an external fixation construct. Decreasing the distance from the bar to the bone increases stability and strengthens the construct. Some other methods to increase stability include: good bone- to-bone fracture end apposition, using an increased number of pins, using larger pins, small distance from the near pins to the fracture site (smaller working distance), increased spacing between the near and far pins, and bicortical pin fixation.
Tencer et al looked at biomechanical aspects of external fixation systems. They demonstrated that system rigidity could be increased by maximizing pin separation distance in the fracture component and the number of pins used while minimizing pin separation distance across the fracture site and the sidebar offset distance from bone.
Incorrect Answers: Answer choices 1,2,3, and 5 all act to decrease external fixation construct strength.
A 62-year-old woman with Paget’s disease is started on a non- nitrogen containing bisphosphonate for treatment of her condition.
What is the mechanism of action of this drug?
Inhibition of farnesyl diphosphate synthase
Conversion of drug into a non-functioning ATP-analogue
Interference of isoprenylation of small GTPases
Inhibition of geranylgeranyl diphosphate synthase (GGPPS)
Downregulation of the undecaprenyl diphosphate synthase (UPPS) pathway
Bisphosphonates are a class of antiresorptive agents used to treat diseases characterized by osteoclast-mediated bone resorption. Non-nitrogen containing bisphosphonates (such as etidronate) are metabolized into non-functioning
ATP analogues which cause eventual osteoclast apoptosis. Nitrogen containing bisphsphonates (alendrolate/Fosamax and Zoledronic acid/Zometa) act by inhibiting farnesyl diphosphate synthase (FPPS), resulting in decreased prenylation of small GTPases.
Reszka et al reviewed nitrogen containing bisphosphonates. They outlined the mechanism of action on farnesyl diphosphate synthase in the cholesterol biosynthesis pathway.
Guo et al also reviewed the mechanism of nitrogen-containing bisphosphonates. In addition to showing the decrease in prenylation of GTPase, they were shown to inhibit geranylgeranyl diphosphate synthase (GGPPS), as well as undecaprenyl diphosphate synthase (UPPS).
Morris et al reviewed the bisphosphonates currently approved by the FDA. They outlined their use in the treatment of Paget disease, metastatic bone disease and widening applications in OI and fibrous dysplasia.
Incorrect answers:
1,3,4,5: Mechanism of nitrogen-containing bisphosphonates.
A 58-year-old female falls and sustains the injury shown in Figures A and B. Following surgical treatment of the fracture, which of the following is the most appropriate additional investigation?
MRI of the pelvis
Urine electrophoresis
CT scan of the pelvis
Bone scan
DEXA scan
Figures A and B depicts a femoral neck fracture. Medical management of postmenopausal women with fragility fractures (distal radius, femoral neck, vertebral compression fractures) includes dual-energy x-ray absorptiometry (DEXA) testing.
Following the diagnosis of osteoporosis, bisphosphonates, calcitonin or other medical treatments may be initiated.
Oyen et al examined 1794 patients with fractures of the distal radius. As one- third of the men and half of the women had bone mineral density (BMD) suggesting osteoporosis, they concluded that all patients aged 50 or above should have bone densitometry testing.
Freedman et al reviewed 1162 women with distal radius fractures. They determined that the rate of diagnostic workup and medical treatment decreases as patient age increases at the time of fracture.
A 52-year old woman who is not on any hormone replacement therapy (HRT) falls from standing height and sustains the injury seen in Figure A. Review of her medical history reveals that she carries a diagnosis of osteoporosis, and that her latest T-score was -3.0. How much calcium should she have been consuming on a daily basis prior to sustaining her injury?
Question 30
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month followup appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis? Review Topic

Explanation
(SBQ12TR.54) A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?

Varus malunion
Nonunion
Valgus malunion
Malrotation
Superficial peroneal nerve injury
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Varus malunion is more likely to occur in midshaft tibia fractures with an intact fibula.
Nonunion after a proximal tibial fracture treated with intramedullary nailing is less common than malunion.
Malrotation occurs most commonly after IM nailing of fractures through the distal third of the tibia.
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.
Question 31
The patient is planning on having his contralateral knee replaced as well. He has a mild valgus deformity in his left knee with an overall windswept deformity. Which release is most appropriate in this case if the knee remains tight in extension?
Explanation
Balancing a total knee is important for longevity of the device and functional benefit. The surgeon should be systematic in the release of a varus knee. The deep MCL is typically released as part of the approach and osteophytes are then removed. The semimembranosus tendon can then be released from the posterior medial aspect of the tibia. A downsizing osteotomy can be considered for a large deformity if a patient has adequate tibial sizing. If a patient has the smallest implant available prior to the osteotomy, an osteotomy will lead to overhang of the implant and medial impingement on the MCL.
A valgus knee can be treated with pie crusting of the iliotibial band in mild extension deformity. Surgeons should pause prior to taking down the popliteus and lateral collateral
ligament because this can induce posterior rotatory subluxation of a primary knee, especially in the case of a posterior collateral ligament-sacrificing total knee arthroplasty design.

Question 32
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 33
A 78-year-old man has a history of worsening bilateral calf pain with activity. MRI scans are shown in Figures 31a through 31d. His symptoms are not improved with forward flexion of the lumbar spine. His lower extremity pain is relieved when he sits or ceases activity. Which of the following tests would be most helpful in establishing a diagnosis? Review Topic
Explanation
Decreased range of motion and hip joint pain, especially in internal rotation and abduction, are common findings in patients with degenerative arthritis of the hip. While post-myelography CT has been found superior to MRI as a single study for the preoperative planning of decompression for lumbar spinal stenosis, it will not assist in differentiating vascular from neurogenic claudication.
Question 34
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder “slip out” when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management? Review Topic

Explanation
Question 35
A 6-month-old child has the deformity seen in Figure 10. There are no other known associated problems. What is the etiology of this condition? Review Topic

Explanation
Question 36
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?
Explanation
REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179.
Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Aminian A, Schoenecker PL: Premature closure of the distal radial physis after fracture of the distal radial metaphysis. J Pediatr Orthop 1995;15:495-498.
Question 37
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?

Explanation
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Incorrect Answers: Choices 1-4 are not as predictive of mortality as choice 5.
Question 38
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
REFERENCES: Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.
Question 39
Treatment should now include
Explanation
Extensive laminectomy in patients with degenerative spondylolisthesis does result in postoperative instability. In the study by White and Wiltse, further subluxation did occur in 66 percent of patients who were operated on for degenerative spondylolisthesis , whereas it was observed in only 2 percent of the spondylolisthesis or disc patients who did not have
spondylolisthesis postoperatively. The extent of decompression and facet removal must be limited in the patient with degenerative spondylolisthesis or a fusion of the transverse processes included as part of the treatment. Internal fixation devices have been used in these circumstances to prevent further subluxation while the fusion is consolidating. Wiltse outlined some guidelines for spinal fusion in spinal stenosis: (1) the patient who is less than sixty years old and had degenerative spondylolisthesis with a total loss of posterior stability due to removal of the articular processes (a one-level fusion of the transverse processes); (2) the patient who is less than fifty-five and had a midline decompression for degenerative spondylolisthesis with facet preservation; and
(3) the patient who is less than fifty years old with isthmic spondylolisthesis, if the posterior elements have been removed. Simple degenerative spinal stenosis seldom requires a fusion, even if all posterior stability has been lost. The problem with obtaining a successful spinal fusion is real and conditions are less than optimum in these instances.
Question 40
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
REFERENCES: Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 1831-1835.
Question 41
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 62-67.
Question 42
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of
Explanation
REFERENCES: Boileau P, Brassart N, Watkinson DJ, et al: Arthroscopic repair of full-thickness tears of the supraspinatus: Does the tendon really heal? J Bone Joint Surg Am 2005;87:1229-1240.
Jost B, Zumstein M, Pfirrmann CWA, et al: Long-term outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2006;88:472-479.
Fuchs B, Gilbart MK, Hodler J, et al: Clinical and structural results of open repair of an isolated one-tendon tear of the rotator cuff. J Bone Joint Surg Am 2006;88:309-316.
Question 43
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 44
Acetabular reconstruction followed by external beam irradiation The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. The most likely diagnosis based upon the radiographs would be:
Question 45
Articular cartilage is divided in zones with specific arrangements of the collagen framework and proteoglycan content. The superficial zone is characterized by collagen oriented
Explanation
Question 46
Which of the following is not a cause of childhood osteomalacia (rickets)?
Explanation
Question 47
What is the primary advantage of two incisions compared to one for open reduction internal fixation of a both bones forearm fracture?

Explanation
Question 48
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?
Explanation
REFERENCE: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 265-266.
Question 49
The patient fails nonsurgical treatment for this condition. What is the best next step?
Explanation
Osgood-Schlatter disease is an apophysitis of the tibial tubercle. This condition is present in males more than females and occurs prior to fusion of the tubercle to the epiphysis of the tibia. The apophysis is cartilaginous before 11 years of age and begins to ossify between 11 and 14 years of age. The apophysis fuses to the epiphysis between 14 and 18 years of age (females before males). Symptoms are pain and swelling, and pain is worse with jumping and running. Initial treatment should consist of activity limitation, ice, quadriceps and hamstring stretching, and possible bracing. NSAIDs may be used to control symptoms. When symptoms resolve, the athlete may return to activities. In fewer than 10% of cases, symptoms persist after skeletal maturity. For these patients, excision of the ossicle will usually resolve symptoms. The ossicle is usually not part of the tendon attachment and can be resected without detaching any of the patellar tendon.
RECOMMENDED READINGS
Vergara-Amador E, Davalos Herrera D, Moreno LÁ. Radiographic features of the development of the anterior tibial tuberosity. Radiologia. 2016 Feb 22. pii: S0033-8338(16)00019-9. doi: 10.1016/j.rx.2016.01.005. [Epub ahead of print] English, Spanish. PubMed PMID: 26917430. View Abstract at PubMed
Frank JB, Jarit GJ, Bravman JT, Rosen JE. Lower extremity injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2007 Jun;15(6):356-66. Review. PubMed PMID: 17548885. View Abstract at PubMed
Question 50
Anterior penetration of an iliosacral screw through the sacral ala would most likely lead to weakness of which of the following movements?

Explanation
The referenced study by Routt et al reviewed 177 patients with pelvic ring injuries treated with these screws and found that quality triplanar imaging decreased intraoperative and postoperative complications. They also recommend supplemental fixation of iliosacral screws with posterior plating in noncompliant patients.
Question 51
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
REFERENCES: Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 52
Figures 1 through 3 are the clinical photograph and radiographs of a 25-year-old, left-hand-dominant man who injured his left index finger. Which treatment option will most effectively allow satisfactory fracture alignment and maximize motion?

Explanation
This patient has an oblique index proximal phalanx fracture with malrotation. Buddy-taping and digital splinting would not predictably maintain fracture reduction and would result in a malunion with rotational deformity and possible shortening. Closed reduction and spanning external fixation in extension would result in significant digital stiffness. ORIF (Figures 4 and 5) followed by an early ROM program would allow anatomic fracture alignment and give this patient the best chance to regain the majority of motion in the shortest amount of time.


Question 53
A 77-year-old man with diabetes mellitus has had a nonhealing Wagner grade I ulcer under the medial sesamoid for the past 3 months. He smokes tobacco regularly. He has undergone several debridements and total contact casting. Examination reveals no palpable pulses. He has no erythema or purulence, and he is afebrile. Radiographs reveal no abnormalities. What is the best initial diagnostic test to help determine why the ulcer has failed to heal?
Explanation
REFERENCE: Brodsky JW: Evaluation of the diabetic foot. Instr Course Lect 1999;48:289-303.
Question 54
What is the most common complication following surgery for a "terrible triad" elbow fracture-dislocation?
Explanation
Question 55
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 56
What zone of the physis is widened in rickets?
Explanation
REFERENCES: Hunziker EB, Schenk RK, Cruz-Orive LM: Quantitation of chondrocyte performance in growth-plate cartilage during longitudinal bone growth. J Bone Joint Surg Am 1987;69:162-173.
Iannotti JP: Growth plate physiology and pathology. Orthop Clin North Am 1990;21:1-17.
Question 57
A 72-year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 58
What cell type causes the bone destruction in metastatic lesions?
Explanation
REFERENCES: Cramer SF, Fried L, Carter KJ: The cellular basis of metastatic bone disease in patients with lung cancer. Cancer 1981;48:2649-2660.
Clohisy DR, Palkert D, Ramnaraine ML, Pekurovsky I, Oursler MJ: Human breast cancer induces osteoclast activation and increases the number of osteoclasts at sites of tumor osteolysis. J Orthop Res 1996;14:396-402.
Question 59
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
REFERENCES: Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998,
pp 235-238.
Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262.
Question 60
Which of the following terms describe a rehabilitative exercise in which the foot is mobile and the motion of the knee is independent of hip and ankle motion?
Explanation
Question 61
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
Question 62
Passive glycation of articular cartilage results in
Explanation
REFERENCES: DeGroot J, Verzijl N, Wenting-van Wijk MJ, et al: Accumulation of advanced glycation end products as a molecular mechanism for aging as a risk factor in osteoarthritis. Arthritis Rheum 2004;50:1207-1215.
Chen AC, Temple MM, Ng DM, et al: Induction of advanced glycation end products and alterations of the tensile properties of articular cartilage. Arthritis Rheum 2002;46:3212-3217.
Question 63
What is the most common primary malignant tumor of bone in childhood?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 226.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 64
A 39-year-old male falls off his bicycle and complains of neck pain and tingling in his fingers. Trauma series radiographs are seen in Figures A and B. Which of the following is likely to be true? Review Topic

Explanation
Cervical spine fractures are not uncommon in ankylosing spondylitis because of osteoporosis and the long lever arm from fused vertebrae. They commonly occur because of hyperextension of the cervical spine (usually C5-7) and have a high rate of neurologic injury. AS fractures have a higher rate of neurologic injury than DISH fractures. Posterior decompression and stabilization with long constructs is necessary
Whang et al. reviewed spine injuries in 12 patients with AS and 18 patients with DISH. Most injuries involved C5-C7. Patients with AS were more likely to have severe neurologic injury (41% ASIA A) than DISH (44% ASIA E). There was 81% good-excellent outcome and 4 deaths related to halo vest use.
Caron et al. reviewed spine fractures in patients with ankylosing spine disorders (AS and DISH). AS patients were younger than DISH patients. Spinal cord injury was present in 58%. Surgery was performed on 67% and comprised instrumentation 3 levels above/below the injury. Mortality correlated with age. Mortality was 32%.
Westerveld et al. performed a systematic review on spine injuries in ankylosing spinal disorders. Most patients had sustained low energy trauma (fall from sitting/standing). In DISH, most fractures were through the vertebral body. In AS, vertebral body fractures equaled those through the disc. Surgery was performed for neurological deterioration, unstable fracture and the presence of an epidural hematoma.
Figure A shows a hyperextension injury at C6-7 (Type I, disc or Type IV,anterior disc, posterior body) cervical spine fracture in ankylosis spondylitis. Visible radiographic characteristics include osteopenia, bamboo spine, marginal syndesmophytes and ossfication of the disc space. Figure B is a chest radiograph showing thoracic syndesmophytes consistent with ankylosing spondylitis. Figure C shows bilateral sacroilitis and hip joint space narrowing typical of ankylosing spondylitis. Illustration A shows the Caron classification of spine fractures in ankylosing spondylitis (Type A, disc injury; Type B, body injury; Type C, anterior body, posterior disc injury; Type D, anterior disc, posterior body injury). Illustration B shows the difference between the marginal osteophytes of AS and nonmarginal osteophytes of DISH in the cervical spine. If you have osteophytes that are building up, and project out anterior to the anterior cortex of the vertebral bodies, like "flowing wax" it is DISH.
Incorrect Answers:
1:
This
is
characteristic
of
Klippel-Feil
syndrome
Question 65
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 66
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of
Explanation
REFERENCE: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 67
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?
Explanation
REFERENCES: Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 68
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 69
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of “weeping” serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
REFERENCE: Killewich LA, Bedford GR, Black KW, et al: Diagnosis of deep venous thrombosis: A prospective study comparing duplex scanning to contrast venography.
Circulation 1989;79:810.
Question 70
A 12-year-old girl has bilateral developmentally dislocated hips. History reveals no previous treatment, and she reports no discomfort. Good long-term clinical results are most likely to occur with
Explanation
REFERENCES: Weinstein SL: Natural history of congenital hip dislocation (CDH) and hip dysplasia. Clin Orthop 1987;225:62-76.
Wedge JH, Wasylenko MJ: The natural history of congenital dislocation of the hip: A critical review. Clin Orthop 1978;137:154-162.
Question 71
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient? Review Topic

Explanation
Question 72
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T 1 -weighted, sagittal T 2 -weighted, axial T 1 -weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 4241-4252.
Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:1-11.
Question 73
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?
Explanation
REFERENCES: Clarke HD, Schwartz JB, Math KR, et al: Anatomic risk of peroneal nerve injury with the “pie crust” technique for valgus release in total knee arthroplasty. J Arthroplasty 2004;19:40-44.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-52, 4-53.
Question 74
Figure 61 shows the current radiograph of a 69-year-old woman who fell getting out of bed 10 months ago. At the time of injury she was diagnosed with a nondisplaced humeral surgical neck fracture. After 2 weeks of sling immobilization, physical therapy was started for range of motion. She continues to have pain and is unable to elevate her arm. What is the most likely diagnosis?

Explanation
(SBQ12TR.96) Interleukin-6 levels have been shown to be a reliable measure of which of the following?
Osteoporosis
Severity of injury
Sarcomatous tumor burden
Bone turnover
Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production. Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
Question 75
Figures 15a through 15d
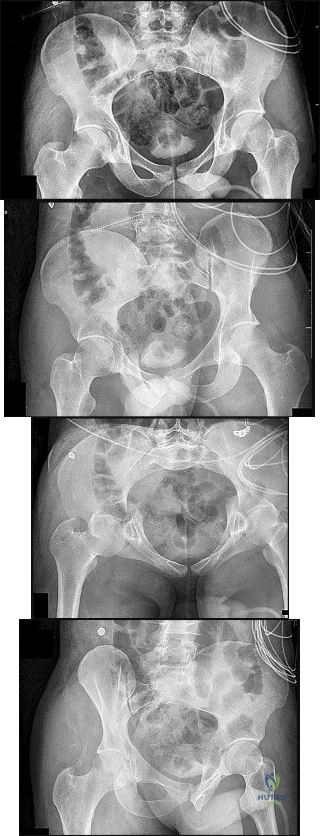
Explanation
Plain radiographic imaging of a patient with an acetabular injury begins with 5 standard views of the pelvis (anteroposterior [AP], iliac oblique, obturator oblique, inlet, and outlet views). These views will show fractures of the acetabulum and help to evaluate for pelvic fractures and hip joint integrity. The obturator oblique view is taken with the injured side rotated 45 degrees forward with the beam centered on the patient’s affected hip. This shows the anterior column and posterior wall and will reveal if any posterior subluxation of the hip is present. The iliac oblique view is taken with the injured side of the patient rolled 45 degrees forward with the beam centered on the affected hip. This shows the posterior column and the anterior wall. Inlet and outlet pelvic radiographs may depict pelvic injuries such as sacroiliac joint fracture or widening.
Judet and Letournel have a classification system for acetabular fractures. The system consists of 5 elementary fracture patterns: anterior wall, anterior column, posterior wall, and posterior column fractures of the acetabulum and a transverse pattern. There are also 5 associated fracture patterns: posterior column/posterior wall, transverse/posterior wall, T-type, anterior column with hemitransverse fracture of the posterior column, and both-column fractures.
Figure 12b shows a fracture of the posterior column on the Iliac oblique, and Figure 12c shows a fracture of the posterior wall in the obturator oblique.
In Question 13, the figures only reveal a fracture of the posterior wall, and this is best appreciated in Figure 13c, the obturator oblique view.
The T-type fracture is a transverse fracture with a secondary fracture line extending inferiorly. This causes the anterior and posterior columns to be separated. The iliac oblique view, Figure 14b, shows a fracture extending through the posterior column. In the obturator oblique view (Figure 14c), the yellow arrow shows a fracture extending through the anterior column, and the red arrow shows a fracture extending inferiorly through the ischium.
Fractures extending through the anterior and posterior columns are seen, which represent a transverse fracture, but there is no extension inferiorly, which eliminates T-type as a possible correct response. The anterior column fracture is best seen on the inlet view (Figure 15b), but it also can be seen in Figure 15d, the obturator oblique view. Figure 15c shows the fracture through the posterior column. For this patient, a small fracture of the posterior wall is visualized on the AP view (Figure 15a).
RECOMMENDED READINGS
Dickson KF, Dowling RM. Treatment of pelvic and acetabular fractures in elderly patients. Orthopaedic Knowledge Online Journal. Volume 11, Number 8 August 2013.
Tornetta P 3rd. Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28. Review. PubMed PMID: 11174160. View Abstract at PubMed
Moed BR, Kregor PJ, Reilly MC, Stover MD, Vrahas MS. Current management of posterior wall fractures of the acetabulum. Instr Course Lect. 2015;64:139-59. Review. PubMed PMID: 25745901. View Abstract at PubMed
Question 76
Which of the following statements is true regarding the posterior oblique portion of the medial collateral ligament of the elbow? Review Topic
Explanation
The medial ulnar collateral ligament is one of the primary static stabilizers of the elbow and is composed of three parts: anterior, posterior and transverse. The MCL provides resistance to valgus and distractive stresses. The anterior oblique fibers (of the anterior bundle) are the most important against valgus stresses. The posterior bundle is involved elbow contractures and releasing it can yield significant flexion gains, without creating valgus instability.
Morrey et al. performed a pilot study on 4 specimens and found the valgus stability is equally divided among the medial collateral ligament complex, anterior capsule, and bony articulation in full extension; whereas, at 90 degrees of flexion the contribution of the anterior capsule is assumed by the medial collateral ligament which provides approximately 55% of the stabilizing contribution to valgus stress.
Regan et al. was a subsequent study by the same group that found the posterior medial collateral ligament (PMCL) was taut only when the elbow was in a flexed position. Among the collateral ligaments, the anterior (AMCL) was the strongest and stiffest. (Of note, using present terminology these would be referred to as posterior oblique and anterior oblique portions of the medial ulnar collateral complex).
Wada et al. reported a series of open medial releases for post-traumatic elbow contracture and found scarring on the posterior oblique bundle in all cases. Large increases in flexion were achieved by releasing this structure and the capsule without the need for a lateral incision in most cases.
Illustrations A and B show the posterior oblique portion of the medial collateral ligament. Illustration C shows the most recent terminology and identifies the area to be resected for stiffness.
Incorrect Answers:
Question 77
Antegrade femoral nailing has an increased rate of which of the following when compared to retrograde femoral nailing?

Explanation
was significantly greater in the retrograde group. The referenced study by Winquist et al noted a 99.1% union rate with intramedullary nailing. The referenced study by Moed et al noted a 6% nonunion rate in non-reamed retrograde femoral nailing with nail dynamization at 6-12 weeks and early weightbearing.
Question 78
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?

Explanation
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability between both groups.
Question 79
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment? Review Topic
Explanation
Question 80
A 15-year-old right-handed pitcher reports shoulder pain after throwing. His symptoms have been present for 3 months and have been getting progressively worse. Clinical examination shows no atrophy of the shoulder muscles, but he has pain with resisted motion of the shoulder, especially internal rotation. Radiographs are shown in Figures 73a and 73b. What is the next step in the evaluation and treatment of his shoulder pain? Review Topic

Explanation
Question 81
Closed reduction and functional bracing would lead to significant upper extremity disability due to malunion.
Explanation
The referenced review article by Michelson covers rotational ankle fractures, with a review of the diagnosis, treatment options, and patient outcomes. He notes that unstable fractures (bimalleolar, bimalleolar equivalent, etc.) usually are managed with open reduction and internal fixation for optimal outcomes.
Incorrect answers:
Figure B shows a Weber C (high fibular) ankle fracture, PER, without any evidence of a medial malleolar fracture.
Figures C (SER IV), D (PER IV), and E (isloated medial malleolar fracture) all show fractures not suitable for screw fixation of the medial malleolus parallel to the joint since their fracture lines are not vertical.
OrthoCash 2020
Which of the following is an advantage of using blocking screws for tibial nailing?
Decrease risk of nail breakage
Eliminate use of interlocking screws
Allow for larger nail use
Enhance construct stiffness
Decrease torsional rigidity Corrent answer: 4
Blocking screws can be used to help obtain and maintain reductions, increase construct stiffness, and neutralize translational forces. There are no studies as of yet that find a blocking screw to decrease nail failure.
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased
rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
OrthoCash 2020
Following operative repair of lower extremity long bone and periarticular fractures, what is the time frame for patients to return to normal automobile braking time?
6 weeks after initiation of weight bearing
4 weeks postoperatively
8 weeks from the date of injury
Once full range of motion of the ankle and knee exist
At the time of bony union Corrent answer: 1
According to the first referenced study by Egol et al, appropriate braking time returns at a point 6 weeks after initiation of weightbearing after treatment of lower extremity long bone and periarticular fractures, as examined with a driving simulator. No differences were seen in return of braking time between periarticular fractures and long bone injuries.
The second reference by Egol studied only operatively treated ankle fractures and found that time to appropriate braking returns at 9 weeks postoperatively. Interestingly, no significant association was found between the functional scores and normalization of total braking time.
OrthoCash 2020
A 42-year-old male sustains the injury seen in figure A. What negative sequelae would occur with displacement of this fracture in the characteristic fashion?

Post-traumatic subtalar arthrosis
Stress fracture of the fibula
Reflex sympathetic dystrophy
Achilles tendon rupture
Posterior skin necrosis Corrent answer: 5
The radiograph shows a tongue-type calcaneus fracture, with major displacement of the posterior calcaneal body/tuberosity. The Achilles tendon insertion here causes characteristic proximal and posterior displacement, and with increasing displacement, posterior skin necrosis can be caused in a short period. Per the references, this should be treated urgently to prevent this sequelae. Lag screw fixation is appropriate for this fracture pattern, placed perpendicular to the fracture.
OrthoCash 2020
A 34-year-old male falls 10 feet from a balcony and is brought to the emergency room with the deformity seen in Figure A. Radiographs shown are shown in Figure B and C. Which of the following structures can block closed reduction of this injury pattern?

Flexor hallucis longus tendon
Extensor digitorum brevis muscle
Posterior tibial tendon
Tibialis anterior tendon
Plantar fascia
Figures A through C show a medial subtalar dislocation. Irreducible dislocations are typically the result of either inadequate sedation or interposed soft tissue structures.
In medial dislocations, the extensor digitorum brevis, the deep peroneal neurovascular bundle, or the joint capsule may block a closed reduction. In lateral dislocations, the most common structure implicated as a block to reduction is the posterior tibial tendon, although the flexor digitorum longs, posterior tibial neurovascular bundle or flexor hallucis may also block reduction.
Bibbo et al found that subtalar dislocations were irreducible 32% of the time and that 88% had ipsilateral foot and ankle injuries. At follow up, 89% of patients demonstrated radiographic changes of the subtalar joint, and had worse function on the side of the subtalar dislocation as demonstrated by lower
AOFAS scores.
Incorrect Answers:
OrthoCash 2020
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?
Non-displaced distal radius fracture
Non-displaced Rolando fracture
Second metacarpal base fracture
Boxer's fracture
Non-displaced radial styloid fracture Corrent answer: 1
Rupture of the extensor pollicis longus (EPL) tendon after non operative treatment for a distal radius fracture occurs with a 0.3-5% incidence. The causes of EPL rupture include mechanical irritation, attrition, and vascular impairment leading to delayed rupture. Synovitis of the extensor carpi radialis due to repetitive use may invade the EPL tendon and lead to rupture.
Recommended treatment in the pre-rupture setting includes a third dorsal compartment release with or without an extensor retinacular patch graft. Palmaris longus graft or a transfer from the extensor indicis proprius to the EPL tendon are reasonable treatment options. Results of all treatments seem to be clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
OrthoCash 2020
A 79-year-old cyclist is involved in an accident and sustains a displaced femoral neck fracture as seen in Figure A. What is the
optimal treatment?

Open reduction internal fixation
Bipolar hemiarthroplasty
Unipolar hemiarthroplasty
Total hip arthoplasty
Nonoperative treatment
An AP pelvis radiographs with a displaced femoral neck fracture is seen in Figure A. It important to note that degenerative changes are seen on this image. Both references suggest that elderly active individuals should be treated with a primary total hip after displaced femoral neck fractures.
In the first study by Blomfeldt et al, the group reviewed a series of patients who underwent either an acute primary total hip arthroplasty for a femoral neck fracture or a delayed primary hip after an attempt at ORIF. They found that the group treated with an acute primary total hip arthroplasty had better Harris hip and quality of life scores.
The second reference from Blomfeldt et al, studies a population of active elderly patients randomized to either a total hip arthroplasty or bipolar for femoral neck fractures. The group found no mortality or dislocation difference between the groups, but higher Harris hip scores at 1 year in patients treated with a total hip
arthroplasty.
OrthoCash 2020
A 53-year-old man sustains the injury seen in figure A and later undergoes open reduction and internal fixation. What variable will
most significantly increase his rate of degenerative arthritis in the long-term?

Postoperative joint stepoff
Alteration of limb mechanical axis
Fracture type
Male sex
Age greater than 50
Maintenance of mechanical axis correlates most with a satisfactory clinical outcome when managing an intra-articular fracture of the proximal tibia.
According to the study of plateau fractures with up to 27 year follow-up by Rademakers et al, malalignment of the limb by greater than 5 degrees tripled the rate of degenerative osteoarthritis (27% v. 9%). Age at time of injury had no effect on outcome; 31% had joint space narrowing but 64% of those knees were well tolerated.
Weigel and Marsh's study looked at high energy plateau fractures treated with staged external fixation followed by internal fixation, and noted a low rate of severe arthrosis even with mild to moderate joint incongruity.
Stevens et al noted a worse outcome with increasing age at presentation with these injuries; fracture type had a small influence and adequacy of reduction had no significant influence on outcome.
Figure A is a coronal CT image showing a lateral tibial plateau fracture with significant joint depression.
OrthoCash 2020
A 69-year-old male sustained a proximal humerus fracture that underwent open reduction and internal fixation nine months ago. He complains of constant pain and weakness; repeat radiographs are shown in Figures A and B. What is the most appropriate surgical treatment at this time?
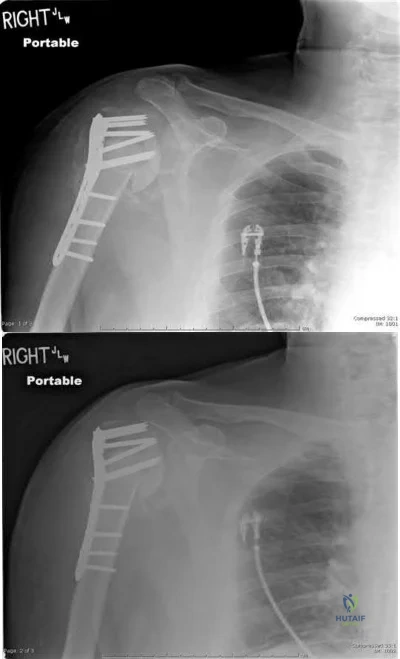
Revision open reduction and internal fixation
Valgus corrective osteotomy of proximal humerus
Shoulder arthroplasty
Shoulder arthrodesis
Humeral head resection Corrent answer: 3
Figures A and B show loss of fixation of a proximal humerus fracture. The most appropriate treatment for this scenario is a humeral arthroplasty, as the tenuous blood supply of the proximal humerus is likely chronically disrupted, leading to osteonecrosis and poor healing potential of the proximal humerus.
Traditionally, hemiarthroplasty was performed for these presentations, but reverse total shoulder arthroplasty has emerged as a potentially better
treatment method, especially if the rotator cuff function/status is unknown or poor.
According to the referenced article by Norris et al, delayed shoulder hemiarthroplasty decreased shoulder pain in 95% of patients but warned of technical difficulties and limited postoperative range of motion. A total shoulder arthroplasty is needed if glenoid erosion from the screw(s) or bone occurs.
OrthoCash 2020
During the ilioinguinal approach to the pelvis, the corona mortis artery must be identified and ligated if present. The corona mortis artery joins the external illiac artery with which other major artery?
Pudendal
Deep illiac circumflex
Hypogastric
Obturator
Testicular
The "corona mortis" (translated as “crown of death”) artery is a vascular variant that joins the external illiac and the obturator artery as it crosses the superior pubic ramus. Tornetta et al did a study where "fifty cadaver halves were dissected to determine the occurrence and location of the corona mortis. Anastomoses between the obturator and external iliac systems occurred in 84% of the specimens. Thirty-four percent had an arterial connection, 70% had a venous connection, and 20% had both. The distance from the symphysis to the anastomotic vessels averaged 6.2 cm (range, 3-9 cm)." The corona mortis can be injured in superior ramus fractures and iatrogenically while plating pelvic ring injuries using the ilioinguinal approach.
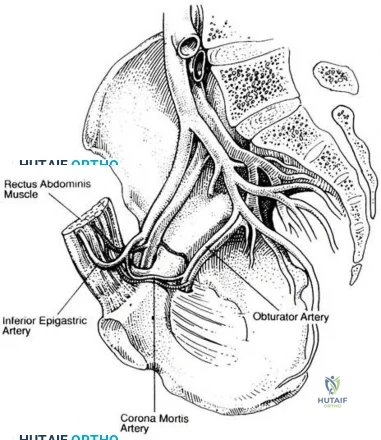
OrthoCash 2020
A 26-year-old male sustains a femoral shaft fracture treated with the implant shown in Figure A. Postoperatively, what muscular deficits can be expected at medium and long-term follow-up?

Weakness with hip abduction and knee flexion
Weakness with hip abduction and knee extension
Weakness with knee flexion and knee extension
Weakness with hip external rotation and hip abduction
Weakness with hip external rotation and hip flexion Corrent answer: 2
Figure A shows a femoral shaft fracture treated with an antegrade femoral nail. Long term deficits are weakness with knee extension (quadriceps) and hip abduction (glutei muscles).
The referenced study by Kapp et al noted long term quadriceps weakness as well as decreased bone mineral density in the femur (femoral neck by 9%, the lateral cortex by 20% and the medial cortex by 13%). It is unclear whether this is due to the injury, treatment, or a combination of both.
The second referenced study by Archdeacon et al also noted weakness in hip abduction, which showed time dependent improvement. He reports that increased early ipsilateral trunk lean is associated with worse recovery of abduction strength.
OrthoCash 2020
A 33-year-old male sustains the injury seen in Figure A as a result of a high-speed motor vehicle collision. Based on this image, what is the most likely acetabular fracture pattern?

Both column
Anterior column
Anterior column posterior hemitransverse
Transverse
T-type
The radiograph in Figure A shows a transverse acetabulum fracture. The iliopectineal (anterior column) and ilioischial lines (posterior column) are interrupted, revealing bicolumnar involvement; however, this is different than the both column fracture, as a transverse pattern has articular surface still in continuity with the axial skeleton via the sacroiliac joint.
The referenced article by Patel et al showed a wide variation of inter and intra-observer agreement in interpreting radiographs of acetabular fractures, with high agreement for basic radiographic classification and only slight to moderate agreement for other radiologic variables such as impaction.
The other referenced article by Letournel is a great review article regarding the initial classification of these fractures as well as a quick summary of his outcomes.
OrthoCash 2020
A 56-year-old carpenter sustains the closed injury seen in Figures A, B, and C. After temporary spanning external fixation is performed and soft tissue conditions improve, what strategy provides the optimal fixation for this fracture pattern?
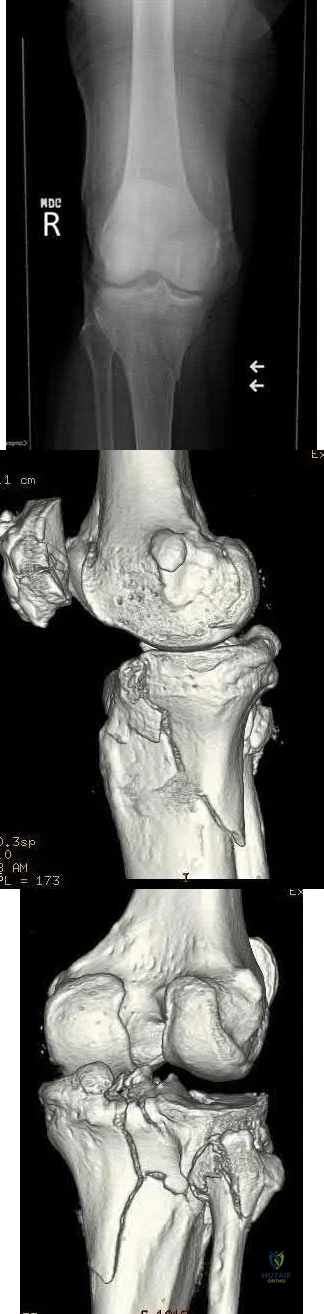
Anatomic lateral locking plate
Posteromedial and lateral plates
Anatomic medial locking plate
Conversion of the spanning external fixator to a hinged external fixator
Posterior buttress plate Corrent answer: 2
Figures A and B show a bicondylar tibial plateau fracture, with a typical appearing lateral fracture line and a posteromedial fracture line. The posteromedial sheared fracture piece is difficult, and/or sometimes impossible, to achieve appropriate stable fixation with a single lateral locking plate, as there will be limited screw purchase and fixation into the posteromedial fragment.
The referenced article by Georgiadis notes that a dual incision approach is safe and is associated with improved outcomes over their historical comparisons.
They describe the dual incisions and approaches in length, and review risks/issues with each approach.
The other referenced study by Bhattacharyya et al notes that these fractures have a typical appearance of the posteromedial fracture piece and that articular reduction quality is correlated with short-term results. They recommended buttress-type fixation of these fracture pieces.
OrthoCash 2020
A 31-year-old male sustains an irreducible ankle fracture-dislocation with the foot maintained in an externally rotated position. An AP and lateral radiograph are shown in figures A and B respectively. The attempted post reduction AP and lateral are shown in C and D. What structure is most likely preventing reduction?

Anterior-inferior tibiofibular ligament
Posterior-inferior tibiofibular ligament
Peroneus brevis tendon
Posterolateral ridge of the tibia
Flexor hallucis longus tendon Corrent answer: 4
As described by Hoblitzell et al, the so-called "Bosworth fracture-dislocation" is a rare fracture-dislocation of the ankle where the fibula becomes entrapped behind the tibia and becomes irreducible. It can cause compartment syndrome, as reported by Beekman and Watson.
Hoblitzell et al stress the importance and difficulty of recognizing these injuries. Standard radiographs are difficult to interpret due to the often severe external rotation of the foot. Prompt treatment, though can lead to good results in patients. The posterolateral ridge of the distal tibia hinders reduction and reduction often requires an open technique
Mayer and Evarts stated AP and mortise radiographs can be hard to interpret due to the external rotation posture of the foot. In their series a closed reduction consisting of traction and medial rotation applied to the foot while the fibular shaft is pushed laterally was successful in 3/4 patients.
OrthoCash 2020
A 37-year-old female sustains the injury seen in Figures A and B. At long-term follow up, degeneration of which of the following joints has been shown to have the highest rate of patient symptoms?

Tibiotalar joint
Talonavicular joint
Calcaneocuboid joint
Lisfranc joint
Subtalar joint
Figures A and B show a medial subtalar dislocation, which is more common than a lateral dislocation (65% vs. 35%).
The referenced article by Bibbo et al looked at long-term follow up of these patients, and noted that radiographic degeneration of the ankle and subtalar joints were 89%, although 31% of ankle joints were symptomatic and 68% of subtalar joints were symptomatic. Midfoot degeneration was seen radiographically in 72% (15% symptomatic).
OrthoCash 2020
In treating a lateral split-depression type tibial plateau fracture, which of the following adjuncts has been shown to have the least articular surface subsidence when used to fill the bony void?
Crushed cancellous allograft
Hydroxyapatite
Calcium phosphate cement
Autogenous iliac crest
Bisected diaphyseal humeral allograft Corrent answer: 3
In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations.
The referenced study by Russell et al noted a significantly increased rate of subsidence at 12 months with autograft as compared to calcium phosphate cement (in types I-VI).
The other referenced study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement.
OrthoCash 2020
The pelvic spur sign on plain radiography is indicative of the following injuries?
Transtectal transverse acetabular fracture
Vertical shear pelvic ring injury
Displaced H-type sacral fracture
Both column acetabular fracture
Anterior-posterior type III pelvic ring injury Corrent answer: 4
The pelvic spur sign is indicative of a both column acetabular fracture. It is best seen on an AP or obturator oblique x-ray. The spur is the intact portion of the ilium, still attached to the axial skeleton and seen posterosuperior to the displaced acetabulum (typically medially displaced).
Illustration A shows the spur sign (arrows) on a CT image, while illustration B shows an obturator oblique of the pelvis and the spur sign is shown with the long tailed arrow (on the left of the image).
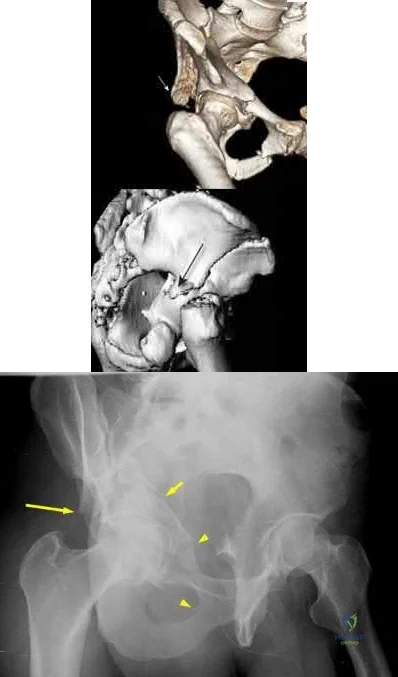
OrthoCash 2020
A 33-year-old male sustains a distal humerus fracture and is treated with open reduction and internal fixation of the distal humerus with olecranon osteotomy. A postoperative radiograph is shown in Figure A. A new deficit of the anterior interosseous nerve is now noted in the recovery room. What physical exam finding would be expected with this nerve injury?

Inability to flex radiocarpal joint
Loss of sensation over palmar aspect of thumb
Loss of sensation over dorsal hand first webspace
Inability to abduct index finger
Inability to flex thumb interphalangeal joint Corrent answer: 5
A deficit in the anterior interosseous nerve (AIN) would result in an inability to flex the interphalangeal joint (IPJ) of the thumb.
Injury to the AIN can be seen with K-wires that penetrate through the anterior cortex of the proximal ulna, such as mentioned above. The AIN is a branch of the median nerve that provides motor function to forearm/hand. It branches off from the median nerve 4 cm distal to the medial epicondyle, passes between the 2 heads of the pronator teres, travels through the forearm anterior to the interosseous membrane between the flexor pollicis longs (FPL) and flexor digitorum profundus (FDP), and then terminates in the pronator quadratus (PQ). The nerve gives of branches to the FDP, FPL, and PQ enabling for flexion of the distal phalangeal joint of the index and middle fingers, flexion of the IPJ of the thumb, and aids with pronation of the forearm, respectively.
Injury to the nerve will result in weakness in motor function to these muscles.
Mekail et al. reviewed the anterior approach to the proximal radius in order to describe and identify important neurovascular and musculoskeletal structures in the area. They were specifically aiming to determine the safest anatomic orientation for plate and screw fixation in regards to the posterior interosseous nerve. The authors, however, did discuss that medial plating was especially dangerous to the AIN, and significantly increased the risk of iatrogenic injury to the branch sent to the FPL.
Parker et al. reported a case report in a patient who experienced an AIN deficit postoperatively after tension banding of an olecranon fracture.
Intraoperatively, there were multiple passes of the K-wires in an attempt to find purchase in the anterior cortex of the ulna. The authors believed that during these passes, the nerve was injured and concluded that placing K-wires should not occur without radiologic visualization.
Figure A is a postoperative lateral radiograph after tension banding of the olecranon. Perforation of the anterior ulnar cortex can be seen by the K-wire which can cause damage to the AIN nerve. Illustration A is a schematic of the path of the AIN, its branches, and its function.
Incorrect Answers:
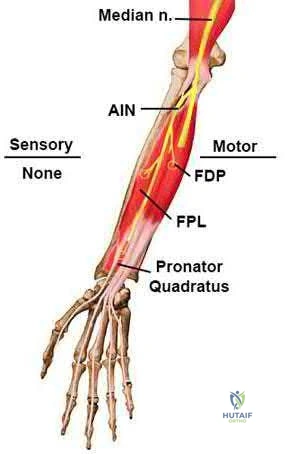
OrthoCash 2020
A computed tomography (CT) scan has been shown to be indicated for evaluation of all of the following aspects of acetabular fractures, EXCEPT:
Determination of surgical planning
Intra-articular loose bodies
Marginal impaction
Fracture piece size and position
Determination of pre-existing degenerative changes Corrent answer: 5
CT scanning is indicated in acetabular fractures for determination of surgical approach and techniques, evaluation of marginal impaction and presence of intra-articular loose bodies (especially after hip dislocation), and evaluation of fracture piece sizes and relative positions.
Kellam et al reviewed their initial experience with CT scanning and acetabular fractures, and noted a 25% change in surgical planning when CT was utilized versus plain radiographs; they also noted the ability to detect marginal impaction and fracture size/position was improved with CT.
OrthoCash 2020
A 69-year-old woman falls while getting out of her car and lands on her right shoulder sustaining a 4-part proximal humerus fracture. She subsequently undergoes surgery to treat the fracture, with immediate postoperative radiographs shown in Figure A. Six months following surgery, she denies shoulder pain, but she is unable to actively raise her hand above her shoulder. Which of the following is the most likely cause of this limitation?

Joint infection
Retroversion of the prosthesis
Glenoid arthritis
Axillary nerve injury
Greater tuberosity malunion Corrent answer: 5
The radiograph demonstrates a humeral hemiarthroplasty. Malunion of the greater tuberosity is a known complication of this procedure, and the most likely cause for loss of shoulder elevation.
Frankle et al in 2004 reported a 25% rate of greater tuberosity malunion. They discuss surgical techniques to improve fixation of the tuberosities following hemiarthroplasty for proximal humerus fractures.
Frankle et al in 2002 evaluated 5 different techniques to reattach the tuberosities following shoulder hemiarthroplasty in human cadavers. Findings suggested that a circumferential medial cerclage should be placed around the tuberosities to enhance the stability of the tuberosity repair.
Bosch et al reviewed 39 consecutive 3 or 4 part proximal humerus fractures that were treated with either primary hemiarthroplasty or secondary hemiarthroplasty following a primary ORIF. Patients who underwent primary
hemiarthroplasty reported better clinical outcomes. The authors concluded that elderly patients with 3 or 4 part humerus fractures are best treated with early arthroplasty.
OrthoCash 2020
An acetabular fracture with all segments of the articular surface detached from the intact posterior ilium is defined as what fracture pattern?
Transverse
Both column
Anterior column posterior hemitransverse
Posterior column with posterior wall
Anterior column with anterior wall Corrent answer: 2
A both column acetabular fracture is defined as an acetabular fracture with no articular surface in continuity with the remaining posterior ilium (and therefore, axial skeleton). The spur sign is a radiological sign seen with these fractures, and is the posterio-inferior aspect of the intact posterior ilium. The spur sign and other radiographic findings consistent with a both column acetabular fracture can be seen in Illustration A (AP), Illustration B (obturator oblique), and Illustration C (iliac oblique).
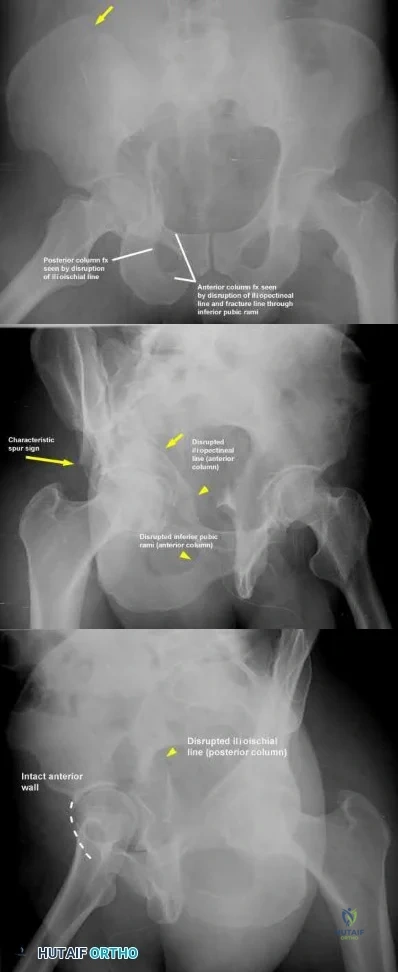
OrthoCash 2020
A large posteromedial tibial plateau fracture pattern, as seen with the bicondylar tibial plateau fracture shown in Figures A and B, is important to recognize because of which of the following factors?

Association with posteromedial corner of the knee injury
Association with anterior tibial artery injury
Possible need for dual plate fixation
Possible need for single extensile anterior approach to the knee
Increased risk of deep venous thrombosis Corrent answer: 3
Figures A and B show a bicondylar tibial plateau fracture with a large posteromedial fracture piece. This has clinical importance, as currently available plate/screw constructs often have poor fixation of this fracture segment, and this pattern often requires a second, posteromedial, approach and placement of a second plate/screw construct.
The referenced article by Barei et al notes a prevalence of posteromedial fracture pieces of nearly 33% of all bicondylar tibial plateau fractures. They also recommend supplementary or alternative fixation techniques when this pattern is recognized.
The referenced article by Higgins et al notes a 59% incidence of this fracture pattern (consisting of nearly 25% of the total joint surface) in bicondylar tibial plateau fractures, and recommends appropriate fixation to combat the vertical shear instability through a separate approach.
The last referenced study by Higgings et al notes a significantly increased rate of late fracture displacement in a biomechanical model with a single lateral locking plate as compared to a dual plate construct.
OrthoCash 2020
At the elbow, the anterior bundle of the medial collateral ligament inserts at which site?
Radial tuberosity
3mm distal to the tip of the coronoid
Anteromedial process of the coronoid
Medial border of the olecranon fossa
Radial side of ulna at origin of annular ligament Corrent answer: 3
The anterior bundle of the medial collateral ligament of the elbow inserts at the anteromedial process of the coronoid, also known as the sublime tubercle.
Fractures at this site have been shown to have worse results with nonoperative
treatment, due to increased rates of instability and post-traumatic arthrosis.
The referenced articles by Ring and Steinmann are great reviews of the topic of coronoid fractures. They review the diagnosis, treatment options, rehabilitation, and outcomes of these injuries. They focus on the importance of the coronoid in elbow stability, especially with base fractures, or ones that involve the sublime tubercle.
Illustration A depicts the anterior bundle of the MCL inserting at the sublime tubercle.
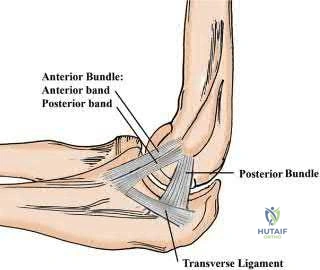
OrthoCash 2020
In the Lauge-Hansen classification system, a pronation-abduction ankle fracture has what characteristic fibular fracture pattern?
Transverse fracture below the level of the syndesmosis
Short oblique fracture running from anteroinferior to posteriosuperior
Short oblique fracture running from posteroinferior to anteriosuperior
Comminuted fracture at or above the level of the syndesmosis
Wagstaff fracture
In the Lauge-Hansen classification, the characteristic fibular fracture pattern in a pronation-abduction injury is a comminuted fibular fracture above the level of the syndesmosis. In the first stage of this injury pattern, the deltoid fails in tension, or an avulsion fracture of the medial malleolus occurs. In the second stage, the anterior inferior tibiofibular ligament ruptures, or a small bony avulsion of this ligament's insertion/origin occurs. The final stage includes the creation of a comminuted fibular fracture above the level of the syndesmosis.
The referenced article by Siegel et al noted that extraperiosteal bridge plating of these ankle injuries was safe and had excellent radiographic and clinical outcomes at final follow-up.
OrthoCash 2020
A 38-year-old male sustains the closed injury shown in Figures A and B. When treating this injury with an intramedullary nail, addition of blocking screws into which of the following positions can prevent the characteristic malunion deformity?
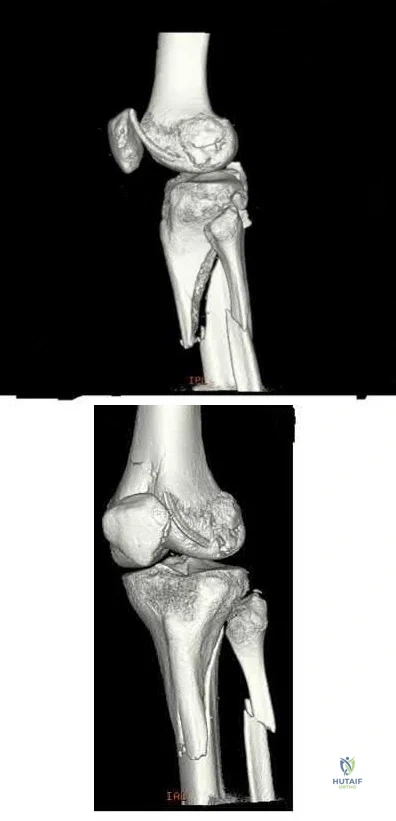
Anterior to the nail in the proximal segment; medial to the nail in the proximal segment
Anterior to the nail in the proximal segment; lateral to the nail in the proximal segment
Posterior to the nail in the proximal segment; lateral to the nail in the proximal segment
Anterior to the nail in the distal segment; lateral to the nail in the distal segment
Posterior to the nail in the distal segment; medial to the nail in the proximal segment
Figures A and B show a proximal tibia fracture, which is prone to malreduction/malunion into a characteristic valgus and procurvatum (apex anterior) deformity. Placement of screws in this instance posterior to the nail (medial to lateral) and lateral to the nail (anterior to posterior) in the proximal segment will prevent iatrogenic malalignment.
Intramedullary nails will not effect a reduction in metaphyseal proximal tibia fractures. Valgus and apex anterior deformities in these injuries may be caused by deforming muscular forces, limb positioning in hyper flexion, as well as iatrogenic deformity created by improper nail insertion technique. Blocking (Poller) screws are utilized to redirect intramedullary nails by creating an artificial cortex to guide the nail into appropriate position.
The referenced biomechanical study by Krettek et al noted that addition of blocking screws added increased stability to metaphyseal fractures.
Ricci et al noted no malalignment intraoperatively or at final follow-up of proximal tibia fractures treated with intramedullary nails if blocking screws were used.
OrthoCash 2020
In an uninjured proximal tibia which statement best describes the shape and position of the medial tibial plateau relative to the lateral tibial plateau?
More concave and more proximal
More convex and more proximal
More concave and more distal
More convex and more distal
Symetric in conture and more distal
The medial tibial plateau is more concave and more distal relative to the lateral tibial plateau.
Watson et al report "the medial tibial plateau has a more concave shape and is larger in both length and width than the lateral tibial plateau, which has a slightly convex shape. The lateral tibial plateau lies proximal to the medial plateau. The convexity of the lateral plateau helps differentiate it from the medial plateau on a lateral radiograph of the proximal tibia."
Illustration A shows the relative concavity of the medial and lateral proximal tibia.
OrthoCash 2020
On average, the radial nerve travels from the posterior compartment of the arm and enters the anterior compartment at which of the following sites?
Spiral groove of the humerus
At the arcuate ligament of Osborne
10 cm distal to the lateral acromion
10 cm proximal to radiocapitellar joint
At the origin of the deep head of the triceps Corrent answer: 4
The radial nerve enters the anterior compartment through the intercompartmental fascia on average 10 cm proximal to the radiocapitellar joint. It has never been found to remain in the posterior compartment within
Question 82
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
REFERENCES: Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Fukuda H: Partial-thickness rotator cuff tears: A modern view on Codman’s classic. J Shoulder Elbow Surg 2000;9:163-168.
Question 83
The condition shown in Figures 9a and 9b is most likely the result of

Explanation
Question 84
Examination of a 45-year-old man with Charcot-Marie-Tooth disease reveals a cavus foot, a tight Achilles tendon, and forefoot callus formation. Radiographs reveal advanced degenerative changes in the hindfoot. Shoe wear modifications have failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth disease. J Bone Joint Surg Br 1989;71:17-20.
Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Question 85
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?
Explanation
REFERENCES: O’Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 529-530.
Question 86
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
REFERENCES: Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Elliot DC: An evaluation of the end points of resuscitation. J Am Coll Surg 1998;187:536-547.
Question 87
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 88
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?
Explanation
REFERENCE: Unidia-Kallio L, et al: Serum c-reactive protein, ESR and WBC in acute hematogenous osteomyelitis in children. Pediatrics 1994;93:59-62.
Question 89
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Loebenberg MI, Plate AM, Zuckerman JD: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 90
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?

Explanation
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non-functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are
more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Question 91
When comparing arthroscopic and open rotator cuff repairs, which of the following tears shows a decreased recurrent tear rate in the open versus the arthroscopic group? Review Topic
Explanation
Question 92
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10°. Initial management should consist of
Explanation
REFERENCES: Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 93
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3800-3833.
Question 94
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer's representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacturer's representative suggests a partnership in a boat costing $200,000. The manufacturer's representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
Question 95
5 units PRBCs. The estimated blood loss was 1276cc and not affected by the fracture pattern or high/low energy pattern. They concluded that preoperative hemorrhage contributed to transfusion needs more than intraoperative blood loss.
Explanation
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?
Decreased joint penetration of distal screws
Increased rigidity
Decreased need for delayed hardware removal
Decreased peroneal irritation
Improved distal fixation Corrent answer: 4
Posterior antiglide plating is a technique that involves placement of a plate on the posterior aspect of the distal fibula, using the plate as a reduction tool and direct buttress against distal fracture fragment displacement.
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
OrthoCash 2020
A 24-year-old female sustains a surgical neck proximal humerus fracture in a motor-vehicle collision. She undergoes open reduction and internal fixation but heals in 45 degrees of varus and has significant limitation of shoulder range of motion despite 9 months of conservative treatments. What is the most appropriate treatment at this time?
Manipulation under anesthesia
Humeral head resurfacing
Shoulder hemiarthroplasty
Revision open reduction internal fixation with osteotomy
Reverse total shoulder arthroplasty Corrent answer: 4
Malunions of the proximal humerus typically result in significant restrictions in range of motion. This young patient has sustained a proximal humeral malunion, and treatment should include a corrective osteotomy for improved outcomes, as she has failed conservative treatment.
The cited reference by Williams et al as well as the referenced article by Siegel et al explain various techniques in management of proximal humerus malunions. They state that the two primary indications for surgical management of proximal humerus malunion include 1) pain and 2) diminished function resulting from limited range of motion. Because this patient is young, you would attempt revision ORIF/osteotomy as opposed to humeral head arthroplasty.
OrthoCash 2020
A 6-year-old boy with progressive bilateral genu varum undergoes the surgeries shown in Figure A. On postoperative rounds later that day, the patient appears sedated after several doses of pain medication. His toes are pink with brisk capillary refill however, passive motion of his toes causes pain. Among the answer choices listed, what is the best management strategy for this child?

Elevate his legs and reevaluate on morning rounds
Adjust his pain medication to accommodate for his increasing pain
Administer a muscle relaxant for leg spasms
Cast removal and measurement of compartment pressures with a standard device
Examine the cast for areas of constriction and reevaluate in the morning Corrent answer: 4
Intracompartmental pressure measurements should be performed when pain with passive motion of the toes is found in young patients with insufficient clinical data to establish a definitive diagnosis of compartment syndrome. The child in this clinical vignette has Blount’s disease which was treated with bilateral tibial osteotomies, a procedure commonly associated with compartment syndrome.
Pain with passive stretch is the most sensitive clinical sign of elevated compartment pressures prior to the onset of ischemia in compartment syndrome. Pain is difficult to assess in children at baseline, therefore, a high level of suspicion should exist and compartment pressure monitoring should be performed in unreliable patients.
Mubarak et al. reported on a series of 27 patients subjected to intracompartmental pressure monitoring for a clinical suspicion of acute compartment syndrome. The wick catheter technique was employed not only to aid in the diagnosis of compartment syndrome at an early stage but also to indicate the effectiveness of the decompressions when used intraoperatively during fasciotomies.
Matsen et al. reported on 24 children with compartment syndrome following injuries and surgery. The most common etiologies identified were fractures, vascular injuries, and tibial osteotomies. Compartment pressure measurements were helpful in establishing the diagnosis of compartment syndrome in young patients and in those with neurologic or vascular injuries with ambiguous clinical findings.
Figure A reveals an AP radiograph of bilateral knees status post valgus-producing tibial osteotomies and epiphysiolyses of the medial tibial physes in a 6-year-old male with Blount’s disease.
Incorrect Answers:
OrthoCash 2020
A 16-year-old male was struck by an automobile while riding his bicycle. He sustained the injuries in Figure A. Which of the following orthopedic injuries is MOST associated with this injury?

Brachial plexus injury
Ipsilateral clavicle fracture
Pelvic ring injury
Rib fracture
Spine fracture
Figure A demonstrates a scapula body fracture. Rib fractures are the most common orthopedic injury associated with these high-energy fractures, with a 52% incidence.
Scapula fractures are associated with high-energy trauma and have a reported mortality rate of 2-5%. Approximately 50% of high-energy scapular fractures involve the body and spine. Most scapular fractures may be treated conservatively with sling immobilization followed by early motion with no expected functional deficits. Indications for operative management of scapular fractures include glenohumeral instability with >25% of glenoid involvement or
>5mm of articular step-off, excessive medialization of the glenoid, displaced scapular neck or coracoid fractures, and open fractures.
Baldwin et al. retrospectively reviewed 9,543 scapular fractures utilizing the US National Trauma Database. They reported that the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). They concluded that lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Brown et al. retrospectively reviewed the association between scapular fractures (SF) and blunt thoracic aortic injury (BTAI). They found that in 35,541 blunt trauma admissions, SF and BTAI occurred in 1.1% and 0.6% of patients, respectively. They noted that most of the patients with SF had associated injuries (99%), but only four patients with SF had BTAI. The most common injuries associated with SF were rib (43%), lower extremity (36%), and upper extremity (33%) fractures. They concluded that SF is uncommon after blunt trauma, but patients with SF almost always have significant associated injuries and indicates a high amount of energy.
Figure A demonstrates a high-energy scapular body fracture which may benefit from surgical intervention
Incorrect Answers:

OrthoCash 2020
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?
Above-knee-amputation (transfemoral)
Below-knee-amputation (transtibial)
Through Knee
Syme
Midfoot
The general trend is increasing energy requirement for more proximal amputations. Amputation should be performed at the lowest possible level in order to preserve the most function.
Pinzur compared 5 patients with amputations at midfoot, Syme’s, BKA, through knee, and AKA with five controls. Walking speed and cadence decreased while oxygen consumption per meter walked increased with each more proximal amputation.
The only exception is the Syme which was the most energy efficient even though it is more proximal to the midfoot amputation.
OrthoCash 2020
An otherwise healthy 30-year-old male sustains a left forearm injury as a result of a fall from a ladder. Initial examination in the emergency room reveals a clean 2 centimeter laceration over the volar forearm associated with the radiographs shown in Figures A and B. Treatment should consist of irrigation and debridement of the wound followed by which of the following?

Closed reduction and casting of left radius and ulna
Temporary external fixation of the left radius and ulna
Definitive external fixation of the left radius and ulna
Open reduction and internal fixation of the left radius and ulna with delayed skin closure
Open reduction and internal fixation of the left radius and ulna with immediate skin closure
The clinical scenario is consistent with an open fractures of the distal radial and ulnar shafts. Literature shows that definitive plating of an open forearm fracture followed by primary closure of the wound is acceptable treatment at the time of injury.
Chapman et al performed a retrospective review of 50 patients with immediate internal plate fixation of an open diaphyseal fracture of the forearm. The functional results were excellent or good in 85%.
The review by Levin is a comprehensive review of the literature on early versus delayed closure of open fractures, and covers the change in thought from previous literature, including change in technology, surgical techniques, and a more critical review of previous literature.
OrthoCash 2020
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.
Releasing the posterior tibialis tendon
Preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base
Myodesis of the anterior tibialis to the medial and middle cuneiforms
Lengthening of the gastrocsoleus (achilles tendon)
Osteotomy through 1st metatarsal Corrent answer: 2
A Lisfranc amputation is through the tarsometatarsal joints, except the 2nd metatarsal, which is osteotomized to preserve the stability of the medial cuneiform. To prevent the patient from supinating the foot following this amputation, the evertors on the foot must be maintained. The principal evertors are the peroneus brevis and longus (Illustration A). Therefore, the function of the peroneus brevis must be preserved. Technically this is done preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base.
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
The posterior tibialis is the primary supinator of the foot, and releasing it
would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved.
The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot.
A lengthened Achilles would lead to increased dorsiflexion, not supination.
Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
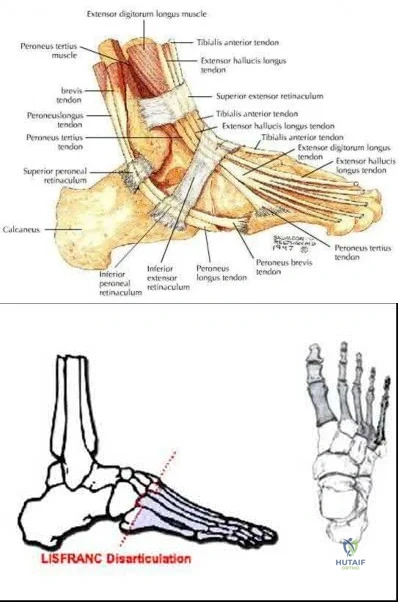
OrthoCash 2020
A 39-year-old male is thrown from his motorcycle into a fast-food restaurant and sustains a closed pelvic ring injury. During placement of percutaneous iliosacral screws, the outlet radiograph in Figure A is obtained. What purpose does this view serve?
Evaluation of possible injury to L5 nerve root
Evaluation of anterior-posterior position of screw(s)
Best visualization of sagittal curvature of sacral ala
Best visualization of spinal canal
Best visualization of sacral neural foramina Corrent answer: 5
Figure A shows an intraoperative outlet view, which provides the best visualization of the neural foramina (and possible screw placement into these foramina). This view provides information regarding cephalad-caudad placement of the screw, whereas the inlet view provides information regarding the anterior-posterior position of the screw. The lateral sacral view provides information regarding the sagittal curvature of the sacral ala and gives information regarding possible iatrogenic L5 nerve injury as it goes over the sacral ala.
The referenced article by Routt et al is a review article regarding the safety and techniques of percutaneous pelvic ring fixation.
OrthoCash 2020
A 35-year-old male sustains a closed Schatzker VI tibial plateau fracture. Two weeks following external fixation, examination reveals intact sensation, palpable pulses and no soft tissue compromise. An axial CT image is shown in Figure A. What is the optimal surgical plan?
Medial and lateral plate fixation through two approaches
Medial and lateral plate fixation through a single anterior approach
Lateral locking plate fixation
Continued external fixation until union
Multiplanar transarticular external fixator Corrent answer: 1
The Figure shows a bicondylar tibial plateau fracture. The goals that need to be met when treating tibial plateau fractures are the following: restoration of mechanical axis alignment, restoration of condylar width, articular reduction, and restoration of knee stability. Since the soft tissue envelope is favorable, open reduction internal fixation with dual incisions and dual plates will provide the best probablity of achieving those goals.
Gosling et al did a biomechanical evaluation in cadavers comparing lateral locked plating with a combined medial and lateral plate and found no difference in resistance to vertical subsidence even with loads exceeding the average body weight. However, this was a cadaveric study with no mention and capability of analyzing articular reduction. Lateral locked plating only allows for indirect reduction of the medial plateau.
Barei et al in a retrospective review found that comminuted bicondylar tibial plateau fractures can be successfully treated with open reduction and medial and lateral plate fixation using 2 incisions, and postulate that the use of 2 incisions may contribute to a lower wound complication rate. A two incision approach allows not necessarily for a stronger construct as some studies are controversial, but for a more accurate reduction and restoration of alignment.
OrthoCash 2020
Which of the following is true regarding the use of the saline injection load test to diagnose traumatic knee arthrotomies?
Addition of methylene blue to the saline load test increases the sensitivity of the test
Injection of 110ml of saline will diagnose 95% of knee arthrotomies
Injection of 175ml of saline will diagnose 99% of knee arthrotomies
A superomedial injection location requires significantly less fluid than a inferoeromedial injection location
A history and physical exam by an orthopaedic surgeon has equivalent sensitivity to saline load test at detecting a traumatic arthrotomy
Injection of 175ml of saline will diagnose 99% of knee arthrotomies.
Clinical evaluation alone to determine if a periarticular laceration has penetrated the joint can often be incorrect. A Saline Load Test (SLT) is an effective methods to detect intraarticular penetration. New studies have shown addition of methylene blue does not improve the diagnostic value of the saline load test. The use of a CT scan can be helpful, especially in the presence of intra-articular air.
Voit et al. investigated the sensitivity of the clinical exam and a saline load test in 50 consecutive patients with periarticular lacerations suggestive of joint penetration. In 14 there was leakage of fluid on saline load test. In six of these patients, the clinician had judged there was no traumatic arthrotomy based on physical exam and clinical history. They therefore concluded performing a saline load test is important adjunct and the clinical exam alone can not be relied on to detect traumatic arthrotomies.
Nord et al. found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were
110, 145, 155, and 175 mL, respectively. They also found that an inferomedial injection location required significantly less fluid than a superomedial injection location did.
Metzger et al. studied 58 patients that underwent saline load test with about 100ml of saline injected (methylene blue 29, normal saline 29). They found that the false-negative rate was 67% (methylene blue 69%, normal saline 66%). They concluded the addition of methylene blue does not improve the diagnostic value of the saline load test.
Konda et al. performed a study evaluationg the role of CT scan versus saline load test. They found that the sensitivity and specificity of the CT scan to detect traumatic arthrotomy was 100%. In a subgroup of 37 patients that received both a CT scan and the conventional saline load test, the sensitivity and specificity of the CT scan was 100% compared to 92% for the saline load test (p<0.001).
Incorrect Answers:
OrthoCash 2020
A 36-year-old rancher is involved in a tractor roll-over accident and sustains the injury shown in Figure A to his dominant right arm. After undergoing rigid anatomic fixation of the fracture, the distal radio-ulnar joint (DRUJ) remains incongruent. What is the next step in management?

Revision plating of the fracture
Revision reduction and intramedullary fixation
Reduction of interposed extensor carpi ulnaris tendon
Reduction of interposed pronator quadratus tendon
Reduction of interposed flexor carpi ulnaris tendon Corrent answer: 3
The most likely cause of persistent DRUJ incongruity after anatomic reduction and fixation of the radial shaft fracture of the answers above is interposition of the extensor carpi ulnaris (ECU) tendon. The tendon must be extricated from the joint to permit DRUJ reduction.
Gaeleazzi fracture-dislocations, such as that seen in Figure A, are typically stable once the radial shaft fracture is anatomically reduced. After fixation, the DRUJ is translated in pronation, supination, and in a neutral position to test for stability. A “clunk” during passive motion of the DRUJ is further evidence of gross instability. Gross laxity can be treated by splinting in supination or by pinning the DRUJ. However, ECU tendon interposition has been reported as a possible cause of a persistently irreducible DRUJ. Radiographic findings typically demonstrate a dorsally displaced ulnar head and a widened DRUJ. The interposed tendon must be removed from the joint, often through a separate dorsal approach to permit DRUJ reduction.
Bruckner et al. review the evaluation and management of complex dislocations of the DRUJ. The authors note that these injuries are associated with frequent irreducibility, recurrent subluxation, or soft reduction of the DRUJ secondary to interposed tissue. In their institutional series, four of the 11 cases of Galeazzi fractures were associated with complex DRUJ dislocations, most commonly due to displacement of the ECU tendon volar to the ulna, necessitating open reduction. They cautioned that unobtainable or unconvincing reductions should warrant surgical exploration.
Paley et al. reported two cases of an irreducible DRUJ after radial shaft fracture fixation. The authors describe an empty ECU tendon sulcus on the dorsum of the wrist in both cases. One case was noted and addressed intraoperatively.
However, the second case was not identified and this patient went on to endure persistent subluxation and diastasis of the DRUJ, ultimately experiencing a poor result. The authors advocate a separate dorsal exposure to reduce the ECU.
Hanel and Scheid reported a case of entrapment of the ECU in the DRUJ in a skeletal immature 12 year old boy. They noted that intraoperative radiographic analysis was significant for a widened DRUJ and dorsally displaced ulnar head. These authors too advocated a separate dorsal exposure to approach and extricate the ECU tendon.
Incorrect answers
OrthoCash 2020
A 58-year-old right-hand-dominant computer programmer trips and falls onto his right arm. He reports right arm pain and that his elbow felt "sloppy". His initial lateral radiograph is shown in Figure A. The orthopedic junior resident counsels him that he will likely need a radial head arthroplasty, ligament repair, and possible fixation of the ulna. What factor would most significantly affect the decision to surgically address the ulna fracture?

Degree of radial head comminution
The deforming force acting on the avulsed fracture fragment
Size of fragment and elbow stability after radial head replacement
The degree of fracture displacement
Patient age and bone quality Corrent answer: 3
The size of the fragment and degree of elbow instability following radial head fixation or replacement most often determines the intraoperative decision on coronoid fragment fixation.
The radial head is a secondary restraint to posterolateral rotatory instability (PLRI) of the elbow, while the coronoid provides an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. The medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid, so large medial facet fractures may displace and cause varus posteromedial instability (PMRI). However, in terrible triad injuries (causing PLRI), small coronoid tip fractures are more common. These are typically left as they most often do not contribute to elbow instability. Therefore in most cases, radial head replacement and lateral ligamentous repair are sufficient to restore stability.
However larger coronoid base fractures may require fixation in order to stabilize the elbow. In these cases, the coronoid fracture may be addressed through the lateral window after radial head resection and before the trial implant is assessed. The anterior capsule can be tied down to the ulna or if the fracture is large enough, it may sometimes tolerate internal fixation.
Conversely, a buttress plate for the coronoid may be applied via a medial approach in the setting of a large coronoid base fracture as in PMRI.
Ring et al. reviewed 11 terrible triad injuries including 7 of which had the radial head surgically addressed and 4 of which had undergone radial head excision. The authors found that all four patients who underwent radial head excision dislocated after surgery. Only four patients had a satisfactory result, and all of these had fixation of the radial head, two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries were unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Pugh et al. reviewed 36 cases of terrible triad injuries in which all coronoid fractures were addressed, either with screw fixation or suture repair of the anterior capsule. The authors reported that the average arc of motion postoperatively was 112 degrees, Mayo score was 88, and concentric stability was restored in 34/36. There were 8 complications requiring re-operation. They concluded that coronoid fixation with radial head fixation or replacement yields a stable elbow suitable for early motion.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LUCL lead to posterolateral laxity. Furthermore, if 30% of the coronoid tip was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was
excised, even with a radial head replacement dislocation occurred. They concluded that so long as the radial head is replaced, small coronoid fractures may not need to be repaired.
Figure A demonstrates a comminuted radial head fracture, a small coronoid fracture, and subluxation of the ulnohumeral joint.
Incorrect answers:
OrthoCash 2020
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?
Tension band plating
Antiglide plating
Bridge plating
Neutralization plating
Submuscular plating
A supination-adduction ankle fracture leads to a vertical fracture of the medial malleolus. Traditional fixation of the medial malleolus with oblique screws from the tip of the malleolus directed proximally will ineffectively protect against shear forces at the fracture site; these also are directed quite obliquely to the vertical fracture line, and therefore have poor biomechanical resistance to failure. An antiglide plate is used medially to prevent displacement of the fracture segment due to shear forces.
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are
biomechanically the most important aspect of the construct whether a plate is used or not.
OrthoCash 2020
A 25-year-old Norwegian amateur curler slips on the ice, falling onto an outstretched right elbow. He is taken to the local teaching hospital and radiographs demonstrate a significantly comminuted radial head fracture and coronoid base fracture. His elbow is reduced and splinted. To restore stability and allow early range of motion, which of the following will most likely need to be performed in most cases?
Radial head fixation or replacement
Radial head fixation or replacement and coronoid fixation
Radial head fixation or replacement, coronoid fixation, and lateral ulnar collateral ligament (LUCL) repair
Radial head fixation or replacement, coronoid fixation, LUCL and medial ulnar collateral ligament (MUCL) repair
Radial head fixation or replacement, coronoid fixation, LUCL and MUCL repair, and application of a hinged fixator
The patient has sustained a "terrible triad" injury, classically involving a radial head fracture, coronoid fracture, and elbow dislocation. These often involve LUCL injuries and a traumatic injury in the radiocapitellar joint. Stability is achieved with radial head replacement (or fixation), coronoid fixation (in cases with a large coronoid fracture), and lateral soft tissue repair.
Posterolateral rotatory instability (PLRI) following a terrible triad injury is usually caused by a fall on an extended arm that produces a valgus, axial, and rotatory force. The mechanism of injury begins laterally and moves medially.
Hence, the LUCL fails first, followed by the anterior capsule (or coronoid), and lastly the MUCL. Even following fixation, patients often lose some degree of their flexion-extension arc, may develop post-traumatic arthritis, or most commonly may have persistent instability. The radial head is a primary restraint to PLRI and must be either replaced with a prosthesis or fixed in the setting of a terrible triad injury. Replacement is typically chosen when the radial head is in more than 3 fragments. Coronoid fractures should be fixed when they involve >30-50% of the coronoid base. However, the best way to determine if coronoid fixation is necessary is with an intraoperative fluoroscopic examination.
Forthman et al. reviewed outcomes following the management of 34 elbow fracture-dislocations. In all cases, the radial head was replaced or underwent fixation. The MUCL was not repaired in any case. The authors noted only 2 cases of post-operative instability, one terrible triad, and one combined capitellum and trochlea fracture. The authors noted that both cases were related to non-compliance. The remaining 32 averaged 120 degrees of flexion-extension and 74% had good-excellent outcomes. The authors concluded that MUCL repair is not required for elbow dislocations so long as the radial head, large coronoid fractures, and LUCL are addressed.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LCL leads to posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was excised, even with a radial head replacement, dislocation occurred. This led the authors to conclude that long as the radial head was replaced, small coronoid fractures may not need to be repaired.
Papatheodorou et al. reviewed 14 terrible triad injuries (all of which had Regan-Morrey type 1 or 2 coronoid fractures) that underwent surgical fixation or replacement of the radial head combined with LUCL repair. The authors noted that intraoperative stability was confirmed in all cases without coronoid fixation, MCL repair, or an external fixator. The authors concluded that coronoid fixation is not required in fractures up to 50% the height of the coronoid and that MCL repair is not necessary.
Incorrect answers:
OrthoCash 2020
A 32-year-old female sustains the injury shown in Video A. The right-sided pelvic injury is best classified as which of the following?
Lateral compression 1
Lateral compression 2
Vertical shear
Anterior-posterior compression 2
Anterior-posterior compression 3
The injury shown in Video V reveals a right sided posterior ilium fracture, which is known as a crescent fracture. The presence of a crescent fracture is consistent with a lateral compression type 2 injury; this differentiates this from a type I injury. The ipsilateral anterior sacrum has a small impaction injury anteriorly while the contralateral SI joint has a minor amount of anterior sacral impaction indicative of a lateral compression type I injury.
The reference by Burgess et al is the primary source of the mechanism classification of pelvic ring injuries. Overall blood replacement averaged 5.9 units (lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units). Overall mortality was 8.6% (lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear,
0%; combined mechanical, 18.0%).
Incorrect answers:
1: The presence of a crescent fracture means this is at least a LC-2 injury. The left-sided fracture pattern is consistent with an LC-1 pattern.
3: A vertical shear fracture pattern would exhibit some vertical displacement and does not typically exhibit the crescent fragment.
4: The fracture pattern does not match an anterior-posterior compression pattern.
5: The fracture pattern does not match an anterior-posterior compression pattern.
OrthoCash 2020
A 35-year-old zookeeper fell 10 feet while preparing an exhibit for a grand reopening, landing on his left arm. The patient is then evaluated by a keen orthopedic resident in the emergency room who describes the zookeeper's injuries to his chief. He describes a comminuted radial head fracture and posterolateral ulnohumeral dislocation. The chief resident orders a CT scan which demonstrates a coronoid fracture involving 50% the height with no involvement of the anteromedial facet. During surgery, the trauma surgeon replaces the radial head and repairs the lateral collateral ligament complex. The
elbow is splinted in elbow flexion and pronation. The patient begins range of motion exercises with her occupational therapist 3 days after surgery, and her elbow dislocates. What is the most likely reason for her instability?
Length of immobilization
Position of immobilization
Lack of coronoid fixation with medial buttress plate
Lack of coronoid fixation from lateral approach
Lack of medial collateral ligament repair Corrent answer: 4
The zookeeper sustained a "terrible triad" injury with resulting posterolateral rotatory instability (PLRI). To prevent post-operative instability, large coronoid fractures should be fixed, and this would be performed through a lateral approach given that the radial head will be replaced.
The coronoid serves as an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. Though the coronoid tip has no soft tissue attachments, the medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid. A coronoid fracture through the anteromedial facet, such as in the setting of posteroMEDIAL rotatory instability, would require a medial buttress plate to restore varus stability. In a coronoid base fracture involving 50% of the coronoid, fixation is required even when a radial head arthroplasty is performed. This can be done with suture fixation via a bone tunnel through the ulna or with screws from dorsal to volar. Failure to fix a large coronoid base fracture would result in persistent instability, as with the patient in this vignette.
Ring et al. reviewed 11 terrible triad injuries - including 7 of which had the radial head surgically addressed and 4 of which underwent radial head excision. They noted that all four patients who underwent radial head excision dislocated after surgery. Moreover, only four patients had a satisfactory result, and all of these had fixation of the radial head, with two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries are unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They showed that radial head excision even with an intact LUCL resulted in persistent posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement alone. If 50% of the coronoid was excised, even with
a radial head replacement, dislocation occurred. The authors concluded that so long as the radial head was replaced, small coronoid fractures may not need to be repaired, but large fractures involving 50% or more would require fixation even if the radial head and LUCL were addressed.
Moro et al. treated 25 unreconstructible radial head fractures with a metal radial head arthroplasty. The authors reported a DASH score of 17, PRWE of 17, and Mayo elbow score of 80. Poor outcomes were seen in those with psychiatric disorders or those involved in a worker's compensation claim. The authors reported that radial head arthroplasty resulted in stable elbows with mild-moderate physical impairment.
Ring, Quintero, and Jupiter reviewed 56 patients with radial head fractures who underwent surgical fixation. Of the comminuted Mason type-3 fractures that underwent ORIF, they found that 13/14 had a poor result. The authors recommend that fractures with 3 or fewer fragments are amenable to fixation while those with 4 or more articular fragments are not.
Incorrect answers:
OrthoCash 2020
Which of the following injuries would require plating of the radius along with closed reduction and evaluation of the distal radioulnar joint (DRUJ)?
Nightstick fracture
Galeazzi fracture
Monteggia fracture
Rolando fracture
Smith fracture
A Galeazzi fracture is a fracture of the distal third of the radius with dislocation of the distal radioulnar joint. It commonly results from a fall onto an outstretched hand with the forearm in pronation.
A Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction and fixation of the radial shaft, and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. Otherwise, either open or closed reduction with pinning can be undertaken to stabilize the joint. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Acute intervention results in improved outcomes as compared to delayed reconstruction.
Rettig et al. retrospectively analyzed 40 patients with Galeazzi fracture-dislocations that were treated with open reduction and internal fixation of the radial shaft fracture. They noted that a radial shaft fracture located within
Question 96
Avascular necrosis
Explanation
A 9-year-old girl sustains an injury (Slide) as a result of a fall. What is her risk of avascular necrosis:
Question 97
Figure 48 shows the radiograph of a 17-year-old boy who sustained a gunshot wound to his forearm. There is a small entrance wound on the volar surface. The exit wound is dorsal and more than 15 cm in size, with loss of skin and an extensive amount of devitalized muscle hanging out of the wound. Vascular supply to the hand is excellent, the ulnar and median nerves are intact in the hand, but the radial sensory nerve function is absent. After repeated surgical debridements of the wound and bone, definitive treatment for the fracture would most likely be which of the following? Review Topic

Explanation
Question 98
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?
Explanation
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.
REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 99
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes? Review Topic
Explanation
Question 100
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
REFERENCES: O’Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: “Dancer’s Fracture.” Am J Sports Med 1996;24:240-243.
DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Hamilton WG: Foot and ankle injuries in dancers, in Yokum L (ed): Sports Clinics of North America. Philadelphia, PA, Williams and Wilkins, 1988.
