Orthopedic Board Review MCQs: Adult Reconstruction, Trauma & Ankle Part 97

Key Takeaway
This page presents Part 97 of a professional Orthopedic Surgery Board Review. It offers 100 high-yield, verified MCQs in OITE/AAOS format, authored by Dr. Mohammed Hutaif. Designed for orthopedic residents and surgeons, this quiz provides critical practice for AAOS and ABOS board certification exams.
About This Board Review Set
This is Part 97 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 97
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Hip, Nerve.
Sample Questions from This Set
Sample Question 1: A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsop...
Sample Question 2: Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?...
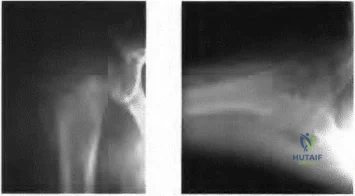
Sample Question 3: Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed sta...
Sample Question 4: Figure 70 is the radiograph of a 14-year-old girl with increasing posterior ankle pain, especially during pointe technique exercises. Nonsurgical measures such as modification, stretching, and injection have been unsuccessful. Which nerve i...
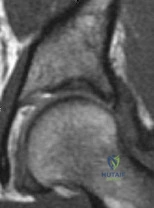
Sample Question 5: Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hippain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsophalangeal joint that was aggravated by weight bearing. A removable walker boot partially relieved the pain, and she was able to complete the season. Her pain has now returned; however, she denies any history of injury. Examination reveals tenderness over the medial sesamoid but no deformities. A radiograph and bone scan are shown in Figures 22a and 22b. What is the best treatment option at this time?
Explanation
REFERENCES: Sanders R: Fractures of the midfoot and forefoot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1601-1603.
Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals. Foot Ankle Int 2003;24:415-419.
Question 2
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?
Explanation
REFERENCES: Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Ritter MA, Keating EM, Faris PM: Closed wound drainage in total hip or total knee replacement: A prospective, randomized study. J Bone Joint Surg Am 1994;76:35-38.
Question 3
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include
Explanation
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
Question 4
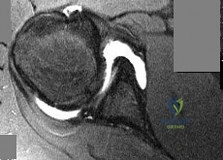
Figure 70 is the radiograph of a 14-year-old girl with increasing posterior ankle pain, especially during pointe technique exercises. Nonsurgical measures such as modification, stretching, and injection have been unsuccessful. Which nerve is most vulnerable to injury during endoscopic excision of this lesion?
Explanation
The pathology is that of posterior ankle impingement, which is secondary to a symptomatic os trigonum. Endoscopic excision necessitates posteromedial and posterolateral ankle portals. Although plantar numbness has been described as a relatively common postsurgical complication, the neurovascular structure most commonly injured is the sural nerve.
Question 5
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 6
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
Explanation
this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA.
Question 7
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.
Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.
Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 8
Figure 48 shows a current lateral radiograph of a 23-year-old man who sustained a closed femoral diaphyseal fracture 5 months ago. Treatment consisted of placement of a retrograde femoral nail for the femoral fracture. The patient now reports a sudden onset of pain in the midthigh and cannot bear weight on his leg. Management should consist of

Explanation
In Webb, et al. one hundred five consecutive patients with a diagnosis of delayed union (61 patients) or nonunion (44 patients) of the femoral shaft from February 1968 to November 1983 were managed by intramedullary reaming and nailing. The procedure was accomplished by closed techniques in 82 of the cases. Adequate follow-up study was obtained in 101 patients; all but four showed clinical and radiologic union at an average of 20 weeks following the procedure, with an overall union rate of 96%. The four patients whose fractures failed to consolidate with this treatment had repeat procedures with placement of thicker nails, and all subsequently healed.
The fracture pictured for this question is an oblique, distal 1/3 diaphyseal femur fracture with a butterfly fragment, an axially and rotationally unstable fracture configuration. The clinical history and x-ray are consistent with delayed union, therefore response #4 is the only sensible management option.
Question 9
A medial plate is best used to treat tibial plateau fractures when there is
Explanation
The patient's plain radiographs demonstrate a bicondylar tibial plateau fracture with complete separation of the diaphysis from the epiphysis, making this a Schatzker VI injury. Clinically, the patient is neurovascularly intact with symmetric palpable pulses, and ankle brachial indices are not necessary.
There is significant lateral tibial plateau displacement with the lateral femoral condyle down into the plateau defect. Considering the swelling, abrasions, and severity of the injury, a bridging external fixator is warranted followed by CT imaging.
The ligamentotaxis will provide better definition of the injury and joint fragments and allow for soft-tissue rest and subsidence of the swelling for eventual surgical intervention. Oblique views will not add as much information as CT imaging, which will show the bicondylar nature of the injury and the proximal tibia essentially split centrally with the tubercle as a separate fragment. A midline incision with medial and lateral plating has fallen out of
favor secondary to wound-healing complications. Comminution of the metaphysis or the lateral side is not an absolute indication for a medial plate. Open lateral fractures can still be managed with a laterally based plate depending on the soft-tissue injury.
RECOMMENDED READINGS
Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. View Abstract at PubMed Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: how does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma. 2007 May;21(5):301-6. PubMed PMID: 17485994. View Abstract at PubMed
Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. View Abstract at PubMed
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi:10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
View Abstract at PubMed
Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. PubMed PMID: 16882892. View Abstract at PubMed
Hall JA, Beuerlein MJ, McKee MD; Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:74-88. doi: 10.2106/JBJS.G.01165. PubMed PMID: 19255201. View Abstract at PubMed
Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. View Abstract at PubMed
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
Question 10
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of
Explanation
REFERENCES: Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibial physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Gruber HE, Phieffer LS, Wattenbarger JM: Physeal fractures: Part II. Fate of interposed periosteum in a physeal fracture. J Pediatr Orthop 2002;22:710-716.
Question 11
Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now reports progressive lower back pain and a feeling of being shifted to the right. If surgical intervention is considered, what is the most important goal in improving her health-related quality of life (HRQL) outcomes? Review Topic

Explanation
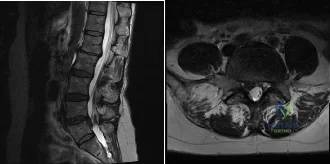
(SBQ12SP.24) A 39-year-old man presents to clinic with a 3-week history of low back pain that radiates to the right lower extremity. On examination, he has mildly decreased sensation over the dorsum of the foot and positive straight leg raise on the right side. MRI images are shown in Figure A and B. Which of the following is true regarding this patient's condition? Review Topic
Nonoperative management with NSAIDS and physical therapy is effective for 50% of patients
Surgical treatment is indicated in patients with diminished sensation
Surgical treatment is equivalent to nonoperative management in terms of pain and function
Good surgical outcome is associated with mainly back complaints
Size of disc herniations typically decrease over time without surgical intervention
The patient is presenting with a lumbar disc herniation at the L4-L5 level. The size of disc herniations decrease in most patients over time without surgical intervention.
Lumbar disc herniations are the result of recurrent torsional strain, which leads to small tears of the annulus fibrosus, ultimately allowing herniation of the nucleus pulposis. First line treatment consists of NSAIDS, muscle relaxants and physical therapy and is effective in 90% of patients. Second line treatment typically involves epidural and selective nerve root corticosteroid injections. Microdiscectomy is reserved for patients with more than 6 weeks of disabling pain that has failed nonoperative management, progressive weakness, or cauda equina syndrome.
In the Spine Patient Outcomes Research Trial (SPORT), Weinstein et al. investigated patient outcomes and satisfaction after operative and nonoperative management of lumbar disc herniations. While the randomized arm of the study did show statistically significant differences in the intent-to-treat analysis due to significant crossover of patients, the observational cohort revealed a significant improvement in pain, function, and disability for patients treated with surgery versus nonoperative measures.
Benson et al. looked at the natural history of massive herniated discs in 37 patients with 7-year follow up. They found a more than 60% reduction in disc size over this time period. Reduction in disc size did not correlate with clinical improvement.
Figure A and B are sagittal and axial T2 MRI images, respectively, showing a right sided lumbar disc herniation at the L4-L5 level.
Incorrect Answers:
Question 12
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 13
A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?
Explanation
REFERENCES: Waters PM, Stewart SL: Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84:915-920.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391-401.
Question 14
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
Question 15
A 12-year-old male sustains a ulnar fracture with an associated posterior-lateral radial head dislocation. After undergoing closed reduction, the radiocapitellar joint is noted to remain non-concentric. What is the most likely finding?

Explanation
Question 16
The use of bisphosphonates in children with osteogenesis imperfecta is becoming more widely accepted as treatment to improve quality of life and to decrease the risks of fracture. What is the mechanism by which bisphosphonates work?
Explanation
Question 17
Placing a plate too anteriorly against the lateral aspect of the bicipital groove while performing open reduction and internal fixation (ORIF) of a proximal humerus fracture has an increased risk of what complication?
Explanation
the other complications noted.
Question 18
A 65-year-old female presents with the injury seen in Figures A and B after a motor vehicle collision. She is hemodynamically unstable and undergoes emergent pelvic supra-acetabular external fixation followed by laparotomy. She is now hemodynamically stable and cleared for surgery. She has no evidence of neurologic deficit on examination. Which of the following factors is a relative contraindication to open reduction and plating of her posterior pelvic injury from an anterior approach?

Explanation
Posterior pelvic ring injuries that are unable to be reduced by closed techniques may require open reduction via anterior or posterior approaches. Relative contraindications to anterior approach include comminuted sacral fractures, morbid obesity, iliac wing external fixation, and ipsilateral diverting colostomy. In the presence of a comminuted sacral fracture, aggressive medial dissection would be required and would place the L5 nerve root at risk.
Simpson et al describe their initial results with open reduction and internal fixation of the SI joint via an anterior exposure in a series of 16 patients. They note that sacral alar comminution is a contraindication to the anterior approach
Jones provides an overview of the operative treatment of posterior pelvic ring injuries. He demonstrates reduction and fixation techniques via both anterior and posterior exposures.
Incorrect Answers:
Question 19
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
REFERENCES: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine lumbar spine study. Spine 2005;30:927-935.
Question 20
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a
Explanation
Question 21
Figures 128a and 128b show the radiograph and MRI scan of a 74-year-old woman with severe neck pain and upper extremity numbness, tingling, and clumsiness. She also reports that she has balance problems and sustained a distal radius fracture in a fall 6 months ago. Examination reveals hyperreflexia in bilateral quadriceps and Achilles reflexes, bilateral Hoffman's signs, and eight beats of clonus in both lower extremities. What is the best treatment option? Review Topic

Explanation
Question 22
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 23
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 24
An otherwise healthy 16-year-old boy who has had thoracolumbar pain with an increasingly worse deformity for the past 2 years now reports that the pain is worse at night. He responded well to nonsteroidal anti-inflammatory drugs initially, but they have become less effective. He denies any neurologic or constitutional symptoms. Examination is consistent with a mild thoracolumbar scoliosis and is otherwise normal. Laboratory studies show a normal CBC, erythrocyte sedimentation rate, and C-reactive protein. Standing radiographs show a 20 degrees left thoracolumbar scoliosis, and he has a Risser stage of 4. A bone scan shows increased uptake at L2; a CT scan through this level is shown in Figure 18. Management should now consist of
Explanation
REFERENCES: Cove JA, Taminiau AH, Obermann WR, Vanderschueren GM: Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine 2000;25:1283-1286.
Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Pettine KA, Klassen RA: Osteoid-osteoma and osteoblastoma of the spine. J Bone Joint Surg Am 1986;68:354-361.
Question 25
A 58-year-old woman has had a slowly progressing mass over the distal interphalangeal (DIP) joint of her dominant hand with a worsening deformity of her nail. She has no significant medical history but underwent bilateral knee arthroplasties 1 year ago. Radiographs reveal a small osteophyte at the DIP joint dorsally. A clinical photograph and a biopsy specimen are shown in Figures 76a and 76b. What is the most likely diagnosis?
Explanation
REFERENCES: Fritz GR, Stern PJ, Dickey M: Complications following mucous cyst excision. J Hand Surg Br 1997;22:222-225.
Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
Question 26
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 27
Amphotericin exerts antifungal activity by
Explanation
Question 28
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 29
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 30
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.
Question 31
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 32
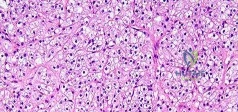
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 33
A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?
Explanation
REFERENCES: Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Clark CR, White AA III: Fractures of the dens: A multicenter study. J Bone Joint Surg Am 1985;67:1340-1348.
Question 34
- In revision hip arthroplasty, which of the following is the 5- to 10-year reported graft failure rate when using structural acetabular allografts in the repair of acetabular deficiencies?
Explanation
Question 35
What is the principal advantage of surgical repair for the lesion shown in Figure 19?
Explanation
REFERENCES: Bhandari M, Guyatt GH, Siddiqui F, et al: Treatment of acute Achilles tendon ruptures: A systematic overview and meta-analysis. Clin Orthop 2002;400:190-200.
Schepsis AA, Jones HE, Haas AL: Achilles tendon disorders in athletes. Am J Sports Med 2002;30:287-305.
Question 36
Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?
Explanation
REFERENCES: Green DP: Operative Hand Surgery, ed 2. New York, NY, Churchill Livingstone, 1988, pp 269-271.
Goldberg MJ, Meyn M: The radial clubhand. Orthop Clin North Am 1976;7:341-359.
Question 37
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of
Explanation
REFERENCES: Morrey BF: Distraction arthroplasty: Clinical applications. Clin Orthop 1993;293:46-54.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
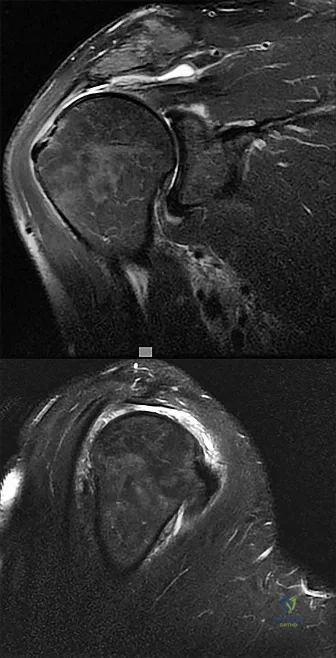
Question 38
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
Explanation
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.


Question 39
Figures 136a through 136c are the weight-bearing anteroposterior and lateral radiographs of a 28-year-old construction worker who has had 6 months of progressive knee pain isolated to the medial aspect of his right knee. The pain has not responded to nonsurgical treatment. His body mass index is 26. He has knee range of motion from 0 to 125 degrees, and his knee is stable to ligament examination. What is the most appropriate surgical treatment?
Explanation
Proximal tibial osteotomy is the best option for this young patient who has good range of motion and arthritis isolated to the medial compartment. Distal femoral osteotomy is more appropriate for correction of valgus deformity. In the setting of most varus deformities as shown in this patient’s radiographs, there is varus angulation of the proximal tibial. Correction of alignment at the femur results in obliquity of the joint line and abnormal loading. Medial
unicompartmental knee arthroplasty and TKA are less optimal in this setting because of this patient’s young age and high demands as a laborer. Unicompartmental knee arthroplasty and TKA are not preferred options for this patient because risk for premature failure is high.
Question 40
Figures 24a and 24b are the radiographs of a 7-year-old boy who fell off the monkey bars and has a closed injury. His hand appears warm and well perfused with an absent radial pulse. What is the best initial treatment?
Explanation
In displaced extension-type supracondylar fractures, the neurovascular structures get kinked anteriorly or anteromedially related to the displacement. In almost all cases, there is a spontaneous resolution of this kink following closed fracture reduction.
Question 41
A 52-year-old man has had groin and deep buttock pain for the past 2 months. Examination reveals that hip range of motion is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 28. Management should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip:. A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 42
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The AP radiograph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage? Review Topic

Explanation
Question 43
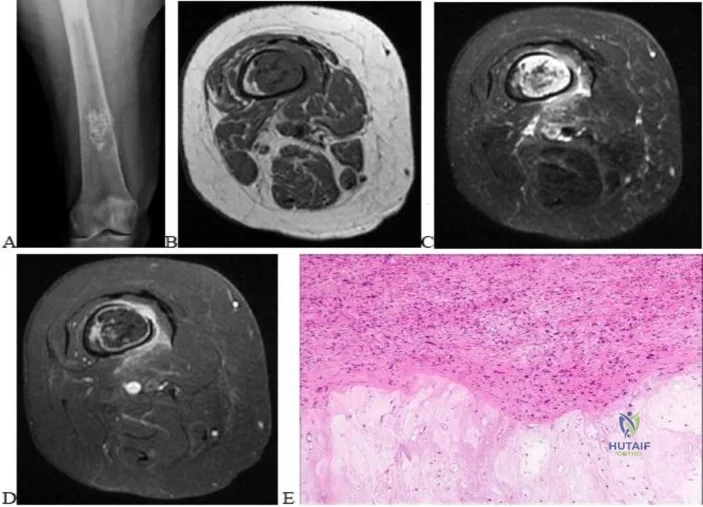
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
REFERENCES: Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 44
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and Review Topic
Explanation
Question 45
A lO'/z-year-old boy sustained the injury shown in Figure 72 when he fell out of a tree. This is a closed, neurologically intact injury and the patient has no head injury or loss of consciousness. He weighs 115 pounds and is otherwise healthy. What is the optimal treatment option for this injury?
Explanation
REFERENCES: Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295-1301.
Figure 73a Figure 73b
Question 46
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 307-317.
Rosenberg ZS, Cheung Y, Jahss MH, Noto AM, Norman A, Leeds NE: Rupture of the posterior tibial tendon: CT and MR imaging with surgical correlation. Radiology 1988;169:229-235.
Question 47
A 20-year-old girl reports a shoulder dislocation while reaching for a high shelf. Her history reveals multiple past dislocations with spontaneous reduction and no obvious traumatic event at onset. A photograph of her hand is shown in figure
Explanation
The first line of treatment for shoulder dislocations in patients with MDI should consist of physical therapy aimed at strengthening the rotator cuff and scapular stabilizers. For those who fail to respond to 3 to 6 months of nonsurgical treatment, surgical intervention can be considered with inferior capsular shift being the procedure of choice for multidirectional instability. Good results have been achieved with surgical procedures for posterior and multidirectional instability, but results have been less predictable than those achieved with procedures for traumatic anterior instability.
Ide et al. evaluated the results of an 8-week rehabilitation program with shoulder-strengthening exercises and a novel scapular-stabilizing shoulder orthosis in 46 patients with MDI. There was a significant increase in mean total scores on the modified Rowe grading system and mean torque of internal and external rotation with a normalization of mean external/internal torque ratios at the completion of the program. The authors concluded that shoulder strengthening exercises represent a
useful treatment option for patients with MDI.
Levine et al. reviewed treatments of multidirectional shoulder instability in athletes. Nonoperative management remains the initial treatment of choice. Open capsular shifts remain the operative treatment of choice, however, arthroscopic electrothermal capsulorrhaphy has become increasingly used as an alternative to an open approach.
Beasley et al. reviewed multidirectional instability in the shoulder of female athletes. The authors note that women tend to have greater ligamentous laxity than men and female athletes have a greater risk of converting laxity to symptomatic instability.
Figure A demonstrates metacarpophalangeal hyperextension, which is a sign of generalized ligamentous laxity.
Incorrect Answers:
Question 48
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical management has failed to provide relief. What is the treatment of choice?
Explanation
REFERENCES: Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.
Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
Question 49
A 32-year-old man underwent a total medial meniscectomy 2 years ago. He now reports pain and recurrent swelling for the past 3 months. Work-up includes full standing hip-knee-ankle radiographs, standing AP radiographs of both knees in full extension, an axial view of the patellofemoral joint, and a 45-degree flexion AP radiograph. Contraindication to meniscus allograft transplantation includes which of the following? Review Topic
Explanation
Question 50
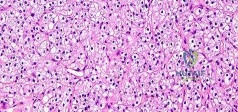
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
REFERENCES: Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
McDermott EM, Weiss AP: Glomus tumors. J Hand Surg Am 2006;31:1397-1400.
Question 51
Nutritional rickets in the US occurs more frequently in infants older than 6 months of age who do not receive vitamin D supplementation and are Review Topic
Explanation
Question 52
At a minimum 2-year follow-up and compared with the metacarpophalangeal (MCP) joint, pyrolytic carbon resurfacing arthroplasties of the proximal interphalangeal (PIP) joint
Explanation
Wall and Stern published a report on MCP joint pyrolytic carbon arthroplasty for osteoarthritis and another on PIP joint pyrolytic carbon resurfacing arthroplasty for osteoarthritis. They found different outcomes, and MCP joint implants outperformed PIP joint implants. Of eleven MCP joint arthroplasties, two produced asymptomatic squeaking and clicking, whereas eleven of 31 PIP joint implants produced this problem. No dislocations were reported among the MCP joint implants, but five PIP joint dislocations were observed. Outcomes were measured by the Michigan Hand Outcomes Questionnaire in both studies and were satisfactory for the MCP joint implants, with an average score of 80. The PIP implants did not fare as well, showing a higher degree of pain along with an average score of 53. The authors noted that, in the 15 patients in the PIP study who had unilateral surgery, the uninvolved, nonsurgical hand motion was actually statistically significantly (P<0.01) better than the surgical hand. MCP joint motion increased from 62º before surgery to 76º after surgery, whereas PIP joint motion got worse after surgery, with the average motion decreasing from 57º to 31º.
Question 53
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of
Explanation
REFERENCES: Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Muller EB, Nordwall A: Brace treatment of scoliosis in children with myelomeningocele. Spine 1994;19:151-155.
Question 54
Which of the following tumors have characteristic chromosomal translocations?
Explanation
REFERENCES: Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 55
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
Explanation
REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.
Question 56
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
REFERENCES: Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Hershman EB: Brachial plexus injuries. Clin Sports Med 1990;9:311-329.
Question 57
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?
Explanation
REFERENCES: Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Gie GA, Linder L, Ling RS, Simon JP, Slooff TJ, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Question 58
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
REFERENCES: Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed):
Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 59
Which of the following is more likely to occur with use of a bone patellar bone allograft instead of a bone patellar bone autograft for anterior cruciate ligament (ACL) reconstruction in an 18-year-old high school or collegiate athlete? Review Topic
Explanation
Many factors can potentially contribute to the failure of ACL reconstructions, including the surgical technique, the selection of graft material, the integrity of the secondary restraints, the condition of the articular and meniscal cartilage, and postoperative rehabilitation. Early failure, usually within the first 6 months, most often is the result of technical errors, incorrect or overly aggressive rehabilitation,
premature return to sports, or failure of graft incorporation. Later failure, usually after one year, is more typically the result of recurrent injury.
Kaeding et al. report data from the MOON multicenter research consortium. They present Level 2 evidence that the odds of graft rupture with an allograft reconstruction are 4 times higher than those of autograft reconstruction in athletes aged 10-19 years old. For each age, the number of autograft ACL reconstructions (ACLRs) performed to prevent one failure is as follows: 14 years, 7 ACLRs; 18 years, 8 ACLRs; 22 years,
11 ACLRs; 30 years, 25 ACLRs; 40 years, 50 ACLRs.
Krych et al. present a systematic review of prospective trials using BTB autograft and BTB allograft tissue for ACL reconstruction with a minimum 2-year follow-up. They found that BTB allograft patients were more likely to rupture their graft than BTB autograft patients (OR, 5.03; P = .01), however once irradiated and chemically processed allografts were excluded there was no statistical difference in graft re-rupture between the groups.
Greenberg et al. conducted a study of nearly 1300 patients and found no increased clinical risk of infection with the use of allograft tissue compared with autologous tissue for primary anterior cruciate ligament reconstruction.
Incorrect Answers:
1: There is no proven increased clinical risk of postoperative superficial or deep bacterial infection with the use of allograft tissue compared with autologous tissue for primary anterior cruciate ligament reconstruction. 2: There is no definitive data suggesting different arthritis progression rates based on autograft versus allograft. 4: Cyclops lesion formation is not related to graft choice. 5: There is some literature that tunnel osteolysis and enlargement is more common and greater with hamstring soft tissue grafts, however it does not appear to affect the clinical outcome in the first 2 postoperative years. There is no definitive data comparing BTB auto vs allograft in regards to tunnel osteolysis.
Question 60
A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?
Explanation
REFERENCES: Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3.
Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.
Fountas KN, Kapsalaki EZ, Karampelas I, et al: Results of long-term follow-up in patients undergoing anterior screw fixation for type II and rostral type III odontoid fractures. Spine 2005;30:661-669.
Question 61
Which local treatment option is most appropriate?
Explanation
This patient has a pathologic femur fracture. Her history of antecedent pain in the context of a previously well-functioning implant suggests that a new process such as dedifferentiation of a long-standing lesion may have occurred. The initial radiograph reveals a well-mineralized lesion within the intramedullary canal with punctate calcifications. This by itself suggests an enchondroma or low-grade chondrosarcoma. It is important to note that enchondromas in the long bones rarely cause pathologic fractures. This is not the case when they are present in the hands and feet, where enchondromas frequently have a more aggressive radiologic appearance and pose higher risk. Radiographic findings concerning for malignant dedifferentiation of an enchondroma
include cortical thinning or breach, a soft-tissue mass, or periosteal elevation. The pathologic fracture obscures the ability to identify these hallmarks of malignant degeneration.
Multiple myeloma, renal cell carcinoma, and osteolysis are all typically radiolucent. Implant-associated osteolysis lesions are commonly multiple and periarticular. The histopathology reveals a cartilage tumor. The chondroid tissue appears to be low grade. However, in an adjacent region there is a high-grade component seen both on the low-power view and the second higher-power sample that does not resemble cartilage. This is highly suggestive of a dedifferentiated chondrosarcoma. This component signifies that a portion of the original tumor (low-grade chondrosarcoma), which resembled the tissue of origin, converted into a different cell lineage with more aggressive properties (nearly any type of high-grade sarcoma). Dedifferentiated chondrosarcoma is a highly aggressive malignancy, with average 5-year survivals of less than 50%. As with most sarcomas, the most likely site of metastatic dissemination of chondrosarcoma is pulmonary. Consequently, standard staging entails a high-resolution CT scan of the lungs.
Serum protein electrophoresis and a skeletal survey are used for diagnosis of multiple myeloma. Positron emission tomography/CT fusion scans are used at many centers in the staging of osteosarcoma, but their role in chondrosarcoma staging is an emerging modality that is being investigated. Radiation is not typically used for local treatment of extremity chondrosarcoma. Extended curettage is not appropriate for a high-grade lesion such as this. Revision arthroplasty alone does not address the tumor. Wide resection is the local treatment of choice for high-grade chondrosarcoma; because of the fracture, this patient may require an amputation to achieve wide margins.
RECOMMENDED READINGS
Henderson ER, Pala E, Angelini A, Rimondi E, Ruggieri P. Dedifferentiated peripheral chondrosarcoma: a review of radiologic characteristics. Sarcoma. 2013;2013:505321. doi: 10.1155/2013/505321. Epub 2013 Mar 25. PubMed PMID: 23589702. View Abstract at PubMed
Grimer RJ, Gosheger G, Taminiau A, Biau D, Matejovsky Z, Kollender Y, San-Julian M, Gherlinzoni F, Ferrari C. Dedifferentiated chondrosarcoma: prognostic factors and outcome from a European group. Eur J Cancer. 2007 Sep;43(14):2060-5. Epub 2007 Aug 27. View Abstract at PubMed
Mavrogenis AF, Gambarotti M, Angelini A, Palmerini E, Staals EL, Ruggieri P, Papagelopoulos PJ. Chondrosarcomas revisited. Orthopedics. 2012 Mar 7;35(3):e379-90. doi: 10.3928/01477447-20120222-30. PubMed PMID: 22385450. View Abstract at PubMed
Flemming DJ, Murphey MD. Enchondroma and chondrosarcoma. Semin Musculoskelet Radiol. 2000;4(1):59-71. Review. PubMed PMID: 11061692. View Abstract at PubMed
Question 62
When performing a flexor tendon repair of a digit other than the thumb, what structures of the flexor tendon sheath should be preserved?
Explanation
REFERENCES: Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system.
J Hand Surg Am 1988;13:473-484.
Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 63
To control most spontaneous bleeding into the knee in children with hemophilia, factor VIII must be replaced to what percentage of normal?
Explanation
(per kg body weight) of factor VIII administered.
REFERENCES: Rodriquez-Merchan EC: Management of the orthopaedic complications of hemophilia. J Bone Joint Surg Br 1998;80:191-196.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 235.
Question 64
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
REFERENCES: Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
Clarke E, Robinson PK: Cervical myelopathy: A complication of cervical spondylosis. Brain 1956;79:486-510.
Question 65
A 12-year-old boy has a head-on head collision while playing soccer. He had no loss of consciousness but has persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
Explanation
Question 66
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
REFERENCES: Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38. 500.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 67
After open reduction and internal fixation of long bone fractures, at what time period should C-reactive protein start to decrease?

Explanation
The first referenced study by Waleczek et al noted that CRP was the earliest sign of developing infection and that clinical diagnosis, ultrasound, and WBC counts all lagged significantly behind CRP as a diagnostic tool. They report that latency to the clinical diagnosis based on clinical signs, ultrasound, WBC in blood and wound drainage was up to
14 days, while there was no patient with CRP increasing after day 2 without an infection.
The second referenced article by de Zwart et al noted an increased sensitivity and specificity of CRP as compared to ESR in the scenario of a clinically suspected infection. They advocate for determination of two CRP-levels with a short interval to screen for a clinically suspected infection.
Furthermore, Mok et al found that CRP showed an exponential decrease with a half-life of 2.6 days in postoperative spine patients. They found that CRP is a reliable test in the early postoperative period compared with ESR.
Question 68
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Explanation
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 69
-Thirty minutes later the gymnast is experiencing headache and difficulty concentrating. If her symptoms persist 1 week later, the next treatment step should be
Explanation
The National Collegiate Athletic Association’s (NCAA) 2011 revised health and safety guidelines regarding concussion management (available at www.ncaa.org) recommend no return to play on the same day of an injury. In particular, athletes sustaining a concussion should not return to play the same day as their injury. Before resuming exercise, athletes must be asymptomatic or returned to baseline symptoms at rest and have no symptoms with cognitive effort. They must be off of medications that could mask or alter concussion symptoms. Neurocognitive testing can be a helpful tool in determining brain function even after all symptoms of concussion have resolved. With a comparison baseline test, this evaluation, in conjunction with a physician’s examination, may reduce risk for second impact syndrome. The athlete’s clinical neurological examination findings (cognitive, cranial nerve, and balance testing) must return to baseline before resuming exercise. Research has shown that among youth athletes it may take longer for tested functions to return to baseline
(compared to the recovery rate in adult athletes). Brain MRI scan has no role in evaluating athletes for return to play in this situation.
Question 70
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
Explanation
Question 71
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
Explanation
REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.
Question 72
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
REFERENCES: Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 293-303.
Question 73
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Warner JJ, Higgins L, Parsons IM, et al: Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
Question 74
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
Question 75
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?
Explanation
REFERENCES: Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
McCarty EC, Warren RF, Deng XH, et al: Temperature along the axillary nerve during radiofrequency-induced thermal shrinkage. Am J Sports Med 2004;32:909-914.
Question 76
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Ramesh M, O’Byrne JM, McCarthy N, et al: Damage to the superior gluteal nerve after the Hardinge approach to the hip. J Bone Joint Surg Br 1996;78:903-906.
Question 77
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
Question 78
A 4-year-old child has droopy shoulders. Examination shows that the child has a large head, short stature, and a narrow chest. Radiographs of the spine and chest show absent clavicles, delayed ossification of the pubis and ischium, and mild coxa vara. What is the inheritance pattern for this condition?
Explanation
REFERENCES: Dietz FR, Mathews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Joint Bone Surg Am 1996;78:1583-1598.
Lee B, Thirunavukkarasu K, Zhou L, et al: Missense mutations abolishing DNA binding of osteoblast-specific transcription factor OSF2/CBFA1 in cleidocranial dysplasia. Nat Genet 1997;16:307-310.
AL-Madena Copy cU.u^Ml <UjJlU
Question 79
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?
Explanation
REFERENCES: Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 1146-1167.
Question 80
Figure 53 is a coronal-cut CT scan of a 63-year-old woman who has a longstanding pes planus. She is seen for lateral ankle discomfort. Upon examination she is tender over the sinus tarsi and distal to the fibula. She has painless passive hindfoot eversion with 5/5 eversion strength. The most appropriate diagnosis is

Explanation
With the use of CT scans, adults with symptomatic flatfoot deformity have been noted to develop subluxation of the talocalcaneal joint with resulting lateral hindfoot pain. Impingement of the talus and calcaneus in the sinus tarsi and/or between the tip of the fibula and the calcaneus may occur. This impingement is known as lateral impaction syndrome. Hindfoot motion is painless; therefore, this patient does not have symptomatic subtalar arthritis. Middle facet and calcaneonavicular coalitions are not present (hindfoot motion is present).
RECOMMENDED READINGS
Malicky ES, Crary JL, Houghton MJ, Agel J, Hansen ST Jr, Sangeorzan BJ. Talocalcaneal and subfibular impingement in symptomatic flatfoot in adults. J Bone Joint Surg Am. 2002 Nov;84-A(11):2005-9. PubMed PMID: 12429762. ? View Abstract at PubMed
Ananthakrisnan D, Ching R, Tencer A, Hansen ST Jr, Sangeorzan BJ. Subluxation of the talocalcaneal joint in adults who have symptomatic flatfoot. J Bone Joint Surg Am. 1999 Aug;81(8):1147-54. PubMed PMID: 10466647. ?View Abstract at PubMed
Question 81
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.
Question 82
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 83
A 20-year-old man has a symptomatic lesion of fibrous dysplasia in the femoral neck. Management should consist of
Explanation
REFERENCES: Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 197.
Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415.
Question 84
A 33-year-old woman reports a mass on the right hand that has been enlarging for 1 year. An intraoperative photograph is shown in Figure 28a, and a biopsy specimen is shown in Figure 28b. What is the most likely diagnosis?
Explanation
REFERENCES: Walsh EF, Mechrefe A, Akelman E, et al: Giant cell tumor of tendon sheath. Am J Orthop 2005;34;116-121.
Weiss SW, Goldblum JR (eds): Enzinger and Weiss’s Soft Tissue Tumors, ed 4. St Louis, MO, Mosby, 2001, pp 1038-1047.
Question 85
What is the most common long-term complication of the fracture shown in Figure 32?
Explanation
REFERENCES: Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Higgins TF, Baumgaertner MR: Diagnosis and treatment of fractures of the talus: A comprehensive review of the literature. Foot Ankle Int 1999;20:595-605.
Question 86
A 23-year-old male is involved in a motor vehicle accident and sustains a left open femur fracture, right open humeral shaft fracture, and an LC-II pelvic ring injury. Which of the following best describes the radiographic findings associated with this pelvic injury pattern using the Young-Burgess Classification system?

Explanation
Burgess et al discuss the effectiveness of a treatment protocol as determined by their pelvic injury classification and hemodynamic status. The injury classification system was based on lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury types. They found that their classification-based treatment protocols reduce the morbidity and mortality related to pelvic ring disruption.
Tile discusses acute pelvic trauma and his classification system for pelvic injuries (ie. Types A, B, and C). He states that any classification system must be seen only as a general guide to treatment, and that the management of each patient requires careful, individualized decision making.
Incorrect
2:
This
describes
an
APC-II
injury
3:
This
describes
an
APC-III
injury
4:
This
describes
and
LC-I
injury
Question 87
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis? Review Topic
Explanation
Question 88
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
Question 89
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
REFERENCES: Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 90
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
REFERENCES: Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233.
Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526.
Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 91
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of
Explanation
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 92
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
REFERENCES: Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Schulte KR, Callaghan JJ, Kelley SS, Johnston RC: The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up: The results of one surgeon. J Bone Joint Surg Am 1993;75:961-975.
Question 93
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. The athlete undergoes repair of the injury, and postsurgical radiographs are shown in Figures 1 and 2. At his first postsurgical visit, he reports no pain but describes weakness in his hand and decreased sensation over his lateral forearm. Upon examination, he has decreased 2-point discrimination over the lateral forearm and an inability to actively extend his thumb and fingers at the metacarpophalangeal joints. He can extend at the finger interphalangeal joints. He can extend his wrist weakly, and it deviates radially as he extends. His distal sensation is intact. Considering his examination findings, which two nerves are injured?

Explanation
elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
Question 94
In the initial evaluation of acute low back pain (duration of less than 4 weeks), plain radiographs are recommended in which of the following situations?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 95
Which of the following medications inhibits release of neurotransmitters by binding to presynaptic calcium channels?
Explanation
Gabapentin (also known as Neurontin) is a medication that is commonly used to treat neuropathic pain. It acts by binding the alpha2delta subunit of voltage-dependent calcium channels on the presynaptic membrane. This serves to increase GABA synthesis, as well as inhibit the release of excitatory neurotransmitters. These neurotransmitters are believed to be part of the pathway leading to neuropathic pain.
Bennett et al. provide a review of the pharmacology of gabapentin for the use of neuropathic pain. They note effective antihyperalgesic and antiallodynic properties of gabapentin but not significant anti-nociceptive action. Among patients with neuropathic pain they found an average pain score reduction of 2.05 points on an 11 point Likert scale, which compared favorably to placebo.
Mehta et al. explored outcomes of gabapentin and pregabalin (Lyrica) for use in patients with spinal cord injury. Both agents were found to decrease pain and secondary conditions such as sleep disturbance. They did not directly compare these agents to other analgesic medications.
Guy et al. present a meta-analysis of the use of anticonvulsants (such as gabapentin) to treat pain in patients with spinal cord injury. Large effect size was seen in 4 of 6 studies looking at the effectiveness of gabapentin.
Illustration A show the mechanism of currently available antiepileptic drugs (AEDs) that target several molecules at the excitatory synapse. Gabapentin and pregabalin bind to the a2d subunit of voltage-gated Ca2+ channels, which is thought to be associated with a decrease in neurotransmitter release.
Incorrect Answers
Question 96
A 45-year-old IV drug abuser has sternoclavicular (SC) joint pain for the past 2 weeks. He is afebrile and physical exam findings include point tenderness and swelling. He most likely has septic arthritis of the sternoclavicular joint. If so, what is the most likely infecting organism?

Explanation
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
Question 97
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
Explanation
REFERENCES: Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229.
Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.
Montella BJ; Nunley JA, Urbaniak JR: Osteonecrosis of the femoral head associated with pregnancy: A preliminary report. J Bone Joint Surg Am 1999;81:790-798.
Question 98
A 28-year-old professional football player reports painless loss of ankle motion after sustaining a “severe” ankle sprain 12 months ago. A mortise radiograph is shown in Figure 1. Surgical treatment should be reserved for which of the following conditions?
Explanation
REFERENCES: Whiteside LA, Reynolds FC, Ellsasser JC: Tibiofibular synostosis and recurrent ankle sprains in high performance athletes. Am J Sports Med 1978;6:204-208.
Henry JH, Andersen AJ, Cothren CC: Tibiofibular synostosis in professional basketball players. Am J Sports Med 1993;21:619-622.
Andrish J: The leg, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2155-2181.
Question 99
Figure 21 shows the radiograph of an 18-year-old man who was brought to the emergency department with shoulder pain following a rollover accident on an all-terrain vehicle. Examination reveals a fracture with massive swelling; however, the skin is intact and not tented over the fracture. Based on these findings, initial management should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR (eds): Disorders of the Shoulder. Philadelphia, PA, Lippincott, 1999, pp 632-635.
Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Question 100
An 76-year-old woman falls from standing and sustains the injury shown in Figure A. Her most recent T score was -1.9, 3 months prior to presentation. If labwork were performed, which values would be consistent with her bone density score?

Explanation
In the setting of osteopenia/osteoporosis, there is a positive feedback to increase PTH in response to low serum calcium levels. In response, there is a corresponding increase in alkaline phosphatase and decrease in phosphorous and circulating vitamin D levels.
Fraser writes a concise, yet thorough synopsis on primary and secondary hyperparathyroidism. In the article, the summary regarding osteopenia/osteoporosis (typically a state of hypovitamin D) begins by stating an initial state of decreased ionised calcium, which increases PTH, results in 3 primary effects: an attempt to increase gut absorption of Ca, mobilize Ca from the bone via osteoclasts and activate vitamin D at the kidney (1,25-vitamin D).
Figure A exhibits a left femoral neck fracture, which is a fragility fracture associated with poor bone density. Illustration A is a figure from Fraser's article exhibiting the feedback loop from the hypothalamus, pituitary, adrenal/glandular axis.
Incorrect answers:
