Comprehensive Introduction and Patho-Epidemiology
The reconstruction of congenital hand anomalies represents one of the most intellectually demanding and technically unforgiving disciplines within orthopedic surgery. It necessitates a profound, multi-dimensional understanding of pediatric biomechanics, microvascular anatomy, and the natural history of embryological failures. Among the most functionally critical reconstructions in this domain are the restoration of thumb opposition in the setting of thenar hypoplasia or aplasia, and the anatomical reorganization of central ray deficiencies (cleft hand). The human hand relies implicitly on the thumb for nearly all prehensile activities; without robust opposition, global hand function is severely compromised. The abductor digiti minimi (ADM) opponensplasty, originally described by Huber in 1921, remains a cornerstone technique for restoring this complex spatial movement, uniquely providing both biomechanical function and cosmetic thenar bulk.
To fully appreciate the patho-epidemiology of these conditions, one must examine the intricate embryological timeline of the upper extremity, which develops between the fourth and eighth weeks of gestation. Limb bud outgrowth and patterning are governed by highly conserved signaling centers: the Apical Ectodermal Ridge (AER) dictates proximodistal outgrowth via Fibroblast Growth Factor (FGF) signaling; the Zone of Polarizing Activity (ZPA) regulates anteroposterior (radioulnar) patterning via Sonic Hedgehog (Shh) expression; and the dorsal ectoderm controls dorsoventral patterning through Wnt7a signaling. Disruptions in these complex molecular cascades result in a spectrum of congenital anomalies. Thenar hypoplasia frequently manifests as a component of radial longitudinal deficiency, a failure of the pre-axial border of the upper limb often linked to Shh or Gli3 pathway aberrations. Conversely, isolated thenar aplasia is a rare entity, occasionally associated with Cavanagh's syndrome, where the thumb skeleton is normal but the intrinsic musculature is profoundly deficient.
Central deficiencies of the hand, historically and pejoratively termed "lobster claw" or "ectrodactyly," represent a distinct pathoanatomic spectrum characterized by the longitudinal failure of formation of the second, third, or fourth rays. In modern academic orthopedics, the preferred terminology is Cleft Hand or Central Longitudinal Deficiency. The true cleft hand (typical pattern) presents as a central V-shaped cleft, frequently associated with syndactyly of the border digits, and is inextricably linked to mutations in the Split Hand/Foot Malformation (SHFM) gene loci. This demonstrates an autosomal dominant mode of inheritance with variable expressivity and incomplete penetrance. The estimated incidence of true cleft hand is approximately 1 per 90,000 live births. According to the Centripetal Suppression Theory proposed by Maisels, this deformity represents a spectrum of central ray suppression, ranging from a simple soft-tissue cleft to progressive centripetal loss of the central osseous structures.
Conversely, the atypical pattern of central deficiency, as delineated by modern embryological studies by Ogino, is not a true cleft hand but rather a severe form of symbrachydactyly. This presents as a wide U-shaped deficiency, occurs sporadically without a predictable inheritance pattern, and lacks associated foot deformities. The surgical management of both thenar hypoplasia and central deficiencies requires meticulous classification, highly individualized preoperative planning, and staged reconstruction to optimize both prehension and cosmesis in the developing child. This masterclass delineates the operative nuances of the Huber opponensplasty and the academic framework surrounding the reconstruction of central hand deficiencies.
Detailed Surgical Anatomy and Biomechanics
Successful execution of the Huber transfer relies entirely on an exacting knowledge of the surgical anatomy of the hypothenar eminence and the preservation of the abductor digiti minimi's neurovascular pedicle. The ADM is the most superficial muscle of the hypothenar group. Its primary origin is the pisiform bone, with substantial fascial contributions from the tendon of the flexor carpi ulnaris (FCU) and the pisohamate ligament. Distally, the muscle transitions into two distinct tendinous slips: one inserts into the ulnar base of the proximal phalanx of the little finger, and the other inserts into the ulnar slip of the extensor expansion. This dual insertion provides the physiological function of abducting the little finger away from the central axis of the hand while assisting in the extension of the interphalangeal joints.
The critical neurovascular anatomy of the ADM dictates the limits of surgical mobilization. The muscle is innervated by the deep motor branch of the ulnar nerve. As the ulnar nerve exits Guyon's canal, it divides into superficial (sensory) and deep (motor) branches. The deep branch dives dorsally and radially between the ADM and the flexor digiti minimi brevis, sending a dedicated motor branch that enters the ADM on its deep, proximal, and radial aspect. The vascular supply mirrors this innervation, deriving from muscular branches of the ulnar artery that arborize in the same proximal-radial neurovascular hilum. Strict avoidance of dissection in this proximal-radial zone is mandatory; overzealous mobilization will result in catastrophic denervation or devascularization of the transfer.
Biomechanically, thumb opposition is a complex, multi-planar movement requiring sequential palmar abduction, flexion, and pronation of the first metacarpal, followed by flexion of the metacarpophalangeal (MCP) and interphalangeal (IP) joints. In the normal hand, this is primarily driven by the abductor pollicis brevis (APB) and the opponens pollicis. Unlike traditional tendon transfers (such as the flexor digitorum superficialis or extensor indicis proprius), which rely on a narrow tendinous vector, the Huber procedure transfers the entire ADM muscle belly to the thenar region. By mobilizing the ADM on its proximal pedicle and folding it over 180 degrees—akin to turning a page in a book—into the subcutaneous thenar space, the muscle's line of pull is fundamentally redirected. The deep surface of the ADM becomes superficial, and its distal tendinous insertions are sutured to the radial aspect of the thumb MCP joint. This creates a robust vector that perfectly mimics the APB, providing powerful pronation and palmar abduction while simultaneously reconstructing the cosmetic bulk of the deficient thenar eminence.
In the context of central deficiencies, the surgical anatomy is defined by the absence of normal structures and the presence of pathological deforming forces. The hallmark of the true cleft hand is the absence of the deep transverse metacarpal ligament between the divergent rays bordering the cleft. This ligament is essential for maintaining the transverse metacarpal arch; its absence leads to progressive splaying of the hand. Furthermore, transverse bones (cross-bones) may be present at the base of the cleft, acting as mechanical struts that force the border digits into further divergence as the child grows. The intrinsic musculature is often anomalous, with interossei frequently absent or aberrantly inserted into the cleft-bordering digits, exacerbating the rotational and angular deformities. Reconstruction demands not only the closure of the soft-tissue cleft but the anatomic reconstitution of the deep transverse metacarpal ligament to restore biomechanical stability to the metacarpal arch.
Exhaustive Indications and Contraindications
The decision to proceed with complex congenital hand reconstruction must be carefully weighed against the patient's functional deficit, anatomical variants, and overall systemic health. The Huber opponensplasty and cleft hand reconstructions are highly specialized procedures with specific inclusion criteria.
Indications for Abductor Digiti Minimi Opponensplasty
The Huber procedure is primarily indicated for pediatric patients presenting with absent or severely deficient thumb opposition, provided the thumb has a stable carpometacarpal (CMC) joint and adequate skeletal support. Specific indications include:
* Isolated Thenar Aplasia: A rare anomaly where the thumb skeleton and extrinsic tendons are intact, but intrinsic thenar musculature is absent. The Huber transfer provides both functional opposition and cosmetic thenar bulk.
* Radial Longitudinal Deficiency (Blauth Type II or IIIA): In hypoplastic thumbs where the CMC joint is stable but intrinsic muscles are deficient, the Huber transfer is utilized after or concurrent with MCP joint stabilization (capsulodesis or ulnar collateral ligament reconstruction).
* Post-Pollicization Augmentation: Patients who exhibit weakness in apposition and pinch strength following index finger pollicization for Blauth Type IIIB or IV thumb aplasia. The ADM can be transferred to the pollicized digit to enhance the pronation vector.
* Severe Median Nerve Palsy (Congenital or Early Acquired): In cases where the thenar muscles are profoundly atrophied and traditional tendon transfers are deemed insufficient for cosmetic restoration.
Indications for Cleft Hand Reconstruction
Surgical intervention for central deficiencies is indicated to improve prehension, close the aesthetic defect, and prevent progressive deformity.
* Progressive Splaying: Presence of transverse bones or an unyielding cleft that causes progressive divergence of the border digits.
* Syndactyly Release: Release of syndactyly between the border digits (especially the first web space) to restore independent motion and thumb opposition.
* Functional Deficit: Inability to perform stable pinch or grasp due to the absence of the central rays and the splaying of the metacarpal arch.
* Psychosocial Impact: Severe aesthetic deformity causing significant psychological distress as the child approaches school age.
| Parameter | Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Huber Opponensplasty | Blauth II/IIIA hypoplastic thumb; Isolated thenar aplasia; Post-pollicization weakness; Congenital median nerve palsy. | Absent or non-functional ADM; Ulnar nerve palsy; Unstable/absent CMC joint (Blauth IIIB/IV without prior pollicization); Severe vascular anomalies precluding pedicle survival. | Stiff or arthrogrypotic MCP joint; Severe soft-tissue contracture of the first web space (requires preliminary release). |
| Cleft Hand Reconstruction | Progressive metacarpal splaying; First web space syndactyly; Presence of transverse cross-bones; Severe aesthetic deformity (Flatt Groups 1-3). | Severe atypical symbrachydactyly where intervention would downgrade existing function; Medically unstable patient. | Mild Group 0 clefts with excellent function and no progressive splaying; Patient age < 6 months (anesthetic risks). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of successful congenital hand reconstruction. The clinical examination must assess the passive mobility of all joints, particularly the thumb CMC and MCP joints. A stiff CMC joint will negate the benefits of an opponensplasty, as the transferred muscle will be unable to mobilize the first metacarpal. In cleft hands, the flexibility of the border digits and the presence of syndactyly must be carefully documented. The functional status of the ulnar nerve and the ADM muscle must be confirmed clinically; the presence of a strong hypothenar contraction upon resisted little finger abduction is a prerequisite for the Huber procedure.
Standardized radiographic evaluation includes anterior-posterior, lateral, and oblique views of the hand and wrist. For thumb hypoplasia, radiographs are scrutinized to classify the deformity according to the Blauth system, specifically evaluating the presence and stability of the trapezium and the first metacarpal base. For cleft hands, radiographs are essential to identify transverse bones, aberrant metacarpal articulations, and the precise extent of the longitudinal deficiency according to Flatt's classification. In complex or syndromic cases, advanced imaging such as ultrasonography can be utilized to quantify the muscle bulk of the ADM prior to transfer. If severe vascular anomalies are suspected (e.g., in radial longitudinal deficiency), magnetic resonance angiography (MRA) or Doppler ultrasound may be indicated to map the vascular anatomy and ensure the safety of the ADM pedicle.
The timing of surgery is a critical consideration. For cleft hand reconstruction, surgery is typically performed between 6 and 18 months of age. This early intervention harnesses the innate neuroplasticity of the developing brain, allowing the child to integrate the reconstructed hand into their evolving motor patterns, while simultaneously preventing the progressive widening of the cleft by transverse bones. For the Huber opponensplasty, the procedure is often performed slightly later, typically between 2 and 5 years of age, to allow for sufficient growth of the ADM muscle belly, facilitating an easier transfer and a more robust functional outcome.
Patient positioning is standardized for both procedures. The patient is placed supine on the operating table with the affected upper extremity extended onto a radiolucent hand table. General anesthesia is employed. A well-padded pediatric pneumatic tourniquet is applied to the proximal arm. Tourniquet pressure is strictly regulated, typically set to 100 mmHg above the patient's systolic blood pressure, or generally 200-250 mmHg depending on the child's age and size. Exsanguination is achieved via gravity elevation or careful application of an Esmarch bandage, avoiding excessive compression of delicate congenital structures. The use of loupe magnification (3.5x to 4.5x) is considered mandatory by academic surgeons to ensure the meticulous dissection and preservation of the microscopic neurovascular pedicles.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of these procedures demands atraumatic soft-tissue handling and precise anatomical orientation. The following details the operative steps for the Huber Opponensplasty, followed by the principles of Cleft Hand closure.
The Abductor Digiti Minimi Opponensplasty (Huber Procedure)
1. Incision and Exposure
The procedure begins with the design of the hypothenar incision. Make an initial incision beginning over the ulnar border of the proximal phalanx of the little finger, extending proximally along the ulnar border of the palm. As the incision approaches the wrist, curve it radialward, crossing the wrist crease on the radial side of the pisiform to avoid crossing perpendicular to the flexion creases.
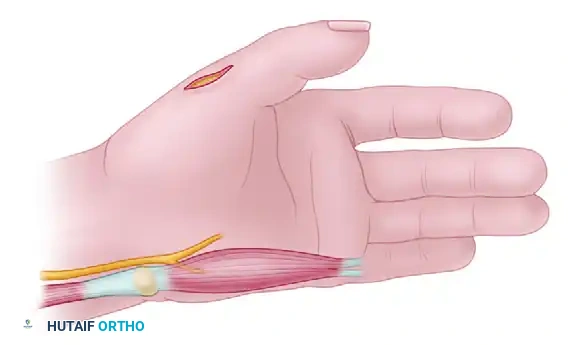
Elevate the skin flaps to expose the underlying hypothenar fascia. Identify the sensory branches of the ulnar nerve and carefully retract them to prevent painful postoperative neuromas.
2. Tendon Detachment
Proceed distally to identify the insertions of the ADM. The muscle typically exhibits a bifurcated insertion. Carefully detach the tendinous slip inserting into the extensor hood and the slip inserting into the base of the proximal phalanx of the little finger. It is critical to retain the maximum possible length of these tendinous slips, as this length is essential for secure, tension-free fixation at the thumb MCP joint.
Place a 4-0 non-absorbable locking traction suture (e.g., Ethibond or Prolene) into the detached tendon ends to facilitate manipulation during the subsequent proximal dissection.
3. Muscle Mobilization and Pedicle Preservation
Starting distally at the detached insertion, systematically dissect the ADM muscle belly out of its fascial sheath, elevating it proximally toward its origin at the pisiform and the FCU tendon. As the dissection proceeds proximally, extreme caution must be exercised. The deep motor branch of the ulnar nerve and the arterial branches from the ulnar artery enter the muscle on its deep, proximal, and radial aspect (the neurovascular hilum).
Strict avoidance of dissection in this specific proximal-radial zone is mandatory. Do not attempt to skeletonize the pedicle. The muscle should be freed sufficiently to allow it to reach the thumb without tension, but overzealous proximal dissection will inevitably result in denervation or devascularization, leading to complete failure of the transfer.
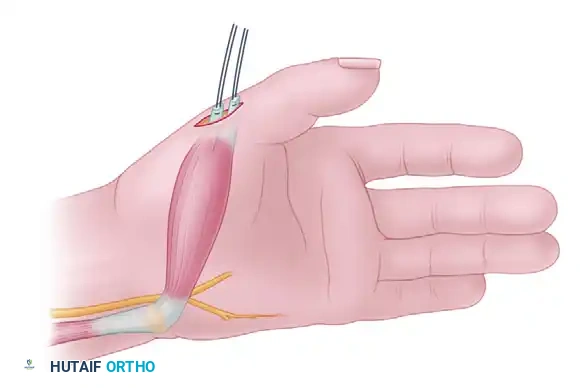
4. Tunnel Creation and Muscle Transfer
Make a second longitudinal or slightly curved incision over the dorsoradial aspect of the MCP joint of the thumb, exposing the extensor pollicis longus (EPL) tendon and the radial collateral ligament complex. Next, create a capacious subcutaneous tunnel connecting the thumb incision to the proximal aspect of the hypothenar incision across the palm. This tunnel must be wide enough to accommodate the entire bulk of the ADM muscle belly without any constriction.
Pass the mobilized ADM muscle through this tunnel. Ensure that the muscle glides freely. A tight tunnel will cause venous congestion, muscle ischemia, and necrosis. The critical biomechanical step is the rotation of the muscle: the ADM must be rotated 180 degrees on its longitudinal axis (like turning a page) so that its deep surface becomes superficial. This rotation optimizes the vector of pull, directing it from the pisiform toward the radial aspect of the thumb, perfectly mimicking the native abductor pollicis brevis.
5. Tendon Insertion Strategies and Fixation
The method of insertion at the thumb MCP joint is dictated by the specific pathoanatomy and the presence of joint instability:
* Isolated Thenar Aplasia with MCP Instability: These patients frequently present with profound MCP joint instability and a redundant ulnar capsule. First, stabilize the MCP joint by imbricating the redundant ulnar capsule in a robust "pants-over-vest" fashion using 4-0 clear PDS or non-absorbable sutures. Following stabilization, suture one of the ADM tendinous insertions to the radial capsule or the rudimentary APB insertion. Suture the second slip to the imbricated ulnar capsule and the EPL tendon. This dual insertion provides powerful abduction and extension-pronation vectors.
* Thenar Aplasia with Other Radial Anomalies: Suture one tendinous slip to the soft tissue at the radial aspect of the base of the proximal phalanx. Suture the second slip to the EPL tendon over the dorsal aspect of the MCP joint, as recommended by the classic techniques of Riordan, Powers, and Hurd.
* Post-Pollicization: If augmenting a pollicized index finger, suture one slip to the radial lateral band and the other to the central slip at the proximal interphalangeal (PIP) joint (which now functions as the new MCP joint) of the pollicized digit.
Fixation is performed with the thumb held in maximal palmar abduction and opposition. The tension should be set such that the thumb rests in an opposed position when the wrist is in neutral. Deflate the tourniquet prior to closure to achieve meticulous hemostasis and confirm the perfusion of the transferred muscle belly. Close the incisions using absorbable sutures (e.g., 5-0 chromic gut or Monocryl) to avoid the need for suture removal in a pediatric patient.
Principles of Cleft Hand Reconstruction
The surgical approach to the true cleft hand is highly variable and depends on the Flatt classification. The fundamental goals are the closure of the cleft, release of syndactyly, excision of deforming forces, and reconstruction of the deep transverse metacarpal ligament.
1. Incision Design and Flap Creation
The most critical aspect is the design of the skin flaps to reconstruct the first web space and close the central defect. The Snow-Littler procedure is a mainstay technique. It utilizes a broad, palmar-based flap from the skin of the cleft, which is elevated and transposed radially to reconstruct a deep, wide first web space. The index ray is subsequently transposed ulnarward to close the central defect. Alternatively, the Miura-Komedal procedure utilizes dorsal and palmar triangular flaps to achieve a similar release of the first web space and closure of the cleft.
2. Skeletal and Ligamentous Reconstruction
Once the flaps are elevated, identify and excise any transverse cross-bones at the base of the cleft. These bones act as wedges, driving the metacarpals apart. If the index ray is transposed ulnarward to close the gap (e.g., to the base of the third metacarpal), perform a precise osteotomy and fix the metacarpal using smooth Kirschner wires.
The most vital soft-tissue step is the reconstruction of the deep transverse metacarpal ligament between the index and ring metacarpals (or the adjacent digits bordering the cleft). This is typically achieved using heavy non-absorbable sutures (e.g., 2-0 or 3-0 Ethibond) passed through drill holes in the metacarpal heads, or by utilizing local tendon slips or fascial grafts. Failure to reconstruct this ligament will result in recurrent splaying of the hand.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, congenital hand reconstruction carries a distinct profile of complications. The delicate nature of pediatric tissues, combined with the inherent unpredictability of anomalous anatomy, requires the surgeon to be prepared for both acute and chronic postoperative challenges.
In the Huber opponensplasty, the most devastating acute complication is ischemia of the transferred muscle. This is almost universally iatrogenic, resulting either from overzealous proximal dissection that disrupts the neurovascular hilum, or from a subcutaneous tunnel that is too tight, leading to venous congestion and subsequent arterial inflow compromise. If the muscle appears congested upon tourniquet deflation, the tunnel must be immediately widened.
Chronic complications include stretching out of the transfer, resulting in a loss of the opposition vector. This is frequently due to unrecognized and unaddressed MCP joint instability at the time of the index procedure. If the MCP joint hyperextends during pinch, the force of the ADM is dissipated, and the transfer will eventually fail. Salvage requires secondary MCP joint stabilization (e.g., chondrodesis or formal arthrodesis in older children) and potential retensioning of the transfer.
In cleft hand reconstruction, the most common long-term complication is web creep or recurrence of the syndactyly, particularly in the reconstructed first web space. This occurs due to longitudinal growth of the child outstripping the growth of the scarred web space skin. Furthermore, failure to adequately reconstruct the deep transverse metacarpal ligament will lead to recurrent splaying of the metacarpal arch, destroying the aesthetic and functional result of the primary cleft closure.
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage Management / Prevention |
|---|---|---|---|
| ADM Ischemia / Necrosis | < 2% | Disruption of proximal-radial neurovascular hilum; Subcutaneous tunnel constriction causing venous congestion. | Prevention: Wide tunnel; avoid proximal skeletonization. Salvage: Debridement; secondary FDS or EIP tendon transfer once healed. |
| Loss of Opposition Vector | 10 - 15% | Unaddressed MCP joint instability; Inadequate initial tensioning; Stretching of the tendinous insertion. | Salvage: Secondary MCP joint capsulodesis, chondrodesis, or arthrodesis; Retensioning of the ADM insertion. |
| Recurrent Metacarpal Splaying | 15 - 20% | Failure to reconstruct or failure of the deep transverse metacarpal ligament repair; Retained transverse bones. | Prevention: Robust ligament reconstruction with heavy non-absorbable suture/graft. Salvage: Revision surgery with bone grafting and secondary ligamentous reconstruction. |
| Web Creep / Contracture | 20 - 30% | Differential growth between scar tissue and normal bone; Inadequate flap design during primary syndactyly release. | Salvage: Secondary Z-plasties, local tissue rearrangement, or full-thickness skin grafting to deepen the web space. |
| Neuroma Formation | < 5% | Injury to the superficial sensory branches of the ulnar nerve during hypothenar exposure. | Prevention: Careful loupe-assisted dissection. Salvage: Neuroma excision and burying the nerve stump into deep muscle tissue. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following pediatric congenital hand reconstruction differs fundamentally from adult tendon transfer protocols. The innate cortical plasticity of the developing child's brain allows for spontaneous integration of transferred muscles and reorganized digits into their global motor schema, largely obviating the need for the rigid, formal motor retraining and biofeedback required in adults. However, strict adherence to a phased immobilization protocol is critical to protect the delicate soft-tissue repairs and tendon insertions during the initial healing phases.
Phase I: Maximum Protection (0 to 3 Weeks Postoperative)
Immediately following surgery, the extremity is immobilized in the operating room. For the Huber procedure, a bulky, well-padded dressing is applied, reinforced with a custom fiberglass long-arm cast or a rigid thumb spica splint. The thumb must be held in maximal palmar abduction and opposition to remove all tension from the ADM insertion and the MCP capsulorrhaphy. For cleft hand reconstructions, a long-arm cast extending beyond the fingertips is utilized to protect the soft-tissue flaps, Kirschner wires, and ligament reconstructions. The elbow is typically flexed to 90 degrees to prevent the child from inadvertently removing the cast. Strict elevation is maintained for the first 48 to 72 hours to minimize edema.
Phase II: Controlled Mobilization and Splinting (3 to 6 Weeks Postoperative)
At approximately 3 to 4 weeks, the patient is brought to the clinic, and the initial rigid cast and bulky dressings are removed. If Kirschner wires were utilized for metacarpal stabilization in a cleft hand, they are typically removed at this stage in the clinic.
For the Huber transfer, the thumb is transitioned into a custom-molded thermoplastic thumb spica splint that continues to hold the thumb in opposition. This splint is worn full-time, removed only for hygiene and supervised therapy. During this phase, the child is actively encouraged to use the hand for light, play-based activities. The occupational therapist introduces age-appropriate toys (e.g., large blocks, soft balls) that encourage gross grasp and wide pinch, naturally recruiting the transferred ADM without applying excessive resistance.
Phase III: Integration and Strengthening (6 Weeks Postoperative and Beyond)
At 6 weeks postoperative, the tendinous insertions and capsular repairs are considered biologically secure. All rigid daytime splinting is discontinued. Some surgeons prefer to continue nighttime splinting for an additional 4 to 6 weeks to prevent contractures, particularly in the reconstructed first web space of a cleft hand.
The focus shifts entirely to spontaneous, play-based functional integration. The child is encouraged to engage in bilateral, bimanual activities. Formal strengthening exercises are rarely necessary; the child will naturally build strength in the transferred ADM as they incorporate the newly opposed thumb into their daily activities. Regular clinical follow-up is essential during the first year, and subsequently on an annual basis, to monitor for signs of web creep, recurrent splaying, or loss of the opposition vector as the child undergoes periods of rapid skeletal growth.
Summary of Landmark Literature and Clinical Guidelines
The academic foundation of congenital hand reconstruction is built upon decades of meticulous anatomical study and long-term clinical outcome tracking. A thorough understanding of this landmark literature is essential for the practicing orthopedic surgeon.
- Huber (1921): The foundational description of the abductor digiti minimi transfer. Huber recognized that transferring the entire muscle belly, rather than just a tendon, provided a unique solution for restoring both the biomechanics of opposition and the cosmetic contour of the thenar eminence in patients with severe poliomyelitis and congenital aplasia.
- **M
