Operative Management of Hand Trauma: Anesthesia, Tourniquet Protocols, and Vascular Reconstruction
Key Takeaway
The initial management of hand trauma requires meticulous attention to anesthesia, tourniquet application, and wound preparation. This guide provides an evidence-based approach to upper extremity arterial injuries, detailing indications for microvascular repair versus ligation. Proper execution of these foundational steps—combined with targeted antibiotic prophylaxis and precise debridement—is critical for optimizing functional outcomes and minimizing the risk of limb loss or deep infection.
INTRODUCTION TO HAND TRAUMA MANAGEMENT
The traumatized hand presents a complex anatomical and physiological challenge that demands a systematic, evidence-based approach. Successful restoration of function relies heavily on the foundational steps of surgical preparation: appropriate anesthesia, judicious tourniquet use, meticulous wound bed preparation, and precise management of vascular injuries. This masterclass provides an advanced, textbook-level analysis of these critical early phases of operative hand trauma management, designed for the practicing orthopedic consultant, fellow, and senior resident.
ANESTHESIA IN HAND SURGERY
The selection of an anesthetic modality is a critical preoperative decision that dictates not only patient comfort but also the surgeon’s ability to perform dynamic intraoperative assessments. A digital block, regional block, or general anesthetic may be selected depending on a multitude of factors: the patient’s age, medical comorbidities, the severity and anatomical extent of the injury, the presence of concomitant polytrauma, fasting status, and the potential need for distant flap coverage or autologous graft harvesting.
Digital and Regional Blocks
For isolated digital injuries, a well-executed digital block provides excellent anesthesia. Historically, the use of epinephrine in digital blocks was strictly contraindicated; however, contemporary evidence has thoroughly debunked the "no epinephrine in digits" myth. The use of lidocaine with epinephrine (1:100,000 or 1:200,000) is now considered safe in healthy patients and provides the added benefit of local hemostasis, often negating the need for a digital tourniquet.
Regional anesthesia (e.g., axillary, supraclavicular, or infraclavicular brachial plexus blocks) is the workhorse for extensive hand and wrist trauma. It provides profound intraoperative anesthesia, excellent muscle relaxation, and prolonged postoperative analgesia, which is highly beneficial for mitigating vasospasm following microvascular repair.
General Anesthesia
General anesthesia is reserved for specific indications:
* Pediatric patients or uncooperative adults.
* Polytrauma patients requiring simultaneous interventions by multiple surgical teams.
* Complex reconstructions requiring prolonged operative times (e.g., major replantations exceeding 4-6 hours).
* Procedures necessitating the harvest of distant tissue (e.g., latissimus dorsi free flap, sural nerve graft, or iliac crest bone graft).
CLINICAL PEARL:
The advent of WALANT (Wide Awake Local Anesthesia No Tourniquet) has revolutionized hand surgery. By utilizing a tumescent mixture of lidocaine and epinephrine, surgeons can perform complex tendon repairs and tenolyses while actively assessing the patient's active range of motion intraoperatively, ensuring the integrity and excursion of the repair before skin closure.
TOURNIQUET PRINCIPLES AND APPLICATION
A pneumatic tourniquet is indispensable during the initial phases of hand trauma surgery. It provides a bloodless field, which is absolutely necessary while the wound is being cleansed, inspected, and while delicate deep structures (nerves, vessels, tendons) are being identified and repaired.
Exsanguination Techniques and Crush Injuries
Standard exsanguination is typically achieved by tightly wrapping the extremity with an elastic Esmarch or Martin bandage from distal to proximal prior to tourniquet inflation. However, this technique is strictly contraindicated in specific trauma scenarios.
🚨 SURGICAL WARNING:
For a large wound associated with fractures, severe crush injuries, or avulsions, wrapping the limb with an elastic bandage can cause catastrophic displacement of fracture fragments, further soft tissue crushing, and potential embolization of thrombi or fat.
In these high-risk scenarios, exsanguination should be achieved by simple elevation of the hand and arm for 2 to 3 minutes prior to tourniquet inflation. This utilizes gravity to drain venous blood without applying compressive shearing forces to the traumatized tissues.
Ischemia Time and Tissue Viability
When the viability of an area of skin or a digit is questionable due to a crushing or avulsing mechanism, the tourniquet should be used as briefly as possible. Prolonged ischemia exacerbates cellular hypoxia and reperfusion injury in already compromised tissues.
* Standard Pressure: Typically set at 250 mm Hg for adults, or 100 mm Hg above the patient's systolic blood pressure.
* Time Limits: Ischemia time should generally not exceed 120 minutes. If prolonged surgery is required, the tourniquet should be deflated for 15 to 20 minutes to allow for reperfusion and clearance of anaerobic metabolites before re-inflation.
WOUND PREPARATION: CLEANSING, IRRIGATION, AND DRAPING
The fate of a traumatized hand is often sealed during the initial debridement and irrigation. After the patient is anesthetized and the tourniquet is applied, the first aid dressing is removed under sterile conditions.
Irrigation Mechanics
The wound must be thoroughly irrigated with sterile normal saline solution. A pulsating lavage apparatus is generally preferred, as it provides a stream with sufficient mechanical force to dislodge small foreign particles, soil, and large hematomas that serve as a nidus for infection.
PITFALL:
Antiseptic solutions (e.g., chlorhexidine gluconate, povidone-iodine, hydrogen peroxide) should never be used directly within the open wound bed. These agents exhibit profound tissue toxicity, destroying viable fibroblasts, osteoblasts, and chondrocytes, thereby severely delaying wound healing and increasing the risk of tissue necrosis. Antiseptics are strictly reserved for intact skin preparation surrounding the wound.
Principles of Debridement
Debridement must be systematic and tissue-specific:
* Vessels: Small bleeding vessels, which are often more easily visualized when floating under a pool of saline, are clamped with mosquito hemostats and cauterized or ligated.
* Fat and Fascia: Small flaps and tags of devitalized fat and fascia seen floating in the solution are highly susceptible to necrosis and infection; they must be sharply excised at their bases.
* Nerves and Tendons: Nerve ends and tendons are not aggressively debrided. Even if ragged, their length must be preserved to facilitate primary or secondary repair without tension.
* Skin: Ragged skin edges may be sharply trimmed to healthy, bleeding margins, but skin excision in the hand must be highly conservative to prevent coverage deficits.
EVIDENCE-BASED ANTIBIOTIC PROPHYLAXIS
The administration of prophylactic antibiotics in hand trauma must be stratified by the mechanism of injury, the degree of contamination, and the host's immune status. Indiscriminate use of broad-spectrum antibiotics contributes to resistance and provides no clinical benefit in low-risk wounds.
Risk Stratification and Pathogen Targeting
- Low-Risk, Traumatic Injuries: Clean wounds with easily demarcated borders and no devitalized tissue require no antibiotic prophylaxis. Thorough irrigation and primary closure are sufficient.
- Immunocompromised Hosts: Patients with diabetes mellitus, HIV, or those on immunosuppressive therapy should receive Gram-positive cocci coverage (e.g., first-generation cephalosporins like Cefazolin) even for relatively clean wounds.
- Contaminated Wounds / Devitalized Tissue: If the wound, tendon sheath, or joint space is contaminated, aggressive surgical debridement is the primary treatment. This is supplemented with Gram-positive cocci coverage.
- Animal and Human Bites: These are high-risk injuries. Prophylaxis must cover Pasteurella multocida (cats/dogs) and Eikenella corrodens (humans). Amoxicillin-clavulanate potassium (Augmentin) is the gold standard. In penicillin-allergic or immunocompromised patients, consider erythromycin, doxycycline, or a combination of ciprofloxacin and clindamycin.
- Severe Sepsis / Petechial Rash: Patients presenting with systemic toxicity require immediate hospitalization, blood cultures, and broad-spectrum intravenous coverage (e.g., Ciprofloxacin and Clindamycin).
MANAGEMENT OF UPPER EXTREMITY ARTERIAL INJURIES
Vascular injuries in the upper extremity demand rapid identification and precise microsurgical management to prevent catastrophic limb loss or ischemic contracture. A 15-year epidemiological study of upper extremity arterial injuries (167 patients, 189 arterial injuries) identified the brachial artery as the most frequently injured vessel (55%).
Vascular Assessment
Clinical evaluation begins with the assessment of capillary refill, skin turgor, temperature, and the Allen test. It is critical to remember that the ulnar artery is the dominant blood supply to the hand in the majority of patients, and anatomical variations exist where the ulnar artery does not have a connection with the superficial palmar arterial arch.
Pulse volume measurements, handheld Doppler ultrasonography, and digital oximetry are invaluable adjuncts in assessing the adequacy of circulation to the hand and individual digits.
Radial and Ulnar Artery Injuries: Ligation vs. Repair
The decision to ligate versus repair a transected radial or ulnar artery depends on patient age, collateral circulation, and concomitant nerve injury.
- Indications for Ligation: If an injury involves only one artery (e.g., isolated radial artery laceration) in a young, healthy patient without associated nerve injury, and the intact artery provides robust, pulsatile collateral circulation to the entire hand (confirmed by a negative Allen test and intraoperative Doppler), simple ligation remains a safe and satisfactory option.
- Indications for Primary Repair: In both younger and older patients with inadequate collateral circulation through the intact artery, repair is mandatory. Furthermore, if a concomitant nerve injury is present (e.g., ulnar artery and ulnar nerve transection at the wrist), repair of the injured artery is highly preferable. Restoring pulsatile flow optimizes the vascular bed for the regenerating nerve, significantly improving functional outcomes.
- Bilateral Transection: If both the radial and ulnar arteries are transected, repair of both arteries should be attempted, especially in older patients and those with extensive soft tissue or nerve damage.
CLINICAL PEARL:
In a definitive series of 28 patients with upper extremity arterial injuries treated at an urban trauma center, the overall limb salvage rate was 96%. Most were managed with primary repair or ligation; however, six required reversed saphenous vein bypass grafts due to zones of crush injury precluding tension-free primary anastomosis. Never attempt a primary microvascular anastomosis under tension; always interpose a vein graft if a gap exists after debridement to healthy intima.
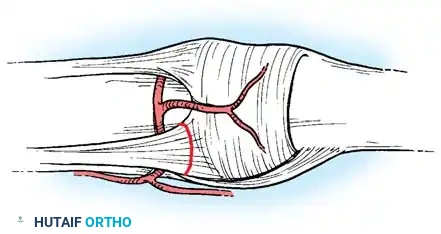
Palmar Arch and Digital Artery Trauma
Injuries to the superficial/deep palmar arterial arches and the digital arteries require formal microsurgical exploration and repair if circulatory impairment threatens digital viability.
* Microvascular Techniques: These injuries necessitate the use of an operating microscope, systemic heparinization (if not contraindicated), and meticulous adventitial stripping to prevent thrombogenic material from entering the lumen.
* Ischemic Digits: A digit that remains pale and pulseless after fracture reduction and rewarming requires immediate exploration of the digital vessels.
Prognostic Factors and Limb Salvage
Risk factors for limb loss in upper extremity vascular trauma include:
* Early microvascular graft failure or thrombosis.
* Missed or delayed diagnosis of compartment syndrome.
* Associated massive skeletal comminution and brachial plexus avulsion.
* High-velocity military mechanisms of injury (blast/fragmentation).
Furthermore, evidence indicates that arterial injuries caused by blunt trauma (crush/traction) yield worse functional outcomes than those caused by sharp penetrating trauma. Blunt trauma causes extensive intimal damage far beyond the macroscopic zone of injury, necessitating wider vascular resection and a higher reliance on vein grafting.
POSTOPERATIVE PROTOCOLS
Following complex hand trauma surgery, particularly cases involving vascular repair, the postoperative protocol is as critical as the surgery itself.
* Monitoring: The replanted or revascularized limb must be monitored hourly for the first 24-48 hours using clinical observation (color, capillary refill, temperature) and surface temperature probes. A drop in temperature >2°C compared to the control digit is highly suggestive of vascular compromise.
* Positioning: The hand should be elevated slightly above heart level to promote venous drainage while not compromising arterial inflow.
* Pharmacotherapy: Depending on the surgeon's preference and the nature of the vascular repair, postoperative antithrombotic therapy may include aspirin, low-molecular-weight heparin, or dextran infusions, though evidence for the latter remains controversial.
* Rehabilitation: Early, protected mobilization under the guidance of a specialized hand therapist is initiated as soon as the soft tissue and skeletal stability allow, to prevent tendon adhesions and joint contractures.
You Might Also Like