Operative Management of Fracture Nonunions: A Comprehensive Guide

Key Takeaway
Fracture nonunion represents a profound failure of the osteogenic process, demanding meticulous surgical intervention. This comprehensive guide details the systemic and local etiologies, Weber-Cech and Paley classification systems, and evidence-based operative strategies. Emphasizing the critical balance between biomechanical stability and biological vitality, it provides orthopedic surgeons with step-by-step protocols for managing hypertrophic and atrophic nonunions, optimizing soft-tissue envelopes, and executing advanced fixation techniques to achieve definitive osseous union.
Introduction to Fracture Nonunion
Despite the multitude of biomechanical and biological studies dedicated to fracture healing, establishing a universally accepted, rigid criterion for declaring a fracture a "nonunion" remains clinically challenging. A diagnosis of nonunion is fundamentally a clinical and radiographic determination, justified only when evidence unequivocally demonstrates that the biological process of healing has ceased and that osseous union is highly improbable without surgical intervention.
In 1986, for the purposes of standardizing the testing of bone-healing devices, a U.S. Food and Drug Administration (FDA) panel defined a nonunion as being established "when a minimum of 9 months has elapsed since injury and the fracture shows no visible progressive signs of healing for 3 months." However, as practicing orthopedic surgeons recognize, this rigid temporal criterion cannot be universally applied across all anatomical locations and injury patterns.
For instance, a fracture of the shaft of a long bone (e.g., the tibial diaphysis) should generally not be considered a nonunion until at least 6 months post-injury, as the physiological timeline for union often requires extended duration, particularly in the presence of local complications such as severe soft-tissue stripping or subclinical infection. Conversely, an intracapsular fracture of the femoral neck, which lacks a robust periosteal blood supply, can often be definitively diagnosed as a nonunion after only 3 months of radiographic stagnation.
Etiology and Pathophysiology
The exact pathogenesis of delayed union and nonunion is multifactorial, representing a failure in the "Diamond Concept" of fracture healing: osteogenic cells, osteoconductive scaffolds, osteoinductive growth factors, and a stable mechanical environment. Both systemic and local factors profoundly influence this delicate equilibrium.
Systemic Factors
Systemic contributors to nonunion include the patient’s baseline metabolic state, nutritional status, endocrine health (e.g., diabetes mellitus, thyroid dysfunction), and overall activity level.
Tobacco Use: The use of tobacco is one of the most significant, modifiable systemic risk factors implicated in the development of nonunions. Nicotine acts as a potent vasoconstrictor, decreasing microvascular arborization at the fracture site. Castillo et al. demonstrated that nicotine not only decreases vascularization but also significantly increases the susceptibility to osteomyelitis. Kyro et al. reported a statistically significant increase in tibial nonunions among smokers compared to nonsmokers. Furthermore, Hak et al. highlighted that tobacco use detrimentally impacts the success rates of secondary interventions, such as exchange reamed intramedullary nailing for femoral shaft nonunions. Physiologically, smokers exhibit decreased tissue oxygen tension in cutaneous and subcutaneous tissues, leading to compromised wound healing and impaired osteogenesis.
Clinical Pearl: Even though approximately 50% of smokers relapse into their habit, absolute abstinence must be mandated during the perioperative and postoperative phases of nonunion treatment to optimize the biological milieu for bone and soft-tissue healing.
Nonsteroidal Anti-inflammatory Drugs (NSAIDs): The role of NSAIDs in fracture healing remains a topic of intense academic debate. NSAIDs inhibit cyclooxygenase (COX) enzymes, thereby decreasing prostaglandin E2 (PGE2) synthesis, which is critical for endochondral ossification. Multiple animal models have demonstrated that NSAIDs decrease fracture healing rates. While human studies present conflicting data—with some refuting the hypothesis that NSAIDs delay healing—the potential risk warrants caution. We strongly suggest that patients with a delayed union or established nonunion abstain from using NSAIDs or systemic corticosteroids during their fracture treatment.
Local Factors
Local factors dictate the immediate biological and mechanical environment of the fracture. In a landmark review of 842 long-bone nonunions by Boyd, Lipinski, and Wiley, nonunions were found to be significantly more common when fractures were:
1. Open injuries with periosteal stripping.
2. Complicated by deep infection.
3. Segmental, resulting in impaired medullary and periosteal blood supply (usually to the intercalary segment).
4. Highly comminuted due to high-energy trauma.
5. Insecurely fixed, leading to excessive strain (violating Perren’s strain theory).
6. Immobilized for an insufficient duration.
7. Treated by ill-advised, biologically destructive open reduction techniques.
8. Distracted, either by excessive skeletal traction or by poorly applied plate-and-screw constructs.
9. Located in previously irradiated bone.
Heppenstall et al., analyzing 185 tibial nonunions, noted that 92.4% of patients had an initial delay in weight-bearing exceeding 6 weeks. The severity of the initial soft-tissue injury, postoperative infection following primary closure, the presence of an intact fibula (which can hold the tibia in distraction), and location in the distal third of the tibia (an area of precarious vascularity) are critical local determinants.
Green, Moore, and Spohn’s review of 72 tibial shaft nonunions revealed that 76% occurred following open fractures, and 51% were infected. This underscores the modern orthopedic consensus: the development of a nonunion is often more closely related to the severity of the initial soft-tissue injury than to the specific method of initial osseous stabilization.
Epidemiology and Incidence
The incidence of nonunion varies significantly depending on the specific bone, the energy of the injury, and the primary treatment modality. Historically, the tibia and femur shared high rates of nonunion. However, with the advent and widespread adoption of interlocking intramedullary (IM) nails for acute femoral fracture management, femoral nonunions have become exceedingly rare (approximately 1% in our institutional experience of over 2,500 cases).
Conversely, due to the subcutaneous nature of the tibia and its susceptibility to severe, high-energy open fractures with concurrent soft-tissue devastation, the tibia remains the most frequent site of long-bone nonunion (approximately 2% even with IM nailing, and significantly higher in open fractures).
Preoperative Evaluation and Optimization
Successful management of a nonunion requires meticulous preoperative planning, addressing both the host and the local environment.
Status of Soft Tissues and Neurovascular Structures
With contemporary advancements in bone grafting, orthobiologics, and internal/external fixation, definitive surgery can often be performed earlier. However, the condition of the soft-tissue envelope surrounding the nonunion is the primary rate-limiting step.
Unyielding scar tissue, particularly on the concave side of an angular deformity, may result in catastrophic skin necrosis upon acute correction. Deep scarring may preclude local bone transport or the application of massive bone grafts. The necessity for soft-tissue coverage (e.g., rotational or free tissue transfer) must be integrated into the treatment algorithm early.
Surgical Warning: Soft-tissue contractures must be carefully evaluated if the nonunion treatment involves lengthening the extremity. Acute lengthening stretches neurovascular structures and tight fascial compartments, risking neurapraxia or compartment syndrome.
In patients with a history of high-energy trauma, vascular injuries, or diminished peripheral pulses, a preoperative arteriogram or CT angiogram is mandatory. Significant vascular abnormalities must be corrected by a vascular surgeon prior to, or concomitant with, orthopedic intervention. Nerve injuries must be documented; occasionally, an extremity must be intentionally shortened to facilitate primary repair of a nerve defect. If nerves are irreparably damaged resulting in an insensate, flail lower extremity, amputation (e.g., below-knee amputation) is often the most functional and practical choice.

Classification of Nonunions
The status of the bone ends at the nonunion site dictates the surgical strategy. The most widely utilized classification systems are those of Weber and Cech (based on biological viability) and Paley (based on bone loss and deformity).
Weber and Cech Classification
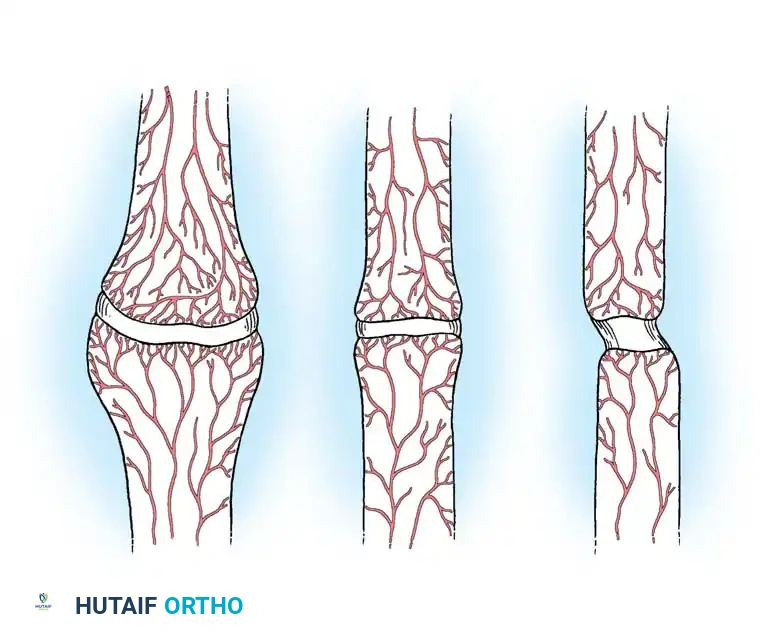
Weber and Cech classified nonunions into two primary categories based on the viability and vascularity of the fracture ends, historically demonstrated by strontium-85 uptake studies.
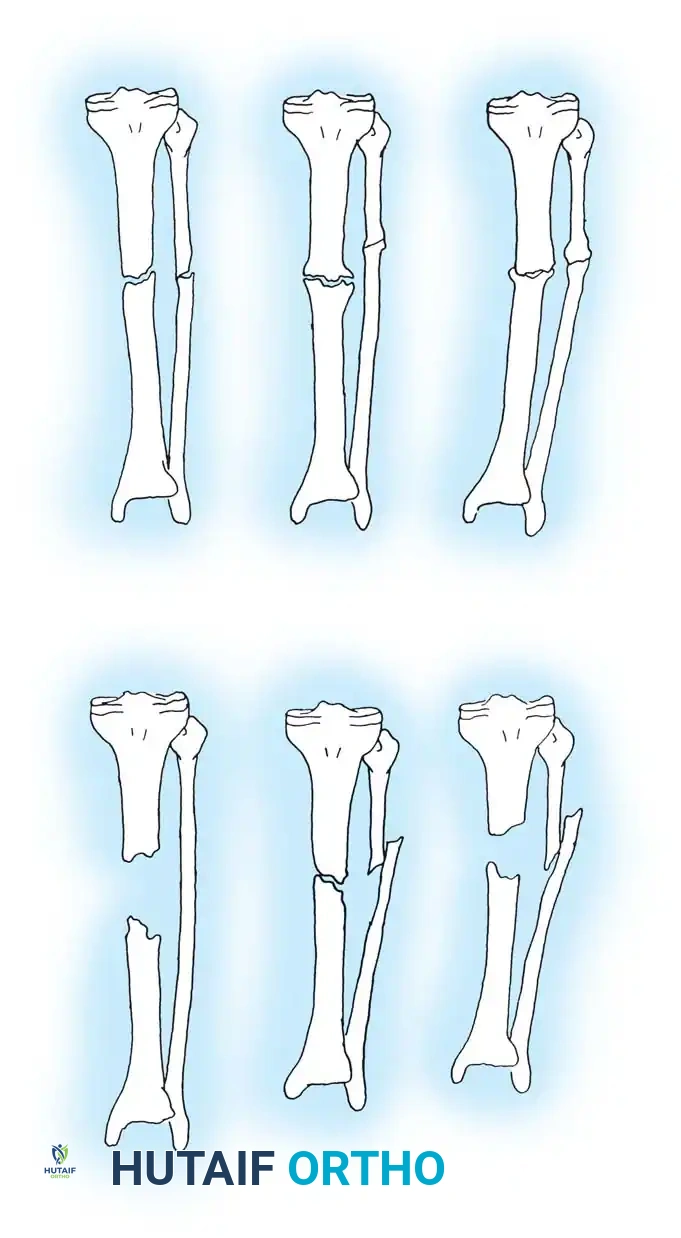
1. Hypervascular (Hypertrophic or Viable) Nonunions:
These nonunions possess a rich blood supply and are biologically capable of mounting a healing response. The failure here is mechanical (instability). They are subdivided into:
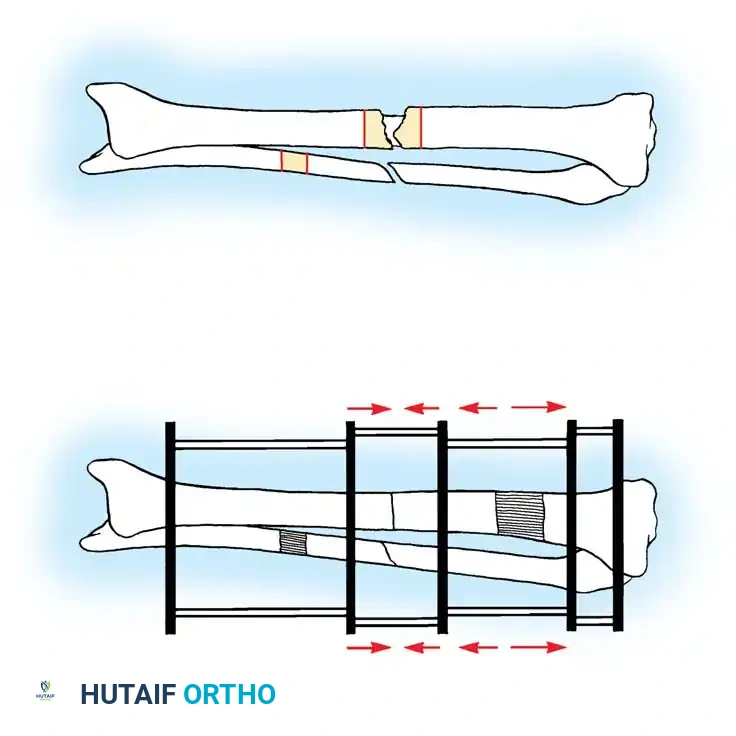
* "Elephant foot" nonunions: Hypertrophic and rich in exuberant callus. They result from insecure fixation, inadequate immobilization, or premature weight-bearing in a well-reduced fracture.
* "Horse hoof" nonunions: Mildly hypertrophic with poor callus formation. Typically seen after moderately unstable fixation (e.g., a loose plate). The bone ends show insufficient callus and mild sclerosis.
* Oligotrophic nonunions: Not hypertrophic, but biologically vascular. Callus is absent. These occur after major displacement, distraction of fragments, or internal fixation without accurate cortical apposition.
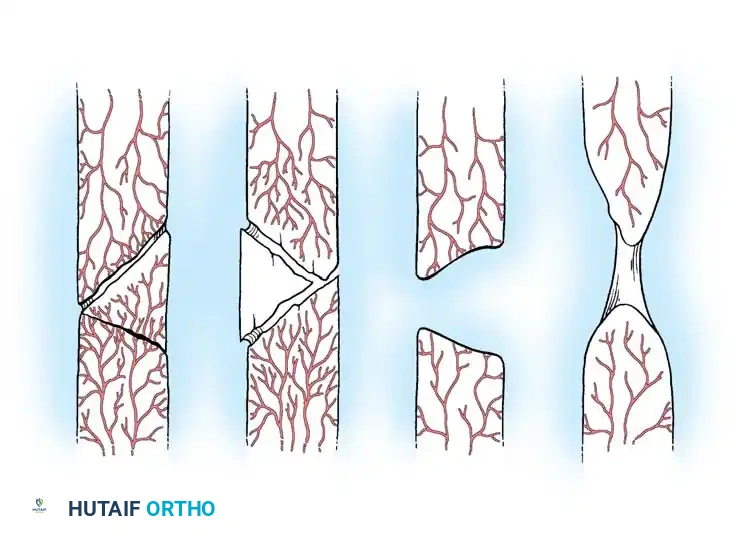
2. Avascular (Atrophic or Inert) Nonunions:
These nonunions lack biological reaction and have poor blood supply. They are incapable of uniting without biological intervention (decortication and bone grafting). They are subdivided into:
* Torsion wedge nonunions: Characterized by a necrotic intermediate butterfly fragment that has healed to one main fragment but not the other. Often seen after rigid plating that strips the periosteal supply of the wedge.
* Comminuted nonunions: Multiple necrotic intermediate fragments with an absolute absence of callus. Often results from catastrophic failure (breakage) of a primary fixation plate.
* Defect nonunions: Characterized by a segmental diaphyseal bone loss. The main fragment ends are viable, but the gap exceeds the biological capacity for bridging. Common after severe open fractures, tumor resections, or osteomyelitis debridement.
* Atrophic nonunions: The end-stage result where intermediate fragments are missing or resorbed, replaced by inert scar tissue lacking osteogenic potential. The bone ends are osteoporotic, tapered, and avascular.
Paley Classification
Paley et al. introduced a highly practical classification system, particularly useful for tibial nonunions, focusing on bone loss and deformity to guide Ilizarov and reconstructive techniques.
- Type A (Bone loss < 1 cm):
- Type A1: Lax (mobile) nonunion.
- Type A2: Stiff (nonmobile) nonunion.
- Type A2-1: No deformity.
- Type A2-2: Fixed deformity.
- Type B (Bone loss > 1 cm):
- Type B1: Bony defect, no shortening.
- Type B2: Shortening, no bony defect.
- Type B3: Both bony defect and shortening.
Both systems can be further modified by the presence or absence of active infection, which radically alters the treatment algorithm.
General Principles of Surgical Management
The treatment of nonunions has evolved significantly with advancements in electrical stimulation, ultrasound, orthobiologics (e.g., Bone Morphogenetic Proteins - BMPs), and sophisticated fixation systems.
The fundamental requirements for successful nonunion surgery are:
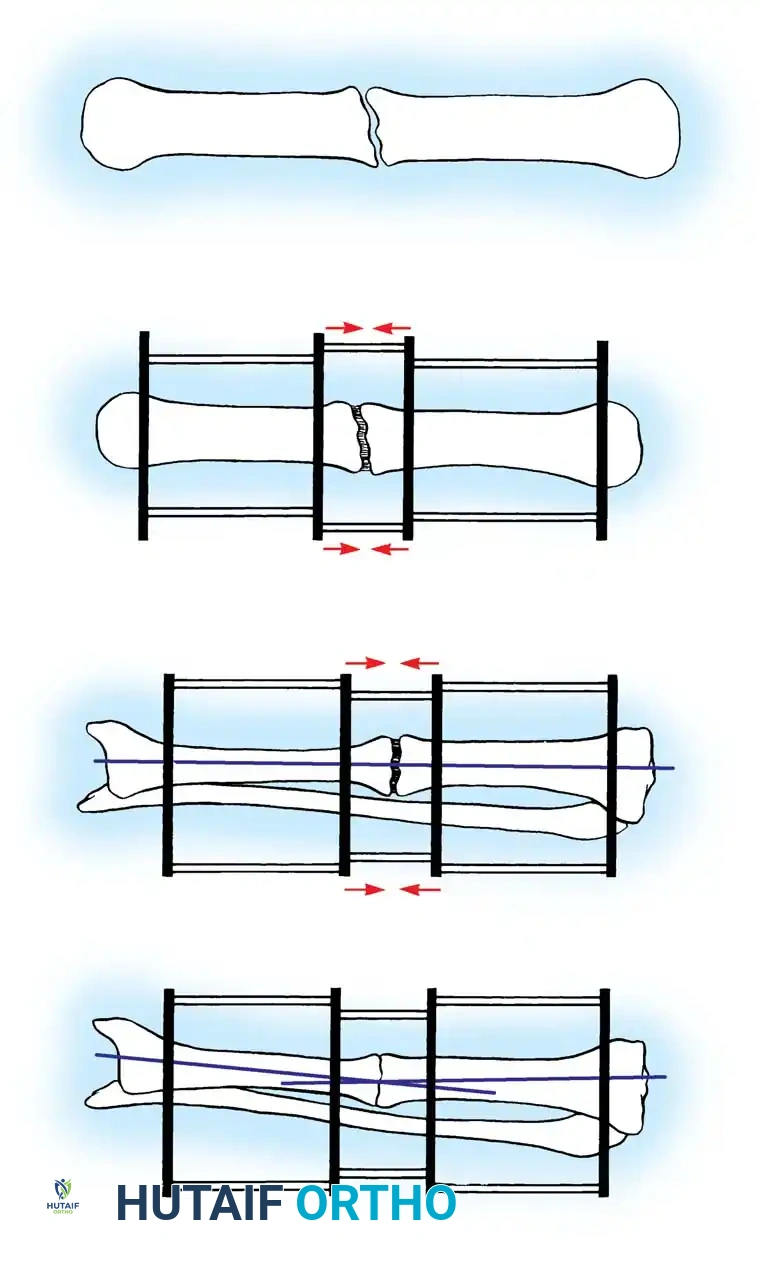
1. Biomechanical Stability: Providing a mechanical environment that minimizes strain at the fracture gap, allowing for woven bone formation.
2. Biological Vitality: Ensuring adequate vascularity, osteoprogenitor cells, and osteoinductive signals.
Hypertrophic nonunions generally require only the restoration of mechanical stability (e.g., rigid internal fixation with compression). The exuberant callus already present will rapidly consolidate once the mechanical strain is neutralized. Conversely, atrophic nonunions require both mechanical stabilization and biological augmentation (e.g., autologous bone grafting, decortication, and potentially BMP application).
Reduction of Fragments and Soft Tissue Handling
When fragments are in acceptable alignment but separated by fibrous tissue, extensive circumferential dissection is contraindicated. Leaving the periosteum, existing callus, and fibrous tissue intact around the major fragments preserves their precarious vascularity.
For displaced or bayonet nonunions, gradual traction using a simple pin fixator or skeletal traction prior to definitive internal fixation (such as closed intramedullary nailing) is preferred to acute, forceful intraoperative reduction, which can devastate the remaining soft-tissue attachments.
Operative Techniques Step-by-Step
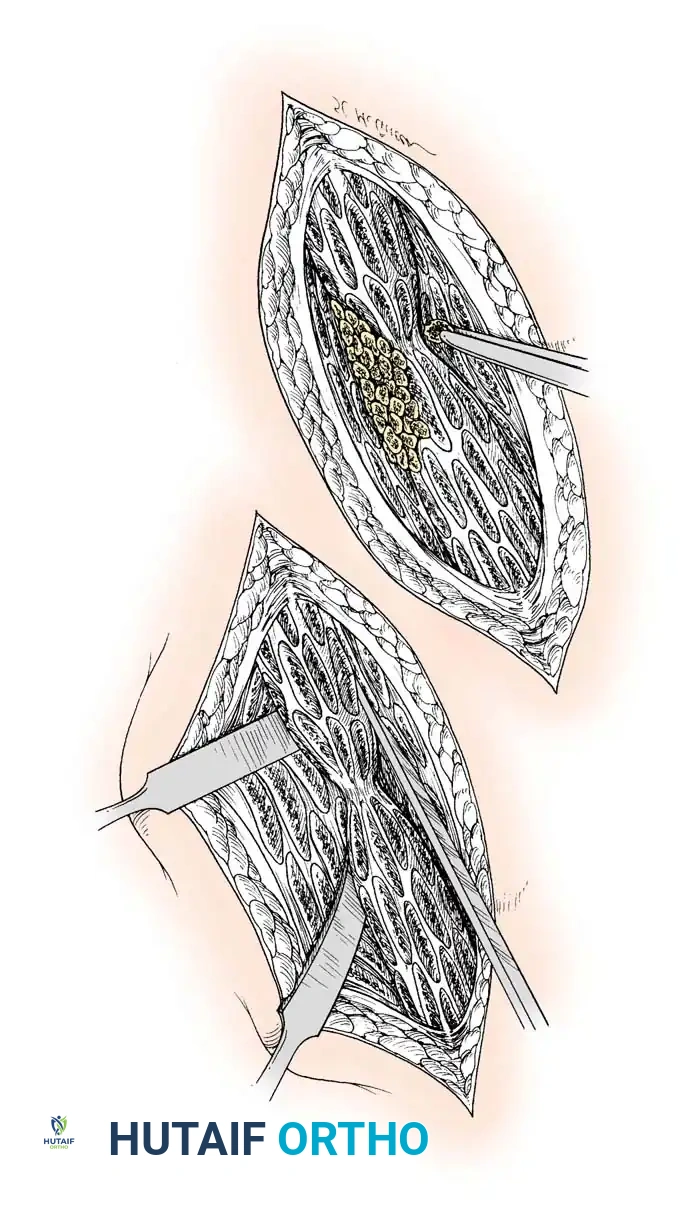
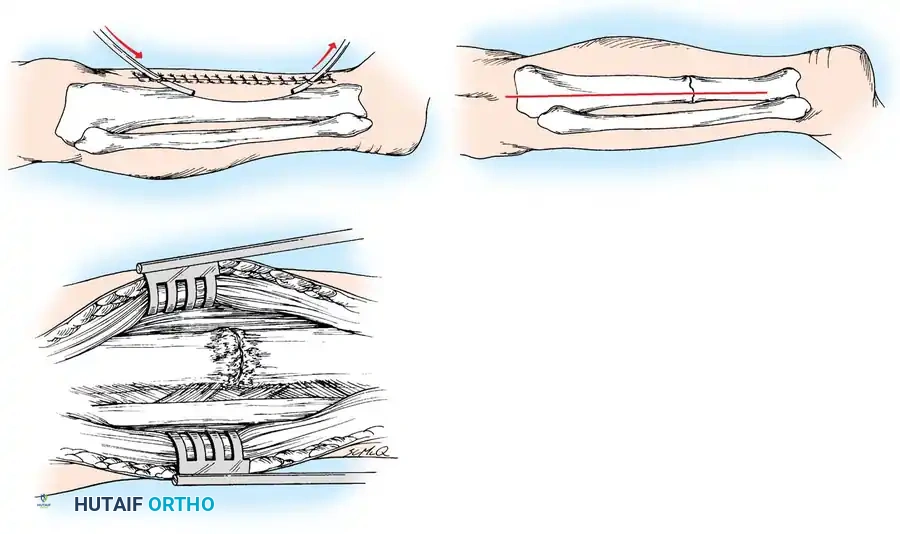
1. Decortication (Judet Technique)
For atrophic and oligotrophic nonunions, osteoperiosteal decortication is a powerful biological tool.
* Approach: Expose the nonunion site meticulously, avoiding excessive stripping.
* Technique: Using a sharp osteotome, elevate thin, continuous slivers of cortical bone along with the overlying intact periosteum and muscle attachments from the major fragments.
* Mechanism: This creates a highly vascularized, osteogenic "shingle" or envelope around the nonunion site. When combined with autogenous bone grafting, it dramatically enhances the biological healing potential.
2. Intramedullary Nailing (Exchange Nailing)
Exchange reamed intramedullary nailing is the gold standard for diaphyseal nonunions of the femur and tibia, particularly hypertrophic types.
* Indications: Aseptic diaphyseal nonunions previously treated with a smaller diameter nail, or primary treatment of diaphyseal nonunions.
* Technique:
1. Remove the existing hardware.
2. Pass a ball-tipped guide wire across the nonunion.
3. Sequentially over-ream the medullary canal. Reaming generates autologous bone graft (reamings) that is deposited at the nonunion site, while also stimulating endosteal blood flow.
4. Insert a new, larger diameter nail (typically 1-2 mm larger than the last reamer) to achieve rigid, interference fit stability.
5. Dynamization or static interlocking depends on the fracture pattern and inherent stability.
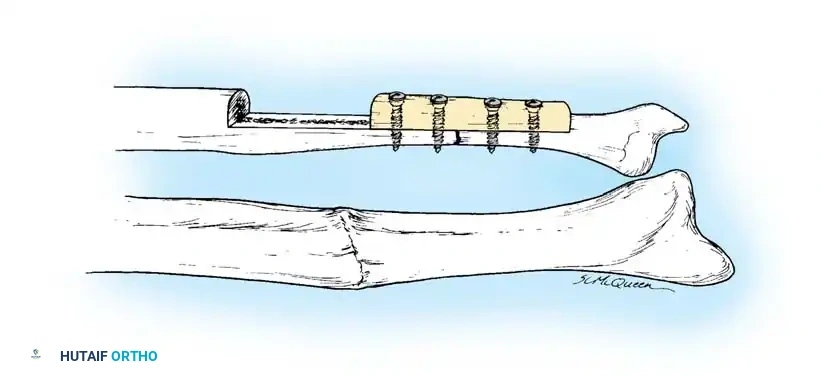
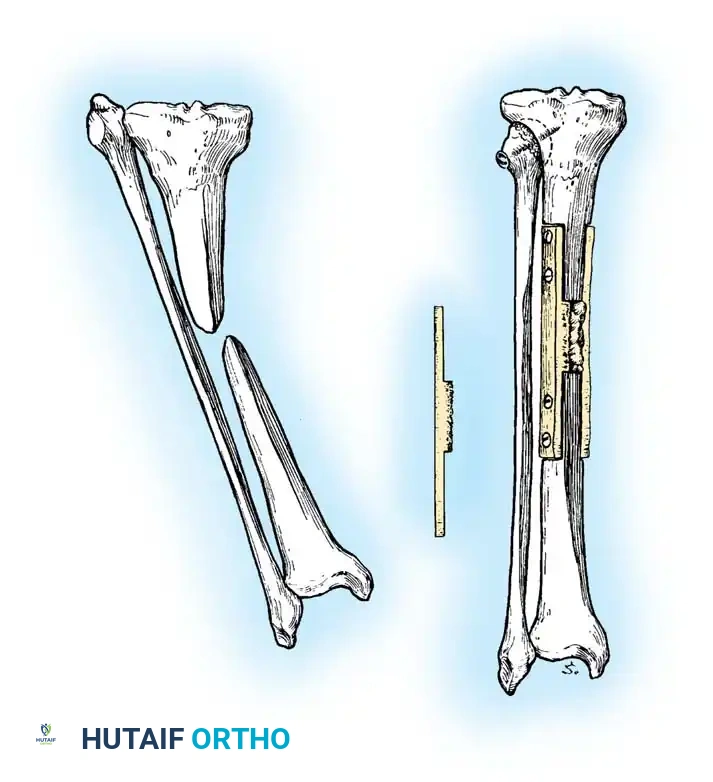
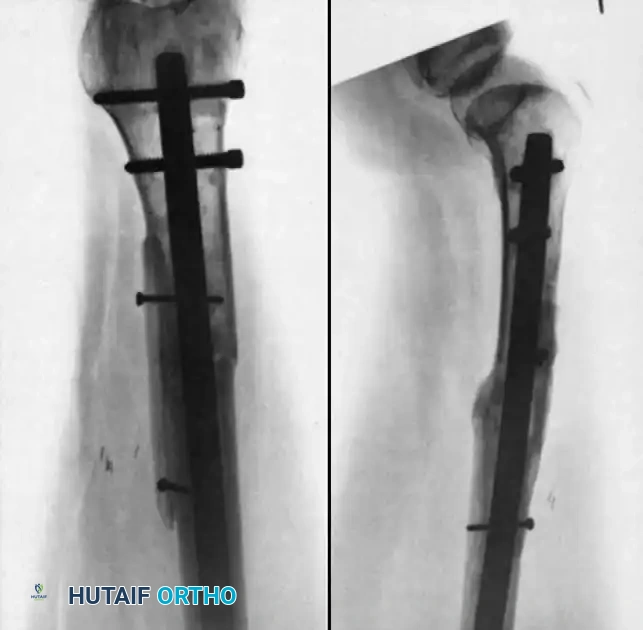
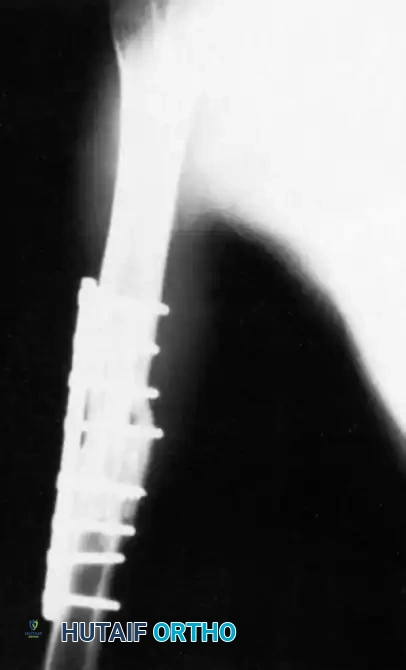
3. Plate Osteosynthesis
Compression plating is highly effective for nonunions near the metaphysis where IM nails lack purchase, or for hypertrophic nonun
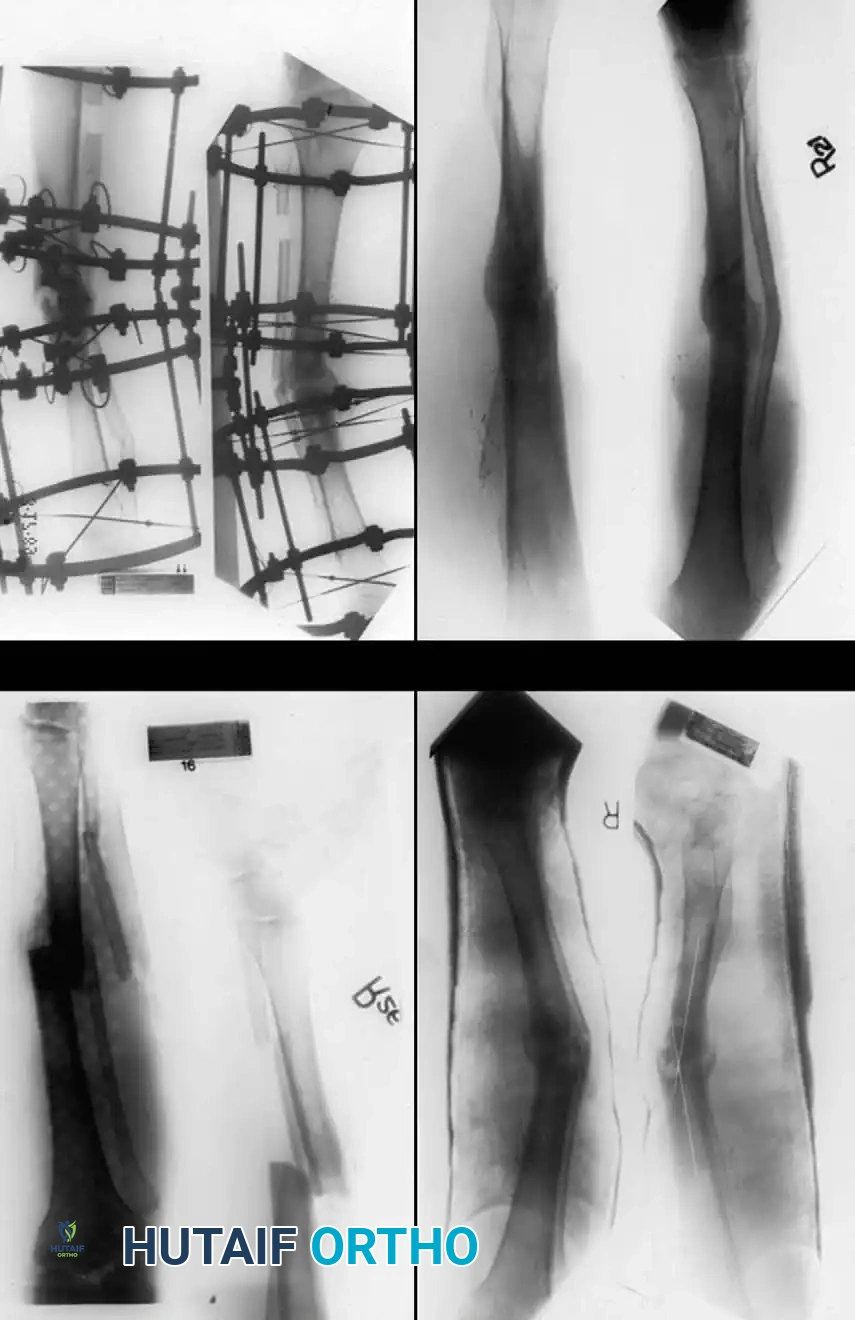
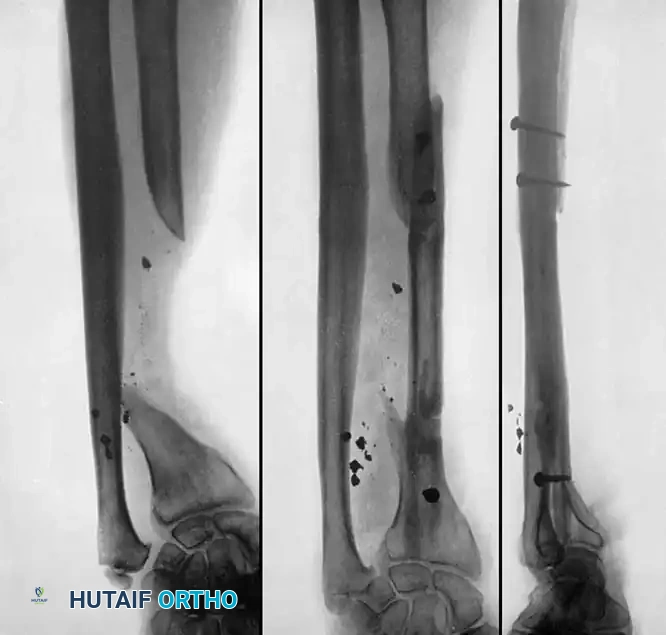
Associated Surgical & Radiographic Imaging


📚 Medical References
- fracture nonunion in children, J Pediatr Orthop 22:448, 2002.
- Green DP: Hand injuries in children, Pediatr Clin North Am 24:903, 1977.
- Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint, J Bone Joint Surg 55A:1480, 1973.
- Greene MH, Hadied AM, LaMont RL: Scaphoid fractures in children, J Hand Surg 9A:536, 1984.
- Greene WB, Anderson WJ: Simultaneous fracture of the scaphoid and radius in a child: case report, J Pediatr Orthop 2:191, 1982.
- Kaplan EB: Dorsal dislocation of the metacarpophalangeal joint of the
You Might Also Like

