OPEN REDUCTION AND INTERNAL FIXATION OF OLECRANON FRACTURES
Olecranon fractures disrupt the extensor mechanism of the elbow and compromise the articular congruity of the greater sigmoid notch. Because the triceps muscle exerts a continuous displacing force on the proximal fragment, operative intervention is indicated for almost all displaced fractures to restore the articular surface, reestablish the extensor mechanism, and allow for early range of motion. While tension band wiring is suitable for simple transverse fractures, plate osteosynthesis is the gold standard for comminuted, oblique, or Monteggia-variant olecranon fractures.
Preoperative Planning and Positioning
- Positioning: The patient may be positioned supine with the arm draped across the chest, or in the lateral decubitus position with the arm resting over a radiolucent post. The lateral position often provides superior access to the posterior elbow and facilitates fluoroscopic imaging.
- Tourniquet: A sterile tourniquet is applied high on the brachium.
- Incision: Make a posterior longitudinal skin incision. To prevent painful scar adherence over the bony prominence, curve the incision slightly radial or ulnar to the tip of the olecranon, extending an adequate distance distally along the subcutaneous border of the ulna to secure plate fixation.
Surgical Approach and Debridement
- Elevate full-thickness fasciocutaneous flaps to preserve the vascular supply to the skin.
- Identify, dissect out, and protect the ulnar nerve, particularly in complex injuries, comminuted fractures, or when placing medial-to-lateral lag screws.
- Carefully débride the fracture edges and evacuate the hematoma.
Surgical Warning: Strictly preserve the periosteum and soft tissue attachments to comminuted fragments. Stripping these fragments will lead to avascular necrosis and subsequent nonunion.
Surgical Technique: Simple Fractures
- Articular Inspection and Reduction: Inspect the articular surface of the greater sigmoid notch. Irrigate the joint to remove intra-articular debris. Reduce the fracture anatomically using pointed reduction forceps (tenaculums).
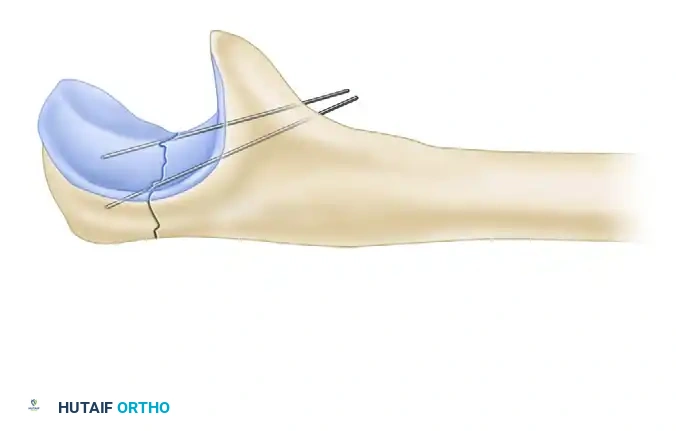
Figure 57-78A: Anatomical reduction of the olecranon fracture utilizing a pointed bone tenaculum.
- Provisional Fixation: Insert Kirschner wires (K-wires) for provisional fixation. Ensure these wires are placed out of the planned trajectory of the plate and screws. If the fracture pattern allows, consider independent lag screw fixation to compress the articular surface.
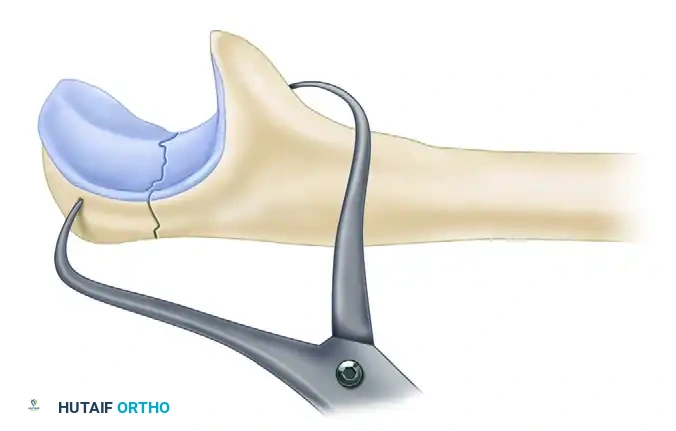
Figure 57-78B: Provisional stabilization achieved with Kirschner wires prior to plate application.
- Plate Application: Position a precontoured anatomical olecranon plate over the proximal fragment. The plate should sit directly on top of the triceps insertion; splitting the triceps tendon longitudinally allows the plate to sit flush against the bone.
- Proximal Fixation: Place the proximal "home run" screw in an intramedullary fashion, crossing the fracture site and advancing down the ulnar shaft to provide robust resistance against triceps pull.
- Distal Fixation: Utilize an adequate number of bicortical screws distally (typically a minimum of three to four screws).
- Fluoroscopic Confirmation: Confirm anatomical reduction, restoration of the articular contour, and appropriate screw length with orthogonal fluoroscopy. Ensure no screws penetrate the radioulnar joint.
Surgical Technique: Comminuted or Complex Fractures
- Sequential Reduction: Reduce and stabilize the fracture sequentially. Address one fragment at a time using small (2.0 mm or 2.4 mm) lag screws.
- Coronoid and Anterior Fragments: If a large anterior oblique fragment (coronoid base) is present, stabilize it to the ulnar shaft first. This critical step restores the anterior buttress of the elbow joint and facilitates the sequential reduction of the remaining olecranon.
- Subchondral Support: Reduce impacted subchondral segments. Stabilize them with K-wires and support the articular elevation with cancellous bone graft or bone substitute if a void exists.
- Definitive Plating: Apply the precontoured plate. In osteoporotic bone or highly comminuted patterns, utilize locking screws to enhance construct stability.
- Closure: Close the wound in layers, ensuring meticulous closure of the fascia over the plate if possible. Splint the elbow in extension with an anterior plaster slab to minimize tension on the wound and the repair.
Postoperative Care
The initial splint is worn for 2 to 5 days. If rigid fixation was achieved and the elbow is stable, protected active-assisted range-of-motion exercises are initiated early to prevent arthrofibrosis, advancing as tolerated by the patient.
ESSEX-LOPRESTI FRACTURE-DISLOCATIONS
The Essex-Lopresti lesion is a severe longitudinal radioulnar dissociation (LRUD) characterized by a triad of injuries: a fracture of the radial head or neck, disruption of the distal radioulnar joint (DRUJ), and tearing of the interosseous membrane (IOM) for a considerable distance proximally.
Pathoanatomy and Biomechanics
This injury typically results from a high-energy fall on an outstretched hand. The axial load transmits through the carpus to the radius, fracturing the radial head. As the radial head fails, the energy propagates proximally to distally, rupturing the central band of the interosseous membrane and ultimately disrupting the DRUJ ligaments.
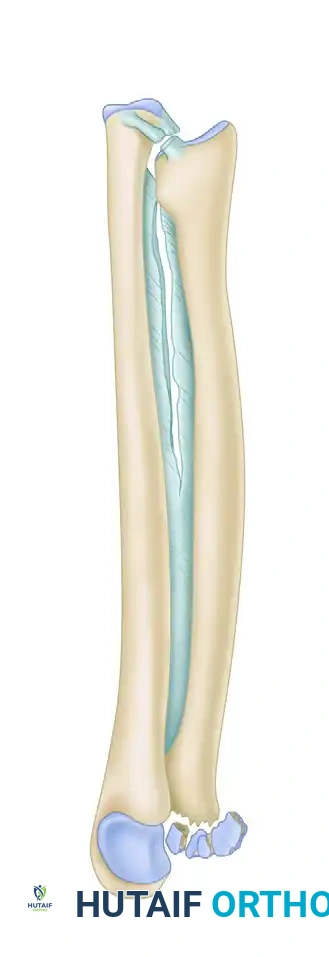
Figure 57-79: Diagrammatic representation of an Essex-Lopresti fracture-dislocation demonstrating radial head fracture, interosseous membrane rupture, and subsequent proximal radial migration.
The tethering effect of the proximal radial-oriented fibers of the interosseous membrane is lost. If the radial head is resected or fails to provide a proximal buttress, rapid proximal migration of the radius occurs. This catastrophic collapse results in severe wrist pain from ulnocarpal impingement and elbow pain from radiocapitellar impingement.
Clinical Pearl: Disruption of the DRUJ must be recognized early, before irreversible radial migration occurs. Pain in the distal radioulnar joint or wrist in the presence of a displaced radial head fracture should immediately alert the surgeon to a potential Essex-Lopresti injury.
Surgical Management
When proximal migration has occurred, late reconstruction is notoriously difficult and often yields unsatisfactory results. Therefore, acute anatomical restoration is paramount.
- Radial Head Reconstruction: The proximal radial fracture must be addressed first to restore the longitudinal column. Open reduction and internal fixation (ORIF) is performed if the radial head is reconstructable. If the radial head is unrepairable (highly comminuted), Edwards and Jupiter strongly advise immediate radial head arthroplasty. Never resect the radial head without replacement in the setting of an IOM tear.
- DRUJ Stabilization: Following restoration of the radiocapitellar joint, the DRUJ must be reduced. The forearm is typically placed in supination to reduce the DRUJ anatomically.
- Pinning: The DRUJ is pinned transversely with heavy K-wires (e.g., 0.062 inch) from the ulna into the radius to maintain reduction and allow the interosseous membrane to heal. The pins are left in place for approximately 6 weeks.
Case Example: Essex-Lopresti Reconstruction
The following sequence demonstrates the complex management of an Essex-Lopresti injury complicated by radial shortening.
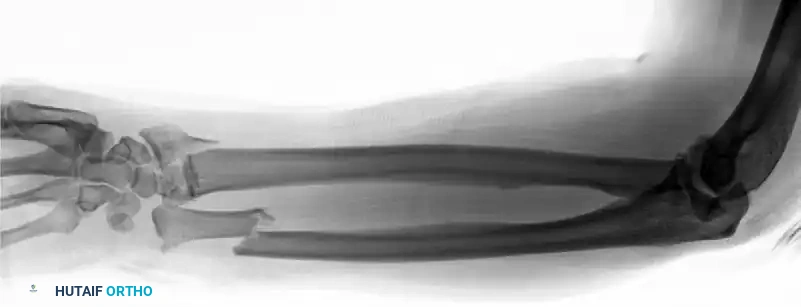
Figure 57-80A: Initial presentation showing radial head fracture and longitudinal instability.

Figure 57-80B: Associated DRUJ disruption and ulnar variance.

Figure 57-80C: Attempted initial stabilization.

Figure 57-80D: Progressive proximal migration of the radius due to unrecognized or inadequately treated IOM disruption.
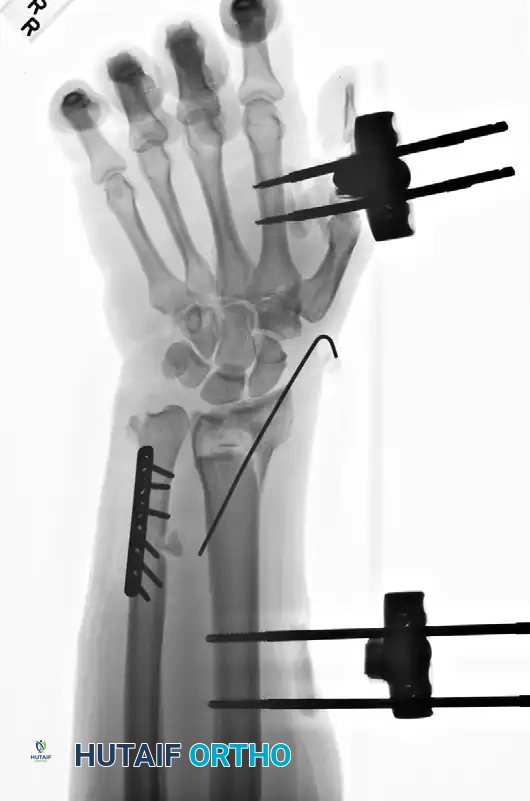
Figure 57-80E: Application of an external fixator; however, profound radial shortening and ulnocarpal impaction remain evident.
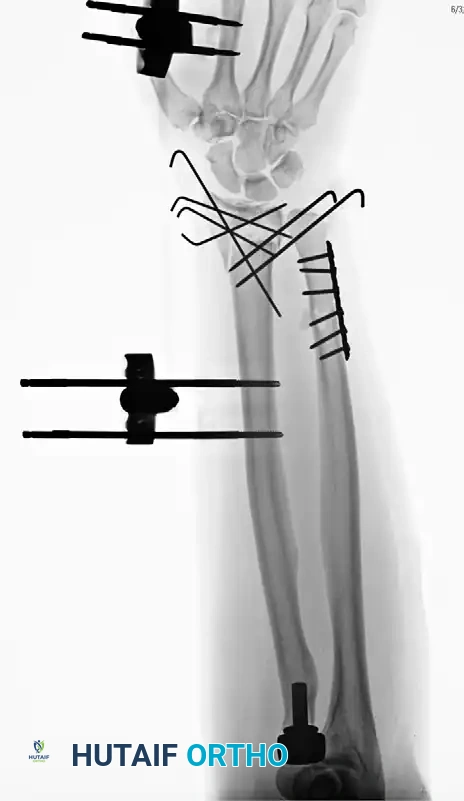
Figure 57-80F: Definitive revision surgery utilizing a radial head prosthesis to restore the proximal buttress and reestablish anatomical radial length.
MONTEGGIA FRACTURE-DISLOCATIONS
The Monteggia fracture-dislocation is a treacherous combination of a fracture of the proximal third of the ulna with a concomitant dislocation of the radial head. As Watson-Jones famously stated, “No fracture presents so many problems, no injury is beset with greater difficulty, no treatment is characterized by more general failure.”
Bado Classification
Bado classified these injuries into four distinct types based on the direction of the radial head dislocation and the apex of the ulnar fracture angulation:
-
Type 1: Fracture of the middle or proximal third of the ulna with anterior dislocation of the radial head and characteristic apex-anterior angulation of the ulna. This is the most common type.
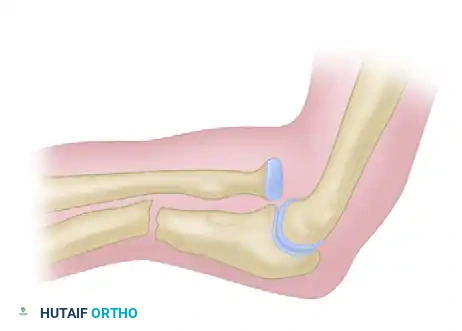
Figure 57-81A: Bado Type 1 Monteggia fracture-dislocation. -
Type 2: Fracture of the middle or proximal third of the ulna (apex usually posteriorly angulated) with posterior dislocation of the radial head. This is often associated with a fracture of the radial head and carries a higher risk of poor outcomes due to greater soft tissue compromise and associated coronoid fractures.
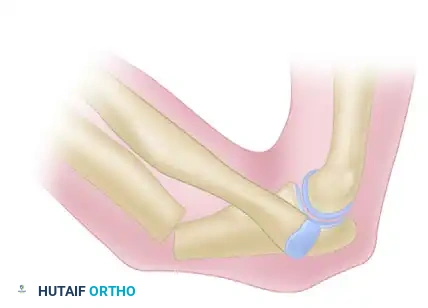
Figure 57-81B: Bado Type 2 Monteggia fracture-dislocation. -
Type 3: Fracture of the ulna just distal to the coronoid process with lateral dislocation of the radial head.
Figure 57-81C: Bado Type 3 Monteggia fracture-dislocation. -
Type 4: Fracture of the proximal or middle third of the ulna, anterior dislocation of the radial head, and a fracture of the proximal third of the radius below the bicipital tuberosity.

Figure 57-81D: Bado Type 4 Monteggia fracture-dislocation.
Surgical Principles and Techniques
While closed treatment is often successful in pediatric populations, Monteggia injuries in adults mandate surgical intervention. The fundamental principle of treating a Monteggia lesion is that the ulna dictates the radius. Anatomical ORIF of the ulna with rigid, stable fixation almost always (in >90% of cases) results in spontaneous, closed reduction of the radial head dislocation.
- Ulnar Fixation: We routinely utilize 3.5-mm limited-contact dynamic compression plates (LC-DCP) or precontoured proximal ulnar locking plates for ulnar fixation.
- Restoring the Ulnar Bow: Plate contouring must perfectly match the proximal ulnar bow (PUDA - Proximal Ulna Dorsal Angulation). Applying a straight, uncontoured plate to the proximal ulna will result in an apex-dorsal malreduction, which will mechanically force the radial head into persistent posterior subluxation.
- Managing Comminution: If comminution is present, anatomical length and rotation must be restored. Use small-diameter lag screws to reconstruct the tubular structure of the ulna before applying a neutralization plate.
- Evaluating the Radiocapitellar Joint: Following ulnar fixation, a thorough fluoroscopic evaluation of the radiocapitellar joint through a full range of motion is critical.
Pitfall: Continued radiocapitellar instability most frequently is caused by malreduction of the ulna. If the radial head remains subluxated, reevaluate the ulnar length and bow immediately.
Management of Persistent Radial Head Dislocation
When radial head subluxation persists despite perfect anatomical reduction of the ulna, the radiocapitellar joint must be surgically explored. Soft tissue interposition—often the joint capsule, annular ligament, or even the posterior interosseous nerve (PIN)—must be extracted from the joint. Exposure is achieved via a Boyd-Thompson or Kocher approach. Direct repair or reconstruction of the annular ligament is rarely necessary once the obstruction is cleared and the ulna is anatomically fixed.
If a concomitant radial head fracture is present (common in Bado Type 2), it must be repaired or replaced. Early resection of the radial head in a Monteggia variant leads to delayed union or nonunion of the ulna due to increased angular forces on the ulnar plate.
Complications
Complications of Monteggia fractures are severe and include arthrofibrosis, radioulnar synostosis, nonunion, malunion, infection, and PIN palsy. Egol et al. noted that Bado Type 2 fractures have the highest rate of fair or poor outcomes, frequently complicated by heterotopic ossification and post-traumatic arthritis requiring revision surgery.
BOTH-BONE FOREARM FRACTURES IN ADULTS
The forearm functions as a complex, dynamic joint. The radius bows laterally and dorsally, rotating around the fixed axis of the ulna to provide pronation and supination. Fractures of both the radius and ulna completely disrupt this relationship. Operative treatment is indicated for almost all both-bone forearm fractures in adults to reestablish length, alignment, rotation, and the critical radial bow.
Surgical Approaches
- Radius: The volar approach of Henry is utilized for fractures of the middle and distal thirds of the radius. For proximal third radial fractures, a dorsal Thompson approach is preferred to safely navigate the posterior interosseous nerve.
- Ulna: The ulna is approached directly via an incision along its subcutaneous border.
Surgical Warning: Never use a single incision to approach both bones, as this drastically increases the risk of cross-union (radioulnar synostosis). Maintain a wide skin bridge between the two incisions.
Fixation Techniques
Rigid plate-and-screw fixation is the gold standard. Intramedullary nailing has limited indications, primarily reserved for highly comminuted fractures with poor soft tissue envelopes where plating would require excessive stripping.
- Plate Selection: We routinely use 3.5-mm LC-DCP plates. For distal ulnar fractures or proximal radial fractures where a 3.5-mm plate may cause soft tissue irritation, 2.7-mm plates with locking screws provide a lower profile while maintaining rigid stabilization.
- Fracture Patterns:
- Transverse/Short Oblique: Utilize dynamic compression plating techniques to achieve absolute stability.
- Butterfly Fragments: Anatomically reduce the wedge fragment using 2.4-mm or 2.7-mm lag screws, followed by the application of a neutralization plate.
- Sequence of Fixation: Typically, the less comminuted bone is fixed first to establish length and alignment, making the reduction of the second bone easier.

Figure 57-82A: Preoperative AP radiograph of a displaced both-bone forearm fracture in an adult.

Figure 57-82B: Preoperative lateral radiograph demonstrating significant translation and loss of the radial bow.

Figure 57-82C: Postoperative AP radiograph demonstrating anatomical reduction and rigid fixation with 3.5-mm compression plates.

Figure 57-82D: Postoperative lateral radiograph confirming restoration of alignment and appropriate plate contouring.
Open Fractures
Open both-bone forearm fractures with minimal contamination (Gustilo-Anderson Type I and II) are treated with thorough surgical débridement, copious pulsatile irrigation, and immediate internal fixation. Immediate plating provides the stability necessary for soft tissue healing and reduces infection rates compared to delayed fixation.
Postoperative Protocol
Following rigid internal fixation, the arm is placed in a bulky Jones dressing or a removable splint. Because absolute stability is achieved via compression plating, early active range of motion of the elbow, wrist, and forearm (pronation/supination) is initiated within the first week to prevent stiffness. Weight-bearing is restricted until radiographic evidence of bridging callus or obliteration of the fracture lines is observed, typically around 8 to 12 weeks.
