Principles of Ankle Fracture Management
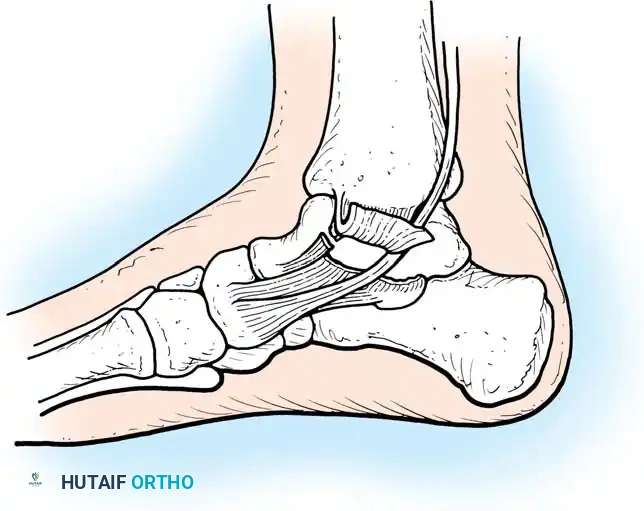
Injuries around the ankle joint cause destruction of not only the bony architecture but also, critically, the ligamentous and soft-tissue components. The ankle is a highly congruent, weight-bearing hinge joint. With fractures of the ankle, only slight variation from normal anatomy is compatible with good long-term joint function. Classic biomechanical studies have demonstrated that even a 1-mm lateral shift of the talus reduces the tibiotalar contact area by 42%, leading to exponentially increased peak contact stresses and rapid post-traumatic arthrosis.
Radiographs after reduction must be scrutinized with three absolute requirements in mind:
1. The normal relationships of the ankle mortise must be perfectly restored.
2. The weight-bearing alignment of the ankle must be at a right angle to the longitudinal axis of the leg.
3. The contours of the articular surface must be as smooth and congruent as possible.
The best functional outcomes are obtained by anatomical joint restoration. While closed manipulation and casting may suffice for stable, non-displaced fracture patterns, open reduction and internal fixation (ORIF) is the gold standard for unstable injuries. For most displaced fractures, operative intervention ensures anatomical joint restoration, rigid stability, and reliable union, permitting early range of motion.

Classifications of Ankle Fractures
Understanding fracture morphology and the mechanism of injury is paramount for preoperative planning. The two most widely utilized systems are the Lauge-Hansen and the Danis-Weber classifications.
Lauge-Hansen Classification
Lauge-Hansen correlated fracture patterns with the mechanism of injury, proposing a detailed classification system based on cadaveric studies. The first word in the designation refers to the foot’s position at the time of injury (supination or pronation); the second word refers to the direction of the deforming force relative to the tibia.
Clinical Pearl: In the Lauge-Hansen system, the term "eversion" is historically used but is a biomechanical misnomer; it more correctly represents external or lateral rotation.
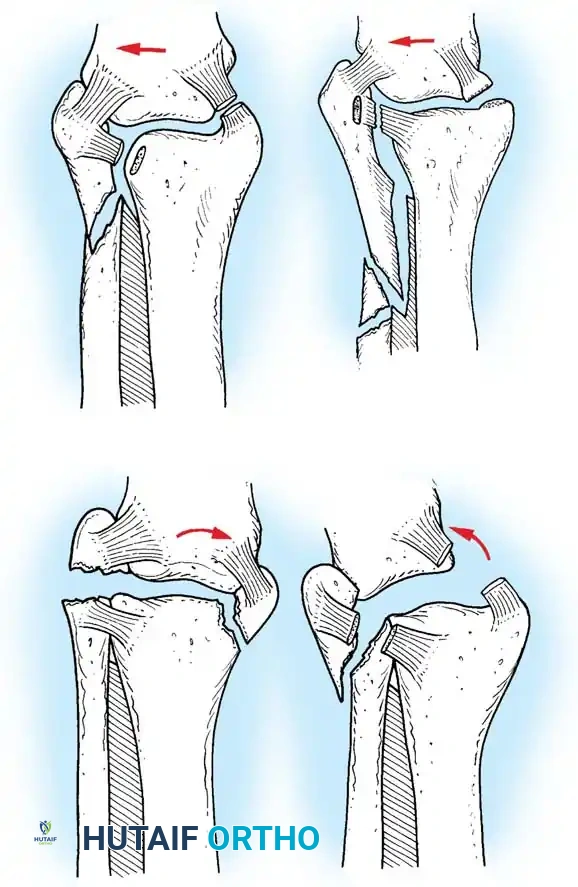
- Supination-Eversion (External Rotation) (SER): The most common mechanism. The identifying feature is a spiral oblique fracture of the distal fibula. It progresses in four stages: (1) disruption of the anterior tibiofibular ligament, (2) spiral oblique fracture of the distal fibula, (3) disruption of the posterior tibiofibular ligament or fracture of the posterior malleolus, and (4) fracture of the medial malleolus or rupture of the deltoid ligament.
- Supination-Adduction (SA): Characterized by a transverse avulsion-type fracture of the fibula below the level of the joint (or tear of the lateral collateral ligaments) and a relatively vertical shear fracture of the medial malleolus.
- Pronation-Abduction (PA): Involves a transverse fracture of the medial malleolus (or deltoid rupture), rupture of the syndesmotic ligaments, and a short, horizontal, oblique fracture of the fibula above the level of the joint.
- Pronation-Eversion (External Rotation) (PER): Begins with a transverse fracture of the medial malleolus or deltoid disruption, followed by anterior tibiofibular ligament disruption, a short oblique fracture of the fibula high above the joint level, and finally, posterior tibiofibular ligament rupture or posterolateral tibial avulsion.
- Pronation-Dorsiflexion (PD): A rare pattern involving fracture of the medial malleolus, fracture of the anterior margin of the tibia, supramalleolar fracture of the fibula, and transverse fracture of the posterior tibial surface.
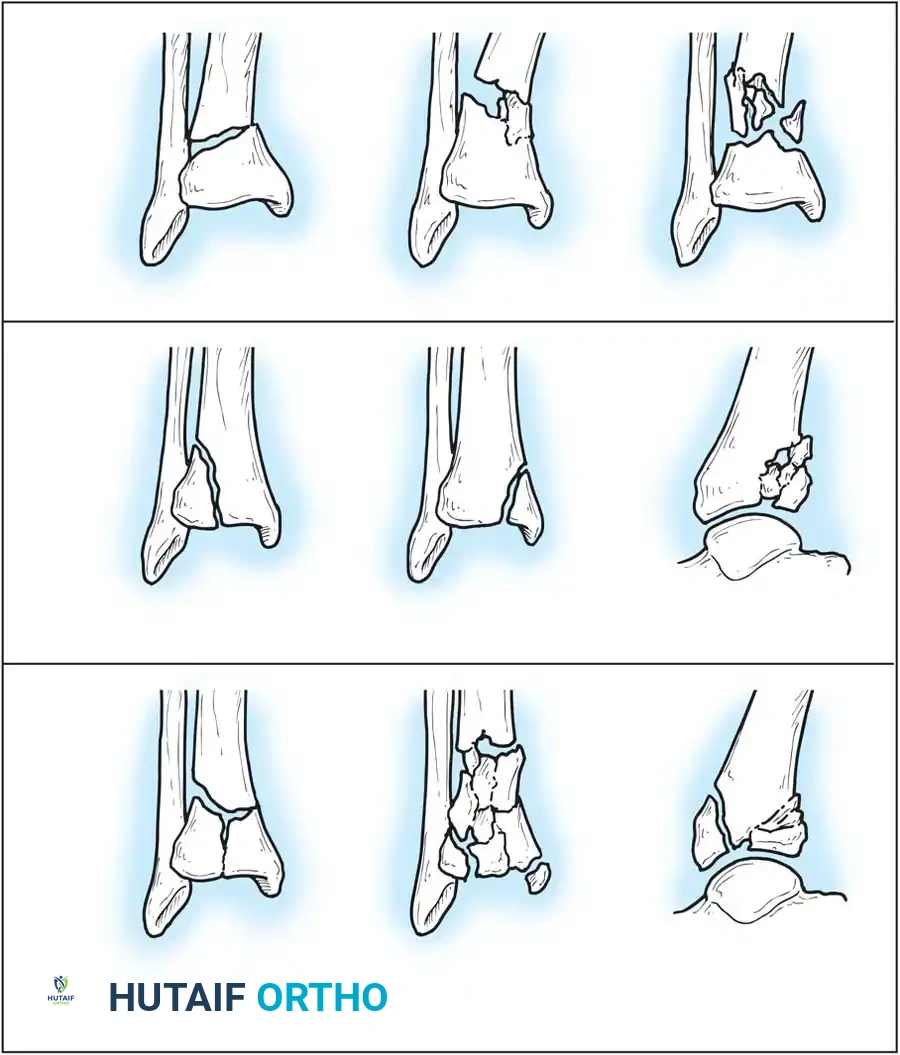
Danis-Weber Classification
The Danis-Weber classification is based purely on the anatomic location of the fibular fracture relative to the syndesmosis. It is highly practical for determining the likelihood of syndesmotic instability.
- Type A: Fibula fracture below the syndesmosis (infrasyndesmotic). The syndesmosis is intact. Correlates with Lauge-Hansen SA.
- Type B: Fibula fracture at the level of the syndesmosis (transsyndesmotic). The syndesmosis may or may not be torn. Correlates with Lauge-Hansen SER. Approximately 80% to 90% of lateral malleolar fractures fall into this category.
- Type C: Fibula fracture above the syndesmosis (suprasyndesmotic). The syndesmosis is invariably disrupted. Correlates with Lauge-Hansen PER or PA.
AO/OTA Classification of Malleolar Fractures
The AO classification expands upon the Danis-Weber system, subdividing injuries based on the presence of medial or posterior lesions.
* Type A (Infrasyndesmotic): A1 (isolated), A2 (with medial malleolus fracture), A3 (with posteromedial fracture).
* Type B (Transsyndesmotic): B1 (isolated), B2 (with medial lesion), B3 (with medial lesion and posterolateral tibia fracture).
* Type C (Suprasyndesmotic): C1 (diaphyseal fibula, simple), C2 (diaphyseal fibula, complex), C3 (proximal fibula fracture / Maisonneuve).
Isolated Fractures of the Lateral Malleolus
Although fractures of the lateral malleolus without significant medial injury are common, the indications for open reduction remain a topic of academic debate. The maximal acceptable displacement of the fibula reported in the literature ranges from 0 to 5 mm, though most surgeons accept 2 to 3 mm depending on patient demands.
Biomechanical studies by Brown et al. and Michelson et al. demonstrated that isolated fractures of the lateral malleolus do not disturb joint kinematics or cause talar displacement with axial loading, provided the deep deltoid ligament is intact. Long-term clinical follow-up of closed treatment for SER stage II fractures yields 94% to 98% good functional results.
Surgical Warning: If the stability of a lateral malleolar fracture is uncertain, gravity stress or manual external rotation stress radiographs must be obtained. Medial clear space widening >4 mm indicates deep deltoid disruption (an SER IV equivalent), necessitating operative fixation.
Operative Techniques for the Lateral Malleolus
When operative intervention is indicated, several techniques are available:
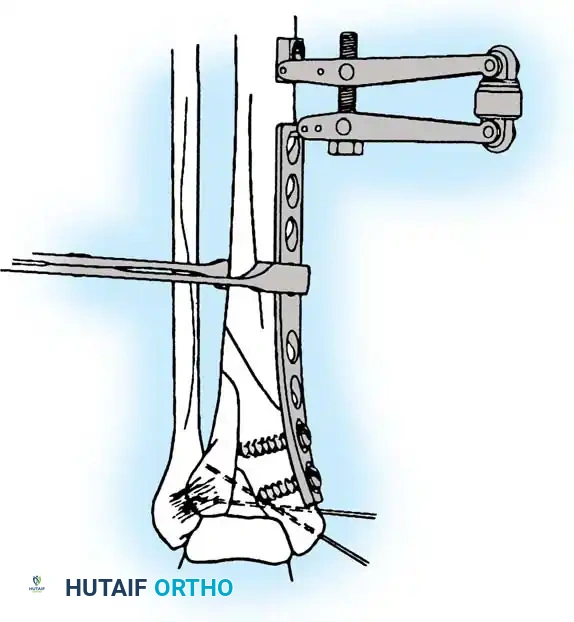
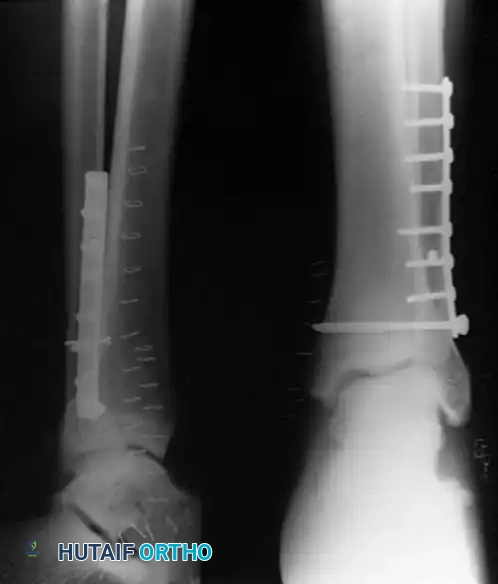
- Lateral Plating (Neutralization): The standard approach utilizes a direct lateral incision. The fracture is anatomically reduced with pointed reduction forceps. An interfragmentary 3.5-mm lag screw is placed perpendicular to the fracture plane, followed by a 1/3 tubular neutralization plate applied to the lateral aspect of the fibula.
- Posterior Antiglide Plating: Advocated by Ostrum for Weber B fractures, this technique involves placing the plate on the posterior aspect of the fibula. It biomechanically resists the posterior and proximal displacement of the distal fragment. It decreases the incidence of palpable hardware and avoids intraarticular screw penetration.
- Lag Screw Only Fixation: For young patients (<50 years) with simple, long oblique fractures and excellent bone quality, Tornetta et al. demonstrated that fixation with two 3.5-mm lag screws placed at least 1 cm apart provides sufficient stability without the soft-tissue irritation associated with plates.
Isolated Fractures of the Medial Malleolus
Medial malleolar fractures rarely occur in isolation; they are typically part of a rotational injury complex. When they do occur, anatomical reduction is critical to restore the medial shoulder of the ankle mortise.
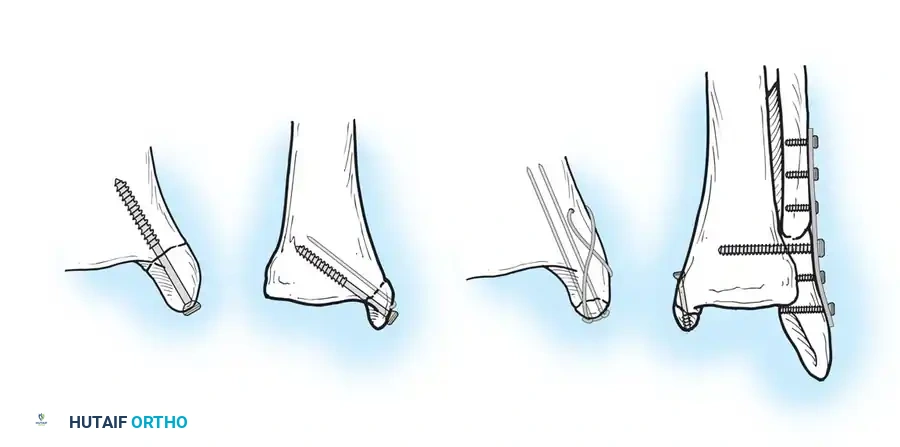
Operative Techniques for the Medial Malleolus
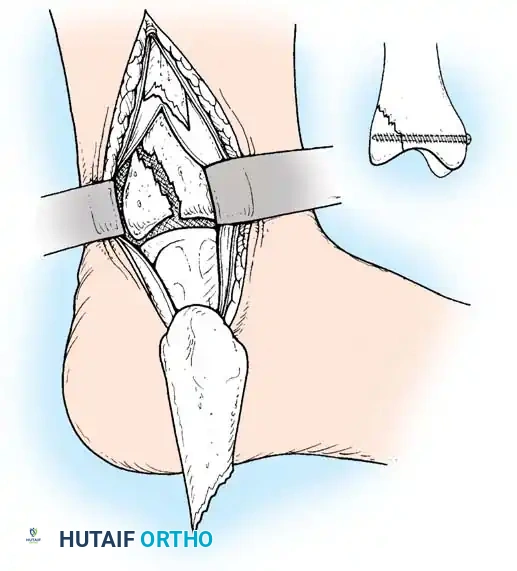
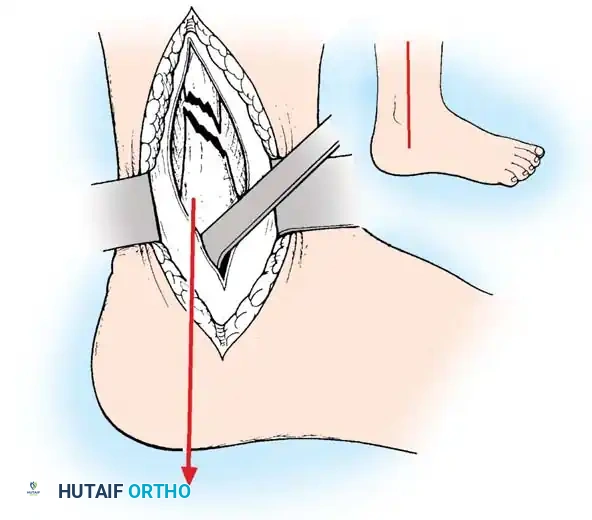
The approach is via a standard longitudinal or slightly curved medial incision centered over the malleolus. Care must be taken to protect the saphenous vein and nerve. The fracture site is exposed, and any interposed periosteum or osteochondral debris is meticulously cleared.
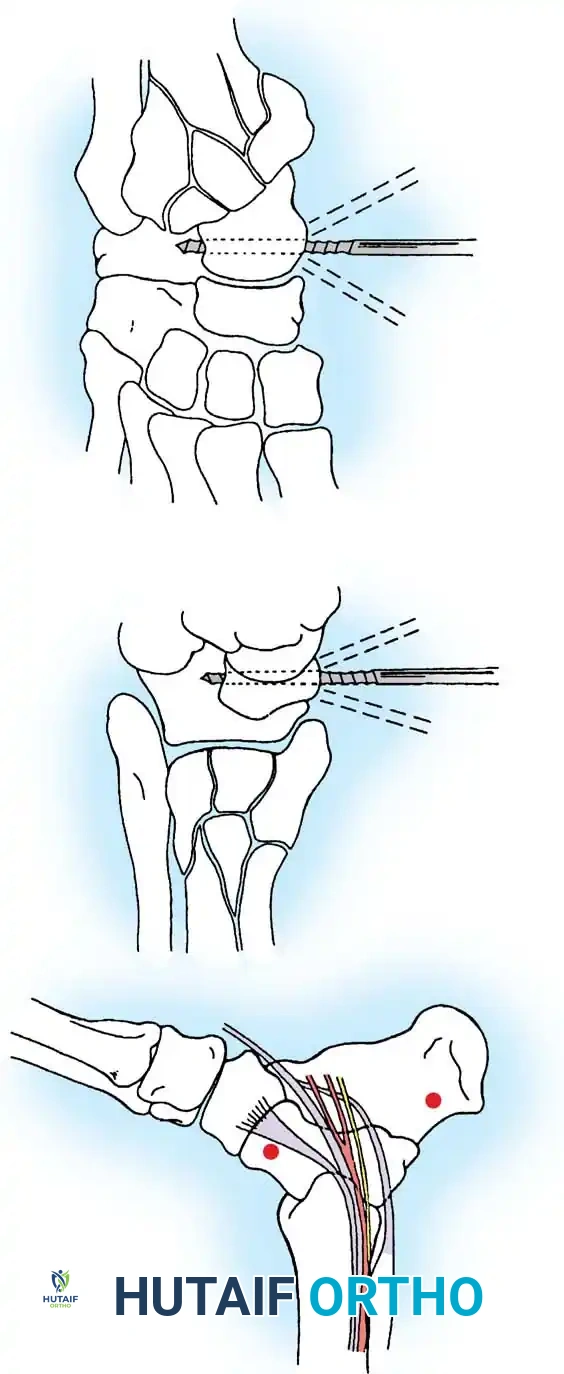
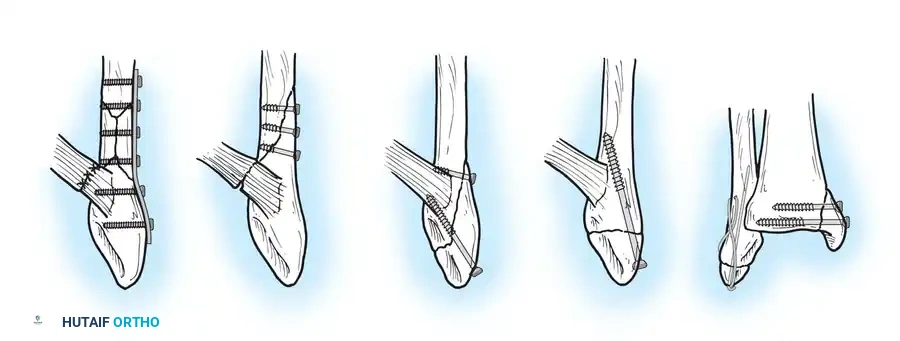
- Lag Screw Fixation: The most common construct consists of two 4-mm partially threaded cancellous lag screws oriented perpendicular to the fracture line.
- Small Fragment Fixation: Smaller fragments can be fixed with one lag screw and one parallel Kirschner wire (K-wire) to prevent rotational instability.
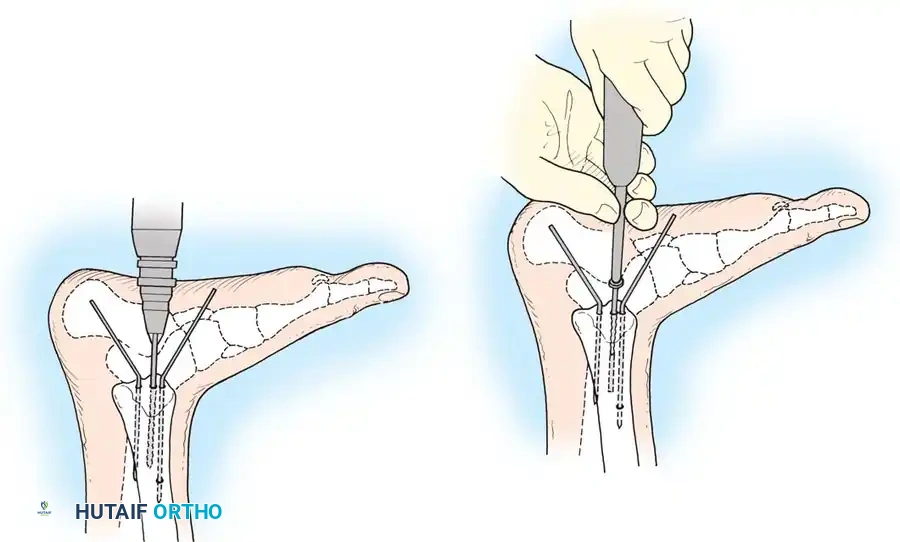
- Tension Band Wiring: Fragments that are too small or comminuted for screw fixation are best stabilized with two K-wires and a figure-of-eight tension band wire. This converts tensile forces into compressive forces at the articular surface.
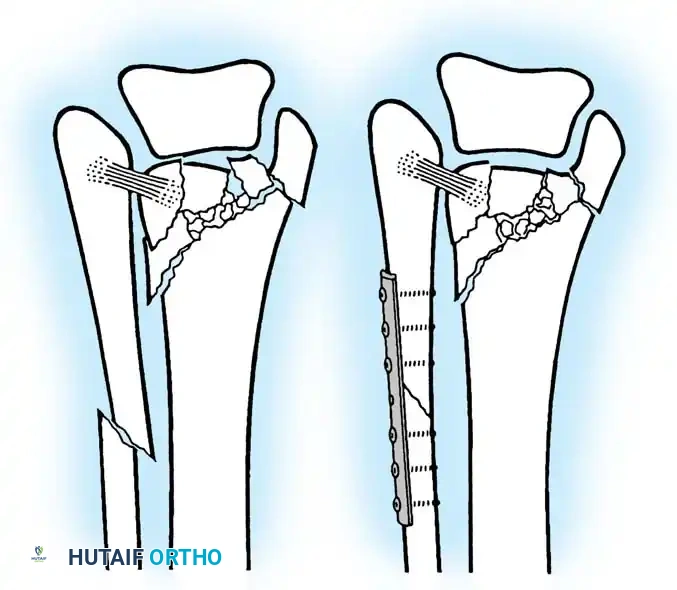
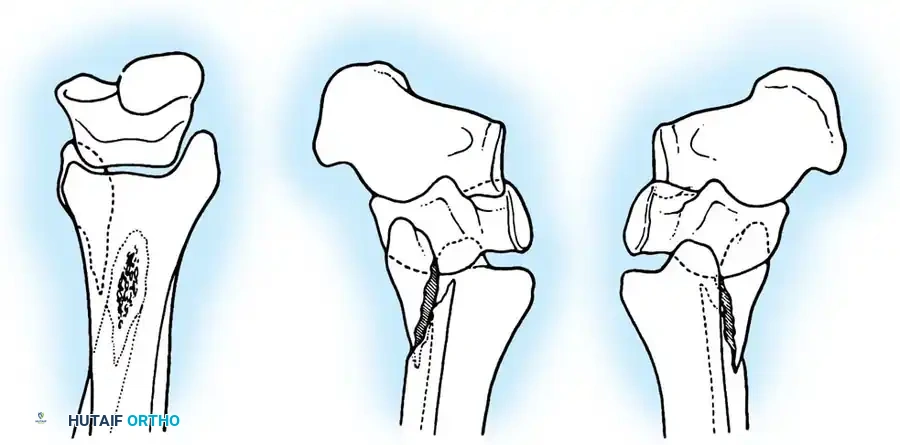
- Buttress Plating: Vertical shear fractures (characteristic of SA injuries) require horizontally directed screws or, more reliably, a small semitubular buttress plate applied to the medial apex to resist vertical displacement.
Bioabsorbable Implants in Medial Fixation
The safety and efficacy of bioabsorbable implants have been extensively investigated to mitigate the need for secondary hardware removal due to medial prominence.
* Polyglycolide Implants: Early studies reported high union rates but a 5% to 10% incidence of late sterile sinus drainage related to polymer breakdown.
* Polylactide Implants: Bucholz et al. found no differences in functional results between 4-mm polylactide screws and stainless steel screws, with a significantly lower inflammatory profile. However, some studies still report unacceptable rates of localized inflammatory cystic reactions. Currently, metallic fixation remains the gold standard, with bioabsorbables reserved for highly specific indications.

Bimalleolar Fractures
Bimalleolar ankle fractures disrupt both the medial and lateral stabilizing structures of the ankle joint. Displacement drastically reduces the tibiotalar contact area and alters joint kinematics. While closed reduction can often be accomplished acutely, it is rarely maintained as swelling subsides.
Nonunion has been reported in approximately 10% of bimalleolar fractures treated nonoperatively. Furthermore, 20% of bimalleolar fractures involve intraarticular osteochondral injuries to the talus and tibia, which go unaddressed with closed management.
Surgical Indication: The AO Foundation and modern orthopedic consensus mandate open reduction and internal fixation of both malleoli for almost all displaced bimalleolar fractures to prevent post-traumatic arthrosis.


Surgical Sequence for Bimalleolar Fixation
- Lateral Side First: The fibula is typically addressed first to restore the length and rotation of the lateral column. This often indirectly reduces the talus and simplifies the medial reduction.
- Medial Side Second: Once the lateral mortise is established, the medial malleolus is directly reduced and fixed.
- Syndesmotic Evaluation: After bimalleolar fixation, the syndesmosis must be tested using the "Cotton test" (lateral traction on the fibula using a bone hook). If widening occurs, syndesmotic screws or flexible suture-button constructs are required.

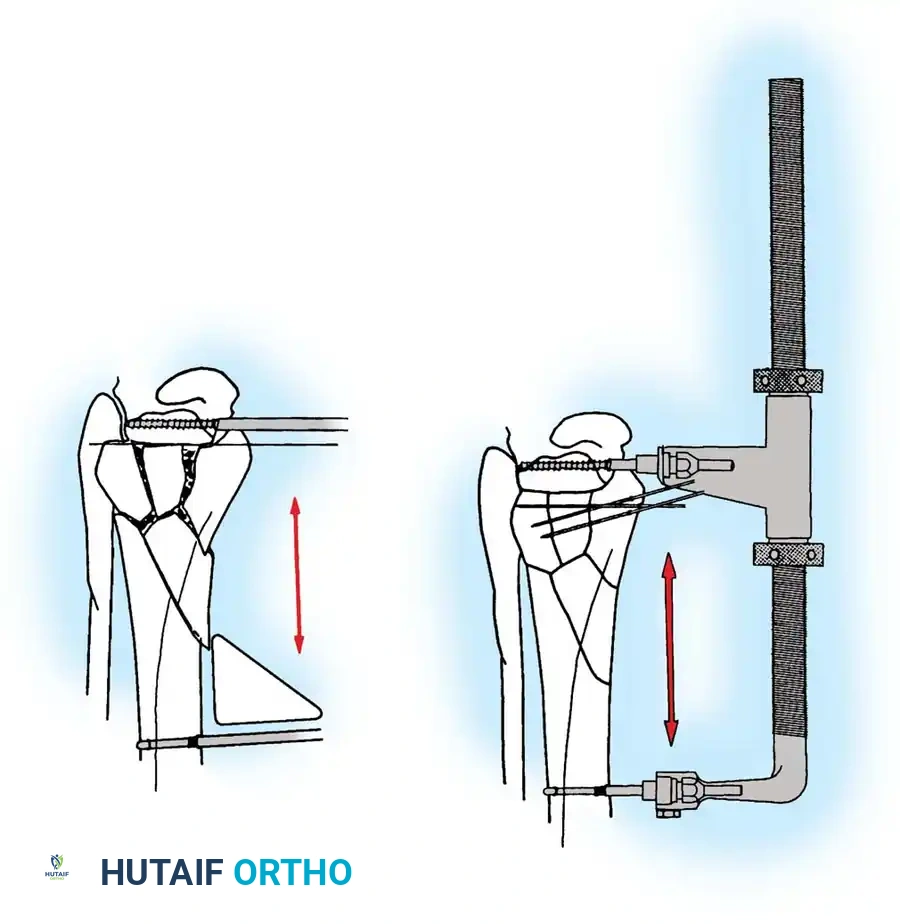
Stress Fractures of the Medial Malleolus
Stress fractures of the medial malleolus are unique entities primarily seen in athletes engaged in running or jumping sports. Patients present with localized pain, swelling, and tenderness over the medial ankle, often with a joint effusion.
Boden and Osbahr identified medial malleolar stress fractures as high-risk injuries prone to progression to complete fracture, delayed union, or nonunion.
- Diagnosis: Initial radiographs may be negative. Diagnosis often requires MRI, CT, or bone scintigraphy.
- Nonoperative Management: Requires strict restriction of impact activities for 4 to 5 months. Premature return to sport frequently results in recurrence.
- Operative Management: For fractures apparent on plain radiographs, or for athletes failing conservative management, aggressive treatment is warranted. Surgical drilling of the fracture line or internal fixation with percutaneous lag screws yields reliable healing and faster return to play.
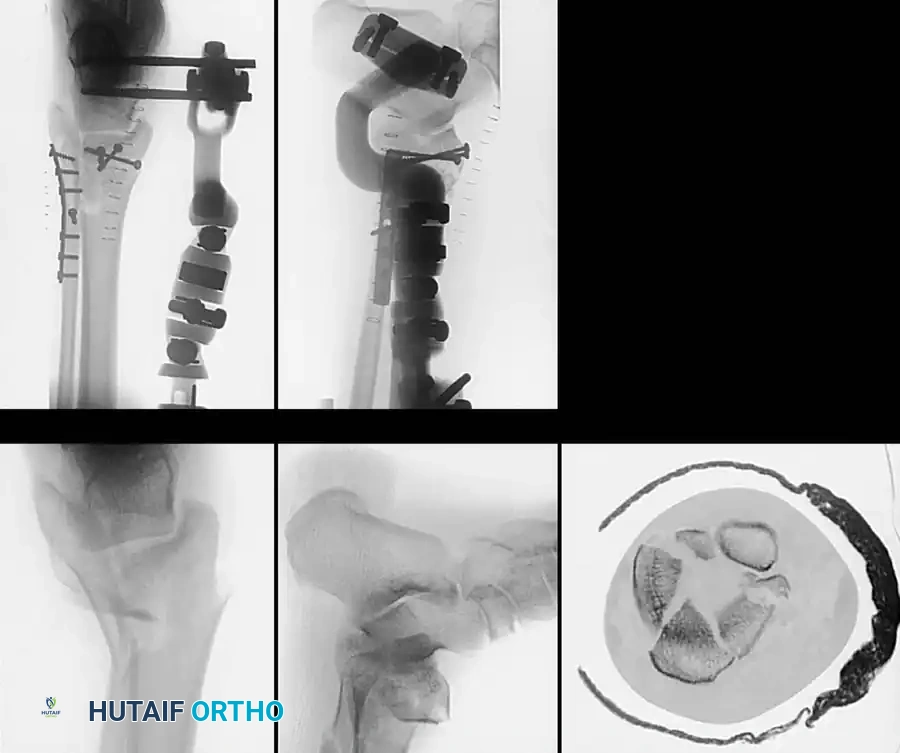
Complex Fracture Patterns and External Fixation
In cases of severe soft-tissue compromise (e.g., fracture blisters, massive edema, or open fractures), immediate internal fixation is contraindicated due to the high risk of wound dehiscence and deep infection.
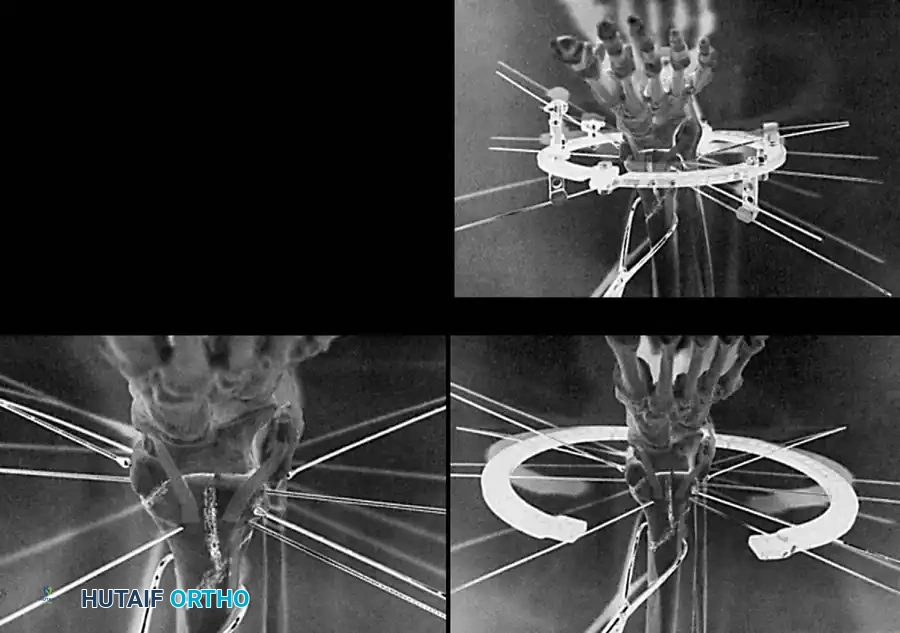
In these scenarios, damage-control orthopedics is employed. A spanning external fixator is applied to restore length, alignment, and rotation while allowing the soft-tissue envelope to recover.
Once the "wrinkle sign" appears (typically 7 to 14 days post-injury), indicating resolution of edema, the patient is returned to the operating room for definitive ORIF.

Postoperative Protocol and Rehabilitation
The success of ankle fracture surgery relies heavily on meticulous postoperative care.
- Phase I (0-2 Weeks): The ankle is immobilized in a well-padded posterior splint in a neutral position. The patient is strictly non-weight-bearing (NWB). Elevation is critical to minimize edema.
- Phase II (2-6 Weeks): Sutures are removed at 2 weeks. The patient is transitioned to a removable controlled ankle motion (CAM) boot. Active range of motion (ROM) exercises (dorsiflexion and plantarflexion) are initiated to prevent capsular contracture. Weight-bearing status depends on fracture stability and bone quality; typically, patients remain NWB or progress to touch-down weight-bearing.
- Phase III (6-12 Weeks): Radiographs are obtained at 6 weeks to assess callus formation. If clinical and radiographic union is progressing, the patient is advanced to full weight-bearing in the CAM boot, eventually weaning into a supportive shoe. Physical therapy focuses on proprioception, peroneal strengthening, and gait normalization.
Conclusion
The operative management of ankle fractures demands a profound understanding of joint biomechanics, precise surgical execution, and respect for the soft-tissue envelope. By adhering to the principles of anatomical reduction and rigid internal fixation, orthopedic surgeons can reliably restore the ankle mortise, minimize the risk of post-traumatic osteoarthritis, and return patients to their pre-injury level of function.
📚 Medical References
- ankle fractures in children, Orthop Clin North Am 21:381, 1990.
- Lang AG, Peterson HA: Osteomyelitis following puncture wounds of the foot in children, J Trauma 16:993, 1976.
- Letts RM, Gibeault D: Fractures of the neck of the talus in children, Foot Ankle 1:74, 1980.
- Lyritis G: Developmental disorders of the proximal epiphysis of the hallux, Stereoradiology 10:250, 1983.
- Manderson EL, Ollivierre CO: Closed anatomic reduction of a juvenile Tillaux fracture by dorsifl exion of the ankle: a case report, Clin Orthop Relat Res 276:262, 1992.
- McCullough CJ, Venugopal V: Osteochondritis dissecans of the talus: the natural history, Clin Orthop Relat Res 144:264, 1979.
- Mulfi nger GL, Trueta J: The blood supply of the talus, J Bone Joint Surg 52B:160, 1970.
- Parisien JS: Arthroscopic treatment of osteochondral lesions of the talus, Am J Sports Med 14:211, 1986.
- Pickle A, Benaroch TE, Guy P, et al: Clinical outcome of pediatric
