Comprehensive Introduction and Patho-Epidemiology
Metacarpophalangeal (MCP) joint dislocations represent a formidable challenge in acute hand trauma, demanding a profound understanding of intricate digital biomechanics and precise surgical intervention. These injuries most frequently occur in the border digits—specifically the index and little fingers—due to their relatively exposed anatomical positions and the inherent lack of robust collateral support compared to the central digits. The pathomechanics are typically precipitated by a high-energy, forced hyperextension injury, often sustained during athletic endeavors, falls from a height, or industrial accidents. Clinically and radiographically, these injuries are broadly dichotomized into simple (reducible) and complex (irreducible) dislocations, a classification system originally championed by Emanuel Kaplan in his seminal anatomical studies.
The hallmark of a complex MCP joint dislocation is the interposition of the fibrocartilaginous volar plate between the base of the proximal phalanx and the metacarpal head. This anatomical interposition acts as an absolute physical impediment to closed reduction maneuvers. In a classic complex dislocation of the index finger, the metacarpal head is violently driven volarly, rupturing the proximal membranous attachment of the volar plate at the metacarpal neck. The volar plate, however, remains tenaciously attached to the base of the proximal phalanx via its thick distal insertion. As the proximal phalanx translates dorsally, the volar plate is flipped dorsally over the metacarpal head, becoming wedged in the articular space.
This displacement creates a constricting anatomical "noose" around the metacarpal neck, a phenomenon uniquely predisposing the joint to irreducibility. Traction applied during misguided attempts at closed reduction only serves to tighten this noose, further strangulating the metacarpal neck, exacerbating soft tissue trauma, and rendering the dislocation truly irreducible. The application of longitudinal traction without simultaneous wrist flexion and MCP joint hyperextension is a common pitfall among inexperienced practitioners, often converting a simple dislocation into a complex one by drawing the volar plate into the joint space. Consequently, once a complex dislocation is diagnosed, open reduction is strictly and unconditionally indicated.
Furthermore, these high-energy hyperextension injuries rarely occur in isolation. The sheer force required to rupture the volar plate and dislocate the joint frequently results in concurrent osteochondral shear fractures of the metacarpal head, avulsion fractures of the proximal phalanx base, or even diaphyseal and metaphyseal fractures of the metacarpals. The treating orthopedic surgeon must maintain a high index of suspicion for these associated injuries, as missed osteochondral fragments can lead to catastrophic mechanical locking, rapid articular degradation, and early-onset post-traumatic osteoarthritis. Comprehensive management, therefore, extends beyond mere joint reduction to encompass the meticulous restoration of articular congruity and overall skeletal stability.
Detailed Surgical Anatomy and Biomechanics
The metacarpophalangeal joint is a diarthrodial condyloid joint, uniquely engineered to permit a wide arc of flexion and extension, coupled with a limited degree of abduction, adduction, and circumduction. The metacarpal head is distinctly asymmetric; it is broader on its volar aspect than on its dorsal aspect, creating a cam effect. This cam morphology dictates that the collateral ligaments are relatively lax in extension—allowing for maximal digital abduction and adduction—and maximally taut in flexion, providing critical mediolateral stability during power grip. The articular cartilage of the metacarpal head extends significantly further volarly than dorsally, accommodating the extensive arc of flexion required for normal hand function.
The volar plate is a robust, specialized fibrocartilaginous structure that serves as the primary static restraint against hyperextension of the MCP joint. Distally, it is firmly anchored to the volar base of the proximal phalanx. Proximally, it transitions into a thinner, more membranous tissue that attaches to the metacarpal neck, forming a redundant pouch that accommodates joint flexion. The volar plate is intimately associated with the deep transverse metacarpal ligament, which tethers the volar plates of adjacent digits together, and the sagittal bands of the extensor mechanism. In a complex dislocation, it is the proximal membranous attachment that fails, allowing the thick, distal fibrocartilaginous portion to become incarcerated within the joint space.
Kaplan’s anatomical description of the constricting noose remains a cornerstone of hand surgery education. When the metacarpal head is driven volarly, it herniates through a specific anatomical window. The volar boundary of this noose is formed by the natatory ligament and the superficial transverse metacarpal ligament, which become taut and tether the palmar skin, creating the pathognomonic "pucker" sign. The dorsal boundary is the displaced, inverted volar plate. The radial boundary is formed by the lumbrical muscle, while the ulnar boundary consists of the flexor tendons (flexor digitorum superficialis and profundus). This unyielding perimeter tightly grips the metacarpal neck, explaining why simple longitudinal traction is highly counterproductive.
The neurovascular anatomy surrounding the MCP joint is of paramount surgical importance, particularly when selecting the operative approach. The radial and ulnar digital nerves course volarly, intimately associated with the flexor tendon sheath and the lumbrical muscles. In the setting of a complex volar dislocation of the metacarpal head, the radial digital nerve (in the index finger) is violently displaced and severely tented directly beneath the proximal palmar skin crease. This abnormal superficial displacement places the nerve at imminent risk of iatrogenic transection if a traditional volar surgical approach is utilized. The dorsal approach, conversely, maintains these critical neurovascular structures safely volar to the dissection field, fundamentally altering the risk profile of the procedure.
Exhaustive Indications and Contraindications
The decision-making process for managing MCP joint dislocations hinges on the accurate differentiation between simple and complex variants, as well as the identification of concurrent skeletal and soft tissue injuries. Absolute indications for operative intervention are primarily dictated by the mechanical irreducibility of the joint and the presence of intra-articular pathology that precludes a stable, congruent closed reduction. The presence of the pathognomonic palmar skin dimple, or "pucker," is a definitive clinical indicator that the volar plate is interposed and the natatory ligament is tethering the dermis. Upon observation of this sign, further attempts at closed reduction must be immediately abandoned to prevent iatrogenic chondral scoring of the metacarpal head.
Historically, the volar approach, as initially described by Kaplan, was utilized to directly release the constricting volar structures. However, the paradigm has shifted significantly toward the dorsal approach, championed by Becton et al. The dorsal approach is now considered the gold standard for complex MCP dislocations due to its superior neurovascular safety profile and the direct trajectory it provides to the primary offending pathology—the interposed volar plate. Furthermore, the dorsal approach allows for seamless extension of the incision to address concurrent dorsal capsular avulsions, sagittal band ruptures, or osteochondral shear fractures of the metacarpal head, which are exceedingly difficult to visualize and fixate from a volar perspective.
Relative indications for open reduction include delayed presentations (injuries presenting more than 24-48 hours post-trauma), where profound soft tissue edema and early contracture of the intrinsic musculature render closed reduction highly improbable and excessively traumatic. Additionally, the presence of an intra-articular sesamoid bone on preoperative radiographs is a strong predictor of irreducibility, as the sesamoid is embedded within the volar plate and signifies its interposition. Concurrent metacarpal shaft or neck fractures with unacceptable rotational malalignment or shortening also necessitate open reduction and internal fixation, which can often be addressed concurrently through the same or an extended dorsal approach.
Contraindications to the dorsal open reduction are remarkably few but clinically significant. Active superficial or deep space infections of the hand represent an absolute contraindication to elective open reduction and internal fixation, necessitating source control and antibiotic therapy prior to definitive joint management. Severe, medically unoptimized comorbidities that preclude the safe administration of regional or general anesthesia may force the surgeon to accept a sub-optimal closed reduction or pursue non-operative management, though this is exceedingly rare. Simple dislocations that reduce concentrically with a single, gentle closed maneuver (utilizing wrist flexion and MCP hyperextension) without residual instability or mechanical block do not require open intervention.
| Parameter | Indications for Dorsal Open Reduction | Contraindications |
|---|---|---|
| Clinical Findings | Presence of palmar skin "pucker" / dimple; Failed single attempt at closed reduction; Irreducible joint. | Simple, easily reducible dislocation with concentric joint space; Lack of mechanical block. |
| Radiographic Findings | Widened joint space; Sesamoid interposed in joint; Osteochondral shear fractures; Concurrent unstable metacarpal fractures. | Concentric reduction confirmed on post-reduction true lateral and AP radiographs. |
| Timing & Tissue | Acute complex dislocation; Delayed presentation (>48 hours) with irreducible joint. | Active cellulitis or deep space infection overlying the dorsal MCP joint. |
| Patient Factors | High-demand patient requiring anatomical restoration; Polytrauma requiring rigid fixation for mobilization. | Medically unstable patient unfit for anesthesia; Severe baseline dementia precluding post-op splinting (relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning begins with a comprehensive clinical and radiographic evaluation. The physical examination must meticulously document the resting posture of the hand, the presence of the palmar pucker sign, and a rigorous assessment of the digital neurovascular status. Two-point discrimination should be tested and recorded for both the radial and ulnar aspects of the involved digit, as the digital nerves are under extreme tension and may exhibit preoperative neuropraxia. Radiographic evaluation must include true anteroposterior (AP), lateral, and oblique views of the specific digit, not merely standard views of the hand. The lateral view is critical for identifying the dorsal displacement of the proximal phalanx and the presence of interposed sesamoids, while the AP view may reveal subtle widening of the joint space indicative of soft tissue interposition.
In cases where plain radiography suggests an osteochondral shear fracture of the metacarpal head, preoperative Computed Tomography (CT) scanning with fine cuts (0.5 mm to 1.0 mm) and 3D reconstructions should be strongly considered. CT imaging allows for precise templating of the fracture fragments, determining their size, location, and the feasibility of internal fixation versus excision. If internal fixation is anticipated, the surgeon must ensure that appropriate micro-fragment sets (1.5 mm and 2.0 mm screws), headless compression screws, and bioabsorbable pins are readily available in the operating theater. Templating also involves anticipating the need for concurrent metacarpal shaft fixation, ensuring that intramedullary K-wires or low-profile titanium plates are on hand.
Anesthesia selection is a collaborative decision between the surgeon, the anesthesiologist, and the patient. A regional brachial plexus block (supraclavicular or axillary) is generally preferred, as it provides profound intraoperative muscle relaxation—essential for overcoming the deforming forces of the intrinsic and extrinsic musculature—and affords excellent postoperative analgesia. General anesthesia is a viable alternative, particularly in polytrauma patients or those with contraindications to regional blockade. Regardless of the anesthetic modality, complete paralysis of the forearm and hand musculature is critical; attempting an open reduction against active muscle tone significantly increases the risk of iatrogenic cartilage damage.
Patient positioning and operating room setup must be optimized for microsurgical precision and fluoroscopic access. The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table. A well-padded pneumatic arm tourniquet is applied to the proximal arm. Following standard skin preparation and draping, the limb is exsanguinated utilizing an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg (or strictly 100 mm Hg above the patient's systolic blood pressure). A completely bloodless field is absolutely mandatory; the visual differentiation between the interposed fibrocartilaginous volar plate and the articular cartilage of the metacarpal head is notoriously difficult and relies heavily on subtle color and texture variations that are easily obscured by minor bleeding. Intraoperative fluoroscopy (mini C-arm) must be positioned perpendicularly to the hand table, draped sterilely, and readily available to confirm concentric reduction and evaluate hardware placement.
Step-by-Step Surgical Approach and Fixation Technique
1. Incision and Superficial Dissection
The surgical approach begins with a 4-cm longitudinal midline incision centered directly over the dorsal aspect of the dislocated metacarpophalangeal joint. While slightly curved or lazy-S incisions can be utilized to prevent scar contracture, a straight longitudinal incision provides the most direct and extensile access to the extensor mechanism. Dissection proceeds through the subcutaneous tissues using sharp and blunt techniques. Extreme care must be exercised to identify, mobilize, and protect the dorsal sensory branches of the radial or ulnar nerves, as well as the prominent dorsal venous network. Retraction of these structures should be performed with vessel loops or blunt retractors to prevent neuropraxia or postoperative venous congestion.
2. Extensor Mechanism Splitting
Once the subcutaneous tissues are cleared, the extensor digitorum communis (EDC) tendon is identified. The EDC tendon is split longitudinally in the exact midline over the MCP joint using a #15 scalpel blade. This longitudinal split is carried directly through the underlying dorsal joint capsule, effectively performing a dorsal arthrotomy to expose the articular space. The split halves of the extensor tendon and the dorsal capsule are then gently retracted radially and ulnarly using fine skin hooks or small Senn retractors. It is crucial to maintain the integrity of the sagittal bands during this split to prevent postoperative extensor tendon subluxation.
3. Identification of the Volar Plate
Upon entering the joint space, the surgeon will immediately observe the dorsal base of the proximal phalanx. However, the metacarpal head will be conspicuously absent from view, obscured by a smooth, glistening structure covering its dorsal aspect. This structure is the interposed fibrocartilaginous volar plate.
⚠️ Surgical Warning: Visualizing the Volar Plate
The fibrocartilaginous volar plate can be exceptionally difficult to identify because its color and texture are nearly identical to the articular cartilage of the metacarpal head. Furthermore, its torn proximal margin may be folded, tucked, or completely hidden beneath the base of the proximal phalanx. Do not aggressively scrape, curette, or incise what you believe to be the volar plate without absolute confirmation, as you may inadvertently score the pristine articular cartilage of the metacarpal head, leading to irreversible iatrogenic damage.
To safely confirm the identity of the tissue, the surgeon should make a very small, cautious test incision (a "nick") into the center of the structure using the tip of a #15 blade. If the structure is indeed the volar plate, the surgeon will feel the distinct, gritty fibrous resistance of the tissue. As the nick is deepened, the true, pearlescent articular cartilage of the metacarpal head will be revealed beneath it.
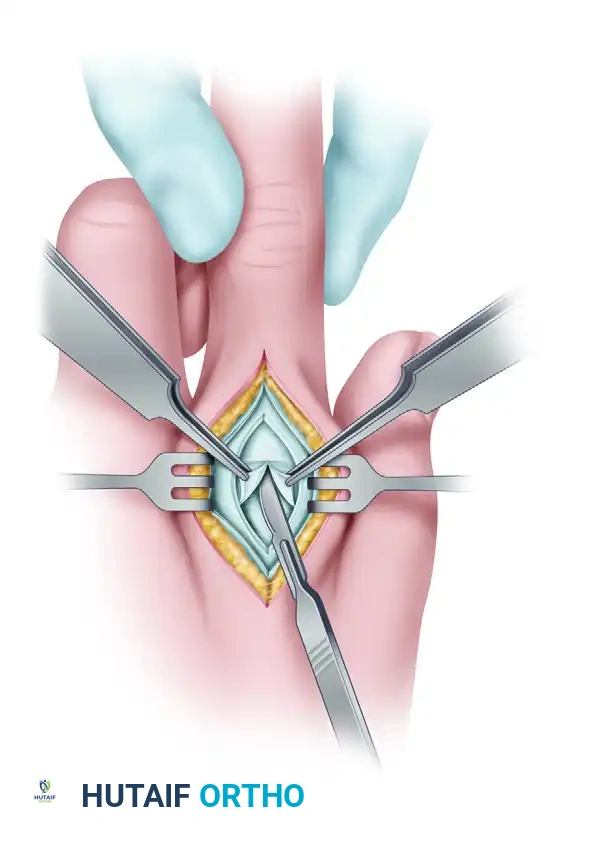
4. Incision of the Volar Plate and The Reduction Maneuver
Once the volar plate is positively identified, the longitudinal incision is completed directly through its center, bisecting the structure from proximal to distal. This is the critical, defining step of the dorsal approach: bisecting the volar plate effectively breaks the dorsal aspect of the constricting anatomical noose, instantly releasing the tension holding the metacarpal head captive.
With the volar plate incised, the reduction maneuver can be performed atraumatically. The sequence of movements is biomechanically critical:
* Flex the wrist volarward: This step is paramount. Wrist flexion releases the passive tension on the flexor digitorum superficialis and profundus tendons, which form the unyielding ulnar border of the constricting noose.
* Apply longitudinal traction: Apply gentle, sustained traction to the affected finger.
* Flex the MCP joint: While maintaining traction and wrist flexion, gently flex the metacarpophalangeal joint. The base of the proximal phalanx should easily glide over the metacarpal head, achieving a palpable and visual concentric reduction. Under no circumstances should the joint be hyperextended during this reduction maneuver, as this replicates the primary mechanism of injury and will exacerbate soft tissue trauma.
5. Joint Inspection, Debridement, and Concurrent Fracture Management
Following successful reduction, the joint must be thoroughly irrigated with sterile saline. The articular surface of the metacarpal head is meticulously inspected for osteochondral shear fractures, which may have occurred during the initial dislocation or during prior forceful closed reduction attempts. Any loose cartilaginous or osteochondral bodies lodged in the collateral ligament recesses or the volar pouch must be meticulously removed to prevent mechanical locking and post-traumatic osteoarthritis.
Management of Concurrent Metacarpal Fractures
If a large, structural osteochondral fragment is present, it must be anatomically reduced and fixed utilizing 1.5 mm headless compression screws or bioabsorbable pins, ensuring the hardware is countersunk beneath the articular surface. Furthermore, if the trauma resulted in concurrent metacarpal shaft or neck fractures, these must be addressed immediately following joint reduction.
* Transverse/Short Oblique Fractures: Highly amenable to intramedullary fixation using the "Bouquet" technique. Multiple pre-bent 0.8 mm or 1.0 mm K-wires are introduced retrograde through the collateral ligament recesses of the metacarpal head, providing excellent longitudinal stability.
* Long Oblique/Spiral Fractures: Require interfragmentary lag screw fixation (1.5 mm or 2.0 mm) placed exactly perpendicular to the fracture plane. If comminution is present, a dorsal neutralization plate (2.0 mm low-profile titanium) is applied to resist torsional forces. Rotational alignment must be clinically verified via the tenodesis effect before final tightening of any hardware.
6. Closure
The incised volar plate does not require primary repair. It will heal reliably via secondary intention. Attempting to repair the bisected volar plate is not only technically demanding but significantly increases the risk of severe, intractable postoperative flexion contractures. The longitudinally split dorsal joint capsule and the extensor tendon are repaired as a single layer using a running or interrupted 4-0 non-absorbable or slowly absorbable suture (e.g., PDS, Prolene, or Ethibond). The skin is closed with 5-0 nylon horizontal mattress sutures to ensure skin edge eversion. A sterile, non-adherent dressing is applied, followed by a custom dorsal blocking splint.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, open reduction of complex MCP dislocations carries a distinct profile of potential complications. The most ubiquitous complication is postoperative stiffness, specifically a loss of terminal MCP joint extension and varying degrees of flexion contracture. This stiffness is multifactorial, stemming from capsular scarring, extensor tendon adhesions at the site of the longitudinal split, and the inherent fibroplasia associated with joint trauma. The incidence of clinically significant stiffness can approach 30-40%, underscoring the absolute necessity of rigorous, supervised hand therapy.
Iatrogenic neurovascular injury is a devastating complication that historically plagued the volar approach. Transection of the radial digital nerve can lead to painful neuroma formation and permanent sensory deficits. The advent of the dorsal approach has reduced the incidence of digital nerve injury to near zero, provided the surgeon respects the dorsal sensory branches during the superficial dissection. If a dorsal sensory nerve is inadvertently injured, it should be cleanly transected and buried into adjacent muscle or bone to prevent symptomatic neuroma formation.
Post-traumatic osteoarthritis is a late complication, directly correlated with the severity of the initial chondral impact and the presence of missed osteochondral shear fragments. Avascular necrosis (AVN) of the metacarpal head is an exceedingly rare but reported complication, resulting from extensive stripping of the collateral ligaments and the dorsal capsular blood supply. Salvage management for end-stage osteoarthritis or AVN depends heavily on the patient's age and functional demands. In low-demand or elderly patients, silicone arthroplasty (e.g., Swanson implant) provides excellent pain relief and functional motion. In young, high-demand laborers, MCP joint arthrodesis positioned in 25-30 degrees of flexion provides a stable, pain-free grip, albeit at the cost of joint mobility.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Joint Stiffness / Adhesions | 30% - 40% | Prolonged immobilization; Extensor tendon splitting; Capsular scarring. | Prevention: Early active motion at 3-5 days. Salvage: Tenolysis and dorsal capsulectomy at 6 months post-op. |
| Post-Traumatic Osteoarthritis | 10% - 20% | Missed osteochondral fragments; Severe initial cartilage impaction. | Prevention: Meticulous joint debridement. Salvage: Silicone arthroplasty or MCP joint arthrodesis. |
| Iatrogenic Nerve Injury | < 1% (Dorsal) / ~10% (Volar) | Tented digital nerves in volar approach; Careless superficial dorsal dissection. | Prevention: Strict adherence to dorsal approach. Salvage: Microsurgical nerve repair or neuroma burial. |
| Recurrent Instability | < 2% | Failure to recognize collateral ligament avulsions; Premature return to sport. | Prevention: Strict adherence to 3-week dorsal blocking splint protocol. Salvage: Ligament reconstruction. |
| Avascular Necrosis (AVN) | < 1% | Excessive soft tissue stripping of the metacarpal neck and collateral ligaments. | Prevention: Preserve collateral ligament attachments. Salvage: Arthroplasty or Arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation paradigm for complex MCP dislocations is a delicate balancing act: the surgeon and hand therapist must protect the healing soft tissues from recurrent hyperextension while simultaneously initiating early motion to prevent crippling extensor tendon adhesions and capsular contractures. A rigid, protocol-driven approach is essential for optimizing functional outcomes.
Phase I: Immediate Postoperative Protection (Weeks 0-3)
Immediately following skin closure in the operating room, the hand is placed in a custom-fabricated thermoplastic dorsal blocking splint. The wrist is positioned in 20 to 30 degrees of extension to optimize the mechanical advantage of the flexor tendons. Crucially, the MCP joints must be blocked from extending past 30 degrees of flexion, effectively neutralizing the tension on the healing volar structures and preventing hyperextension. The interphalangeal (IP) joints are left completely free. Within 3 to 5 days postoperatively, once acute edema subsides, the patient begins early active and active-assisted MCP joint flexion exercises within the constraints of the splint. Active IP joint motion is encouraged immediately to facilitate edema pumping and prevent flexor tendon adhesions. The splint is worn 24 hours a day, removed only for supervised hygiene and therapy sessions.
Phase II: Splint Weaning and Progressive Motion (Weeks 3-6)
At precisely three weeks postoperatively, the dorsal blocking splint is discontinued during the day, though it may be worn at night for an additional week if the patient is apprehensive. The focus shifts to restoring full active and passive range of motion. Progressive active extension exercises are initiated. If the patient exhibits a persistent flexion contracture, dynamic extension splinting (e.g., a Capener splint or dynamic outrigger) may be introduced during the day for 30-minute intervals. Scar massage and desensitization techniques are aggressively employed over the dorsal incision. Strengthening exercises utilizing therapeutic putty and hand grippers are gradually introduced toward the end of week five.
Phase III: Strengthening and Return to Function (Weeks 6-12)
By week six, the soft tissues are sufficiently healed to withstand normal physiological loads. Aggressive strengthening of the intrinsic and extrinsic hand musculature is the primary objective. Patients are cleared for heavy lifting and unrestricted activities of daily living. For athletes or laborers engaged in strenuous activities, "buddy taping" the affected digit to an adjacent stable digit is highly recommended for an additional 2 to 4 weeks to provide dynamic collateral support and prevent accidental hyperextension injuries during sudden loading events. Final clinical and radiographic evaluation is typically performed at 12 weeks, at which point maximum medical improvement is generally achieved, though subtle improvements in motion may continue for up to a year.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for complex MCP joint dislocations is a fascinating study in anatomical discovery and surgical refinement. Emanuel Kaplan’s original 1957 publication in the Journal of Bone and Joint Surgery remains the foundational text for understanding the pathomechanics of this injury. Kaplan brilliantly delineated the anatomical "noose" that entraps the metacarpal head, and logically, he advocated for a volar surgical approach to directly incise the constricting natatory and transverse metacarpal ligaments. While anatomically sound, Kaplan’s volar approach was fraught with peril due to the severe displacement of the digital neurovascular bundles, leading to unacceptably high rates of iatrogenic nerve transection in the hands of less experienced surgeons.
The paradigm shifted dramatically in 1975 when Becton, Christian, Goodwin, and Jackson published their landmark series advocating for the dorsal approach. Becton et al. recognized that the primary impediment to reduction was not the volar ligaments, but the interposed volar plate itself. By approaching the joint dorsally, they demonstrated that the digital nerves were completely protected, the volar plate could be directly visualized and bisected, and concurrent osteochondral fractures could be easily managed. The dorsal approach rapidly became the gold standard, fundamentally altering the risk-benefit ratio of the procedure.
Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) unequivocally support the dorsal approach for all complex MCP joint dislocations. The guidelines emphasize the critical importance of recognizing the "pucker" sign, avoiding repeated and forceful closed reduction attempts, and ensuring the availability of micro-fixation equipment for potential osteochondral shear fractures. Recent literature has also begun to explore arthroscopically assisted reductions for complex dislocations, utilizing standard radiocarpal portals adapted for the MCP joint. While technically demanding and requiring specialized small-joint equipment, arthroscopic management offers the theoretical advantages of minimized capsular scarring and faster rehabilitation, representing the next frontier in the evolution of managing these complex digital injuries.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons ---
