Open Reduction of MCP Dislocations: Dorsal Approach
Key Takeaway
Complex metacarpophalangeal (MCP) joint dislocations are characterized by the interposition of the volar plate, rendering them irreducible to closed maneuvers. The dorsal surgical approach, as advocated by Becton et al., provides superior visualization of the entrapped volar plate while minimizing the risk of iatrogenic injury to the digital neurovascular bundles. This guide details the step-by-step dorsal approach for open reduction and addresses concurrent metacarpal fractures.
PATHOMECHANICS OF COMPLEX METACARPOPHALANGEAL JOINT DISLOCATIONS
Metacarpophalangeal (MCP) joint dislocations most frequently occur in the index or little fingers and are typically the result of a forced hyperextension injury. These injuries are broadly classified into simple (reducible) and complex (irreducible) dislocations. The hallmark of a complex MCP joint dislocation is the interposition of the fibrocartilaginous volar plate between the base of the proximal phalanx and the metacarpal head, which physically blocks closed reduction maneuvers.
In a classic complex dislocation of the index finger, the metacarpal head is driven volarly through the proximal membranous attachment of the volar plate. The volar plate remains attached to the base of the proximal phalanx and is flipped dorsally over the metacarpal head. A constricting anatomical "noose" is subsequently formed around the metacarpal neck:
* Volar: The natatory ligament and the superficial transverse metacarpal ligament.
* Dorsal: The displaced volar plate.
* Radial: The lumbrical muscle.
* Ulnar: The flexor tendons (flexor digitorum superficialis and profundus).
Traction applied during attempted closed reduction only tightens this noose, further strangulating the metacarpal neck and rendering the dislocation truly irreducible. Consequently, open reduction is strictly indicated.
RATIONALE FOR THE DORSAL APPROACH
Historically, the volar approach (as described by Kaplan) was utilized to release the constricting structures. However, the volar approach carries a significant risk of iatrogenic injury to the digital neurovascular bundles. In a complex dislocation, the metacarpal head is displaced volarly, severely tenting the radial digital nerve directly beneath the skin crease. A volar incision places this nerve at imminent risk of transection.
Becton et al. revolutionized the management of these injuries by advocating for the dorsal approach, which offers several distinct biomechanical and anatomical advantages over the volar approach:
1. Neurovascular Safety: The digital nerves remain volar to the dissection field and are highly unlikely to be injured.
2. Direct Visualization of the Pathology: The dorsal approach provides immediate, full exposure of the interposed fibrocartilaginous volar plate, which is the primary structure blocking reduction.
3. Access to Osteochondral Fractures: Occult fractures of the metacarpal head or osteochondral shear fragments are easily identified, reduced, and internally fixed through a dorsal window.
4. Simplicity of Release: Longitudinally splitting the entrapped volar plate from a dorsal perspective immediately releases the constricting noose, allowing for a gentle, atraumatic reduction.
💡 Clinical Pearl: The "Puckered" Skin Sign
A pathognomonic clinical finding of a complex MCP joint dislocation is the presence of a skin dimple or "pucker" in the proximal palmar crease. This occurs because the natatory ligament is pulled dorsally by the displaced proximal phalanx, tethering the palmar skin. If this sign is present, closed reduction should be abandoned immediately to prevent further cartilaginous damage, and the patient should be prepared for open reduction.
PREOPERATIVE PREPARATION AND POSITIONING
- Anesthesia: Regional anesthesia (brachial plexus block) or general anesthesia is preferred to ensure complete muscle relaxation, which is critical for overcoming the deforming forces of the intrinsic and extrinsic musculature.
- Positioning: The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic arm tourniquet is applied and inflated to 250 mm Hg (or 100 mm Hg above systolic blood pressure) after exsanguination of the limb with an Esmarch bandage. A bloodless field is mandatory for identifying the volar plate and assessing cartilaginous integrity.
- Imaging: Intraoperative fluoroscopy (C-arm) must be available to confirm concentric reduction and evaluate for occult fractures.
SURGICAL TECHNIQUE: OPEN REDUCTION—DORSAL APPROACH
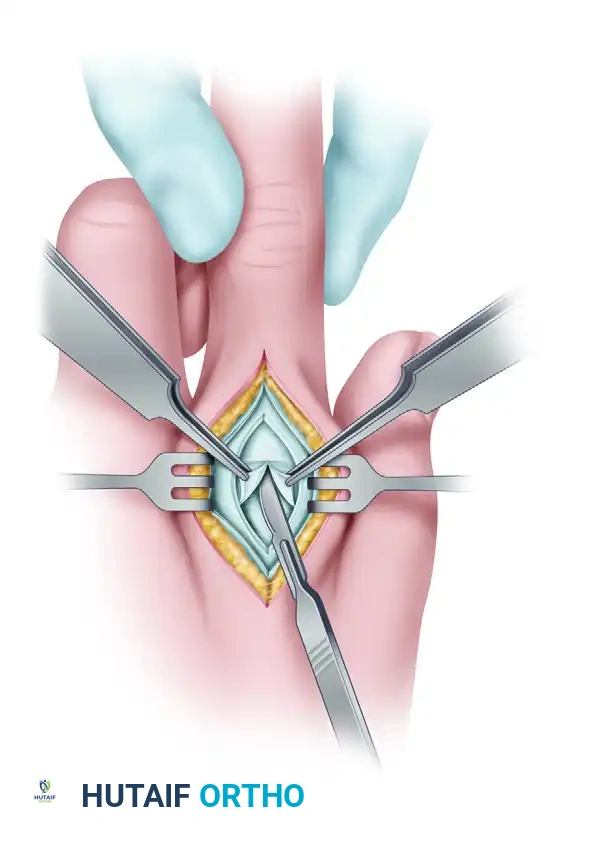
1. Incision and Superficial Dissection
Make a 4-cm longitudinal midline incision directly over the dorsal aspect of the dislocated metacarpophalangeal joint. Carefully dissect through the subcutaneous tissues, taking care to identify and retract the dorsal sensory branches of the radial or ulnar nerves, as well as the dorsal venous network.
2. Extensor Mechanism Splitting
Identify the extensor digitorum communis (EDC) tendon. Split the EDC tendon longitudinally in the midline over the MCP joint. Continue this longitudinal split directly through the underlying dorsal joint capsule to expose the articular space. Retract the split halves of the extensor tendon and capsule radially and ulnarly using fine skin hooks or small Senn retractors.
3. Identification of the Volar Plate
Upon entering the joint, the base of the proximal phalanx will be visible dorsally, but the metacarpal head will be obscured. The structure covering the dorsal aspect of the metacarpal head is the interposed fibrocartilaginous volar plate.
⚠️ Surgical Warning: Visualizing the Volar Plate
The fibrocartilaginous volar plate can be exceptionally difficult to identify because its color and texture are nearly identical to the articular cartilage of the metacarpal head. Furthermore, its torn proximal margin may be folded or hidden. Do not aggressively scrape or incise what you believe to be the volar plate without confirmation, as you may inadvertently score the articular cartilage of the metacarpal head.
To safely confirm the identity of the tissue, make a very small, cautious test incision (a "nick") into the structure. If it is the volar plate, you will feel the fibrous resistance of the tissue and eventually reveal the true articular cartilage of the metacarpal head beneath it.
4. Incision of the Volar Plate
Once the volar plate is positively identified, complete the longitudinal incision directly through its center. This critical step bisects the volar plate, effectively breaking the dorsal aspect of the constricting anatomical noose and releasing the tension holding the metacarpal head captive.
5. The Reduction Maneuver
With the volar plate incised, the reduction can be performed atraumatically.
* Flex the wrist volarward: This is a crucial biomechanical step. Wrist flexion releases the passive tension on the flexor digitorum superficialis and profundus tendons, which form the ulnar border of the constricting noose.
* Apply longitudinal traction: Apply gentle traction to the affected finger.
* Flex the MCP joint: While maintaining traction, flex the metacarpophalangeal joint. The proximal phalanx should easily glide over the metacarpal head, achieving a concentric reduction.
Do not hyperextend the joint during reduction, as this was the primary mechanism of injury and will only exacerbate soft tissue trauma.
6. Joint Inspection and Debridement
Following reduction, thoroughly irrigate the joint. Observe the articular surface of the metacarpal head to see if any free cartilage is missing. Osteochondral shear fractures can occur during the initial dislocation or during forceful closed reduction attempts. Any loose cartilaginous or osteochondral bodies lodged in the joint space must be meticulously removed to prevent post-traumatic osteoarthritis and mechanical locking. If a large, structural osteochondral fragment is present, it should be reduced and fixed with headless compression screws or bioabsorbable pins.
7. Closure
The incised volar plate does not require repair; it will heal via secondary intention, and repairing it may lead to severe flexion contractures.
* Repair the longitudinally split dorsal joint capsule and the extensor tendon using a running or interrupted 4-0 non-absorbable or slowly absorbable suture (e.g., PDS or Prolene).
* Close the skin with 5-0 nylon sutures.
* Apply a sterile, non-adherent dressing.
POSTOPERATIVE PROTOCOL FOR MCP DISLOCATIONS
The primary goal of postoperative rehabilitation is to prevent stiffness while protecting the joint from recurrent hyperextension.
* Immobilization: Immediately postoperatively, place the hand in a dorsal blocking splint. The wrist should be in 20 degrees of extension, and the MCP joints must be blocked from extending past 30 degrees of flexion. The interphalangeal (IP) joints are left free.
* Early Motion: Begin early active MCP joint flexion exercises within the constraints of the dorsal blocking splint within 3 to 5 days postoperatively. Active IP joint motion is encouraged immediately to prevent tendon adhesions.
* Splint Duration: Protect the MCP joint from hyperextension with the splint for exactly 3 weeks.
* Weaning: After 3 weeks, the splint is discontinued, and progressive active and passive extension exercises are initiated. Buddy taping may be utilized for an additional 2 to 3 weeks during athletic or strenuous activities.
METACARPAL SHAFT AND NECK FRACTURES
While complex MCP dislocations require meticulous soft tissue management, high-energy trauma to the hand frequently results in concurrent fractures of the metacarpal shafts or necks. The management of these fractures is dictated by the fracture pattern, the degree of displacement, and the presence of soft tissue compromise.
Indications for Operative Intervention
Metacarpal shaft fractures are usually treated by closed methods (e.g., ulnar gutter splinting for boxer's fractures) when angulation is within acceptable limits and no rotational deformity is present. However, internal fixation is strictly indicated under the following conditions:
1. Multiple Metacarpal Fractures: Loss of the internal splinting effect of adjacent intact metacarpals leads to profound instability.
2. Open Fractures: Associated with severe soft tissue trauma requiring rigid skeletal stabilization to facilitate wound care and soft tissue healing.
3. Rotational Malalignment: The most critical factor in metacarpal reduction. Even 5 degrees of rotational malalignment at the metacarpal shaft can result in 1.5 cm of digital overlap (scissoring) at the fingertips during composite fist flexion, severely impairing grip function.
4. Unacceptable Angulation or Shortening: Apex dorsal angulation exceeding 10-15 degrees in the index/long fingers, or shortening greater than 3-5 mm, alters the biomechanics of the intrinsic muscles and weakens grip strength.
💡 Clinical Pearl: Assessing Rotational Alignment
Rotational alignment cannot be accurately assessed on standard anteroposterior or lateral radiographs. It is a purely clinical diagnosis. Intraoperatively, after provisional fixation, the wrist must be extended, and the fingers passively flexed into the palm (the tenodesis effect). All fingertips should point symmetrically toward the scaphoid tubercle. Any crossing or "scissoring" of the digits indicates unacceptable rotational malalignment that must be corrected.
Surgical Fixation Strategies
The choice of internal fixation depends heavily on the fracture morphology:
Transverse Midshaft Fractures
Transverse fractures typically present with significant apex dorsal angulation due to the deforming forces of the volar interosseous muscles.
* Intramedullary (IM) Wires: These fractures are highly amenable to fixation with intramedullary K-wires. The "Bouquet" technique utilizes multiple pre-bent, blunt-tipped K-wires introduced antegrade through the metacarpal base or retrograde through the collateral ligament recesses of the metacarpal head. This provides excellent longitudinal and angular stability while allowing for early mobilization.
* Plate Fixation: For rigid fixation, especially in multiple fractures or open injuries, dorsal plating with 2.0 mm or 2.4 mm low-profile titanium plates provides absolute stability.
Oblique and Spiral Fractures
Oblique fractures are inherently unstable and prone to shortening and rotational deformity.
* Interfragmentary Screws: Certain long oblique fractures (where the fracture length is at least twice the diameter of the bone) can be fixed with multiple interfragmentary lag screws (1.5 mm or 2.0 mm). The screws must be placed exactly perpendicular to the fracture plane to achieve maximum interfragmentary compression without inducing shear forces.
* Lag Screw and Neutralization Plate: If the oblique fracture is highly comminuted or the bone quality is poor, interfragmentary lag screws should be protected with a dorsally applied neutralization plate to resist torsional and bending forces during early rehabilitation.
Postoperative Rehabilitation for Metacarpal Fractures
Following rigid internal fixation, the goal is immediate, controlled mobilization to prevent extensor tendon adhesions, which are the most common complication of dorsal hand surgery. A custom thermoplastic splint is fabricated, allowing for active range of motion exercises under the guidance of a certified hand therapist. Heavy lifting and contact sports are restricted until radiographic union is confirmed, typically at 6 to 8 weeks postoperatively.
You Might Also Like