Mastering Open Reduction of Hip and Sternoclavicular Dislocations

Key Takeaway
Open reduction of a hip dislocation is indicated when closed reduction fails or when intra-articular incarcerated fragments prevent concentric reduction. The surgical approach mandates meticulous capsular assessment, removal of intervening soft tissue or osteochondral debris, and precise labral repair. Concurrently, sternoclavicular dislocations require rigorous diagnostic imaging and careful reduction maneuvers, with posterior dislocations necessitating urgent intervention due to mediastinal risks.
INTRODUCTION TO HIGH-ENERGY ARTICULAR DISLOCATIONS
High-energy trauma frequently results in complex articular dislocations that demand immediate, precise, and evidence-based orthopedic intervention. Among the most critical of these are hip dislocations and sternoclavicular (SC) joint dislocations. Both injuries present unique biomechanical challenges, severe risks to adjacent neurovascular structures, and a high potential for long-term morbidity if mismanaged.
This comprehensive guide details the surgical techniques, closed reduction maneuvers, and postoperative protocols required to manage these complex dislocations effectively. The principles outlined herein are designed for orthopedic residents, fellows, and practicing consultants striving for mastery in operative trauma management.
PART I: OPEN REDUCTION OF HIP DISLOCATION
Hip dislocations are severe injuries typically resulting from high-velocity dashboard impacts or falls from a significant height. While closed reduction under conscious sedation or general anesthesia is the first line of treatment, open reduction becomes mandatory under specific clinical scenarios.
Indications for Open Reduction
Open reduction of a hip dislocation is not a routine primary procedure but is strictly indicated in the following scenarios:
* Irreducible Dislocation: Failure to achieve a concentric closed reduction after two to three well-executed attempts under adequate muscle relaxation.
* Non-Concentric Reduction: Post-reduction imaging (radiographs or CT) reveals a widened joint space, indicating incarcerated osteochondral fragments, labrum, or capsular tissue.
* Neurological Deterioration: A sciatic nerve deficit that develops or worsens after a closed reduction attempt.
* Associated Fractures: Dislocation accompanied by displaced femoral head fractures (Pipkin classification) or complex acetabular fractures requiring surgical fixation.
Surgical Warning: Repeated, forceful attempts at closed reduction in an irreducible hip significantly increase the risk of iatrogenic femoral head cartilage damage, femoral neck fracture, and subsequent osteonecrosis (AVN). If the hip does not reduce with smooth, controlled maneuvers, proceed directly to open reduction.
Closed Reduction Maneuvers: A Prerequisite to Open Intervention
Before resorting to open reduction, the surgeon must be adept at various closed reduction techniques. These maneuvers rely on specific biomechanical principles to navigate the femoral head back over the acetabular rim.
1. The Allis Maneuver
The patient is placed supine. The surgeon applies in-line traction to the flexed hip and knee, gradually increasing the force while an assistant stabilizes the pelvis. Gentle internal and external rotation helps guide the femoral head into the acetabulum.

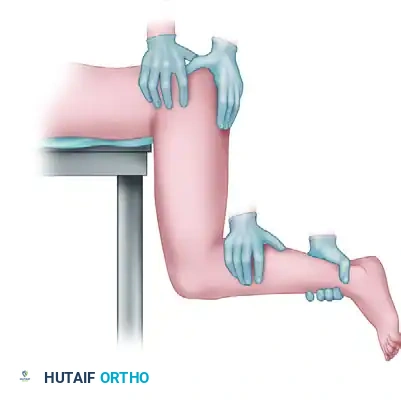
2. The Stimson Maneuver
The patient is placed prone with the affected leg hanging off the edge of the stretcher, flexing the hip and knee to 90 degrees. Gravity assists the surgeon as downward pressure is applied to the proximal calf.
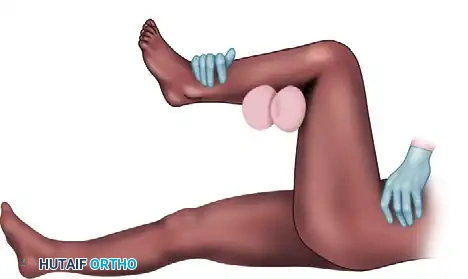
3. The Lefkowitz Maneuver
This technique utilizes the physician’s knee as a fulcrum for the affected limb. The surgeon's left hand levers the ipsilateral ankle and controls rotation, providing a mechanical advantage to gently lift the femoral head into the joint.


4. The East Baltimore Lift
This highly effective maneuver requires three providers. The physician and an assistant stand on opposite sides of the patient, crossing their arms under the patient's flexed calf to act as a fulcrum, while the ankle is used as a lever. A second assistant firmly stabilizes the pelvis.


Surgical Technique: Open Reduction (Technique 60-4)
When closed methods fail, open reduction must be executed with meticulous respect for the delicate vascular supply to the femoral head, primarily the medial femoral circumflex artery (MFCA).
Step 1: Approach and Exposure
* Posterior Dislocations: Utilize the Kocher-Langenbeck approach. This provides excellent visualization of the posterior column, capsule, and sciatic nerve.
* Anterior Dislocations: Utilize the Smith-Petersen (anterior) or Watson-Jones (anterolateral) approach, depending on the exact location of the femoral head and associated fractures.
Step 2: Capsular Assessment and Arthrotomy
* Regardless of the direction of the dislocation, once the deep approach has been made, assess the joint capsule first.
* If the femoral head is "buttonholed" through a small capsular defect, do not attempt to force it back through the tight rent. Instead, extend the traumatic capsulotomy in a T-shaped fashion along the acetabular rim.
* Crucial Step: Carefully preserve the acetabular labrum during this capsulotomy.
Step 3: Joint Inspection and Debridement
* Inspect the joint thoroughly for any intervening structures that prevented closed reduction. Common culprits include the capsule itself, a torn labrum, the piriformis muscle, or osteochondral bony fragments.
* If necessary, retract or distract the hip manually. For a superior assessment of the joint space, apply skeletal traction through a fracture table or utilize a femoral distractor (Schanz pins in the ilium and proximal femur).
Step 4: Reduction and Repair
* When the joint has been meticulously cleared of all debris, reduce the hip joint by releasing the traction and gently guiding the head into the acetabulum.
* Confirm concentric reduction visually and fluoroscopically.
* Repair the capsule along with the labrum using heavy non-absorbable sutures or suture anchors if the labrum is avulsed from the bony rim.
* Close the wound routinely in layers over a suction drain.
Clinical Pearl: Always palpate the acetabular fossa with a finger or a blunt instrument before reduction. Even a 2 mm osteochondral fragment left in the fossa can lead to rapid, catastrophic post-traumatic osteoarthritis.
Postoperative Care and Rehabilitation
Postoperative management is tailored to the stability of the reduction and the presence of associated injuries.
- Mobilization: Gait training is initiated as soon as the patient regains adequate motor control of the affected limb.
- Weight Bearing: Some authors have historically advocated for postoperative skeletal traction and protected weight-bearing to decrease the incidence of femoral head collapse from osteonecrosis. However, the biomechanical benefits of these measures remain unproven in contemporary literature. Touch-down weight bearing (TDWB) for 6 weeks is generally preferred if a fracture was fixed; otherwise, weight-bearing as tolerated (WBAT) may be permitted for simple dislocations.
- Positioning Precautions: Patients are strictly advised to avoid putting the hip in the position of the initial dislocation (e.g., flexion, adduction, and internal rotation for posterior dislocations).
- Orthotics: An abduction pillow is highly useful in the postoperative period, particularly for sedated, polytraumatized, or noncompliant patients with a previous posterior dislocation.
- Physical Therapy: Hip abductor and flexor strengthening, alongside gentle range-of-motion (ROM) exercises, are initiated early to prevent capsular contracture.
Complications of Hip Dislocation
1. Recurrent Instability
Recurrent instability occurs extremely rarely after a simple hip dislocation without an associated fracture. When it does occur, it is typically caused by massive capsular or labral defects, or profound capsular laxity.
* Management: Capsular repair, labral repair, and bone block augmentation have been advocated for the surgical treatment of recurrent hip instability. Soft tissue repair is warranted initially, with the addition of bony augmentation if acceptable stability cannot be demonstrated intraoperatively.
2. Post-Traumatic Osteoarthritis
Osteoarthritis is the most common long-term complication after hip dislocation.
* While a percentage of this results from late-stage osteonecrosis (AVN), a significant number of patients develop osteoarthritic changes without any radiographic signs of AVN.
* The radiographic distinction between these two entities can be challenging. Indentation fractures and transchondral fractures of the femoral head larger than 4 mm have been strongly associated with an increased risk of rapid-onset osteoarthritis.
3. Sciatic Nerve Palsy
Sciatic nerve palsy complicates simple posterior hip dislocations in approximately 13% of patients. Notably, no neurological sequelae have been reported after anterior hip dislocations.
* Anatomical Vulnerability: The peroneal portion of the sciatic nerve is significantly more commonly affected than the tibial branch. Possible explanations for this increased risk include the relationship of the peroneal distribution to the piriformis muscle, tethering of the nerve at the sciatic notch and fibular neck, and the overall internal morphology of the peroneal division (fewer supporting connective tissues).
* Prognosis: At least partial recovery of nerve function can be expected in approximately two-thirds of patients.
* Surgical Exploration: Significant controversy exists regarding the merits and timing of surgical exploration of the sciatic nerve if closed reduction has been successfully performed but nerve function does not improve. Tornetta and Mostafavi recommended nerve exploration only if sciatic function was normal before reduction and deteriorated immediately after closed reduction, suggesting iatrogenic entrapment.
PART II: STERNOCLAVICULAR JOINT DISLOCATIONS
While anatomically distant from the hip, sternoclavicular (SC) joint dislocations share the high-energy trauma etiology and require equally rigorous diagnostic and therapeutic precision. The SC joint is the sole true articular connection between the axial skeleton and the upper extremity.
Anatomy and Biomechanics
Whether the sternoclavicular joint subluxates or completely dislocates depends entirely on the extent of the injury to its stabilizing structures:
* The capsular ligaments (anterior and posterior).
* The intra-articular disc.
* The interclavicular ligament.
* The costoclavicular (rhomboid) ligament.
Diagnostic Pearl (Rockwood's Rule): Rockwood stressed the critical importance and frequency of injuries to the physis of the medial end of the clavicle. In patients younger than 25 years old, what appears to be an SC dislocation is very frequently a Salter-Harris physeal fracture-separation.
Diagnostic Imaging
Standard anteroposterior (AP) radiographs are often difficult to interpret due to overlapping mediastinal structures.
* Apical Lordotic View: An apical lordotic view of the upper thorax centered over the sternum is usually diagnostic. In this view, the medial end of the clavicle will project anteriorly or posteriorly relative to the normal clavicle on the opposite side.
* Special Radiographs: Additional special views, such as those suggested by Heinig, Hobbs, Kattan, and Rockwood, can be helpful.
* CT Scanning: Computed Tomography (CT) is the gold standard. It provides definitive visualization of the dislocation direction and assesses for compression of posterior mediastinal structures.
Management of Anterior SC Dislocations
Anterior dislocations are the most common and are generally benign regarding life-threatening complications.
- Closed Reduction (Heinig Technique): Heinig recommended closed reduction after infiltrating the hematoma with a local anesthetic using meticulous sterile technique.
- Positioning: The patient is placed supine with a large sandbag between the scapulae.
- Maneuver: Traction is applied to the affected extremity, and the arm is abducted and extended while direct downward pressure is applied over the dislocated medial end of the clavicle.
- Post-Reduction: When the dislocation is reduced, the joint is frequently unstable. The surgeon must decide whether to accept a residual subluxation or perform open reduction. Generally, in anterior dislocations, the cosmetic deformity is accepted due to the high complication rate of surgery. If later instability becomes painful, ligament reconstruction or resection of the medial end of the clavicle may be indicated.
Management of Posterior SC Dislocations
Posterior SC dislocations are true orthopedic emergencies due to the proximity of the medial clavicle to the trachea, esophagus, brachiocephalic veins, and subclavian arteries.
- Timing: Groh et al. found that early recognition (< 10 days) of posterior dislocations significantly improves the probability of accomplishing a successful closed reduction.
- Closed Reduction Maneuver: The patient is placed supine with a large sandbag between the scapulae. Traction is applied to the affected extremity, and the arm is abducted and extended. The clavicle is grasped with the fingers or a sterile towel clip (after sterile skin preparation), and anterior traction is exerted to assist in reduction.
- Buckerfield and Castle Maneuver: This alternative consists of traction on the affected arm with the shoulder in adduction, while a posteriorly directed force is applied to the shoulder and distal clavicle, levering the medial clavicle anteriorly.
- Immobilization: Most posterior dislocations are stable once reduced. Immobilization is achieved with a figure-of-eight soft dressing, a commercially prepared clavicular strap, or a figure-of-eight plaster dressing for 4 weeks. Activities are restricted for 6 weeks.
Open Reduction of the SC Joint
If reduction of a posterior dislocation cannot be obtained by closed methods under general anesthesia, open reduction is strictly indicated because of the severe dangers of leaving the joint dislocated into the mediastinum.
- Multidisciplinary Approach: If open reduction is necessary, a surgeon with thoracic or vascular surgery experience should be consulted and available on standby.
- Surgical Technique: Kennedy recommends open reduction and ligament reconstruction (using autograft or allograft) because of the significant injury to the joint capsule, articular disc, and extra-articular ligaments.
🚨 CRITICAL SURGICAL WARNING: If open reduction is necessary, the surgeon MUST obtain stable fixation without the use of transarticular pins (e.g., Steinmann pins or Kirschner wires). Several fatalities have been reported in the literature resulting from the migration of broken pins directly into the heart, aorta, or great vessels. Suture fixation or specialized plating is the only acceptable method.
Conclusion
Both hip and sternoclavicular dislocations represent severe traumatic insults requiring a deep understanding of regional anatomy, biomechanics, and evidence-based surgical indications. Whether executing a complex East Baltimore lift for a posterior hip or navigating the perilous mediastinal anatomy during a posterior SC joint reduction, the orthopedic surgeon must prioritize concentric reduction, joint stability, and the absolute protection of adjacent neurovascular structures.
You Might Also Like

