Comprehensive Introduction and Patho-Epidemiology
The lesser metatarsals (the second, third, fourth, and fifth rays) serve as the fundamental structural conduits of the human forefoot, playing an indispensable role in the biomechanical transfer of forces during the ambulatory gait cycle. Fractures of these osseous structures represent a substantial proportion of foot and ankle trauma, accounting for approximately 5% to 6% of all skeletal fractures encountered in the acute setting. While isolated, minimally displaced fractures are frequently managed with conservative immobilization, the orthopedic community has increasingly recognized the profound morbidity associated with malunited or nonunited lesser metatarsal fractures. Open Reduction and Internal Fixation (ORIF) with specialized low-profile plating systems has evolved into the gold standard for displaced, unstable, or recalcitrant fractures, aiming to meticulously restore the functional anatomy of the forefoot.
The patho-epidemiology of lesser metatarsal fractures is broadly bifurcated into two distinct clinical entities: acute high-energy traumatic fractures and chronic fatigue (stress) fractures. Acute fractures typically result from direct axial loading, severe crush injuries, or high-velocity mechanisms such as motor vehicle collisions and industrial accidents. These injuries are frequently characterized by multiplanar displacement, comminution, and severe compromise of the delicate dorsal soft tissue envelope. In extreme cases, multiple simultaneous metatarsal fractures produce a "floating forefoot," a highly unstable configuration that catastrophically disrupts the longitudinal and transverse arches of the foot, obligating prompt surgical stabilization to prevent debilitating long-term deformity.
Conversely, stress fractures of the lesser metatarsals—historically documented in military recruits as "march fractures"—arise from repetitive, submaximal cyclical loading that outpaces the intrinsic osteoblastic remodeling capacity of the bone. The second and third metatarsals are disproportionately affected due to their rigid proximal articulations and relative length. Pathophysiologically, this begins as a localized periosteal stress reaction. Continued loading leads to cortical microcracking, which, if uninterrupted by rest or immobilization, propagates into a frank, complete fracture. When these stress fractures fail to achieve osseous union due to continued micro-motion, metabolic deficiencies, or avascularity, they progress to hypertrophic or atrophic nonunions, necessitating meticulous surgical debridement, bone grafting, and rigid plate fixation.
Understanding the demographic distribution of these injuries is critical for the operating surgeon. Acute fractures demonstrate a bimodal distribution, frequently affecting young, active males involved in high-energy trauma, and older, osteopenic females sustaining low-energy fall mechanisms. Stress fractures, however, are predominantly observed in endurance athletes, military personnel, and post-menopausal women with underlying metabolic bone disease. The clinical decision-making process must inherently synthesize the mechanism of injury, patient baseline functional demands, and the local physiological environment to determine the appropriateness of operative intervention via open reduction and plating.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the forefoot is non-negotiable for the orthopedic surgeon undertaking operative fixation of the lesser metatarsals. The osteology of the forefoot is defined by the metatarsal parabola, a critical architectural cascade where the second metatarsal is typically the longest, followed sequentially by the third, first, fourth, and fifth. This parabolic alignment ensures an even distribution of weight-bearing forces across the metatarsal heads during the terminal stance and preswing phases of gait. Any surgical intervention must prioritize the absolute restoration of this length cascade; a residual shortening of even 2 to 3 millimeters can disrupt the parabola, transferring supraphysiologic loads to adjacent, uninjured metatarsal heads—a painful and notoriously difficult-to-treat condition known as transfer metatarsalgia.
Biomechanically, the forefoot is subjected to immense ground reaction forces. While the robust first metatarsal absorbs approximately one-third of the total load, the remaining two-thirds are distributed across the lesser rays. The second metatarsal acts as the central keystone of the foot. Its base is rigidly recessed and locked within the mortise formed by the medial, intermediate, and lateral cuneiforms at the Lisfranc joint complex. This rigid proximal fixation, combined with its extended distal lever arm, subjects the second metatarsal diaphysis to massive bending moments during the toe-off phase of gait. It is this exact biomechanical vulnerability that renders the second metatarsal highly susceptible to fatigue failure and stress fractures.
The vascular anatomy of the lesser metatarsals is intricate and highly relevant to both fracture healing and surgical approach. The arterial supply is derived primarily from the dorsalis pedis artery, which gives rise to the arcuate artery and the dorsal metatarsal arteries. Crucially, the nutrient artery to the lesser metatarsals enters the diaphysis at the lateral aspect of the middle third of the bone, coursing obliquely in a distal-to-proximal direction. High-energy trauma or aggressive surgical periosteal stripping can easily disrupt this tenuous endosteal blood supply, precipitating delayed union or frank nonunion. Surgeons must employ meticulous, minimally invasive soft tissue handling, preserving the periosteal sleeve wherever possible to maintain the extrinsic vascular contributions to the healing callus.
Neurologically, the dorsal aspect of the forefoot is innervated by a superficial network of nerves that are highly vulnerable to iatrogenic injury during surgical exposure. The superficial peroneal nerve bifurcates into the medial and intermediate dorsal cutaneous nerves, which supply sensation to the majority of the dorsal forefoot. The lateral aspect of the fifth ray is supplied by the sural nerve. Most critically, the deep peroneal nerve courses alongside the dorsalis pedis artery within the first intermetatarsal space, lying immediately adjacent to the base of the second metatarsal. Deep dissection or aggressive medial retraction in this zone carries a high risk of neurovascular catastrophe. Precise anatomical knowledge, combined with blunt dissection and the utilization of silastic vessel loops, is mandatory to protect these vital structures during plate application.
Exhaustive Indications and Contraindications
The decision to transition from conservative management to surgical intervention in lesser metatarsal fractures requires a nuanced evaluation of radiographic parameters, patient comorbidities, and functional expectations. The overarching goal of operative treatment is the restoration of the sagittal and coronal alignment, the preservation of the metatarsal parabola, and the establishment of a stable mechanical environment conducive to primary or secondary bone healing. Sagittal plane displacement remains the absolute most critical determinant of long-term functional outcomes.
Operative indications are strictly defined by the degree of displacement and the failure of conservative modalities. Fractures exhibiting greater than 10 degrees of sagittal angulation, or those resulting in dorsal or plantar translation of the metatarsal head, mandate surgical correction. Plantar displacement of the metatarsal head effectively creates a prominent osseous spike on the sole of the foot, leading to intractable plantar keratosis (IPK) and severe, localized metatarsalgia. Conversely, dorsal displacement unloads the affected ray, shifting the burden of weight-bearing to the adjacent metatarsals, thereby inducing transfer lesions. Furthermore, shortening of the diaphysis exceeding 2 to 3 millimeters, intra-articular extension into the metatarsophalangeal (MTP) or tarsometatarsal (TMT) joints, and the presence of a "floating forefoot" (multiple displaced metatarsal fractures) are universally accepted indications for formal open reduction and internal fixation.
Contraindications to operative management must be carefully weighed to prevent catastrophic postoperative complications. The dorsal soft tissue envelope of the foot is notoriously thin, possessing minimal subcutaneous fat to buffer surgical incisions or underlying hardware. Consequently, severe peripheral vascular disease (PVD), marked by an absent dorsalis pedis pulse or an Ankle-Brachial Index (ABI) of less than 0.5, represents an absolute contraindication to elective plating due to the unacceptably high risk of wound necrosis and subsequent deep infection. Active local soft tissue infection, profound uncontrolled diabetes mellitus with severe peripheral neuropathy, and non-ambulatory patient status are also strong contraindications.
In cases where open plating is deemed too hazardous due to soft tissue compromise (e.g., severe acute crush injuries with massive edema or blistering), alternative stabilization methods must be employed. Closed reduction and percutaneous pinning (CRPP) with smooth Kirschner wires, or the application of a bridging external fixator, may serve as a temporizing or definitive damage-control measure. The surgical team must constantly balance the mechanical necessity of rigid internal fixation against the biological tolerance of the host tissue envelope.
| Parameter | Absolute Indications for Plating | Relative Indications for Plating | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Displacement | Sagittal translation > 2mm | Coronal translation > 3-4mm | N/A | Mild coronal shift without shortening |
| Angulation | Sagittal angulation > 10 degrees | Coronal angulation > 10 degrees | N/A | Angulation in a non-ambulatory patient |
| Shortening | Shortening > 2-3 mm | Shortening 1-2 mm in high-demand athlete | N/A | Shortening in a neuropathic foot |
| Fracture Pattern | "Floating forefoot" (multiple rays) | Displaced oblique diaphyseal fractures | Active local osteomyelitis | Severe comminution precluding screw purchase |
| Patient Factors | Recalcitrant symptomatic nonunions | Delayed union at 3-4 months | Severe Peripheral Vascular Disease (ABI < 0.5) | Uncontrolled Diabetes Mellitus (HbA1c > 8.5%) |
| Soft Tissue | Open fractures requiring debridement | Impending skin compromise from bone spike | Active soft tissue infection / cellulitis | Severe acute crush edema / fracture blisters |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful metatarsal osteosynthesis. The initial evaluation mandates a complete radiographic series, strictly obtained in a weight-bearing state whenever the patient's pain tolerance allows. Standard Anteroposterior (AP), Lateral, and Oblique projections are scrutinized to evaluate the fracture morphology, the degree of comminution, and the overall integrity of the metatarsal cascade. The lateral radiograph is particularly critical for assessing sagittal plane angulation, while the oblique view provides unparalleled visualization of the diaphyseal cortices and unmasks subtle multiplanar translations that may be obscured on the AP projection.

Preoperative anteroposterior (AP) radiograph demonstrating a lesser metatarsal fracture requiring operative intervention.

Preoperative oblique radiograph providing a secondary orthogonal view to assess coronal and sagittal plane displacement.
In complex clinical scenarios, such as chronic recalcitrant stress fractures, suspected intra-articular extension, or high-energy trauma with potential occult midfoot instability, advanced cross-sectional imaging is highly recommended. A fine-cut Computed Tomography (CT) scan with 3D reconstructions offers invaluable data regarding the precise geometry of the fracture line, the extent of medullary sclerosis in nonunions, and the volumetric assessment of any cortical defects that will necessitate structural bone grafting. While Magnetic Resonance Imaging (MRI) is the gold standard for diagnosing early stress reactions prior to radiographic visibility, its utility in the preoperative planning of displaced, plate-requiring fractures is limited.
Digital templating is an essential preparatory step, allowing the surgeon to anticipate the required hardware inventory. For the lesser metatarsals, low-profile small fragment systems—typically utilizing 2.0 mm or 2.4 mm titanium or stainless steel plates—are the standard of care. The surgeon must template the plate length to ensure a minimum of four cortices of purchase (two bicortical screws) both proximal and distal to the fracture zone. Furthermore, the necessity for specialized implants, such as T-plates for basilar fractures or locking plates for osteopenic bone, must be determined preoperatively. If a nonunion is being addressed, the surgical team must also prepare for autologous bone graft harvesting, typically from the ipsilateral proximal tibia or calcaneus.
Patient positioning is standardized but requires meticulous attention to detail to facilitate intraoperative imaging and surgical ergonomics. The patient is placed in the supine position on a radiolucent operating table. A small gel bump is placed under the ipsilateral hip to internally rotate the lower extremity, bringing the foot into a neutral, upward-facing position. A well-padded pneumatic tourniquet is applied to the proximal thigh or the calf; a calf tourniquet is often preferred by foot and ankle specialists as it provides excellent hemostasis while minimizing the risk of thigh-level deep vein thrombosis. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, entering perpendicular to the operative field, ensuring unobstructed, real-time orthogonal imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
1. Surgical Exposure and Neurovascular Protection
Following the administration of a regional popliteal sciatic nerve block and the inflation of the tourniquet, a longitudinal dorsal incision is centered directly over the fractured metatarsal. The incision length typically ranges from 3 to 5 centimeters, dictated by the fracture pattern and the templated plate length. The dissection proceeds carefully through the thin subcutaneous layer. The immediate priority is the identification and mobilization of the superficial sensory nerves. Depending on the ray involved, branches of the medial dorsal cutaneous, intermediate dorsal cutaneous, or sural nerves will be encountered. These structures must be gently freed from the surrounding adventitia and retracted using silastic vessel loops to prevent traction neuropraxia or inadvertent transection, which can result in painful postoperative neuromas.

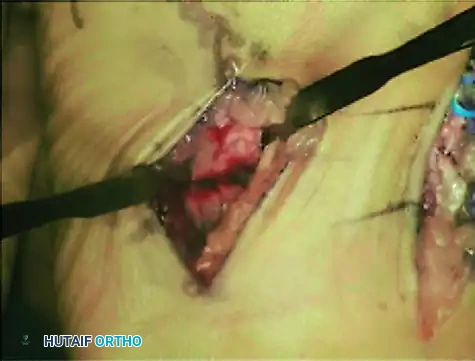
Intraoperative photograph demonstrating curettage and preparation of the second metatarsal. Note the blue vessel loop carefully retracting the dorsalis pedis artery and deep peroneal nerve away from the surgical field.
Deep to the subcutaneous tissue, the extensor retinaculum is incised longitudinally. The tendons of the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) are identified and retracted either medially or laterally, depending on the specific fracture geometry and the planned plate location. The underlying periosteum is then incised sharply along the midline of the diaphysis. Using a Freer elevator, the periosteum is elevated just enough to expose the fracture site and accommodate the footprint of the plate. Aggressive circumferential stripping of the periosteum is strictly avoided, as it devitalizes the cortical bone and significantly increases the risk of atrophic nonunion.
2. Fracture Site Preparation and Grafting
In the setting of an acute fracture, the fracture hematoma is evacuated, and the bone ends are gently irrigated. However, in the surgical management of a chronic stress fracture or an established nonunion, the fracture gap will invariably be occupied by dense, avascular fibrous tissue and sclerotic bone. This interposed material must be meticulously excised using a small curette or a rongeur until healthy, punctate bleeding bone (the "paprika sign") is visualized on both the proximal and distal fragments. To further stimulate osteogenesis and open the medullary canal, multiple drill holes (osteostixis) are created in the sclerotic bone ends using a 1.5 mm or 2.0 mm drill bit. If a structural defect remains after aggressive debridement, the void must be densely packed with osteoconductive and osteoinductive autologous cancellous bone graft prior to plate application.
3. Anatomical Reduction
Achieving absolute anatomical reduction is the most technically demanding phase of the procedure. The surgeon must simultaneously restore length, correct rotational malalignment, and perfectly re-establish the sagittal plane. Reduction is typically facilitated using small pointed reduction forceps, dental picks, or a miniature lamina spreader placed within the fracture gap. Once the gross alignment is corrected, the reduction is provisionally stabilized utilizing 1.1 mm or 1.6 mm smooth Kirschner wires driven obliquely across the fracture site. The accuracy of the reduction is immediately verified via multiplanar intraoperative fluoroscopy, paying specific attention to the alignment of the metatarsal head relative to the adjacent rays to ensure the parabola is restored.
4. Plate Contouring and Application
Selection of the appropriate low-profile implant is critical. While the dorsal surfaces of the second and third metatarsals are relatively linear and often accept a straight 2.0 mm or 2.4 mm plate without modification, the lateral rays present a distinct anatomical challenge. The fourth and fifth metatarsals possess a natural lateral and plantar bow. Consequently, plates applied to these bones must be precisely contoured using plate benders to match the native osseous curvature. Failure to contour the plate will result in iatrogenic displacement of the fracture when the screws are tightened, pulling the bone to the straight plate and inducing a malunion.

Exposure and plating of the fourth metatarsal. Notice the slight contouring of the plate required to accommodate the anatomical curvature of the lateral forefoot.
The plate is applied to the dorsal, tension-band surface of the metatarsal. In simple, transverse, or short oblique fracture patterns, the principles of absolute stability are employed. If the fracture geometry permits, an interfragmentary lag screw is placed independently or through the plate to generate dynamic compression across the fracture interface. The plate is then secured using standard non-locking cortical screws, ensuring a minimum of two bicortical screws (four cortices) on each side of the fracture. In osteopenic bone, or in highly comminuted fractures acting as a bridge plate, locking screws may be utilized to construct a fixed-angle device, providing superior pull-out strength.
Intraoperative view of the second metatarsal following the application of a low-profile dorsal plate. Note the flush seating of the plate against the diaphyseal bone.
5. Final Verification and Closure
Following definitive fixation, a final fluoroscopic sweep is performed to confirm hardware placement, ensuring no screws are penetrating the MTP or TMT joints, and verifying the absolute restoration of the metatarsal cascade. The wound is copiously irrigated with sterile saline. Closure is performed in a layered fashion. Whenever possible, the periosteum is re-approximated over the dorsal plate using fine 4-0 absorbable sutures. This vital step provides a smooth soft-tissue gliding layer, preventing the extensor tendons from adhering to or attritionally rupturing against the metallic hardware. The subcutaneous tissues are closed, followed by the skin utilizing 4-0 or 5-0 non-absorbable nylon sutures in a horizontal mattress or simple interrupted configuration to optimize wound edge eversion and vascularity.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, open reduction and plating of lesser metatarsal fractures carries a distinct risk profile. The unique anatomical constraints of the forefoot—specifically the paucity of soft tissue coverage and the high biomechanical demands placed upon the implants—predispose patients to several well-documented complications. The surgeon must be adept at not only preventing these adverse events but also executing complex salvage procedures when they arise.
The most ubiquitous complication, occurring in up to 15% to 20% of cases, is symptomatic hardware prominence. The low-profile plates, while mechanically robust, sit directly beneath the thin dorsal skin, frequently leading to irritation, bursitis, and pain with enclosed shoe wear. The primary prevention strategy involves utilizing the thinnest possible implant that provides adequate stability and ensuring meticulous periosteal closure over the plate. When symptomatic prominence occurs, the surgeon must exercise patience; hardware removal is strictly contraindicated until complete cortical remodeling is achieved, typically 9 to 12 months postoperatively. Premature removal of the plate drastically increases the risk of a catastrophic refracture through the screw holes.
Nonunion and delayed union represent a more severe complication, with an incidence ranging from 2% to 5% in acute fractures, but significantly higher in the surgical treatment of chronic stress fractures. Biological failures are often driven by patient-specific factors, most notably tobacco use, uncontrolled diabetes, and Vitamin D deficiency. Mechanical failures arise from inadequate fixation rigidity, excessive periosteal stripping, or failure to address underlying biomechanical deformities (e.g., a rigid cavovarus foot overloading the lateral rays). Salvage management of an established nonunion requires a revision operation involving complete hardware removal, aggressive debridement of the fibrous cleft, application of a larger structural autograft (e.g., iliac crest), and revision fixation with a more robust, potentially locking, plate construct.
Malunion, specifically involving sagittal plane displacement, is a devastating complication that directly alters the weight-bearing mechanics of the foot. A metatarsal head that heals in a plantarflexed position will inevitably produce an intractable plantar keratosis (IPK) and severe localized pain. Conversely, a dorsiflexed malunion unloads the affected ray, precipitating transfer metatarsalgia to the adjacent, uninjured metatarsals. If conservative management with custom orthotics and offloading pads fails, salvage requires formal corrective osteotomies. A dorsal closing wedge osteotomy or a distal Weil osteotomy is frequently utilized to elevate a plantarflexed metatarsal head or restore length and alignment to a shortened, dorsiflexed ray.
Infection and wound dehiscence are less common (1% to 3%) but potentially limb-threatening complications, particularly in patients with vascular compromise or in the setting of high-energy open trauma. Superficial wound edge necrosis can often be managed with local wound care and oral antibiotics. However, deep infections involving the hardware require immediate return to the operating room for aggressive irrigation and debridement, hardware removal if the fracture is sufficiently healed (or replacement with an external fixator if unstable), and targeted intravenous antibiotic therapy guided by intraoperative cultures.
| Complication | Estimated Incidence | Primary Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Symptomatic Hardware | 15% - 20% | Use low-profile plates; meticulous periosteal closure. | Hardware removal (strictly > 12 months post-op); orthotic shoe modification. |
| Nonunion / Delayed Union | 2% - 5% (Higher in stress fx) | Preserve periosteal blood supply; rigid fixation; smoking cessation. | Revision ORIF with structural autograft (iliac crest/calcaneus) and locking plate. |
| Transfer Metatarsalgia | 5% - 10% | Absolute restoration of sagittal alignment and metatarsal parabola. | Custom orthotics; Salvage via Weil osteotomy or corrective diaphyseal osteotomy. |
| Wound Dehiscence / Infection | 1% - 3% | Respect soft tissue envelope; delay surgery until acute edema subsides. | Superficial: Oral Abx. Deep: Immediate I&D, hardware removal/exchange, IV Abx. |
| Iatrogenic Nerve Injury | < 2% | Blunt dissection; utilize silastic vessel loops for nerve retraction. | Gabapentinoids for neuropraxia; surgical excision and burying of stump for frank neuroma. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following open reduction and plating of lesser metatarsal fractures is a highly structured, multiphasic process designed to balance the mechanical protection of the healing osteosynthesis with the prevention of soft tissue contractures and joint stiffness. The protocol is heavily influenced by the surgeon's intraoperative assessment of bone quality, the rigidity of the fixation construct, and the patient's baseline physiological healing capacity.
Phase I: Maximum Protection (Weeks 0 to 2)
The immediate postoperative period prioritizes wound healing and edema control. Upon completion of the surgery, the patient is placed in a bulky, sterile compressive dressing reinforced with a rigid posterior splint or a short-leg cast, maintaining the ankle in a neutral position to prevent Achilles tendon contracture. The patient is instructed to maintain strict non-weight-bearing (NWB) status using crutches or a knee scooter. Absolute, continuous elevation of the operative limb above the level of the heart is mandatory for the first 48 to 72 hours to mitigate forefoot edema, which is the primary antagonist to successful surgical wound healing. At the 10 to 14-day mark, the patient returns to the clinic for splint removal, radiographic evaluation, and suture removal, provided the incision demonstrates complete epithelialization without signs of dehiscence.

Postoperative anteroposterior radiograph demonstrating anatomic alignment and rigid internal fixation of the lesser metatarsals with low-profile plates and screws.
Phase II: Controlled Mobilization (Weeks 2 to 6)
Following successful wound healing, the patient is transitioned into a removable Controlled Ankle Motion (CAM) boot. The advancement of weight-bearing status during this phase is highly individualized. For young, healthy patients with acute fractures treated with rigid compression plating, progressive heel-touch to partial weight-bearing may be initiated. However, in the setting of chronic stress fractures, atrophic nonunions requiring bone graft, or highly comminuted injuries, strict NWB in the CAM boot is typically extended for a full 4 to 6 weeks to prevent hardware failure. During this phase, patients are instructed to remove the boot multiple times daily to perform active and passive range of motion (ROM) exercises of the ankle, subtalar, and particularly the metatarsophalangeal (MTP) joints, preventing the debilitating toe stiffness that frequently plagues forefoot trauma.

Postoperative lateral radiograph confirming the restoration of the sagittal plane. The metatarsal heads are perfectly aligned, preventing postoperative transfer metatarsalgia.
Phase III: Progressive Loading and Strengthening (Weeks 6 to 12)
At the 6-week postoperative milestone, repeat weight-bearing radiographs are obtained to assess for the presence of bridging fracture callus and the obliteration of the fracture lines. Upon radiographic confirmation of early clinical union, the patient is gradually weaned from the CAM boot into a stiff-soled, wide-toe-box shoe or a postoperative surgical shoe. Formal physical therapy is initiated, focusing on aggressive MTP joint mobilization, intrinsic foot muscle strengthening, and proprioceptive gait retraining. Custom orthotics featuring a metatarsal pad or a Morton's extension may be prescribed to mechanically offload the healing ray and support the transverse arch during the transition to full, unprotected weight-bearing.
Adjunctive Therapies and Return to Activity
For patients identified as high-risk for delayed healing—including chronic smokers, diabetics, or those treated for long-standing nonunions—the adjunctive use of bone stimulation technology is highly recommended. Pulsing Electromagnetic Field (PEMF) or Low-Intensity Pulsed Ultrasound (LIPUS) devices are typically initiated at the 2-week mark and utilized daily to upregulate osteogenic activity. Return to high-impact sports or heavy labor is strictly prohibited until complete radiographic consolidation is evident, typically occurring between 12 and 16 weeks postoperatively, and the patient demonstrates a pain-free, symmetrical gait pattern.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of lesser metatarsal fractures has been heavily influenced by a paradigm shift in the orthopedic literature over the past three decades. Historically, the default management for nearly all central metatarsal fractures was non-operative, utilizing casting or stiff-soled shoes, under the assumption that the robust soft tissue envelope and the splinting effect of adjacent intact rays would ensure adequate functional outcomes. However, landmark retrospective reviews in the late 1980s and 19
