Open Reduction and Internal Fixation of Tarsometatarsal (Lisfranc) Fractures
Key Takeaway
Open reduction and internal fixation (ORIF) is the gold standard for displaced tarsometatarsal (Lisfranc) joint injuries. This procedure restores the critical biomechanical arch of the midfoot, utilizing dorsal incisions to access the medial and middle columns. Rigid internal fixation with cortical screws or dorsal spanning plates ensures anatomic alignment, preventing post-traumatic osteoarthritis and chronic midfoot instability in the active patient population.
INTRODUCTION AND BIOMECHANICS OF THE LISFRANC JOINT
The tarsometatarsal (TMT) joint complex, commonly referred to as the Lisfranc joint, represents the critical biomechanical transition zone between the midfoot and the forefoot. Injuries to this complex range from subtle ligamentous sprains to highly comminuted fracture-dislocations. Because the midfoot dictates the stability of the longitudinal and transverse arches during the terminal stance phase of gait, missed or inadequately treated Lisfranc injuries inevitably lead to severe post-traumatic osteoarthritis, planovalgus deformity, and chronic, debilitating pain.
Osteology and the "Keystone" Concept
The inherent stability of the Lisfranc joint is derived from its unique osseous architecture. The bases of the five metatarsals articulate with the three cuneiforms and the cuboid, forming a transverse Roman arch. The base of the second metatarsal is recessed proximally between the medial and lateral cuneiforms, locking into the intermediate cuneiform. This recessed articulation acts as the "keystone" of the arch, providing immense static osseous stability. Disruption of this keystone is the hallmark of a severe Lisfranc injury.
Ligamentous Anatomy
While the osseous anatomy provides static stability, the ligamentous network provides dynamic restraint. The plantar ligaments are significantly thicker and stronger than their dorsal counterparts, explaining why dorsal dislocations are far more common.
Crucially, there is no transverse intermetatarsal ligament connecting the bases of the first and second metatarsals. Instead, stability between the medial and middle columns relies entirely on the Lisfranc ligament—a robust, oblique ligamentous band originating from the lateral aspect of the medial cuneiform and inserting onto the medial base of the second metatarsal.
Clinical Pearl: The Lisfranc ligament is the strongest ligament in the TMT complex. In high-energy trauma, the ligament may avulse a small fragment of bone from the base of the second metatarsal, visible on an anteroposterior (AP) radiograph as the pathognomonic "fleck sign."
CLINICAL EVALUATION AND PREOPERATIVE IMAGING
Clinical Presentation
Patients typically present following an axial load applied to a plantarflexed foot (e.g., a missed step, athletic trauma, or motor vehicle collision). Clinical examination reveals profound midfoot swelling, inability to bear weight, and pain elicited by pronation and abduction of the forefoot.
Surgical Warning: Plantar ecchymosis in the setting of midfoot trauma is considered pathognomonic for a Lisfranc injury until proven otherwise. Furthermore, surgeons must maintain a high index of suspicion for acute compartment syndrome of the foot, particularly in high-energy crush injuries.
Radiographic Evaluation
Standard weight-bearing radiographs (AP, lateral, and 30-degree internal oblique) are mandatory.
* AP View: The medial border of the second metatarsal must align perfectly with the medial border of the intermediate cuneiform.
* Oblique View: The medial border of the fourth metatarsal must align with the medial border of the cuboid.
* Lateral View: The dorsal cortices of the metatarsals should be flush with the dorsal cortices of the cuneiforms. Any dorsal step-off indicates instability.

FIGURE 1: Preoperative anteroposterior and oblique radiographs demonstrating a fracture of the medial cuneiform and disruption of the tarsometatarsal articulation (arrows).
Advanced Imaging (CT Scan)
Computed tomography (CT) is highly recommended for all suspected Lisfranc injuries. CT scans delineate the exact fracture pattern, identify intra-articular comminution, and reveal subtle non-displaced fractures that are frequently missed on plain radiographs.

FIGURE 2: Preoperative axial CT scan confirming the comminution and displacement of the medial cuneiform fracture (asterisk), providing critical detail for preoperative planning.
INDICATIONS FOR SURGERY
Non-operative management is strictly reserved for truly non-displaced injuries (less than 2 mm of diastasis on weight-bearing radiographs) with no evidence of dynamic instability.
Indications for Open Reduction and Internal Fixation (ORIF):
* Displacement of any TMT joint > 2 mm.
* Loss of the longitudinal or transverse arch.
* Bony comminution involving the keystone (2nd TMT joint).
* Open fractures or impending compartment syndrome.
Note: Purely ligamentous injuries in older or highly active patients may be considered for primary arthrodesis rather than ORIF, given the high rate of hardware failure and subsequent arthritis associated with ligamentous healing.
SURGICAL TECHNIQUE: STEP-BY-STEP
Patient Positioning and Anesthesia
With the patient under a regional or general anesthetic, place them in the supine position on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral position. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
The Surgical Approach
Optimal visualization of the TMT complex requires a dual-incision technique to access the medial, middle, and lateral columns without creating excessively wide skin flaps that could compromise wound healing.
1. The Dorsomedial Incision (First and Second TMT Joints)
Make a longitudinal dorsal incision lateral to the extensor hallucis longus (EHL) tendon, directly over the interval between the base of the first and second metatarsals. The incision can be placed slightly more lateral if access to the intermediate cuneiform is required.
Carefully dissect through the subcutaneous tissues. The extensor hallucis brevis (EHB) muscle belly will be encountered; retract it laterally.
Surgical Pitfall: The neurovascular bundle, consisting of the dorsalis pedis artery and the deep peroneal nerve, runs directly through the first intermetatarsal space. This bundle must be meticulously identified, mobilized, and protected. Retract the bundle laterally with the EHB to safely expose the first and second TMT joints.
2. The Dorsolateral Incision (Third and Fourth TMT Joints)
If the lateral column requires reduction, make a second longitudinal incision centered over the third and fourth TMT joints, lateral to the extensor digitorum longus (EDL) tendons. Maintain a minimum skin bridge of 5 to 7 cm between the two incisions to prevent skin necrosis. Identify and protect the terminal branches of the superficial peroneal nerve during this approach.
Joint Preparation and Debridement
Once the joints are exposed, use a Freer elevator and rongeurs to clear the articulations of hematoma, capsular debris, and small osteochondral fragments. Incarcerated soft tissue—most commonly the anterior tibial tendon or fragments of the Lisfranc ligament—frequently blocks anatomic reduction and must be cleared.
Use a 2.0 mm drill bit or a curette to fenestrate the subchondral bone if primary arthrodesis is planned, though for standard ORIF, the articular cartilage should be preserved as much as possible.
Sequence of Reduction
Reduction must proceed in a strict, systematic anatomical order, moving from medial to lateral.
- The Medial Column (1st TMT): Reduce the first metatarsal onto the medial cuneiform. Ensure the plantar and medial cortices are perfectly flush. Temporarily secure the reduction with a 1.6 mm Kirschner wire (K-wire) driven from the dorsal-distal first metatarsal into the plantar-proximal medial cuneiform.
- The Middle Column (2nd TMT): Reduce the second metatarsal base into its keystone position between the medial and lateral cuneiforms. Clamp the medial cuneiform to the second metatarsal base using a large pointed reduction forceps.
- The Lateral Column (3rd, 4th, 5th TMT): Once the medial and middle columns are anatomically restored, the lateral column often reduces spontaneously. If not, reduce and pin the third metatarsal to the lateral cuneiform. The 4th and 5th TMT joints are highly mobile and are typically stabilized with temporary K-wires rather than rigid screws.
Internal Fixation Strategy
The "Home Run" Screw
The most critical piece of fixation is the Lisfranc screw, which recreates the trajectory of the native Lisfranc ligament. Drill a glide hole in the medial cuneiform and a thread hole in the base of the second metatarsal. Insert a 3.5 mm or 4.0 mm solid cortical screw from the medial aspect of the medial cuneiform, aiming distally and laterally into the base of the second metatarsal.
Clinical Pearl: Solid cortical screws provide superior bending strength compared to cannulated screws. Given the immense shear forces across the midfoot during weight-bearing, solid screws are highly recommended to prevent hardware breakage.
Column Fixation
* First TMT Joint: Fixate with one or two 3.5 mm cortical screws placed in a lag fashion from the dorsal first metatarsal into the medial cuneiform.
* Second and Third TMT Joints: Place individual transarticular screws from the metatarsal bases into their respective cuneiforms.
* Alternative - Dorsal Bridge Plating: To avoid iatrogenic damage to the articular cartilage caused by transarticular screws, dorsal spanning plates are increasingly favored. These plates bridge the joint, providing rigid stability while preserving the articular surface, which may reduce the incidence of post-traumatic arthritis.

FIGURE 3: Postoperative anteroposterior radiograph demonstrating anatomic reduction and internal fixation utilizing solid cortical screws across the medial and middle columns.

FIGURE 4: Postoperative lateral radiograph confirming the restoration of the longitudinal arch and appropriate intraosseous hardware placement without dorsal step-off.
Intraoperative Imaging and Closure
Before closure, obtain final AP, lateral, and oblique fluoroscopic images to confirm anatomic reduction of all joints and verify that no screws are penetrating the adjacent articulations or plantar cortices.
Deflate the tourniquet and achieve meticulous hemostasis. Close the extensor retinaculum with absorbable sutures to prevent tendon bowstringing. Close the subcutaneous tissue and skin in layers. Apply a sterile, non-adherent dressing followed by a well-padded short-leg posterior splint with the ankle in neutral dorsiflexion.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of Lisfranc ORIF requires strict adherence to a phased rehabilitation protocol to ensure ligamentous healing and prevent hardware failure.
Phase 1: Maximum Protection (Weeks 0-6)
- The patient is strictly non-weight-bearing (NWB).
- At 2 weeks, sutures are removed, and the patient is transitioned to a rigid short-leg cast or a locked controlled ankle motion (CAM) boot.
- Elevation and edema control are paramount.
Phase 2: Progressive Loading (Weeks 6-12)
- At 6 weeks, repeat weight-bearing radiographs are obtained out of the boot.
- If radiographic alignment is maintained, the patient begins progressive partial weight-bearing in the CAM boot, advancing to full weight-bearing as tolerated by week 10.
- Physical therapy is initiated, focusing on active ankle and midfoot range of motion, intrinsic foot muscle strengthening, and proprioceptive training.
Phase 3: Hardware Removal and Return to Activity (Months 4-6)
- Transarticular screws crossing the TMT joints restrict normal midfoot motion and are highly prone to fatigue failure (breakage) once the patient resumes normal ambulation.
- Routine hardware removal is generally recommended at 4 to 6 months postoperatively, prior to allowing the patient to return to high-impact activities or sports.
- If dorsal bridge plates were utilized, removal is optional and based on symptomatic hardware irritation.
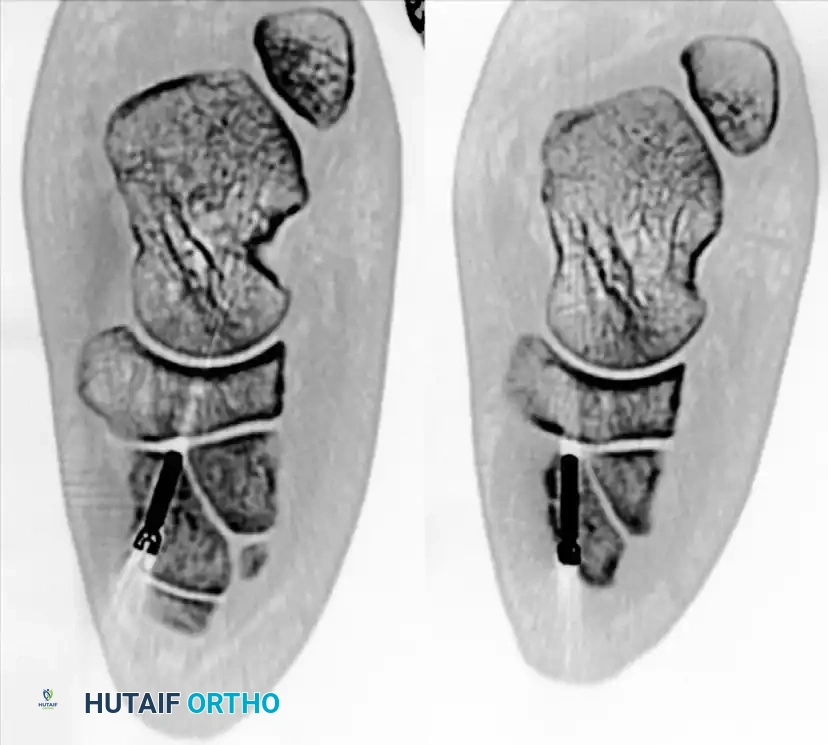
FIGURE 5: Postoperative axial CT scan verifying the precise intraosseous trajectory of the fixation screws and the anatomic restoration of the medial cuneiform and TMT articulations.
COMPLICATIONS AND PITFALLS
Despite anatomic reduction and rigid fixation, Lisfranc injuries carry a high morbidity rate. Surgeons must counsel patients extensively regarding potential long-term outcomes.
- Post-Traumatic Osteoarthritis: This is the most common complication, occurring in up to 50% of patients, particularly those with intra-articular comminution or purely ligamentous injuries. If conservative management (orthotics, NSAIDs, injections) fails, midfoot arthrodesis is the definitive salvage procedure.
- Hardware Failure: Screw breakage is common if patients bear weight prematurely or if transarticular screws are left in place during high-impact activities. Broken screws retained within the bone can complicate future arthrodesis procedures.
- Nerve Injury: Iatrogenic injury to the deep peroneal nerve or superficial peroneal nerve during the surgical approach can lead to painful neuromas or complex regional pain syndrome (CRPS). Meticulous soft-tissue handling is essential.
- Loss of Reduction: Failure to recognize and fixate subtle instability in the middle or lateral columns can lead to progressive arch collapse and a severe planovalgus deformity.
CONCLUSION
Open reduction and internal fixation of Lisfranc injuries is a demanding procedure that requires a profound understanding of midfoot biomechanics and meticulous surgical technique. By utilizing strategic dorsal approaches, protecting the neurovascular structures, and adhering to a strict sequence of reduction—anchored by the restoration of the second metatarsal keystone—surgeons can reliably restore the functional anatomy of the foot. While post-traumatic arthritis remains a persistent risk, anatomic ORIF provides the highest probability of returning the patient to a pain-free, active lifestyle.
You Might Also Like
