Comprehensive Introduction and Patho-Epidemiology
The Bennett fracture represents a classic, highly unstable intra-articular fracture-subluxation involving the base of the first metacarpal. Originally described by the eminent Irish surgeon Edward Hallaran Bennett in 1882, this specific injury pattern is defined by the avulsion of the volar ulnar aspect of the metacarpal base. The defining characteristic of this fracture is not merely the bony disruption, but the profound biomechanical destabilization of the first carpometacarpal (CMC) joint. Because the thumb CMC joint is a highly mobile, biconcave saddle joint critical for opposition, prehension, and overall hand function, any disruption to its articular congruity or ligamentous stability can result in severe, debilitating functional deficits.
Epidemiologically, Bennett fractures are the most common fractures involving the base of the thumb. They predominantly occur in young, active male populations, frequently resulting from high-energy axial loading applied to a partially flexed thumb metacarpal. Common mechanisms of injury include striking a solid object with a closed fist (often seen in pugilistic endeavors), falls onto an outstretched hand with the thumb tucked, and high-velocity sporting collisions. The axial force drives the metacarpal base into the trapezium, shearing off the volar ulnar fragment while the remainder of the metacarpal shaft subluxates dorsally, proximally, and radially under the influence of powerful extrinsic and intrinsic muscle forces.
Understanding the pathophysiology of the Bennett fracture requires an appreciation of the unique forces acting upon the thumb ray. The injury is inherently unstable because the fracture line separates the major ligamentous stabilizing structure from the majority of the bony metacarpal. The small volar ulnar fragment remains anatomically secured to the trapezium by the robust anterior oblique ligament (AOL), maintaining its position within the CMC joint. Conversely, the larger metacarpal shaft fragment is subjected to powerful, uninhibited muscular forces that drive the characteristic displacement pattern.
Because of these persistent, unopposed deforming forces, closed reduction and cast immobilization are frequently insufficient to maintain articular congruity over the course of fracture healing. Even when initial closed reduction appears satisfactory, the continuous muscular pull often leads to insidious displacement within the cast. When conservative measures fail, or when the initial articular step-off exceeds acceptable biomechanical parameters (typically greater than 1 to 2 mm), open reduction and internal fixation (ORIF) becomes the absolute gold standard of treatment. The primary objective is to prevent early-onset post-traumatic osteoarthritis, which develops rapidly in the presence of articular incongruity due to the massive contact stresses concentrated at the thumb CMC joint during normal pinch and grasp activities.
Detailed Surgical Anatomy and Biomechanics
Thorough knowledge of the dorsoradial anatomy of the thumb and the intricate biomechanics of the first CMC joint is essential to safely execute the surgical approach and achieve a stable reduction. The first CMC joint is a highly specialized trapeziometacarpal articulation, functioning as a biconcave saddle joint. This unique geometry allows for a wide range of motion in multiple planes—flexion, extension, abduction, adduction, and the complex rotational movement of opposition. The stability of this joint is heavily reliant on a complex network of capsuloligamentous structures, the most critical of which is the anterior oblique ligament (AOL), often referred to as the "beak ligament."
The volar ulnar fragment of the Bennett fracture serves as the attachment site for the AOL. During the injury, the AOL remains intact, tethering this small articular fragment firmly to the trapezium. Meanwhile, the larger metacarpal shaft fragment is entirely devoid of this critical volar stabilization. The abductor pollicis longus (APL), which inserts onto the dorsal-radial base of the first metacarpal, exerts a massive proximal, dorsal, and radial pull on the metacarpal shaft. Concurrently, the adductor pollicis, inserting on the ulnar sesamoid and the base of the proximal phalanx, pulls the metacarpal head toward the palm. This combined muscular action results in a profound supination and adduction deformity of the thumb ray, causing the metacarpal base to subluxate dorsoradially out of the saddle joint.
The surgical anatomy overlying the first CMC joint presents several critical neurovascular hazards that must be meticulously navigated. The superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve (LABC) arborize extensively over the dorsoradial aspect of the thumb and wrist. These sensory branches are highly susceptible to traction injury or direct laceration during the surgical approach. Iatrogenic injury to these nerves can result in debilitating, painful neuromas that often overshadow the outcome of a perfectly executed fracture fixation. The surgeon must employ careful blunt dissection in the subcutaneous tissues and utilize vessel loops for gentle, atraumatic retraction of these nerve branches.
Furthermore, the first dorsal compartment of the wrist, housing the APL and extensor pollicis brevis (EPB) tendons, lies directly over the surgical field. The radial artery, a major vascular structure, courses dorsally through the anatomic snuffbox, crossing the scaphoid and trapezium just proximal to the CMC joint before diving between the two heads of the first dorsal interosseous muscle. Preoperative planning and intraoperative dissection must respect these structures. The vascular supply to the critical volar ulnar fragment is tenuous, derived almost entirely from the capsular attachments and the AOL. Overzealous soft tissue stripping during open reduction can inadvertently devascularize this fragment, leading to avascular necrosis, nonunion, and catastrophic joint failure.
Exhaustive Indications and Contraindications
The primary goal in the management of a Bennett fracture is the meticulous restoration of a congruent CMC joint and the rigid stabilization of the first metacarpal shaft to allow for early, aggressive rehabilitation. While some minimally displaced fractures can be managed with closed reduction and percutaneous pinning (CRPP), open reduction is strictly indicated when anatomic reduction cannot be achieved or maintained by closed means. The threshold for surgical intervention is low, given the severe functional consequences of a malunited thumb CMC joint.
Open reduction is definitively indicated in cases where closed reduction fails to achieve an articular step-off of less than 1 to 2 mm. Biomechanical studies have unequivocally demonstrated that even a 1 mm articular incongruity drastically alters contact stresses across the trapeziometacarpal joint, predisposing the patient to rapid and severe post-traumatic arthritis. Furthermore, when the volar ulnar fragment constitutes more than 20% to 25% of the articular surface, percutaneous capture becomes technically arduous and mechanically unstable, necessitating direct visualization and internal fixation. Additional indications include an articular gap greater than 2 mm, delayed presentations where early callus formation prevents closed manipulation, and polytrauma or open fractures requiring immediate rigid stabilization to facilitate comprehensive hand rehabilitation or complex soft tissue management.
Contraindications to open reduction and internal fixation must be carefully weighed against the risks of non-operative management. Absolute contraindications include active, severe local soft tissue infections or osteomyelitis, which must be eradicated prior to the introduction of internal hardware. Patients who are medically unfit for surgery due to severe systemic comorbidities or those who are unable to comply with strict postoperative rehabilitation protocols may also be poor candidates for ORIF. In such cases, the surgeon may have to accept a suboptimal radiographic outcome in favor of patient safety.
Relative contraindications involve the timing of the presentation. Attempting a primary open reduction and internal fixation on a Bennett fracture that is older than 4 to 6 weeks is fraught with complications. By this time, significant bony remodeling, severe soft tissue contracture, and early degenerative changes have already occurred. Forcible reduction attempts in these delayed scenarios will likely result in iatrogenic cartilage damage, crushing of the osteopenic fragment, and profound joint stiffness. In these late-presenting cases, the surgeon should either allow the fracture to consolidate and plan for a subsequent corrective osteotomy, or proceed directly to a salvage procedure if advanced arthrosis is already present.
| Indication / Contraindication Category | Specific Clinical Scenarios | Rationale / Biomechanical Implication |
|---|---|---|
| Absolute Indications | Failure of closed reduction (>1-2mm step-off) | Prevents exponential increase in joint contact stresses and subsequent osteoarthritis. |
| Absolute Indications | Large volar ulnar fragment (>25% articular surface) | Too large for stable percutaneous pinning; requires rigid interfragmentary compression. |
| Absolute Indications | Open fractures or severe polytrauma | Requires immediate rigid stabilization for soft tissue care and early mobilization. |
| Relative Indications | Delayed presentation (2-4 weeks) | Early callus prevents closed manipulation; requires open debridement of fracture hematoma. |
| Absolute Contraindications | Active local infection / untreated osteomyelitis | High risk of deep hardware infection and catastrophic joint destruction. |
| Absolute Contraindications | Medically unstable patient | Anesthetic and surgical risks outweigh the orthopaedic benefits of joint restoration. |
| Relative Contraindications | Late presentation (>6 weeks) without osteotomy plan | High risk of iatrogenic cartilage damage due to forced reduction of remodeled bone. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful Bennett fracture ORIF. The planning phase begins with obtaining high-quality, specialized radiographic imaging. Standard anteroposterior (AP) and lateral radiographs of the hand are grossly insufficient for evaluating the thumb CMC joint, as the thumb ray lies in a plane approximately 30 to 40 degrees pronated relative to the rest of the hand. Therefore, standard hand views will project the CMC joint obliquely, obscuring the true extent of the articular step-off and the exact size of the volar ulnar fragment.
To accurately assess the injury, a true AP of the thumb (often referred to as a Robert's view) and a true lateral of the first CMC joint are absolutely mandatory. The Robert's view is obtained by maximally pronating the patient's forearm so that the dorsum of the thumb rests flat against the radiographic cassette. In cases of severe comminution or when the size of the volar ulnar fragment is difficult to ascertain on plain films, a dedicated computed tomography (CT) scan with fine (1 mm or less) sagittal and coronal reconstructions is highly recommended. The CT scan allows the surgeon to accurately template the fracture, determining whether the fragment is of sufficient size to accommodate a lag screw or if multiple Kirschner wires (K-wires) will be required.
Once the imaging is analyzed, templating dictates the choice of implants. If the volar ulnar fragment is large enough—specifically, if its width is at least three times the diameter of the intended screw (e.g., a 6 mm fragment for a 2.0 mm screw)—lag screw fixation is the preferred method, as it provides superior interfragmentary compression and allows for earlier mobilization. If the fragment is smaller, highly comminuted, or osteopenic, the surgeon must plan for fixation using multiple small-caliber K-wires (0.035-inch or 0.045-inch) to neutralize the deforming forces without shattering the fragment.
Patient positioning and operating room setup must be optimized for unimpeded fluoroscopic access and surgical ergonomics. The patient is placed in the supine position with the affected upper extremity extended on a radiolucent hand table. Regional anesthesia, such as a supraclavicular or axillary brachial plexus block, is highly preferred. It provides excellent intraoperative muscle relaxation, which is crucial for overcoming the powerful deforming forces of the APL and adductor pollicis, and offers superior postoperative pain control. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage to ensure a pristine, bloodless surgical field. A mini-C-arm fluoroscopy unit must be positioned parallel to the hand table, allowing the surgeon to obtain true orthogonal views of the thumb CMC joint effortlessly throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The Wagner approach is the standard, time-tested surgical exposure for the base of the first metacarpal. It provides excellent, direct visualization of the first CMC joint and the fracture site, facilitating precise anatomic reduction while minimizing the risk to surrounding neurovascular structures. The incision begins as a gentle curve on the dorsoradial aspect of the first metacarpal shaft, extending proximally and curving volarward at the level of the wrist crease, following the glabrous border of the skin.
Superficial dissection must be performed with the utmost care. The surgeon should bluntly dissect through the subcutaneous tissues using tenotomy scissors or a hemostat. It is imperative to identify, mobilize, and meticulously protect the sensory branches of the superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve (LABC) that cross this area. These branches should be gently retracted using vessel loops. Once the nerves are secured, the deep dissection involves identifying the interval between the first dorsal compartment (APL and EPB tendons) and the thenar musculature. The thenar muscles (opponens pollicis and abductor pollicis brevis) are elevated subperiosteally from the metacarpal shaft and retracted volarward to expose the fracture site. A longitudinal or T-shaped capsulotomy of the CMC joint is then performed to expose the articular surface and the fracture hematoma.
Reduction of the Bennett fracture requires a deliberate sequence of maneuvers designed to reverse the specific deforming forces. First, the joint space is irrigated, and any interposed soft tissue or non-viable osteochondral debris is gently removed with a dental pick or small curette. The surgeon then applies longitudinal traction to the thumb ray to restore length. Next, the thumb is pronated to correct the supination deformity caused by the adductor pollicis. Finally, palmar abduction and direct pressure are applied over the dorsal base of the first metacarpal. This pushes the shaft fragment volarly and ulnarly, reducing it anatomically to the captive volar ulnar fragment. The articular surface must be inspected under direct vision to confirm perfect congruity.
Once anatomic reduction is achieved, provisional fixation is established. If utilizing Kirschner wires, a small-caliber K-wire (0.035-inch or 0.045-inch) is driven across the fracture site under direct vision. Crucially, fixation by a single wire is mechanically insecure and acts only as an axis of rotation. Additional wires must be added in a parallel or slightly divergent fashion to achieve rotational stability and rigid fixation. If the volar ulnar fragment is too small to capture securely, the wires can be driven from the metacarpal shaft directly across the CMC joint into the trapezium to neutralize the deforming forces of the APL.
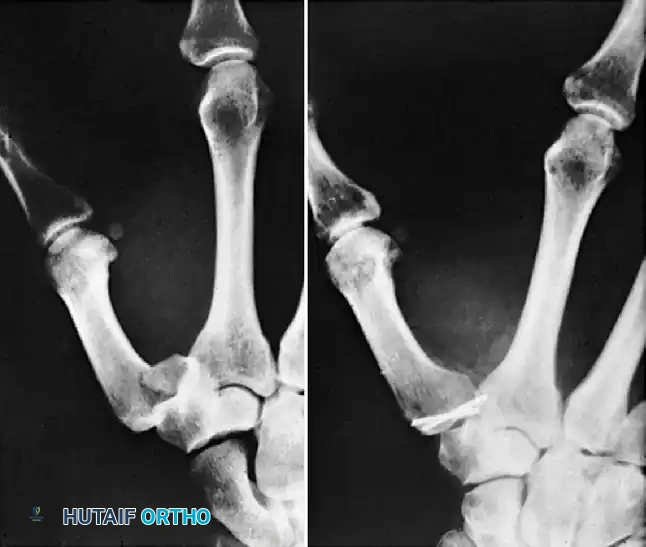
FIGURE 67-12: Comminuted Bennett fracture treated by open reduction. Two Kirschner wires were necessary to keep articular fragments reduced. Note the parallel placement to ensure rotational control.
Alternatively, if the fragment is sufficiently large, rigid internal fixation with a 2.0-mm or 2.7-mm lag screw is performed. A reduction forceps with pointed tines is used to hold the reduction. A gliding hole is drilled in the near cortex (metacarpal shaft), and a thread hole is drilled in the far cortex (volar ulnar fragment). The near cortex is carefully countersunk to prevent the screw head from causing soft tissue irritation or acting as a stress riser. The appropriate length screw is then inserted, achieving robust interfragmentary compression. Regardless of the fixation method, the final reduction and hardware placement must be rigorously confirmed with fluoroscopy in multiple planes before closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the open reduction and internal fixation of Bennett fractures can occur, ranging from minor soft tissue issues to catastrophic joint failure. Understanding these potential pitfalls is critical for prompt recognition and appropriate management. The most significant and functionally debilitating complication is post-traumatic arthritis, which arises primarily from malunion with persistent subluxation or unrecognized articular step-off.
Even a seemingly trivial 1 to 2 mm articular step-off alters the contact stresses across the CMC joint exponentially, leading to rapid cartilage degradation. Iatrogenic complications also represent a significant burden. Injury to the superficial radial nerve (SRN) during the surgical approach can result in a painful neuroma, which often causes more morbidity than the fracture itself. Pin tract infections are relatively common when K-wires are left protruding through the skin, occurring in up to 10-15% of cases, though they usually resolve with oral antibiotics and pin removal. Loss of reduction or hardware failure can occur if the fixation construct is mechanically inadequate or if the patient is non-compliant with postoperative immobilization.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Management Strategies |
|---|---|---|---|
| Post-Traumatic Arthritis | 15% - 30% (Long-term) | Articular step-off >1mm, persistent subluxation, cartilage necrosis. | Anatomic reduction, rigid fixation. Late management requires arthrodesis or LRTI. |
| SRN Neuritis / Neuroma | 5% - 10% | Traction injury, direct laceration during the Wagner approach. | Meticulous blunt dissection, atraumatic retraction with vessel loops. Gabapentinoids, surgical excision if refractory. |
| Pin Tract Infection | 10% - 15% (if K-wires used) | Exposed hardware, poor local hygiene. | Meticulous pin care, burying pins under skin if possible. Treat with oral antibiotics; early removal if deep infection suspected. |
| Loss of Reduction | < 5% | Inadequate fixation (single K-wire), severe comminution, non-compliance. | Use multiple K-wires for rotational control or lag screws. Strict cast immobilization. Revision surgery if recognized early. |
Management of Malunion: Corrective Osteotomy
For a malunion that is recognized early—specifically, before frank degenerative changes and complete loss of cartilage space are noted on radiographs—a corrective osteotomy is indicated to restore joint congruity and normal biomechanics. Attempting to simply "take down" a healed intra-articular fracture is often impossible without destroying the joint. Instead, Giachino described a highly effective, specialized technique for the corrective osteotomy of a malunited Bennett fracture that preserves the articular surface while restoring alignment.
The Giachino corrective osteotomy technique begins with exposing the malunited metacarpal base via the standard Wagner approach. The site of the previous fracture and subsequent malunion is carefully identified. An osteotomy cut is meticulously planned to separate the malunited, shortened metacarpal shaft from the volar ulnar fragment, effectively recreating the original fracture line without violating the joint space.
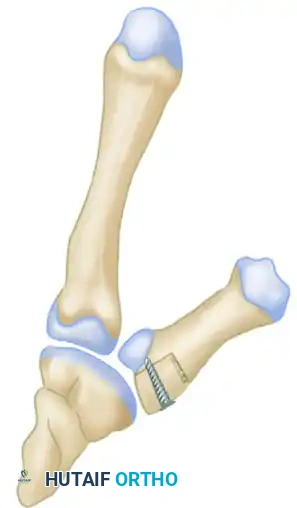
Surgical Diagram A: Identification of the malunion and the planned trajectory for the corrective osteotomy cut to mobilize the metacarpal shaft.
Once the osteotomy is performed, the metacarpal shaft is mobilized. Because the shaft has typically shortened and adducted due to chronic, unopposed muscle pull over several weeks or months, it must be forcefully distracted and realigned. A structural bone graft, most commonly harvested from the distal radius metaphysis or the iliac crest, is fashioned into a precise geometric block. This structural graft is inserted into the osteotomy gap, serving to restore the anatomic length of the metacarpal, correct the adduction deformity, and perfectly realign the articular surface.
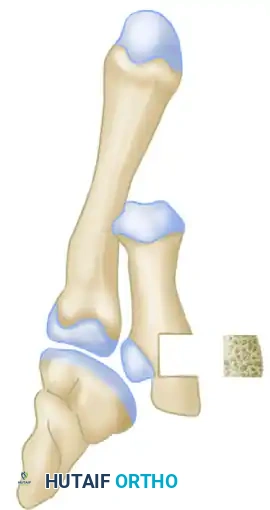
Surgical Diagram B: Distraction of the osteotomy site and insertion of a precisely contoured structural bone graft block to restore metacarpal length and articular congruity.
The newly reconstructed metacarpal base, now incorporating the structural interpositional bone graft, must be rigidly fixed to allow for graft incorporation, bony union, and early mobilization. A lag screw (or multiple K-wires if the fragment is small) is passed through the metacarpal shaft, directly through the center of the bone graft block, and into the volar ulnar fragment. This creates a single, unified construct, compressing the graft and ensuring absolute stability.

Surgical Diagram C: Final construct demonstrating rigid internal fixation with a lag screw compressing the metacarpal shaft, the interpositional bone graft, and the articular fragment.
When a malunion is neglected and advanced degenerative arthritis has already developed, joint-preserving osteotomies like the Giachino technique are no longer viable. In these late-stage scenarios, the cartilage is irreparably damaged, and salvage procedures are advised. Depending on the patient's age, functional demands, and manual labor requirements, the surgeon should proceed with either a first CMC joint arthrodesis (which provides a highly stable, pain-free, but stiff joint ideal for heavy laborers) or a trapeziectomy with ligament reconstruction and tendon interposition (LRTI) arthroplasty (which provides excellent pain relief and restores mobility, preferred for lower-demand or older patients).
Phased Post-Operative Rehabilitation Protocols
Meticulous postoperative care and a highly structured, phased rehabilitation protocol are essential to ensure bony union while preventing the debilitating joint stiffness that frequently plagues hand trauma. The rehabilitation timeline is heavily dictated by the method of fixation utilized (K-wires vs. rigid lag screws) and the overall stability of the osteosynthesis achieved intraoperatively. Close collaboration between the orthopedic surgeon and a certified hand therapist (CHT) is paramount to achieving an optimal functional outcome.
Phase I: Immediate Postoperative Immobilization (Weeks 0 to 4)
Immediately following the surgical closure, the wound is dressed with sterile, non-adherent gauze, and a bulky, well-molded thumb spica forearm cast or rigid fiberglass splint is applied in the operating room. The thumb is immobilized in a position of functional palmar abduction and slight pronation to neutralize the deforming forces of the adductor pollicis and APL. The interphalangeal (IP) joint of the thumb may be left free to allow for early active motion, preventing extensor tendon adhesions, provided the fracture pattern does not require IP immobilization for absolute ray stability. The patient is instructed to keep the extremity elevated above heart level to minimize edema and to perform active range of motion exercises of the fingers, elbow, and shoulder. At 10 to 14 days, the initial cast is removed for wound inspection, suture removal, and radiographic evaluation to ensure maintenance of reduction. The patient is then placed back into a rigid thumb spica cast until 4 weeks post-surgery.
Phase II: Hardware Removal and Early Motion (Weeks 4 to 6)
At the 4-week mark, if Kirschner wires were utilized and left protruding through the skin, they are typically removed in the outpatient clinic, provided there is radiographic evidence of early clinical union (bridging callus and absence of fracture line radiolucency). Following K-wire removal, the patient is transitioned from a rigid fiberglass cast to a custom-molded thermoplastic thumb spica splint. This splint is worn continuously, but the patient may remove it 3 to 4 times a day to initiate supervised active range of motion (AROM) exercises of the CMC and metacarpophalangeal (MCP) joints under the guidance of a hand therapist. Passive range of motion (PROM) and forceful pinching are strictly prohibited during this phase to avoid stressing the newly formed, immature callus.
Accelerated Protocol for Rigid Screw Fixation: If rigid internal fixation was achieved using a lag screw, the rehabilitation timeline can be significantly accelerated. In a compliant patient with radiographically confirmed rigid osteosynthesis, the transition to a removable thermoplastic splint and the initiation of AROM can begin as early as 10 to 14 days postoperatively, dramatically reducing the incidence of long-term joint stiffness.
Phase III: Strengthening and Functional Return (Weeks 6 to 12+)
By 6 weeks postoperatively, radiographic union is typically solid enough to allow for the weaning of the thermoplastic splint during daytime activities, though it may still be worn at night or during high-risk activities for an additional 2 weeks. The hand therapy protocol advances to include gentle passive range of motion and progressive strengthening exercises. Isometric strengthening of the thenar musculature is initiated, followed by dynamic pinch and grip strengthening using therapeutic putty and hand dynamometers. Most patients can expect to return to light duty or non-manual labor by 8 weeks. However, return to heavy manual labor, contact sports, or activities requiring forceful, repetitive gripping is generally restricted until 10 to 12 weeks postoperatively, once full clinical strength and radiographic consolidation are unequivocally confirmed.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the management of Bennett fractures is deeply rooted in landmark orthopedic literature and biomechanical studies that have shaped our current clinical guidelines. Edward Hallaran Bennett's original description in 1882 laid the foundation for understanding the unique pathoanatomy of this injury, differentiating it from simple extra-articular base fractures and highlighting the critical role of the volar ulnar fragment.
Modern surgical indications are heavily influenced by the biomechanical studies of researchers such as Bethel and colleagues, and Lutz et al. These pivotal studies utilized pressure-sensitive film and biomechanical modeling to demonstrate that an articular step-off of as little as 1 mm at the trapeziometacarpal joint decreases the contact area by over 40%, thereby exponentially increasing peak contact stresses. This biomechanical reality forms the basis for the strict, universally accepted guideline that any articular incongruity greater than 1 to 2 mm necessitates open reduction and internal fixation to mitigate the risk of rapid-onset osteoarthritis.
Clinical outcome studies comparing closed versus open management further validate the aggressive surgical approach. Livesley et al. and Cannon et al. published long-term follow-up studies demonstrating that patients treated with anatomic open reduction and rigid internal fixation had significantly lower rates of radiographic arthritis, superior grip and pinch strength, and higher patient-reported outcome scores (such as the DASH score) compared to those managed with closed reduction and casting, particularly when the initial displacement was significant.
Current clinical guidelines from major orthopedic bodies, including the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH), strongly advocate for surgical intervention in displaced Bennett fractures. The consensus dictates that while closed reduction and percutaneous pinning (CRPP) is acceptable for reducible fractures with small fragments, open reduction and internal fixation (ORIF) with either K-wires or lag screws is the definitive standard of care for irreducible fractures, large articular fragments (>20%), or step-offs exceeding 1 mm. These guidelines emphasize that the ultimate goal is not merely bony union, but the precise restoration of joint mechanics to preserve the complex, vital function of the human thumb.
