INTRODUCTION TO BICONDYLAR TIBIAL PLATEAU FRACTURES
Bicondylar tibial plateau fractures (Schatzker types V and VI; AO/OTA type 41-C) represent severe, high-energy intra-articular injuries characterized by metaphyseal-diaphyseal dissociation and profound disruption of both the medial and lateral articular columns. The management of these complex fractures is one of the most formidable challenges in orthopedic traumatology. Successful outcomes depend not only on the anatomic restoration of the articular surface and mechanical axis but, critically, on the meticulous management of the compromised soft tissue envelope.
The surgical approach to complex tibial plateau fractures must be highly individualized on the basis of the particular fracture configuration, the degree of comminution, and the condition of the overlying soft tissues. The following comprehensive guide details a standardized, evidence-based dual-incision approach applicable to the vast majority of these severe injuries.
💡 Clinical Pearl: The Soft Tissue Envelope
The timing of definitive open reduction and internal fixation (ORIF) is dictated entirely by the soft tissue envelope. In high-energy trauma, immediate ORIF is often contraindicated due to massive swelling and fracture blisters. A damage-control approach utilizing a spanning external fixator until the "wrinkle sign" appears (typically 10 to 21 days post-injury) is the gold standard to prevent catastrophic wound complications.
PREOPERATIVE PLANNING AND IMAGING
Thorough preoperative planning is mandatory. Standard orthogonal radiographs (anteroposterior, lateral, and oblique views) provide an initial assessment, but a fine-cut Computed Tomography (CT) scan with 2D sagittal and coronal reformats, as well as 3D reconstructions, is the definitive imaging modality.
CT imaging allows the surgeon to:
* Identify the exact location and size of the posteromedial shear fragment.
* Quantify the depth and location of lateral articular depression.
* Assess the presence of a tibial tubercle fragment, which may alter the surgical approach and postoperative weight-bearing protocol.
* Map the fracture lines to plan optimal plate positioning and screw trajectories.
Based on these imaging studies, the surgeon must map the proposed surgical incisions. Marking the incisions both medially and laterally prior to inflation of the tourniquet aids in confirming that a sufficient soft tissue bridge will be present.
🚨 Surgical Warning: The Soft Tissue Bridge
A minimum skin bridge of 7 centimeters must be maintained between the anterolateral and posteromedial incisions. Violating this rule severely compromises the angiosomal blood supply to the anterior tibial skin flap, drastically increasing the risk of full-thickness skin necrosis, hardware exposure, and deep infection.
PATIENT POSITIONING AND PREPARATION
Optimal positioning is critical for unimpeded fluoroscopic access and surgical ergonomics.
- Table Selection: Place the patient supine on a fully radiolucent fluoroscopic table.
- Positioning Aids: Place a small bump under the ipsilateral hip to correct the natural external rotation of the lower extremity, bringing the patella to a direct anterior position.
- Tourniquet: Apply a well-padded proximal thigh tourniquet. Exsanguination should be performed carefully; in cases of severe comminution or suspected deep vein thrombosis, elevation alone without an Esmarch bandage is preferred before tourniquet inflation.
- Fluoroscopy: Position the C-arm on the contralateral side of the table. Ensure that perfect AP and lateral fluoroscopic views of the proximal tibia can be obtained without obstruction before prepping and draping.
- Draping: The leg is prepped and draped free to allow full flexion and extension of the knee, which is essential for fracture reduction and intraoperative imaging.
SURGICAL APPROACHES
The dual-incision technique utilizes a posteromedial approach to address the medial column and an anterolateral approach to address the lateral column.
The Posteromedial Approach
Typically, the medial or posteromedial approach is performed first. The incision is made along the posteromedial border of the proximal tibia.
* Superficial Dissection: The saphenous nerve and long saphenous vein are identified and protected anteriorly.
* Deep Dissection: The interval is developed between the medial head of the gastrocnemius (retracted posteriorly) and the pes anserinus tendons (retracted anteriorly or distally).
* Exposure: This provides direct access to the posteromedial apex of the fracture, which is typically a vertical shear fragment.
The Anterolateral Approach
The lateral condylar component is exposed through a standard anterolateral approach.
* Incision: A curvilinear incision is made centered over Gerdy's tubercle, extending proximally toward the lateral epicondyle and distally along the anterior tibial crest.
* Deep Dissection: The iliotibial band is incised in line with its fibers. The origin of the extensor musculature (tibialis anterior) is elevated off the proximal lateral tibia.
* Arthrotomy: A submeniscal arthrotomy is performed. The anterior horn of the lateral meniscus is tagged with non-absorbable suture and elevated proximally to provide direct visualization of the lateral articular surface.
STEP-BY-STEP SURGICAL TECHNIQUE
Step 1: Medial Column Reduction and Provisional Fixation
The fundamental strategy in bicondylar fracture management is to first reduce and stabilize the medial condylar segment. The medial fragment is typically a non-comminuted, apex-distal shear fracture.
By anatomically reducing the medial column to the tibial diaphysis, the surgeon restores the length, alignment, and rotation of the tibia, effectively converting a complex bicondylar injury (Schatzker VI) into a simpler unicondylar fracture (Schatzker II or III).
- Reduction: The posteromedial fragment is reduced using a pointed reduction forceps or a ball-spike pusher. The reduction is confirmed fluoroscopically and by direct palpation of the posterior cortical ridge.
- Fixation: Small fragment plates (3.5-mm system) are commonly used. Depending on the fracture morphology, a one-third tubular plate, a reconstruction plate, a T-plate, or a precontoured posteromedial locking plate is applied.
- Biomechanics: The medial plate functions as a true antiglide buttress plate. It is placed at the apex of the fracture to resist the vertical shear forces.
💡 Clinical Pearl: Unicortical Medial Fixation
When apical comminution is present, proximal fixation on the medial plate may be necessary to maintain reduction. We have found temporary unicortical locking screws to be of immense benefit. This technique prevents longer medial screws from crossing the joint line and interfering with the subsequent lateral articular reduction and rafting screw placement. Once the lateral reduction and fixation are complete, these unicortical screws can be exchanged for longer bicortical implants if necessary.
Step 2: Lateral Articular Reconstruction
With the medial column stabilized, attention is turned to the anterolateral approach. Meticulous soft tissue handling is paramount.
- Exposure of the Defect: Retract the lateral meniscus proximally to inspect the articular surface. The lateral condyle typically exhibits a split-depression pattern. The lateral cortical wall is hinged open like a book to expose the central articular depression.
- Elevation: Using a bone tamp introduced through the metaphyseal fracture window, the depressed articular fragments are carefully elevated en masse to restore joint congruity.
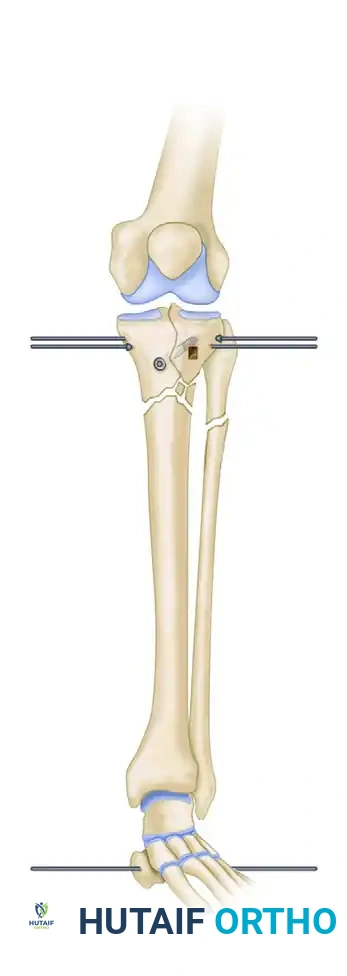
FIGURE 54-59 A: Elevation of the depressed lateral plateau using a bone tamp through a cortical window, with provisional stabilization using a large periarticular clamp.
Step 3: Bone Grafting and Provisional Stabilization
Elevation of the depressed articular segments inevitably leaves a substantial metaphyseal cancellous void. If left unfilled, the articular surface will subside under physiological loading.
- Grafting: The void must be densely packed. Autologous iliac crest bone graft remains the gold standard, but allograft cancellous chips, demineralized bone matrix (DBM), or structural synthetic bone substitutes (e.g., calcium phosphate cement) are highly effective alternatives that eliminate donor site morbidity.
- Provisional Fixation: Once the articular surface is flush with the medial condyle and the meniscus, large periarticular clamps are used to effect compression between the medial and lateral condyles, restoring the normal tibial plateau width.
- Wire Placement: Opposing olive wires (Kirschner wires with a stopper) are placed subchondrally to hold the reduction.

FIGURE 54-59 B: Placement of opposing olive wires and a cannulated screw to maintain articular reduction and compression after subchondral bone grafting.
Step 4: Definitive Anterolateral Fixation
Perform definitive anterolateral fixation with a precontoured proximal tibial locking plate (typically a 3.5-mm or 4.5-mm system).
- Plate Positioning: The plate is slid submuscularly down the lateral shaft. The proximal portion of the plate must sit flush against the lateral condyle.
- Rafting Screws: Proximal locking screws are inserted parallel to the joint line. These "rafting screws" act as a mechanical floor, supporting the elevated articular fragments and the bone graft, preventing secondary subsidence. The proximal fixation of modern precontoured plates allows the screws to reach across and capture the medial condylar segment, providing a highly stable construct.
- Diaphyseal Fixation: The distal portion of the plate is secured to the tibial diaphysis using a combination of non-locking cortical screws (to pull the bone to the plate) and locking screws (for angular stability in osteopenic bone).
Step 5: Finalizing Medial Fixation and Meniscal Repair
Return to the medial side to finalize fixation. If temporary unicortical screws were used proximally, they can now be safely exchanged for longer bicortical screws, ensuring they interdigitate with, but do not strike, the lateral rafting screws.
Any meniscal pathological process must be addressed before closure. Peripheral detachments of the lateral meniscus are extremely common in these injuries. The meniscus must be meticulously repaired and sutured back to the joint capsule or directly to the lateral tibial rim through drill holes or suture anchors. A competent meniscus is vital for containing the lateral condyle and preventing late post-traumatic osteoarthritis.
Step 6: Closure
Thorough irrigation of both wounds is performed to remove bone debris and hematoma.
* The iliotibial band and tibialis anterior fascia are loosely approximated to cover the lateral plate, avoiding excessive tension.
* The medial wound is closed in layers.
* Skin is closed with non-absorbable sutures or surgical staples. Meticulous, tension-free skin closure is critical to prevent wound dehiscence.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for early joint mobilization (to prevent arthrofibrosis and promote cartilage nutrition) with the mechanical necessity of protecting the fracture fixation.
- Drainage: Closed suction drains are routinely placed medially and laterally to prevent hematoma formation, which can compromise the skin flaps. Drains are typically removed on postoperative day 1 or 2.
- Early Motion: After postoperative day 1 to 2, gentle active and active-assisted exercises are instituted. Controlled passive motion (such as the use of a Continuous Passive Motion or CPM machine) may be utilized to achieve 0 to 90 degrees of flexion within the first week.
- Weight-Bearing: Strict adherence to weight-bearing restrictions is mandatory. Weight bearing is not permitted for 12 weeks postoperatively. Premature weight-bearing is the leading cause of hardware failure and articular subsidence. Patients are mobilized non-weight-bearing with crutches or a walker.
- Protocol Modifications: Any associated soft tissue issues (e.g., delayed wound healing, skin flap necrosis) may delay the initiation of aggressive motion. Furthermore, certain fracture patterns, such as those involving a concomitant avulsion of the tibial tubercle, require immobilization in extension for 4 to 6 weeks to protect the extensor mechanism repair before flexion exercises can safely commence.
- Radiographic Follow-up: Serial radiographs are obtained at 2, 6, and 12 weeks to monitor the maintenance of articular reduction, hardware integrity, and progressive fracture consolidation. Progressive weight-bearing is initiated only after radiographic evidence of bridging callus is observed at the metaphyseal-diaphyseal junction, typically around the 12-week mark.
📚 Medical References
- Bicondylar tibial plateau fractures treated with a hybrid ring external fi xator: a preliminary study, J Orthop Trauma 8:455, 1994.
- [Taylor JC, Martin SL: Use of the Ilizarov external fi xator for fractures, nonunions, and malunions. In Gustilo RB, Kyle RF, Templeman DC, eds: Fractures and dislocations, St Louis, 1993, Mosby.
Tornetta P III, Weiner L, Bergman M, et al: Pilon fractures: treatment with combined internal and external fi xation, J Orthop Trauma 7:489, 1993.](https://pubmed.ncbi.nlm.nih.gov/?term=Taylor%20JC%2C%20Martin%20SL%3A%20Use%20of%20the%20Ilizarov%20external%20%EF%AC%81%20xator%20for%20fractures%2C%20nonunions%2C%20and%20malunions.%20In%20Gustilo%20RB%2C%20Kyle%20RF%2C%20Templeman%20DC%2C%20eds%3A%20Fractures%20and%20dislocations%2C%20St%20Louis%2C%201993%2C%20Mosby.%0A%0ATornetta%20P%20III%2C%20Weiner%20L%2C%20Bergman%20M%2C%20et%20al%3A%20Pilon%20fractures%3A%20treatment%20with%20combined%20internal%20and%20external%20%EF%AC%81%20xation%2C%20J%20Orthop%20Trauma%207%3A489%2C%201993.)
- Vidal MJ: Notre expérience du fi xateur externe d’Hoffmann, Soc Chir Montpellier 14:451, 1968.
- Weiner L, Kelley M, Yang E, et al: Treatment of severe proximal tibia fractures with minimal internal and external fi xation, J Orthop Trauma 5:236, 1991.
- Weiner LS, Kelley M, Yang E, et al: The use of combination internal fi xation and hybrid external fi xation in severe proximal tibia fractures, J Orthop Trauma 9:244, 1995.
- Yang EC, Weiner L, Strauss E, et al: Metaphyseal dissociation fractures of the proximal tibia: an analysis of treatment and complications, Am J Orthop 24:695, 1995.
- Zinman C, Norman D, Hamoud K, et al: External fi xation for severe open fractures of the humerus caused by missiles, J Orthop Trauma 11:536, 1997.
