Comprehensive Introduction and Patho-Epidemiology
Fractures and fracture-dislocations of the distal interphalangeal (DIP) joint, along with those of the distal phalanx, represent some of the most frequently encountered injuries in both emergency departments and specialized hand surgery clinics. Despite their prevalence, these injuries are frequently underestimated by primary care providers, leading to delayed presentations, chronic deformities, and significant functional impairment. The delicate interplay between the terminal extensor tendon, the flexor digitorum profundus (FDP), and the collateral ligament complex demands meticulous anatomic restoration to preserve digital function. Open reduction and internal fixation (ORIF) utilizing Kirschner wires (K-wires) remains a highly versatile, reliable, and fundamental technique in the armamentarium of the hand surgeon, offering rigid stabilization while minimizing the footprint of implanted hardware in a profoundly constrained soft-tissue envelope.
The epidemiology of distal phalangeal and DIP joint injuries reveals a bimodal distribution, predominantly affecting young, active males engaged in athletic pursuits or manual labor, and older individuals sustaining low-energy falls. Crush injuries, axial loads, and forced flexion against an actively extending digit are the hallmark mechanisms of injury. In the athletic population, the classic "mallet finger" occurs when a ball strikes the extended fingertip, forcing it into sudden flexion and resulting in either a tendinous rupture or an osteochondral avulsion fracture of the dorsal proximal articular surface of the distal phalanx. Conversely, industrial crush injuries often result in highly comminuted, open tuft or shaft fractures that require meticulous soft tissue management in tandem with osseous stabilization.
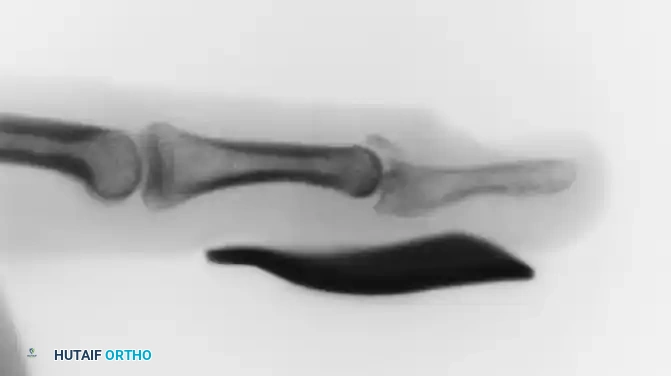
FIGURE 67-65 A: Acute type 1 mallet finger demonstrating the classic flexion deformity at the DIP joint with secondary “swanning” (hyperextension) of the proximal interphalangeal joint.
The pathophysiology of these injuries is dictated by the precise vector of force and the integrity of the surrounding tendinous insertions. In the setting of a bony mallet finger, the fracture fragment is tethered proximally by the terminal extensor tendon, while the remaining distal phalanx is subjected to the unopposed, powerful flexion force of the FDP. This biomechanical mismatch frequently leads to volar subluxation of the distal phalanx relative to the middle phalanx, a condition that rapidly accelerates articular cartilage degradation and leads to post-traumatic osteoarthritis if left unreduced. Furthermore, the intimate relationship between the distal phalangeal physis and the nail matrix in pediatric patients creates a unique pathoanatomic entity known as the Seymour fracture, where a juxta-epiphyseal fracture is almost universally accompanied by a laceration of the sterile or germinal matrix, effectively rendering it an open fracture with a high risk of osteomyelitis.
Understanding the complex patho-epidemiology of these injuries is paramount for the orthopedic surgeon. The decision to pursue operative intervention via K-wire fixation is not merely a question of radiographic alignment, but a nuanced calculation involving the patient's functional demands, the degree of soft tissue compromise, the presence of articular step-off, and the inherent stability of the fracture pattern. This comprehensive chapter will dissect the biomechanical principles, surgical anatomy, and step-by-step operative execution required to master K-wire fixation of the distal phalanx and DIP joint, ensuring optimal outcomes in the face of challenging digital trauma.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
The distal phalanx is a unique osseous structure, lacking a medullary canal in its distal tuft and relying heavily on the surrounding highly vascularized pulp for its blood supply. The base of the distal phalanx expands into a bicondylar articular surface that interfaces with the corresponding head of the middle phalanx to form the DIP joint. This joint is a classic ginglymus (hinge) joint, allowing primarily for flexion and extension, with a normal arc of motion ranging from 0 degrees of extension to approximately 80 degrees of flexion. The articular geometry is stabilized dynamically by the surrounding tendons and statically by the joint capsule, the volar plate, and the collateral ligaments.
The volar plate of the DIP joint is a robust, fibrocartilaginous structure that attaches firmly to the volar base of the distal phalanx and more proximally and loosely to the neck of the middle phalanx. It serves to prevent hyperextension and deepens the articular concavity. The collateral ligaments consist of the proper collateral ligaments, which are taut in flexion, and the accessory collateral ligaments, which are taut in extension and blend into the lateral margins of the volar plate. Surgical approaches to the DIP joint must respect these stabilizing structures; indiscriminate division of the collateral ligaments during open reduction can lead to chronic coronal plane instability.
Biomechanically, the DIP joint is subjected to extraordinary forces during normal activities of daily living, particularly during pinch and grasp. The joint reaction forces can exceed several times the patient's body weight during a forceful pinch. The moment arm of the FDP is significantly greater than that of the terminal extensor tendon, creating an inherent imbalance that must be counteracted by the extensor mechanism. When a dorsal articular fracture occurs (bony mallet), this delicate balance is destroyed, and the mechanical advantage of the FDP drives the distal phalanx into volar subluxation, highlighting the necessity for rigid internal fixation to counteract these deforming forces during the healing phase.
The Extensor and Flexor Mechanisms
The extensor mechanism at the level of the DIP joint is an intricate confluence of tendinous slips and retinacular structures. The terminal extensor tendon is formed by the convergence of the two lateral bands, which themselves receive contributions from the intrinsic musculature (lumbricals and interossei) and the extrinsic extensor digitorum communis. The terminal tendon inserts broadly into the dorsal base of the distal phalanx, immediately distal to the articular margin. Disruption of this insertion results in the classic mallet deformity. The triangular ligament, located dorsally over the middle phalanx, prevents volar subluxation of the lateral bands, while the oblique retinacular ligament of Landsmeer coordinates motion between the PIP and DIP joints.
On the volar aspect, the FDP tendon travels through the digital fibro-osseous sheath, emerging from the bifurcation of the flexor digitorum superficialis (Camper's chiasm) to insert onto the entire volar base of the distal phalanx. The insertion is broad and robust, extending from the proximal metaphyseal-diaphyseal junction to the volar articular margin. The FDP is nourished by the vincula brevia and longa, and its excursion is constrained by the A5 pulley and the C3 pulley. In the context of DIP joint trauma, the powerful pull of the FDP is the primary deforming force in dorsal avulsion fractures and must be neutralized, either via extension block pinning or direct rigid fixation of the articular fragment.
Understanding the dynamic interplay between the flexor and extensor mechanisms is critical for surgical planning. For instance, when treating a chronic mallet finger or a delayed presentation of a bony mallet, the surgeon must account for the proximal retraction and contracture of the extensor mechanism, as well as the secondary hyperextension deformity that often develops at the PIP joint (swan-neck deformity) due to the proximal migration of the lateral bands and the unopposed pull of the central slip. Successful K-wire fixation must therefore not only address the osseous anatomy but also restore the resting tension of these complex tendinous networks.
The Perionychium and Microvascular Supply
The perionychium, comprising the nail bed and its surrounding structures, is intimately associated with the dorsal cortex of the distal phalanx. The nail bed is divided into the proximal germinal matrix, responsible for the generation of the nail plate, and the distal sterile matrix, which tightly adheres the nail plate to the underlying periosteum. The proximal extent of the germinal matrix extends beneath the eponychial fold, resting directly over the dorsal base of the distal phalanx and, crucially in pediatric patients, directly overlying the physis.
This anatomic proximity dictates that any displaced fracture of the distal phalangeal base or physis will almost invariably lacerate the overlying nail matrix. Failure to recognize and meticulously repair these lacerations can lead to catastrophic complications, including permanent nail dystrophy (ridging, splitting, or non-adherence), chronic osteomyelitis, and nonunion. Surgical approaches to the dorsal DIP joint must therefore be executed with extreme care to avoid iatrogenic injury to the germinal matrix. When placing retrograde K-wires through the tip of the distal phalanx, the surgeon must ensure the wire enters perfectly centrally, just volar to the hyponychium, to avoid traversing and damaging the sterile matrix.
The microvascular supply to the distal phalanx and perionychium is derived from the terminal arborizations of the proper palmar digital arteries. These vessels form a rich anastomotic arcade within the digital pulp, supplying both the osseous tuft and the nail bed via multiple perforating branches. The venous drainage is primarily dorsal. Surgical dissection, particularly during the elevation of dorsal skin flaps or the placement of pull-out buttons on the volar pulp, must be performed judiciously to avoid devascularizing the skin edges or causing ischemic necrosis of the highly innervated digital pulp, which can result in chronic, debilitating pain.
Exhaustive Indications and Contraindications
Classification Systems and Operative Thresholds
The decision to proceed with open reduction and K-wire fixation of the DIP joint is heavily influenced by the classification of the injury. The Wehbe and Schneider classification for mallet finger fractures is widely utilized, categorizing injuries based on the size of the articular fragment and the degree of subluxation. Type I involves <33% of the articular surface, Type II involves 33-66%, and Type III involves >66%. Each type is further subclassified by the presence (B) or absence (A) of volar subluxation. While Type I and most Type IIA injuries can be managed non-operatively with strict extension splinting, Type IIB and Type III injuries generally mandate surgical intervention to restore joint congruity and prevent post-traumatic arthritis.
Operative thresholds are not solely dictated by radiographic parameters. The patient's occupation, compliance, and functional demands play a critical role. A concert pianist with a 25% articular fracture without subluxation may benefit from the precise anatomic restoration afforded by ORIF, whereas an elderly, low-demand patient with a similar fracture might be best served by conservative splinting. Furthermore, the chronicity of the injury alters the indication paradigm; acute fractures (less than 3-4 weeks old) are highly amenable to K-wire fixation, whereas chronic, malunited fractures may require corrective osteotomy or primary arthrodesis.
Contraindications to K-wire fixation must be carefully considered. Absolute contraindications include active, untreated local infection (e.g., paronychia, felon) or profound vascular compromise to the digit that precludes safe surgical dissection. Severe, pre-existing osteoarthritis of the DIP joint is a relative contraindication to ORIF, as restoring the articular surface of an already degenerate joint will not relieve pain; in such cases, primary arthrodesis is the procedure of choice. Poor patient compliance with postoperative splinting and pin care protocols is also a strong relative contraindication, as it drastically increases the risk of pin-tract infection and hardware failure.
The Mallet Finger Spectrum
The spectrum of mallet finger injuries ranges from closed, isolated tendinous disruptions to complex, open fracture-dislocations. Type 1 (closed soft tissue mallet) and Type 2 (open tendinous mallet) injuries are primarily soft tissue problems. Type 1 injuries are almost universally managed with continuous extension splinting for 6 to 8 weeks. However, if a patient presents with an open laceration over the DIP joint (Type 2), direct operative repair of the extensor tendon is indicated, frequently augmented by a transarticular K-wire to protect the repair during the initial healing phase.

FIGURE 67-65 B: Aluminum splint achieving full extension of the distal interphalangeal joint.
Type 3 injuries involve complex open trauma with significant soft tissue and tendon loss, often resulting from industrial abrasions or crush injuries. These devastating injuries require a multidisciplinary approach, often necessitating local or regional flap coverage (e.g., cross-finger flap, reverse cross-finger flap) in conjunction with K-wire stabilization of the osseous structures. If the joint surface is irreparably destroyed, primary arthrodesis is performed concurrently with soft tissue coverage to expedite functional recovery and minimize the number of surgical interventions.
Type 4 injuries (bony mallets) are the primary indication for the techniques detailed in this chapter. When the dorsal articular fragment is large enough to compromise the stability of the DIP joint, the unopposed pull of the FDP causes volar subluxation. This is an absolute indication for surgery. The goal is to reduce the joint, restore the articular contour, and neutralize the deforming forces. Whether this is achieved via closed extension block pinning (Ishiguro technique) or open reduction with direct K-wire fixation or pull-out wires depends on the size of the fragment, the degree of comminution, and the presence of soft tissue interposition.
Pediatric Seymour Fractures
Pediatric Seymour fractures are a distinct clinical entity that demands aggressive and timely surgical management. These are juxta-epiphyseal fractures of the distal phalanx, typically occurring in children and adolescents prior to physeal closure. The pathoanatomy is characterized by a flexion deformity of the epiphyseal fragment (tethered by the FDP) and extension of the diaphyseal fragment (tethered by the terminal extensor). Crucially, the nail plate is almost always avulsed proximally, slipping dorsal to the eponychial fold and exposing the fracture site to the external environment.
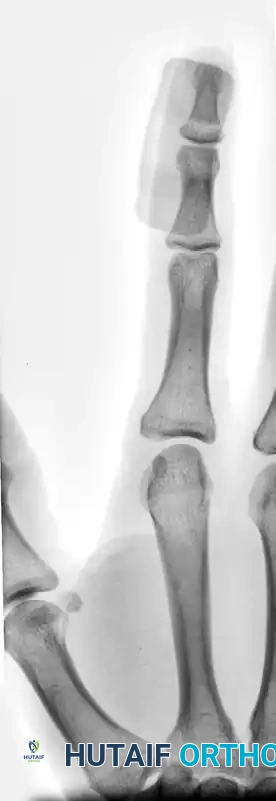
FIGURE 67-64 A and B: Displaced and angulated distal phalangeal fracture associated with a severe nail bed laceration in a 22-year-old patient, demonstrating the classic presentation of a complex open distal phalanx injury.
The indication for operative intervention in a Seymour fracture is absolute. Misdiagnosis as a simple soft-tissue mallet finger and subsequent application of an extension splint without formal irrigation and debridement is a catastrophic error that routinely leads to deep space infection, osteomyelitis of the distal phalanx, and premature physeal arrest. The surgical imperative is to perform a thorough washout of the fracture hematoma, extract any interposed germinal matrix or soft tissue from the fracture site, anatomically reduce the physis, and stabilize it with a longitudinal K-wire.
Following osseous stabilization, the nail bed must be meticulously repaired with fine absorbable sutures (e.g., 6-0 chromic gut), and the nail plate (or a synthetic substitute) must be replaced beneath the eponychial fold to stent the matrix open and prevent synechiae formation. The K-wire is typically left in place for 3 to 4 weeks, and the patient is maintained on a course of prophylactic oral antibiotics to mitigate the high risk of infection inherent to these open physeal injuries.
| Indication / Contraindication | Criteria / Details | Rationale / Management Strategy |
|---|---|---|
| Absolute Indication | Bony mallet with volar subluxation | Prevents rapid onset post-traumatic osteoarthritis; restores joint kinematics. |
| Absolute Indication | Open Seymour Fracture (Pediatric) | High risk of osteomyelitis; requires I&D, anatomic physeal reduction, and nail bed repair. |
| Relative Indication | Bony mallet >33% articular surface, without subluxation | Controversial; high-demand patients benefit from ORIF to ensure absolute joint congruity. |
| Absolute Contraindication | Active local infection (Felon, Paronychia) | Hardware insertion will seed infection into the bone/joint; requires I&D and antibiotics first. |
| Relative Contraindication | Severe pre-existing DIP osteoarthritis | Anatomic reduction will not relieve arthritic pain; primary arthrodesis is preferred. |
| Relative Contraindication | Extreme non-compliance / Severe dementia | High risk of premature pin removal, pin-tract infection, and catastrophic failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Advanced Imaging
A meticulous clinical evaluation is the foundation of successful pre-operative planning. The surgeon must assess the vascular status of the digit, utilizing capillary refill and digital Allen's tests if necessary. The integrity of the extensor and flexor mechanisms must be evaluated, noting any resting deformities, active range of motion deficits, or the presence of a swan-neck deformity. In cases of acute trauma, the skin envelope must be carefully inspected for abrasions, lacerations, or signs of impending necrosis resulting from pressure exerted by a displaced osseous fragment.
Standard radiographic evaluation includes true anteroposterior (AP), lateral, and oblique views of the affected digit. The true lateral view is paramount for assessing the size of the dorsal articular fragment in a bony mallet, the degree of volar subluxation, and the congruity of the joint space. Oblique views are particularly useful for identifying subtle condylar fractures or avulsions of the collateral ligament insertions. In cases of severe comminution or delayed presentation where the osseous anatomy is obscured by callus, a dedicated computed tomography (CT) scan with 3D reconstructions can be invaluable for precise surgical templating and implant selection.
Templating involves determining the optimal trajectory and caliber of the K-wires. For transarticular pinning of the DIP joint in an adult, a 0.045-inch or 0.035-inch K-wire is typically selected, balancing the need for rigidity against the risk of iatrogenic chondral damage. In pediatric patients, smaller wires (0.028-inch) are utilized to minimize trauma to the physis. The surgeon must mentally map the entry point—typically just volar to the hyponychium for retrograde transarticular wires—and anticipate the necessary depth of penetration into the middle phalanx to achieve adequate cortical purchase without violating the PIP joint.
Anesthesia, Tourniquet Selection, and Positioning
The choice of anesthesia is dictated by patient preference, comorbidities, and the anticipated duration of the procedure. Wide Awake Local Anesthesia No Tourniquet (WALANT) has revolutionized hand surgery and is highly applicable to DIP joint fixation. Utilizing a mixture of lidocaine and epinephrine injected locally provides excellent anesthesia and a bloodless field without the need for a tourniquet, allowing the surgeon to assess active tendon excursion and joint stability intra-operatively. Alternatively, a traditional digital block or a regional block (axillary or supraclavicular) can be employed.
If WALANT is not utilized, a tourniquet is essential for meticulous visualization of the delicate articular and soft tissue structures. A sterile digital tourniquet (such as a Penrose drain or a dedicated silicone ring) is often sufficient for isolated DIP joint procedures. However, the surgeon must be mindful of the duration of digital ischemia, generally keeping it under 60 minutes to prevent neurovascular neurapraxia. For more extensive procedures requiring proximal dissection, a forearm or upper arm pneumatic tourniquet is preferred, set to approximately 250 mmHg.
Patient positioning is critical for ergonomic execution of the surgery. The patient is positioned supine with the operative arm extended on a radiolucent hand table. The hand is pronated for dorsal approaches to the DIP joint. Intraoperative fluoroscopy (a mini C-arm) is brought in from the head or the foot of the table, positioned to allow seamless transition between AP and lateral views without requiring the surgeon to alter the position of the stabilized digit. The display monitor must be positioned directly in the surgeon's line of sight to facilitate real-time, image-guided wire placement.
Implant Selection and Templating
While K-wires remain the workhorse for distal phalangeal fixation due to the minimal soft tissue envelope, the surgeon must be prepared with a variety of sizes and configurations. Double-ended K-wires are preferred for techniques requiring retrograde and subsequent antegrade driving. Threaded K-wires may be considered for increased pull-out strength in osteoporotic bone, though they carry a higher risk of stress risers and breakage during removal.
In addition to K-wires, the surgeon must have access to fine non-absorbable sutures (e.g., 4-0 or 5-0 Prolene or Nylon) and sterile buttons for pull-out wire techniques. If the fracture pattern involves a large, non-comminuted dorsal fragment, the surgeon might also template for the use of a specialized hook plate or a micro-screw (1.0 mm or 1.2 mm), though these implants require a larger surgical exposure and carry a higher risk of symptomatic hardware prominence compared to low-profile K-wire constructs.
Pre-operative templating also involves planning the trajectory of the extension block pin in the Ishiguro technique. The pin must be driven into the middle phalanx at an angle of approximately 45 degrees, entering just proximal to the dorsal articular margin of the middle phalanx. The goal is to create a rigid backstop that prevents the dorsal fragment of the distal phalanx from displacing proximally when the DIP joint is brought into extension. Precise templating of this angle on the pre-operative lateral radiograph minimizes the need for multiple passes and reduces iatrogenic damage to the extensor mechanism.
Step-by-Step Surgical Approach and Fixation Technique
Soft Tissue Handling and Surgical Approaches
When closed reduction fails or is contraindicated due to severe articular displacement or soft tissue interposition, open reduction is mandated. The choice of surgical approach must balance adequate visualization of the fracture with the preservation of the fragile dorsal skin envelope and the underlying perionychium. A midlateral incision is frequently favored, as it avoids creating a dorsal scar that could tether the extensor mechanism or a volar scar that could lead to a painful flexion contracture. The incision is centered over the DIP joint, staying dorsal to the neurovascular bundle and volar to the lateral bands.
Alternatively, a dorsal H-incision, Y-incision, or a gull-wing approach can be utilized for direct exposure of the dorsal articular fragment. These approaches require meticulous full-thickness flap elevation to preserve the subdermal vascular plexus. Once the skin flaps are retracted, the dorsal capsule and the terminal extensor tendon are identified. In the setting of a bony mallet, the fracture hematoma is evacuated, and the joint is thoroughly irrigated. The surgeon must carefully inspect the joint space for incarcerated fragments of cartilage, avulsed portions of the volar plate, or interposed collateral ligaments that may physically block anatomic reduction.
Handling of the articular fragments must be exceptionally delicate. Small dental picks, fine Freer elevators, or single skin hooks are used to manipulate the fragments. Crushing the fragment with heavy forceps will destroy the articular cartilage and compromise the fixation. The surgeon must also identify the insertion of the terminal extensor tendon onto the dorsal fragment; preserving this attachment is critical, as it provides the vascular supply to the fragment and is essential for the restoration of active extension post-operatively.
Closed and Percutaneous Techniques: The Ishiguro Extension Block
For many Type 4 bony mallet fingers, particularly those without severe comminution or soft tissue interposition, the closed extension block pinning technique described by Ishiguro offers an elegant, minimally invasive solution. This technique relies on ligamentotaxis and the creation of a physical osseous block to achieve reduction. Under fluoroscopic guidance, the DIP joint is maximally flexed. This maneuver pulls the dorsal fragment distally via the tension of the terminal extensor tendon, reducing it into its anatomic bed.
While maintaining flexion, a 0.045-inch K-wire is driven dorsally through the extensor tendon, just proximal to the reduced dorsal fragment, and directed obliquely into the head and neck of the middle phalanx at a 45-degree angle. This wire serves as the "extension block." The DIP joint is then gently extended. As the distal phalanx extends, the volar subluxation is corrected, and the dorsal fragment is compressed against the extension block pin, locking it into anatomic position
Clinical & Radiographic Imaging Archive









