INTRODUCTION TO DISTAL INTERPHALANGEAL JOINT FIXATION
Fractures and fracture-dislocations of the distal interphalangeal (DIP) joint present unique biomechanical and surgical challenges. The delicate interplay between the terminal extensor tendon, the flexor digitorum profundus (FDP), and the collateral ligament complex demands meticulous anatomic restoration to preserve digital function. Open reduction and internal fixation (ORIF) utilizing Kirschner wires (K-wires) remains a highly versatile, reliable, and fundamental technique in the armamentarium of the hand surgeon.
This comprehensive guide details the indications, biomechanical principles, and step-by-step surgical execution for K-wire fixation of the DIP joint, with a specific focus on complex intra-articular fractures, the spectrum of mallet finger injuries, and pediatric Seymour fractures.
SURGICAL ANATOMY AND BIOMECHANICS
Successful operative intervention at the DIP joint requires a profound understanding of its functional anatomy. The DIP joint is a hinge joint stabilized by a robust volar plate and true and accessory collateral ligaments.
- Extensor Mechanism: The terminal slip of the extensor tendon inserts into the dorsal base of the distal phalanx. Disruption here results in a mallet deformity, characterized by an inability to actively extend the DIP joint.
- Flexor Mechanism: The FDP tendon inserts broadly into the volar base of the distal phalanx. In the setting of a dorsal articular fracture (bony mallet), the unopposed pull of the FDP can cause volar subluxation of the distal phalanx.
- Nail Bed Complex: The germinal matrix extends proximally beneath the eponychial fold, resting directly over the base of the distal phalanx. Fractures in this region frequently lacerate the nail bed, converting a closed injury into an open fracture.
Clinical Pearl: The proximity of the germinal matrix to the distal phalangeal physis in pediatric patients means that physeal fractures (Seymour fractures) almost invariably involve a laceration of the nail bed, necessitating formal open debridement to prevent osteomyelitis.
CLASSIFICATION AND INDICATIONS FOR SURGERY
The Mallet Finger Spectrum
Mallet fingers are classified based on the extent of soft tissue and bony involvement. Treatment algorithms are dictated by this classification.
Type 1: Closed Soft Tissue Mallet
These injuries involve a closed disruption of the terminal extensor tendon, often presenting with secondary "swan neck" posturing of the proximal interphalangeal (PIP) joint due to proximal retraction of the extensor mechanism.
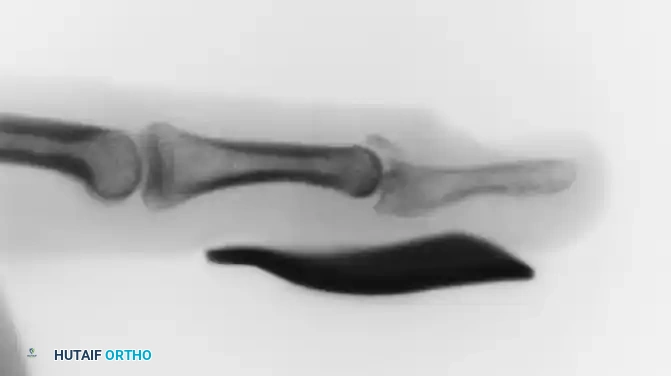
FIGURE 67-65 A: Acute type 1 mallet finger demonstrating the classic flexion deformity at the DIP joint with secondary “swanning” (hyperextension) of the proximal interphalangeal joint.
Management: Treatment is almost exclusively nonoperative. Continuous DIP joint extension splinting using a molded polythene (Stack) or aluminum splint is required for 6 to 8 weeks.

FIGURE 67-65 B: Aluminum splint achieving full extension of the distal interphalangeal joint.
Surgical Warning: When applying volar or dorsal splints, extreme care must be taken to prevent skin maceration and ulceration. Hyperextension of the DIP joint must be strictly avoided; it causes blanching of the dorsal skin, leading to ischemia and subsequent full-thickness skin breakdown over the joint.
Type 2: Open Mallet Injuries
These involve an open laceration over the dorsum of the DIP joint, transecting the tendon.
Management: While closed reduction and splinting can be attempted after meticulous wound care, splint management is often complicated by the wound. Direct operative repair of the extensor tendon using a core suture, augmented by transarticular K-wire fixation of the DIP joint in full extension for 4 to 6 weeks, is highly recommended.
Type 3: Complex Open Mallet with Tissue Loss
These injuries feature deep abrasions or avulsions with loss of skin, subcutaneous tissue, and tendon substance.
Management: Requires formal soft tissue coverage (e.g., local rotational flaps, cross-finger flaps), transarticular pinning of the DIP joint, and potentially primary arthrodesis if the joint surface is irreparably destroyed.
Type 4: Bony Mallet Fingers (Fracture-Dislocations)
Type 4 injuries involve a fracture of the dorsal articular base of the distal phalanx.
* Type 4A: Pediatric physeal injuries.
* Type 4B: Fracture involving 20% to 50% of the articular surface.
* Type 4C: Fracture involving >50% of the articular surface.
Management Controversy: The treatment of Type 4B and 4C injuries remains debated. Nonoperative treatment via extension splinting is advocated by some, arguing that joint congruity may not strictly correlate with final functional outcomes. However, operative intervention is strongly indicated for fractures involving more than one-third of the articular surface that are associated with volar subluxation of the distal phalanx.
PEDIATRIC SEYMOUR FRACTURES
Pediatric mallet equivalents, or Seymour fractures, are juxta-epiphyseal fractures of the distal phalanx. They are frequently open, mimicking a simple mallet finger but carrying a much higher morbidity if mismanaged.
Pathoanatomy: The fracture occurs through the physis (often Salter-Harris Type I or II). The proximal fragment (epiphysis) remains flexed by the FDP, while the distal fragment (shaft) is extended by the terminal tendon. The nail plate is typically avulsed proximally and rests dorsally on the eponychial fold, exposing the fracture site to the environment. Continuous bleeding around the nail base is a hallmark sign.
Management Protocol:
1. Anesthesia: Administer an adequate digital block (single injection at the palmar digital crease).
2. Irrigation: The wound must be aggressively cleaned and irrigated. This is facilitated by gently flexing the distal fragment to open the fracture book.
3. Reduction: The fracture is reduced closed with mild extension of the distal phalanx. The nail plate must be carefully placed back beneath the eponychial fold to stabilize the fracture and stent the germinal matrix.
4. Fixation: Displaced Salter-Harris Type III fractures, or any Seymour fracture where closed reduction cannot be maintained, require open reduction and K-wire fixation of the epiphyseal fragment.
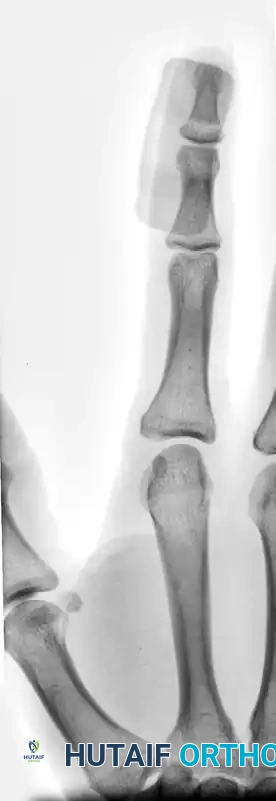
FIGURE 67-64 A and B: Displaced and angulated distal phalangeal fracture associated with a severe nail bed laceration in a 22-year-old patient, demonstrating the classic presentation of a complex open distal phalanx injury.



FIGURE 67-64 C and D: Postoperative radiographic and clinical appearance after precise bone fixation with a K-wire, which provided the necessary stability to permit subsequent realignment and microsurgical repair of the nail bed.
SURGICAL TECHNIQUE: OPEN REDUCTION AND K-WIRE FIXATION
When closed reduction fails or is contraindicated due to soft tissue interposition or severe articular displacement, open reduction is mandated.
1. Patient Positioning and Preparation
- The patient is positioned supine with the arm extended on a radiolucent hand table.
- A regional block (axillary or supraclavicular) or a local digital block is administered.
- A sterile finger tourniquet or forearm tourniquet is applied to ensure a bloodless surgical field.
- Intraoperative fluoroscopy (mini C-arm) must be positioned for orthogonal views.
2. Surgical Approach
- Incision: Make a midlateral incision at the level of the affected DIP joint. This approach avoids the creation of a volar scar that could lead to flexion contractures and provides excellent visualization of the collateral ligaments and joint space.
- Dissection: Carefully elevate the skin flaps, protecting the dorsal sensory branches and the volar neurovascular bundle.
3. Joint Exposure and Debridement
- Expose the joint capsule. In the setting of trauma, the capsule is often already breached.
- Hematoma Evacuation: Thoroughly irrigate the joint to remove all granulation tissue, fibrinous exudate, and organized hematoma.
- Obstacles to Reduction: Inspect the joint under direct vision. Often, the volar plate is avulsed and lies incarcerated between the joint surfaces, physically blocking reduction. If the volar plate is irreparably damaged and blocking reduction, it must be excised. Similarly, damaged portions of the collateral ligaments may need to be excised to allow the distal phalanx to hinge back into an anatomic position.
4. Reduction and Fixation
- Reduce the joint anatomically under direct vision. Use a dental pick or a small Freer elevator to manipulate small articular fragments.
- K-Wire Placement: Once reduced, hold the joint securely. Drive a 0.035-inch or 0.045-inch Kirschner wire obliquely across the joint to maintain the reduction.
- Alternatively, a transarticular wire can be driven retrograde through the tip of the distal phalanx, across the DIP joint, and into the middle phalanx. Ensure the wire engages the subchondral bone of the middle phalanx for maximum purchase.
- Confirm anatomic reduction and hardware placement with orthogonal fluoroscopic views.
Salvage Pathway: If, upon surgical exploration, the articular surface of the joint is found to be completely destroyed, comminuted beyond repair, or devoid of cartilage, primary arthrodesis of the DIP joint should be performed immediately to prevent chronic, debilitating pain.
5. Specialized Technique: Pull-Out Wire for Type 4 Mallet Fingers
For large dorsal articular fractures (Type 4B/4C) with volar subluxation, a pull-out wire technique combined with transarticular pinning is highly effective.

FIGURE 67-66 A: Type 4 bony mallet finger in a high-demand athlete, demonstrating a large dorsal fragment and volar subluxation of the distal phalanx.
- Technique: A small dorsal incision is made over the DIP joint. The fracture is identified. A fine wire (or non-absorbable suture) is passed through the terminal tendon just proximal to the bony fragment using a Bunnell or Krackow weave.
- The two ends of the wire are passed through drill holes in the distal phalanx, exiting the volar pulp.
- The joint is reduced, and a transarticular K-wire is placed to hold the DIP joint in neutral extension.
- The pull-out wire is then tensioned and tied over a padded button on the volar pulp, compressing the dorsal fragment into its anatomic bed.




FIGURE 67-66 B: Radiographic results of the pull-out wire and transarticular pin fixation of the distal interphalangeal joint, demonstrating anatomic restoration of the articular surface. Images taken just before pin removal at 4 weeks.

FIGURE 67-66 C: The pull-out wire is typically left in place until 6 weeks after surgery to ensure complete bony union before dynamic stress is applied.
POSTOPERATIVE CARE AND REHABILITATION
The success of DIP joint fixation relies heavily on strict adherence to postoperative protocols.
- Immediate Postoperative Phase (0-2 Weeks):
- The finger is placed in a protective volar splint.
- Elevation is encouraged to minimize edema.
- At 2 weeks, skin sutures are removed. The K-wire (if left protruding) is inspected for signs of pin-tract infection.
- Intermediate Phase (2-6 Weeks):
- For simple oblique K-wire fixation of non-tendinous fractures, the wire can often be removed at 3 to 4 weeks, and active motion is begun.
- For transarticular pins protecting a tendon repair or a Type 4 bony mallet, the pin is maintained for 4 to 6 weeks.
- Pull-out wires are generally removed at 6 weeks.
- Late Phase (6+ Weeks):
- Once pins are removed, active range of motion (AROM) exercises are initiated.
- Night splinting may be recommended for an additional 2 to 6 weeks to prevent an extensor lag.
- Passive flexion is introduced gradually, avoiding forceful manipulation that could rupture the healing extensor mechanism.
COMPLICATIONS AND PITFALLS
Operative treatment of the DIP joint is technically demanding and carries a distinct complication profile:
- Infection: Pin-tract infections are common. Meticulous pin care and early oral antibiotics for erythema are required. Deep joint space infections are catastrophic and require immediate hardware removal and washout.
- Nail Deformity: Iatrogenic injury to the germinal matrix during pin placement or surgical approach will result in permanent ridging or splitting of the nail.
- Loss of Reduction: Often due to premature pin removal or inadequate initial fixation. May require revision surgery or acceptance of the deformity.
- Tender Pulp Scars: Volar incisions or overly tight pull-out buttons can cause chronic pain in the highly innervated digital pulp.
- Post-Traumatic Osteoarthritis: Even with anatomic reduction, cartilage damage at the time of injury can lead to late-onset arthritis. Painful chronic mallet fingers resulting from fracture-dislocations that fail conservative or initial operative management are best treated with definitive DIP joint arthrodesis.
