- Nutritional rickets (see Table 1.16)
- Vitamin D–deficiency rickets
- Rare after addition of vitamin D to milk, except in the following populations:
- Asian immigrants
- Patients with dietary peculiarities
- Premature infants
- Patients with malabsorption (celiac sprue)
- Patients receiving long-term parenteral nutrition
- Decreased intestinal absorption of calcium and phosphate leads to secondary hyperparathyroidism.
- Laboratory findings
-
Low-normal calcium level (maintained by high PTH level)
-
Low phosphate level (excreted because of the effect of PTH)
-
Increased alkaline phosphatase level
-
Low vitamin D level
-
Increased PTH level leads to higher bone absorption
- Physical examination
- Enlargement of the costochondral junction (rachitic rosary)
- Bowing of the knees
- Muscle hypotonia
- Dental disease
- Pathologic fractures (Looser zones: pseudofractures on the compression sides of bones)
- Milkman’s fracture
- Waddling gait
- Radiographic findings
-
Physeal widening and cupping
- Coxa vara
- Codfish vertebrae
- Retarded bone growth (defect in the hypertrophic zone, widened osteoid seams)
- In affected children, height is commonly below the fifth percentile for age.
-
Treatment with vitamin D (1000–6000 IU daily
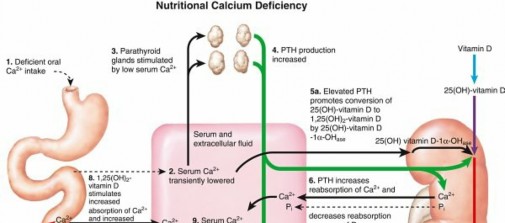
based on weight) resolves most deformities. - Calcium-deficiency rickets ( Fig. 1.19)
- Phosphate-deficiency rickets
- Hereditary vitamin D–dependent rickets
- Rare disorders with features similar to those of vitamin D–deficiency (nutritional) rickets, except that symptoms may be worse and patients may have total baldness
-
Type I: defect in renal 25(OH)D 1α-
hydroxylase, inhibiting conversion of inactive vitamin D to its active form
- Autosomal recessive inheritance
- Gene on chromosome 12q14
- Type II: defect in an intracellular receptor for 1,25(OH)2D3
- Familial hypophosphatemic rickets (vitamin D–resistant rickets or phosphate diabetes)
- Most commonly encountered form of rickets
-
X-linked dominant inheritance


FIG. 1.19 Nutritional calcium deficiency. From Netter FH: CIBA collection of medical illustrations, vol 8: Musculoskeletal system, part I: Anatomy, physiology and developmental disorders, Basel, Switzerland, 1987, CIBA, p 184. - Impaired renal tubular reabsorption of phosphate
- Normal GFR with an impaired vitamin D3 response
- Normal serum calcium, low serum phosphorus and 1, (OH)2D3, and high serum alkaline phosphatase levels
- Treatment:
- First line treatment with burosumab (anti-FGF23 monoclonal antibody)
- Second line elemental phosphate (1–2 g/day plus vitamin D 0.5–1 µg/day)
- Hypophosphatasia
- Autosomal recessive
- Error in the tissue-nonspecific isoenzyme of alkaline phosphatase
-
Leads to low levels of alkaline phosphatase, which is required for
synthesis of inorganic phosphate (Pi) and important in bone matrix formation - Features are similar to those of rickets.
- Increased urinary phosphoethanolamine is diagnostic.
-
Treatment may include phosphate therapy.
Table 1.15 Laboratory Findings and Clinical Data Regarding Patients Changes in Level or Concentration
---
Disorder Serum Serum Alka Calcium Phosphastase Phos Hypopara-thyroidism
| ↓
| ↑
| Non Pseudohypoparathyroidism | ↓
| ↑
| Non Renal osteodystrophy (high-turnover bone disease resulting from renal disease [secondary hyperparathyroidism]) | ↓ or
none
| ↑↑↑
| ↑
| |
| ---|---|---|--- Renal osteodystrophy | ↑ or
none
| None or ↑
| ↑ (low-turnover bone | | disease due to renal | | disease [aluminum | | toxicity]) | |
↓, Decreased; ↑, increased.
Table 1.16 Laboratory Findings and Clinical Data Regarding Patients Changes in Level or Concentration --- Disorder Serum Serum Alkaline PTH Calcium Phos phos Nutritional rickets: vitamin D deficiency | ↓ or
none
| ↓
| ↑
| ↑
| |
| |
| ---|---|---|---|---|
Nutritional rickets: calcium deficiency
| ↓ or
none
| ↓
| ↑
| ↑
Nutritional rickets: phosphate deficiency
| None
| ↓
| ↑
| None
Hereditary vitamin D–dependent rickets type I (pseudo–vitamin D deficiency)
| ↓
| ↓
| ↑
| ↑
Hereditary vitamin D–dependent rickets type II [hereditary resistance to 1,25(OH) 2D]
| ↓
| ↓
| ↑
| ↑ Hypophosphatemic rickets (also known as vitamin D–resistant rickets and phosphate diabetes; Albright syndrome is an example of a | None
| ↓↓↓
| ↑
| None
hypophosphatemic syndrome)
| |
| |
| ---|---|---|---|---|
Hypophosphatasia
| ↑
| ↑
| ↓↓↓
| None
↓, Decreased; ↑, increased;
phos,
phosphatase.
Table 1.17 Differential Diagnosis of Metabolic Bone Diseases Based Calcium Level --- Increased | Decreased Primary | Hypoparathyroidism Pseudohypoparathyr Renal osteodystrophy (high-turnover bo
disease) Nutritional rickets: vi
D deficiency Nutritional rickets: ca
deficiency Hereditary vitamin D
dependent rickets (types I and II)
Malignancy with bon metastasis
Malignancy without metastasis
Multiple myeloma Lymphoma Hyperthyroidism Vitamin D intoxicatio Sarcoidosis
Milk-alkali syndrome Severe generalized
immobilization
hyperparathyroidism Hyperthyroidism Vitamin D intoxication Malignancy without bony metastasis Malignancy with bony metastasis Multiple myeloma Lymphoma Sarcoidosis Milk-alkali syndrome Severe generalized immobilization Multiple endocrine neoplasias Addison disease Steroid administration Peptic ulcer disease Hypophosphatasia Pseudohypoparathyroidism Renal osteodystrophy Nutritional rickets: vitamin D deficiency Nutritional rickets: calcium deficiency Hereditary vitamin D– dependent rickets (types I and II)
