Nontraumatic Soft-Tissue Disorders
The surgical treatment of nontraumatic abnormalities affecting muscles, tendons, tendon sheaths, fascia, and bursae requires a profound understanding of soft-tissue biomechanics and pathophysiology. The etiology of these disorders is multifactorial, encompassing degenerative cascades, developmental anomalies, repetitive microtrauma, or a synergistic combination of these factors. While many of these conditions are frequently encountered in outpatient orthopedic practice and respond favorably to conservative modalities—such as structured physical therapy, cryotherapy, thermotherapy, extremity elevation, and targeted pharmacotherapy (local or systemic anti-inflammatory medications)—a distinct subset of fibrotic contractures mandates meticulous surgical intervention to restore function and prevent irreversible articular degradation.
Pathophysiology of Muscle Contractures
Muscle contractures can manifest in virtually any myotendinous unit. The underlying etiology may be obscure, as observed in congenital contractures, or explicitly identifiable, such as in cases of deep-seated infection, ischemic necrosis, direct trauma, or injection myositis.
Injection-induced fibrosis is a well-documented iatrogenic pathology. It most frequently afflicts the quadriceps femoris complex but has also been extensively described in the gluteal, deltoid, and triceps musculature. In the pediatric population, these contractures often emerge as a delayed sequela of intramuscular antibiotic administration during infancy. In the adult demographic, profound multifocal fibrosis and severe contractures are frequently associated with the chronic, addictive intramuscular injection of pentazocine (Talwin) or other myotoxic agents. The pathogenesis involves a combination of direct chemical myotoxicity and localized ischemic necrosis secondary to the volume of the injected bolus compressing delicate capillary networks within the muscle bundles. This dual insult triggers a robust inflammatory cascade, culminating in fibroblastic proliferation and the replacement of contractile muscle fibers with dense, inelastic collagenous scar tissue.
Clinical Pearl: Always maintain a high index of suspicion for injection myositis in patients presenting with painless, progressive loss of joint motion and a history of frequent intramuscular injections or substance abuse. The fibrotic process can continue to evolve for years after the cessation of the offending injections.
Quadriceps Contracture of Infancy and Childhood
Etiology and Clinical Presentation
The etiology of quadriceps contracture is broadly categorized into congenital and acquired types, with some clinical presentations exhibiting a hybrid of both. Historically, Hnevkovsky characterized this pathology as "progressive fibrosis of the vastus intermedius muscle in children." Familial and genetic predispositions have been suggested; Fairbank and Barrett documented identical twins with congenital quadriceps contractures, while Nozawa et al. reported familial occurrences and postulated a higher epidemiological incidence in patients of central and eastern Asian descent.
Conversely, the acquired form is predominantly iatrogenic. Lloyd-Roberts and Thomas, alongside Sengupta, definitively linked infantile quadriceps contractures to multiple intramuscular injections or infusions administered into the anterolateral thigh shortly after birth. Sengupta’s seminal series of 33 children (52 extension contractures) highlighted the profound functional deficits: an inability to squat or sit on the floor, accompanied by a highly unstable, compensatory quadriceps gait.
The clinical hallmark of quadriceps contracture is a progressive, painless limitation of knee flexion. As the child grows, the unyielding fibrotic tether creates a severe biomechanical mismatch. This can lead to:
* Hyperextension and subluxation of the knee joint.
* Absence of normal transverse skin creases over the anterior knee.
* A pathognomonic cutaneous "dimple" overlying the epicenter of the fibrotic mass, which becomes highly accentuated during forced knee flexion.
* Habitual or obligatory dislocation of the patella due to lateral vector forces from a fibrotic vastus lateralis or iliotibial band.
If left untreated, the chronic abnormal joint reaction forces precipitate severe secondary skeletal changes. Jackson and Hutton described the triad of patella alta, fragmentation of the inferior patellar pole, and global patellar hypoplasia. In neglected cases, older children will exhibit flattening of the femoral condyles, severe genu recurvatum, anterior subluxation of the tibia, and premature, gross degenerative osteoarthritis.
Classification of Quadriceps Contractures
The Ad Hoc Committee of the Japanese Orthopaedic Association (JOA) for Muscular Contractures established a highly pragmatic classification system based on the physical examination of the patient in the prone position. This classification dictates the surgical approach by identifying the specific muscular components involved.
Table: JOA Quadriceps Contracture Classification
- Rectus Femoris Type: Knee flexion is restricted when the hip is extended. When the knee is forced into flexion, the hip is obligatorily forced to flex (positive Ely's test equivalent).
- Vastus Type: Knee flexion is restricted regardless of hip position. When the knee is forced into flexion, the hip position remains unchanged.
- Mixed Type: Knee flexion is slightly restricted with hip extension, and forced knee flexion causes obligatory hip flexion, indicating involvement of both the biarticular rectus femoris and the uniarticular vasti.
Surgical Indications and Principles
Early recognition is paramount. While passive stretching protocols are crucial for prevention in infants receiving IM injections, established scar contractures are refractory to conservative management. Surgical release is definitively indicated to halt the progression of deformity and prevent irreversible architectural changes to the femoral condyles and patellofemoral joint. Early intervention is particularly critical in patients exhibiting habitual patellar dislocation.
Nicoll delineated the four primary pathological components that must be addressed during surgical reconstruction:
1. Dense fibrosis of the vastus intermedius, which tethers the rectus femoris to the anterior femur and obliterates the suprapatellar pouch.
2. Intra-articular adhesions binding the patella to the femoral trochlea and condyles.
3. Fibrosis and contracture of the lateral and medial retinacular expansions of the vasti, adhering them to the condyles.
4. True structural shortening of the rectus femoris muscle belly.
For early-stage contractures lacking significant intra-articular degenerative changes, Sengupta advocates for a proximal release. This approach effectively eliminates extensor lag and minimizes the risk of postoperative hemarthrosis. In advanced cases with profound fibrosis, a distal Thompson-type quadricepsplasty is required. If severe genu recurvatum has already developed, a supracondylar femoral osteotomy may be necessary to restore a functional arc of motion.
Surgical Warning: Sasaki et al. noted that surgical outcomes tend to deteriorate over time if performed too early. They recommend delaying definitive surgical release until the child is at least 6 years of age, provided that severe secondary bony changes are not rapidly progressing.
Operative Techniques for Quadriceps Contracture
Proximal Release of the Quadriceps (Sengupta Technique)
This technique is highly effective for moderate contractures before the onset of significant bony deformity. It focuses on releasing the proximal tethers while preserving the distal extensor mechanism to prevent postoperative extension lag.
Step-by-Step Surgical Technique:
- Positioning and Incision: Place the patient supine with a bump under the ipsilateral hip. Make a sweeping, curved incision beginning at the base of the greater trochanter and extending vertically downward along the lateral aspect of the thigh. The distal extent is dictated by the palpable limits of the fibrotic mass.
- Iliotibial Band Release: Deepen the incision through the subcutaneous tissues. Identify the iliotibial band (ITB) in the proximal aspect of the wound. The ITB is frequently hypertrophied and fibrotic, acting as a major secondary tether. Section the ITB transversely to relieve the lateral tension.
- Vastus Lateralis Mobilization: Expose the proximal origin of the vastus lateralis just inferior to the greater trochanter. Meticulously detach the origin of the vastus lateralis from the intertrochanteric line and continue the release distally along the lateral intermuscular septum.
- Vastus Intermedius Release: As the vastus lateralis is mobilized and retracted anteriorly, the underlying vastus intermedius is exposed. This muscle is typically replaced by a dense, glistening sheet of fibrous tissue.
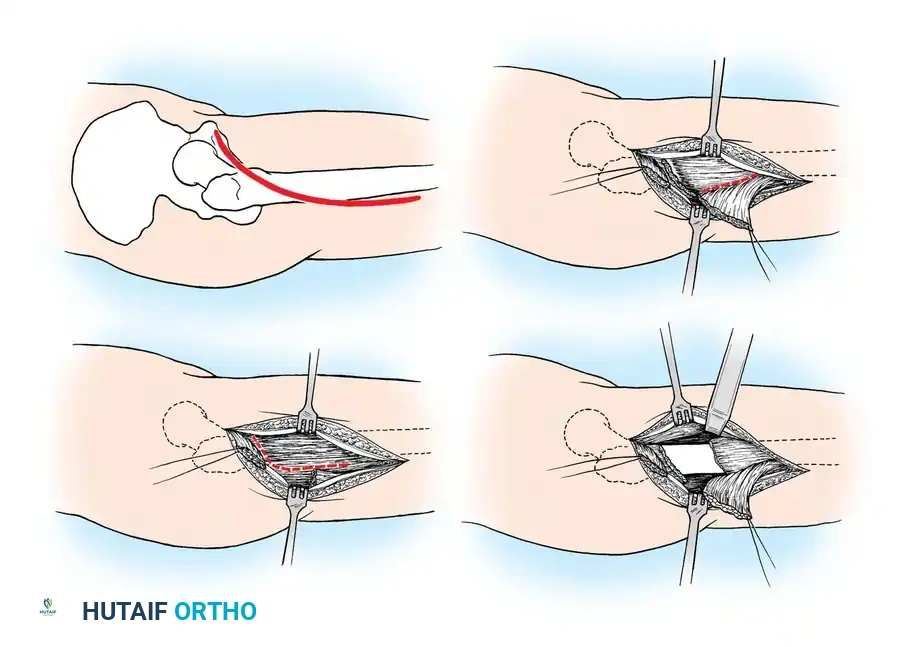
- Femoral Stripping: Utilizing a broad periosteal elevator, systematically elevate and release the fibrotic vastus intermedius from the anterior surface of the femoral shaft. Proceed from proximal to distal until the suprapatellar pouch is reached.
- Dynamic Assessment: Gently flex the knee to assess the gain in motion and to identify any residual adhesive bands.
- Rectus Femoris Release (If Indicated): If the JOA classification indicates a Mixed or Rectus type contracture, the rectus femoris must be addressed. Expose its origin at the anterior inferior iliac spine (AIIS) through the proximal extent of the incision.
- Crucial Step: Identify and meticulously retract the branches of the femoral nerve before detaching the rectus origin.
- Closure: Full knee flexion should now be achievable. Capsulotomy is rarely required in pediatric patients. Achieve meticulous hemostasis, close the wound in layers over a suction drain, and apply a posterior plaster splint with the knee positioned in maximal safe flexion.
Postoperative Protocol (Sengupta):
The splint is maintained until acute postoperative tenderness subsides (typically 3 to 4 weeks). Following splint removal, an aggressive, supervised physical therapy regimen focusing on active quadriceps strengthening and passive flexion is initiated. Extension lag typically resolves rapidly. Patients are usually ambulatory by 4 weeks and can perform a full squat by 3 months. Night splinting and daily stretching must continue until skeletal maturity to prevent recurrence.
Thompson-Type Quadricepsplasty (Technique 24-2)
Reserved for severe, recalcitrant cases with extensive distal fibrosis.
Step-by-Step Surgical Technique:
- Hemostasis: Utilize an electrocoagulation unit extensively throughout the procedure, as the release of dense scar tissue can result in significant diffuse bleeding.
- Incision: Utilize an anterior longitudinal incision extending from the proximal third of the anterior thigh down to the distal pole of the patella. Incorporate or excise previous injection scars if possible.
- Fascial Release: Divide the deep investing fascia longitudinally along both the medial and lateral borders of the rectus femoris. Carefully develop the planes to separate the rectus femoris from the adjacent vastus medialis and vastus lateralis.
- Retinacular Release: Divide the anterior joint capsule and the fibrotic lateral and medial expansions of the vasti on both sides of the patella. Extend this release proximally enough to completely overcome the retinacular contracture.
- Excision of Vastus Intermedius: The vastus intermedius is typically found as a dense, avascular scarred band binding the posterior surface of the rectus femoris directly to the anterior femur. Do not simply release it; excise the fibrotic vastus intermedius completely to prevent readherence.
- Closure and Rehabilitation: Close the subcutaneous tissue and skin. Postoperative management historically involved casting, but modern protocols favor the immediate use of Continuous Passive Motion (CPM) machines to maintain the intraoperative gains in flexion while preventing intra-articular adhesion formation.
Deltoid Contracture
Etiology and Pathomechanics
Deltoid contracture is an analogous fibrotic disorder, predominantly occurring as a sequela of repeated intramuscular injections into the shoulder. While congenital cases exist, they are exceedingly rare. The pathogenesis mirrors that of quadriceps contracture, where myotoxic drugs and volume-induced ischemia lead to focal muscle necrosis and subsequent replacement by dense collagenous cords.
Patients typically present with a progressive, painless abduction contracture of the shoulder. Clinical hallmarks include:
* Inability to adduct the arm to the side of the torso.
* Prominent dimpling of the skin overlying the deltoid during attempted adduction.
* Compensatory winging of the scapula.
* Chronic, aching pain around the neck and shoulder girdle due to altered scapulothoracic kinematics and muscle fatigue.
Magnetic Resonance Imaging (MRI) is the gold standard for preoperative planning. It typically demonstrates a distinct, low-signal fibrotic cord residing within the substance of the deltoid muscle, extending from the superior surface of the acromion down to the deltoid tuberosity on the lateral humerus.
Surgical Management
Surgical intervention is indicated for patients with significant cosmetic deformity, functional impairment, or intractable pain who have failed a comprehensive, prolonged physical therapy program.
Historically, proximal release at the acromial origin was performed; however, this approach is fraught with complications, including prominent scarring, incomplete release, and potential injury to the terminal branches of the axillary nerve.
Contemporary evidence strongly supports a distal surgical release. Ko et al. and Chen et al. demonstrated superior clinical outcomes, improved shoulder kinematics, and significantly decreased wound complication rates utilizing the distal approach.
Principles of Distal Deltoid Release:
1. A longitudinal incision is made over the distal aspect of the deltoid, centered over the palpable fibrotic band near the deltoid tuberosity.
2. The deep fascia is incised, and the fibrotic cord is isolated from the surrounding healthy muscle fibers.
3. A transverse or Z-lengthening release of the fibrotic cord is performed just proximal to its insertion on the humerus.
4. The arm is brought into full adduction across the chest to ensure complete release of all tethering bands.
5. Immediate postoperative physical therapy is instituted to maintain adduction and restore normal glenohumeral and scapulothoracic rhythm. In the series by Ko et al., 96% of patients achieved a good or excellent clinical result with this immediate mobilization protocol.
Congenital Torticollis
Congenital torticollis represents a specific manifestation of muscle contracture, characterized by traumatic or ischemic fibrosis of the sternocleidomastoid muscle. This condition results in a complex rotational and lateral flexion deformity of the cervical spine. The pathophysiology, clinical evaluation, and specialized surgical lengthening techniques (such as bipolar release or Z-plasty of the sternocleidomastoid) require distinct considerations and are discussed comprehensively in dedicated pediatric orthopedic literature (see Chapter 28).
📚 Medical References
- Chen CK, Yeh L, Chen CT, et al: Contracture of the deltoid muscle: imaging fi ndings in 17 patients, AJR Am J Roentgenol 170:449, 1998.
- Chen WJ, Wu CC, Lin YH, et al: Treatment of deltoid contracture in adults by distal release of the deltoid, Clin Orthop Relat Res 378:136, 2000.
- Fairbank TJ, Barrett AM: Vastus intermedius contracture in early childhood, J Bone Joint Surg 43B:326, 1961.
- Hnevkovsky O: Progressive fi brosis of the vastus intermedius muscle in children: a cause of limited knee fl exion of the patella, J Bone Joint Surg 43B:318, 1961.
- Jackson AM, Hutton PAN: Injection-induced contractures of the quadriceps in childhood: a comparison of proximal release and distal quadricepsplasty, J Bone Joint Surg 67B:97, 1985.
- Ko JY, An KN, Yamamoto R: Contracture of the deltoid muscle: results of distal release, J Bone Joint Surg 80A:229, 1998.
- Lloyd-Roberts GC, Thomas TG: The etiology of quadriceps contracture in children, J Bone Joint Surg 46B:498, 1964.
- Milcan A, Eskandari MM, Öztuna V, et al: Injection-induced contracture of the quadriceps femoris muscle in children, Orthopedics 27:65, 2004.
- Nicoll EA: Quadricepsplasty, J Bone Joint Surg 45B:483, 1963.
- Nozawa S, Tanaka C, Shikata J, et al: Congenital contracture of the quadriceps muscle: a case report with magnetic resonance imaging, Arch Orthop Trauma Surg 124:272, 2004.
- Sasaki T, Fukuhara H, Iisaka H, et al: Postoperative evaluation of quadriceps contracture in children: comparison of three different procedures, J Pediatr Orthop 5:702, 1985.
- Sengupta S: Pathogenesis of infantile quadriceps fi brosis and its correction by proximal release, J Pediatr Orthop 5:187, 1985.
- Thompson TC: Quadricepsplasty to improve knee function, J Bone Joint Surg 26:366, 1944.
