NONOPERATIVE MANAGEMENT
The management of the upper extremity in cerebral palsy (CP) is highly complex, requiring a nuanced understanding of dynamic spasticity versus fixed myostatic contracture. Traditionally, early and aggressive splinting was universally employed to prevent fixed contractures of the muscles and joints. However, contemporary evidence-based practice has largely abandoned continuous rigid splinting. Fixed contractures rarely occur in very young children, and during sleep, the upper extremity often relaxes, becoming supple and obviating the need for cumbersome night splinting.
Daytime splinting is frequently rejected by active children due to its restrictive nature. If splinting is deemed necessary—primarily to maintain joint alignment or stretch specific muscle groups—a well-formed, custom-molded orthosis without pressure points should be utilized. The splint should hold the wrist in as much extension as tolerated, with the fingers in almost complete extension and the thumb abducted out of the palm.


Hand Therapy and Modalities
Hand therapy is a cornerstone of nonoperative care. Although rarely successful in training a child to voluntarily relax spastic muscles, targeted therapy strengthens weakened antagonistic muscles and helps control exaggerated reflexes. Furthermore, therapy is invaluable in providing psychosocial support to the patient and family, evaluating patients for potential surgical procedures, and guiding postoperative recovery of functional activities.
Electrical stimulation, aimed at strengthening nonspastic but weak extensor compartment muscles, may have a role in nonoperative management, though literature yields conflicting results. Scheker and Ozer reported functional improvement when electrical stimulation was used in conjunction with dynamic splinting; however, they emphasized the necessity of lifelong application to maintain gains.
Neuromodulation: Botulinum Toxin Type A
Interest in the use of botulinum toxin type A (BoNT-A) in the treatment of cerebral palsy has increased exponentially. By temporarily blocking acetylcholine release at the neuromuscular junction, BoNT-A decreases spasticity, which helps improve the control of movement patterns. This is achieved through a combination of functionally lengthening spastic muscle groups, improving posture, and allowing the strengthening of antagonistic muscles.
Clinical Pearl: BoNT-A serves as both a therapeutic modality and a diagnostic tool. A positive response to an injection can help the surgeon differentiate between dynamic spasticity (which will improve) and a fixed myostatic contracture (which will not), thereby guiding future surgical decision-making.
While several studies have shown promising short-term results, long-term functional improvement remains debated. Chin and Graham reported dramatic initial improvement, but lasting results were observed in only 3% to 5% of children. Approximately 70% of children showed improvement that lasted only 6 to 9 months. The most common reasons for failure include unrecognized fixed joint contractures, absence of selective motor control in antagonist muscles, profound sensory impairment, and learned nonuse.
OPERATIVE MANAGEMENT
Surgical Goals and Expectations
The goals of operative treatment in a child with cerebral palsy must be highly specific, realistic, and tailored to the individual. Surgery should primarily be aimed at providing useful grasp and release mechanisms and facilitating acceptable hygiene.




In severely involved patients, improving the appearance of the hand by correcting an unsightly contracture or allowing the palm to be opened for washing may be a modest but highly impactful goal. Fine manipulation is rarely improved by surgery, and achieving "normal" hand function is an unrealistic expectation that must be clearly communicated to the family.
Grasp and release are possible only in children who possess sufficient sensibility to allow an awareness of the extremity. Interestingly, stereognosis has been shown to improve with postoperative gains in motor function and functional use of the upper extremity.
Surgical Warning: Undercorrection rather than overcorrection of the deformity or dysfunction is always preferred. Over-lengthening a spastic flexor can lead to a devastating loss of grip strength, rendering the hand functionally useless.
Principles of Patient Selection
The ideal candidate for surgery is a patient with spastic hemiplegia who is cooperative, intelligent, well-motivated, and who already possesses a rudimentary pattern of grasp and release. The hand should be reasonably sensitive.
Conversely, a poor candidate for functional surgery is a patient who is severely cognitively impaired, exhibits definite athetosis or dystonia, possesses an insensitive hand with rigid joint contractures, or has a wrist that cannot be passively brought to neutral. Children with spastic diplegia rarely have sufficient upper extremity spasticity to warrant surgery, while those with spastic quadriplegia or total body involvement typically lack the voluntary control necessary to benefit from grasp-and-release reconstructions. However, the latter group may still benefit from hygiene-focused procedures.
Surgical Timing and Options
Surgical options include myotomy, tenotomy, tendon lengthening, tendon transfer, tenodesis, capsulotomy, excisional arthroplasty, and arthrodesis.
* Tendon Lengthening: Requires minimal postoperative compliance and can be performed in spastic and athetoid patients. It weakens the muscle, diminishes its excursion, and reduces the stretch reflex, allowing antagonistic muscles to function better.
* Tendon Transfers: Require strict postoperative compliance, must be synergistic, cannot overcome fixed deformities, and are highly unreliable in athetoid patients.
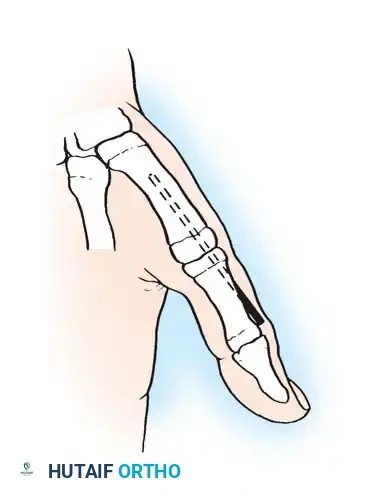
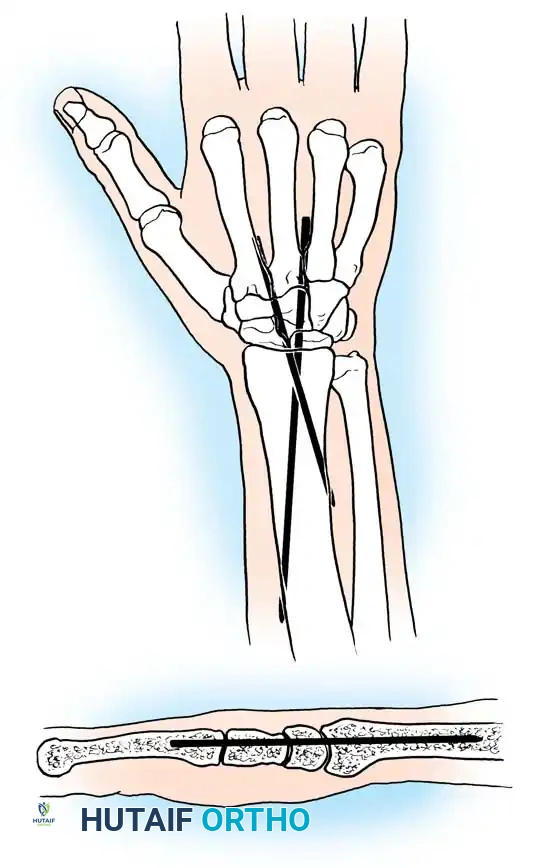
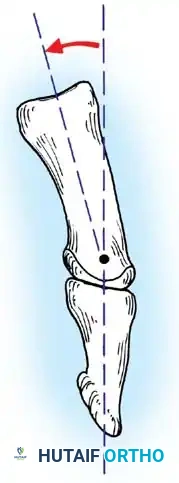
* Arthrodesis: Useful for stabilizing the thumb metacarpophalangeal (MCP) joint during thumb-in-palm reconstruction or correcting fixed wrist flexion deformities when sacrificing the "windlass" effect is justifiable.
Indicated surgery is usually carried out between 4 to 8 years of age, ideally before significant fixed contractures develop. Soft-tissue operations to correct flexion deformity of the wrist and pronation deformity of the forearm are typically indicated earliest.
The House Classification of Functional Use
House et al. developed a validated classification for upper extremity functional use in cerebral palsy. Van Heest, House, and Cariello utilized this system to review 134 patients undergoing 718 procedures. Surgical intervention yielded an average improvement of 2.6 functional levels, independent of mentation, 2-point discrimination, stereognosis, or CP subtype. The only reliable predictor of outcome was voluntary motor control: patients with poor voluntary control exhibited less improvement than those with fair-to-good control.
Table 69-1: Upper Extremity Functional Use (House et al.)
* Level 0: Does not use.
* Level 1 (Poor passive assist): Uses as stabilizing weight only.
* Level 2 (Fair passive assist): Can hold object placed in hand.
* Level 3 (Good passive assist): Can hold object and stabilize it for use by other hand.
* Level 4 (Poor active assist): Can actively grasp object and hold it weakly.
* Level 5 (Fair active assist): Can actively grasp object and stabilize it well.
* Level 6 (Good active assist): Can actively grasp object and manipulate it.
* Level 7 (Spontaneous use, partial): Can perform bimanual activities and occasionally uses the hand spontaneously.
* Level 8 (Spontaneous use, complete): Uses hand completely independently.
PRONATION CONTRACTURE OF THE FOREARM
Pronation deformity of the forearm is a common and disabling manifestation of CP, driven primarily by spasticity of the pronator teres and, occasionally, the pronator quadratus. This deformity can be paradoxically aggravated by lengthening the biceps tendon for an elbow flexion contracture.
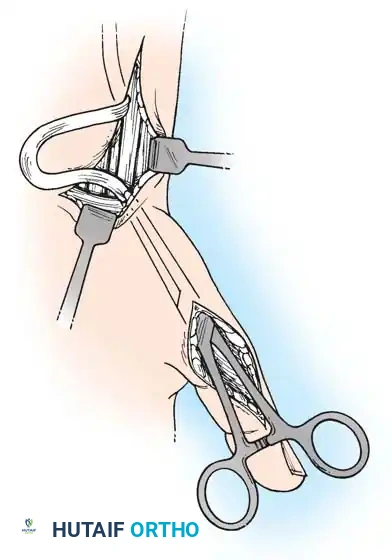
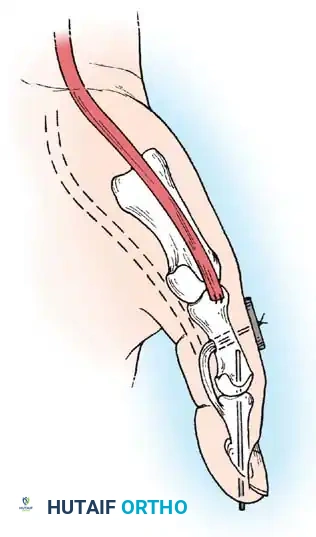
Mild deformities may be improved by simple tenotomy of the pronator teres insertion. If a contracted biceps aponeurosis (lacertus fibrosus) is present, its division may further improve supination. Supination can also be augmented by transferring the flexor carpi ulnaris (FCU) around the ulnar border of the forearm to the extensor digitorum communis (EDC) or extensor carpi radialis brevis (ECRB).
Gschwind Classification and Surgical Algorithm
Gschwind and Tonkin classified pronation deformities into four distinct groups to guide surgical decision-making:
Table 69-2: Gschwind Classification of Pronation Deformities
* Group 1: Active supination beyond neutral. Recommendation: No specific surgery.
* Group 2: Active supination to or less than neutral. Recommendation: Pronator quadratus release ± flexor aponeurotic release.
* Group 3: No active supination, yet free passive supination. Recommendation: Pronator teres rerouting procedure.
* Group 4: No active supination and limited passive supination. Recommendation: Pronator quadratus release and flexor aponeurotic release. (If active supination remains impossible, add pronator teres rerouting).
Pitfall: Gschwind et al. caution against performing a pronator teres transfer simultaneously with a pronator quadratus release, as an undesirable, irreversible supination deformity may ensue.
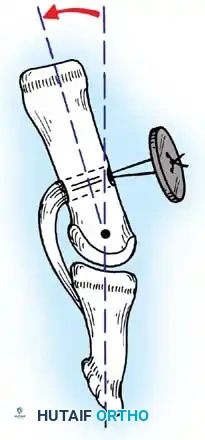
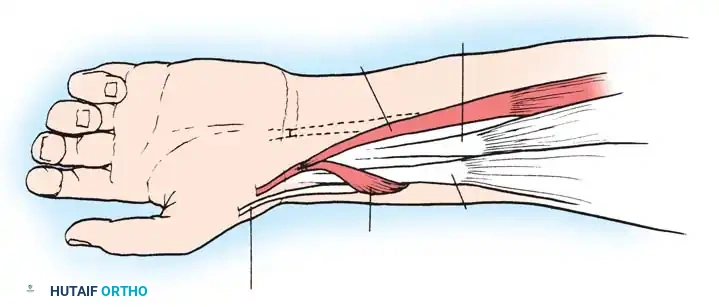
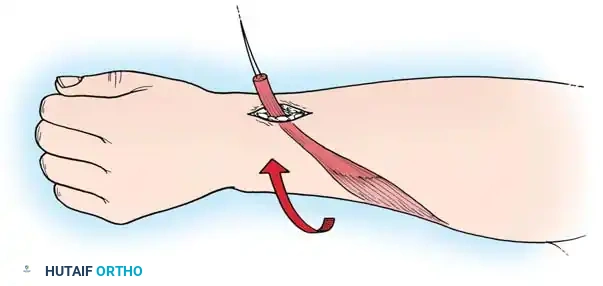
Technique 69-1: Transfer of the Pronator Teres (Sakellarides et al.)
Sakellarides et al. demonstrated that transferring the pronator teres tendon produces superior correction by eliminating a deforming force while simultaneously providing an active force for supination.
Surgical Steps:
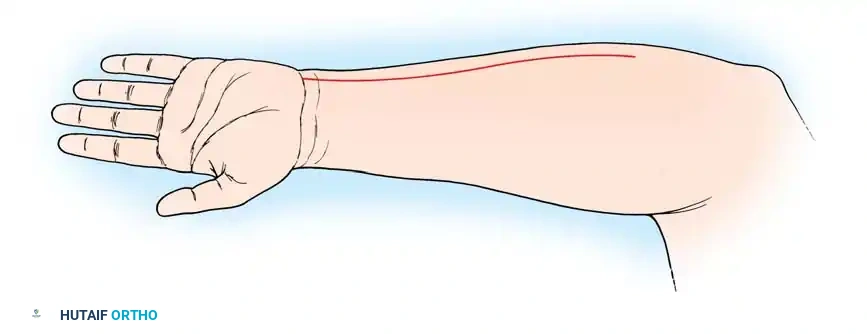
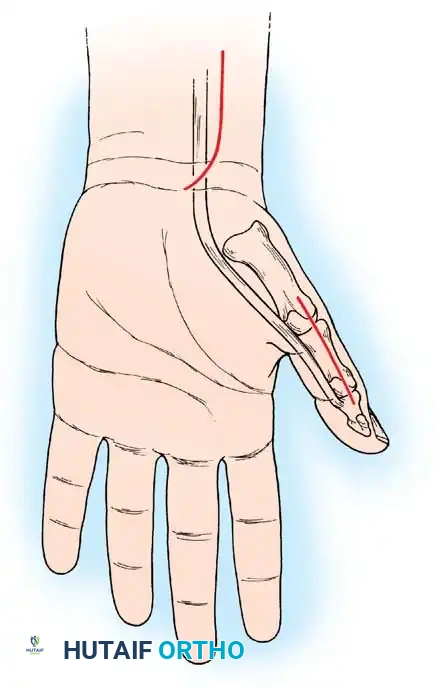
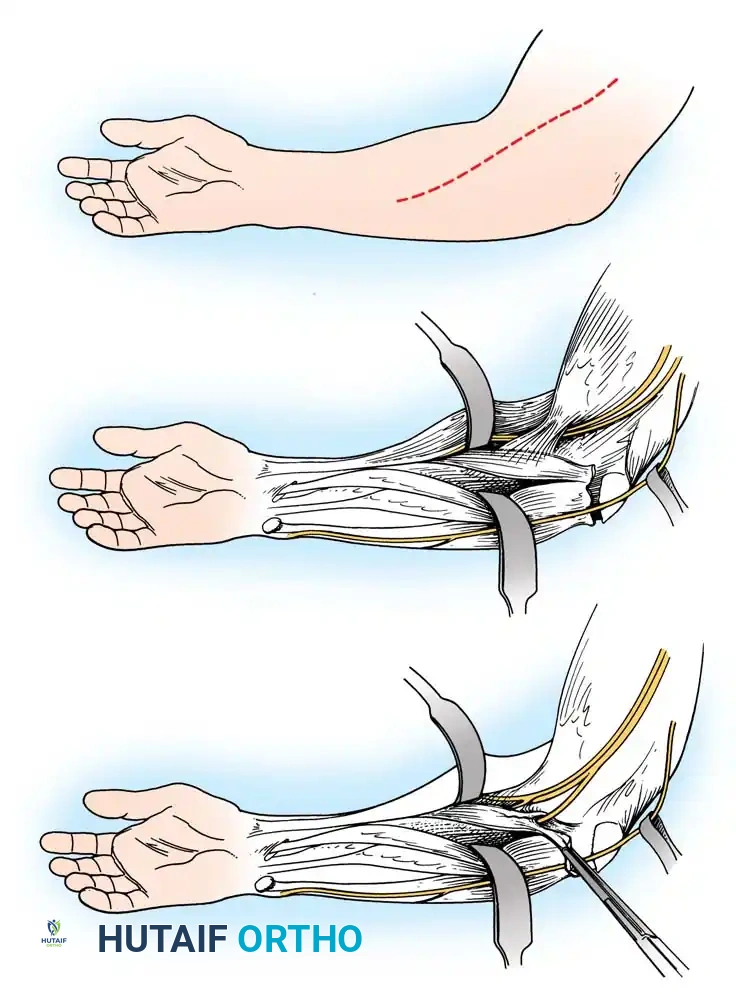
1. Incision: Make a zigzag, curvilinear, or straight longitudinal incision over the anterior and radial aspects of the midforearm, centered over the insertion of the pronator teres.
2. Nerve Protection: Meticulously identify and protect the lateral antebrachial cutaneous nerve and the superficial branch of the radial nerve.
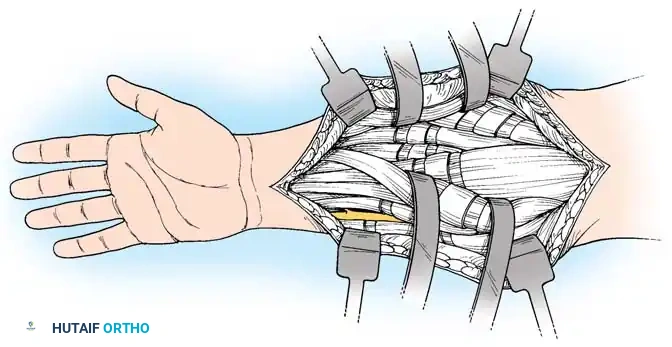
3. Exposure: Develop the interval between the brachioradialis and the extensor carpi radialis longus (ECRL).
4. Detachment: Identify the oblique fibers inserting into the bone at the musculotendinous junction of the pronator teres. Use sharp dissection to detach the insertion along with an attached strip of periosteum to maximize length.
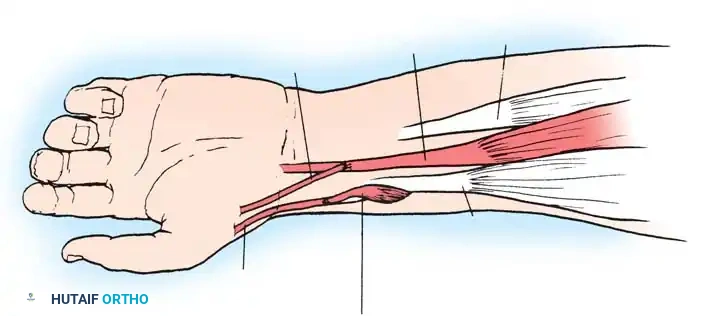
5. Mobilization: Mobilize the muscle extraperiosteally, well proximal into the forearm. Free the interosseous membrane from the radius as far as necessary to achieve maximum passive supination.
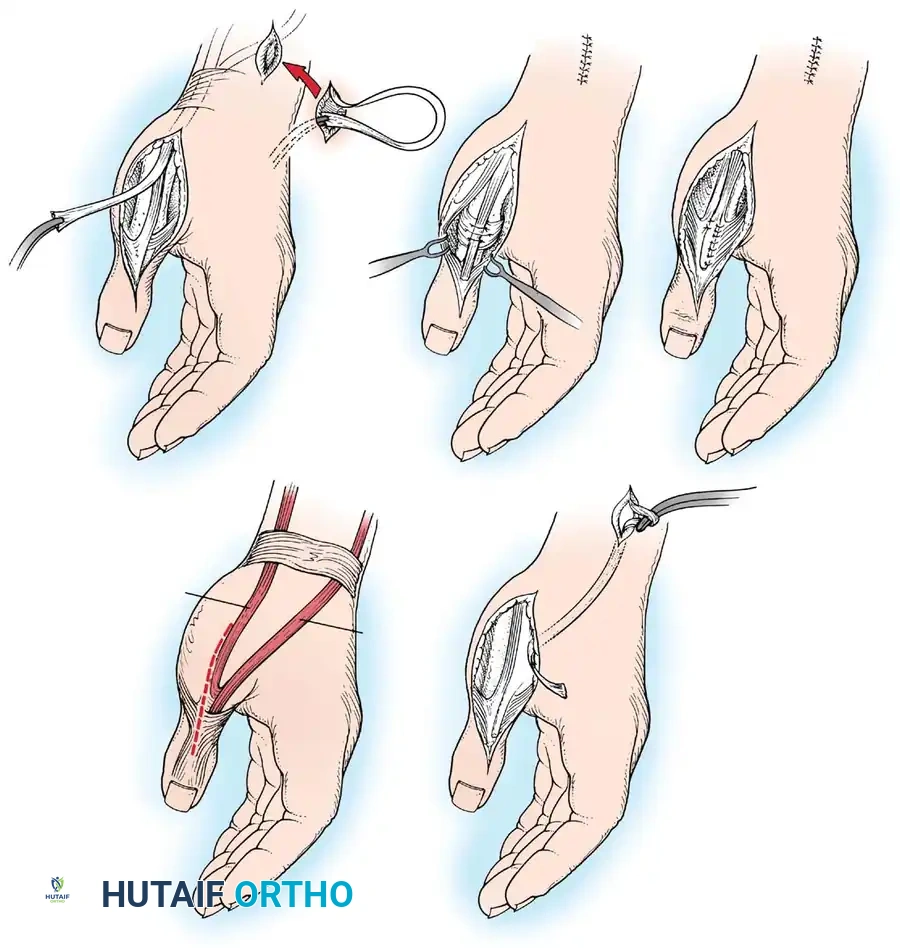
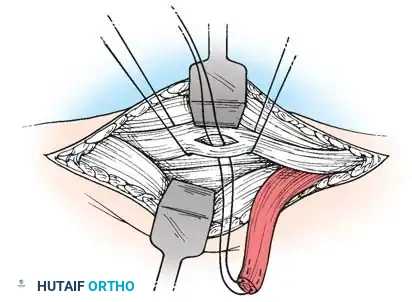
6. Rerouting: Pass the pronator teres and its attached periosteum posteriorly and laterally around the radius.
7. Bone Preparation: At the level of the original insertion, drill an anchoring hole on the anterolateral aspect of the radial cortex. Drill a smaller hole through the posteromedial part of the radius using a 1.6-mm Kirschner wire. Enlarge the anterolateral hole to 2.8 mm.
8. Fixation: Pass a heavy nonabsorbable suture (with the tendon attached) through the two holes from anterolateral to posteromedial. Draw the tendon into the larger hole and secure it.
9. Tensioning: Hold the forearm in approximately 45 degrees of supination and snug the tendon to hold this position. Allow the brachioradialis to fall back into place and close the incision in layers.
Postoperative Protocol:
Apply a long-arm cast maintaining the elbow in 45 degrees of flexion and the forearm in 60 degrees of supination. Elevate the arm immediately. Sutures are removed at 2 weeks, and a new long-arm cast is applied for an additional 4 weeks. Nighttime supination splinting must be continued for at least 6 months.
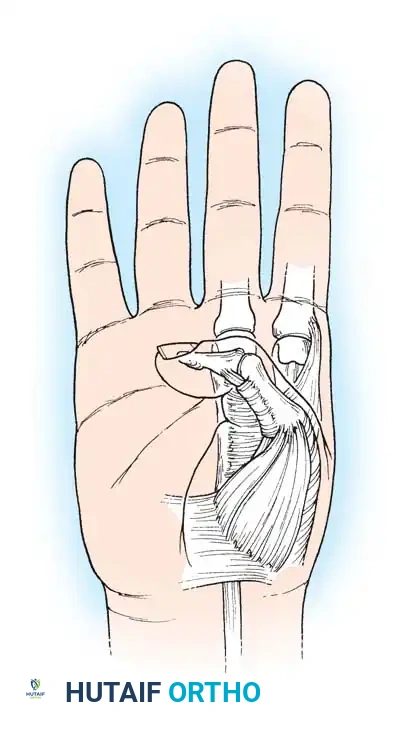
FLEXION DEFORMITIES OF THE WRIST AND FINGERS
Flexion deformities of the wrist and fingers are the most frequent upper extremity manifestations of spastic paralysis. These are typically accompanied by forearm pronation, elbow flexion, and a thumb-in-palm deformity.
Zancolli Classification of Flexion Deformities
Zancolli et al. classified spastic flexion deformities of the wrist and hand into three distinct patterns, which dictate the surgical approach:
Table 69-3: Zancolli Classification
* Group 1: Active finger extension is possible with the wrist in less than 20 degrees of flexion. This is a mild deformity where grasp and release are functional.
* Management: Consider FCU tenotomy combined with fractional lengthening of the finger flexors at the musculotendinous junction.
* Group 2: Active finger extension is possible only with the wrist in more than 20 degrees of flexion.
* Group 2a: Voluntary wrist extension is present with fingers flexed (active wrist extensors, spastic finger flexors).
* Group 2b: No active wrist extension with fingers flexed (weak wrist extensors, spastic finger flexors).
* Group 3: Wrist and finger extension are absent even with maximal passive wrist flexion. Severe fixed contractures are present.
Surgical Strategies for Wrist and Finger Flexion
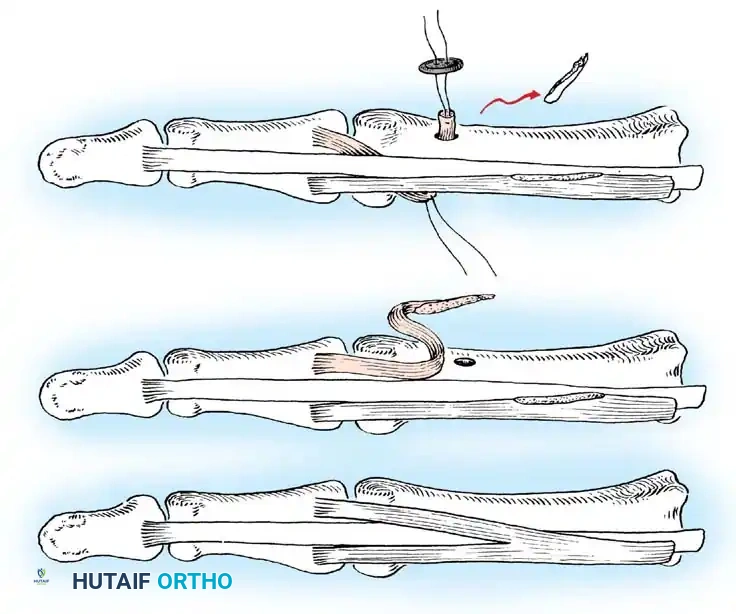
For Group 1 and 2a patients, the primary goal is to weaken the spastic flexors without destroying their function. Fractional lengthening of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) at the musculotendinous junction is preferred over Z-lengthening, as it preserves the continuity of the muscle fibers and prevents over-lengthening.
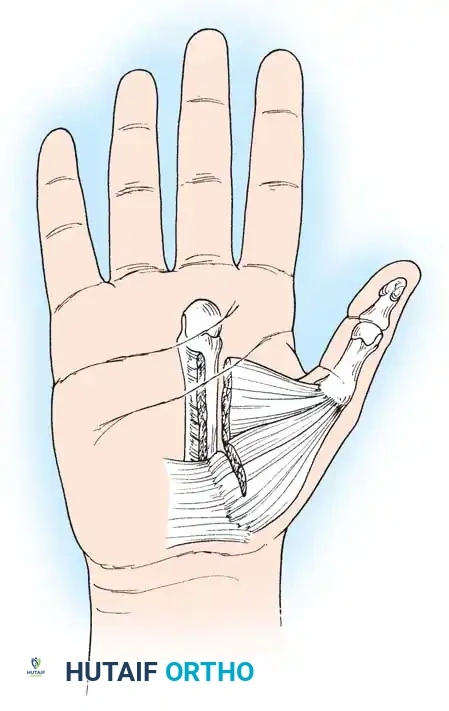
For Group 2b patients, augmentation of wrist extension is required. The classic procedure is the transfer of the Flexor Carpi Ulnaris (FCU) to the Extensor Carpi Radialis Brevis (ECRB). The FCU is a strong, often spastic deforming force; transferring it to the ECRB removes the volar deforming
Associated Surgical & Radiographic Imaging