Neurovascular Island Graft Transfer: Advanced Surgical Techniques and Protocols

Key Takeaway
The neurovascular island graft transfer is a highly specialized microsurgical technique utilized to restore critical sensation to the thumb following severe nerve injury. By harvesting a sensate, vascularized skin paddle from an expendable donor digit—typically the ulnar aspect of the ring finger—surgeons can reconstruct the thumb's tactile surface. This procedure demands meticulous dissection of the neurovascular bundle to ensure graft viability and optimal functional recovery.
INTRODUCTION AND RATIONALE
The human thumb is responsible for approximately 40% to 50% of overall hand function, serving as the critical post for pinch, grasp, and fine motor manipulation. However, the mechanical utility of the thumb is severely compromised without protective and tactile sensation. In cases of irreparable median nerve damage, severe crush injuries, or extensive pulp loss where primary nerve repair or nerve grafting is unfeasible, the Neurovascular Island Graft Transfer (often historically associated with the Littler flap) remains a gold-standard reconstructive option.
This procedure involves the transposition of a sensate, vascularized composite island of skin and subcutaneous tissue from a less critical donor digit to the volar aspect of the thumb. By transferring the tissue on its intact neurovascular pedicle, the surgeon provides immediate, durable, and sensate coverage to the thumb pulp, bypassing the prolonged and often unpredictable process of axonal regeneration associated with conventional nerve grafts or conduits.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Irreparable Nerve Injury: Permanent loss of median nerve sensation to the thumb where proximal nerve reconstruction has failed or is impossible.
- Severe Pulp Loss: Traumatic avulsions or deep burns of the thumb pulp requiring both soft tissue coverage and sensory restoration.
- Failed Nerve Reconstruction: Cases where previous epineurial repairs, autologous nerve grafts, or bioabsorbable conduits (e.g., polyglycolic acid or collagen tubes) have failed to restore functional two-point discrimination.
Contraindications
- Vascular Compromise: Peripheral vascular disease, severe Raynaud's phenomenon, or a positive Allen's test indicating an incomplete superficial palmar arch.
- Widespread Nerve Damage: Concomitant ulnar nerve injury that renders the potential donor sites (ring or little finger) insensate.
- Donor Digit Trauma: Previous trauma or scarring along the volar aspect of the intended donor digit or the fourth web space.
Clinical Pearl: Always perform a rigorous preoperative vascular assessment. Doppler ultrasonography or digital plethysmography should be utilized to map the palmar arch and ensure that sacrificing a proper digital artery will not induce ischemia in the donor or adjacent digits.
ANATOMY AND BIOMECHANICS
The success of the neurovascular island graft relies on a profound understanding of the palmar microvascular and neural anatomy.
The common palmar digital arteries arise from the superficial palmar arch and travel distally within the lumbrical canals. At the level of the web spaces, they bifurcate into the proper palmar digital arteries. The venous drainage of the island flap relies entirely on the delicate venae comitantes accompanying the digital artery and the subcutaneous venous plexus, which must be meticulously preserved during dissection.
Neurologically, the common palmar digital nerves arise from the median and ulnar nerves. The fourth web space is typically supplied by the ulnar nerve. The proper digital nerve to the ulnar side of the ring finger must be carefully separated from the common digital nerve via intraneural dissection to allow adequate mobilization of the pedicle without tethering.
PREOPERATIVE PLANNING AND DONOR SITE SELECTION
The ideal donor site must provide adequate skin territory while minimizing donor site morbidity. The hierarchy of donor sites is as follows:
- Ulnar Aspect of the Ring Finger: The primary choice. It is outside the primary radial pinch mechanism (thumb, index, middle fingers) and is innervated by the ulnar nerve, making it ideal for median nerve deficits.
- Radial Aspect of the Little Finger: An alternative if the ring finger is unavailable.
- Ulnar Aspect of the Middle Finger: Only utilized if the median nerve is completely intact and the deficit is strictly localized to the thumb, though this risks compromising a primary pinch digit.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Preparation and Flap Design
The procedure is performed under regional anesthesia (brachial plexus block) or general anesthesia. The patient is positioned supine with the arm extended on a hand table.
- Exsanguination: Exsanguinate the limb by elevation or using an Esmarch bandage, and inflate a pneumatic upper arm tourniquet to 250 mmHg.
- Recipient Site Marking: Using a sterile skin marker, accurately outline the area of sensory deficit or scarring on the volar thumb.
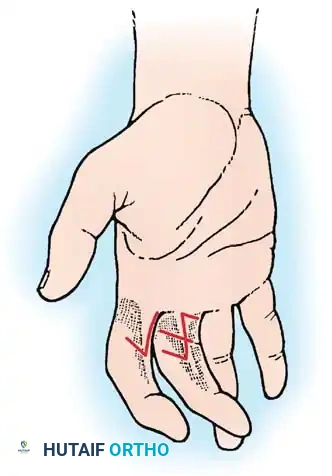
- Donor Site Marking: Transfer this template to the ulnar side of the ring finger. If the entire palmar surface of the thumb is insensitive, outline the maximal donor area on the ring finger.
- Flap Geometry: Shape the donor area to include most of the ulnar side of the finger. Crucially, incorporate V-shaped darts extending near the midline on both the palmar and dorsal surfaces between the interphalangeal joints. This geometry prevents linear scar contracture during postoperative finger flexion. The outlined area must include skin supplied by the dorsal branch of the proper digital nerve.
2. Incision and Exposure
Beginning proximally near the base of the palm, make a zigzag (Bruner) incision extending distally to the fourth web space.
- Recipient Preparation: Proceed to make a second zigzag incision across the palm, conforming to the natural skin creases, connecting the proximal end of the original incision to the thumb recipient site.
- Excision: Excise the insensitive skin from the thumb. If this skin is structurally intact (merely insensate), preserve it in moist saline; it can be defatted and utilized as a full-thickness skin graft (FTSG) for the donor site later.
3. Neurovascular Dissection
This is the most critical phase of the operation and requires loupe magnification (3.5x to 4.5x) or an operating microscope.
- Identify the common volar digital artery and nerve to the ring and little fingers within the fourth web space.
- Dissect the proper digital artery and nerve to the ulnar side of the ring finger, preserving a cuff of surrounding areolar tissue to protect the venae comitantes and microscopic venous drainage.
- Arterial Ligation: Identify, ligate, and divide the proper digital artery supplying the radial side of the little finger. This allows the common digital artery to be mobilized exclusively with the flap.
- Intraneural Dissection: Carefully dissect and split the proper digital nerve to the ulnar side of the ring finger proximally away from the common volar digital nerve. This requires micro-scissors and precise epineurial separation to avoid axonal injury.

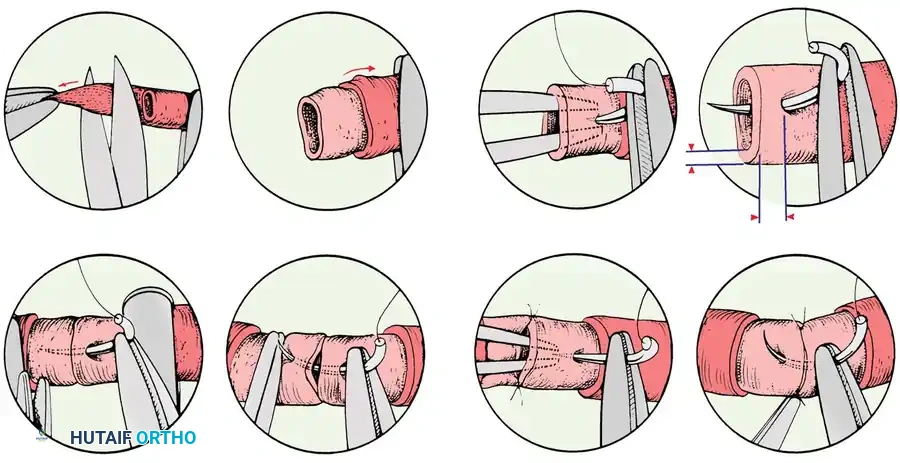
4. Flap Elevation
Continue the dissection distally. Excise the previously outlined skin island from the ulnar side of the ring finger in continuity with its attached neurovascular bundle.
* Hemostasis: Use bipolar electrocautery exclusively to divide any small, unnamed branches of the artery. Monopolar cautery is strictly contraindicated near the pedicle.
* Venous Preservation: Preserve as many subcutaneous veins as possible within the pedicle's areolar tissue to prevent postoperative venous congestion.
Surgical Warning: Do not skeletonize the artery and nerve. Leaving a perivascular cuff of tissue is mandatory to preserve the delicate venous outflow tract. Venous congestion is the most common cause of flap failure in island transfers.
5. Flap Transfer and Insetting
Free the composite graft and gently carry the island across the open palmar incision to the recipient area on the thumb.
- Tension Check: Ensure that the neurovascular bundle is sufficiently long to permit the transfer without any longitudinal tension. The island graft should cover the majority of the pulp area on the palmar aspect of the thumb, extending to the ulnar aspect (the primary contact point for pinch), but should not extend to the distal edge of the nail bed to avoid nail matrix deformity.
- Suturing: Suture the island graft into place on the thumb using non-absorbable monofilament sutures (e.g., 5-0 or 6-0 nylon).

6. Pedicle Inspection and Closure
Before closing the palmar incisions, carefully inspect the entire length of the transposed neurovascular bundle.
* Check for stretching, kinking, or twisting. The pedicle should lie in a gentle, sweeping curve.
* Close the palmar zigzag incisions loosely to avoid compressing the pedicle.
7. Donor Site Management
The donor defect on the ring finger must be covered.
* Use the full-thickness skin graft (FTSG) harvested from the recipient thumb (carefully defatted), or obtain a thick split-thickness skin graft (STSG) from the hypothenar eminence or proximal forearm.
* Secure the graft with a tie-over bolster (stent) dressing to ensure intimate contact with the graft bed and prevent hematoma formation.
8. Tourniquet Release and Reperfusion
Release the pneumatic tourniquet.
* Position the wrist in slight flexion and the thumb in palmar abduction to completely eliminate tension on the transferred bundle.
* Observation: Carefully observe the island graft for the return of capillary refill. The graft should eventually become pink.
Pitfall: Vascular spasm is common immediately following tourniquet release and can cause transient ischemia for several minutes. Bathe the pedicle in warm saline or topical vasodilators (e.g., papaverine or lidocaine) if spasm persists. If the flap remains pale or becomes deeply cyanotic, you must immediately re-check the wrist/thumb position. If necessary, reopen the palmar incision to explore the bundle for mechanical kinking or hematoma compression.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is designed to protect the microvascular pedicle while preventing joint stiffness.
Phase I: Protection (Days 0 to 14)
- Immobilization: Apply a bulky, non-compressive dressing and a dorsal plaster blocking splint. The wrist is held in 20° to 30° of flexion, the thumb in palmar abduction, and the fingers in intrinsic-plus positioning (MCPs flexed 60°, IP joints extended) to relieve all tension on the pedicle.
- Elevation: The hand must be elevated continuously above heart level for 4 to 5 days to promote venous drainage and minimize edema.
- Monitoring: Flap checks (color, capillary refill, turgor, temperature) should be performed every 2-4 hours for the first 48 hours.
Phase II: Early Motion (Weeks 2 to 4)
- Sutures are removed between 10 to 14 days, provided the flap and donor site grafts are fully incorporated.
- The dorsal blocking splint is maintained, but gentle, protected active range of motion (AROM) exercises are initiated under the guidance of a certified hand therapist.
- The splint is typically discontinued at 3 to 4 weeks, depending on the healing status of the thumb and the donor finger.
Phase III: Sensory Re-education (Weeks 4 and Beyond)
Sensory re-education is the most critical aspect of long-term functional recovery. Because the transferred nerve is still connected to its original cortical map, the patient will initially perceive tactile stimuli on the thumb as if the ring finger is being touched (cortical misdirection).
* A structured program of cortical reorientation is required. Patients use visual feedback (watching the thumb being touched) to retrain the brain to associate the sensory input with the thumb.
* Over 6 to 12 months, most patients achieve functional integration, though some degree of dual perception may persist.
MANAGEMENT OF NEUROMAS AND PAIN CONTROL
If the original thumb nerve injury resulted in a painful end neuroma, the neuroma must be excised prior to flap insetting.
* Dissect the injured nerve proximally into healthy tissue.
* If the distal branches cannot be found or are encased in dense scar tissue, release the nerve proximally to relieve traction pain.
* Resect the neuroma and bury the proximal nerve stump deep into the pronator quadratus or thenar musculature to prevent recurrent neuroma formation.
* Recent literature supports the use of collagen conduits or muscle-in-vein nerve guides to cap the resected nerve ends, reducing the incidence of painful postoperative neuromas.
CONCLUSION
The neurovascular island graft transfer is a highly demanding but immensely rewarding procedure. When executed with meticulous microsurgical precision, it restores the critical protective and tactile sensation necessary for a functional thumb. Strict adherence to anatomical principles—particularly the preservation of venous outflow and the prevention of pedicle kinking—combined with aggressive postoperative sensory re-education, ensures optimal outcomes for patients suffering from devastating sensory deficits of the hand.
You Might Also Like