Neuromuscular Scoliosis: Comprehensive Surgical Management and Spinopelvic Fixation
Key Takeaway
Neuromuscular scoliosis presents unique challenges due to early onset, rapid progression, and associated systemic comorbidities. Surgical intervention aims to achieve a solid arthrodesis, balancing the spine in coronal and sagittal planes over a level pelvis. This guide details evidence-based protocols for preoperative optimization, complex spinopelvic fixation techniques, and postoperative management, ensuring optimal functional outcomes and quality of life for patients with severe neuromuscular spinal deformities.
Introduction to Neuromuscular Scoliosis
Neuromuscular scoliosis encompasses a heterogeneous group of spinal deformities arising from myopathic or neuropathic diseases. Unlike adolescent idiopathic scoliosis (AIS), neuromuscular curves typically present at a younger age, progress more rapidly, and relentlessly continue to deteriorate even after skeletal maturity. The specific etiology of the spinal deformity often remains multifactorial; however, the fundamental biomechanical failure is driven by a loss of truncal muscle strength, absent voluntary motor control, and profound deficits in sensory feedback mechanisms, such as proprioception.
In the flexible, rapidly growing spinal column of a juvenile patient, these neuromuscular deficits lead to asymmetric loading. As the spine collapses under gravity, increased pressure on the concave side of the curve inhibits physeal growth (the Hueter-Volkmann principle), resulting in structural wedging of the vertebral bodies. Furthermore, the vertebrae in these patients are frequently compromised by severe disuse osteopenia and chronic malnutrition, complicating surgical instrumentation and arthrodesis.

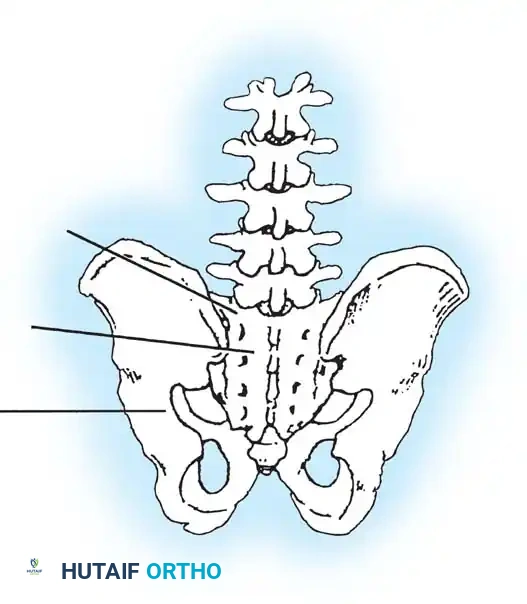
Many neuromuscular curves manifest as long, sweeping, C-shaped deformities that extend distally to include the sacrum, making pelvic obliquity a hallmark of the disease. The overarching goal of treatment is not cosmetic; rather, it is to maintain a balanced spine in the coronal and sagittal planes over a level pelvis, thereby optimizing sitting balance, pulmonary function, and overall quality of life.
Classification of Neuromuscular Spinal Deformity
The Scoliosis Research Society (SRS) classification for neuromuscular scoliosis divides the etiology into two primary categories: Neuropathic and Myopathic.
Neuropathic Deformities
Upper Motor Neuron Lesions:
* Cerebral palsy (CP)
* Spinocerebellar degeneration (Friedreich ataxia, Charcot-Marie-Tooth, Roussy-Levy syndrome)
* Syringomyelia
* Spinal cord tumor or trauma
Lower Motor Neuron Lesions:
* Poliomyelitis and other viral myelitides
* Traumatic paraplegia/quadriplegia
* Spinal muscular atrophy (Werdnig-Hoffmann, Kugelberg-Welander)
* Dysautonomia (Riley-Day syndrome)

Myopathic Deformities
- Arthrogryposis multiplex congenita
- Muscular dystrophy (Duchenne, Limb-girdle, Facioscapulohumeral)
- Fiber-type disproportion
- Congenital hypotonia
- Myotonia dystrophica
Clinical Pearl: Differentiating between a neuropathic and myopathic etiology is critical for preoperative planning. For instance, patients with Duchenne muscular dystrophy have a high incidence of intrinsic cardiomyopathy and malignant hyperthermia susceptibility, demanding specialized anesthetic protocols.
Clinical Evaluation and Nonoperative Management
Observation
Not all neuromuscular spinal deformities require immediate intervention. Small curves (less than 20 to 25 degrees) can be observed with serial radiographs. Furthermore, in severely cognitively impaired patients where a large curve does not hinder nursing care, seating, or functional baseline, observation may be the most humane and appropriate course of action. However, if the functional ability of the patient is compromised by increasing curvature, treatment must be instituted promptly.

Orthotic Management
Progressive neuromuscular scoliosis in very young patients is initially managed with an orthosis. While bracing rarely halts the progression of a neuromuscular curve entirely, it serves as a crucial temporizing measure. The primary goal of orthotic management is to slow the rate of progression, allowing for further spinal and thoracic growth before definitive spinal fusion is mandated.
For ambulatory patients with some trunk control, a dynamic Thoracolumbosacral Orthosis (TLSO) or Milwaukee brace may be considered. However, the vast majority of neuromuscular patients lack normal righting reflexes and voluntary muscle control. Therefore, passive, custom-molded, total-contact TLSOs are generally required.
- Soft Boston Orthosis: Fabricated from malleable materials, this brace is well-tolerated and provides excellent trunk support for flaccid patients, freeing their upper extremities for functional use. The primary complication is heat retention and skin maceration.
- Custom Seating Devices: Patients with severe involvement and absent head control frequently require custom-fabricated wheelchair seating matrices combined with head-control devices.

Preoperative Optimization and Planning
The physiological toll of major spinal reconstruction in a neuromuscular patient cannot be overstated. A multidisciplinary approach is mandatory.
Pulmonary Evaluation
Most patients with neuromuscular scoliosis exhibit restrictive lung disease. Preoperative pulmonary function tests (PFTs) are essential if the patient is cooperative.
* Evaluate Forced Vital Capacity (FVC) and Forced Expiratory Volume in 1 second (FEV1).
* Historical data (e.g., Nickel et al.) indicates that patients with a vital capacity of less than 30% of predicted normal will require prolonged postoperative respiratory support.
* Patients with severe pulmonary compromise and an absent voluntary cough reflex may require a planned postoperative tracheostomy or prolonged nasotracheal intubation.
Nutritional and Gastrointestinal Status
Malnutrition is rampant due to uncoordinated swallowing, gastroesophageal reflux disease (GERD), and hiatal hernias. Surgery exponentially increases metabolic demand.
* Preoperative hyperalimentation may be required.
* A preoperative gastrostomy tube (G-tube) placement and Nissen fundoplication should be strongly considered to improve nutritional status, enhance wound healing, and prevent catastrophic postoperative aspiration pneumonia.
Neurological and Medical Optimization
- Seizure Control: Anticonvulsant levels must be optimized. Note that chronic anticonvulsant use exacerbates osteopenia, directly impacting instrumentation purchase.
- Cardiac Evaluation: Mandatory for myopathic conditions (e.g., Duchenne) and specific neuropathies (e.g., Friedreich ataxia) due to associated cardiomyopathies.
- Ambulatory Status: A patient with marginal, energy-intensive ambulation may lose the ability to walk following a long spinal fusion. This must be explicitly discussed with the family during informed consent.

Blood Conservation Strategies
Neuromuscular spinal surgery is notoriously bloody due to extensive exposures, osteopenic bone, and altered vasomotor tone.
* Preoperative autodonation is rarely feasible due to chronic anemia and low body weight.
* Intraoperative strategies must include a cell saver, meticulous electrocautery, hypotensive anesthesia (if tolerated neurologically and hemodynamically), and modern antifibrinolytics (e.g., Tranexamic Acid).
Biomechanics and Curve Assessment
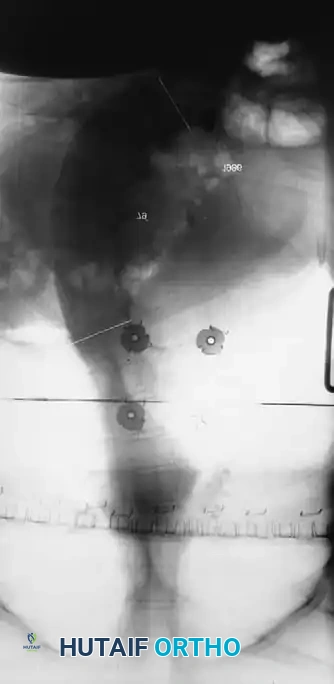
Evaluating Pelvic Obliquity
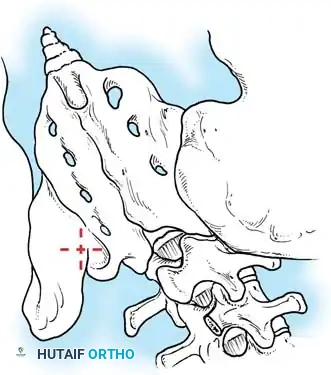
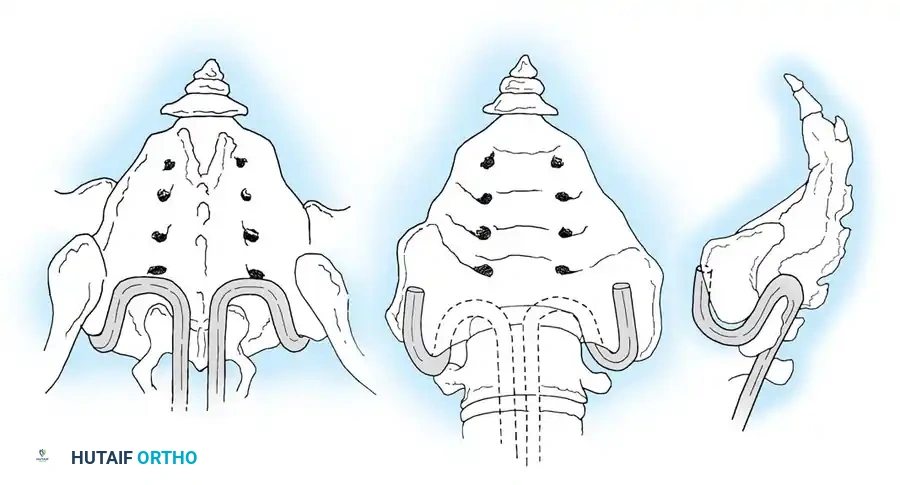
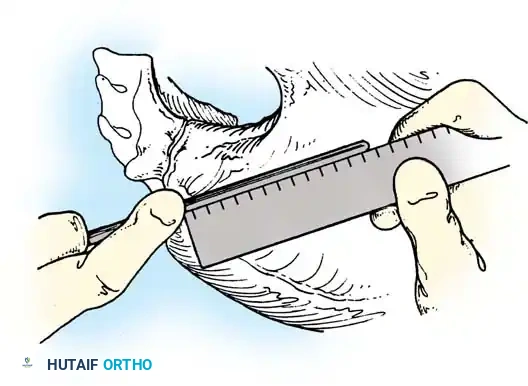
Pelvic obliquity is a primary driver of seating imbalance and decubitus ulcer formation over the ischial tuberosities. The surgeon must differentiate between a fixed spinopelvic deformity and obliquity caused by infra-pelvic contractures.
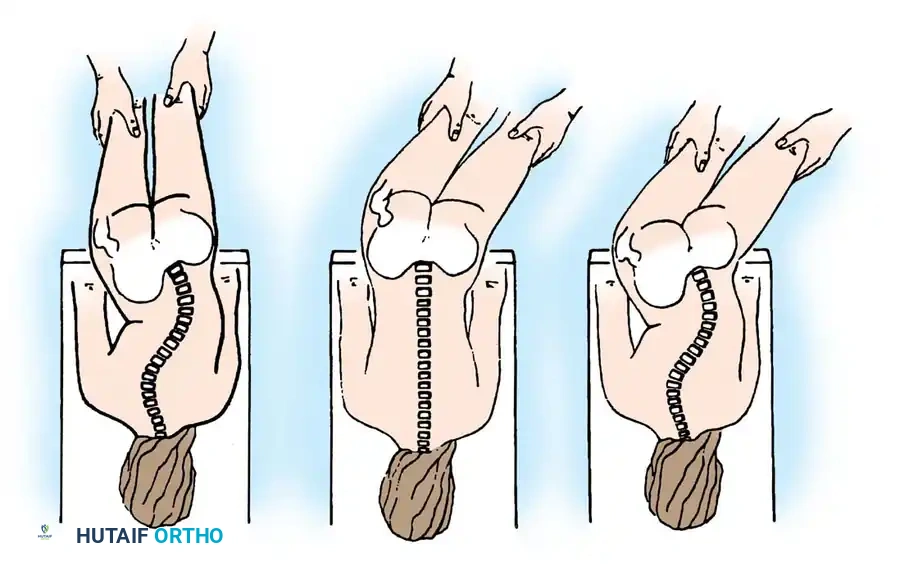
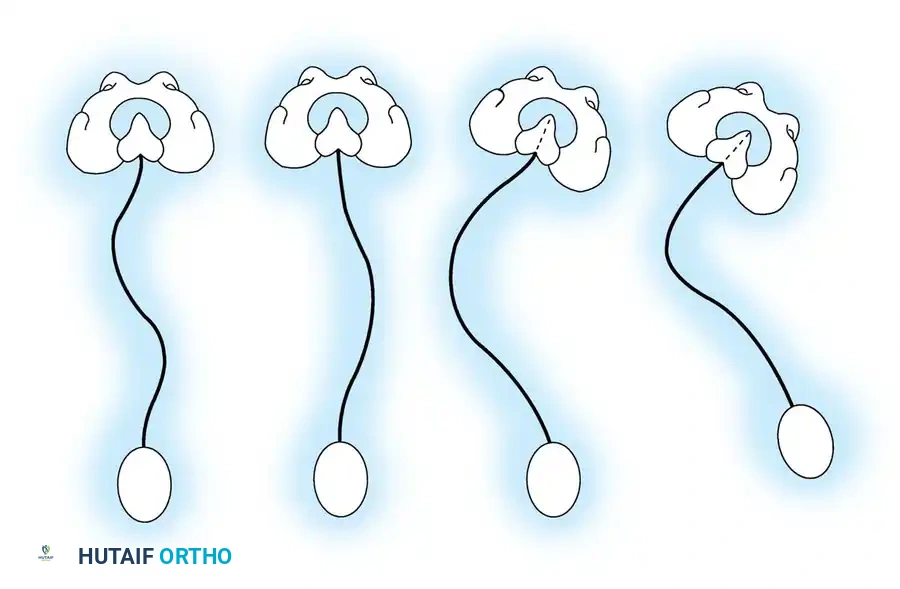
- A: Clinical presentation of pelvic obliquity.
- B: If the pelvic obliquity resolves with abduction or adduction of the hips, the primary cause is a pelvic-femoral muscle contracture (infra-pelvic).
- C: If the obliquity persists despite hip positioning, a fixed spinopelvic deformity exists, necessitating fusion to the pelvis.
Surgical Warning: Failure to recognize and release severe hip contractures prior to or concurrent with spinal fusion will result in persistent seating imbalance and immense stress on the distal spinopelvic instrumentation, leading to catastrophic hardware failure.
Operative Management: Indications and Goals
The primary goal of operative intervention is to achieve a solid arthrodesis that maintains the spine balanced in both the coronal and sagittal planes over a level pelvis.
Determining Fusion Levels
Neuromuscular curves require significantly longer fusions than idiopathic curves.
* Proximal Extent: Fusion should routinely extend to T4 or higher. Stopping at or below T4 carries a high risk of cephalad progression of the deformity ("adding on") and subsequent proximal junctional kyphosis (PJK).
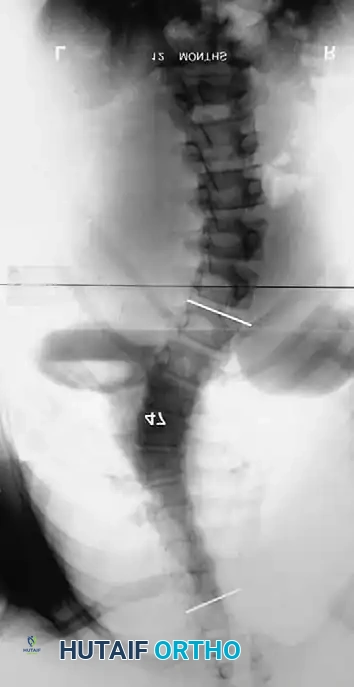
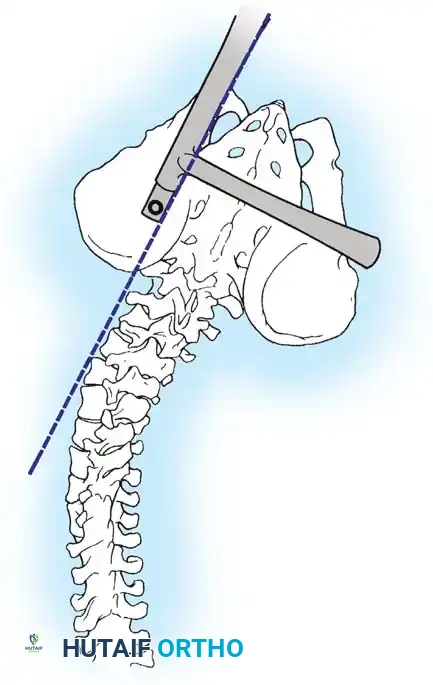
* Distal Extent: The decision to fuse to the sacrum/pelvis is critical.
* Excluding the Sacrum: Can be considered in ambulatory patients who require lumbosacral motion, possess no significant pelvic obliquity, and demonstrate a horizontal L5 vertebral body.
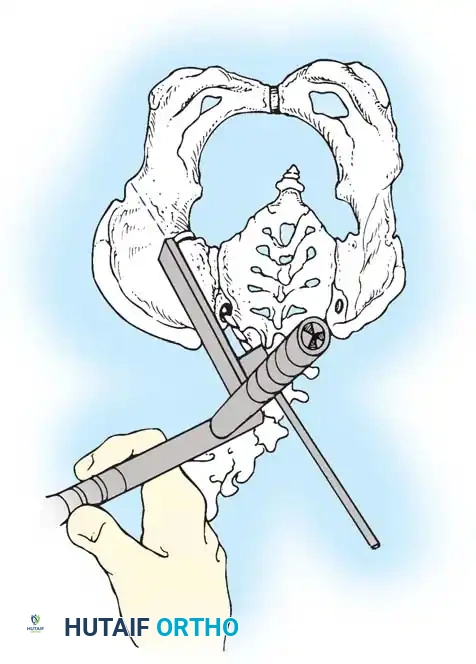
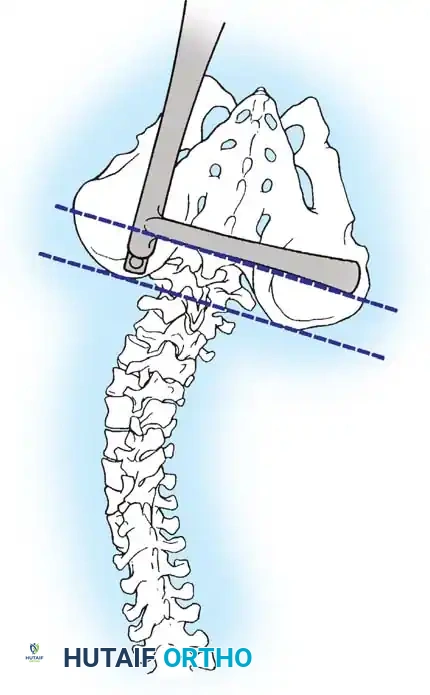
* Including the Pelvis: Mandatory for nonambulators with fixed spinopelvic obliquity. If bending or traction films reveal more than 10 to 15 degrees of L4 or L5 tilt relative to the interiliac crest line, the fusion must extend to the pelvis.

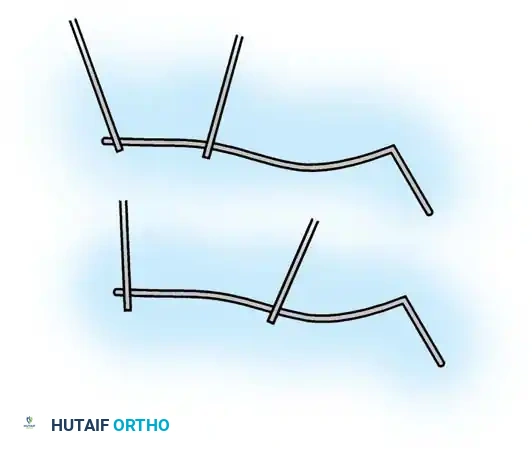
Maintaining physiological lumbar lordosis is paramount in insensate patients fused to the pelvis. Proper sagittal alignment distributes body weight equally beneath the ischial tuberosities and posterior thighs, drastically reducing the risk of pressure sores over the coccyx and sacrum.
Surgical Approaches and Step-by-Step Techniques
1. Positioning and Anesthesia
Patients are positioned prone on a specialized spinal frame (e.g., Jackson table) to allow the abdomen to hang free, reducing intra-abdominal pressure and minimizing epidural venous bleeding. All bony prominences must be meticulously padded. Intraoperative neuromonitoring (Somatosensory Evoked Potentials [SSEPs] and Motor Evoked Potentials [MEPs]) is utilized, though baseline signals may be degraded or absent in severe neuromuscular disease. If monitoring is unreliable, a Stagnara wake-up test may be attempted, though cooperation is often impossible.

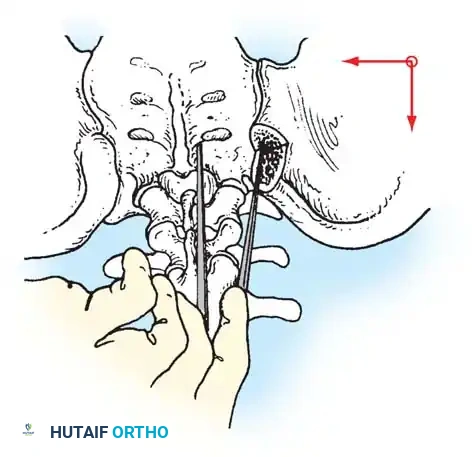
2. Surgical Exposure
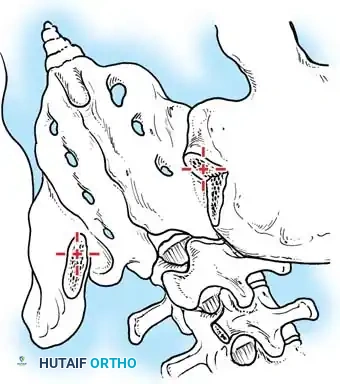
A standard midline longitudinal incision is made. Meticulous subperiosteal dissection is performed to expose the posterior elements from the upper thoracic spine down to the sacrum and ilium. In neuromuscular patients, the soft tissues are often fibrotic, and the bone is osteopenic. Complete facetectomies are performed at every level to ensure a robust posterior fusion mass.
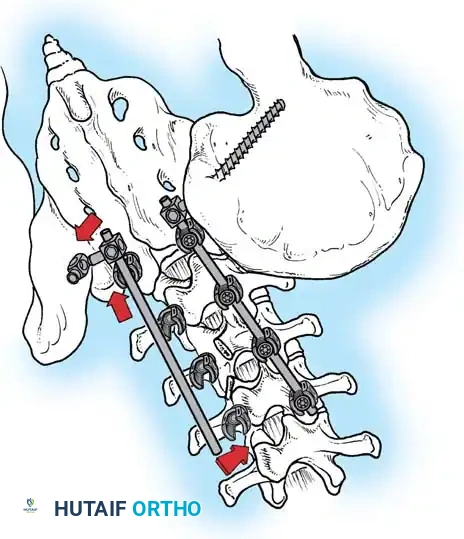
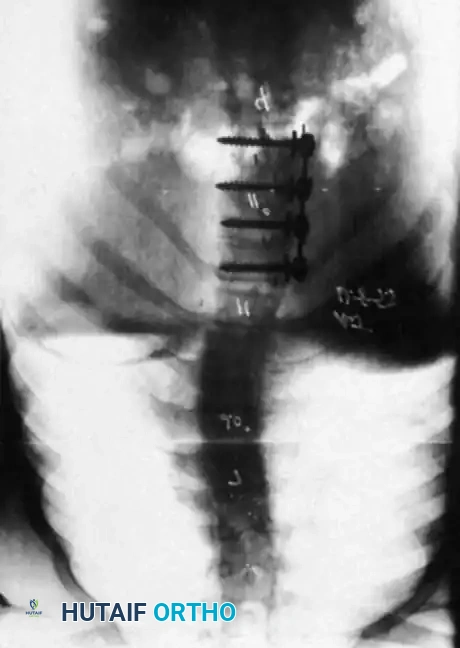
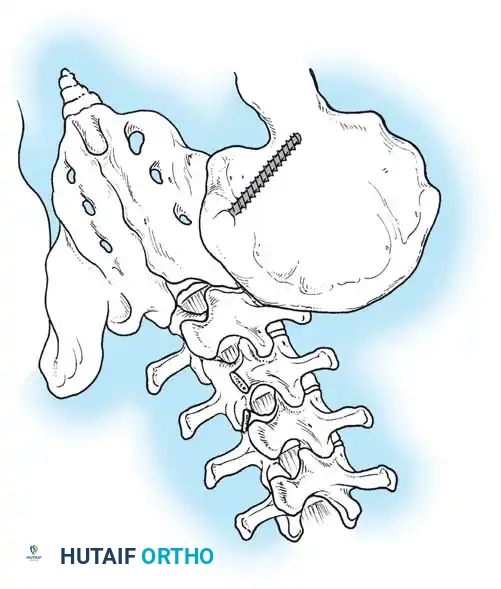
3. Instrumentation Strategies
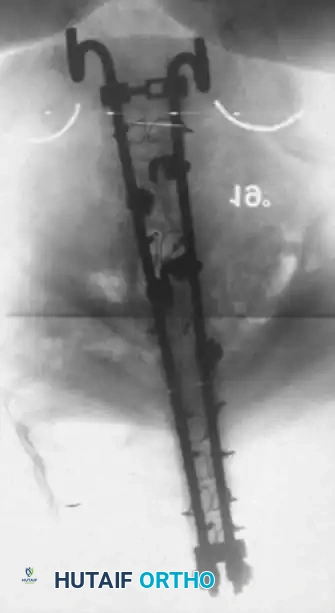
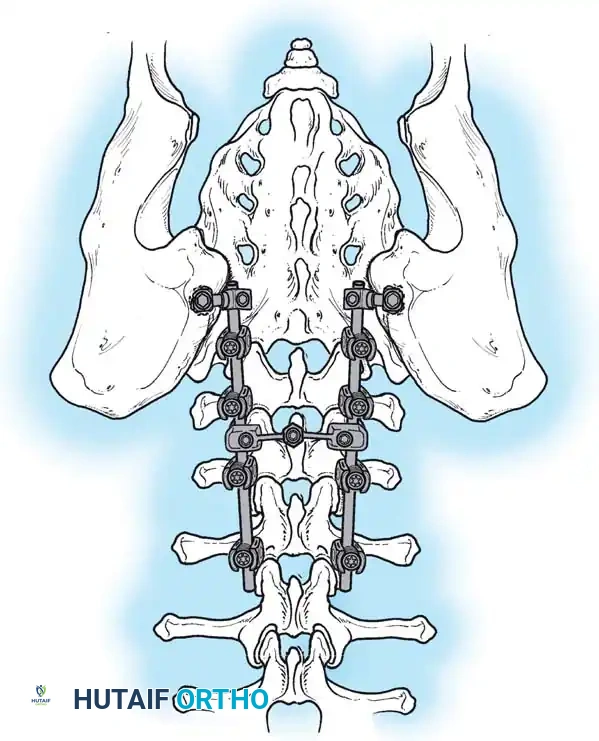
Due to poor bone stock, multiple points of fixation are required to distribute corrective forces.
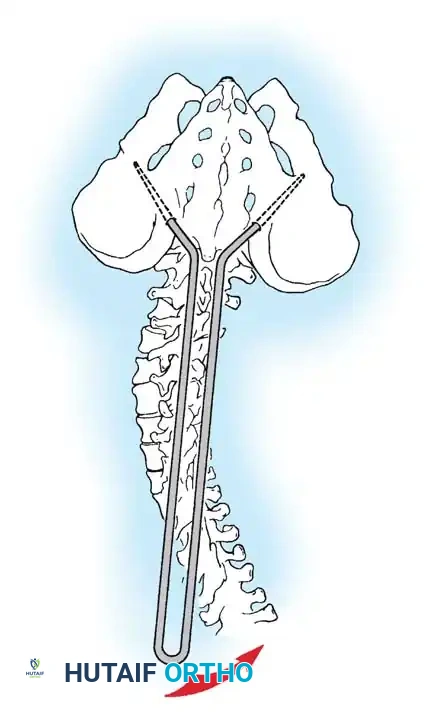
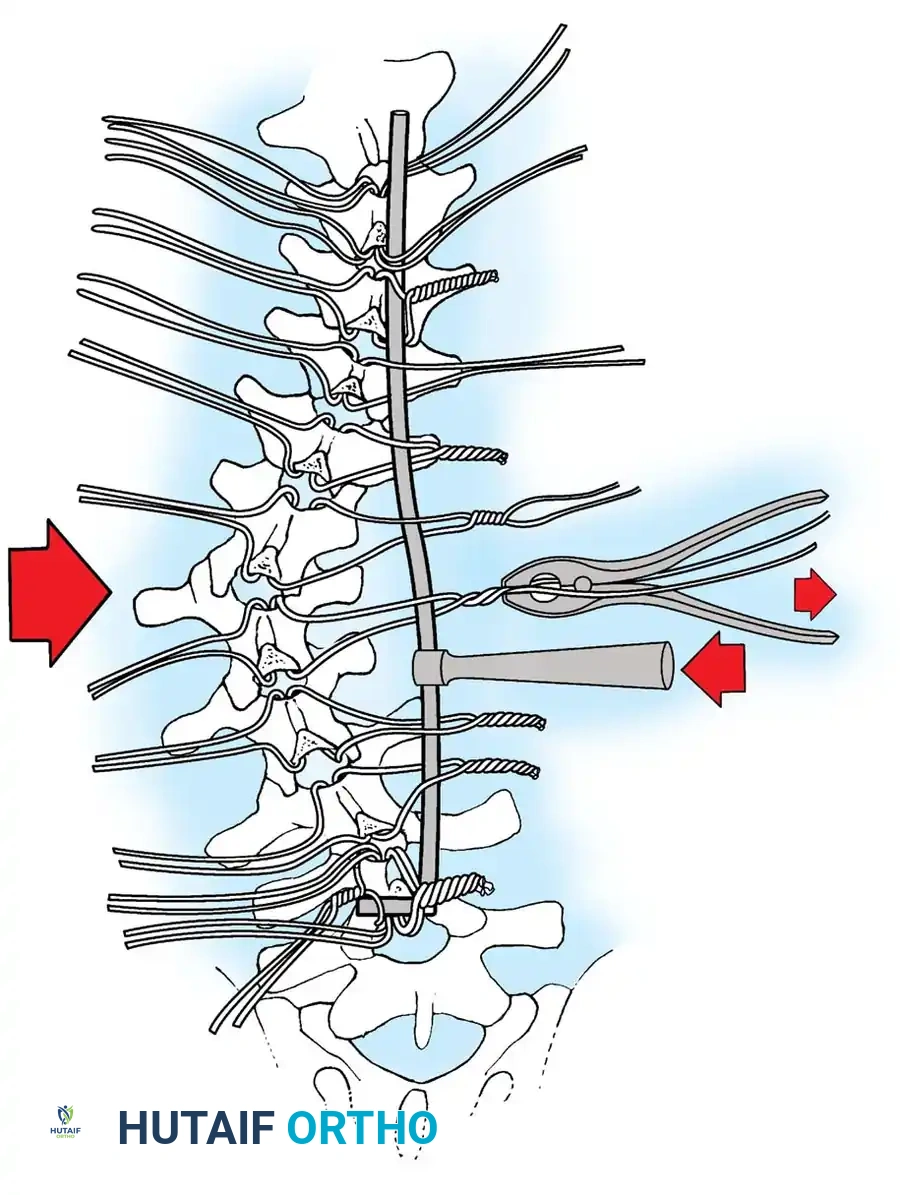
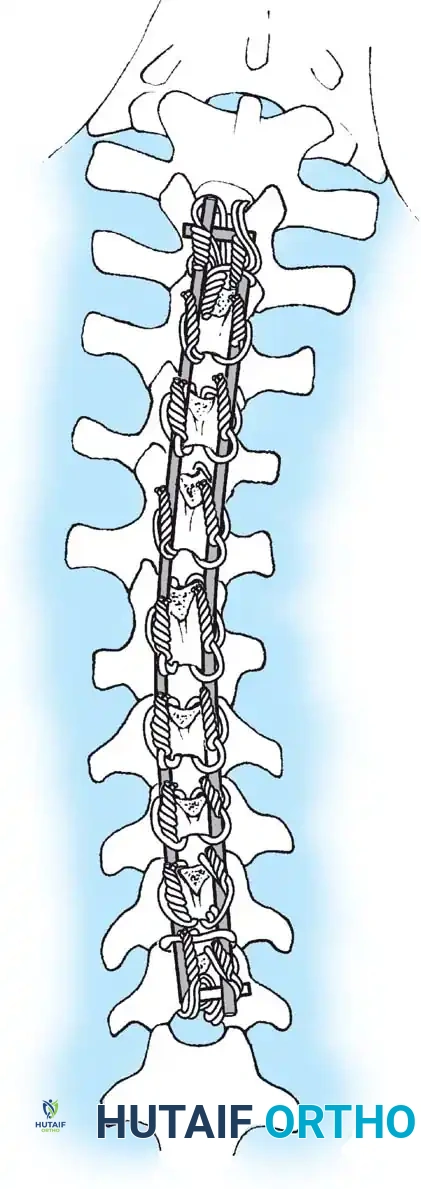
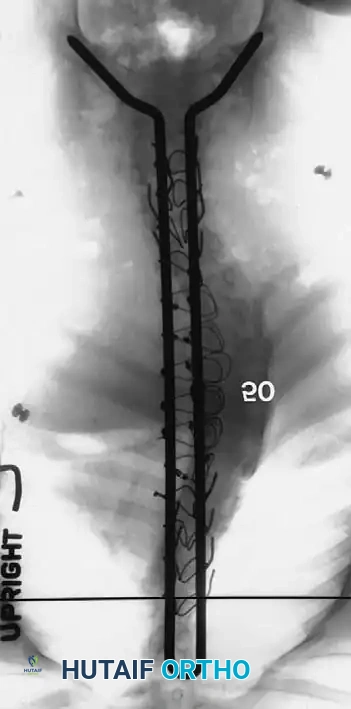
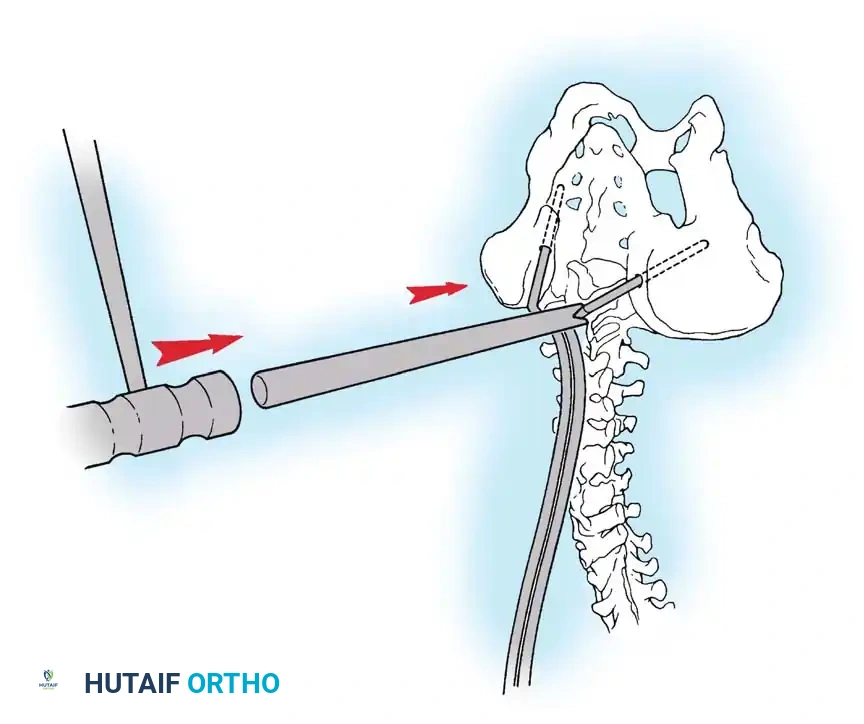
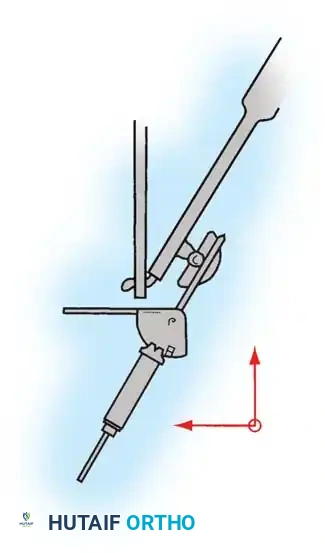
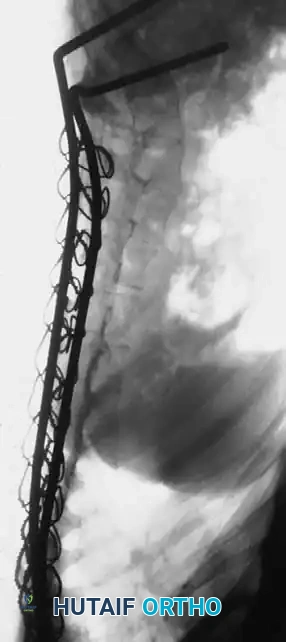
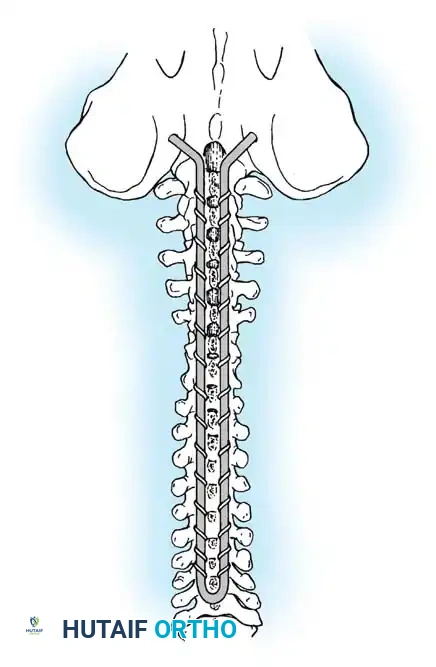
* Segmental Instrumentation: The gold standard involves rigid rod constructs (e.g., Cotrel-Dubousset principles) utilizing pedicle screws, hooks, and sublaminar wires or cables.
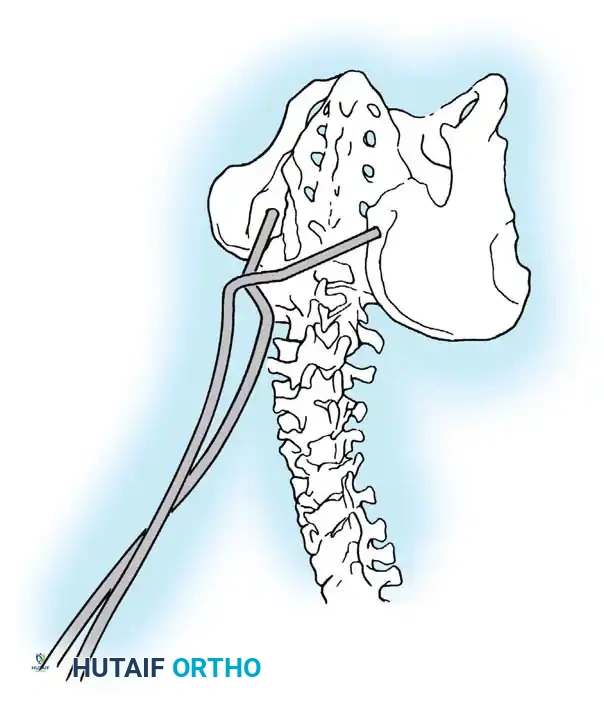
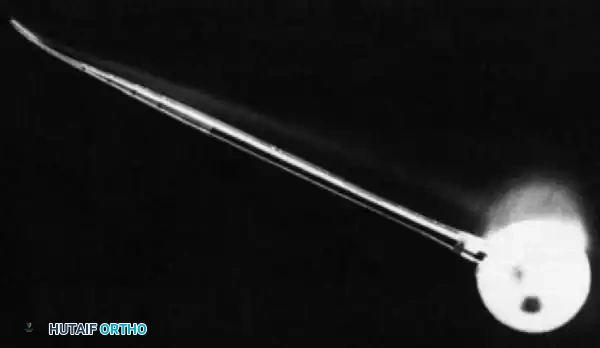
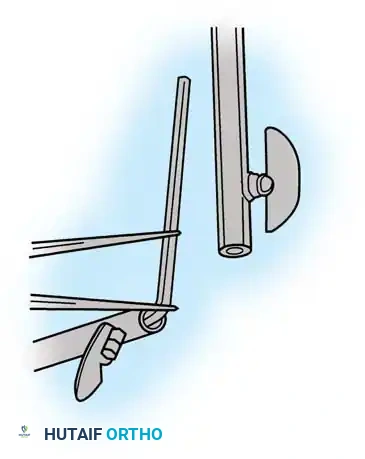
* Sublaminar Wires/Cables: Techniques pioneered by Luque remain highly relevant in neuromuscular scoliosis. Sublaminar cables provide excellent pull-out strength in osteopenic bone and distribute translational forces evenly across the apex of the deformity.
Associated Surgical & Radiographic Imaging





📚 Medical References
You Might Also Like


