Comprehensive Introduction and Patho-Epidemiology
The reconstruction of peripheral nerve injuries remains one of the most technically demanding and biologically complex challenges in operative orthopaedics, hand surgery, and microsurgery. When a peripheral nerve is transected, a highly orchestrated, albeit destructive, cascade of cellular events immediately ensues. The distal segment undergoes Wallerian degeneration, a process characterized by the breakdown of the axonal cytoskeleton and myelin sheath, orchestrated by calcium influx and the activation of calpain proteases. Simultaneously, Schwann cells dedifferentiate, proliferate, and align to form the bands of Büngner, while macrophages infiltrate the endoneurial tubes to clear myelin debris. Proximally, the nerve stump attempts to regenerate via robust axonal sprouting, driven by a complex upregulation of neurotrophic factors including Nerve Growth Factor (NGF), Brain-Derived Neurotrophic Factor (BDNF), and Glial Cell Line-Derived Neurotrophic Factor (GDNF). For functional recovery to occur, these regenerating axonal growth cones must successfully navigate the zone of injury, cross the coaptation site, and enter the precise endoneurial tubes of the distal stump to reach their target end-organs.
While primary end-to-end neurorrhaphy remains the unequivocal gold standard for clean, sharp transections, the reality of orthopaedic trauma dictates that high-energy mechanisms, severe crush injuries, blast trauma, or delayed presentations frequently result in a segmental nerve defect. In these complex clinical scenarios, attempting to forcefully mobilize the nerve ends to achieve a primary repair will inevitably introduce pathological tension across the coaptation site. Tension is universally recognized as the absolute enemy of nerve regeneration. Biomechanical and microvascular studies have conclusively demonstrated that an elongation of just 8% significantly impairs intraneural venular blood flow, initiating a cascade of localized hypoxia. Furthermore, an elongation of 15% causes complete obliteration of the vasa nervorum, resulting in profound ischemia of the nerve. This ischemic environment heavily favors fibroblast proliferation over axonal growth, leading to dense intraneural scarring, neuromatous disorganization, and an impenetrable barrier to axonal advancement.
Epidemiologically, peripheral nerve injuries occur in approximately 2% to 3% of all patients admitted to Level I trauma centers, with the upper extremity disproportionately affected due to its prehensile function and exposure to occupational and ballistic hazards. The incidence of segmental defects requiring grafting has risen alongside the survival rates of high-energy polytrauma and combat-related injuries. When a tension-free primary repair is rendered anatomically impossible due to these segmental losses, the reconstructive surgeon must bridge the gap utilizing autogenous nerve grafts, synthetic bioabsorbable conduits, or decellularized nerve allografts. The selection of the optimal bridging strategy requires a profound understanding of nerve topography, the underlying biological microenvironment, and the mechanical properties of the available reconstructive materials.
Detailed Surgical Anatomy and Biomechanics
A comprehensive mastery of peripheral nerve microanatomy is a fundamental prerequisite for successful microsurgical reconstruction. A peripheral nerve is a highly organized, hierarchically structured composite tissue. The outermost layer, the epineurium, is divided into the epifascicular (external) epineurium, which envelops the entire nerve trunk and cushions it against compressive forces, and the interfascicular (internal) epineurium, which separates individual fascicles. The epineurium is composed primarily of type I and type III collagen and carries the extrinsic longitudinal vascular plexus. Beneath the epineurium lies the perineurium, a dense, specialized layer of concentric flattened cells linked by tight junctions. The perineurium is mechanically robust, providing the primary tensile strength to the nerve, and acts as a semi-permeable physiological blood-nerve barrier, maintaining the specialized endoneurial fluid environment crucial for axonal conduction.
Within the perineurial sheath lies the endoneurium, a delicate matrix of loose connective tissue that surrounds individual myelinated and unmyelinated nerve fibers. The spatial arrangement of these fascicles dictates the nerve's topography, which transitions from a polyfascicular, highly interwoven pattern proximally to an oligofascicular or monofascicular pattern distally as the nerve approaches its terminal branches. Understanding this topography is critical during nerve grafting; a mismatch in fascicular alignment between the proximal stump, the graft, and the distal stump results in axonal misdirection, where motor axons erroneously enter sensory endoneurial tubes, leading to a complete failure of functional recovery.
Biomechanically, peripheral nerves exhibit anisotropic, viscoelastic properties, characterized by stress-relaxation and creep. The undulating course of the nerve fibers (the bands of Fontana) allows for physiological excursion and elongation during normal joint movement without transmitting stress to the axons. The blood supply to the nerve is delivered via the mesoneurium, a delicate, adventitia-like suspensory mesentery that carries segmental nutrient vessels from the adjacent regional vasculature. These segmental vessels penetrate the epineurium to anastomose with the intrinsic longitudinal microvascular plexus. Extensive surgical mobilization of a nerve to close a gap disrupts these segmental mesoneurial vessels. While the intrinsic plexus can sustain a mobilized segment to a certain degree, over-mobilization combined with even mild tension will critically compromise the vasa nervorum, precipitating the ischemic cascade and subsequent fibrosis that guarantees graft or repair failure.
Exhaustive Indications and Contraindications
The decision algorithm for addressing a peripheral nerve gap is dictated by the length of the defect, the anatomical location, the functional importance of the injured nerve, and the time elapsed since the injury. The principal indication for nerve grafting in the upper extremity and hand is the necessity to bridge a segmental defect when a tension-free neurorrhaphy cannot be accomplished through standard gap-management techniques. Segmental defects are most commonly the sequelae of extensive tissue destruction from avulsion injuries, blast trauma, shotgun wounds, or the mandatory radical resection of a terminal neuroma or glioma in delayed presentations. In the setting of delayed repair, the nerve ends have inevitably retracted, and the surrounding soft tissue bed is often heavily scarred, further precluding primary coaptation.
Beyond standard trauma, several highly specialized reconstructive scenarios necessitate nerve grafting. These include providing necessary motor innervation to free vascularized functioning muscle transfers, such as a gracilis free flap utilized in late-stage brachial plexus reconstruction or facial reanimation. Nerve grafts are also frequently indicated to innervate free neurovascular island flaps, restoring critical protective sensation to weight-bearing areas of the foot or the pinch-contact areas of the digits. Furthermore, extensive cable grafting remains a cornerstone in the reconstruction of the brachial plexus following severe post-ganglionic rupture injuries, where multiple contiguous nerve roots must be bridged to the distal cords or terminal branches.
Contraindications to nerve grafting must be carefully respected to avoid futile surgical endeavors and unnecessary donor site morbidity. Absolute contraindications include the presence of active, uncontrolled gross infection within the recipient bed, as the highly inflammatory milieu will destroy the delicate graft construct. Similarly, an exceptionally poor, avascular, or heavily irradiated soft tissue envelope precludes grafting, as the graft relies entirely on plasmatic imbibition and subsequent neovascularization from the surrounding bed for survival. A critical relative contraindication relates to the time elapsed since the injury. Motor endplates undergo irreversible degradation and muscle fibers undergo profound fatty atrophy and fibrosis typically between 12 to 18 months post-denervation. Consequently, placing a long nerve graft to a motor target after this critical window is physiologically unsound, as the regenerating axons will arrive at a target incapable of functional reinnervation; in such cases, tendon transfers or free functional muscle transfers are the indicated salvage procedures.
| Clinical Scenario / Parameter | Indications for Nerve Grafting / Conduits | Contraindications / Alternative Strategies Required |
|---|---|---|
| Defect Length | Gaps > 2-3 cm (Autograft); Gaps < 3 cm (Conduit/Allograft) | Gaps < 5 mm achievable without tension (Primary Repair) |
| Soft Tissue Bed | Well-vascularized, healthy muscle/fascial coverage | Irradiated bed, active infection, exposed bone without coverage |
| Timing of Motor Repair | < 6 to 12 months from time of injury | > 18-24 months (Irreversible motor endplate loss -> Tendon Transfer) |
| Donor Site Considerations | Expendable sensory nerve available (e.g., Sural, LABC) | Patient refusal of donor deficit; pre-existing neuropathy |
| Mechanism of Injury | Sharp segmental loss, resected neuroma, traction injury | Severe multilevel crush injury with indeterminate zones of injury |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful peripheral nerve reconstruction. The clinical evaluation must precisely delineate the anatomical level of the lesion, distinguishing between complete transection (neurotmesis) and lesions in continuity. The advancing Tinel's sign is a critical clinical marker; a stationary Tinel's sign over several months strongly suggests a dense neuroma requiring resection and grafting. Electromyography (EMG) and Nerve Conduction Studies (NCS) are essential adjuncts, though they must be timed appropriately (typically 3 to 4 weeks post-injury) to allow for the completion of Wallerian degeneration and the manifestation of denervation potentials (fibrillations and positive sharp waves) in the affected musculature. Increasingly, high-resolution ultrasonography and Magnetic Resonance Neurography (MRN) are utilized to visualize the neuroma, estimate the gap length prior to incision, and assess the quality of the proximal and distal nerve stumps.
Before committing to the harvest of an autogenous nerve graft, the surgeon must exhaust all conservative techniques for closing small gaps. Autogenous grafts inherent introduce two coaptation sites—two distinct physical barriers that regenerating axons must cross—which inherently reduces the final functional outcome compared to a single primary repair. Gap management techniques include extensive, yet careful, proximal and distal mobilization of the nerve ends, preserving the mesoneurial blood supply wherever possible. Joint positioning can be utilized; however, extreme flexion must be avoided. A clinical pearl dictates that if a joint must be flexed beyond 30 degrees to achieve coaptation, the repair will invariably fail due to traction injury when the joint is mobilized postoperatively. Other techniques include nerve transposition (e.g., anterior submuscular transposition of the ulnar nerve at the elbow) or, in the setting of replantation, skeletal shortening.
Patient positioning and operating room setup must accommodate simultaneous access to both the recipient site and the anticipated donor sites. For upper extremity reconstruction requiring a sural nerve graft, the patient is typically positioned supine with a bump under the ipsilateral hip to internally rotate the leg, allowing access to the posterolateral calf. A sterile tourniquet is applied to both the injured extremity and the donor limb to ensure a bloodless field during the critical phases of micro-dissection. The operating microscope must be positioned optimally, and a complete microsurgical instrumentation set—including jeweler's forceps, micro-scissors, vessel dilators, and a variety of 8-0 to 11-0 monofilament sutures—must be prepared. The surgeon must also anticipate the need for multiple donor nerves if a large-caliber polyfascicular nerve (like the sciatic or median nerve) requires extensive cable grafting.
Step-by-Step Surgical Approach and Fixation Technique
Preparation of the Recipient Bed and Nerve Stumps
The surgical approach begins with wide exposure of the injured nerve, extending proximally and distally into virgin, unscarred tissue before tracing the nerve into the zone of injury. Meticulous hemostasis is maintained using bipolar electrocautery. The proximal neuroma and distal glioma must be radically excised. This is performed using a fresh scalpel blade or specialized nerve cutting scissors, taking sequential 1-mm to 2-mm slices. The cut surface is inspected under high microscope magnification. Failure to adequately resect the scarred ends is the single most common cause of nerve graft failure. The surgeon must resect until healthy, unscarred fascicles are clearly visible. A reliable intraoperative indicator of healthy tissue is the "pouting" fascicle sign, where the endoneurial contents bulge slightly outward from the constraining perineurium, accompanied by punctate bleeding from the vasa nervorum.
Autogenous Graft Harvest and Preparation
When an autograft is selected, the sural nerve remains the workhorse donor due to its length (yielding up to 40 cm) and favorable fascicular matching for digital and mixed nerves. Harvest is performed either via a continuous longitudinal incision or a minimally invasive step-ladder incision technique. The nerve is identified posterior to the lateral malleolus, adjacent to the lesser saphenous vein, and traced proximally to its origin at the popliteal fossa. Once harvested, the graft is kept moist in heparinized saline. For large gaps in major peripheral nerves, the sural nerve is divided into multiple segments to create a "cable graft," matching the cross-sectional area of the recipient nerve. The grafts are typically reversed in orientation; placing the graft in a reversed fashion prevents regenerating axons from escaping down small branching vessels or terminal cutaneous branches inherent to the donor nerve.
Microsurgical Coaptation Techniques
Meticulous microsurgical technique under operating microscope magnification (typically 10x to 20x) is mandatory. The choice of neurorrhaphy technique depends on the fascicular architecture of the nerve.
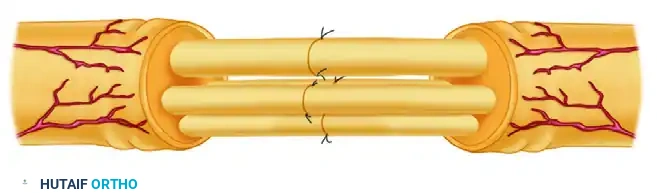
Perineurial (Fascicular) Neurorrhaphy: This technique is indicated when the nerve exhibits a distinct, oligofascicular pattern, allowing specific motor and sensory fascicular groups to be anatomically identified and matched.
* Step A: The epineurium is carefully excised and stripped back a few millimeters to expose the underlying fascicles. This is a critical step, as it prevents epineurial connective tissue from invaginating into the repair site, which would physically block axonal growth.

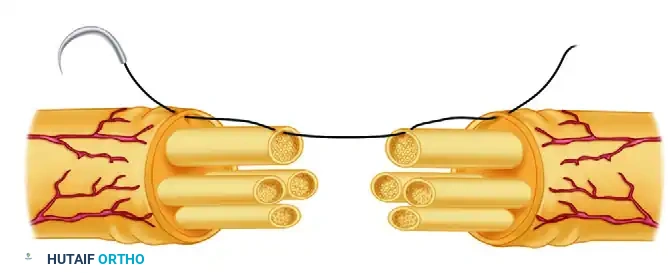
* Step B: A 10-0 or 11-0 nylon suture on a micro-spatula needle is passed precisely through the perineurium of corresponding fascicles on either side of the cut surface of the nerve. The needle must not penetrate the endoneurial contents.

* Step C: The neurorrhaphy is completed, usually requiring two to three 10-0 nylon sutures in each fascicle to ensure precise, watertight coaptation without buckling or mushrooming of the fascicular contents.
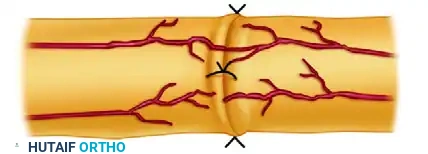
Epi-Perineurial Neurorrhaphy: This hybrid technique is highly effective for polyfascicular nerves. It utilizes the mechanical strength of the epineurium while ensuring precise alignment of the peripheral fascicular groups.
* Step A: The epineurium is excised and retracted slightly. The first suture is placed through the epineurium, near a large, identifiable fascicle at the periphery of the nerve, and then passed directly through the perineurium of that specific fascicle.

* Step B: The suture is then passed through the perineurium of the matching fascicle on the opposite side of the cut surface of the nerve, and finally out through the epineurium.
* Step C: The repair is completed after suturing other suitably matched fascicles around the periphery. This technique provides excellent rotational alignment and superior mechanical stability compared to purely fascicular repairs.
Conduit and Allograft Implantation
For gaps less than 3 cm, synthetic bioabsorbable conduits (e.g., Polyglycolic acid or Polycaprolactone) or decellularized nerve allografts offer excellent alternatives, eliminating donor site morbidity. Conduits act by isolating the regenerating nerve ends from surrounding scar tissue while allowing the accumulation of endogenous neurotrophic factors, creating a localized fluid microenvironment that guides fibrin cable formation.
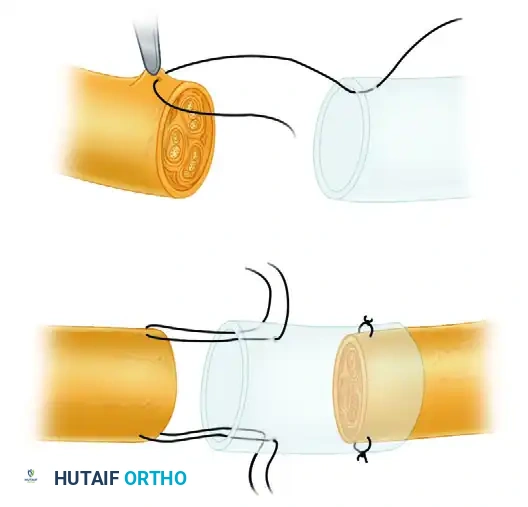
The Weber et al. Conduit Repair Technique: In this landmark technique, the proximal and distal nerve stumps are drawn into the bioabsorbable conduit using horizontal mattress sutures (typically 8-0 or 9-0 nylon).
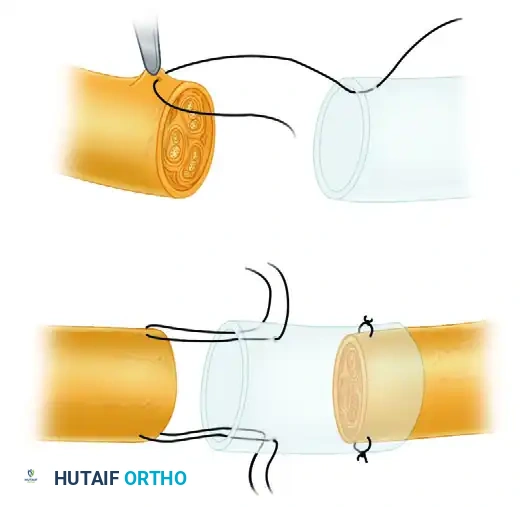
Crucially, the minimal distance between the nerve stumps inside the conduit must be maintained at exactly 5 mm, even in instances where the ends could theoretically be coapted without tension. This 5 mm gap is theorized to optimize the neurotrophic fluid environment, prevent axonal crowding, and allow for the sorting of sensory and motor fibers across the fibrin matrix.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical execution, peripheral nerve grafting is fraught with potential complications driven by the unpredictable nature of axonal biology and the hostile environment of the traumatized extremity. The most devastating complication is the complete failure of axonal regeneration across the graft, resulting in persistent anesthesia, intractable motor paralysis, and the eventual irreversible atrophy of target musculature. The incidence of graft failure correlates directly with the length of the graft, the age of the patient, and the delay to surgery. Grafts exceeding 10 cm in length, particularly in patients over 50 years of age, demonstrate significantly reduced rates of functional motor recovery.
Neuroma-in-continuity at the proximal coaptation site is another frequent complication, occurring in up to 10-15% of extensive cable grafts. This presents clinically as a highly irritable, painful mass with a stationary Tinel's sign and a cessation of distal neurological progression. This phenomenon is typically the result of inadequate initial resection of the proximal stump, leading to axonal escape and disorganized neuroma formation outside the graft construct. Donor site morbidity, particularly following sural nerve harvest, is an unavoidable consequence of autografting. While the sensory deficit on the lateral aspect of the foot is generally well-tolerated, up to 20% of patients report hyperesthesia, cold intolerance, or symptomatic neuroma formation at the proximal transection site of the donor nerve.
When a nerve graft definitively fails, or when the patient presents beyond the 18-to-24-month window of viable motor endplate survival, salvage procedures must be employed. Tendon transfers remain the traditional workhorse for restoring gross motor function (e.g., radial nerve palsy tendon transfers). However, regional nerve transfers (neurotization) have revolutionized salvage management. Techniques such as the Oberlin transfer (utilizing expendable fascicles of the ulnar nerve to reinnervate the biceps motor branch) or transferring the Anterior Interosseous Nerve (AIN) to the deep motor branch of the ulnar nerve allow for the introduction of fresh, powerful axons directly into the target muscle close to the motor endplate, bypassing the long, hostile environment of a proximal graft.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Complete Graft Failure | 15% - 30% (Length dependent) | Inadequate resection, tension, bed ischemia, >10cm gap | Nerve transfers (if early), Tendon transfers, Arthrodesis |
| Neuroma-in-Continuity | 10% - 15% | Axonal escape, poor coaptation, epineurial invagination | Resection and re-grafting, targeted muscle reinnervation (TMR) |
| Donor Site Neuroma | 5% - 20% | Superficial placement of donor stump, traction | Proximal relocation of stump into deep muscle belly |
| Conduit Extrusion/Reaction | < 5% | Superficial placement, poor soft tissue coverage | Removal of conduit, soft tissue flap coverage, autografting |
| Irreversible Muscle Atrophy | Time-dependent (>18 mos) | Delayed presentation, slow regeneration rate (1mm/day) | Free functional muscle transfer (e.g., Gracilis flap) |
Phased Post-Operative Rehabilitation Protocols
The technical success of a nerve graft in the operating theater is only the first step; the ultimate functional outcome relies heavily on strict adherence to a phased, biologically sound postoperative rehabilitation protocol. The rehabilitation strategy must balance the need to protect the fragile micro-coaptations from tensile forces while preventing debilitating joint contractures and facilitating cortical remapping.
Phase I: Protection and Immobilization (Weeks 0 to 3)
Immediately postoperatively, the extremity is immobilized in a bulky, non-compressive splint. The joints are positioned to minimize any tension on the graft site. For example, following a median nerve graft at the wrist, the wrist is placed in 20 to 30 degrees of palmar flexion. Extreme flexion must be avoided to prevent secondary crush or kinking of the graft. During this phase, the fibrin cable is forming, and initial axonal sprouting is crossing the proximal coaptation. Immobilization is absolute; only non-involved joints are mobilized to prevent generalized stiffness.
Phase II: Progressive Mobilization (Weeks 3 to 6)
At 3 weeks, the biological strength of the coaptation site has increased due to early epineurial fibrosis. The static splint is modified, or a dynamic splint is fabricated, and a supervised, progressive range-of-motion (ROM) program is initiated. Extension is regained gradually—typically at a rate of 10 degrees per week—over the next 3 to 4 weeks. This gradual elongation prevents sudden traction on the maturing fibrin cable and the delicate, advancing growth cones. Aggressive passive stretching is strictly contraindicated.
Phase III: Axonal Tracking and Motor Maintenance (Weeks 6 to 12+)
During this phase, the clinician meticulously tracks the advancing Tinel's sign, expecting a regeneration rate of approximately 1 mm per day (or 1 inch per month). For mixed or motor nerves, the target denervated musculature is at high risk for atrophy. Electrical stimulation of the denervated muscle using specific low-frequency, long-duration direct currents may be considered to maintain muscle bulk and contractility while awaiting reinnervation. Once voluntary motor unit potentials return (initially detectable only via EMG, later by visible flicker), biofeedback and gravity-eliminated strengthening exercises are initiated.
Phase IV: Sensory Re-education and Cortical Remapping (Months 3 to 24)
As regenerating sensory axons reach the target end-organs (Meissner's and Pacinian corpuscles), the patient will initially experience altered, often hypersensitive, perception. Because the axons rarely reinnervate their original endoneurial tubes precisely, the somatosensory cortex receives chaotic signals. A formal sensory re-education program is mandatory to drive cortical plasticity. Phase 1 sensory re-education begins before innervation reaches the fingertips, utilizing visual-tactile interaction to maintain cortical maps. Phase 2 begins once protective sensation returns, progressing from low-frequency vibration localization to advanced texture discrimination and blindfolded object identification.
Summary of Landmark Literature and Clinical Guidelines
The evolution of peripheral nerve grafting is deeply rooted in landmark anatomical studies and rigorous prospective clinical trials that have continuously refined surgical decision-making. The foundational classifications of nerve injury by Seddon (neurapraxia, axonotmesis, neurotmesis) and Sunderland (first through fifth-degree injuries) remain the bedrock upon which all reconstructive algorithms are built, dictating when observation is appropriate and when surgical intervention is mandatory.
The modern era of nerve gap management was significantly altered by the landmark randomized prospective study by Weber et al. (2000). This multicenter trial compared polyglycolic acid (PGA) conduits to standard primary repair and autologous nerve grafting for digital nerve defects. The study conclusively demonstrated that for gaps less than 3 cm, PGA conduits yielded functional outcomes equivalent to autografts, thereby eliminating donor site morbidity. Most notably, in patients with defects smaller than 4 mm, the results were statistically superior in the conduit repair group compared to primary repair. This led to the widespread adoption of the 5 mm gap technique within conduits to optimize the neurotrophic fluid environment.
Further advancements were highlighted by Bertleff et al., who investigated transparent polycaprolactone conduits, demonstrating their efficacy for gaps up to 2 cm while allowing direct visual confirmation of stump alignment during surgery. In the realm of large gap reconstruction, the work of Susan Mackinnon has been revolutionary, particularly in her advocacy for regional nerve transfers over long, poorly performing autografts for proximal motor lesions. More recently, the RANGER registry (Registry of Avance Nerve Graft's Extent of Recovery) has provided robust, multicenter data validating the use of processed, decellularized nerve allografts. The registry data indicates that allografts are highly effective and safe for sensory, mixed, and motor nerve gaps up to 5 cm, effectively bridging the therapeutic gap between synthetic conduits (limited to short gaps) and autografts (which carry the burden of donor morbidity). These contemporary guidelines mandate that the modern orthopaedic microsurgeon must be equally adept at primary repair, conduit implantation, allograft utilization, and complex autogenous cable grafting to optimize patient outcomes in peripheral nerve trauma.
